Immediate loading of variable-thread expanding tapered-body implants placed into maxillary post-extraction or healed sites using a guided surgery approach: An up-to-five-year retrospective analysis
September 23, 2016 / Categories: Digital Dentistry, Implant Dentistry

Giovanni, Polizzi
Cantoni, Tommaso
Emanuele, Pasini

Tallarico, Marco
Transitioning from failing dentition to complete-arch implant rehabilitation may involve temporarily rendering the patient edentulous. In order to avoid the use of a removable prosthesis, immediate implant placement and immediate loading with a fixed provisional prosthesis have been proposed.
Introduction
Transitioning from a failing dentition to completearch implant rehabilitation may involve temporarily rendering the patient edentulous.1Turkyilmaz I, Company AM, McGlumphy EA. Should edentulous patients be constrained to removable complete dentures? The use of dental implants to improve the quality of life for edentulous patients.
→ Gerodontology. 2010 Mar;27(1):3–10.
In such cases, interim complete removable dental prostheses have been used after extraction of the hopeless teeth and during the osseointegration period. However, many patients object to a complete removable dental prosthesis for psychological, functional or esthetic reasons, and request fixed provisionalization throughout all phases of the rehabilitation process.2Swelem AA, Gurevich KG, Fabrikant EG, Hassan MH, Aqou S. Oral health-related quality of life in partially edentulous patients treated with removable, fixed, fixedremovable, and implant-supported prostheses.
→ Int J Prosthodont. 2014 Jul-Aug;27(4):338–47.3Emami E, de Souza RF, Kabawat M, Feine JS. The impact of edentulism on oral and general health.
→ Int J Dent. 2013;2013:498305. doi: 10.1155/2013/498305. Epub 2013 May 8. In order to avoid the use of a removable prosthesis, immediate implant placement and immediate loading with a fixed interim prosthesis have been proposed for the rehabilitation of hopeless dentition.4Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. Five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery.
→ Clin Implant Dent Relat Res. 2015 Oct 7. doi: 10.1111/cid.12380. [Epub ahead of print]. Indeed, immediately loaded implants placed into postextraction sockets have recently been demonstrated to provide a reliable option for replacing failing residual teeth.5Degidi M, Nardi D, Piattelli A. 10-year follow-up of immediately loaded implants with TiUnite porous anodized surface.
→ Clin Implant Dent Relat Res. 2012 Dec;14(6):828–38. Although immediate loading may place implants at a higher risk of complications,6Atieh MA, Payne AG, Duncan WJ, Cullinan MP. Immediate restoration/loading of immediately placed single implants: is it an e ective bimodal approach? → Clin Oral Implants Res. 2009 Jul;20(7):645–59. comparable survival rates have been reported for the two loading protocols.7Tallarico M, Canullo L, Pisano M, Penarrocha-Oltra D, Penarrocha-Oltra M, Meloni SM. An up to 7-year retrospective analysis of biologic and technical complication with the All-on-4 concept.
→ J Oral Implantol. 2016 Jun;42(3):265–71. doi: 10.1563/ aaid-joi-D-15-00098. Epub 2015 Dec 11. Furthermore, immediate loading combined with implant placement in post extraction sites may result in improved esthetic outcomes owing to preservation of osseous and gingival architecture, o er reduced treatment time, and provide the patient with the convenience of an immediate tooth replacement.8De Rouck T, Collys K, Cosyn J. Single-tooth replacement in the anterior maxilla by means of immediate implantation and provisionalization: a review.
→ Int J Oral Maxillofac Implants. 2008 Sep-Oct;23(5):897–904. The risk of implant failure can be minimized by proper patient selection, welltrained operators, high primary implant stability and lack of micromovements.9Chen ST, Buser D. Clinical and esthetic outcomes of implants placed in postextraction sites.
→ Int J Oral Maxillofac Implants. 2009;24 Suppl:186–217.
Computer-aided design (CAD) technology allows for the transfer of patient data to a 3-D implant planning program for virtual implant placement.10Van Steenberghe D, Naert I, Andersson M, Brajnovic I, Van Cleynenbreugel J, Suetens P. A custom template and definitive prosthesis allowing immediate implant loading in the maxilla: a clinical report.
→ Int J Oral Maxillofac Implants. 2002 Sep-Oct;17(5):663–70. The virtual planning is then used to generate a custom-made surgical template (computer-aided manufacturing—CAM) with metallic sleeves to precisely guide each dental implant into the position planned virtually. In addition, implant-supported fixed acrylic resin prostheses can be fabricated in advance and immediately delivered to the patient. These aspects of minimally invasive and simplified surgery, along with reducing the treatment time and postoperative discomfort, are beneficial to the patient.11Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial.
→ Eur J Oral Implantol. 2014 Autumn;7(3):229–42. Favorable clinical results of computer-assisted template-guided surgery have been shown in several studies;12Vasak C, Kohal RJ, Lettner S, Rohner D, Zechner W. Clinical and radiological evaluation of a template-guided (Nobel- GuideTM) treatment concept.
→ Clin Oral Implants Res. 2014 Jan;25(1):116–23.13Vasak C, Watzak G, Gahleitner A, Strbac G, Schemper M, Zechner W. Computed tomography-based evaluation of template (NobelGuideTM)-guided implant positions: a prospective radiological study.
→ Clin Oral Implants Res. 2011 Oct;22(10):1157–63.14Vasak C, Strbac GD, Huber CD, Lettner S, Gahleitner A, Zechner W. Evaluation of three di erent validation procedures regarding the accuracy of template-guided implant placement: an in vitro study.
→ Clin Implant Dent Relat Res. 2015 Feb;17(1):142–9.15Van Assche N, Vercruyssen M, Coucke W, Teughels W, Jacobs R, Quirynen M. Accuracy of computer-aided implant placement.
→ Clin Oral Implants Res. 2012 Oct;23 Suppl 6:112–23. however, deviations in 3-D position between virtual planning and actual final position of the implant in the patient’s jaw and techniquerelated perioperative complications have to be taken into account.16Schneider D, Marquardt P, Zwahlen M, Jung RE. A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry.
→ Clin Oral Implants Res. 2009 Sep;20 Suppl 4:73–86.17Platzer S, Bertha G, Heschl A, Wegscheider WA, Lorenzoni M. Three-dimensional accuracy of guided implant placement: indirect assessment of clinical outcomes. → Clin Implant Dent Relat Res. 2013 Oct;15(5):724–34.18D’haese J, Van De Velde T, Komiyama A, Hultin M, De Bruyn H. Accuracy and complications using computer-designed stereolithographic surgical guides for oral rehabilitation by means of dental implants: a review of the literature.
→ Clin Implant Dent Relat Res. 2012 Jun;14(3):321–35.19Pettersson A, Komiyama A, Hultin M, Näsström K, Klinge B. Accuracy of virtually planned and template guided implant surgery on edentate patients. → Clin Implant Dent Relat Res. 2012 Aug;14(4):527–37.20Jung RE, Schneider D, Ganeles J, Wismeijer D, Zwahlen M, Hämmerle CH, Tahmaseb A. Computer technology applications in surgical implant dentistry: a systematic review.
→ Int J Oral Maxillofac Implants. 2009;24 Suppl:92–109.
In 2009, Cantoni and Polizzi described a step-by-tep technique involving a specially designed two-piece radiographic stent that allows the patient to retain hopeless teeth until the day of the surgery, making easier the transition from failing dentition to implant-supported prostheses.21Cantoni T, Polizzi G. Implant treatment planning in fresh extraction sockets: use of a novel radiographic guide and CAD/CAM technology.
→ Quintessence Int. 2009 Oct;40(9):773–81. The present study aimed to retrospectively assess the survival rate of variable-thread expanding tapered-body implants (NobelActive, Nobel Biocare, Zurich, Switzerland) placed into maxillary post-extraction or healed sites using template-guided surgery in combination with a specially designed radiographic stent.22Cantoni T, Polizzi G. Implant treatment planning in fresh extraction sockets: use of a novel radiographic guide and CAD/CAM technology.
→ Quintessence Int. 2009 Oct;40(9):773–81.This study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.23Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. → J Clin Epidemiol. 2008 Apr;61(4):344–9.
Materials and methods
This retrospective study evaluated data collected from 27 consecutive patients of both sexes (19 females, 8 males), aged 18 years or older (range of 38–84; mean of 60.6), presenting with failing maxillary dentition, confirmed by clinical and radiographic examination, and with a preference for a complete-arch implant-supported fixed dental prosthesis or an intolerance to a complete removable dental prosthesis. All of the implants were placed without elevation of a flap in maxillary post-extraction sockets or healed sites using computer-assisted template-guided surgery (Nobel-Guide, Nobel Biocare) between September 2009 and October 2012. The patients were clinically followed for a minimum of two years (range of two to five years; mean of 29 months). All of the patients were treated in a single specialized implant rehabilitation center. Two clinicians performed all of the surgical (GP) and prosthetic (TC) procedures, and two dental laboratories manufactured all of the restorations. One independent examiner (EP) conducted a retrospective chart analysis of the 27 consecutively implanted patients with compromised dentition in the maxilla.
Patients were informed about the clinical procedures, materials to be used, benefits, potential risks and complications, as well as follow-up evaluations required for the clinical trial, and gave their written consent to take part in this study. All of the procedures were conducted in accordance with the Declaration of Helsinki of 1975 for biomedical research involving human subjects, as amended in 2008. The patients were not admitted to the study if any of the following exclusion criteria were present: general contraindications to implant surgery; subjected to irradiation in the head and neck area less than one year before implantation; untreated periodontitis; poor oral hygiene and motivation; uncontrolled diabetes; pregnant or nursing; substance abuse; psychiatric problems or unrealistic expectations; severe bruxism or clenching; immunosuppressed or immunocompromised; treated or under treatment with intravenous amino-bisphosphonates; lack of opposite occluding dentition or prosthesis in the area intended for implant placement; active infection or severe inflammation in the area intended for implant placement; and need of bone augmentation procedures at implant placement.
-

- Fig. 1
-

- Fig. 2a
-
- Fig. 2b
Fig. 1
Initial clinical situation of a female patient with hopeless teeth in the maxilla.
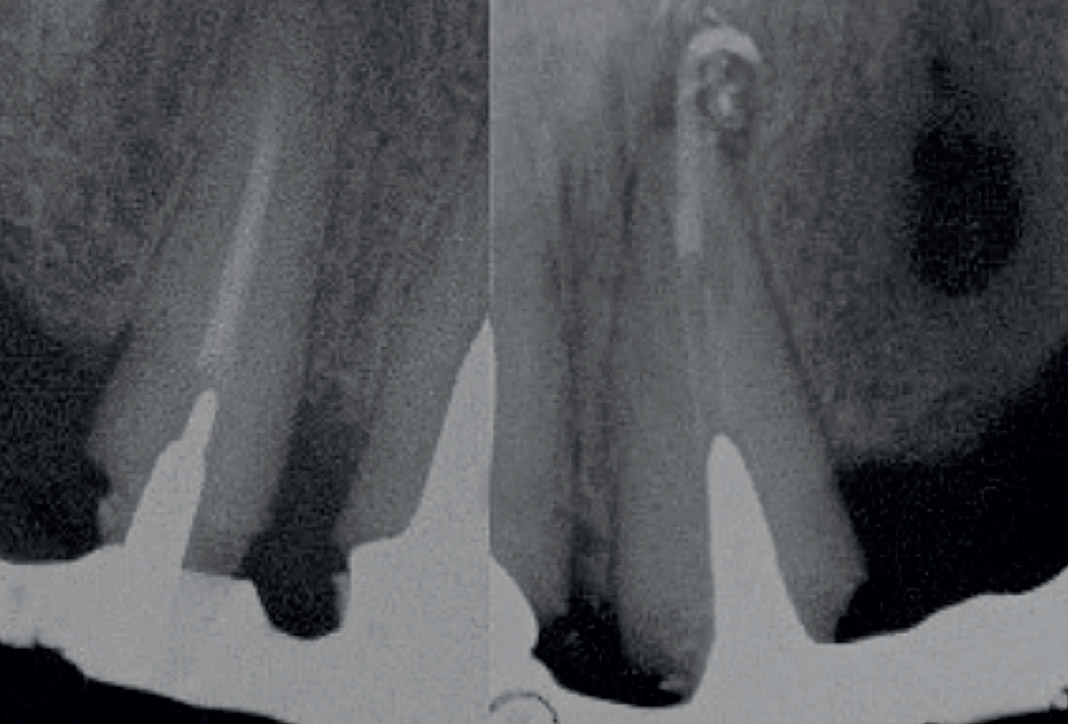
Figs. 2a & 2b
Initial radiographic situation of a female patient with hopeless teeth in the maxilla.
Fig. 3
Two-piece radiographic stent used for the CBCT scan.
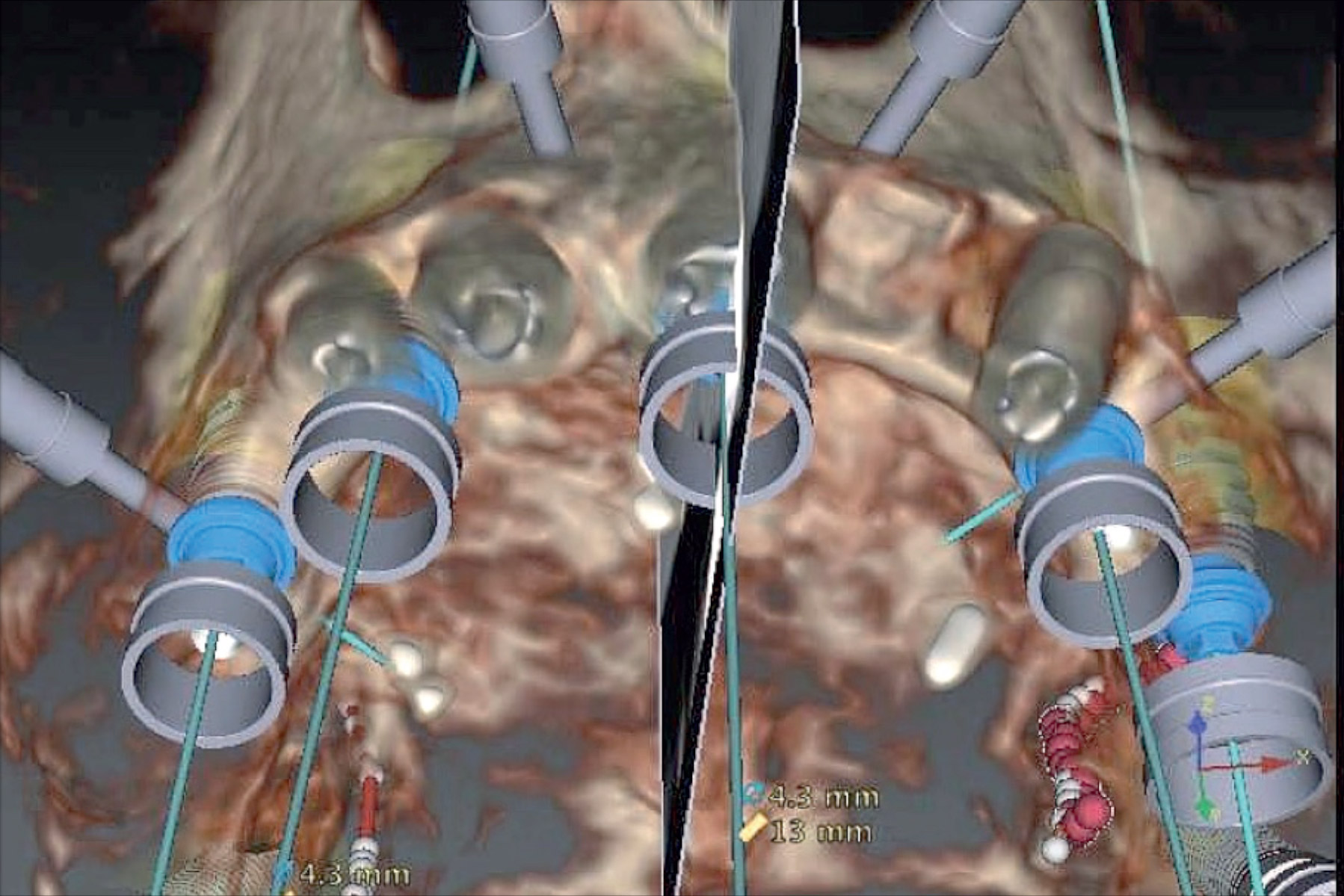
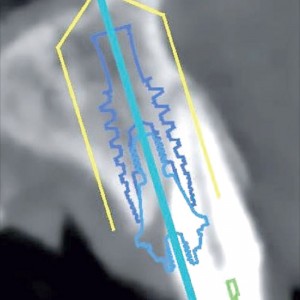
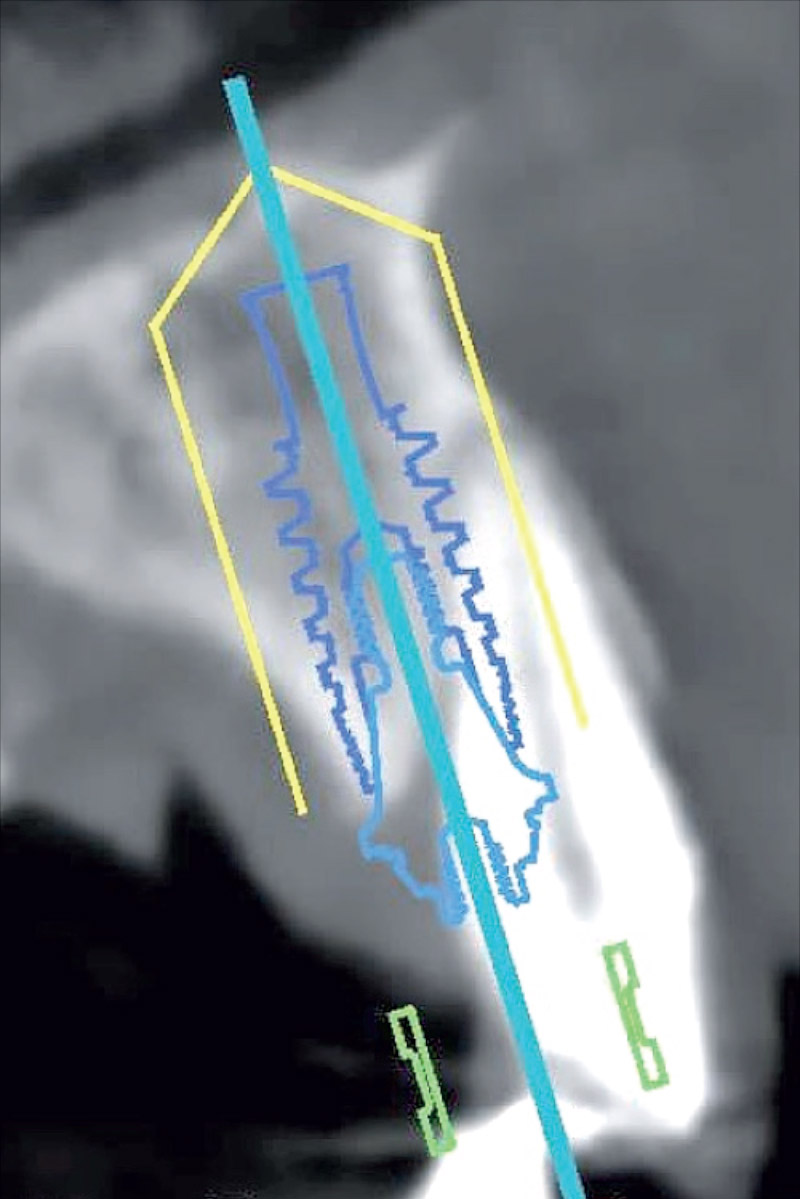
Figs. 4a & 4b
Implant planning with teeth still in place. (a) Occlusal view. (b) Cross-sectional image.
Diagnostic protocol
The patients’ medical histories were recorded and preoperative photographs (Fig. 1) and radiographs, including periapical (Figs. 2a & b) and panoramic radiographs, were obtained for initial screening and evaluation. Before implant placement, all of the patients underwent a cone beam computed tomography (CBCT) scan (New Tom VGi, Quantitative Radiology, Verona, Italy) according to a double-scan protocol.10 A two-piece radiographic guide was used for the diagnostic study and the virtual implant planning according to previously described procedures (Fig. 3) .24Cantoni T, Polizzi G. Implant treatment planning in fresh extraction sockets: use of a novel radiographic guide and CAD/CAM technology.
→ Quintessence Int. 2009 Oct;40(9):773–81.
In order to predictably obtain a surgical template with the same fitting dimensions as the originally scanned radiographic guide, the NobelGuide calibration procedure was performed for each patient according to the manufacturer’s instructions, using a specific calibration object. Finally, the two data sets were converted with the NobelGuide software to preview the patient’s anatomy and to plan treatment (Figs. 4a & b) . Once planning had been completed, the surgical template was ordered.
-

- Fig. 3
-
- Fig. 4a
-
- Fig. 4b
Surgical and prosthetic protocols
Antimicrobial prophylaxis with amoxicillin 1 g (Zimox, Pfizer, Rome, Italy) or clindamycin 600 mg, if allergic to penicillin, was administered b.i.d. for six days, starting 2 h before surgery. Prior to the start of surgery, patients rinsed with a 0.2% chlorhexidine mouthwash for 1 min. Oral premedication with flurazepam monohydrochloride 15 mg (Flunox, Teofarma, Pavia, Italy), octatropine methyl bromide 40 mg and diazepam 5 mg (Valpinax, Crinos, Milan, Italy) was given prior to surgery. Local anesthesia was induced by infiltration of the buccal and palatal regions of the surgical area with a 4% articaine solution with 1:200,000 epinephrine (Ubistesin, 3M Italia, Bergamo, Italy). Conscious sedation with midazolam 0.05–0.15 mg/kg IV (Ipnovel, Roche, Monza, Italy) was performed; ranitidine 100 mg IV (Ranidil, Menarini, Florence, Italy) and ondansetron 4 mg IV (Zofran, GlaxoSmithKline, Brentford, U.K.) were also administered for gastroprotection and prevention of nausea and vomiting. A single postoperative dose of dexamethasone 8 mg IV (Decadron, Visufarma, Rome, Italy) and ketorolac 30 mg IV (Toradol, Recordat, Rome, Italy) was also given.
Hopeless teeth were atraumatically extracted with the aid of a periotome (PT2, Hu-Friedy, Chicago, Ill., U.S.) and the sockets debrided. In cases of multiple-rooted teeth, a rhizotomy was performed, starting from the center of the tooth, followed by careful extraction of the individual roots to prevent damage to the alveolar walls. Upon completion of the extraction, the integrity, depth and inclination of the alveolar socket were checked with a periodontal probe. The surgical templates were positioned using the silicone surgical index derived from the mounted casts, and precise fit was visually and manually assessed. The surgical template was then stabilized with three to five preplanned anchor pins. All of the implants were placed through metallic sleeves in a fully guided surgery approach. Implant sites were prepared according to the manufacturer’s guidelines. Furthermore, a guided screw tapping was performed for half the depth of the osteotomy site, in order to provide an accurate and passive pressure-free seating of the implant into the prepared osteotomy. The bone tap was performed as the last step immediately prior to implant placement. Care was taken not to overheat the bone during the tapping procedure. The bone taps were removed from the site through counterclockwise rotation. Both tapping and implant placement were performed at 20 rpm. In the healed sites, the implant platform was positioned at the bone level, while in immediate post-extraction sockets, the platform was placed 1 mm deeper, below the buccal bone crest, engaging at least 3 mm of the bone apical to the root apex to achieve adequate primary stability of at least 35 N cm (range of 35–70 N cm; mean and standard deviation of 57.1 ± 13.4 N cm).
The residual gap between the buccal bone plate and the implant surface was filled with a mixture of autogenous bone and freeze-dried deproteinized bovine bone (Geistlich Bio-Oss,Geistlich Pharma, Wolhusen, Switzerland). In extraction sockets presenting severe buccal bone dehiscence, the socket was sealed with a collagen membrane (Geistlich Bio-Gide, Geistlich Pharma) or with a connective tissue graft and left to heal without implant placement.
All of the implants were immediately loaded with a metal-reinforced, screw-retained acrylic resin provisional restoration without any cantilever. All of the restorations were prefabricated on a master cast poured from the surgical template, with the implant replica on-site. Nonengaging titanium temporary abutments were connected at the implant or abutment level. The provisional restoration was placed in the mouth and assessed for passive fit around the abutments. If any tension was detected, more space was provided by adjusting the provisional restoration. Once the prosthesis had been completely seated, a preliminary occlusal adjustment was performed. Using a disposable syringe filled with a cold-cure acrylic resin, the abutments were then connected to the temporary restoration by injecting the resin into the space between the abutments and the framework, having the pa-tient close into occlusion. When the cold-cure acrylic resin had fully set, the provisional restoration was unscrewed from the mouth. The restoration was then refined, polished and screwed into the patient’s mouth approximately 2–3 h later. A final check of the occlusion and of the interproximal spaces was then performed. The screw access holes were closed with PTFE and temporary filling material. Periapical radiographs of all of the implants were then obtained. All of the patients received postoperative instructions and prescriptions. In addition, an oral antiseptic and soft brushing were recommended for the first two weeks. Patients were recalled for clinical (Figs. 5a & b) and radiographic (Figs. 6a–c) examination and oral hygiene checks at two and four weeks, three, six and 12 months, and then yearly up to five years after implant placement. On average, the provisional fixed restorations were removed after six months and replaced with titanium or zirconia CAD/CAM screw-retained prostheses, with acrylic or ceramic esthetic material.
-

- Fig. 5a

-

- Fig. 5b

-
- Fig. 6a
-
- Fig. 6b
-
- Fig. 6c
Figs. 5a & 5b
Clinical situation after implant treatment at five years of follow-up. (a) Frontal view.
(b) Lateral view.
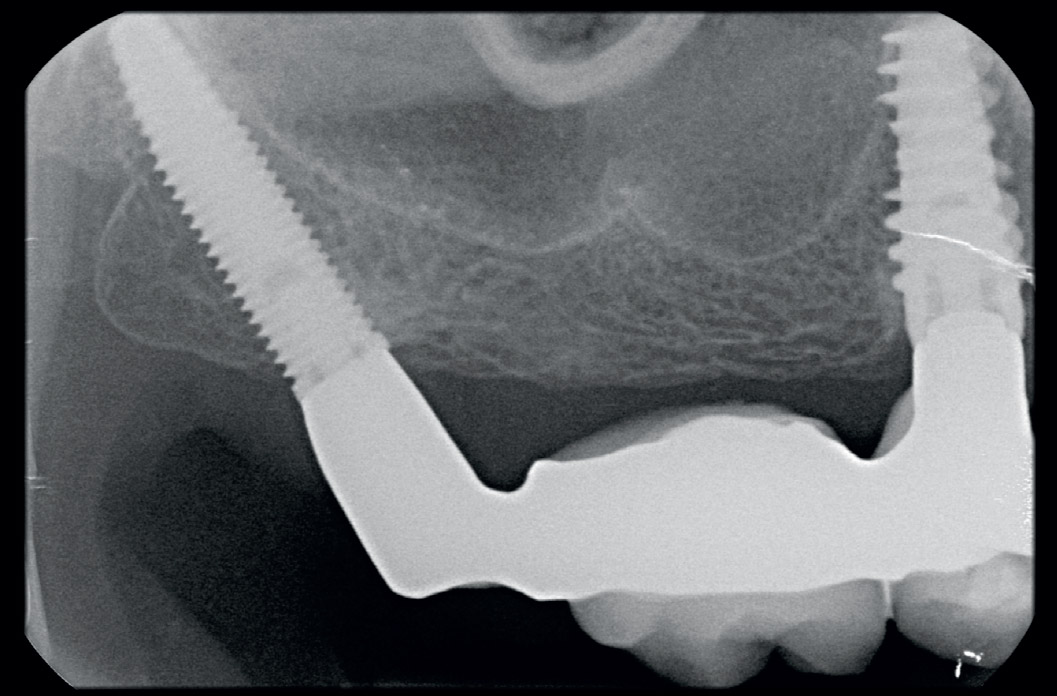
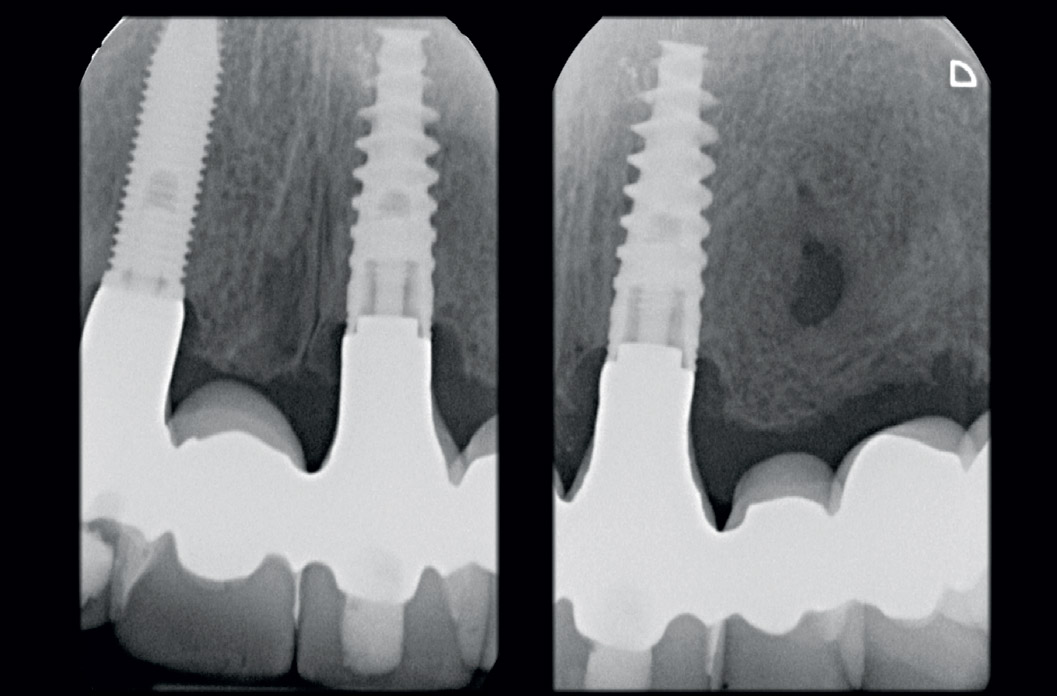
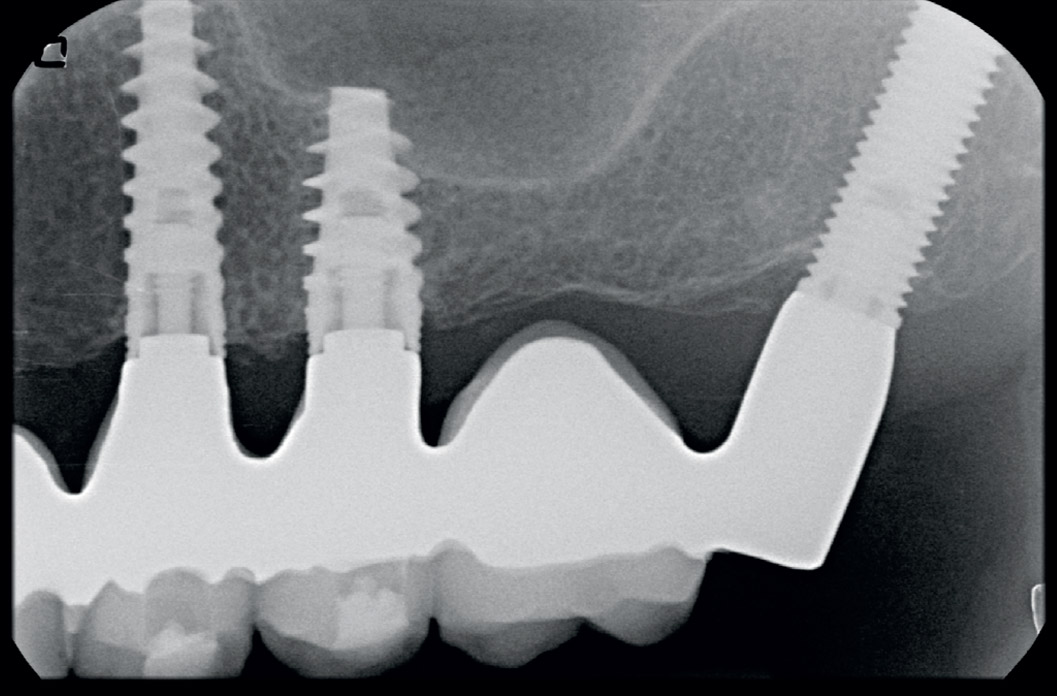
Figs. 6a-c
Radiographic situation after implant treatment at five years of follow-up.
Outcomes
The primary outcomes were implant and prosthetic survival and success rates assessed 15 days after prosthesis delivery and then yearly up to five years after surgery, according to Papaspyridakos et al.25Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: a systematic review.
→ J Dent Res. 2012 Mar;91(3):242–8. This investigation’s prosthetic survival and success rates were defined as follows: a successful implant-supported dental prosthesis was a prosthesis that remained in function and the esthetic evaluation of which by both the dentist and patient was satisfactory at delivery and during the study period; a surviving implant-supported dental prosthesis was a prosthesis that remained in function even though not all success criteria were fulfilled and any discrepancies were regarded as correctable; and a failed implant-supported dental prosthesis was a prosthesis that had been removed, fractured beyond repair, or could not be classified as a successful or surviving dental prosthesis.
The secondary outcomes were any biological (pain, swelling, suppuration, etc.) and/or mecha- nical complications (fracture of the framework and/or the veneering material, screw loosening, etc.) occurring during the entire follow-up period, marginal bone level (MBL) changes, and periodontal parameters.
The distance from the most coronal margin of the implant collar to the most coronal point of bone-to-implant contact was defined as the MBL. The MBL around the implants was evaluated on intra-oral digital radiographs taken with the paralleling technique using a film-holder (Rinn XCP, DENTSPLY, Elgin, Ill., U.S.) at implant placement (baseline) and then annually. The radiographs were accepted or rejected for evaluation based on the visibility of the implant threads. All readable radiographs were displayed in an image analysis program (Scion Image 4.0.2 for Windows, Scion Corporation, Frederick, Md., U.S.) on a 24-in. LCD screen (iMac, Apple, Cupertino, Calif., U.S.) and evaluated under standardized conditions (according to ISO 12646:2004). The software was calibrated for each image using the implant diameter. Measurements of the mesial and distal bone crest level adjacent to each implant were made, with accuracy of 0.01 mm, and averaged at the implant level. Marginal bone remodeling was calculated as the di erence between the reading at the follow-up examination and the baseline value. Three groups were created in order to avoid bias in marginal bone remodeling: all implants, implants placed into postextraction sites and implants placed into healed sites.
Periodontal parameters around the implants were assessed at the last follow-up examination. The sulcus bleeding index was assessed using a plastic periodontal probe (Plast-o-Probe, DENT-SPLY Maillefer, Ballaigues, Switzerland) at four sites around each implant (mesial, distal, buccal and lingual), according to the Mombelli Index,26Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis. → Periodontol 2000. 1998 Jun;17:63–76. and was reported at the implant level. The plaque score was recorded using a plastic periodontal probe (Plast-o-Probe) and defined as the presence of plaque (yes/no) on the abutment– restoration complex. The gingival index was defined as follows: 0 = normal gingiva; 1 = mild inflammation, slight change in color, slight edema, and no bleeding on probing; 2 = moderate inflammation, redness, edema, glazing, and bleeding on probing; and 3 = severe inflammation, marked redness and edema, ulceration and tendency to spontaneous bleeding.
Implant and prosthetic survival and success rates were evaluated by an independent dentist (EP). Complications were assessed and treated by a nonblinded treating clinician (GP). The marginal bone remodeling was evaluated by an independent radiologist. An independent blinded dental hygienist who was not involved in the study performed all of the periodontal measurements.
Statistical analysis
Statistical analysis was performed using SPSS for Windows (Version 18.0; SPSS, Chicago, Ill., U.S.). Descriptive analysis was performed using mean, standard deviation and frequency distribution. A life table analysis of implant cumulative survival rates (CSRs) was calculated. Kaplan– Meier survival analysis was performed to allow estimation of survival over time, even when patients dropped out or were followed for di erent lengths of time. The Wilcoxon signed-rank test for paired data was utilized to compare overall bone levels between baseline (implant placement) and follow-ups in both healed and postextraction sites, and to compare bone remodeling between post-extraction and healed sites at the last follow-up examination. The implant was used as the statistical unit of the analysis. All statistical comparisons were conducted at the 0.05 level of significance.
Results
All 27 selected and analyzed patients met the inclusion criteria. Patients received a total of 160 NobelActive implants (22 narrow diameter, 106 regular diameter and 32 wide diameter) with a moderately rough surface (highly crystalline and phosphate-enriched titanium oxide). One hundred and five implants were placed into healed sites and 55 into post-extraction sockets. Each patient received at least one post-extraction implant. Patients were clinically followed for up to five years.
At the last follow-up, no patients had dropped out and no deviation from the original protocol had occurred. All of the collected data were included in the statistical analysis. Only one post-extraction implant failed in one patient, who showed poor oral hygiene, during the second year, and showed clinical signs of mobility and infection, resulting in an overall implant CSR of 99.4%. The life table analysis is summarized in Table 1. All prostheses were in situ at the last follow-up, accounting for a cumulative prosthetic survival rate of 100% up to five years after insertion.
Two implants (1.25%) showed marginal bone remodeling of greater than 3 mm at the last follow-up. However, none of the implants presented with an exposed implant neck, and no surgical intervention was performed. All of the a ected patients underwent nonsurgical therapy consisting of manual debridement using titanium curettes and a glycine-based air–powder abrasive device, and local application of antimicrobial agents (minocycline HCl 1 mg, Arestin, OraPharma, Horsham, Pa., U.S.), followed by oral hygiene instructions and motivation, together with a strict follow-up protocol. At the subsequent follow-ups, the bone recession had stopped and the soft tissue remained stable. No other biological or mechanical complications occurred during the entire follow-up period, resulting in a cumulative implant and prosthetic success rate of 97.9%.
At the last follow-up (mean of 29 months), the marginal bone remodeling was 0.58 ± 0.98 mm. Implants placed into postextraction sockets (0.42 ± 0.99 mm) showed statistically lower marginal bone remodeling compared with implants placed into healed sites (0.67 ± 0.97 mm; P = 0.026).
At the last follow-up session, bleeding after careful insertion of a periodontal probe 1 mm into the mucosal sulcus parallel to the abutment surface was detected around three implants (1.6%).
Twelve patients with 68 implants showed a slight amount of plaque around the implant–abutment interface; thus, the overall plaque score was 36.0% and 44.4% at implant and patient level, respectively. The gingival index was reported as 90.5% normal gingiva, 7.9% with mild inflammation and 1.6% with moderate inflammation.
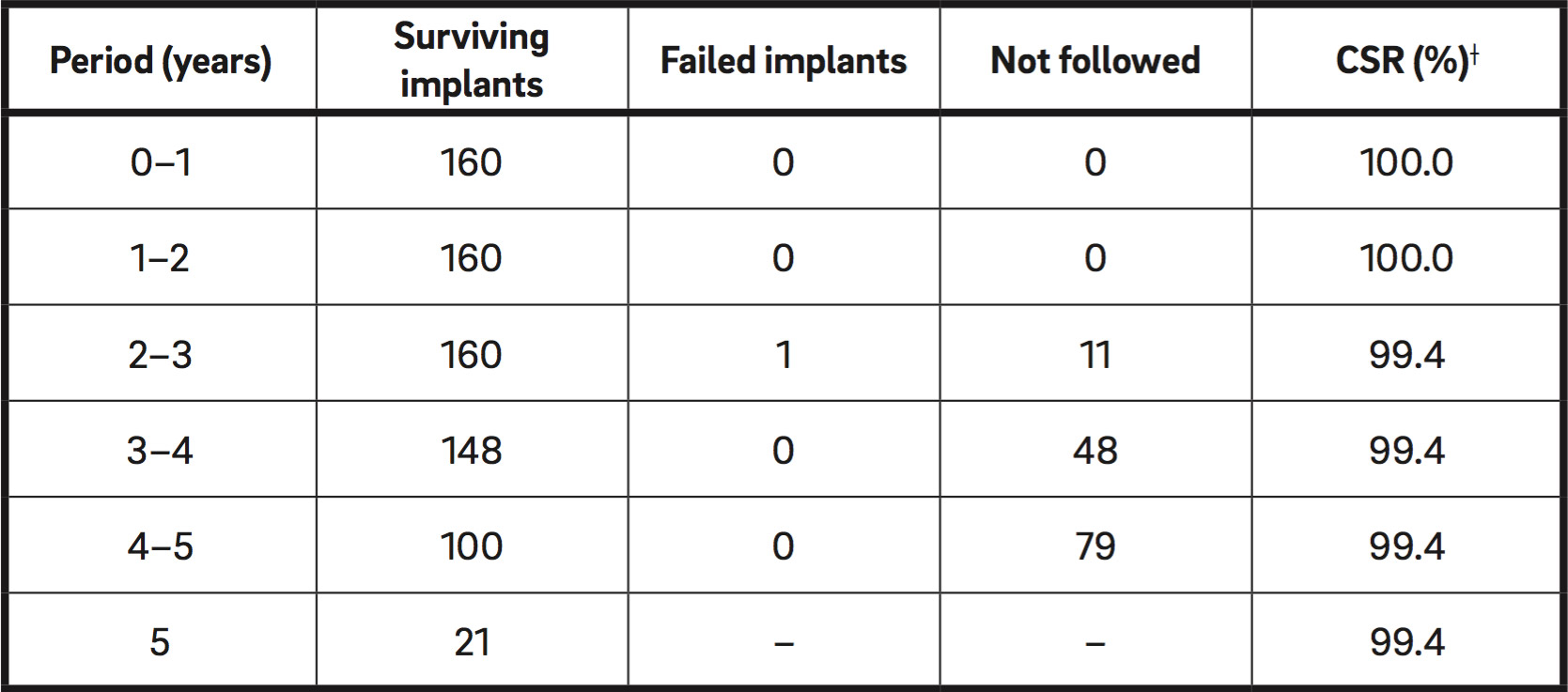
* According to the last recorded patient follow-up. † Cumulative survival rate.
Table 1
Life table analysis of all surviving implants.*
Discussion
This study retrospectively evaluated the success and survival rates of variable-thread tapered-body implants placed into post-extraction or healed sites in the maxilla using computer-assisted template-guided surgery in combination with a specially designed two-piece radiographic stent.27Cantoni T, Polizzi G. Implant treatment planning in fresh extraction sockets: use of a novel radiographic guide and CAD/CAM technology.
→ Quintessence Int. 2009 Oct;40(9):773–81.
The main limitations of this study are its retrospective nature, which may have limited the data collection, and the analysis of possible variables (soft-tissue thickness, time of placement or loading) that may have influenced the bone resorption. Another limitation is the limited number of participants. However, this investigation may be considered as a pilot study for future multicenter randomized controlled trials with sample size calculation and multivariate analysis.
Implants placed into post-extraction sockets showed lower marginal bone remodeling than implants placed into healed sites did; thus, the null hypothesis that there is no di erence between the two protocols in terms of hard-tissue response has to be rejected.
In the present study, one out of 160 implants failed over a period of five years, accounting for an overall implant CSR of 99.4%. The major clinical conclusion of this retrospective study is that immediate post-extraction placement of implants and immediate provisionalization may be considered an e ective and reliable treatment option for patients who would prefer to have a shortened overall treatment time and to be rehabilitated immediately with the aid of computer-assisted template-guided surgery.
Proper patient selection and well-trained operators are necessary to minimize the risk of implant failure. Immediate implant placement and provisionalization in both post-extraction sockets and healed sites are technically demanding procedures, and the surgical and prosthetic skills required are superior to those necessary for conventional implant treatment.
To the best of our knowledge at the time of writing this article, there were no other published studies that evaluated the use of a variable-thread tapered-body implant with internal conical connection, in-built platform shifting and a moderately rough oxidized surface in combination with computer-assisted template-guided surgery to treat failing dentition in the maxilla. For this reason, it is di icult to evaluate how the present results fit with other comparable studies. However, there is a randomized controlled trial that investigated the same implant design that may provide some comparable data.28Pozzi A, Tallarico M, Moy PK. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with di erent prosthetic interfaces and design in partially posterior edentulous mandibles.
→ Eur J Oral Implantol. 2014 Spring;7(1):47–61.
The marginal bone remodeling reported in the present study, measured from implant placement until the last follow-up examination, was 0.58 ± 0.98 mm. This value is slightly lower than the data reported in the literature for two-piece implants, for which after the initial bone loss during the first year post-placement, about 0.1–0.2 mm of crestal bone loss was found at the annual follow-up.29Bahat O, Sullivan RM. Parameters for successful implant integration revisited part I: immediate loading considered in light of the original prerequisites for osseointegration.
→ Clin Implant Dent Relat Res. 2010 May;12 Suppl 1:e2–12.30Bahat O, Sullivan RM. Parameters for successful implant integration revisited part II: algorithm for immediate loading diagnostic factors.
→ Clin Implant Dent Relat Res. 2010 May;12 Suppl 1:e13–22. Pozzi et al. recently published three-year results of a randomized controlled trial, reporting a marginal bone remodeling of 0.83 ± 0.27 mm around NobelActive implants placed into healed sites in the posterior mandible.31Pozzi A, Tallarico M, Moy PK. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with di erent prosthetic interfaces and design in partially posterior edentulous mandibles.
→ Eur J Oral Implantol. 2014 Spring;7(1):47–61. One reason for these di erences may be that surgeons operating freehand tend to elevate wider flaps to better visualize the area in which the implants are to be placed. With dedicated template-guided implant placement, wider flaps were in many cases considered unnecessary, since the surgeons were able to rely on the surgical template.11 Another explanation that may account for the di erences in the observed MBL changes is that, in some of the aforementioned studies, all of the implants were placed into healed sites.32Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial.
→ Eur J Oral Implantol. 2014 Autumn;7(3):229–42. 33Pozzi A, Tallarico M, Moy PK. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with di erent prosthetic interfaces and design in partially posterior edentulous mandibles.
→ Eur J Oral Implantol. 2014 Spring;7(1):47–61.In the present study, statistical analysis showed a statistically significant di erence (P = 0.026) in mean marginal bone remodeling at the last follow-up between implants placed into healed sites (0.67 ± 0.97 mm) and those placed into post-extraction sites (0.42 ± 0.99 mm). These findings are in accordance with a recent systematic review and meta-analysis on the alterations of the bone dimension after immediate implant placement into extraction sockets.34Lee CT, Chiu TS, Chuang SK, Tarnow D, Stoupel J. Alterations of the bone dimension following immediate implant placement into extraction socket: systematic review and meta-analysis.
→ J Clin Periodontol. 2014 Sep;41(9):914–26.
In the present study, the diagnostic protocol included the calibration procedure of the digital workflow for each patient, according to the manufacturer’s instructions. Scanning physical objects like the radiographic guide requires an optimized workflow, because the data are converted into 3-D models, which are used not only for diagnostic purposes but also for physical production. Since the data are digitized using X-ray technology and since material properties or densities are visualized through various kinds of gray value shades, the workflow is highly dependent on the gray values assigned to the scanned 3-D data from the DICOM files. More precisely, the workflow is dependent on the actual gray value that defines the radiographic guide’s borders. This gray value assignment to the DICOM files is unfortunately not standardized for CBCT scanners (almost every scanner assigns di erent gray values to di erent objects and materials), making reliable default values for each scanner model almost impossible. This ultimately has implications regarding the produced dimensions of the surgical template, as these dimensions are defined by the gray value selection representing the borders of the scanned radiographic guide. In order to automatically detect and automatically apply the correct settings needed for the software to define the actual physical borders of the scanned radiographic guide, NobelClinician (Nobel Biocare) is designed to work with the unique and innovative NobelGuide calibration procedure. The calibration object is a highprecision object, milled from a material that behaves the same way when penetrated by X-rays as the resins typically used for the radiographic guide in combination with the scanner. This process ensures that each time the CBCT scanner is used with a known scanner the surgical template produced will have the same fitting dimensions as the originally scanned radiographic guide. As a result, the procedure does not calibrate the scanner, but calibrates the full workflow, from an accurately fitting radiographic guide to an accurately fitting surgical template.
Many factors are likely to a ect the success of immediately loaded implants, including bone quality and quantity, the skill and experience of the clinician, implant design, implant primary stability, microand macromovement, as well as occlusion. The quality and quantity of bone at the implant site have been shown to be important in determining the success of dental implants and are critical for ensuring the initial stability of the implant upon insertion.35Papaspyridakos P, Chen CJ, Chuang SK, Weber HP. Implant loading protocols for edentulous patients with fixed prostheses: a systematic review and meta-analysis.
→ Int J Oral Maxillofac Implants. 2014;29 Suppl:256–70. Primary implant stability and lack of micromovement are considered to be two of the main factors necessary for achieving predictable high success rates for osseointegrated oral implants.36Albrektsson T, Linder L. A method for short- and long-term in vivo study of the bone-implant interface.
→ Clin Orthop Relat Res. 1981 Sep;159:269–73.Thus, a high insertion torque value appears to be one of the prerequisites for a successful immediate or early loading procedure. The variable-thread tapered implant design with a moderately rough surface was introduced into the market to facilitate one-stage surgical procedures and to allow for immediate placement and anticipated loading protocols.37Kielbassa AM, Martinez-de Fuentes R, Goldstein M, Arnhart C, Barlattani A, Jackowski J, Knauf M, Lorenzoni M, Maiorana C, Mericske-Stern R, Rompen E, Sanz M. Randomized controlled trial comparing a variable-thread novel tapered and a standard tapered implant: interim one-year results.
→ J Prosthet Dent. 2009 May;101(5):293–305. According to the results of the present study, in which all of the patients included had failing maxillary dentition and refused interim complete removable dental prostheses, the major indication for such implants is medium or low density bone sites in the maxilla. Nevertheless, a slight modification of the original drilling protocol was adopted in that implant sites were underprepared according to the bone density. However, a guided screw tapping for half the depth of the osteotomy site was performed immediately before the implant placement. Great care was taken to ensure optimal accuracy during implant placement because the implant mount had a smaller diameter than that of the sleeve. Nevertheless, this feature allowed the clinician to perceive the implant stability within the bone, without any friction between the implant mount and the sleeve.
Conclusion
Within the limitations of this retrospective study, variable-thread tapered design implants placed using computer-assisted template-guided surgery, in combination with a specially designed two-piece radiographic stent, can be considered a successful treatment option for immediate implant placement and loading in the maxillae of completely edentulous patients, based on the results of up to five years of follow-up. Post extraction implants showed statistically lower marginal bone remodeling compared with implants placed into healed sites. The results should be interpreted with care and data should be investigated further in randomized controlled clinical trials.
Competing interests
The authors declare that they have no competing interests related to this study. No financial support was received for this study.
Interview
with Dr. Polizzi Giovanni
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
It is the first clinical investigation in which the NobelGuide calibration procedure was performed for each patient, using a specific calibration object, according to a double-scan protocol. The importance of that is that a surgical template is predictably obtained with the same fitting dimensions as the originally scanned radiographic guide, resulting in improved accuracy of the guided surgery.
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Turkyilmaz I, Company AM, McGlumphy EA. Should edentulous patients be constrained to removable complete dentures? The use of dental implants to improve the quality of life for edentulous patients. → Gerodontology. 2010 Mar;27(1):3–10. |
| 2. | ↑ | Swelem AA, Gurevich KG, Fabrikant EG, Hassan MH, Aqou S. Oral health-related quality of life in partially edentulous patients treated with removable, fixed, fixedremovable, and implant-supported prostheses. → Int J Prosthodont. 2014 Jul-Aug;27(4):338–47. |
| 3. | ↑ | Emami E, de Souza RF, Kabawat M, Feine JS. The impact of edentulism on oral and general health. → Int J Dent. 2013;2013:498305. doi: 10.1155/2013/498305. Epub 2013 May 8. |
| 4. | ↑ | Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. Five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery. → Clin Implant Dent Relat Res. 2015 Oct 7. doi: 10.1111/cid.12380. [Epub ahead of print]. |
| 5. | ↑ | Degidi M, Nardi D, Piattelli A. 10-year follow-up of immediately loaded implants with TiUnite porous anodized surface. → Clin Implant Dent Relat Res. 2012 Dec;14(6):828–38. |
| 6. | ↑ | Atieh MA, Payne AG, Duncan WJ, Cullinan MP. Immediate restoration/loading of immediately placed single implants: is it an e ective bimodal approach? → Clin Oral Implants Res. 2009 Jul;20(7):645–59. |
| 7. | ↑ | Tallarico M, Canullo L, Pisano M, Penarrocha-Oltra D, Penarrocha-Oltra M, Meloni SM. An up to 7-year retrospective analysis of biologic and technical complication with the All-on-4 concept. → J Oral Implantol. 2016 Jun;42(3):265–71. doi: 10.1563/ aaid-joi-D-15-00098. Epub 2015 Dec 11. |
| 8. | ↑ | De Rouck T, Collys K, Cosyn J. Single-tooth replacement in the anterior maxilla by means of immediate implantation and provisionalization: a review. → Int J Oral Maxillofac Implants. 2008 Sep-Oct;23(5):897–904. |
| 9. | ↑ | Chen ST, Buser D. Clinical and esthetic outcomes of implants placed in postextraction sites. → Int J Oral Maxillofac Implants. 2009;24 Suppl:186–217. |
| 10. | ↑ | Van Steenberghe D, Naert I, Andersson M, Brajnovic I, Van Cleynenbreugel J, Suetens P. A custom template and definitive prosthesis allowing immediate implant loading in the maxilla: a clinical report. → Int J Oral Maxillofac Implants. 2002 Sep-Oct;17(5):663–70. |
| 11, 32. | ↑ | Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial. → Eur J Oral Implantol. 2014 Autumn;7(3):229–42. |
| 12. | ↑ | Vasak C, Kohal RJ, Lettner S, Rohner D, Zechner W. Clinical and radiological evaluation of a template-guided (Nobel- GuideTM) treatment concept. → Clin Oral Implants Res. 2014 Jan;25(1):116–23. |
| 13. | ↑ | Vasak C, Watzak G, Gahleitner A, Strbac G, Schemper M, Zechner W. Computed tomography-based evaluation of template (NobelGuideTM)-guided implant positions: a prospective radiological study. → Clin Oral Implants Res. 2011 Oct;22(10):1157–63. |
| 14. | ↑ | Vasak C, Strbac GD, Huber CD, Lettner S, Gahleitner A, Zechner W. Evaluation of three di erent validation procedures regarding the accuracy of template-guided implant placement: an in vitro study. → Clin Implant Dent Relat Res. 2015 Feb;17(1):142–9. |
| 15. | ↑ | Van Assche N, Vercruyssen M, Coucke W, Teughels W, Jacobs R, Quirynen M. Accuracy of computer-aided implant placement. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:112–23. |
| 16. | ↑ | Schneider D, Marquardt P, Zwahlen M, Jung RE. A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry. → Clin Oral Implants Res. 2009 Sep;20 Suppl 4:73–86. |
| 17. | ↑ | Platzer S, Bertha G, Heschl A, Wegscheider WA, Lorenzoni M. Three-dimensional accuracy of guided implant placement: indirect assessment of clinical outcomes. → Clin Implant Dent Relat Res. 2013 Oct;15(5):724–34. |
| 18. | ↑ | D’haese J, Van De Velde T, Komiyama A, Hultin M, De Bruyn H. Accuracy and complications using computer-designed stereolithographic surgical guides for oral rehabilitation by means of dental implants: a review of the literature. → Clin Implant Dent Relat Res. 2012 Jun;14(3):321–35. |
| 19. | ↑ | Pettersson A, Komiyama A, Hultin M, Näsström K, Klinge B. Accuracy of virtually planned and template guided implant surgery on edentate patients. → Clin Implant Dent Relat Res. 2012 Aug;14(4):527–37. |
| 20. | ↑ | Jung RE, Schneider D, Ganeles J, Wismeijer D, Zwahlen M, Hämmerle CH, Tahmaseb A. Computer technology applications in surgical implant dentistry: a systematic review. → Int J Oral Maxillofac Implants. 2009;24 Suppl:92–109. |
| 21, 22, 24, 27. | ↑ | Cantoni T, Polizzi G. Implant treatment planning in fresh extraction sockets: use of a novel radiographic guide and CAD/CAM technology. → Quintessence Int. 2009 Oct;40(9):773–81. |
| 23. | ↑ | Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. → J Clin Epidemiol. 2008 Apr;61(4):344–9. |
| 25. | ↑ | Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: a systematic review. → J Dent Res. 2012 Mar;91(3):242–8. |
| 26. | ↑ | Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis. → Periodontol 2000. 1998 Jun;17:63–76. |
| 28, 31, 33. | ↑ | Pozzi A, Tallarico M, Moy PK. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with di erent prosthetic interfaces and design in partially posterior edentulous mandibles. → Eur J Oral Implantol. 2014 Spring;7(1):47–61. |
| 29. | ↑ | Bahat O, Sullivan RM. Parameters for successful implant integration revisited part I: immediate loading considered in light of the original prerequisites for osseointegration. → Clin Implant Dent Relat Res. 2010 May;12 Suppl 1:e2–12. |
| 30. | ↑ | Bahat O, Sullivan RM. Parameters for successful implant integration revisited part II: algorithm for immediate loading diagnostic factors. → Clin Implant Dent Relat Res. 2010 May;12 Suppl 1:e13–22. |
| 34. | ↑ | Lee CT, Chiu TS, Chuang SK, Tarnow D, Stoupel J. Alterations of the bone dimension following immediate implant placement into extraction socket: systematic review and meta-analysis. → J Clin Periodontol. 2014 Sep;41(9):914–26. |
| 35. | ↑ | Papaspyridakos P, Chen CJ, Chuang SK, Weber HP. Implant loading protocols for edentulous patients with fixed prostheses: a systematic review and meta-analysis. → Int J Oral Maxillofac Implants. 2014;29 Suppl:256–70. |
| 36. | ↑ | Albrektsson T, Linder L. A method for short- and long-term in vivo study of the bone-implant interface. → Clin Orthop Relat Res. 1981 Sep;159:269–73. |
| 37. | ↑ | Kielbassa AM, Martinez-de Fuentes R, Goldstein M, Arnhart C, Barlattani A, Jackowski J, Knauf M, Lorenzoni M, Maiorana C, Mericske-Stern R, Rompen E, Sanz M. Randomized controlled trial comparing a variable-thread novel tapered and a standard tapered implant: interim one-year results. → J Prosthet Dent. 2009 May;101(5):293–305. |





Leave a Reply
Be the First to Comment!