Open-cohort prospective study on early implant failure and physiological marginal remodeling expected using sandblasted and acid-etched bone level implants featuring an 11° Morse taper connection within one year after loading
March 22, 2017 / Categories: Digital Dentistry, Implant Dentistry

Tallarico, Marco

Meloni, Silvio Mario
The objective of this study was to evaluate the implant survival and success rates as well as the physiological marginal bone remodeling expected using Osstem implants.
Introduction
During the first year of function, a certain amount of physiological marginal bone loss is expected around a dental implant, both horizontally and vertically; thereafter, minimal further bone loss has been observed.1Roos J, Sennerby L, Lekholm U, Jemt T, Gröndahl K, Albrektsson T. A qualitative and quantitative method for evaluating implant success: a 5-year retrospective analysis of the Brånemark implant.
→ Int J Oral Maxillofac Implants. 1997 Jul-Aug;12(4):504–14.2Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success.
→ Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25.
Marginal bone loss (MBL) of 1.5–2.0 mm during the first year of function has been assumed as normal.3Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success.
→ Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. Afterward tissue stability is expected.4Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success.
→ Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25.
5Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz- Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference.
→ Implant Dent. 2008 Mar;17(1):5–15.6Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: a systematic review.
→ J Dent Res. 2012 Mar;91(3):242–8.However, the criteria for defining success in implant dentistry are under constant debate in consensus statements and observational studies. Papaspyridakos et al. proposed parameters related to soft- and hard-tissue stability that can influence the progression of MBL around implants, but is not clear whether the physiological bone remodeling is prosthesis-related, host-related, implant-related or load-dependent. 7Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: a systematic review.
→ J Dent Res. 2012 Mar;91(3):242–8. As a result, although numerous studies have reported improvements in implant design and protocols to minimize this MBL, the utilized criteria for success have remained unchanged.
Several factors may increase MBL around dental implants, including surgical trauma, implant–abutment connection type, biological width establishment, mucosal tissue thickness, keratinized tissue width and bone density.8Nevins M, Nevins ML, Camelo M, Boyesen JL, Kim DM. Human histologic evidence of a connective tissue attachment to a dental implant.
→ Int J Periodontics Restorative Dent. 2008 Apr;28(2):111–21.9Cochran DL, Obrecht M, Weber K, Dard M, Bosshardt D, Higginbottom FL, Wilson TG Jr, Jones AA. Biologic width adjacent to loaded implants with machined and rough collars in the dog.
→ Int J Periodontics Restorative Dent. 2014 Nov-Dec;34(6):773–9.10Jung YC, Han CH, Lee KW. A 1-year radiographic evaluation of marginal bone around dental implants.
→ Int J Oral Maxillofac Implants. 1996 Nov-Dec;11(6):811–8. The stress and strain concentrated at the periimplant crestal bone result in structural and morphological changes, especially during the first year after loading.11Jung YC, Han CH, Lee KW. A 1-year radiographic evaluation of marginal bone around dental implants.
→ Int J Oral Maxillofac Implants. 1996 Nov-Dec;11(6):811–8. Hence, the bone remodeling process is one of the critical factors in evaluating implant success.12Galindo-Moreno P, Leon-Cano A, Ortega-Oller I, Monje A, O’Valle F, Catena A. Marginal bone loss as success criterion in implant dentistry: beyond 2 mm.
→ Clin Oral Implants Res. 2015 Apr;26(4):e28–34. In addition, iatrogenic factors may contribute to periimplant MBL, such as implant positioning, implant–abutment microgap, lack of passive fit of the superstructure and occlusal overloading.13Alfonsi F, Borgia V, Barbato L, Tonelli P, Giammarinaro E, Marconcini S, Romeggio S, Barone A. The clinical effects of insertion torque for implants placed in healed ridges: a two-year randomized controlled clinical trial.
→ J Oral Science Rehabilitation. 2016 Dec;2(4):62–73.14Bahat O, Sullivan RM. Parameters for successful implant integration revisited part II: algorithm for immediate loading diagnostic factors.
→ Clin Implant Dent Relat Res. 2010 May;12 Suppl 1:e13–22.
15Quirynen M, Naert I, van Steenberghe D. Fixture design and overload influence marginal bone loss and fixture success in the Brånemark system.
→ Clin Oral Implants Res. 1992 Sep;3(3):104–11.16Harrel SK, Nunn ME. The effect of occlusal discrepancies on periodontitis. II. Relationship of occlusal treatment to the progression of periodontal disease.
→ J Periodontol. 2001 Apr;72(4):495–505.17Canullo L, Tallarico M, Radovanovic S, Delibasic B, Covani U, Rakic M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered periimplantitis.
→ Clin Oral Implants Res. 2016 Oct;27(10):1243–50.
Many pathological factors, including history of periodontitis, smoking, poor plaque control, genetic predisposition and diabetes, may produce an inflammatory reaction around an implant; nevertheless, no consensus exists with regard to a suitable definition of “periimplantitis” based on clinical and radiographic signs and symptoms or the best way to manage this emerging challenge.18Canullo L, Tallarico M, Radovanovic S, Delibasic B, Covani U, Rakic M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered periimplantitis.
→ Clin Oral Implants Res. 2016 Oct;27(10):1243–50.19Tallarico M, Monje A, Wang HL, Galindo Moreno P, Xhanari E, Canullo L. A systematic review on the definition of periimplantitis: limits related to the various diagnoses proposed.
→ J Oral Science Rehabilitation. 2016 Dec;2(4):42–53. The American Academy of Periodontology in 2013 defined “periimplantitis” as an inflammatory reaction associated with the loss of supporting bone beyond the initial biological bone remodeling around an implant in function.20American Academy of Periodontology. Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications.
→ J Periodontol. 2013 Apr;84(4):436–43.
The aims of the present study were to report the survival and success rates of dental implants placed in private practice and representing the daily realities of implant treatment, and then to determine the entity of the physiological marginal bone remodeling expected using Osstem implants. The data were analyzed to determine any statistical relationships between explanatory variables and early implant failure and physiological marginal bone remodeling (within one year after loading). This study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology statement for improving the quality of observational studies.21Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies.
→ J Clin Epidemiol. 2008 Apr;61(4):344–9.
Materials and methods
This investigation was designed as an open-cohort prospective study. All of the surgical and prosthetic procedures were performed in a private center in Rome, Italy, by an implant-based certified clinician (MT) between September 2014 and December 2016. All of the participants were enrolled and treated in consecutive order after being informed about the clinical procedures, materials to be used, benefits, and potential risks and complications, and once their written consent had been obtained. This study was conducted according to the principles embodied in the Helsinki Declaration of 1975, as revised in 2008.
Any completely or partially edentulous patients who received at least one bone level implant with a sandblasted and acid-etched surface and a Morse taper connection (Osstem TSIII, Osstem, Seoul, South Korea) were considered eligible for this study, independent of the implant and prosthetic protocols used. Exclusion criteria were general medical contraindications to oral surgery (American Society of Anesthesiologists Physical Status Class III or IV), patients treated or under treatment with intravenous aminobisphosphonates, and previous radiotherapy of the oral and maxillofacial region within the last five years. Patients who were diagnosed with active periodontal disease (≥ 6 mm probing depth) underwent periodontal surgery or initial therapy alone, prior to implant surgery.
Surgical and prosthetic protocols
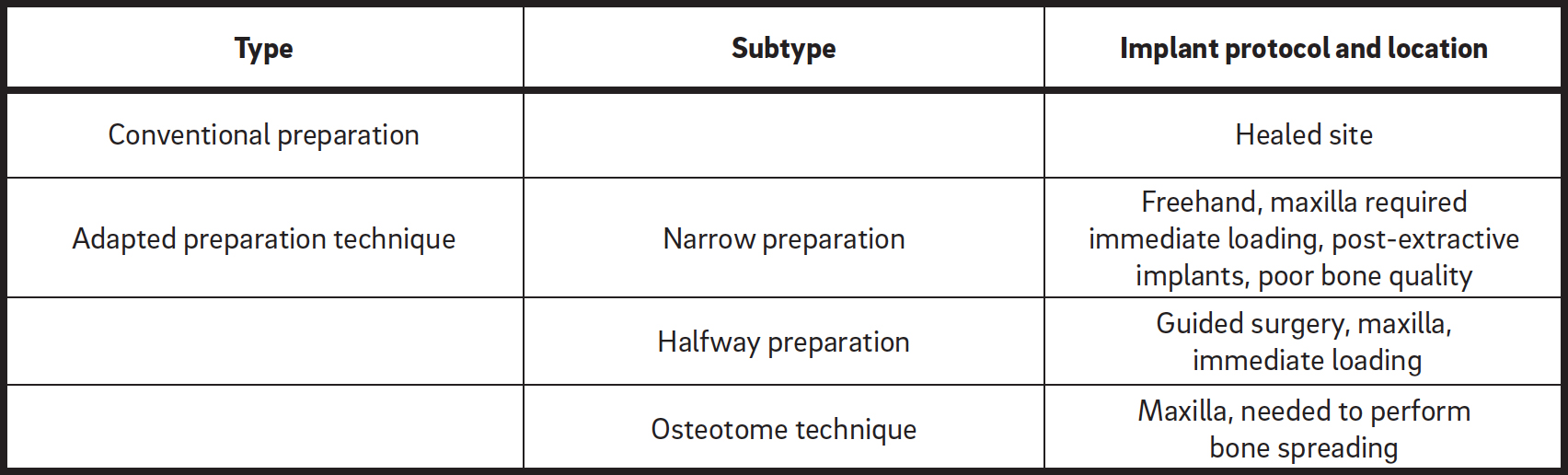
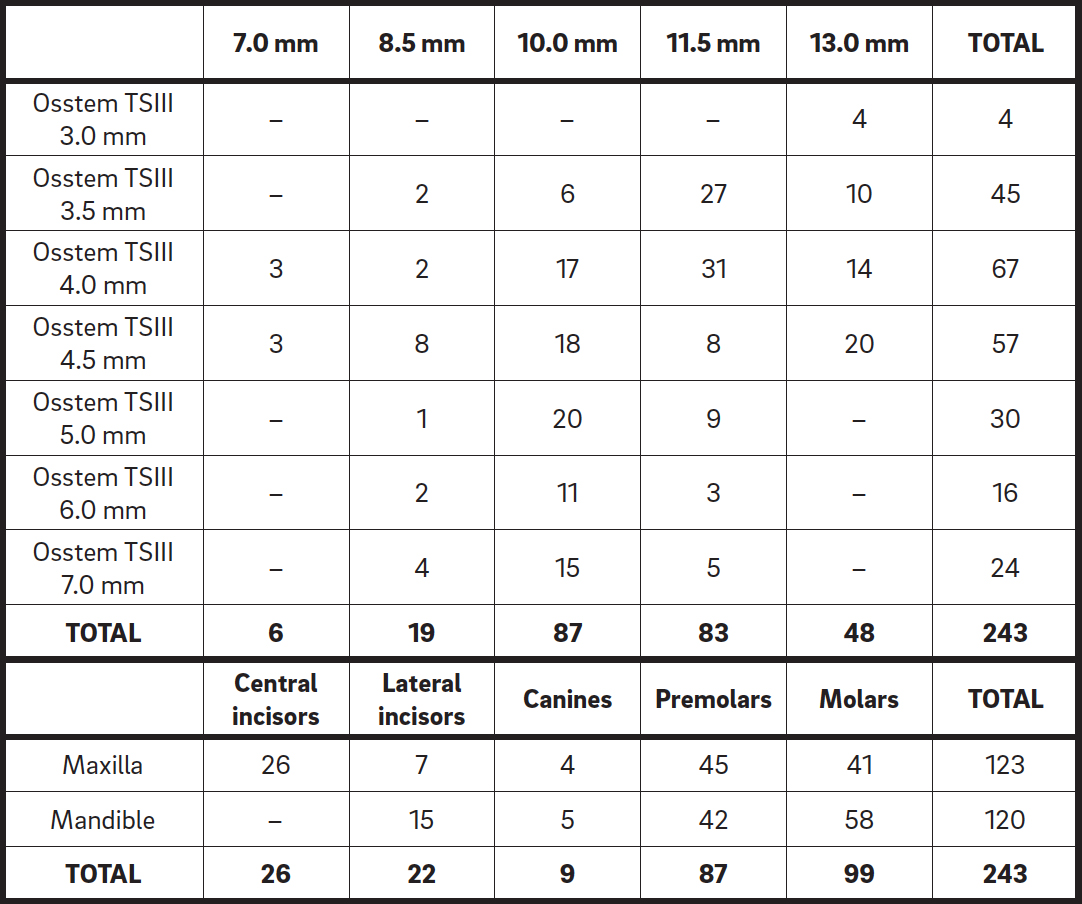
Preoperative photographs, periapical radiographs, panoramic radiographs or cone beam computed tomography (CBCT) scans, and model casts were produced for all of the patients, for initial screening and case evaluation. Before implant placement, all of the patients received a single dose of an antibiotic (2 g of amoxicillin or 600 mg of clindamycin if allergic to penicillin). Prior to the start of surgery, the patients rinsed with 0.2% chlorhexidine for 1 min. The patients received Osstem TSIII bone level implants with a rough surface (Ra of 2.5~3.0 μm) sandblasted with alumina and acid-etched and featuring an internal hex and 11° conical connection. Implant placement was performed using either computer- guided template-assisted implant placement or conventional freehand surgery. Most of the implants were placed according to the drilling protocol recommended by the manufacturer. In the case of immediate loading, post-extractive implants and poor bone quality, the drilling protocol was customized (Table 1).
Surgical protocols included placement in completely or partially edentulous healed ridges with or without bone grafting, as well as in fresh extraction sockets using a flapless or a flap approach. A flapless approach was planned in the case of post-extractive implants or in a healed site, depending on the width of the available keratinized mucosa. In cases of ridge atrophy, defined as a bone height of < 7.0 mm and/or bone width of < 4.5 mm, implant placement was performed simultaneously with guided bone regeneration (GBR). Otherwise, in cases of severe ridge atrophy, implant placement was performed six months after bone regeneration. Sinus lift procedures were performed using the conventional lateral window technique or by a less invasive transcrestal sinus floor elevation (Crestal Approach Sinus KIT, CAS-KIT, Osstem) in the case of a residual alveolar crest of at least 3 mm (maximum of 8 mm) in height and 6 mm in width distal to the canine, measured on a CBCT scan. In all reconstructive cases, the bone graft material was based on autogenous bone, combined with synthetic hydroxyapatite enriched with magnesium (SINTlife, Finceramica, Faenza, Italy) or with beta-tricalcium phosphate (Q-Oss+, Osstem). A resorbable cross-linked collagen membrane (OssGuide, Osstem) was used to protect the graft material during healing in the case of GBR or the lateral window approach.
In the case of immediate post-extractive implants, residual teeth were extracted as atraumatically as possible. Implant insertion was then planned along the palatal socket wall, about 1.5 mm below the buccal alveolar crest. The residual socket was grafted with corticocancellous heterologous bone, with a graft particle size of 250–1,000 μm (OsteoBiol Gen-Os, Tecnoss, Giaveno, Italy). In the case of delayed implants, socket preservation was performed with the same procedure and the implant was placed four months after healing.
Loading protocols varied based on implant stability and/or individual case requirements. Immediate loading (within 48 h of implant placement) was performed in the case of an implant stability of at least 35 N cm and at the patient’s request. Titanium temporary abutments or titanium or zirconia definitive abutments were screwed directly on to the implants or the intermediate abutments (straight or angulated multi-abutments, Osstem) with prosthetic screws tightened to 15 N cm on the day of surgery. Straight or angled multi-abutments (Osstem) were used in the case of multiunit restorations and screw-retained prostheses and/or when there was the need to change the depth or the angle of the implant. Prefabricated, screw-retained or cemented temporary acrylic restorations were trimmed and polished chairside. Partially edentulous patients received nonocclusal temporary restorations. Multiple implants received splinted, metal-reinforced temporary restorations with centric contact and group function, but without any cantilever. If needed, flaps were closed around the abutments. Otherwise, in the case of a bone augmentation procedure or post-extractive implants, a conventional or delayed loading protocol (three to six months after implant placement) was adopted.22Cochran DL, Morton D, Weber HP. Consensus statements and recommended clinical procedures regarding loading protocols for endosseous dental implants.
→ Int J Oral Maxillofac Implants. 2004;19 Suppl:109–13.
After implant placement, all of the patients received oral and written recommendations on medication, oral hygiene maintenance and diet. Postoperative antibiotic therapy (1 g of amoxicillin or 300 mg of clindamycin), administered every 12 h for six days, was limited to cases with immediate socket sites, bone grafting or sinus procedures. Analgesics (500 mg of paracetamol plus 30 mg of codeine, or 600 mg of ibuprofen) were administered as needed.
Final restorations were delivered between eight (single or partial crowns and overdentures) and twenty weeks (full arches). Final restorations were either screw-retained or cemented. Cemented restorations were delivered on either stock or customized CAD/CAM abutments. All of the restorations (metal and zirconia) were cemented using a glass ionomer cement (Ketac Cem, 3M ESPE, Neuss, Germany). Any cement remnant was immediately removed using an air–water syringe with the patient’s mouth closed. After 5 min of setting, the patient was clinically and radiographically inspected. Otherwise, CAD/CAM screw-retained restorations were delivered at implant or abutment level. The final abutments and screw-retained frameworks were screwed on at the torque setting recommended by the manufacturer.
The patients that received cemented restorations were inspected again after three to five days. All of the patients were then enrolled in a standard implant recall program. Oral hygiene maintenance was checked and radiographs were taken early after final prosthesis delivery. Occlusion was checked at every appointment. An explanatory case is illustrated in Figures 1 to 10.
-

- Fig. 1
-

- Fig. 2

-

- Fig. 3

-
- Fig. 4
-
- Fig. 5

-
- Fig. 10
-

- Fig. 6
-

- Fig. 7
-

- Fig. 8
-

- Fig. 9
Fig. 1
Preoperative panoramic radiograph.
Fig. 2
Preoperative intraoral photograph: lateral view.
Fig. 3
Preoperative intraoral photograph: occlusal view.
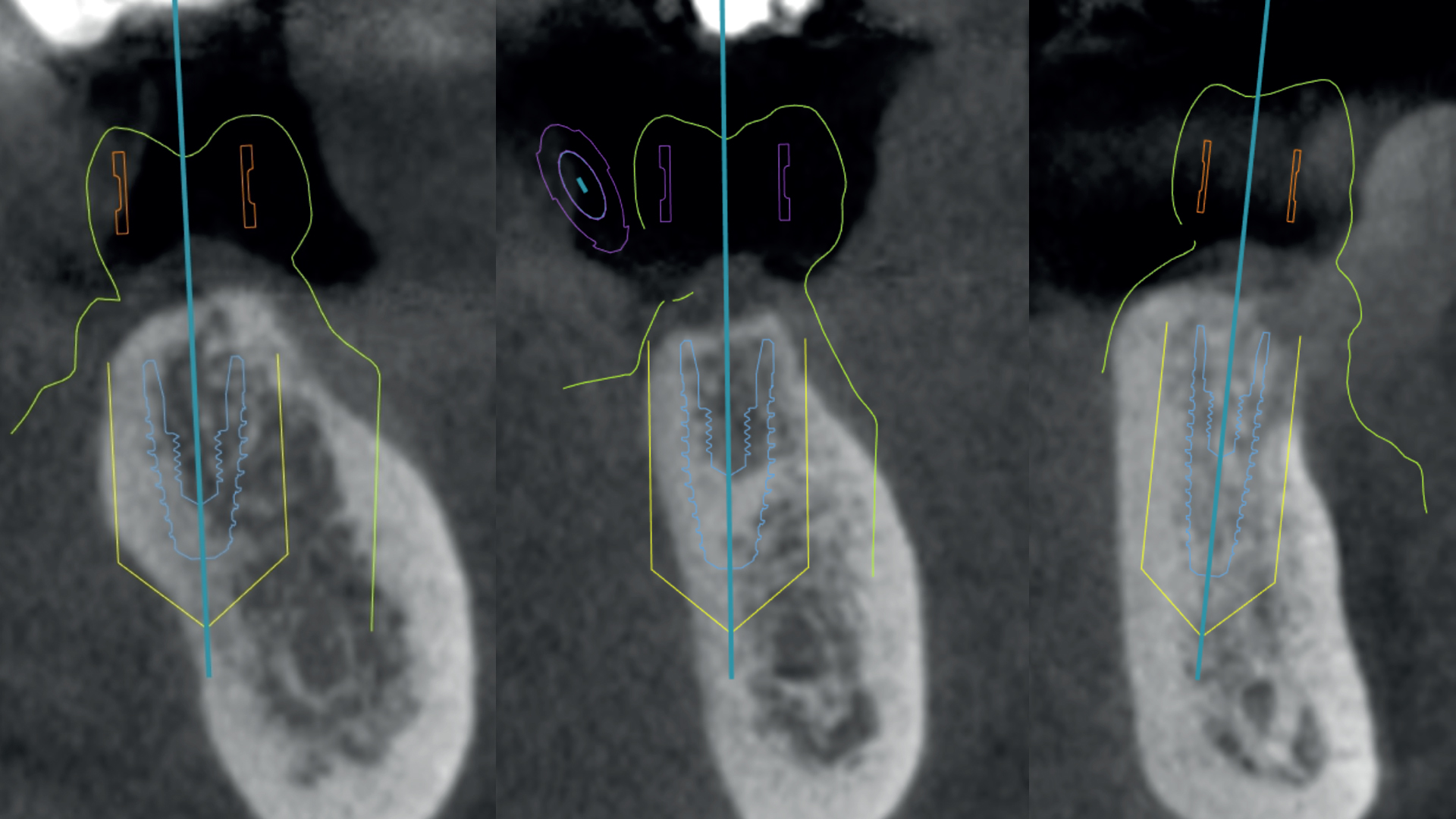
Fig. 4
Virtual planning. From left to right, teeth #47, 46 and 44.
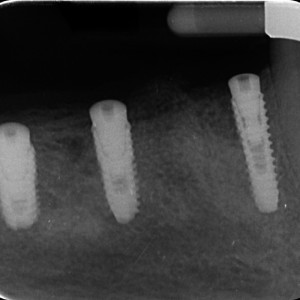
Fig. 5
Periapical radiograph taken after placement of the implants.
Fig. 6
Screw-retained temporary restoration placed eight weeks after implant placement.
Fig. 7
Try-in of the zirconia-based frameworks.
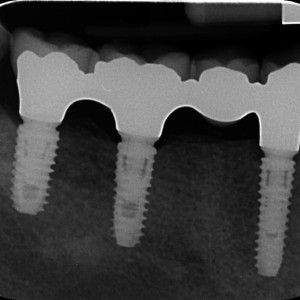
Fig. 8
Delivery of the final restoration.
Fig. 9
Intraoral photograph taken one year after delivery of the definitive restoration.
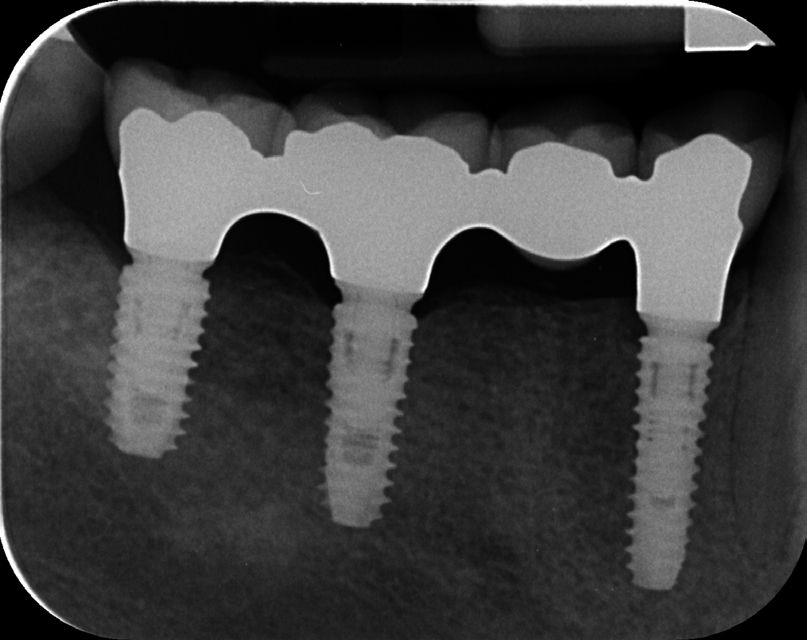
Fig. 10
Periapical radiograph taken one year after delivery of the definitive restoration.
Outcomes
Primary outcome measures were the success rates of the implants and prostheses, evaluated by an independent assessor. An implant was considered a failure if it presented any mobility, assessed by tapping or rocking the implant head with the metallic handles of two instruments, progressive MBL or infection, and any mechanical complications rendering the implant unusable, although still mechanically stable in the bone. A prosthesis was considered a failure if it needed to be replaced with another prosthesis.
Secondary outcomes were as follows:
- Complications: Any biological (pain, swelling, suppuration, etc.) and/or mechanical (screw loosening, fracture of the framework and/or the veneering material, etc.) complications were evaluated and treated by the same surgeon.
- Marginal bone levels: The levels were assessed using intraoral digital periapical radiographs (Digora Optime, SOREDEX, Tuusula, Finland; photostimulable phosphor imaging plate, size 2, pixel size of 30 μm, resolution of 17 lp/mm) at the subsequent follow-ups: implant placement (baseline), second-stage surgery, definitive crown delivery and one year after loading. Intraoral radiographs were taken with the paralleling technique by means of a periapical radiograph with a commercially available film holder (Rinn XCP, Dentsply Rinn, Elgin, Ill., U.S.). The radiographs were accepted or rejected for evaluation based on the clarity of the implant threads. All readable radiographs were uploaded to an image analysis software package (DfW 2.8, SOREDEX) that was calibrated using the known length or diameter of the dental implants and displayed on a 24 in. LCD screen (iMac, Apple, Calif., U.S.) and evaluated under standardized conditions (ISO 12646:2004). The marginal bone levels were determined from linear measurements performed by an independent calibrated examiner on each periapical radiograph, from the mesial and distal margin of the implant neck to the most coronal point where the bone appeared to be in contact with the implant.
- Insertion torque. This was recorded at implant placement by the same surgeon (MT) using the iChiropro surgical unit (Bien-Air, Bienne, Switzerland).
- Implant stability quotient (ISQ): The measurements were performed at implant placement and at the six-month follow-up by the surgeon (MT) using resonance frequency analysis (Osstell Mentor device, Osstell, Gothenburg, Sweden).
- Residual alveolar bone quality: This was assessed during surgery by the same surgeon (MT) and classified according to the Lekholm and Zarb classification.
- Thickness of the gingival biotype: This was assessed at the time of surgery using a periodontal probe (PCPUNC156, Hu-Friedy Italy, Milan, Italy) or a tension-free caliper. The gingival biotype was considered thin if the measurement was 1 mm and thick if > 1 mm.
Statistical analysis
Patients data were collected in an MS Excel spreadsheet. A statistician with expertise in dentistry analyzed the data and performed all of the statistical analysis using SPSS for Macintosh (Version 22.0; IBM, Chicago, Ill., U.S.). The distributions of continuous variables are given as mean ± standard deviation, median and 95% confidence interval (CI), whereas ordinal and dichotomous variables are presented as percentages. The implant or the restoration were the statistical units of analysis. Differences in the proportion of patients with prosthesis failures, implant failures and complications (dichotomous outcomes) were compared between the groups using the Fisher exact test. Differences in mean for continuous outcomes (bone level and ISQ) were compared at patient level by independent samples t-tests and one-way analysis of variance, respectively. Comparisons between each time point and the baseline measurements were made by paired tests, in order to detect any changes in marginal periimplant bone levels. All statistical comparisons were conducted at the 0.05 level of significance.
Results
A total of 243 sandblasted and acid-etched bone level implants featuring an 11° Morse taper connection were placed in 90 consecutive patients recruited and treated between September 2014 and December 2015 and followed for at least one year after loading. All of the initially selected patients were included and no patients dropped out of the study. The data of all of the patients were evaluated in the statistical analysis.
The patients were of both sexes (34 males and 56 females) and had an average age of 53.2 ± 15.4 years (range of 24–81 years). All of the patients were followed up for a minimum period of one year after loading (mean of 17.6 ± 2.5 months; range of 12–24 months). Most of the implants (n = 208) were placed in nonsmoking patients, while 20 implants were placed in patients who smoked ≤ 10 cigarettes per day and 15 implants in patients who smoked > 10 cigarettes per day. The main implant characteristics are shown in Table 2.
Forty-three implants were immediately placed in post-extraction sockets (Type 1),23Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classification and repair technique.
→ Pract Proced Aesthet Dent. 2007 Mar;19(2):99–104. 75 implants were placed 12–16 weeks after a socket preservation procedure (Type 3)24Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classification and repair technique.
→ Pract Proced Aesthet Dent. 2007 Mar;19(2):99–104. and 125 implants were placed late (more than four months after tooth extraction, Type 4).25Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classification and repair technique.
→ Pract Proced Aesthet Dent. 2007 Mar;19(2):99–104. Forty- nine implants were immediately loaded (20.2%) and 76 implants were placed using guided surgery (32.5%). Overall, 172 implants were conventionally placed without bone augmentation. Nineteen implants were placed in conjunction with horizontal GBR using a native collagen membrane and 1:1 ratio of particulated xenograft and autologous bone. Ten implants were placed in conjunction with a transcrestal sinus floor elevation. Three implants were placed with a combination of GBR and transcrestal sinus floor elevation. Thirty-nine immediate implants were placed in combination with socket preservation procedures.
The overall insertion torque ranged between 15.0 and 45.0 N cm (mean of 42.9 ± 4.8 N cm). Two hundred and three implants (83.5%) were placed at an insertion torque ranging from ≥ 35 to 45 N cm. The definitive restorations were delivered 8 to 20 weeks after second-stage surgery (Fig. 11). All of the impressions were taken at implant or abutment level with anatomically customized light-curing acrylic impression trays (Elite LC tray, Zhermack, Badia Polesine, Italy) fabricated on a preliminary cast derived from an irreversible hydrocolloid impression taken with a stock metal impression tray. The impressions were made with plaster (Snow White Plaster No. 2, Kerr, Orange, Calif., U.S.) in the case of edentulous patients or with a polyether material (Impregum Penta, 3M Italia, Milan, Italy) for single and partial restorations.
-

- Fig. 11
Fig. 11
Timing of implant placement and loading according to the surgical and prosthetic protocol adopted.
Overall, 104 single crowns were delivered in 67 patients, 20 fixed partial dentures (FPDs) supported by two to three implants were delivered in 16 patients and the remaining 16 patients received 19 full-arch restorations supported by two to six implants (Table 3). Definitive prostheses were screwed on to 168 implants (71 single crowns, 11 FPDs and 13 full-arch restorations) and cemented on to the remaining 61 implants (33 single crowns, nine FPDs and one full-arch restoration). Three patients (six implants) received overdentures on OT Equator attachments (Rhein 83, Bologna, Italy) and two patients (eight implants) received overdentures fully supported by a titanium CAD/CAM bar (New Ancorvis) and OT Equator attachment screwed on the top.

Five implants failed in five patients, resulting in a cumulative implant survival rate of 97.9% at the follow-up one year after loading. All of those implants failed before definitive loading. Two implants were placed in combination with bone augmentation procedures (p = 0.6310), one implant was immediately loaded (p = 1.000) and two were placed immediately after tooth extraction (p = 0.2108). Of these, two implants were placed using guided surgery (p = 0.6572). No statistically significant differences were found (p > 0.05). Two out of seven implants placed at an insertion torque of < 35 N cm failed (p = 0.0068). No definitive prosthesis failed, resulting in a cumulative prosthetic survival rate of 100%. Four patients experienced one technical complication each, resulting in a cumulative prosthetic success rate of 97.2% at the follow-up one year after loading. One zirconia-based, full-arch framework, delivered on six implants, presented a misfit between the framework and the most distal implant at the try-in appointment. The framework was remade with no further complications. One zirconia-based, full-arch, screw-retained restoration, delivered on six implants, fractured at the bisque bake try-in appointment. The restoration was remade with no further complications. Two patients with a single screw-retained restoration experienced screw loosening. The screws were replaced chairside with no further complications. One patient experienced pain and swelling up to 3 weeks after implant placement, resulting in a MBL greater than 2 mm. Nevertheless, no further pathological MBL was experienced. Most of the implants were placed at crest level or a little below. In the case of post-extractive implants, they were placed 1.0–1.5 mm below the buccal bone plate. At the definitive prosthesis delivery, the mean MBL was 0.26 ± 0.25 mm (95% CI: 0.27–0.30). The cumulative mean MBL between implant placement and the one year after loading follow-up was 0.37 ± 0.25 mm (95% CI: 0.26–0.30). The MBL in the interval between the definitive prosthesis delivery and the one year after loading follow-up was 0.11 ± 0.14 mm (95% CI: 0.08–0.10). Overall, 86.8% of the implants (n = 211) showed an MBL of ≤ 0.5 mm one year after loading, while only three implants showed an MBL of > 1.0 mm. Two patients were asymptomatic, while a third patient presented with pain without suppuration. This patient was treated with an antibiotic and analgesic until the resolution of the pathology. Eighty-two out of 243 patients (33.7%) reached the two-year follow-up. In this cohort of patients, MBL between the oneand the two-year follow-up was 0.05 ± 0.14 mm (range of 0.0–0.2 mm; 95% CI: -0.01–0.10).
Comparison of MBL and the investigated risk factors found statistically higher MBL for smokers, a thin gingival biotype and GBR. Immediate loading and placement of the definitive abutment on the day of surgery were found to be protective factors, with statistically significantly lower MBL.
Most of the implants (n = 203; 83.5%) reached an insertion torque of 45 N cm. The other 40 implants were placed at an insertion torque ranging from ≥ 35 to < 45 N cm (n = 33; 13.6%), > 25 to < 35 N cm (n = 4; 1.6%) and < 25 N cm (n = 3; 1.3%). No statistically significant correlation was found between insertion torque and MBL (p = 0.3726).
At implant placement, the mean ISQ value was 71.6 ± 5.5 (range of 45–88); At the sixmonth follow-up, mean ISQ was 76.7 ± 4.4 (range of 66–89). The difference was statistically significant (p = 0.0001).
One hundred and sixty-six implants were placed in bone of Type 1 and 2 quality (n = 18). The remaining 77 implants were placed in Type 3 and 4 bone. No statistically significant correlation was found between insertion torque and MBL (p = 0.4216).
A thin gingival biotype was associated with higher MBL compared with a thick biotype. The difference was statistically significant (p = 0.0307). All of the radiographic comparisons are reported in Table 4.
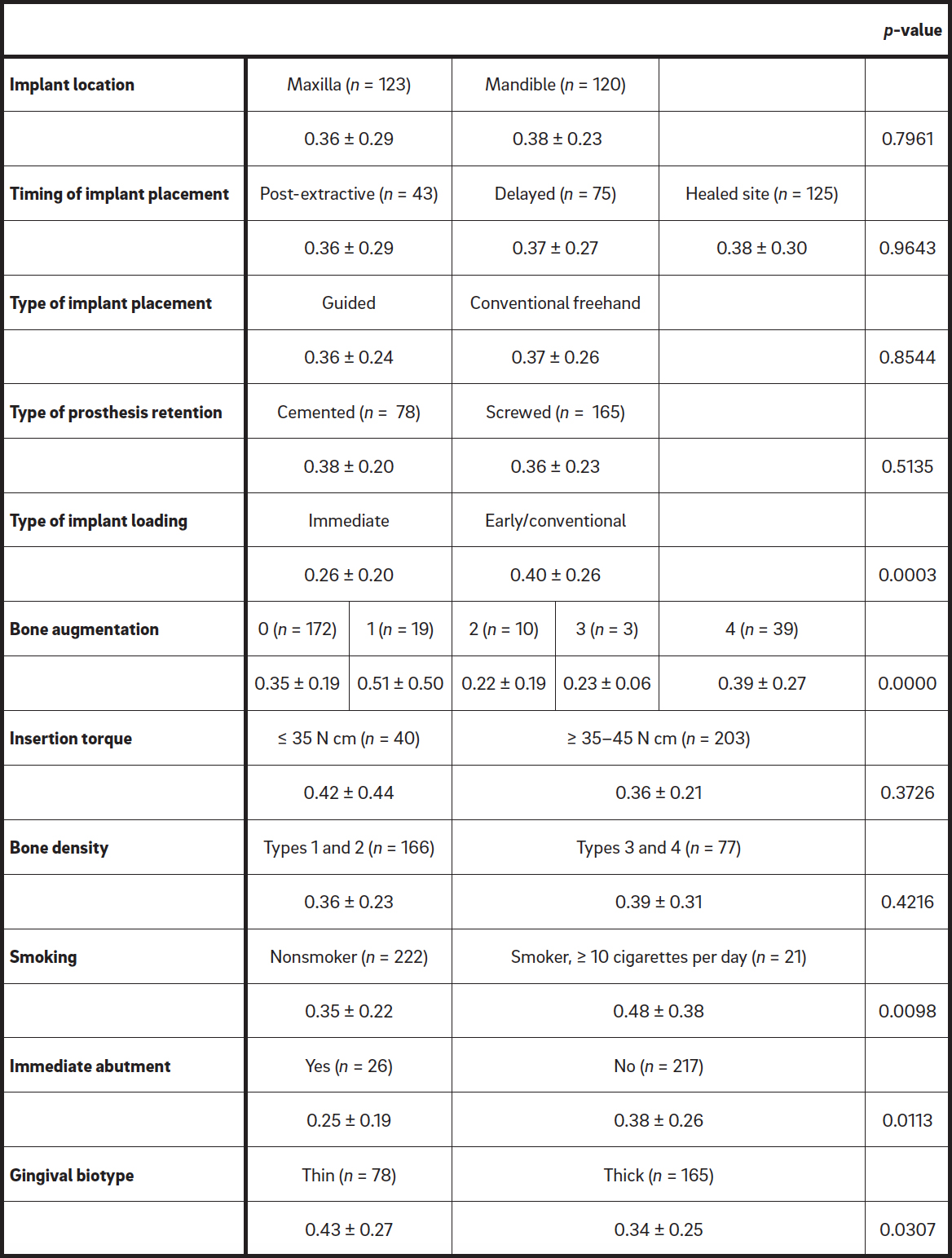
with different risk factors.
Discussion
The aim of this prospective open-cohort study was to investigate, over a 1 year after loading period, the implant survival and success rates of sandblasted and acid-etched bone level implants featuring an 11° Morse taper connection placed in private practice, and to evaluate the physiological marginal bone remodeling among subgroups of exposed and unexposed subjects. The main limitation of the present study was the short follow- up period. Nevertheless, one year after loading is sufficient to evaluate the physiological marginal bone remodeling that was the main topic of this research.
In the present study, five out of 243 implants failed over a period of one year after loading, resulting in a cumulative implant survival rate of 97.9%. No definitive prosthesis failed. One biological and four technical complications were experienced, resulting in a cumulative prosthetic and implant success rate of 97.2 and 99.6%, respectively.
The major clinical conclusion of the present research was that the physiological marginal bone remodeling using Osstem TSIII implants (Osstem) was 0.37 mm within one year after loading, independent of the surgical and prosthetic protocols. Subgroup analysis showed that smoking, a thin tissue biotype and GBR were associated with a statistically significantly higher MBL. This supports Sgolastra et al.’s conclusion that smoking seems to be positively associated with higher MBL, implant failure and risk of periimplantitis.26Sgolastra F, Petrucci A, Severino M, Gatto R, Monaco A. Smoking and the risk of peri-implantitis. A systematic review and meta-analysis.
→ Clin Oral Implants Res. 2015 Apr;26(4):e62–7.
The results of the present study are in agreement with a recent systematic review and meta-analysis that showed that implants placed with an initially thicker periimplant soft tissue have less radiographic MBL in the short-term follow-up. 27Suárez-López Del Amo F, Lin GH, Monje A, Galindo-Moreno P, Wang HL. Influence of soft tissue thickness on peri-implant marginal bone loss: a systematic review and meta-analysis.
→ J Periodontol. 2016 Jun;87(6):690–9. The results of this study also demonstrated that implants placed with GBR are as successful as implants placed into sites with pristine bone. In the present study, the mean MBL experienced around the implants placed in regenerated bone was slightly higher than that of the implants placed in nongrafted sites. No strong evidence is associated with higher MBL and GBR procedures. Nevertheless, data reported in the present study are consistent with, or slightly lower than, that reported in previous studies.28Meloni SM, Jovanovic SA, Urban I, Canullo L, Pisano M, Tallarico M. Horizontal ridge augmentation using GBR with a native collagen membrane and 1:1 ratio of particulated xenograft and autologous bone: a 1-year prospective clinical study.
→ Clin Implant Dent Relat Res. 2017 Feb;19(1):38–45. Immediate loading and the placement of a definitive abutment at implant insertion and never removed have been proven to reduce MBL.29Engelhardt S, Papacosta P, Rathe F, Özen J, Jansen JA, Junker R. Annual failure rates and marginal bone-level changes of immediate compared to conventional loading of dental implants. A systematic review of the literature and meta-analysis.
→ Clin Oral Implants Res. 2015 Jun;26(6):671–87.30Canullo L, Bignozzi I, Cocchetto R, Cristalli MP, Iannello G. Immediate positioning of a definitive abutment versus repeated abutment replacements in post-extractive implants: 3-year follow-up of a randomised multicentre clinical trial.
→ Eur J Oral Implantol. 2010 Winter;3(4):285–96. A possible explanation of this phenomenon could be that most of the immediately loaded implants were placed without a flap, using guided surgery, and received the definitive abutment on the day of surgery, minimizing MBL.
High primary implant stability is considered one of the main factors necessary for achieving a predictable high success rate.31Meloni SM, Tallarico M, Pisano M, Xhanari E, Canullo L. Immediate loading of fixed complete denture prosthesis supported by 4-8 implants placed using guided surgery: a 5-year prospective study on 66 patients with 356 implants.
→ Clin Implant Dent Relat Res. 2017 Feb;19(1):195–206.32Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery.
→ Clin Implant Dent Relat Res. 2016 Oct;18(5):965–72.33Meloni SM, De Riu G, Pisano M, Dell’aversana Orabona G, Piombino P, Salzano G, Quarato D, Riccardi E, Belli E, Ungari C. Computer-assisted implant surgery and immediate loading in edentulous ridges with dental fresh extraction sockets. Two years results of a prospective case series study.
→ Eur Rev Med Pharmacol Sci. 2013 Nov;17(21):2968–73.34Meloni SM, De Riu G, Pisano M, Cattina G, Tullio A. Implant treatment software planning and guided flapless surgery with immediate provisional prosthesis delivery in the fully edentulous maxilla. A retrospective analysis of 15 consecutively treated patients.
→ Eur J Oral Implantol. 2010 Autumn;3(3):245–51.35Pozzi A, Tallarico M, Moy PK. Immediate loading with a novel implant featured by variable-threaded geometry, internal conical connection and platform shifting: three-year results from a prospective cohort study.
→ Eur J Oral Implantol. 2015 Spring;8(1):51–63. Nevertheless, there is no consensus as to the ideal insertion torque required to prevent implant failure. In the present study, two out of seven implants placed at an insertion torque of < 35 N cm failed, reaching a statistically significant difference. In the study, 83.5% of the implants were placed at an insertion torque of 45 N cm. The drilling protocol was customized according to the bone density. Conventional preparation was performed in healed sites with a bone density of Type 2 or 3.20 Narrow or halfway adapted preparations were performed in the case of post-extractive implants and poor bone quality, using freehand or guided surgery, respectively. Finally, the osteotome technique was performed only in the maxilla, in order to perform bone spreading.
Conclusion
Low implant failure and physiological marginal bone remodeling of 0.37 mm within one year after loading can be expected using Osstem TSIII implants in the daily practice. Smoking, GBR and a thin tissue biotype were associated with higher MBL, while immediate loading and placement of the definitive abutment on the day of surgery reduced the MBL.
Competing interests
The first author (MT) is the Research Project Manager at Osstem AIC, Italy. However, this research was self-supported. Hence, the authors declare that they have no competing interests.
Acknowledgments
Dr. Marco Tallarico wishes to thank Ms. Gianina Bizduna and Stephany Zambrano for their important clinical assistance.
References
| 1. | ↑ | Roos J, Sennerby L, Lekholm U, Jemt T, Gröndahl K, Albrektsson T. A qualitative and quantitative method for evaluating implant success: a 5-year retrospective analysis of the Brånemark implant. → Int J Oral Maxillofac Implants. 1997 Jul-Aug;12(4):504–14. |
| 2, 3. | ↑ | Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. → Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. |
| 4. | ↑ | Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. → Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. |
| 5. | ↑ | Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz- Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. → Implant Dent. 2008 Mar;17(1):5–15. |
| 6, 7. | ↑ | Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: a systematic review. → J Dent Res. 2012 Mar;91(3):242–8. |
| 8. | ↑ | Nevins M, Nevins ML, Camelo M, Boyesen JL, Kim DM. Human histologic evidence of a connective tissue attachment to a dental implant. → Int J Periodontics Restorative Dent. 2008 Apr;28(2):111–21. |
| 9. | ↑ | Cochran DL, Obrecht M, Weber K, Dard M, Bosshardt D, Higginbottom FL, Wilson TG Jr, Jones AA. Biologic width adjacent to loaded implants with machined and rough collars in the dog. → Int J Periodontics Restorative Dent. 2014 Nov-Dec;34(6):773–9. |
| 10, 11. | ↑ | Jung YC, Han CH, Lee KW. A 1-year radiographic evaluation of marginal bone around dental implants. → Int J Oral Maxillofac Implants. 1996 Nov-Dec;11(6):811–8. |
| 12. | ↑ | Galindo-Moreno P, Leon-Cano A, Ortega-Oller I, Monje A, O’Valle F, Catena A. Marginal bone loss as success criterion in implant dentistry: beyond 2 mm. → Clin Oral Implants Res. 2015 Apr;26(4):e28–34. |
| 13. | ↑ | Alfonsi F, Borgia V, Barbato L, Tonelli P, Giammarinaro E, Marconcini S, Romeggio S, Barone A. The clinical effects of insertion torque for implants placed in healed ridges: a two-year randomized controlled clinical trial. → J Oral Science Rehabilitation. 2016 Dec;2(4):62–73. |
| 14. | ↑ | Bahat O, Sullivan RM. Parameters for successful implant integration revisited part II: algorithm for immediate loading diagnostic factors. → Clin Implant Dent Relat Res. 2010 May;12 Suppl 1:e13–22. |
| 15. | ↑ | Quirynen M, Naert I, van Steenberghe D. Fixture design and overload influence marginal bone loss and fixture success in the Brånemark system. → Clin Oral Implants Res. 1992 Sep;3(3):104–11. |
| 16. | ↑ | Harrel SK, Nunn ME. The effect of occlusal discrepancies on periodontitis. II. Relationship of occlusal treatment to the progression of periodontal disease. → J Periodontol. 2001 Apr;72(4):495–505. |
| 17, 18. | ↑ | Canullo L, Tallarico M, Radovanovic S, Delibasic B, Covani U, Rakic M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered periimplantitis. → Clin Oral Implants Res. 2016 Oct;27(10):1243–50. |
| 19. | ↑ | Tallarico M, Monje A, Wang HL, Galindo Moreno P, Xhanari E, Canullo L. A systematic review on the definition of periimplantitis: limits related to the various diagnoses proposed. → J Oral Science Rehabilitation. 2016 Dec;2(4):42–53. |
| 20. | ↑ | American Academy of Periodontology. Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications. → J Periodontol. 2013 Apr;84(4):436–43. |
| 21. | ↑ | Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. → J Clin Epidemiol. 2008 Apr;61(4):344–9. |
| 22. | ↑ | Cochran DL, Morton D, Weber HP. Consensus statements and recommended clinical procedures regarding loading protocols for endosseous dental implants. → Int J Oral Maxillofac Implants. 2004;19 Suppl:109–13. |
| 23, 24, 25. | ↑ | Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classification and repair technique. → Pract Proced Aesthet Dent. 2007 Mar;19(2):99–104. |
| 26. | ↑ | Sgolastra F, Petrucci A, Severino M, Gatto R, Monaco A. Smoking and the risk of peri-implantitis. A systematic review and meta-analysis. → Clin Oral Implants Res. 2015 Apr;26(4):e62–7. |
| 27. | ↑ | Suárez-López Del Amo F, Lin GH, Monje A, Galindo-Moreno P, Wang HL. Influence of soft tissue thickness on peri-implant marginal bone loss: a systematic review and meta-analysis. → J Periodontol. 2016 Jun;87(6):690–9. |
| 28. | ↑ | Meloni SM, Jovanovic SA, Urban I, Canullo L, Pisano M, Tallarico M. Horizontal ridge augmentation using GBR with a native collagen membrane and 1:1 ratio of particulated xenograft and autologous bone: a 1-year prospective clinical study. → Clin Implant Dent Relat Res. 2017 Feb;19(1):38–45. |
| 29. | ↑ | Engelhardt S, Papacosta P, Rathe F, Özen J, Jansen JA, Junker R. Annual failure rates and marginal bone-level changes of immediate compared to conventional loading of dental implants. A systematic review of the literature and meta-analysis. → Clin Oral Implants Res. 2015 Jun;26(6):671–87. |
| 30. | ↑ | Canullo L, Bignozzi I, Cocchetto R, Cristalli MP, Iannello G. Immediate positioning of a definitive abutment versus repeated abutment replacements in post-extractive implants: 3-year follow-up of a randomised multicentre clinical trial. → Eur J Oral Implantol. 2010 Winter;3(4):285–96. |
| 31. | ↑ | Meloni SM, Tallarico M, Pisano M, Xhanari E, Canullo L. Immediate loading of fixed complete denture prosthesis supported by 4-8 implants placed using guided surgery: a 5-year prospective study on 66 patients with 356 implants. → Clin Implant Dent Relat Res. 2017 Feb;19(1):195–206. |
| 32. | ↑ | Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery. → Clin Implant Dent Relat Res. 2016 Oct;18(5):965–72. |
| 33. | ↑ | Meloni SM, De Riu G, Pisano M, Dell’aversana Orabona G, Piombino P, Salzano G, Quarato D, Riccardi E, Belli E, Ungari C. Computer-assisted implant surgery and immediate loading in edentulous ridges with dental fresh extraction sockets. Two years results of a prospective case series study. → Eur Rev Med Pharmacol Sci. 2013 Nov;17(21):2968–73. |
| 34. | ↑ | Meloni SM, De Riu G, Pisano M, Cattina G, Tullio A. Implant treatment software planning and guided flapless surgery with immediate provisional prosthesis delivery in the fully edentulous maxilla. A retrospective analysis of 15 consecutively treated patients. → Eur J Oral Implantol. 2010 Autumn;3(3):245–51. |
| 35. | ↑ | Pozzi A, Tallarico M, Moy PK. Immediate loading with a novel implant featured by variable-threaded geometry, internal conical connection and platform shifting: three-year results from a prospective cohort study. → Eur J Oral Implantol. 2015 Spring;8(1):51–63. |





Leave a Reply
Be the First to Comment!