Influence of smoking and oral hygiene on success of implants placed after direct sinus lift
October 2, 2015 / Categories: Digital Dentistry, Implant Dentistry

Martorell Calatayud, Luis

Romero Millán, Javier

Peñarrocha Oltra, David

Peñarrocha Diago, Maria
García Mira, Berta

Peñarrocha Diago, Miguel
The objective of this study was to evaluate the influence of smoking and oral hygiene on the success and periimplant marginal bone loss of implants placed in one-stage and two-stage direct sinus lift procedures.
Introduction
Placing implants in the posterior maxilla can be a complex procedure when there is atrophy of the alveolar ridge and maxillary sinus pneumatization.
In some cases, these anatomical limitations may be overcome using sinus lift procedures.1Huynh-Ba G, Friedberg JR, Vogiatzi D, Ioannidou E. Implant failure predictors in the posterior maxilla: a retrospective study of 273 consecutive implants. → J Periodontol. 2008 Dec;79(12):2256–61. The success rates of implants placed after sinus lift are similar to those of implants placed in mature bone.2Schlegel A, Hamel J, Wichmann M, Eitner S. Comparative clinical results after implant placement in the posterior maxilla with and without sinus augmentation. → Int J Oral Maxillofac Implants. 2008 Mar-Apr;23(2):289–98. However, the residual alveolar bone height appears to influence implant survival. Rios et al. conducted a systematic review and divided the outcomes into two groups according to residual bone height: ≤ 4 mm in Group 1 and > 4 mm in Group 2.3 The implant survival rate was 96% (range: 80–100%) for Group 1 and 99% (range: 97–100%) for Group 2.3Rios HF, Avila G, Galindo P, Bratu E, Wang HL. The influence of remaining alveolar bone upon lateral window sinus augmentation implant survival. → Implant Dent. 2009 Oct;18(5):402–12.
In addition to bone atrophy, factors such as smoking and poor oral hygiene have been suggested to increase the risk of implant failure in the posterior maxilla.4Peñarrocha M, Palomar M, Sanchis JM, Guarinos J, Balaguer J. Radiologic study of marginal bone loss around 108 dental implants and its relationship to smoking, implant location, and morphology. → Int J Oral Maxillofac Implants. 2004 Nov-Dec;19(6):861–7. Several studies have addressed the association between smoking and the outcome of implants placed using conventional techniques; 5Lindquist LW, Carlsson GE, Jemt T. Association between marginal bone loss around osseointegrated mandibular implants and smoking habits: a 10-year follow-up study. → J Dent Res. 1997 Oct;76(10):1667–74.6Bain CA, Weng D, Meltzer A, Kohles SS, Stach RM. A meta-analysis evaluating the risk for implant failure in patients who smoke. → Compend Contin Educ Dent. 2002 Aug;23(8):695–9, 702, 704 passim; quiz 708.7d’Avila S, dos Reis LD, Piattelli A, Aguiar KC, de Faveri M, Borges FL, Iezzi G, Oliveira NT, de G Cardoso LA, Shibli JA. Impact of smoking on human bone apposition at different dental implant surfaces: a histologic study in type IV bone. → J Oral Implantol. 2010 Apr;36(2):85–90. however, few studies have addressed the influence of smoking on the success of implants placed after direct maxillary sinus lift. In all of the published studies, higher tobacco consumption yielded higher complication and/or implant failure rates;8Blomqvist JE, Alberius P, Isaksson S. Retrospective analysis of one-stage maxillary sinus augmentation with endosseous implants. → Int J Oral Maxillofac Implants. 1996 Jul-Aug;11(4):512–21.9Jensen OT, Shulman LB, Block MS, Iacono VJ. Report of the Sinus Consensus Conference of 1996. → Int J Oral Maxillofac Implants. 1998;13 Suppl:11–45.10Kan JY, Rungcharassaeng K, Lozada JL, Goodacre CJ. Effects of smoking on implant success in grafted maxillary sinuses. J Prosthet Dent. 1999 Sep;82(3):307–11.11Kan JY, Rungcharassaeng K, Kim J, Lozada JL, Goodacre CJ. Factors affecting the survival of implants placed in grafted maxillary sinuses: a clinical report. → J Prosthet Dent. 2002 May;87(5):485–9.12Levin L, Herzberg R, Dolev E, Schwartz- Arad D. Smoking and complications of onlay bone grafts and sinus lift operations. → Int J Oral Maxillofac Implants. 2004 May-Jun;19(3):369–73.13Beaumont C, Zafiropoulos GG, Rohmann K, Tatakis DN. Prevalence of maxillary sinus disease and abnormalities in patients scheduled for sinus lift procedures. → J Periodontol. 2005 Mar;76(3):461–7.14Peleg M, Garg AK, Mazor Z. Healing in smokers versus nonsmokers: survival rates for sinus floor augmentation with simultaneous implant placement. → Int J Oral Maxillofac Implants. 2006 Jul-Aug;21(4):551–9.15Barone A, Santini S, Sbordone L, Crespi R, Covani U. A clinical study of the outcomes and complications associated with maxillary sinus augmentation. → Int J Oral Maxillofac Implants. 2006 Jan-Feb;21(1):81–5.,16Huynh-Ba G, Friedberg JR, Vogiatzi D, Ioannidou E. Implant failure predictors in the posterior maxilla: a retrospective study of 273 consecutive implants. → J Periodontol. 2008 Dec;79(12):2256–61.17Lin TH, Chen L, Cha J, Jeffcoat M, Kao DW, Nevins M, Fiorellini JP. The effect of cigarette smoking and native bone height on dental implants placed immediately in sinuses grafted by hydraulic condensation. → Int J Periodontics Restorative Dent. 2012 Jun;32(3):255–61.18Testori T, Weinstein RL, Taschieri S, Del Fabbro M. Risk factor analysis following maxillary sinus augmentation: a retrospective multicenter study. → Int J Oral Maxillofac Implants. 2012 Sep-Oct;27(5):1170–6. 19Zinser MJ, Randelzhofer P, Kuiper L, Zöller JE, De Lange GL. The predictors of implant failure after maxillary sinus floor augmentation and reconstruction: a retrospective study of 1045 consecutive implants. → Oral Surg Oral Med Oral Pathol Oral Radiol. 2013 May;115(5):571–82.20Cha HS, Kim A, Nowzari H, Chang HS, Ahn KM. Simultaneous sinus lift and implant installation: prospective study of consecutive two hundred seventeen sinus lift and four hundred sixty-two implants. → Clin Implant Dent Relat Res. 2014 Jun;16(3):337–47. however, this effect was not always statistically significant (Table 1).21Bain CA, Weng D, Meltzer A, Kohles SS, Stach RM. A meta-analysis evaluating the risk for implant failure in patients who smoke. → Compend Contin Educ Dent. 2002 Aug;23(8):695–9, 702, 704 passim; quiz 708.22Levin L, Herzberg R, Dolev E, Schwartz- Arad D. Smoking and complications of onlay bone grafts and sinus lift operations. → Int J Oral Maxillofac Implants. 2004 May-Jun;19(3):369–73.23Beaumont C, Zafiropoulos GG, Rohmann K, Tatakis DN. Prevalence of maxillary sinus disease and abnormalities in patients scheduled for sinus lift procedures. → J Periodontol. 2005 Mar;76(3):461–7.24Peleg M, Garg AK, Mazor Z. Healing in smokers versus nonsmokers: survival rates for sinus floor augmentation with simultaneous implant placement. → Int J Oral Maxillofac Implants. 2006 Jul-Aug;21(4):551–9.
The influence of oral hygiene has frequently been considered in implant studies. In some studies, poor hygiene was associated with higher periimplant marginal bone loss.25Lindquist LW, Carlsson GE, Jemt T. A prospective 15-year follow-up study of mandibular fixed prostheses supported by osseointegrated implants. Clinical results and marginal bone loss. → Clin Oral Implants Res. 1996 Dec;7(4):329–36. Contrarily, other studies did not find this relationship.26Mombelli A, van Oosten MA, Schürch E Jr, Lang NP. The microbiota associated with successful or failing osseointegrated titanium implants. → Oral Microbiol Immunol. 1987 Dec;2(4):145–51.27Smith DE, Zarb GA. Criteria for success of osseointegrated endosseous implants. → J Prosthet Dent. 1989 Nov;62(5):567–72.28Baelum V, Ellegaard B. Implant survival in periodontally compromised patients. → J Periodontol. 2004 Oct;75(10):1404–12. However, evidence relating patient oral hygiene to the outcome of implants placed after direct sinus lift procedures is scarce. Only one study was found, and it reported a statistically significantly higher implant failure rate in patients with poor oral hygiene.29Kan JY, Rungcharassaeng K, Kim J, Lozada JL, Goodacre CJ. Factors affecting the survival of implants placed in grafted maxillary sinuses: a clinical report. → J Prosthet Dent. 2002 May;87(5):485–9.The objective of this study was to evaluate the influence of smoking and oral hygiene on the success and periimplant marginal bone loss of implants placed in one-stage and two-stage direct sinus lift procedures.
Materials & methods
The study was approved by the University of Valencia ethics committee (#H1410262226693). All patients gave written informed consent before surgery, in accordance with the principles of the Declaration of Helsinki.
Study sample
A retrospective clinical study was performed between September 2009 and June 2012 of patients treated with dental implants placed in one-stage (simultaneous) and two-stage (delayed) direct sinus lift procedures. A minimum follow-up period of 12 months after implant loading was requested. Patients who failed to attend scheduled follow-up visits were excluded.
Surgical procedures
All of the procedures were performed by two expert surgeons, professors at the Oral Surgery Unit, Department of Stomatology, University of Valencia, under local anesthesia with 4% articaine and 1:100,000 epinephrine (Laboratorios Inibsa, Lliçà de Vall, Spain). Full-thickness flaps were raised. A window in the sinus lateral wall was made with round tungsten carbide burs and finalized with ultrasonic tips. The sinus membrane was detached with curettes and elevated using a bone graft material. A xenograft (Geistlich Bio-Oss, Geistlich Pharma, Wolhusen, Switzerland) was used as the only bone graft material (1.5–2 g). The sinus window was covered with a resorbable membrane (Geistlich Bio-Gide, Geistlich Pharma, Wolhusen, Switzerland). The implants used in this study were TSA implants with an Avantblast surface (Phibo Dental Solutions, Sentmenat, Spain). Implants were placed in the same surgery if the residual bone height was 4–6 mm, or delayed by six months if the height was < 4 mm.
All of the patients were prescribed the same postoperative medication: amoxicillin and clavulanic acid (Augmentin, GlaxoSmithKline, Madrid, Spain) 500 mg/8 h for seven days, ibuprofen (Bexistar, Laboratorio Barcino, Barcelona, Spain) 600 mg/8 h for three days, and a 0.12% chlorhexidine mouthrinse (GUM, Sunstar Americas, Chicago, Ill., U.S.) t.i.d. for seven days.
Data collection
Patient oral hygiene was evaluated using the Simplified Oral Hygiene Index (OHI-S).30Greene JC, Vermillion JR. The simplified oral hygiene index. → J Am Dent Assoc. 1964 Jan;68(1):7–13. This was obtained by measuring the presence of debris and calculus on the buccal surfaces of the maxillary right central incisor, mandibular left central incisor and maxillary first molars, as well as on the lingual surfaces of the mandibular first molars. The criteria for classifying debris were as follows: no debris, no stains (0); soft debris covering less than one-third of the tooth surface (1); soft debris covering more than one-third, but less than twothirds of the exposed tooth surface (2); and soft debris covering more than two-thirds of the exposed tooth surface (3). The criteria for classifying calculus were as follows: no calculus (0); supragingival calculus covering less than onethird of the exposed tooth surface (1); supragingival calculus covering more than one-third, but less than two-thirds of the exposed tooth surface (2); and supragingival calculus covering more than two-thirds of the exposed tooth surface (3). The OHI-S was obtained from the combination of the two subindices. The grading scale was 0–1.2 (good oral hygiene), 1.3–3 (regular oral hygiene), or 3.1–6 (poor oral hygiene). Each patient was classified as having good oral hygiene, regular oral hygiene or poor oral hygiene.
The implant success rate was recorded according to the clinical and radiographic criteria of Buser et al.31Buser D, Mericske-Stern R, Dula K, Lang NP. Clinical experience with one-stage, non-submerged dental implants. → Adv Dent Res. 1999 Jun;13(1):153–61. Implants were classified as successful if they fulfilled all of the criteria (absence of clinically detectable implant mobility, absence of pain or any subjective sensation, absence of recurrent periimplant infection, and absence of continuous radiolucency around the implant after 12 months of loading) and as failed if any criterion was not met.
-
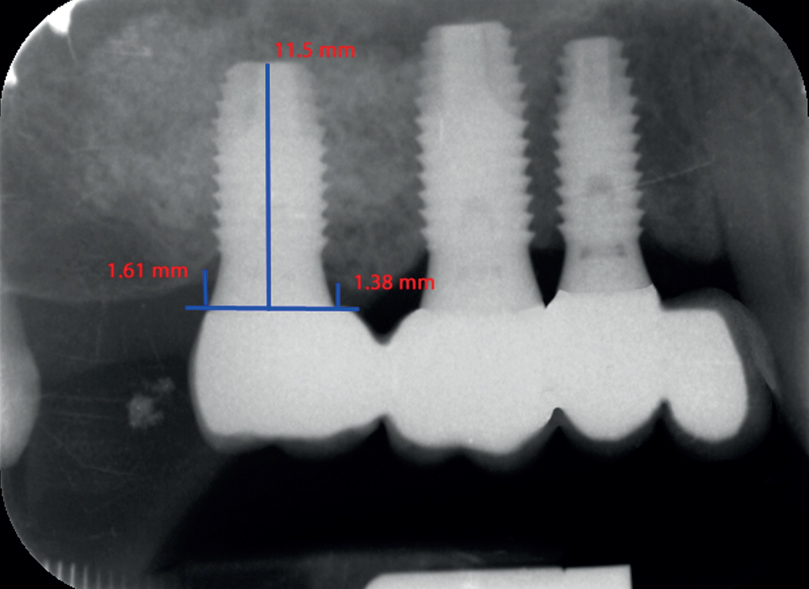
- Fig. 1
-
- Fig. 2
Radiographic assessment of bone level at implant loading.
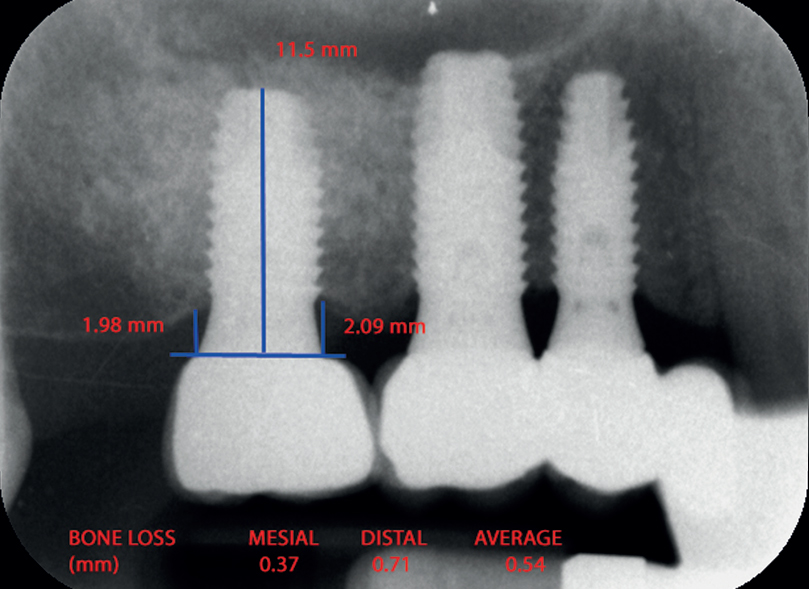
Fig. 2
Radiographic assessment of bone level 12 months after loading.
Radiographic examination was performed with an X-Mind intra-oral system (ACTEON MÉDICO-DENTAL IBÉRICA, Sentmenat, Spain) and an RVG intra-oral digital receptor (RVG 5100, Carestream Dental, Atlanta, Ga., U.S.). In order to reproduce the patient alignments, the Rinn XCP system (DENTSPLY, Des Plaines, Ill., U.S.) was used with a bite registration material in the area in which the parallelometer was fixed. Marginal implant bone loss was measured in millimeters using the RVG software. For measurement purposes, two visible and easily locatable reference points were selected at the junction point between the implant and prosthetic restoration. A straight line was traced between these two reference points and was considered to represent zero height. In order to determine bone loss, a perpendicular line was traced mesial and distal to the implant from zero height to contact with the bone (Fig. 1). The difference between the value recorded at the time of implant loading and after one year of loading was used to calculate bone loss mesial and distal to the implant. The largest value, either mesial or distal, was used as the bone loss value for that implant (Fig. 2).32Boronat A, Peñarrocha M, Carrillo C, Marti E. Marginal bone loss in dental implants subjected to early loading (6 to 8 weeks postplacement) with a retrospective shortterm follow-up. → J Oral Maxillofac Surg. 2008 Feb;66(2):246–50.
Smoking and oral hygiene were recorded at the time of surgery. A patient who smoked > 1 cigarette/ day was considered a smoker following the definition by Wallace.27 Bone loss and success were recorded at 12 months of prosthetic loading.
Statistical analysis
A descriptive analysis was performed of the study variables, with their corresponding frequency distributions and measures of central tendency and dispersion. Statistical comparisons between the groups were conducted using the chi-squared test and Student’s t-test. The SPSS for Windows statistical software package (Version 15.0; SPSS, Chicago, Ill., U.S.) was used throughout. Statistical significance was considered for p< 0.05.
Results
Fifty patients treated with direct sinus lift and implants were monitored during the study period. Four patients failed to attend scheduled follow-up visits and were thus excluded. The final sample consisted of 46 patients (16 men and 30 women) with a mean age of 49 (range: 29–69 years). These patients underwent 58 direct maxillary sinus lift procedures and received a total of 102 implants in the grafted sites: 50 were placed simultaneously with the sinus lift procedure and 52 were placed six months thereafter. Implant lengths and diameters are detailed in Table 2.
Seven implants failed, all prior to loading, yielding an overall implant success rate of 93.1% at 12 months of loading. Five of these implants had been placed simultaneously and two implants six months after the grafting procedure. The survival was 90.0% for implants placed simultaneously and 96.2% for delayed implants. Overall, the mean periimplant marginal bone loss was 0.58 mm (range: 0.24–0.95 mm). Implants placed simultaneously had a mean bone loss of 0.62 mm (range: 0.21–0.97 mm) and implants placed in a second procedure of 0.54 mm (range: 0.27–0.93 mm; Table 3).
With respect to smoking, 69 implants were placed in nonsmokers and 33 in smokers. Nonsmokers presented a higher implant success rate at 12 months (94.2%) and lower mean bone loss (0.52 mm; range: 0.21–0.84 mm) than smokers (90.9% and 0.60 mm; range: 0.24–0.92 mm; Table 4). However, these differences were not statistically significant.
In relation to oral hygiene, 47 of the 102 implants were placed in patients with good oral hygiene, 42 with regular and 13 with poor hygiene. In patients with poor oral hygiene, the success rate at 12 months was lower (81.8%), compared with patients with regular (92.3%) or good hygiene (95.5%). Mean bone loss at 12 months was 0.51 mm (range: 0.21–0.82 mm) in patients with good oral hygiene, 0.57 mm (range: 0.24– 0.82 mm) in patients with regular hygiene, and 0.66 mm in those with poor hygiene (range: 0.32– 0.92 mm; Table 5). The observed differences were in no case statistically significant. The survival rate of implants placed in patients with poor oral hygiene was lower than in patients with regular or good hygiene. These differences were close to statistical significance (p= 0.058).
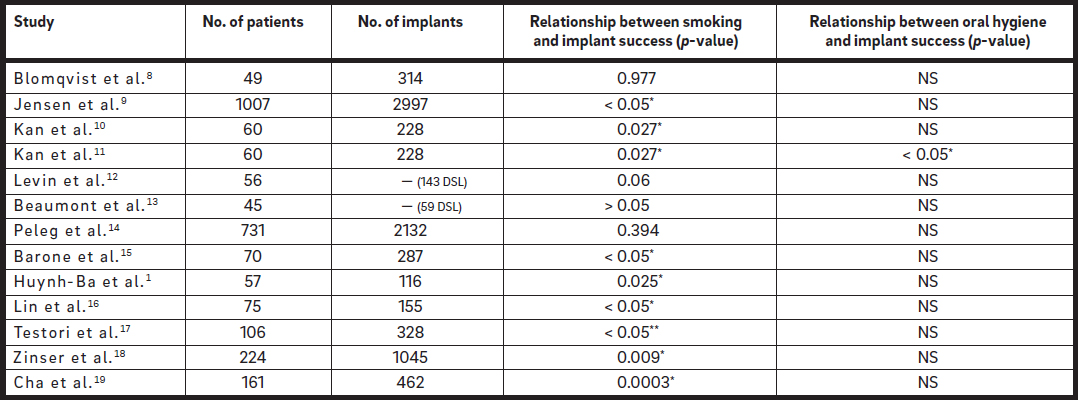 *Significant differences; **significant differences only for > 15 cigarettes/day.
*Significant differences; **significant differences only for > 15 cigarettes/day.
Table 1
Effect of smoking and oral hygiene on success of implants placed after direct sinus lift (DSL = direct sinus lift; NS: not studied).

Table 2
Number of implants placed according to length and diameter.
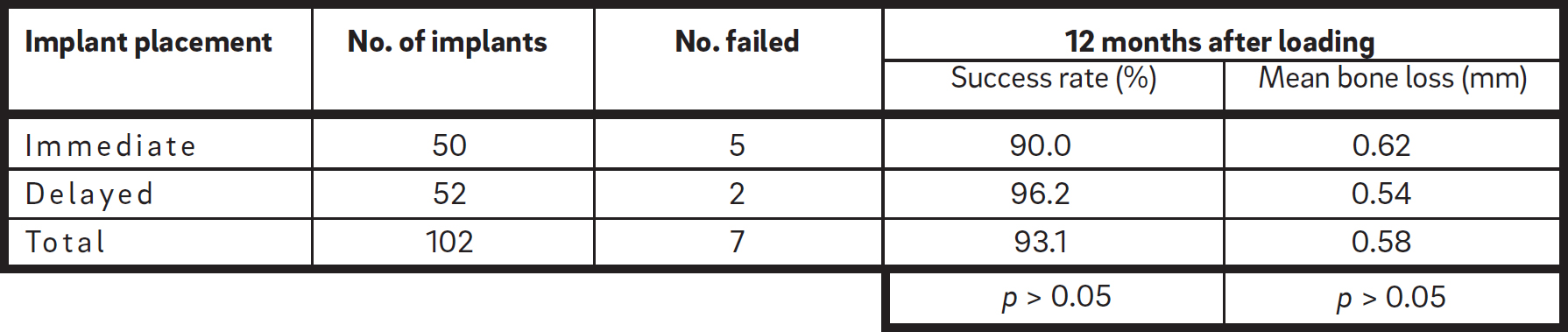
Table 3
Number of implants placed and failed, success rate and mean bone loss according to immediate or delayed placement of implants.

Table 4
Number of implants, success rate and mean bone loss in relation to smoking.
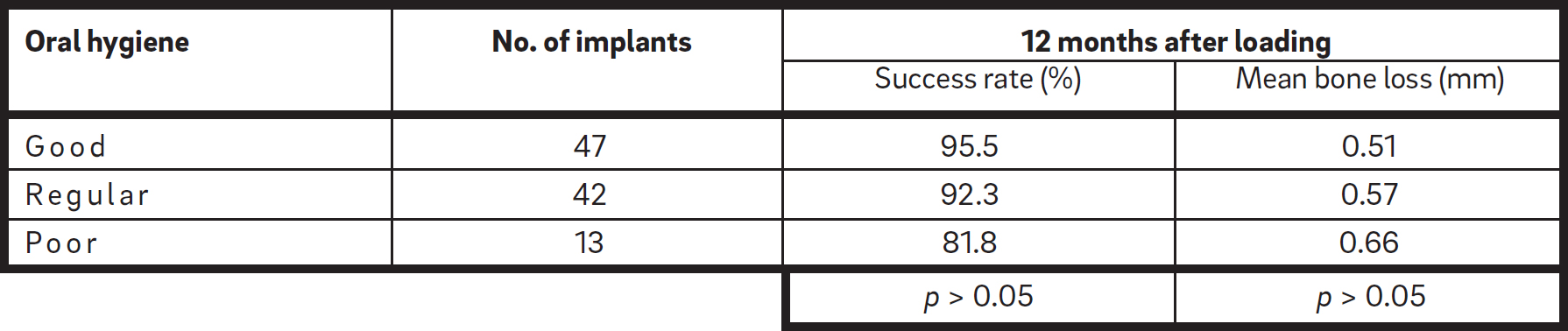
Table 5
Number of implants, success rate and mean bone loss in relation to oral hygiene.
Discussion
Direct maxillary sinus lift is a predictable procedure. Pjetursson et al. performed a systematic review to assess the survival of implants after sinus lift.33Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. → J Clin Periodontol. 2008 Sep;35(8 Suppl):216–40. Meta-analysis indicated an estimated annual failure rate of 3.48% (95% confidence interval: 2.48–4.88%), which translated into a threeyear implant survival of 90.1% (95% confidence interval: 86.4–92.8%).34Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. → J Clin Periodontol. 2008 Sep;35(8 Suppl):216–40. These results are similar to 00_JOSR_A4_Penarrocha_Layout 1 18.09.15 22:20 Seite 4 those obtained in the present study: a success rate of 93.1% for 102 implants placed after 58 direct sinus lifts.
The mean bone loss at 12 months was 0.62 mm for simultaneously placed implants and 0.54 mm for those placed in a second stage. No statistically significant differences were observed. These results were similar to those of Felice et al.: one year after loading, one-stage-treated implants lost an average of 1.01 mm of periimplant bone and two-stage sites about 0.93 mm.35Felice P, Pistilli R, Piattelli M, Soardi E, Barausse C, Esposito M. 1-stage versus 2- stage lateral sinus lift procedures: 1-year post-loading results of a multicentre randomised controlled trial. → Eur J Oral Implantol. 2014 Spring;7(1):65–75. Similarly, after one year of follow-up, Jodia et al.36Jodia K, Sadhwani BS, Parmar BS, Anchlia S, Sadhwani SB. Sinus elevation with an alloplastic material and simultaneous implant placement: a 1-stage procedure in severely atrophic maxillae. → J Maxillofac Oral Surg. 2014 Jul-Sep;13(3):271–80. reported a marginal bone loss of between 0.68 and 1.22 mm for simultaneously placed implants, and Kahnberg and Vannas-Löfqvist37Kahnberg KE, Vannas-Löfqvist L. Sinus lift procedure using a 2-stage surgical technique: I. Clinical and radiographic report up to 5 years. → Int J Oral Maxillofac Implants. 2008 Sep-Oct;23(5):876–84. of 0.8 mm for implants placed in a delayed mode.
In the literature, smoking has often been associated with a higher failure rate for conventionally placed dental implants,
38Bain CA, Moy PK. The association between the failure of dental implants and cigarette smoking. → Int J Oral Maxillofac Implants. 1993 Nov-Dec;8(6):609–15.39Lambert PM, Morris HF, Ochi S. The influence of smoking on 3-year clinical success of osseointegrated dental implants. → Ann Periodontol. 2000 Dec;5(1):79–89.40Nitzan D, Mamlider A, Levin L, Schwartz- Arad D. Impact of smoking on marginal bone loss. → Int J Oral Maxillofac Implants. 2005 Jul-Aug;20(4):605–9. 41Galindo-Moreno P, Fauri M, Ávila-Ortiz G, Fernández-Barbero JE, Cabrera-León A, Sánchez-Fernández E. Influence of alcohol and tobacco habits on peri-implant marginal bone loss: a prospective study. → Clin Oral Implants Res. 2005 Oct;16(5):579–86.42d’Avila S, dos Reis LD, Piattelli A, Aguiar KC, de Faveri M, Borges FL, Iezzi G, Oliveira NT, de G Cardoso LA, Shibli JA. Impact of smoking on human bone apposition at different dental implant surfaces: a histologic study in type IV bone. → J Oral Implantol. 2010 Apr;36(2):85–90. worse osseointegration, as well as more frequent periimplantitis, bone loss and bleeding.43Haas R, Haimböck W, Mailath G, Watzek G. The relationship of smoking on periimplant tissue: a retrospective study. → J Prosthet Dent. 1996 Dec;76(6):592–6.44de Souza JG, Bianchini MA, Ferreira CF. Relationship between smoking and bleeding on probing. → J Oral Implantol. 2012 Oct;38(5):581–6. However, in studies published on sinus lift, there is no unanimity regarding the effect of smoking on treatment outcomes. In five of the reviewed studies (Table 1), statistically significant differences were found, observing a higher success rate in nonsmokers than in smokers.45Jensen OT, Shulman LB, Block MS, Iacono VJ. Report of the Sinus Consensus Conference of 1996. → Int J Oral Maxillofac Implants. 1998;13 Suppl:11–45.46Kan JY, Rungcharassaeng K, Lozada JL, Goodacre CJ. Effects of smoking on implant success in grafted maxillary sinuses. J Prosthet Dent. 1999 Sep;82(3):307–11.47Kan JY, Rungcharassaeng K, Kim J, Lozada JL, Goodacre CJ. Factors affecting the survival of implants placed in grafted maxillary sinuses: a clinical report. → J Prosthet Dent. 2002 May;87(5):485–9.48Barone A, Santini S, Sbordone L, Crespi R, Covani U. A clinical study of the outcomes and complications associated with maxillary sinus augmentation. → Int J Oral Maxillofac Implants. 2006 Jan-Feb;21(1):81–5.49Huynh-Ba G, Friedberg JR, Vogiatzi D, Ioannidou E. Implant failure predictors in the posterior maxilla: a retrospective study of 273 consecutive implants. → J Periodontol. 2008 Dec;79(12):2256–61. In one study, only smoking > 15 cigarettes/day and a residual ridge height of < 4 mm were significantly associated with reduced implant survival.50Testori T, Weinstein RL, Taschieri S, Del Fabbro M. Risk factor analysis following maxillary sinus augmentation: a retrospective multicenter study. → Int J Oral Maxillofac Implants. 2012 Sep-Oct;27(5):1170–6. In other studies,51Blomqvist JE, Alberius P, Isaksson S. Retrospective analysis of one-stage maxillary sinus augmentation with endosseous implants. → Int J Oral Maxillofac Implants. 1996 Jul-Aug;11(4):512–21.52Levin L, Herzberg R, Dolev E, Schwartz- Arad D. Smoking and complications of onlay bone grafts and sinus lift operations. → Int J Oral Maxillofac Implants. 2004 May-Jun;19(3):369–73.53Beaumont C, Zafiropoulos GG, Rohmann K, Tatakis DN. Prevalence of maxillary sinus disease and abnormalities in patients scheduled for sinus lift procedures. → J Periodontol. 2005 Mar;76(3):461–7.54Peleg M, Garg AK, Mazor Z. Healing in smokers versus nonsmokers: survival rates for sinus floor augmentation with simultaneous implant placement. → Int J Oral Maxillofac Implants. 2006 Jul-Aug;21(4):551–9. no statistically significant relationship was found between smoking and implant success, although failure rates were higher among smokers. Moreover, Levin et al. observed relevant complications in one-third of the smokers, compared with only 7.7% of the nonsmokers.55Levin L, Herzberg R, Dolev E, Schwartz- Arad D. Smoking and complications of onlay bone grafts and sinus lift operations. → Int J Oral Maxillofac Implants. 2004 May-Jun;19(3):369–73.
A recent systematic review evaluated the effects of tobacco smoking on the survival rate of dental implants placed in areas of maxillary sinus lift. Eight studies, three prospective and five retrospective, were included. Smoking was associated with increased implant failure rates in most individual studies and in the overall meta-analysis. However, when only prospective studies were considered, no significant differences in implant failure were observed between smokers and nonsmokers.56Chambrone L, Preshaw PM, Ferreira JD, Rodrigues JA, Cassoni A, Shibli JA. Effects of tobacco smoking on the survival rate of dental implants placed in areas of maxillary sinus floor augmentation: a systematic review. → Clin Oral Implants Res. 2014 Apr;25(4):408–16. Similar results were obtained in this study: the implant failure rate and bone loss were slightly higher in smokers, but with the available sample size these differences were not statistically significant.
The literature clearly demonstrates the negative response of the periimplant mucosa to plaque accumulation;57van Steenberghe D, Klinge B, Lindén U, Quirynen M, Herrmann I, Garpland C. Periodontal indices around natural and titanium abutments: a longitudinal multicenter study. → J Periodontol. 1993 Jun;64(6):538–41.58Crespi R, Capparè P, Gherlone E. A 4-year evaluation of the peri-implant parameters of immediately loaded implants placed in fresh extraction sockets. → J Periodontol. 2010 Nov;81(11):1629–34.59Matarasso S, Rasperini G, Iorio Siciliano V, Salvi GE, Lang NP, Aglietta M. A 10-year retrospective analysis of radiographic bone-level changes of implants supporting single-unit crowns in periodontally compromised vs. periodontally healthy patients. → Clin Oral Implants Res. 2010 Sep;21(9):898–903. however, there is disagreement regarding the influence of oral hygiene on the success of conventionally placed implants. Mombelli et al.,60Mombelli A, van Oosten MA, Schürch E Jr, Lang NP. The microbiota associated with successful or failing osseointegrated titanium implants. → Oral Microbiol Immunol. 1987 Dec;2(4):145–51. Smith and Zarb,61Smith DE, Zarb GA. Criteria for success of osseointegrated endosseous implants. → J Prosthet Dent. 1989 Nov;62(5):567–72. and Baelum and Ellegaard argue that hygiene did not influence implant outcomes (success and bone loss) in the short term.62Baelum V, Ellegaard B. Implant survival in periodontally compromised patients. → J Periodontol. 2004 Oct;75(10):1404–12. However, Lindquist et al. observed a higher bone loss in patients with poor oral hygiene.63Lindquist LW, Carlsson GE, Jemt T. Association between marginal bone loss around osseointegrated mandibular implants and smoking habits: a 10-year follow-up study. → J Dent Res. 1997 Oct;76(10):1667–74. The influence of hygiene on the success of implants placed after direct sinus lift has been more rarely studied. Kan et al.64Kan JY, Rungcharassaeng K, Kim J, Lozada JL, Goodacre CJ. Factors affecting the survival of implants placed in grafted maxillary sinuses: a clinical report. → J Prosthet Dent. 2002 May;87(5):485–9. evaluated oral hygiene according to the modified plaque index as described by Mombelli et al.65Mombelli A, van Oosten MA, Schürch E Jr, Lang NP. The microbiota associated with successful or failing osseointegrated titanium implants. → Oral Microbiol Immunol. 1987 Dec;2(4):145–51. and reported a failure rate of 1.4% in patients with good oral hygiene, 13.9% with fair hygiene and 60% with poor oral hygiene; the differences between the groups were statistically significant.66Kan JY, Rungcharassaeng K, Kim J, Lozada JL, Goodacre CJ. Factors affecting the survival of implants placed in grafted maxillary sinuses: a clinical report. → J Prosthet Dent. 2002 May;87(5):485–9. In our study, a lower implant success rate was found in patients with poor hygiene (81.8%), compared with patients with regular and good hygiene (92.3% and 95.5%, respectively). The differences did not reach statistical significance, but the comparison between poor hygiene and the other two categories tended to significance (p = 0.058). In fact, a difference of over 10% with such a predictable treatment technique may be considered of clinical relevance, and the lack of statistical significance is probably related to the small number of patients with poor oral hygiene.
Conclusion
Within its limitations, the present investigation suggests that smoking and poor oral hygiene may negatively influence the outcome of implants placed both in one-stage and two-stage direct sinus lift procedures. However, the differences were in no case statistically significant, and prospective studies with larger sample sizes and longer follow-up are necessary to corroborate or refute these findings.
Competing interests
The authors declare that they have no conflict of interests related to this study.
References
| 1, 16, 49. | ↑ | Huynh-Ba G, Friedberg JR, Vogiatzi D, Ioannidou E. Implant failure predictors in the posterior maxilla: a retrospective study of 273 consecutive implants. → J Periodontol. 2008 Dec;79(12):2256–61. |
| 2. | ↑ | Schlegel A, Hamel J, Wichmann M, Eitner S. Comparative clinical results after implant placement in the posterior maxilla with and without sinus augmentation. → Int J Oral Maxillofac Implants. 2008 Mar-Apr;23(2):289–98. |
| 3. | ↑ | Rios HF, Avila G, Galindo P, Bratu E, Wang HL. The influence of remaining alveolar bone upon lateral window sinus augmentation implant survival. → Implant Dent. 2009 Oct;18(5):402–12. |
| 4. | ↑ | Peñarrocha M, Palomar M, Sanchis JM, Guarinos J, Balaguer J. Radiologic study of marginal bone loss around 108 dental implants and its relationship to smoking, implant location, and morphology. → Int J Oral Maxillofac Implants. 2004 Nov-Dec;19(6):861–7. |
| 5, 63. | ↑ | Lindquist LW, Carlsson GE, Jemt T. Association between marginal bone loss around osseointegrated mandibular implants and smoking habits: a 10-year follow-up study. → J Dent Res. 1997 Oct;76(10):1667–74. |
| 6, 21. | ↑ | Bain CA, Weng D, Meltzer A, Kohles SS, Stach RM. A meta-analysis evaluating the risk for implant failure in patients who smoke. → Compend Contin Educ Dent. 2002 Aug;23(8):695–9, 702, 704 passim; quiz 708. |
| 7, 42. | ↑ | d’Avila S, dos Reis LD, Piattelli A, Aguiar KC, de Faveri M, Borges FL, Iezzi G, Oliveira NT, de G Cardoso LA, Shibli JA. Impact of smoking on human bone apposition at different dental implant surfaces: a histologic study in type IV bone. → J Oral Implantol. 2010 Apr;36(2):85–90. |
| 8, 51. | ↑ | Blomqvist JE, Alberius P, Isaksson S. Retrospective analysis of one-stage maxillary sinus augmentation with endosseous implants. → Int J Oral Maxillofac Implants. 1996 Jul-Aug;11(4):512–21. |
| 9, 45. | ↑ | Jensen OT, Shulman LB, Block MS, Iacono VJ. Report of the Sinus Consensus Conference of 1996. → Int J Oral Maxillofac Implants. 1998;13 Suppl:11–45. |
| 10, 46. | ↑ | Kan JY, Rungcharassaeng K, Lozada JL, Goodacre CJ. Effects of smoking on implant success in grafted maxillary sinuses. J Prosthet Dent. 1999 Sep;82(3):307–11. |
| 11, 29, 47, 64, 66. | ↑ | Kan JY, Rungcharassaeng K, Kim J, Lozada JL, Goodacre CJ. Factors affecting the survival of implants placed in grafted maxillary sinuses: a clinical report. → J Prosthet Dent. 2002 May;87(5):485–9. |
| 12, 22, 52, 55. | ↑ | Levin L, Herzberg R, Dolev E, Schwartz- Arad D. Smoking and complications of onlay bone grafts and sinus lift operations. → Int J Oral Maxillofac Implants. 2004 May-Jun;19(3):369–73. |
| 13, 23, 53. | ↑ | Beaumont C, Zafiropoulos GG, Rohmann K, Tatakis DN. Prevalence of maxillary sinus disease and abnormalities in patients scheduled for sinus lift procedures. → J Periodontol. 2005 Mar;76(3):461–7. |
| 14, 24, 54. | ↑ | Peleg M, Garg AK, Mazor Z. Healing in smokers versus nonsmokers: survival rates for sinus floor augmentation with simultaneous implant placement. → Int J Oral Maxillofac Implants. 2006 Jul-Aug;21(4):551–9. |
| 15, 48. | ↑ | Barone A, Santini S, Sbordone L, Crespi R, Covani U. A clinical study of the outcomes and complications associated with maxillary sinus augmentation. → Int J Oral Maxillofac Implants. 2006 Jan-Feb;21(1):81–5. |
| 17. | ↑ | Lin TH, Chen L, Cha J, Jeffcoat M, Kao DW, Nevins M, Fiorellini JP. The effect of cigarette smoking and native bone height on dental implants placed immediately in sinuses grafted by hydraulic condensation. → Int J Periodontics Restorative Dent. 2012 Jun;32(3):255–61. |
| 18. | ↑ | Testori T, Weinstein RL, Taschieri S, Del Fabbro M. Risk factor analysis following maxillary sinus augmentation: a retrospective multicenter study. → Int J Oral Maxillofac Implants. 2012 Sep-Oct;27(5):1170–6. |
| 19. | ↑ | Zinser MJ, Randelzhofer P, Kuiper L, Zöller JE, De Lange GL. The predictors of implant failure after maxillary sinus floor augmentation and reconstruction: a retrospective study of 1045 consecutive implants. → Oral Surg Oral Med Oral Pathol Oral Radiol. 2013 May;115(5):571–82. |
| 20. | ↑ | Cha HS, Kim A, Nowzari H, Chang HS, Ahn KM. Simultaneous sinus lift and implant installation: prospective study of consecutive two hundred seventeen sinus lift and four hundred sixty-two implants. → Clin Implant Dent Relat Res. 2014 Jun;16(3):337–47. |
| 25. | ↑ | Lindquist LW, Carlsson GE, Jemt T. A prospective 15-year follow-up study of mandibular fixed prostheses supported by osseointegrated implants. Clinical results and marginal bone loss. → Clin Oral Implants Res. 1996 Dec;7(4):329–36. |
| 26, 60, 65. | ↑ | Mombelli A, van Oosten MA, Schürch E Jr, Lang NP. The microbiota associated with successful or failing osseointegrated titanium implants. → Oral Microbiol Immunol. 1987 Dec;2(4):145–51. |
| 27, 61. | ↑ | Smith DE, Zarb GA. Criteria for success of osseointegrated endosseous implants. → J Prosthet Dent. 1989 Nov;62(5):567–72. |
| 28, 62. | ↑ | Baelum V, Ellegaard B. Implant survival in periodontally compromised patients. → J Periodontol. 2004 Oct;75(10):1404–12. |
| 30. | ↑ | Greene JC, Vermillion JR. The simplified oral hygiene index. → J Am Dent Assoc. 1964 Jan;68(1):7–13. |
| 31. | ↑ | Buser D, Mericske-Stern R, Dula K, Lang NP. Clinical experience with one-stage, non-submerged dental implants. → Adv Dent Res. 1999 Jun;13(1):153–61. |
| 32. | ↑ | Boronat A, Peñarrocha M, Carrillo C, Marti E. Marginal bone loss in dental implants subjected to early loading (6 to 8 weeks postplacement) with a retrospective shortterm follow-up. → J Oral Maxillofac Surg. 2008 Feb;66(2):246–50. |
| 33, 34. | ↑ | Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. → J Clin Periodontol. 2008 Sep;35(8 Suppl):216–40. |
| 35. | ↑ | Felice P, Pistilli R, Piattelli M, Soardi E, Barausse C, Esposito M. 1-stage versus 2- stage lateral sinus lift procedures: 1-year post-loading results of a multicentre randomised controlled trial. → Eur J Oral Implantol. 2014 Spring;7(1):65–75. |
| 36. | ↑ | Jodia K, Sadhwani BS, Parmar BS, Anchlia S, Sadhwani SB. Sinus elevation with an alloplastic material and simultaneous implant placement: a 1-stage procedure in severely atrophic maxillae. → J Maxillofac Oral Surg. 2014 Jul-Sep;13(3):271–80. |
| 37. | ↑ | Kahnberg KE, Vannas-Löfqvist L. Sinus lift procedure using a 2-stage surgical technique: I. Clinical and radiographic report up to 5 years. → Int J Oral Maxillofac Implants. 2008 Sep-Oct;23(5):876–84. |
| 38. | ↑ | Bain CA, Moy PK. The association between the failure of dental implants and cigarette smoking. → Int J Oral Maxillofac Implants. 1993 Nov-Dec;8(6):609–15. |
| 39. | ↑ | Lambert PM, Morris HF, Ochi S. The influence of smoking on 3-year clinical success of osseointegrated dental implants. → Ann Periodontol. 2000 Dec;5(1):79–89. |
| 40. | ↑ | Nitzan D, Mamlider A, Levin L, Schwartz- Arad D. Impact of smoking on marginal bone loss. → Int J Oral Maxillofac Implants. 2005 Jul-Aug;20(4):605–9. |
| 41. | ↑ | Galindo-Moreno P, Fauri M, Ávila-Ortiz G, Fernández-Barbero JE, Cabrera-León A, Sánchez-Fernández E. Influence of alcohol and tobacco habits on peri-implant marginal bone loss: a prospective study. → Clin Oral Implants Res. 2005 Oct;16(5):579–86. |
| 43. | ↑ | Haas R, Haimböck W, Mailath G, Watzek G. The relationship of smoking on periimplant tissue: a retrospective study. → J Prosthet Dent. 1996 Dec;76(6):592–6. |
| 44. | ↑ | de Souza JG, Bianchini MA, Ferreira CF. Relationship between smoking and bleeding on probing. → J Oral Implantol. 2012 Oct;38(5):581–6. |
| 50. | ↑ | Testori T, Weinstein RL, Taschieri S, Del Fabbro M. Risk factor analysis following maxillary sinus augmentation: a retrospective multicenter study. → Int J Oral Maxillofac Implants. 2012 Sep-Oct;27(5):1170–6. |
| 56. | ↑ | Chambrone L, Preshaw PM, Ferreira JD, Rodrigues JA, Cassoni A, Shibli JA. Effects of tobacco smoking on the survival rate of dental implants placed in areas of maxillary sinus floor augmentation: a systematic review. → Clin Oral Implants Res. 2014 Apr;25(4):408–16. |
| 57. | ↑ | van Steenberghe D, Klinge B, Lindén U, Quirynen M, Herrmann I, Garpland C. Periodontal indices around natural and titanium abutments: a longitudinal multicenter study. → J Periodontol. 1993 Jun;64(6):538–41. |
| 58. | ↑ | Crespi R, Capparè P, Gherlone E. A 4-year evaluation of the peri-implant parameters of immediately loaded implants placed in fresh extraction sockets. → J Periodontol. 2010 Nov;81(11):1629–34. |
| 59. | ↑ | Matarasso S, Rasperini G, Iorio Siciliano V, Salvi GE, Lang NP, Aglietta M. A 10-year retrospective analysis of radiographic bone-level changes of implants supporting single-unit crowns in periodontally compromised vs. periodontally healthy patients. → Clin Oral Implants Res. 2010 Sep;21(9):898–903. |





Leave a Reply
Be the First to Comment!