Kinesiographic evaluation of patients under orthodontic treatment with or without tooth extraction
June 14, 2017 / Categories: Digital Dentistry, Implant Dentistry

Klimova, Tatiana

Nabiev, Nabi

Cesaretti, Gianfranco

Persin, Leonid
Abstract
Objective
In orthodontic practice, it is always required to decide whether to extract a tooth or to close the gap in the case of edentia. There are no scientific reports on changes to the temporomandibular joint and muscle system after orthodontic treatment including dentition size and shape reduction. The objective of this study was to improve diagnostic methods using computed diagnostic equipment.
Materials and methods
After undergoing orthodontic treatment with dentition size and shape reduction, 127 patients aged between 16 and 32 were examined. Patients with physiological occlusion and without any functional problems were included in the control group. Morpho-functional investigation of mandibular movement was conducted via a kinesiograph.
Results
All of the patients showed some functional problems on the frontal and lateral planes.
Conclusion
Improvements were seen with the regain and restoration of the edentulous spaces.
Keywords
Temporomandibular joint, TMJ, temporomandibular disorder, TMD, occlusal plane, muscular function.
Introduction
In order to determine a correct, comprehensive diagnosis of the maxillofacial system and the muscle chains, different methods of diagnosis are used, such as clinical examination, facial profile and photometry, anthropometric diagnostics of the dentition and occlusion, radiographic diagnostics (dental panoramic tomogram, lateral cephalogram, CT, MRI, etc.) and functional diagnosis (kinesiography, electromyography, myostimulation, posotonic state identification, etc.).
All these methods have been extensively investigated and applied in the orthodontic department of the Moscow State University of Medicine and Dentistry, Moscow, Russia. Owing to these kinds of diagnostic equipment, a correlation between orthodontic treatment with dentition size and shape reduction (owing to tooth extraction [Figs. 1a–c] or partial primary or secondary tooth edentia [Figs. 2a–c]) and temporomandibular disorder (TMD) has been observed.
In orthodontic practice, it is required to decide between extracting a tooth and closing the gap in the case of edentia. It is necessary to state that these border cases arise rather rapidly. It was decided to assess this issue from the perspective of different orthodontic approaches. The study was based on several scientific articles. 1Chua AL, Lim JY, Lubit EC. The effect of extraction versus nonextraction orthodontic treatment on the growth of the lower anterior face height.→ Am J Orthod Dentofacial Orthop. 1993 Oct;104(4):361–8.2Cusimano C, Mc Laughlin RP, Zernik JH. Effect of first bicuspid extractions on facial height in high-angle cases.
→ J Clin Orthod. 1993 Nov;27(11):594–8.3Drobocky OB, Smith RJ. Changes in facial profile during orthodontic treatment with extraction of four first premolars.
→ Am J Orthod Dentofacial Orthop. 1989 Mar;95(3):220–30.4Jones G, Buschang PH, Kim KB, Oliver DR. Class II non-extraction patients treated with the Forsus Fatigue Resistant Device versus intermaxillary elastics.
→ Angle Orthod. 2008 Mar;78(2):332–8.5Akinci Cansunar H, Uysal T. Comparison of orthodontic treatment outcomes in nonextraction, 2 maxillary premolar extraction, and 4 premolar extraction protocols with the American Board of Orthodontics objective grading system.
→ Am J Orthod Dentofacial Orthop. 2014 May;145(5):595–602.6Konstantonis D. The impact of extraction vs nonextraction treatment on soft tissue changes in Class I borderline malocclusions.
→ Angle Orthod. 2012 Mar;82(2):209–17.7Konstantonis D, Anthopoulou C, Makou M. Extraction decision and identification of treatment predictors in Class I malocclusions.
→ Prog Orthod. 2013 Nov 19;14:47. doi:10.1186/2196- 1042-14-47.8Kumari, M, Fida M. Vertical facial and dental arch dimensional changes in extraction vs. non-extraction orthodontic treatment.
→ J Coll Physicians Surg Pak. 2010 Jan;20(1):17–21.9Mair A, Hunder WS. Mandibular growth direction with conventional Class II nonextraction treatment.
→ Am J Orthod Dentofacial Orthop. 1992 Jun;101(6):543–49.10Mew J. Facial changes in identical twins treated by different orthodontic techniques.
→ World J Orthod. 2007 Summer;8(2):174–88.11Nelson B, Hansen K, Hägg U. Class II correction in patients treated with Class II elastics and with fixed functional appliances: a comparative study.
→ Am J Orthod Dentofacial Orthop. 2000 Aug;118(2):142–9.12Park S, Kudlick E, Abrahamian A. Vertical dimensional changes of the lips following four first premolar extractions in the North American Black.
→ Am J Orthod Dentofacial Orthop. 1989 Mar;95(3):270–1.13Sivakumar A, Valiathan A. Cephalometric assessment of dentofacial vertical changes in Class I subjects with and without extraction.
→ Am J Orthod Dentofacial Orthop. 2008 Jun;133(6):869–75.14Staggers JA. A comparison of results of second molar and first premolar extraction treatment.
→ Am J Orthod Dentofacial Orthop. 1990 Nov;98(5):430–6.15Staggers JA. Vertical changes following first premolar extractions.
→ Am J Orthod Dentofacial Orthop. 1994 Jan;105(1):19–24.16Stromboni Y. Facial aesthetics in orthodontic treatment with and without extractions.
→ Eur J Orthod. 1979;1(3):201–6.17Kim TK, Kim JT, Mah J, Yang WS, Baek SH. First or second premolar extraction effects on facial vertical dimension.
→ Angle Orthod. 2005 Mar;75(2):177–82.18Travess H, Roberts-Harry D, Sandy G. Orthodontics. Part 8: extractions in orthodontics.
→ Br Dent J. 2004 Feb 28;196(4):195–203.19Tulley WJ. The role of extractions in orthodontic treatment.
→ Br Dent J. 1959;107:199–205.20Yamaguchi K, Nanda RS. The effects of extraction and nonextraction treatment on the mandibular position.
→ Am J Orthod Dentofacial Orthop. 1991 Nov;100(5):443–52.
All of the structures of our body are phylogenetically connected. There is obvious continuity from vertebral column to cranium. All cranial bones are generated from the first three vertebrae during the evolutionary process. There are also two subsystems that unite the entire body: the craniosacral and craniomandibular ones, joining together in the central nervous system. They are divided into musculoaponeurotic chains, starting from the cranial bones.21Clauzade M, Marty JP. Orthoposturodontie. Perpignan: Éditions SEOO; 1998.22Clauzade M, Marty JP. Orthoposturodontie 2. Perpignan: Éditions SEOO; 2006. In light of this, it is necessary to know that all body systems are able to change during orthodontic treatment. Occlusal changes also influence the connection of cranial bones and as a result they can lead to TMD. By reorganizing the systems, we can improve stability and quality of treatment.
-

- Fig. 1a

-

- Fig. 1b

-

- Fig. 1c

-

- Fig. 2a

-

- Fig. 2b

-

- Fig. 2c

Figs. 1a-c
The patient after orthodontic treatment (several years ago) with the second premolar extraction
Figs. 2a-c
The patient after orthodontic treatment with space closure (primary edentia of tooth #22).
Therefore, while different authors’ conclusions about extraction or nonextraction treatment are based on clinical, radiographic, CT or MRI examination, there are insufficient data on muscle adaptation to decide on the treatment in this case. There are no scientific reports on changes to the temporomandibular joint (TMJ) and muscle system after orthodontic treatment with dentition size and shape reduction (owing to tooth extraction or partial primary or secondary tooth edentia). This makes it difficult to evaluate the treatment choices properly in relation to the effect on the muscles and TMJ. These parameters are known as being essential for patients’ health. Consequently, the aim of this study was to improve diagnostic methods after orthodontic treatment with dentition size and shape reduction using computed diagnostic equipment.
Materials and methods
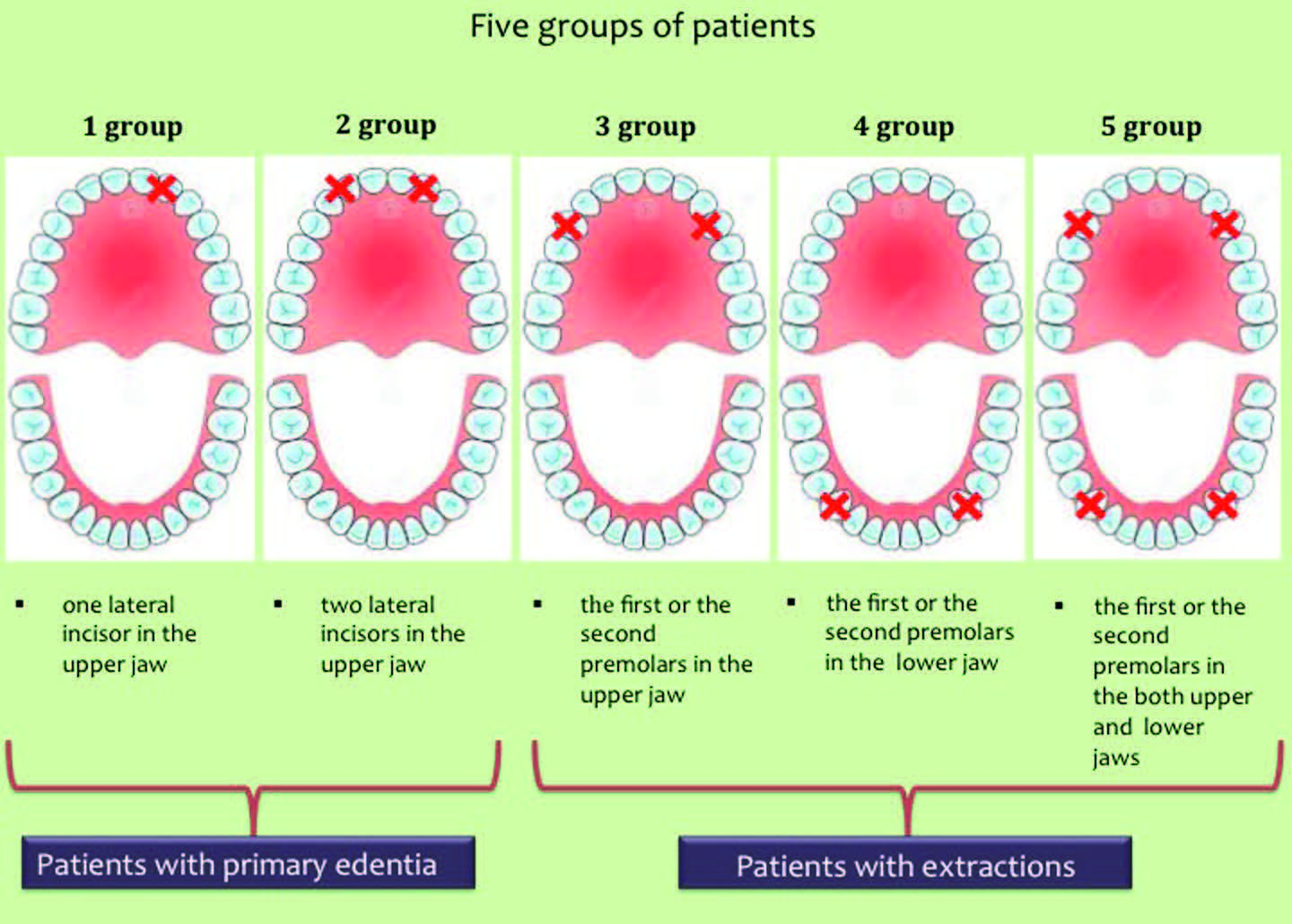
This cross-sectional observational study included 127 patients aged between 16 and 32 during a period of two years. The patients were examined after orthodontic treatment that included dentition size and shape reduction for partial primary or secondary tooth edentia. Five groups of patients were selected according to the area of the absent teeth (Fig. 3):
- absence of one lateral incisor in the upper jaw; composed of 21 patients;
- absence of two lateral incisors in the upper jaw; composed of 16 patients;
- absence of the first or the second premolar in the upper jaw; composed of 24 patients;
- absence of the first or the second premolar in the lower jaw; composed of 19 patients;
- absence of the first or the second premolar in both the upper and lower jaws, composed of 22 patients.
-
- Fig. 3
Fig. 3
Five groups of patients were selected according to the area of the absent teeth.
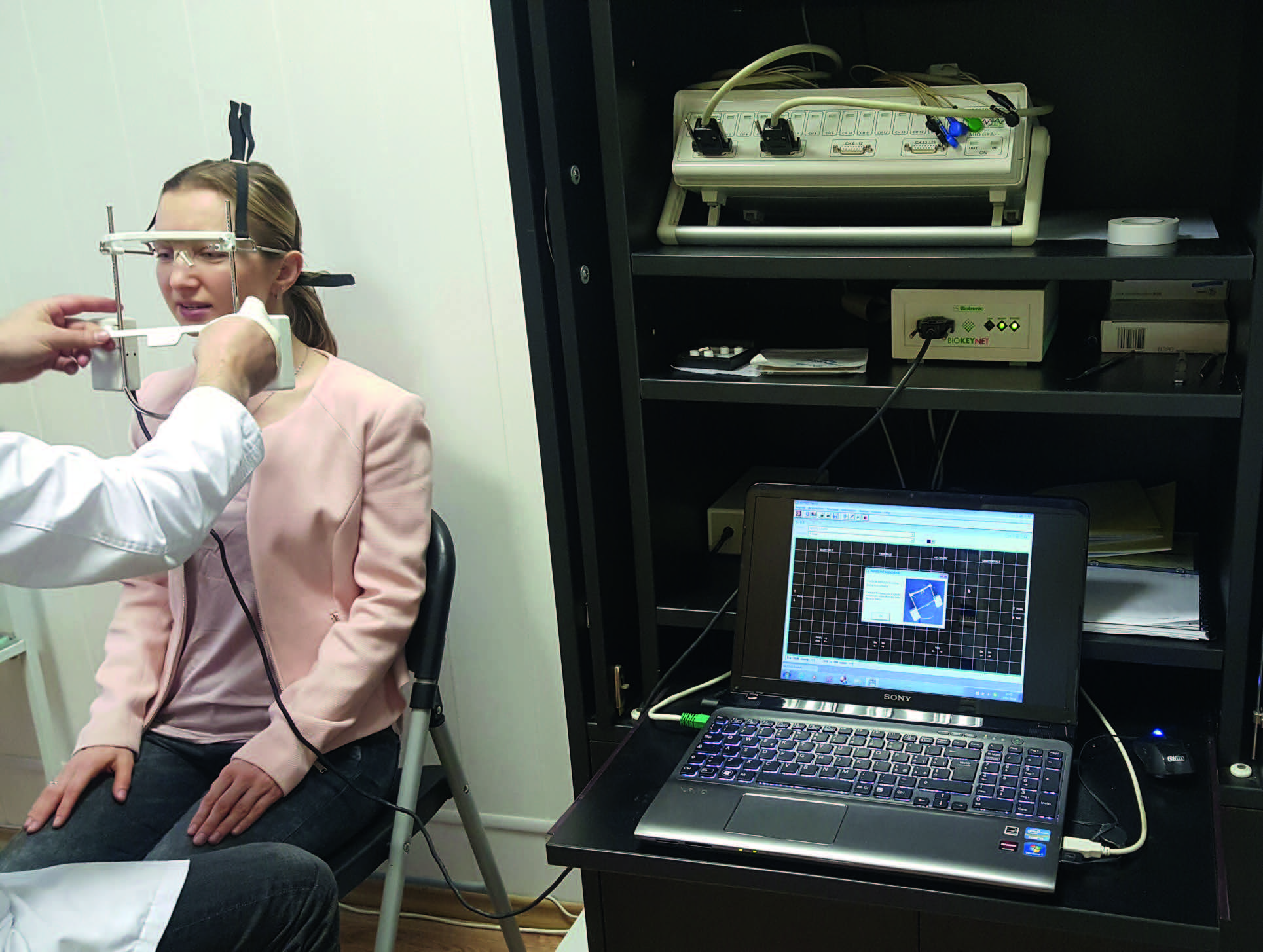
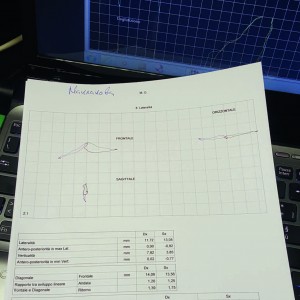
Moreover, a control group was formed of 25 patients with physiological occlusion and without any functional problems. Morpho-functional investigation of mandibular movement was conducted using a kinesiograph (BioKeyNet, Bioket, San Benedetto del Tronto, Italy; Fig. 4). Kinesiography is the precise registration of the various movements of the mandible in three planes—sagittal, frontal and horizontal—including muscle contraction speed with complex performance in graphic and digital forms (Fig. 5).23Cesaretti G, Gobbi G. Affidabilità e riproducibilità dell’ esame kinesiografico [Internet].
→ San Benedetto del Tronto. 2013 Oct [cited 2017 May 17]. Availablefrom: https://drive.google.com/ file/d/0BxWIqv7tas3tb1NXX2k1eGNzSWM/ view.24Klimova T. Study of mandible movements in patients with physiologic and distal occlusion, in different age groups, using the kinesiographic method [thesis]. [Moscow]: Moscow State University of Medicine and Dentistry; 2010.
-

- Fig. 4
-
- Fig. 5
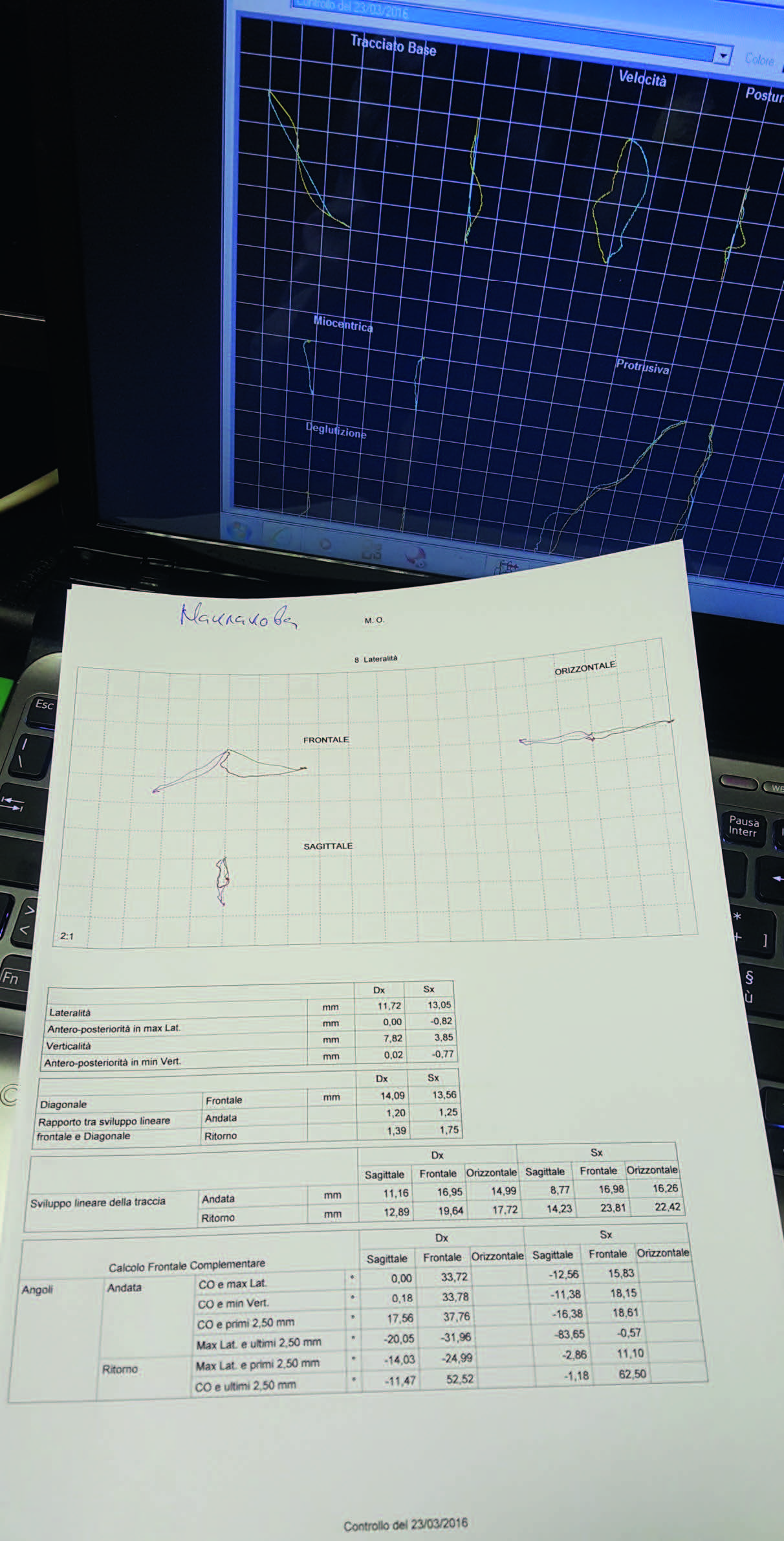
Fig. 4
The BioKeyNet kinesiograph and the patient wearing the kinesiograph mask.
Fig. 5
Kinesiographic interpretation in graphic and digital forms.
In order to assess the current morphofunctional condition of the entire dentoalveolar system, the following functional tests and their further modification were set in various planes:
- maximum mandibular lowering and lifting;
- maximum mandibular lowering and lifting with regular and maximum movement speed;
- maximum mandibular extension (a movement path was studied, including an individual angle of mandibular lowering and the trajectory of mandibular protrusion and its deviation);
- maximum lateral mandibular movement (investigation was conducted on the trajectory of a mandibular movement and its individual angle, turning to the right and to the left);
- mandibular movement from its regular physiological rest position to its common teeth joining myocentric index (an individual angle was tested to perform a mandibular anterior or posterior movement).25Klimova T. Study of mandible movements in patients with physiologic and distal occlusion, in different age groups, using the kinesiographic method [thesis]. [Moscow]: Moscow State University of Medicine and Dentistry; 2010.
Results
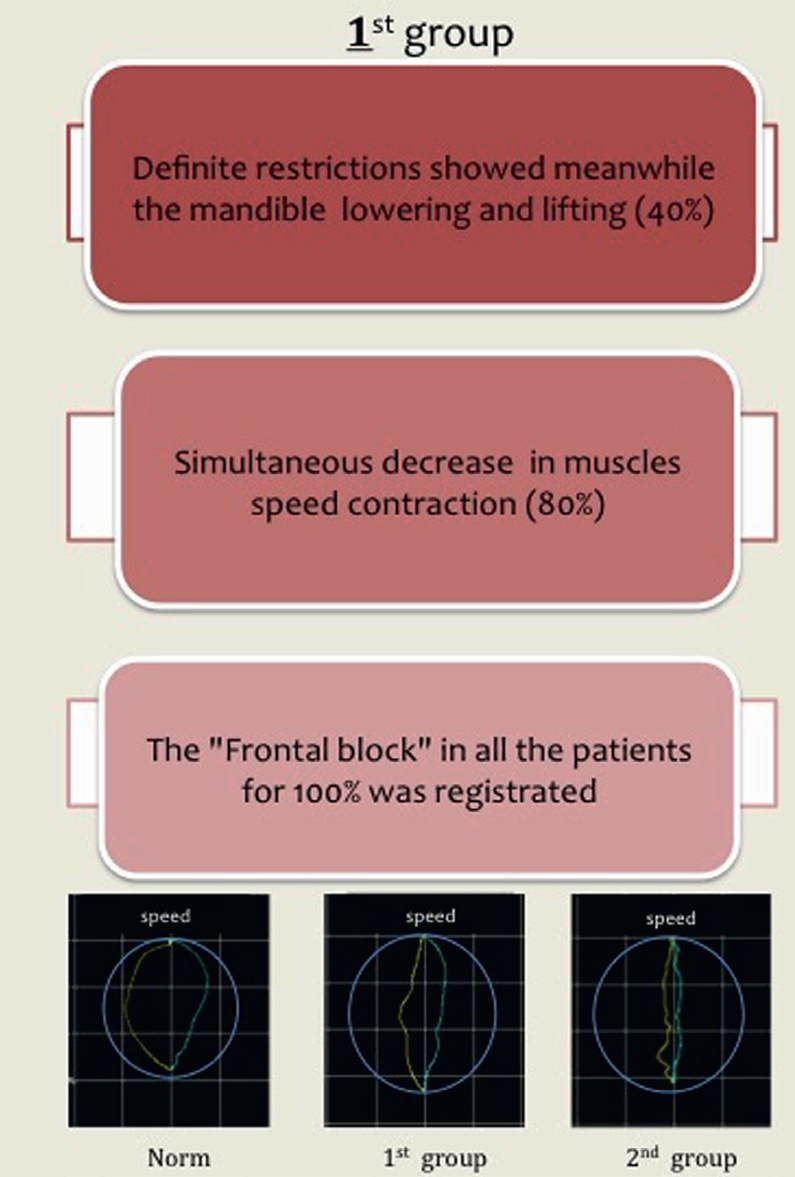
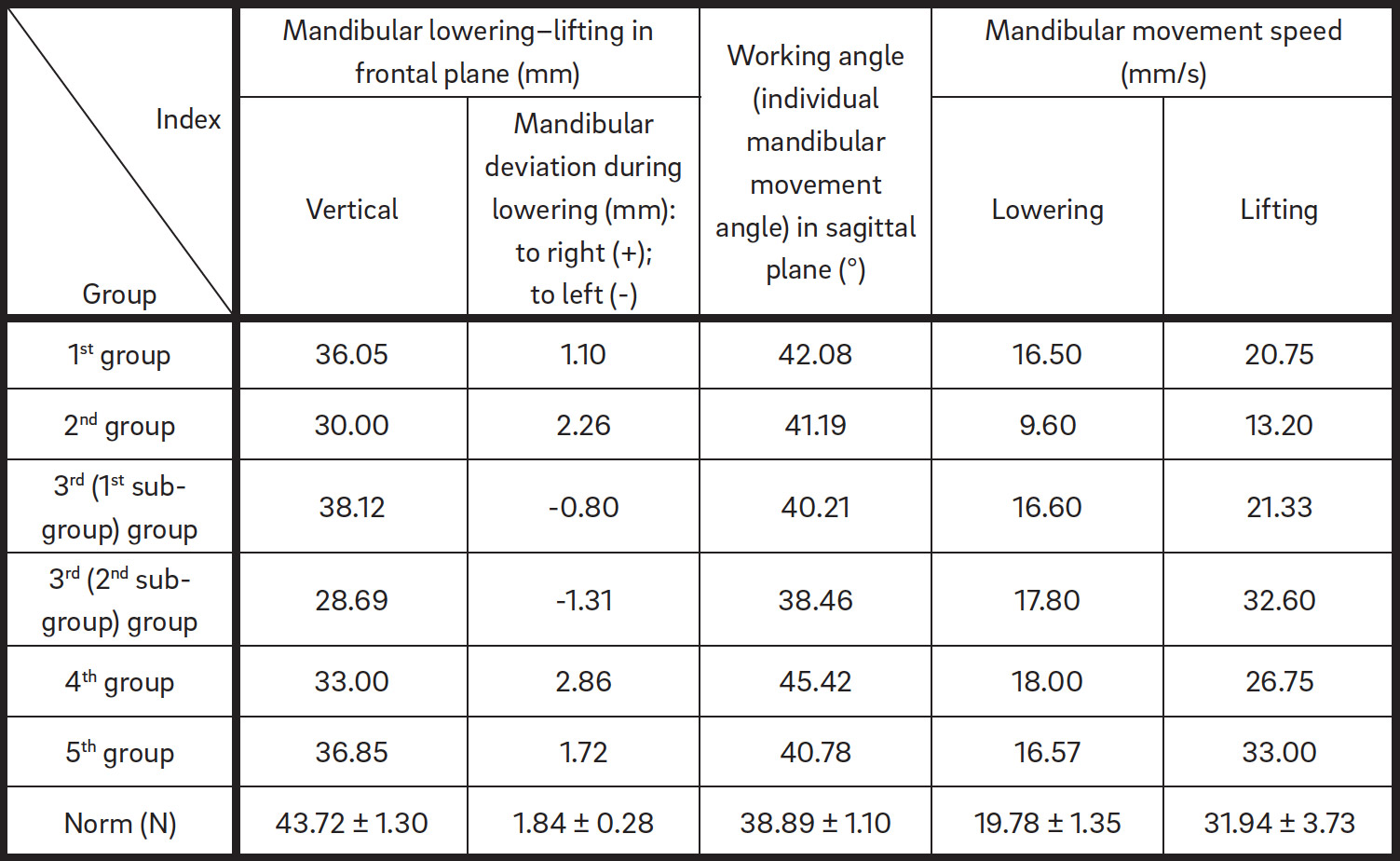
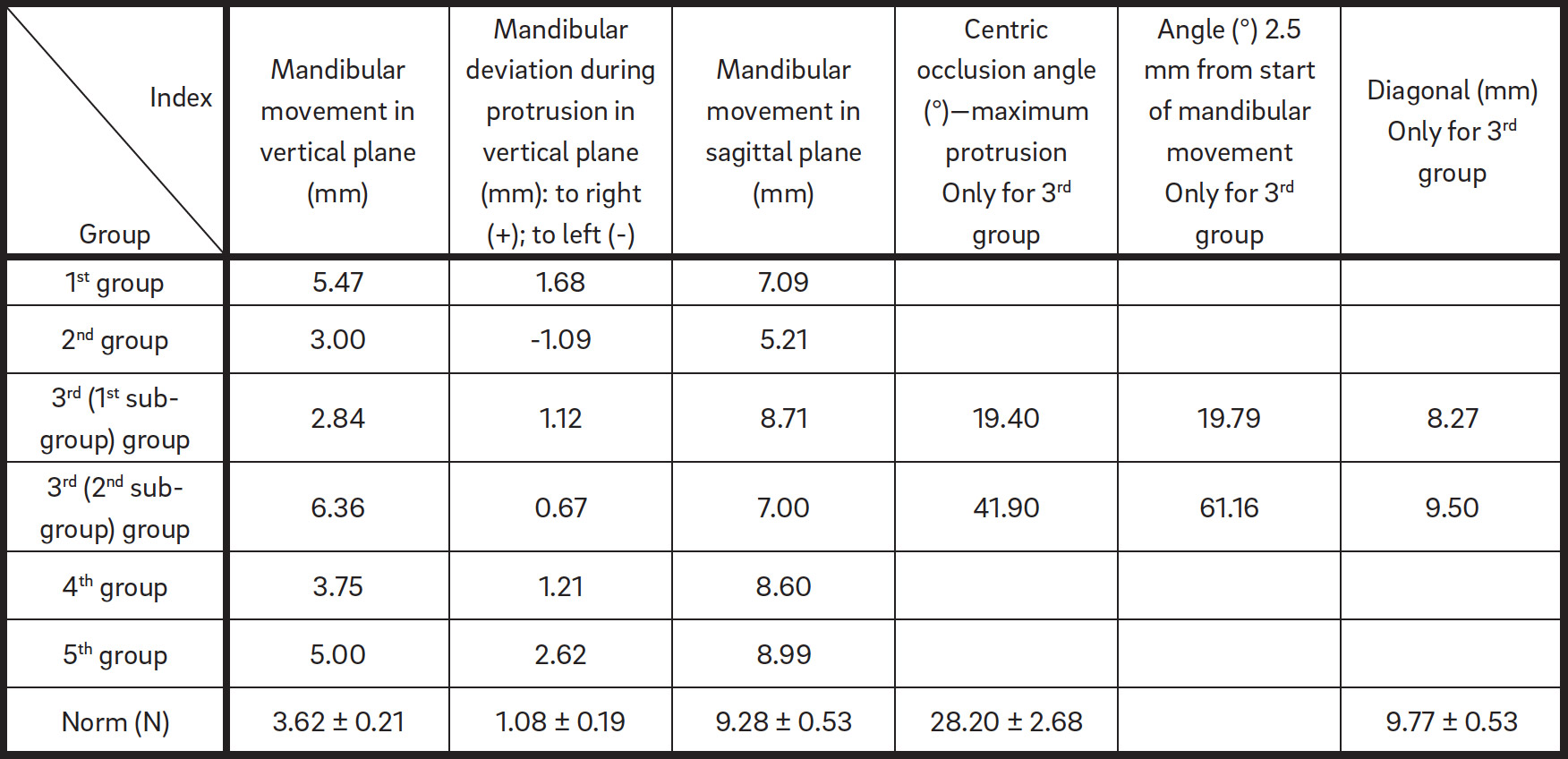
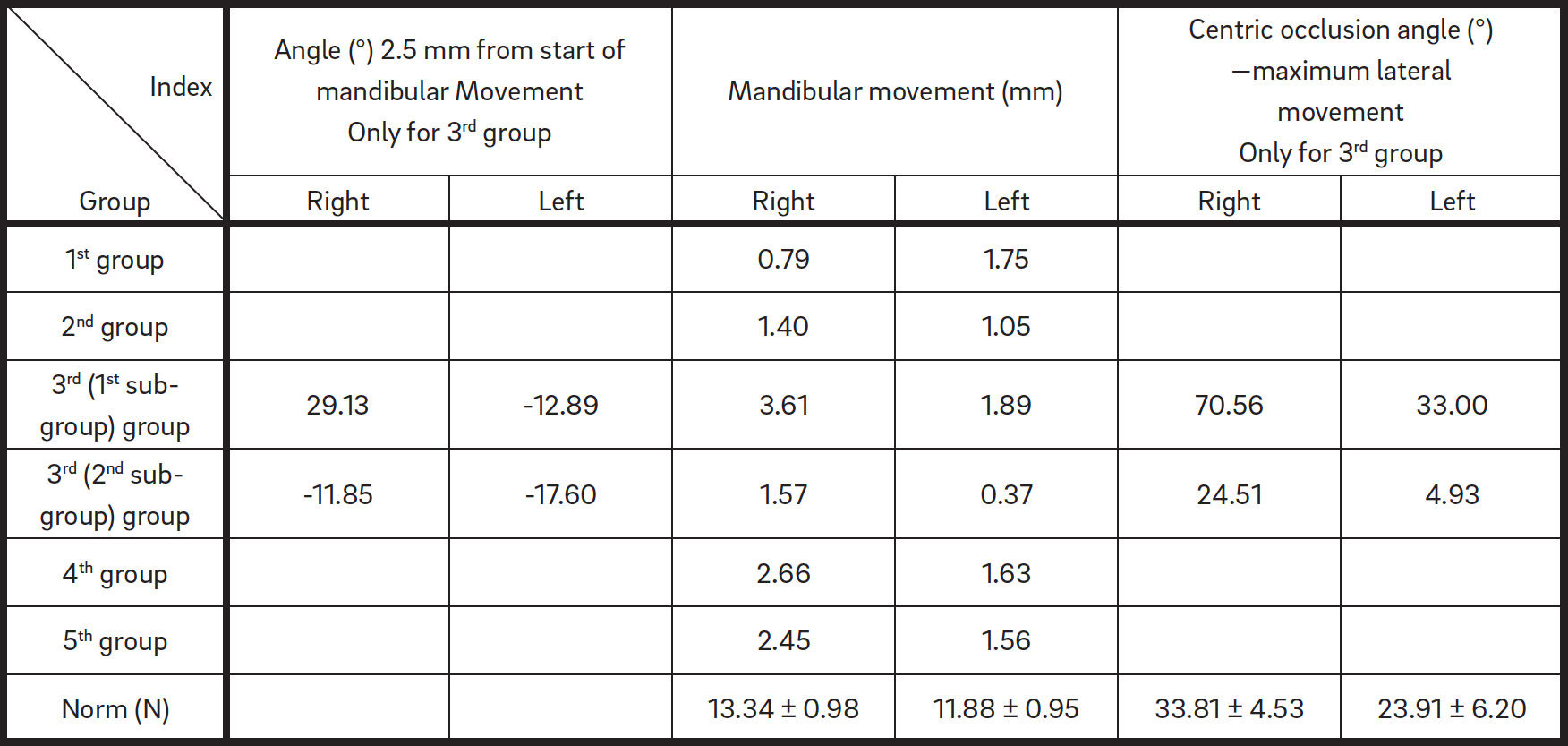
The first group showed well-defined restrictions. While the mandible was lowered and lifted in the frontal plane, a simultaneous decrease in muscle contraction speed was seen in 80% of these patients, particularly in the vertical index (Fig. 6; Table 1). In the mandibular movement in the sagittal plane, a frontal block was observed. This block was also registered in all patients in the remaining groups (Table 2).
In the second group, the mandibular lowering and lifting led to its deviation and to the decreasing of the muscle contraction speed (Fig. 7; Table 1). This occurrence was even more marked compared with that seen in the first group, owing to the more distal position of the mandible (Table 3). The protrusive movement according to angle showed a significant frontal block and difficulty during mandibular movement (Fig. 8; Table 2). This group was also characterized by blocked mandible lateral movement to both the right and the left sides, with trajectories simultaneously shortening (Tables 4 & 5). TMD was seen in 60% of patients, while 40% of patients exhibited full blocking of lateral and protrusive movement.
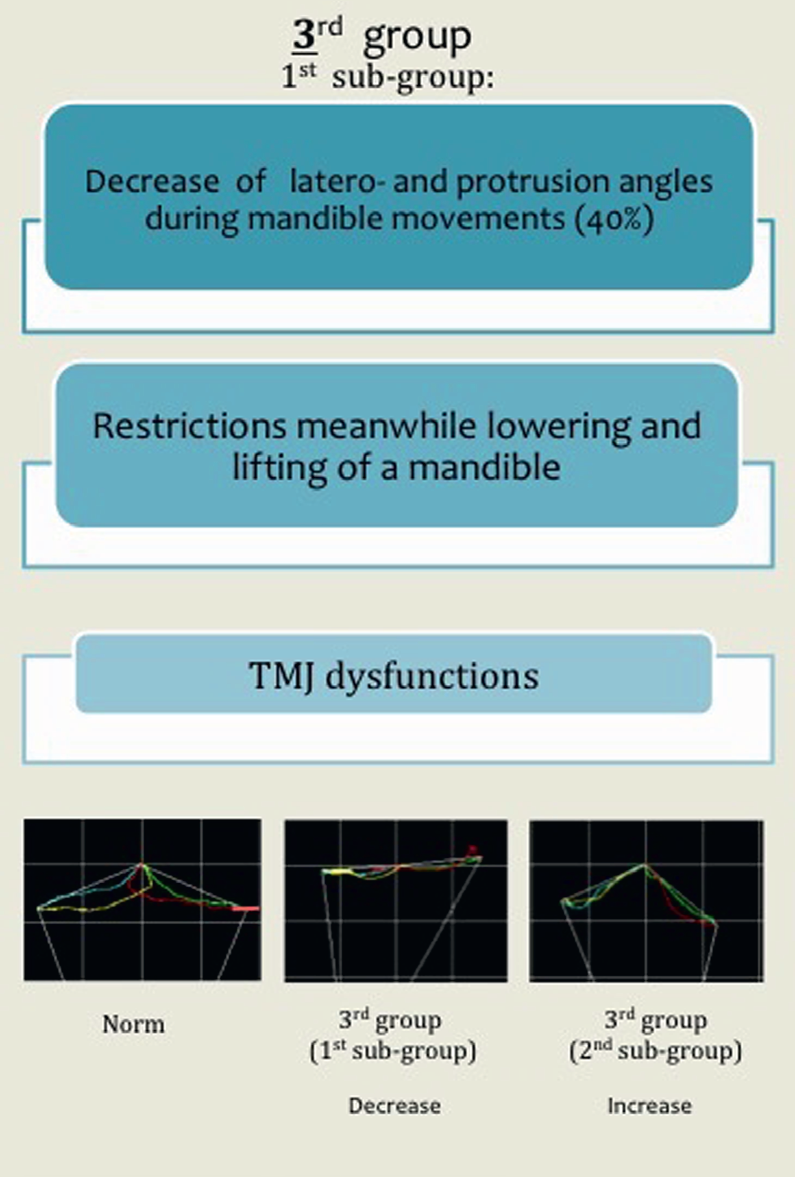
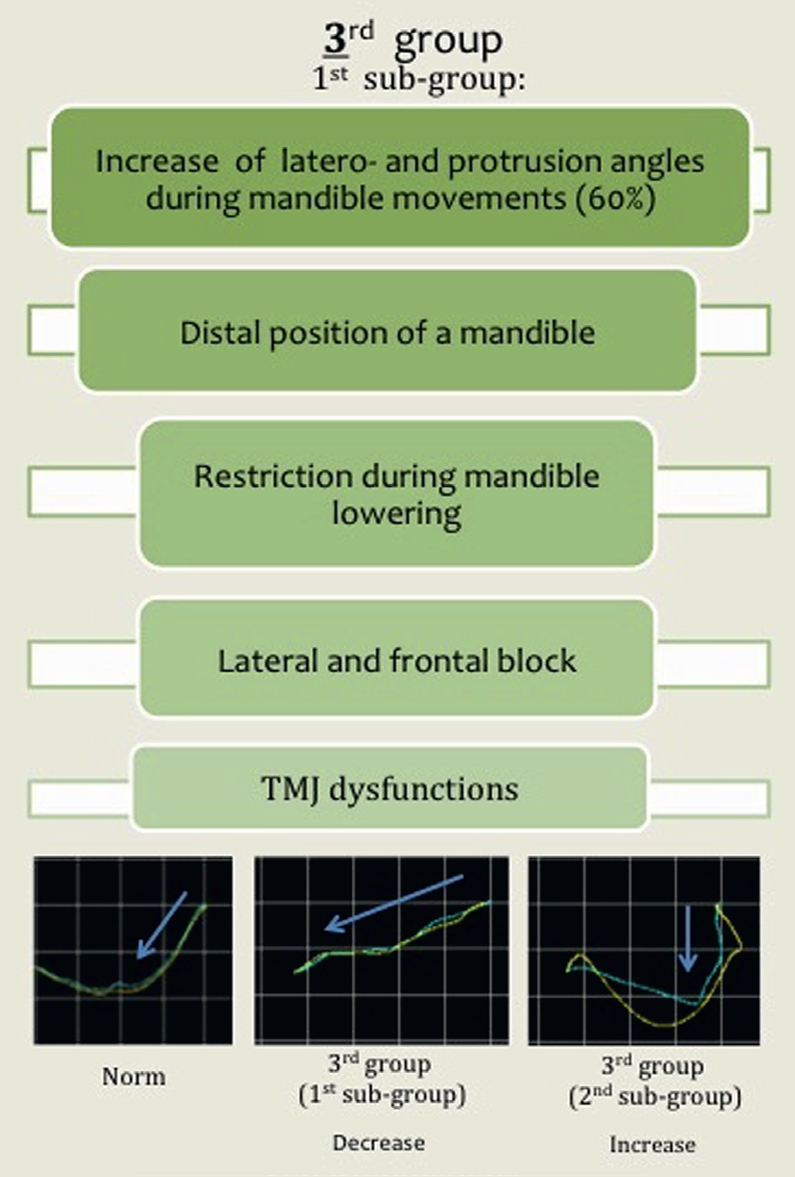
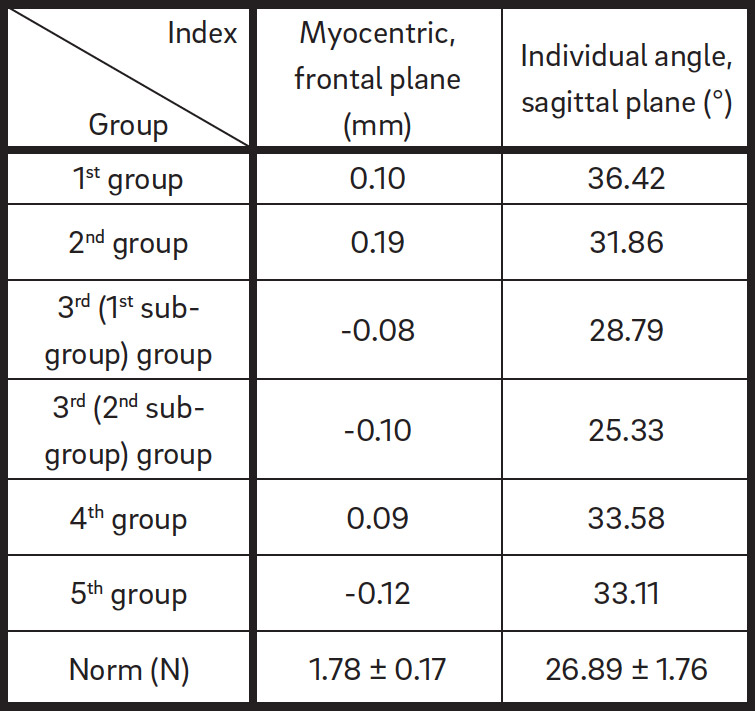
The third group was divided into two subgroups according to the type of mandibular movement. The first subgroup (40% of the patients) was characterized by a severe decrease (flat angles) of lateral and protrusive angles (Tables 2, 4 & 5; Figs. 8 & 9). In contrast, the second subgroup (60% of the patients) showed an obvious increase (deep angles) of the lateral and protrusive angles (Tables 2, 4 & 5; Figs. 8 & 9). These outcomes showed an impairment of the essential lateral and frontal mandibular movements. Furthermore, the second subgroup was characterized by a distal position of the mandible (Table 3), restriction of movement during its lowering and lifting, and TMD (Table 1).
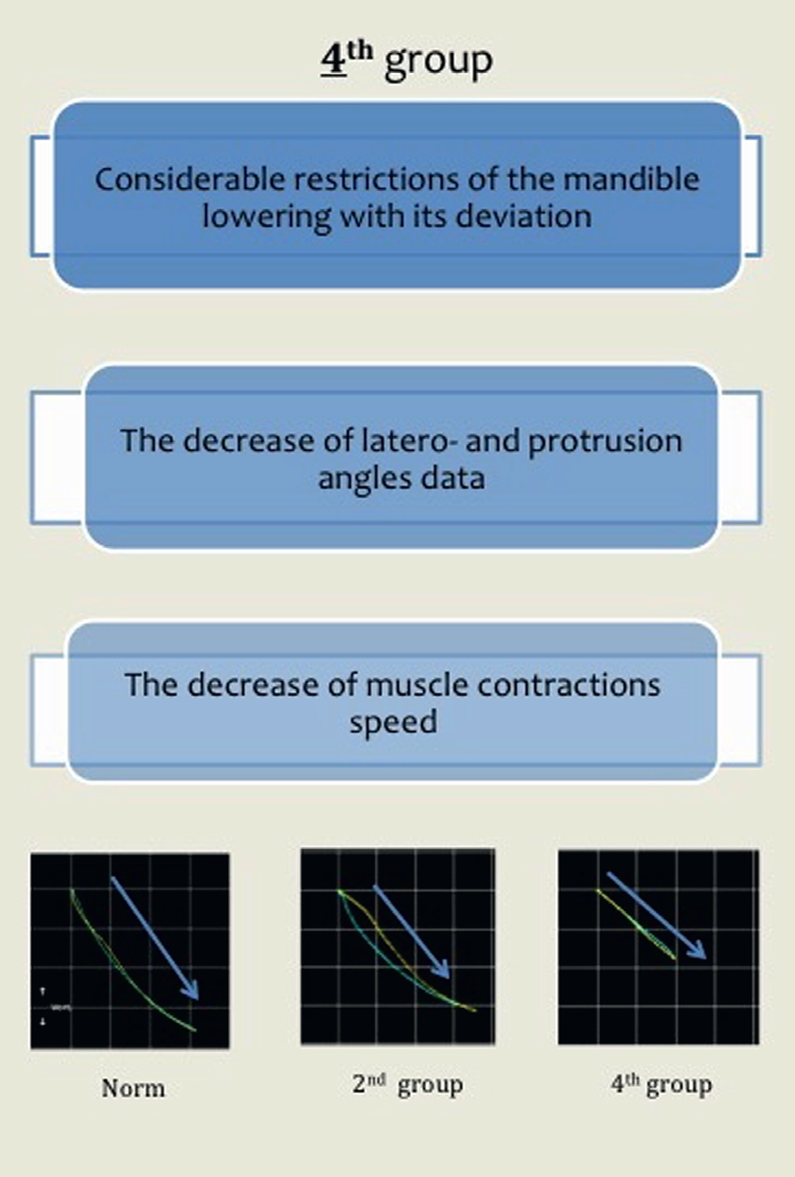
In the fourth group, all of the patients without exception (100%) showed considerable restriction of mandibular lowering with its deviation (Fig. 10), restriction of the muscle contraction speed (Table 1), and a decrease of the lateral and the protrusive angles (Tables 2, 4 & 5).
In the fifth group, restriction of mandibular lowering and lifting (36.85 mm) and its deviation during protrusion (2.62 mm) were observed (Table 2). The mandibular movement restriction to the left side (2.40 mm) showed values double that of the right side (1.56 mm; Tables 4 & 5; Fig. 11). This group exhibited a distal position of the mandible (Table 3) and TMD.
-
- Fig. 6
-

- Fig. 7
-
- Fig. 8
-
- Fig. 9
-
- Fig. 10
-

- Fig. 11
Clinical case
A patient came to our clinic after a previous treatment performed in another private clinic. She complained of great discomfort in the TMJ area. The previous treatment had included the extraction of the second premolars of the lower jaw. The following diagnostic scheme was carried out in our clinic, according to the protocol for patients with TMD:
- anthropometric studies of digital jaw models (3-D scanning);
- radiographic diagnosis;
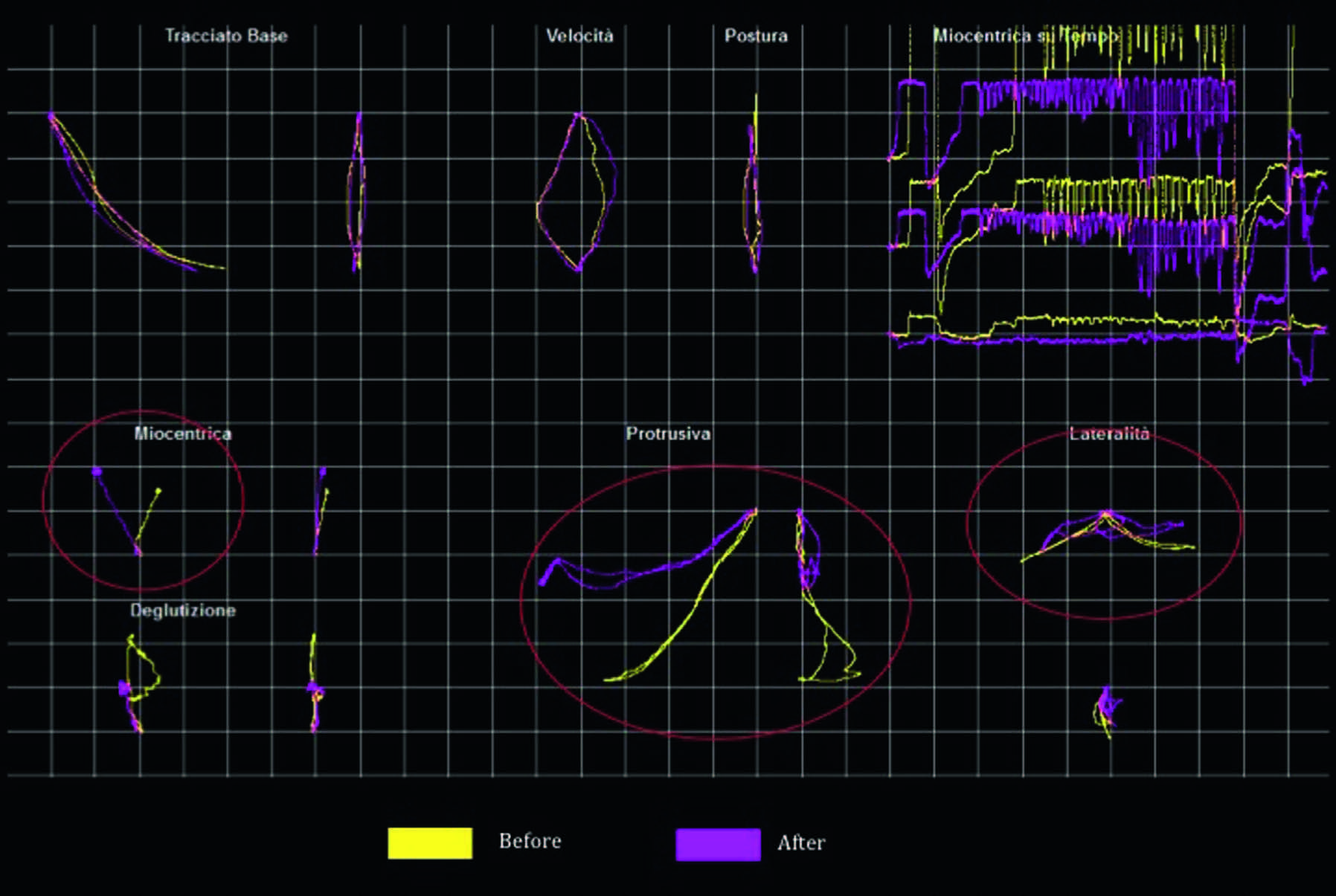
- morpho-functional diagnosis using a kinesiograph (Figs. 12 & 13), which showed a significant frontal block, a distal position of the mandible, TMD and a rotation of the occlusal plane.
During the one-year treatment in our department, the second premolar regions were regained and prepared for implant placement (Figs. 14a–c). After the treatment, the kinesiographic data showed significant improvements. The myocentric graph indicated a change of the mandibular movement direction, the laterotrusion graph revealed normalization of the occlusal plane and the protrusion graph showed elimination of the frontal block (Fig. 13).
-

- Fig. 12
-

- Fig. 13a
-

- Fig. 13b
-

- Fig. 13c
-
- Fig. 14
Discussion
A number of authors have carried out particular assessment in order to compare two approaches to patient treatment: extraction or nonextraction. 26Baumrind S. Adult orthodontic therapy: extraction versus non-extraction.
→ Clin Orthod Res. 1998 Nov;1(2):130–41.27Germeç D, Taner T. Effects of extraction and nonextraction therapy with air-rotor stripping on facial esthetics in postadolescent borderline patients.
→ Am J Orthod Dentofacial Orthop. 2008 Apr;133(4):539–49.28Saelens NA, De Smit AA. Therapeutic changes in extraction versus non-extraction orthodontic treatment.
→ Eur J Orthod. 1998 Jun;20(3):225–36. Various combinations of tooth extraction have been examined, and most of these cases were located in the area of the premolars (from one to four teeth). The requisite data were gained from models and radiographs before, during and after the treatment. Also, authors compared changes in extraction versus nonextraction orthodontic treatment using pre- and post-treatment lateral cephalograms, comparing the skeletal, dental and soft-tissue profile changes, but no functional diagnostics or TMJ condition study was performed. For example, an investigation was carried out at the University of California, San Francisco Graduate Orthodontic Clinic on treatment for correction of a Class I or II malocclusion. There were 148 patients examined. With regard to the primary decision as to whether extraction or nonextraction treatment was to be preferred, agreement among clinicians was higher than had been anticipated, but how did the clinicians make their decision on whether to extract? Crowding was cited as the first reason in 49% of decisions to extract, followed by incisor protrusion (14%). Clinicians focused heavily on appearance-related factors that are qualitatively determinable by physical examination of the surface structures of the face and teeth, but no functional tests were conducted.29Baumrind S, Korn E, Boyd R, Maxwell R. The decision to extract: Part 1—interclinician agreement.
→ Am J Orthod Dentofacial Orthop. 1996 Mar;109(3):297–309.30Baumrind S, Korn E, Boyd R, Maxwell R. The decision to extract: Part II. Analysis of clinicians’ stated reasons for extraction.
→ Am J Orthod Dentofacial Orthop. 1996 Apr;109(4):393–402.
Nevertheless, there is no one common approach to the decision on whether it is necessary to extract teeth as long as such clinical situations continue to arise.31Jones G, Buschang PH, Kim KB, Oliver DR. Class II non-extraction patients treated with the Forsus Fatigue Resistant Device versus intermaxillary elastics.
→ Angle Orthod. 2008 Mar;78(2):332–8. In most cases, authors insist that tooth extractions are significant only for surgical patients. Furthermore, it is known that it is better not to perform tooth extractions with border cases in order to avoid further complications. 32Mair A, Hunder WS. Mandibular growth direction with conventional Class II nonextraction treatment.
→ Am J Orthod Dentofacial Orthop. 1992 Jun;101(6):543–49.
We highly agree with authors who suggest provision of nonextraction orthodontic treatment by using finishing wires of a particular material, size and arch form. The main determinants of final arch form and dimension appear to be the original muscular and occlusally related arch form and dimension and the amount of crowding to be relieved. 33Allan D, Woods M. Arch-dimensional changes in non-extraction cases with finishing wires of a particular material, size and arch form.
→ Aust Orthod J. 2015 May;31(1):26–36. Evident changes in soft tissue and dentoalveolar characteristics appear with tooth extraction than is the case with dental arch expansion and tooth movement. Also, several studies have been conducted to estimate the effect of dental arch length reduction (owing to dental extractions, dental agenesis and dental malpositions) during orthodontic treatment on the upper airway development.34Haddad S, Kerbrat JB, Schouman T, Goudot P. [Effect of dental arch length decrease during orthodontic treatment in the upper airway development. A review].
→ Orthod Fr. 2017 Mar;88(1):25–33. French.
To our regret, there are no scientific reports on changes to the TMJ, muscle system and mandibular movements after orthodontic treatment with extraction. However, in our opinion, these indicators are more important than esthetic indicators. Esthetic indicators will be harmonious only when both morphological and functional indicators are taken into account.
All the methods for orthodontic research can be considered as a background for making a decision on further treatment and precise consequence assessment. The more initial scientific planning is carried out, the more effective the treatment scheme formed and accomplished will be. Overall, orthodontic treatment planning, with or without extraction, is supposed to take into account not only morphological parameters but also parameters vital for function. Functional investigation of patients should be extensive and applied in current orthodontic practice.
Conclusion
In all of the groups examined after orthodontic treatment that included dentition size and shape reduction for partial primary or secondary tooth edentia, problems were registered during mandibular movements. These problems were mainly related to the restriction of mandibular movement during lowering and lifting, of lateral movement and of muscle contraction speed. Moreover, TMD was reported. Improvements were seen with the regain and restoration of the edentulous spaces.
Competing interests
The present study was self-funded. All of the authors declare no conflict of interests.

Interview
with Gianfranco Cesaretti
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Chua AL, Lim JY, Lubit EC. The effect of extraction versus nonextraction orthodontic treatment on the growth of the lower anterior face height.→ Am J Orthod Dentofacial Orthop. 1993 Oct;104(4):361–8. |
| 2. | ↑ | Cusimano C, Mc Laughlin RP, Zernik JH. Effect of first bicuspid extractions on facial height in high-angle cases. → J Clin Orthod. 1993 Nov;27(11):594–8. |
| 3. | ↑ | Drobocky OB, Smith RJ. Changes in facial profile during orthodontic treatment with extraction of four first premolars. → Am J Orthod Dentofacial Orthop. 1989 Mar;95(3):220–30. |
| 4, 31. | ↑ | Jones G, Buschang PH, Kim KB, Oliver DR. Class II non-extraction patients treated with the Forsus Fatigue Resistant Device versus intermaxillary elastics. → Angle Orthod. 2008 Mar;78(2):332–8. |
| 5. | ↑ | Akinci Cansunar H, Uysal T. Comparison of orthodontic treatment outcomes in nonextraction, 2 maxillary premolar extraction, and 4 premolar extraction protocols with the American Board of Orthodontics objective grading system. → Am J Orthod Dentofacial Orthop. 2014 May;145(5):595–602. |
| 6. | ↑ | Konstantonis D. The impact of extraction vs nonextraction treatment on soft tissue changes in Class I borderline malocclusions. → Angle Orthod. 2012 Mar;82(2):209–17. |
| 7. | ↑ | Konstantonis D, Anthopoulou C, Makou M. Extraction decision and identification of treatment predictors in Class I malocclusions. → Prog Orthod. 2013 Nov 19;14:47. doi:10.1186/2196- 1042-14-47. |
| 8. | ↑ | Kumari, M, Fida M. Vertical facial and dental arch dimensional changes in extraction vs. non-extraction orthodontic treatment. → J Coll Physicians Surg Pak. 2010 Jan;20(1):17–21. |
| 9, 32. | ↑ | Mair A, Hunder WS. Mandibular growth direction with conventional Class II nonextraction treatment. → Am J Orthod Dentofacial Orthop. 1992 Jun;101(6):543–49. |
| 10. | ↑ | Mew J. Facial changes in identical twins treated by different orthodontic techniques. → World J Orthod. 2007 Summer;8(2):174–88. |
| 11. | ↑ | Nelson B, Hansen K, Hägg U. Class II correction in patients treated with Class II elastics and with fixed functional appliances: a comparative study. → Am J Orthod Dentofacial Orthop. 2000 Aug;118(2):142–9. |
| 12. | ↑ | Park S, Kudlick E, Abrahamian A. Vertical dimensional changes of the lips following four first premolar extractions in the North American Black. → Am J Orthod Dentofacial Orthop. 1989 Mar;95(3):270–1. |
| 13. | ↑ | Sivakumar A, Valiathan A. Cephalometric assessment of dentofacial vertical changes in Class I subjects with and without extraction. → Am J Orthod Dentofacial Orthop. 2008 Jun;133(6):869–75. |
| 14. | ↑ | Staggers JA. A comparison of results of second molar and first premolar extraction treatment. → Am J Orthod Dentofacial Orthop. 1990 Nov;98(5):430–6. |
| 15. | ↑ | Staggers JA. Vertical changes following first premolar extractions. → Am J Orthod Dentofacial Orthop. 1994 Jan;105(1):19–24. |
| 16. | ↑ | Stromboni Y. Facial aesthetics in orthodontic treatment with and without extractions. → Eur J Orthod. 1979;1(3):201–6. |
| 17. | ↑ | Kim TK, Kim JT, Mah J, Yang WS, Baek SH. First or second premolar extraction effects on facial vertical dimension. → Angle Orthod. 2005 Mar;75(2):177–82. |
| 18. | ↑ | Travess H, Roberts-Harry D, Sandy G. Orthodontics. Part 8: extractions in orthodontics. → Br Dent J. 2004 Feb 28;196(4):195–203. |
| 19. | ↑ | Tulley WJ. The role of extractions in orthodontic treatment. → Br Dent J. 1959;107:199–205. |
| 20. | ↑ | Yamaguchi K, Nanda RS. The effects of extraction and nonextraction treatment on the mandibular position. → Am J Orthod Dentofacial Orthop. 1991 Nov;100(5):443–52. |
| 21. | ↑ | Clauzade M, Marty JP. Orthoposturodontie. Perpignan: Éditions SEOO; 1998. |
| 22. | ↑ | Clauzade M, Marty JP. Orthoposturodontie 2. Perpignan: Éditions SEOO; 2006. |
| 23. | ↑ | Cesaretti G, Gobbi G. Affidabilità e riproducibilità dell’ esame kinesiografico [Internet]. → San Benedetto del Tronto. 2013 Oct [cited 2017 May 17]. Availablefrom: https://drive.google.com/ file/d/0BxWIqv7tas3tb1NXX2k1eGNzSWM/ view. |
| 24, 25. | ↑ | Klimova T. Study of mandible movements in patients with physiologic and distal occlusion, in different age groups, using the kinesiographic method [thesis]. [Moscow]: Moscow State University of Medicine and Dentistry; 2010. |
| 26. | ↑ | Baumrind S. Adult orthodontic therapy: extraction versus non-extraction. → Clin Orthod Res. 1998 Nov;1(2):130–41. |
| 27. | ↑ | Germeç D, Taner T. Effects of extraction and nonextraction therapy with air-rotor stripping on facial esthetics in postadolescent borderline patients. → Am J Orthod Dentofacial Orthop. 2008 Apr;133(4):539–49. |
| 28. | ↑ | Saelens NA, De Smit AA. Therapeutic changes in extraction versus non-extraction orthodontic treatment. → Eur J Orthod. 1998 Jun;20(3):225–36. |
| 29. | ↑ | Baumrind S, Korn E, Boyd R, Maxwell R. The decision to extract: Part 1—interclinician agreement. → Am J Orthod Dentofacial Orthop. 1996 Mar;109(3):297–309. |
| 30. | ↑ | Baumrind S, Korn E, Boyd R, Maxwell R. The decision to extract: Part II. Analysis of clinicians’ stated reasons for extraction. → Am J Orthod Dentofacial Orthop. 1996 Apr;109(4):393–402. |
| 33. | ↑ | Allan D, Woods M. Arch-dimensional changes in non-extraction cases with finishing wires of a particular material, size and arch form. → Aust Orthod J. 2015 May;31(1):26–36. |
| 34. | ↑ | Haddad S, Kerbrat JB, Schouman T, Goudot P. [Effect of dental arch length decrease during orthodontic treatment in the upper airway development. A review]. → Orthod Fr. 2017 Mar;88(1):25–33. French. |





Leave a Reply
Be the First to Comment!