Review of the arterial vascular anatomy for implant placement in the anterior mandible
April 4, 2016 / Categories: Digital Dentistry, Implant Dentistry

Balaguer Marti, José Carlos
Guarinos, Juan
Serrano Sánchez, Pedro
Ruiz Torner, Amparo

Peñarrocha Oltra, David

Peñarrocha Diago, Miguel
The placement of implants in the anterior region of the mandible is not free of risk and can even sometimes be life-threatening. The aim of this article is to review the anatomy of the anterior mandible regarding the placement of implants in this region.
Introduction
Knowledge of the topographic anatomy of the mandibular region is very important in implant dentistry.
Severe, life-threatening complications can occur after dental implant placement in the mandible, especially in the anterior region. In the case of arterial vascular trauma in the floor of the mouth during implant placement in the mandibular anterior region, surgeons should be prepared to manage a severely compromised oropharyngeal airway.1Kalpidis CDR, Setayesh RM. Hemorrhaging associated with endosseous implant placement in the anterior mandible: a review of the literature. → J Periodontol. 2004 May;75(5):631–45.
The number of complications associated with implantology has risen owing to the increasing number of implants being placed. An electronic search performed in the MEDLINE (PubMed) and Embase databases with the search term “dental implants” indicated that the number of articles related to dental implants increases every year. Worthington wrote, “The number of practitioners performing implant surgery has increased dramatically over the last fifteen years. As confidence is gained, they tend to accept increasingly challenging cases and it is to be expected that the incidence of problems and complications will increase. Serious problems and complications may result from inadequate treatment planning, some from careless instrumentation, and some from lack of appropriate precautions.”2Worthington P. Medicolegal aspects of oral implant surgery. → Aust Prosthodont J. 1995;9 Suppl:13–7. Some important early complications after dental implantation may be neurological,3Bartling R, Freeman K, Kraut, RA. The incidence of altered sensation of the mental nerve after mandibular implant placement. → J Oral Maxillofac Surg. 1999 Dec;57(12):1408–10.’ 4Palma-Carrió C, Balaguer-Martínez J, Peñarrocha-Oltra D, Peñarrocha-Diago M. Irritative and sensory disturbances in oral implantology. Literature review. → Med Oral Patol Oral Cir Bucal. 2011 Nov;16(7):e1043–6. infections5Esposito M, Grusovin MG, Worthington HV. Interventions for replacing missing teeth: antibiotics at dental implant placement to prevent complications. → Cochrane Database Syst Rev. 2013 Jul;(7):1–37. doi:10.1002/14651858.CD004152.pub4. and hemorrhages,6Balaguer-Marti JC, Peñarrocha-Oltra D, Balaguer-Martinez J, Peñarrocha-Diago M. Immediate bleeding complications in dental implants: a systematic review. → Med Oral Patol Oral Cir Bucal. 2015 Mar;20(2):e231–8. Epub 2014 Dec 5.’ 7Kalpidis CDR, Setayesh RM. Hemorrhaging associated with endosseous implant placement in the anterior mandible: a review of the literature. → J Periodontol. 2004 May;75(5):631–45.’ 8Lamas Pelayo J, Peñarrocha Diago M, Martí Bowen E, Peñarrocha Diago M. Intraoperative complications during oral implantology. → Med Oral Patol Oral Cir Bucal. 2008 Apr;13(4):E239–43. Neurological complications are the most frequent (8.5%),9Palma-Carrió C, Balaguer-Martínez J, Peñarrocha-Oltra D, Peñarrocha-Diago M. Irritative and sensory disturbances in oral implantology. Literature review. → Med Oral Patol Oral Cir Bucal. 2011 Nov;16(7):e1043–6. followed by infections (1.8%),10Esposito M, Grusovin MG, Coulthard P, Oliver R, Worthington HV. The efficacy of antibiotic prophylaxis at placement of dental implants: a Cochrane systematic review of randomised controlled clinical trials. → Eur J Oral Implantol. 2008 Summer;1(2):95–103. and severe, life-threatening hemorrhagic complications are the most rare, with only 15 cases reported in the literature.11Balaguer-Marti JC, Peñarrocha-Oltra D, Balaguer-Martinez J, Peñarrocha-Diago M. Immediate bleeding complications in dental implants: a systematic review. → Med Oral Patol Oral Cir Bucal. 2015 Mar;20(2):e231–8. Epub 2014 Dec 5.
Although severe immediate hemorrhagic complications are infrequent, the mechanical pressure from sealed bleeding spaces adjacent to the upper airway may become life-threatening extremely quickly.12Kalpidis CDR, Setayesh RM. Hemorrhaging associated with endosseous implant placement in the anterior mandible: a review of the literature. → J Periodontol. 2004 May;75(5):631–45. Therefore, these are the most serious complications, especially when they occur in the anterior region of the mandible. Laceration of the inferior alveolar artery can lead to severe bleeding, but the compression by the implant itself can stop the hemorrhage. The floor of the mouth is not a closed cavity like the canal of the inferior alveolar nerve; therefore, if bleeding occurs, the blood collects in the supramylohyoid space, pressing the tongue to the palate. Thus, perforation of the lingual cortical plate in the anterior region of the mandible can cause uncontrollable bleeding of the sublingual artery, which requires in-hospital treatment.13Balaguer-Marti JC, Peñarrocha-Oltra D, Balaguer-Martinez J, Peñarrocha-Diago M. Immediate bleeding complications in dental implants: a systematic review. → Med Oral Patol Oral Cir Bucal. 2015 Mar;20(2):e231–8. Epub 2014 Dec 5. The practitioner must have an extensive knowledge of the anatomy of the surgical field to avoid this complication.
This paper highlights the essential anatomical details that must form part of the practitioner’s knowledge in order to perform dental implant surgery in the anterior mandible with maximum safety and minimal risk.
Materials & methods
A study of the anatomical body structures located in the anterior mandible and floor of mouth was performed. The cadavers used were donated by the University of Valencia (Valencia, Spain). An intravascular perfusion with colored latex was performed for better discrimination of the vessels. The tissue was dissected with the blunt technique principally—closed scissors were inserted into the connective tissue and then opened. The structures were recorded photographically.A literature review was conducted to assess the anatomy of the anterior mandible, through a search in electronic databases, namely MED-LINE (PubMed), Embase and the Cochrane Library. Boolean operators and truncation were used for the search. The search terms used were “(anatomy OR vessel* OR muscle OR artery) AND anterior AND mandible.” The inclusion criteria were case reports, anatomical studies on cadavers or radiographic studies of the anatomy of the floor of the mouth and the anterior mandible, performed in humans. The exclusion criterion was anticoagulated patients.
Results
Bony anatomy and musculature of the sublingual region
Among the soft tissues surrounding the mandible are the floor of the mouth (made of up the sublingual region and the tongue itself), and the mental and genial areas. The sublingual region is limited below by the mylohyoid muscle, laterally by the hyoglossus, genioglossus and geniohyoid muscles, above by the mucosa of the floor of the mouth, and anteriorly by the body of the mandible (Fig. 1).
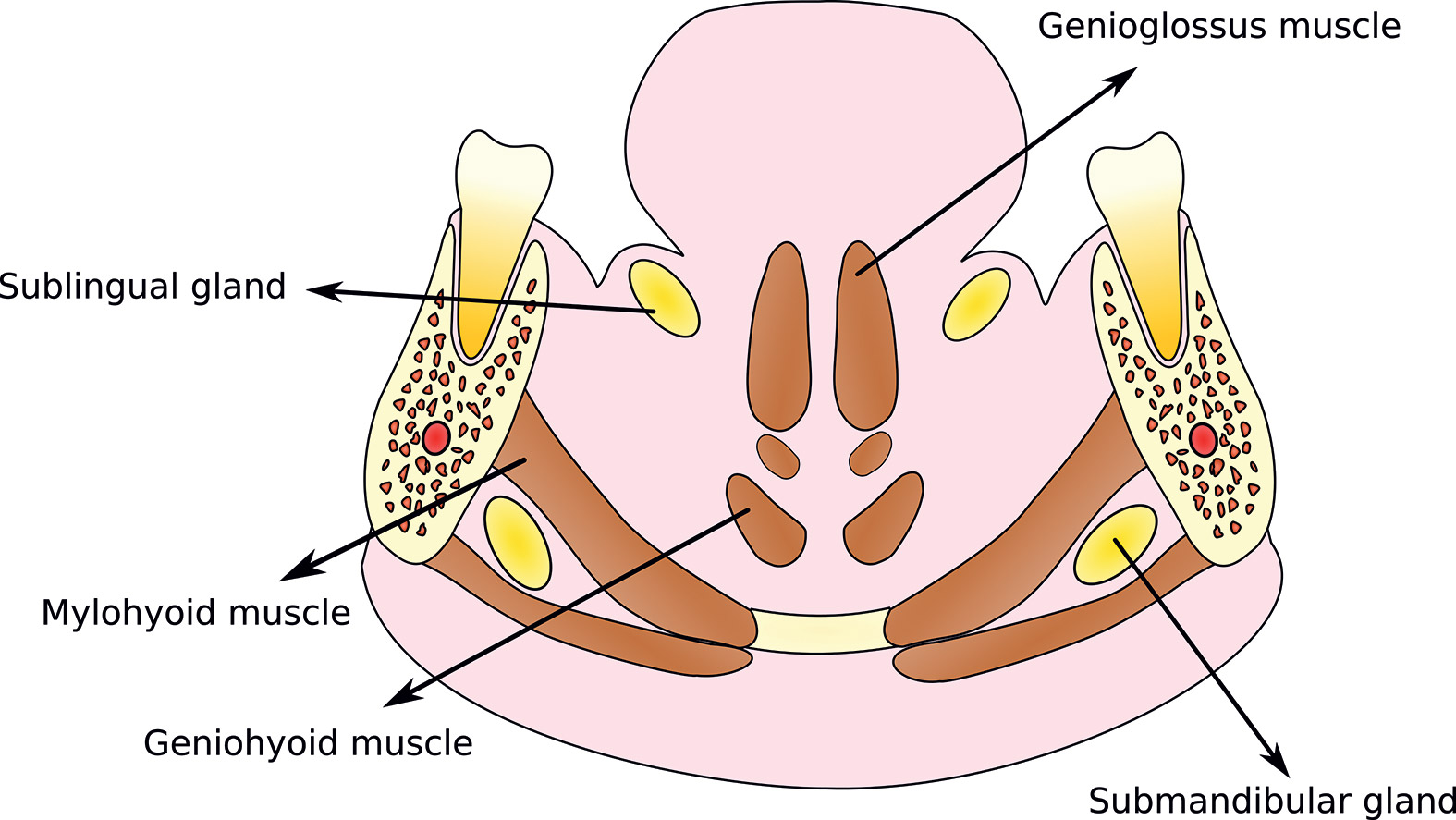
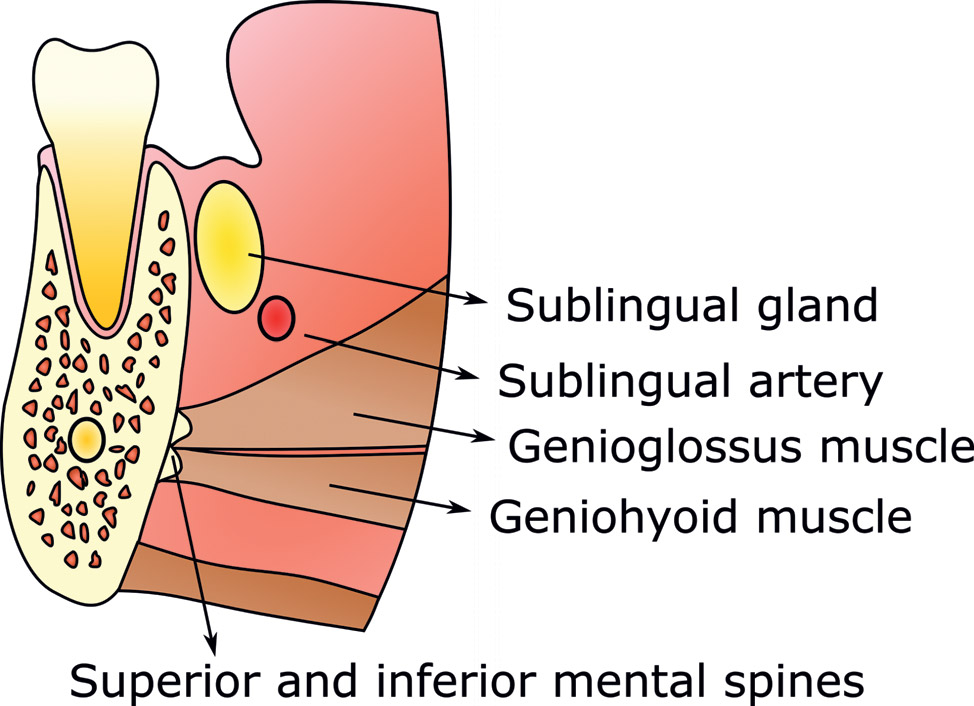 Fig. 2. Anatomical structures of the sublingual space. Sagittal plane.
Fig. 2. Anatomical structures of the sublingual space. Sagittal plane.The mandible in the symphyseal area is drop-shaped and tilted toward the lingual area. The mandibular symphysis is the medial area of the mandible that results from the endochondral ossification and the subsequent mergence of Meckel’s cartilage in the 24th week of intrauterine life.14Smartt JM, Low DW, Bartlett SP. The pediatric mandible: I. A primer on growth and development. → Plast Reconstr Surg. 2005 Jul;116(1):14e–23e. At that time, the musculature forms, affecting the development and subsequent growth of the mandible.15Wyganowska-Świątkowska M, Kawala B, Kozanecka A, Kurlej W. Observations on muscular attachments to human developing mandible. → Adv Clin Exp Med. 2012 Jul-Aug;21(4):447–54. In this region, the mental spines stand out where the quadratus labii inferioris muscle forms. The superior and inferior mental spines are located on the mandible’s inner side (Fig. 2). The genioglossus muscle originates from the superior mental spine, while the geniohyoid muscle originates from the inferior mental spine (Figs. 1 & 2). The digastric fossa, from which the anterior digastric muscle originates, is located on the mandible’s inner side, near the lower edge in the paramedian location (Fig. 3).
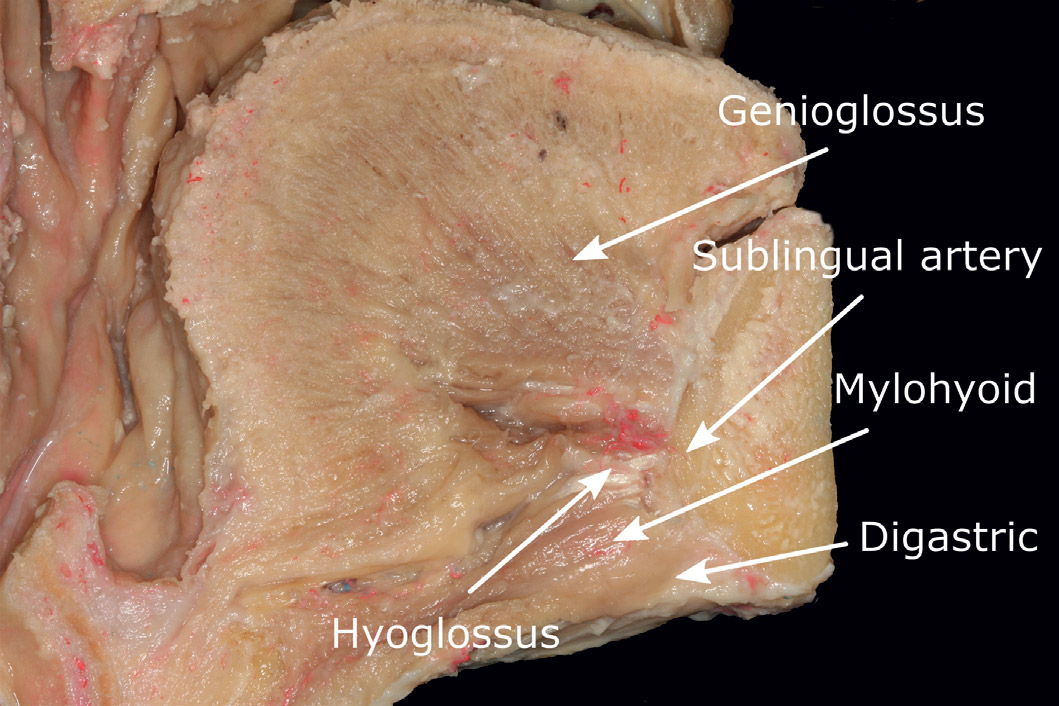
Sublingual artery
The sublingual artery follows a medial course to the mandible within the sublingual gland and supplies the mylohyoid muscle (Fig. 4). It is at the level of this muscle that the sublingual artery issues branches that anastomose with the submental artery.16Rouvière H, Delmas A. Anatomía humana: descriptiva, topografí ca y funcional. → 11a. ed. Barcelona: Masson; 2005. 784 p. The artery ends in the mental spine.
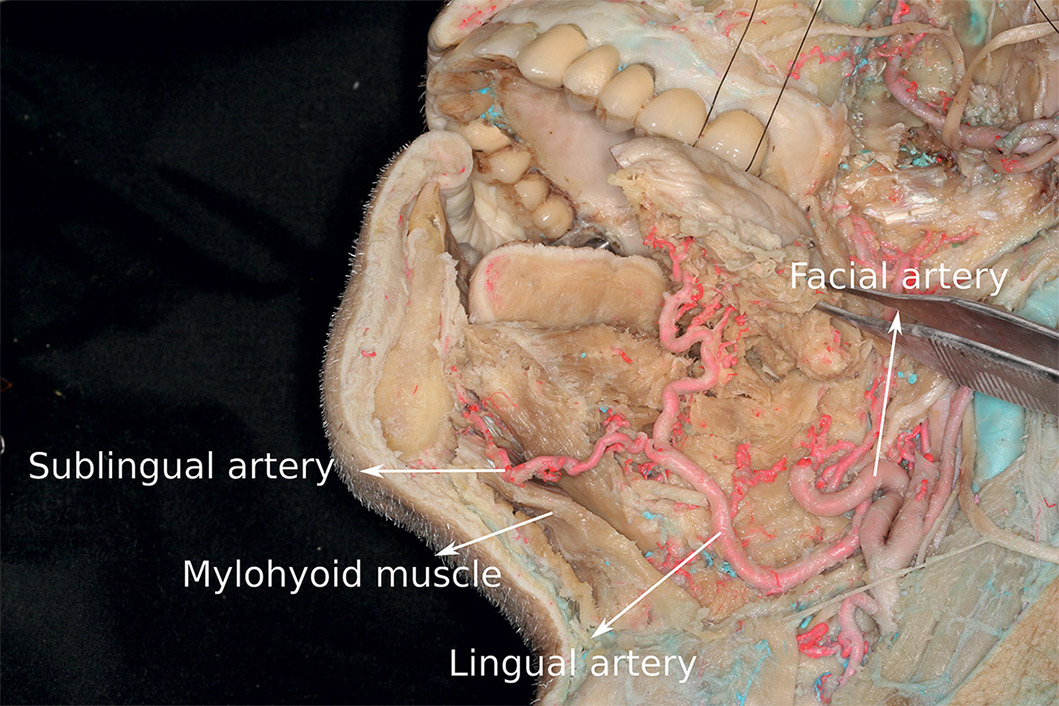
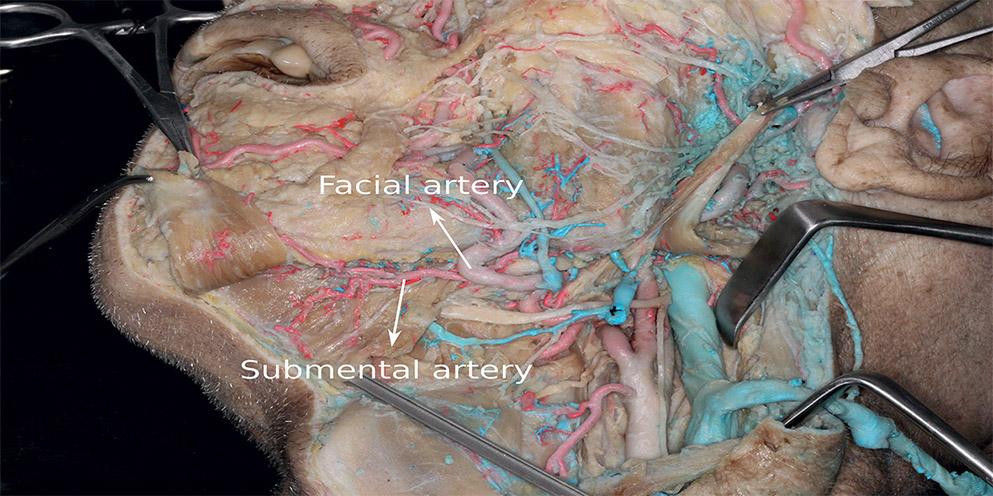
Submental artery
This artery is a branch of the facial artery. It passes together with the mylohyoid nerve along the inferior surface of the homonymous muscle to the anterior region, where it supplies the anterior digastric muscle (Fig. 5). At this anterior level, the perforating branches of the submental artery pierce the mylohyoid muscle to anasto- mose with perforating branches of the sublingual artery.17Troupis TG, Dimitroulis D, Paraschos A, Michalinos A, Protogerou V, Vlasis K, Troupis G, Skandalakis P. Lingual and facial arteries arising from the external carotid artery in a common trunk. → Am Surg. 2011 Feb;77(2):151–4.
Vascular anastomosis
Fig. 4 Anatomical photograph of the arterial supply of the floor of the mouth.
Fig. 5 Course of the facial and submental arteries.
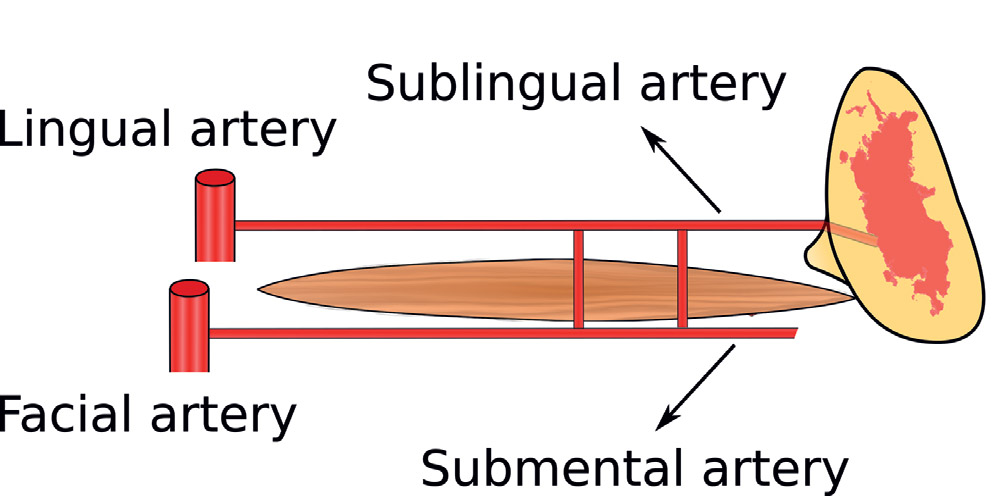
Fig. 6 Location of the sublingual and submental arteries. (Modified from Kalpidis and Setayesh1 with permission from the American Academy of Periodontology.)
There are many anastomoses of the arteries involved in the sublingual region. An anastomosis found between the lingual and the submental arteries runs along the bottom flange of the mandibular body and through the mylohyoid muscle (Fig. 6). Anastomoses between both sublingual contralateral arteries in the symphysis are frequent too (Fig. 7).
In summary, the mandibular symphyseal area is supplied by multiple vascular structures from different origins and presents a variability dependent on the anastomosing relationships established by the terminal branches of these structures.18Kawai T, Sato I, Yosue T, Takamori H, Sunohara M. Anastomosis between the inferior alveolar artery branches and submental artery in human mandible. → Surg Radiol Anat. 2006 Jun;28(3):308–10.19Kim DH, Won SY, Choi DY, Kim HS, Jung UW, Kim HJ, Hu KS. Topography of the submental artery that should be considered in bleeding during dentoalveolar surgery. → J Craniofac Surg. 2012 Sep;23(5):1453–56.20Liang X, Jacobs R, Lambrichts I, Vandewalle G. Lingual foramina on the mandibular midline revisited: a macroanatomical study. → Clin Anat. 2007 Apr;20(3):246–51.
Discussion
The sublingual region is well vascularized, with several anastomoses that can impair hemostasis if bleeding occurs.21Lamas Pelayo J, Peñarrocha Diago M, Martí Bowen E, Peñarrocha Diago M. Intraoperative complications during oral implantology. → Med Oral Patol Oral Cir Bucal. 2008 Apr;13(4):E239–43. Treatment can be uncomfortable for the patient, so the priority is to prevent trauma occurring through good anatomical knowledge of the area and proper planning of the surgery.
Regarding the bony anatomy and musculature of the anterior mandible, the mental spines are located in the mandible’s inner side. Some studies highlight its morphological variability, for example the variability in the distance from the mental spine to the inferior border of the mandible or to apices of the mandibular incisors.22Wang YC, Liao YF, Li HY, Chen YR. Genial tubercle position and dimensions by cone-beam computerized tomography in a Taiwanese sample. → Oral Surg Oral Med Oral Pathol Oral Radiol. 2012 Jun;113(6):e46–50. The genioglossus and geniohyoid muscles originate from the mental spines, so this variability may increase the risk of damage to these structures when dental implants are placed in this area.
The digastric fossa is located on the mandible’s inner side, near the lower edge in the paramedian location. Therefore, an injury caused by piercing of the mandibular cortical bone, for example when placing a dental implant, may affect different muscles depending on whether the implant preparation is in the medial or paramedian location in relation to the mandibular symphysis.23La’porte SJ, Juttla JK, Lingam RK. Imaging the floor of the mouth and the sublingual space. → Radiographics. 2011 Sep-Oct;31(5):1215–30.
Three arteries supply this anatomical region: (a) the sublingual artery, which is a branch of the lingual artery; (b) the submental artery, which is a branch of the facial artery; and (c) the chin artery, which is the terminal branch of the inferior alveolar artery. The lingual and facial arteries are oth branches of the external carotid artery and the inferior alveolar artery is a branch of the maxillary artery.24Rouvière H, Delmas A. Anatomía humana: descriptiva, topografí ca y funcional. → 11a. ed. Barcelona: Masson; 2005. 784 p.
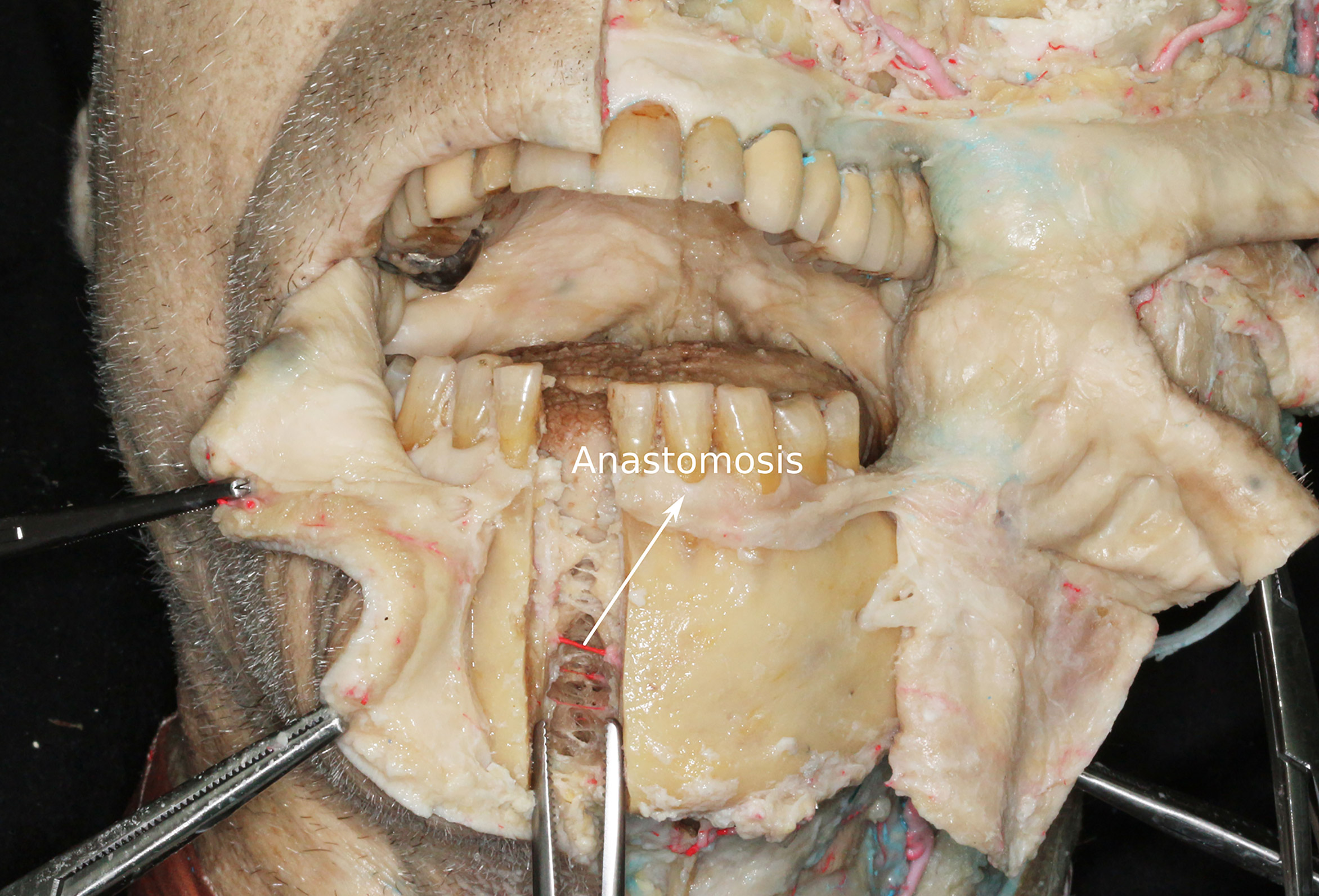 Fig. 7 Anastomosis of the sublingual arteries.
Fig. 7 Anastomosis of the sublingual arteries.
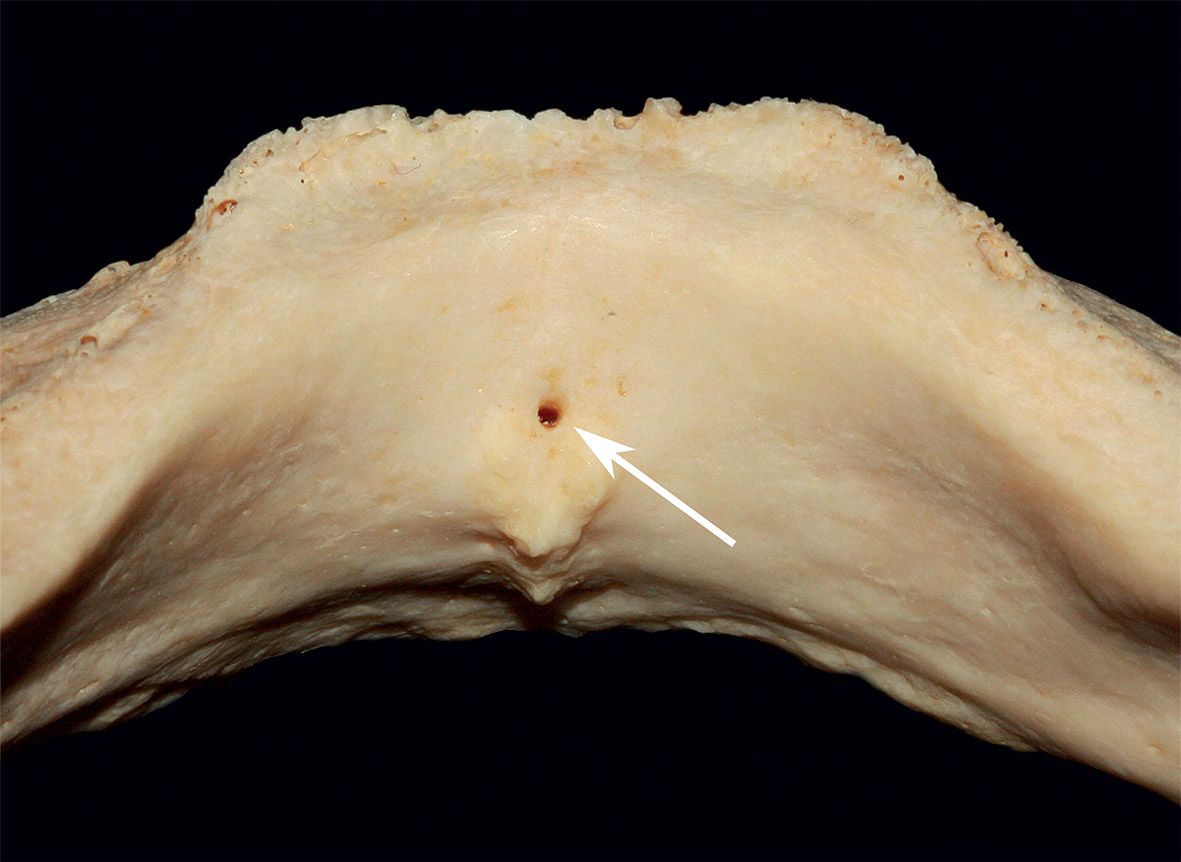 Fig. 8. Mandibular medial lingual canal
Fig. 8. Mandibular medial lingual canalKatsumi et al. classify the arterial supply to the floor of the mouth into four types.25Katsumi Y, Tanaka R, Hayashi T, Koga T, Takagi R, Ohshima H. Variation in arterial supply to the floor of the mouth and assessment of relative hemorrhage risk in implant surgery. → Clin Oral Implants Res. 2013 Apr;24(4):434–40. In Type I, the sublingual region is supplied by the sublingual artery. In Type II, it is supplied by the sublingual and submental arteries. In Types III and IV, it is supplied by the submental artery (the difference between the last two being that in Type III the deep lingual artery—which supplies the tongue—originates from the lingual
artery, and in Type IV it comes from the submental artery).
The sublingual artery is the main supply of the sublingual region. Anatomical and radiographic studies have identified lingual vascular canals in the mandible where the sublingual artery pierces the mandibular lingual cortical plate (Figs. 6 & 8).26Kilic E, Doganay S, Ulu M, Çelebi N, Yikilmaz A, Alkan A. Determination of lingual vascular canals in the interforaminal region before implant surgery to prevent life-threatening bleeding complications. → Clin Oral Implants Res. 2014 Feb;25(2):e90–3.27Tagaya A, Matsuda Y, Nakajima K, Seki K, Okano T. Assessment of the blood supply to the lingual surface of the mandible for reduction of bleeding during implant surgery. → Clin Oral Implants Res. 2009 Apr;20(4):351–5.28Katakami K, Mishima A, Kuribayashi A, Shimoda S, Hamada Y, Kobayashi K. Anatomical characteristics of the mandibular lingual foramina observed on limited cone-beam CT images. → Clin Oral Implants Res. 2009 Apr;20(4):386–90. The frequency of lateral lingual canals in the area of the mandibular incisors varied between 33.1% and 100.0% and in the area of the canines between 69.0% and 80.0% of the cases.29Kilic E, Doganay S, Ulu M, Çelebi N, Yikilmaz A, Alkan A. Determination of lingual vascular canals in the interforaminal region before implant surgery to prevent life-threatening bleeding complications. → Clin Oral Implants Res. 2014 Feb;25(2):e90–3.30Tagaya A, Matsuda Y, Nakajima K, Seki K, Okano T. Assessment of the blood supply to the lingual surface of the mandible for reduction of bleeding during implant surgery. → Clin Oral Implants Res. 2009 Apr;20(4):351–5.31Katakami K, Mishima A, Kuribayashi A, Shimoda S, Hamada Y, Kobayashi K. Anatomical characteristics of the mandibular lingual foramina observed on limited cone-beam CT images. → Clin Oral Implants Res. 2009 Apr;20(4):386–90. The location of the lingual canals coincided with the most frequent sites of clinically important bleeding during implant placement. The diameter of the canals was on average 1.2 mm, which is enough to produce severe sublingual bleeding.32Loukas M, Kinsella CR, Kapos T, Tubbs RS, Ramachandra S. Anatomical variation in arterial supply of the mandible with special regard to implant placement. → Int J Oral Maxillofac Surg. 2008 Apr;37(4):367–71. Katakami et al. observed anastomoses between the lateral lingual canals and the inferior alveolar canal in 20.1% of the cases.33Balaguer-Marti JC, Peñarrocha-Oltra D, Balaguer-Martinez J, Peñarrocha-Diago M. Immediate bleeding complications in dental implants: a systematic review. → Med Oral Patol Oral Cir Bucal. 2015 Mar;20(2):e231–8. Epub 2014 Dec 5.’ 34Katakami K, Mishima A, Kuribayashi A, Shimoda S, Hamada Y, Kobayashi K. Anatomical characteristics of the mandibular lingual foramina observed on limited cone-beam CT images. → Clin Oral Implants Res. 2009 Apr;20(4):386–90.
The inferior alveolar artery provides an intraosseous blood supply to the symphyseal area and the mandibular incisors by an incisal branch that runs through the incisal canal. This canal has an average length of 19.78 mm from the mental foramen toward the midline.35Kawai T, Sato I, Yosue T, Takamori H, Sunohara M. Anastomosis between the inferior alveolar artery branches and submental artery in human mandible. → Surg Radiol Anat. 2006 Jun;28(3):308–10. The mental artery branches from the inferior alveolar artery inside the mandibular canal and exits the mandible through the mental foramen. It supplies the chin and anastomoses with its counterpart on the opposite side and the submental and inferior labial arteries.36Troupis TG, Dimitroulis D, Paraschos A, Michalinos A, Protogerou V, Vlasis K, Troupis G, Skandalakis P. Lingual and facial arteries arising from the external carotid artery in a common trunk. → Am Surg. 2011 Feb;77(2):151–4.
There are several anastomoses between the major arteries supplying the floor of the mouth and the sublingual region. This fact is important because bleeding is more difficult to control whenever anastomoses are present. The following anastomoses have been documented in the literature: between the facial and the lingual arteries,37Kalpidis CDR, Setayesh RM. Hemorrhaging associated with endosseous implant placement in the anterior mandible: a review of the literature. → J Periodontol. 2004 May;75(5):631–45.’ 38Katsumi Y, Tanaka R, Hayashi T, Koga T, Takagi R, Ohshima H. Variation in arterial supply to the floor of the mouth and assessment of relative hemorrhage risk in implant surgery. → Clin Oral Implants Res. 2013 Apr;24(4):434–40. between the inferior alveolar artery and the submental artery, and between the inferior alveolar artery and the sublingual artery through the lingual cortical plate,39Liang X, Jacobs R, Lambrichts I, Vandewalle G. Lingual foramina on the mandibular midline revisited: a macroanatomical study. → Clin Anat. 2007 Apr;20(3):246–51. and in close relationship with the lingual cortical plate in 54% of the cases.40Kim DH, Won SY, Choi DY, Kim HS, Jung UW, Kim HJ, Hu KS. Topography of the submental artery that should be considered in bleeding during dentoalveolar surgery. → J Craniofac Surg. 2012 Sep;23(5):1453–56.’ 41Loukas M, Kinsella CR, Kapos T, Tubbs RS, Ramachandra S. Anatomical variation in arterial supply of the mandible with special regard to implant placement. → Int J Oral Maxillofac Surg. 2008 Apr;37(4):367–71.
Recommendations for placement of implants in mandibular areas
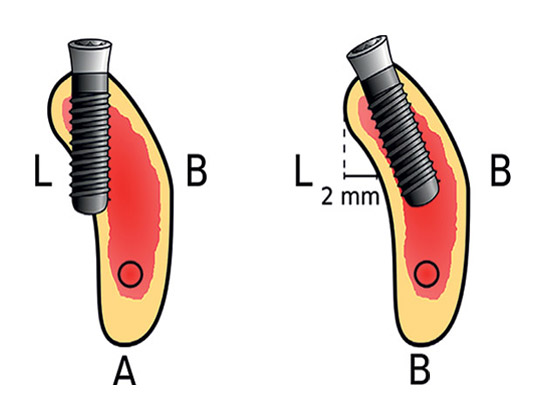
Figs. 10 a & b Implant tilted (b) to avoid perforation of the lingual cortical plate (a) in the posterior region of the mandible when a deep submandibular fossa is present. L: lingual aspect; B: buccal aspect.
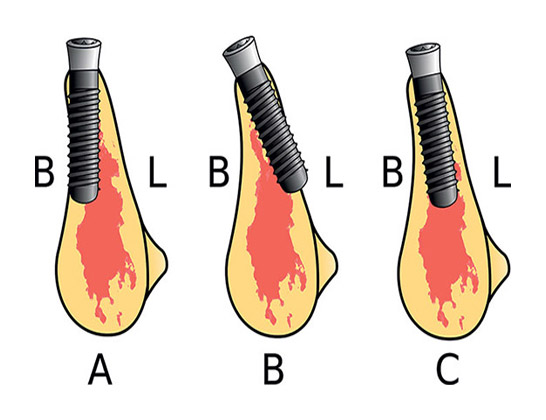
The sites with the highest risk of clinically important bleeding are the symphysis and the canine region—these coincide with the locations of the lingual canals, a fact that might help explain this bleeding.42Balaguer-Marti JC, Peñarrocha-Oltra D, Balaguer-Martinez J, Peñarrocha-Diago M. Immediate bleeding complications in dental implants: a systematic review. → Med Oral Patol Oral Cir Bucal. 2015 Mar;20(2):e231–8. Epub 2014 Dec 5.’ 43Kalpidis CDR, Setayesh RM. Hemorrhaging associated with endosseous implant placement in the anterior mandible: a review of the literature. → J Periodontol. 2004 May;75(5):631–45. Moreover, the concavity in the symphysis may lead to perforation of the vestibular cortical plate if the implant is placed axially in the symphysis, whereas if an implant is placed tilted in the buccolingual direction, with the implant apex toward the lingual cortical plate, it can perforate the lingual cortical plate (Figs. 9a–c). For this reason, implants should be placed slightly tilted toward the vestibular cortical plate, as shown in Figure 9c. The shape of the mandible in the posterior region is as shown in Figure 10, with a depression in the lingual cortical plate under the mylohyoid line. The depth of this submandibular fossa is greater than 2 mm (Figs. 10a & b) in 71.5–80.0% of patients.44Parnia F, Fard EM, Mahboub F, Hafezeqoran A, Gavgani FE. Tomographic volume evaluation of submandibular fossa in patients requiring dental implants. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Jan;109(1):e32–6.’ 45Yildiz S, Bayar GR, Guvenc I, Kocabiyik N, Cömert A, Yazar F. Tomographic evaluation on bone morphology in posterior mandibular region for safe placement of dental implant. → Surg Radiol Anat. 2014 Mar;37(2):167–73.
The presence of this fossa increases the risk of perforating the lingual cortical plate and of injuring the terminal branches of the sublingual artery during implant placement. However, in the posterior mandible, this risk is lower because the sublingual artery passes further from the lingual cortical plate.46Mardinger O, Manor Y, Mijiritsky E, Hirshberg A. Lingual perimandibular vessels associated with life-threatening bleeding: an anatomic study. → Int J Oral Maxillofac Surg. 2007 Jan-Feb;22(1):127–31. To our knowledge, only two cases of perforation of the lingual cortical plate in the posterior mandible have been reported in the literature.47Bidra AS. Management of pain and sublingual hematoma caused by suture irritation after implant surgery: a clinical report. → J Prosthet Dent. 2015 May;113(5):360–5.
Tilting of implants in the posterior mandible is again a possible solution in order to avoid the submandibular fossa and maximize the use of the bone available in patients with bone atrophy in this region. Because the inferior alveolar nerve is closer to the mandibular lingual cortical bone48Gowgiel JM. The position and course of the mandibular canal. → J Oral Implantol. 1992;18(4):383–5. and the alveolar crest height over the submandibular fossa may be limited, a novel approach has been proposed using implants tilted in a buccolingual direction, tipping the implant apex toward the vestibule (Fig. 10).49Peñarrocha Diago M, Maestre Ferrín L, Peñarrocha Oltra D, Canullo L, Calvo Guirado JL, Peñarrocha Diago M. Tilted implants for the restoration of posterior mandibles with horizontal atrophy: an alternative treatment. → J Oral Maxillofac Surg. 2013 May;71(5):856–64.
Conventionally, longer implants have been used in the anterior mandible than in other regions of the mandible or in the maxilla, owing to the lack of important anatomical structures such as the maxillary sinus or the inferior alveolar canal. Several authors have reported the appearance of sublingual hematomas after placement of dental implants of ≥ 15 mm in length in the anterior region of the mandible.50Balaguer-Marti JC, Peñarrocha-Oltra D, Balaguer-Martinez J, Peñarrocha-Diago M. Immediate bleeding complications in dental implants: a systematic review. → Med Oral Patol Oral Cir Bucal. 2015 Mar;20(2):e231–8. Epub 2014 Dec 5.’ 51Kalpidis CDR, Setayesh RM. Hemorrhaging associated with endosseous implant placement in the anterior mandible: a review of the literature. → J Periodontol. 2004 May;75(5):631–45. This is the median distance from the sublingual artery to the top of the alveolar ridge.52Mardinger O, Manor Y, Mijiritsky E, Hirshberg A. Lingual perimandibular vessels associated with life-threatening bleeding: an anatomic study. → Int J Oral Maxillofac Surg. 2007 Jan-Feb;22(1):127–31. The use of shorter dental implants may be advisable in the anterior region to reduce the risk of severe bleeding complications.
The use of 3-D imaging techniques and planning software may be useful to reduce the risk of bleeding complications. Correa et al. found that narrower and shorter implants tended to be selected when the available bone was studied using CBCT cross-sectional images, compared with both digital panoramic radiographs and CBCT-generated panoramic views.53Correa LR, Spin-Neto R, Stavropoulos A, Schropp L, da Silveira HED, Wenzel A. Planning of dental implant size with digital panoramic radiographs, CBCT-generated panoramic images, and CBCT cross- sectional images. → Clin Oral Implants Res. 2014 Jun;25(6):690–5. Moreover, guided implant surgery may potentially enhance safety even further by avoiding vessels, nerves and other anatomical structures if the case is planned properly. However, at present, this cannot be definitively stated yet. In a recent review on guided surgery, Tahmaseb et al. found a mean deviation of up to 7.1 mm.54Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:25–42. It is necessary to control the factors that significantly affect the accuracy of guided surgery, such as the experience of the operator,55Cushen SE, Turkyilmaz I. Impact of operator experience on the accuracy of implant placement with stereolithographic surgical templates: an in vitro study. → J Prosthet Dent. 2013 Apr;109(4):248–54. the software used,56Behneke A, Burwinkel M, Knierim K, Behneke N. Accuracy assessment of cone beam computed tomography-derived laboratory-based surgical templates on partially edentulous patients. → Clin Oral Implants Res. 2012 Feb;23(2):137–43.’ 57Vasak C, Strbac GD, Huber CD, Lettner S, Gahleitner A, Zechner W. Evaluation of three different validation procedures regarding the accuracy of template-guided implant placement: an in vitro study. → Clin Implant Dent Relat Res. 2015 Feb;17(1):142–9. Epub 2013 May 16. the type of support for the guided template (soft tissue, bone or dental support), the type of surgery (flap vs. flapless) and the guided surgery system used.58Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:25–42.
The anterior region of the mandible has a high bone density, Type I according to the Lekholm and Zarb classification.59Lekholm U, Zarb G. Patient selection and preparation. → In: Brånemark P-I, Zarb GA, Albrektsson T, editors. Tissue-integrated prostheses: Osseointegration in clinical dentistry. Chicago: Quintessence Publishing; 1985. p. 199–209. This property helps to achieve adequate primary stability, which, together with the absence of anatomical limitations, such as the inferior alveolar nerve and reduced atrophy, has conventionally led students to place their first implants in this area. The risks of placement of dental implants in the anterior region of the mandible highlight that the conventional recommendation to students to place their first implants in the anterior region of the mandible, owing to the absence of important anatomical structures, should be reviewed.
Conclusion
The sublingual region is densely supplied by several arteries that often anastomose. Injuring these vessels can cause serious bleeding and even threaten the patient’s life through the blocking of the upper airway. In order to avoid these complications, the operator should have an extensive anatomical knowledge of this area. Moreover, tilting of implants, the avoidance of long dental implants, and careful surgical planning with the aid of 3-D imaging and planning software may also help to reduce the risks when placing implants in the anterior mandible.
Competing interests
The authors declare that they have no competing interests related to this study.
References
| 1, 7, 12, 37, 43, 51. | ↑ | Kalpidis CDR, Setayesh RM. Hemorrhaging associated with endosseous implant placement in the anterior mandible: a review of the literature. → J Periodontol. 2004 May;75(5):631–45. |
| 2. | ↑ | Worthington P. Medicolegal aspects of oral implant surgery. → Aust Prosthodont J. 1995;9 Suppl:13–7. |
| 3. | ↑ | Bartling R, Freeman K, Kraut, RA. The incidence of altered sensation of the mental nerve after mandibular implant placement. → J Oral Maxillofac Surg. 1999 Dec;57(12):1408–10. |
| 4, 9. | ↑ | Palma-Carrió C, Balaguer-Martínez J, Peñarrocha-Oltra D, Peñarrocha-Diago M. Irritative and sensory disturbances in oral implantology. Literature review. → Med Oral Patol Oral Cir Bucal. 2011 Nov;16(7):e1043–6. |
| 5. | ↑ | Esposito M, Grusovin MG, Worthington HV. Interventions for replacing missing teeth: antibiotics at dental implant placement to prevent complications. → Cochrane Database Syst Rev. 2013 Jul;(7):1–37. doi:10.1002/14651858.CD004152.pub4. |
| 6, 11, 13, 33, 42, 50. | ↑ | Balaguer-Marti JC, Peñarrocha-Oltra D, Balaguer-Martinez J, Peñarrocha-Diago M. Immediate bleeding complications in dental implants: a systematic review. → Med Oral Patol Oral Cir Bucal. 2015 Mar;20(2):e231–8. Epub 2014 Dec 5. |
| 8, 21. | ↑ | Lamas Pelayo J, Peñarrocha Diago M, Martí Bowen E, Peñarrocha Diago M. Intraoperative complications during oral implantology. → Med Oral Patol Oral Cir Bucal. 2008 Apr;13(4):E239–43. |
| 10. | ↑ | Esposito M, Grusovin MG, Coulthard P, Oliver R, Worthington HV. The efficacy of antibiotic prophylaxis at placement of dental implants: a Cochrane systematic review of randomised controlled clinical trials. → Eur J Oral Implantol. 2008 Summer;1(2):95–103. |
| 14. | ↑ | Smartt JM, Low DW, Bartlett SP. The pediatric mandible: I. A primer on growth and development. → Plast Reconstr Surg. 2005 Jul;116(1):14e–23e. |
| 15. | ↑ | Wyganowska-Świątkowska M, Kawala B, Kozanecka A, Kurlej W. Observations on muscular attachments to human developing mandible. → Adv Clin Exp Med. 2012 Jul-Aug;21(4):447–54. |
| 16, 24. | ↑ | Rouvière H, Delmas A. Anatomía humana: descriptiva, topografí ca y funcional. → 11a. ed. Barcelona: Masson; 2005. 784 p. |
| 17, 36. | ↑ | Troupis TG, Dimitroulis D, Paraschos A, Michalinos A, Protogerou V, Vlasis K, Troupis G, Skandalakis P. Lingual and facial arteries arising from the external carotid artery in a common trunk. → Am Surg. 2011 Feb;77(2):151–4. |
| 18, 35. | ↑ | Kawai T, Sato I, Yosue T, Takamori H, Sunohara M. Anastomosis between the inferior alveolar artery branches and submental artery in human mandible. → Surg Radiol Anat. 2006 Jun;28(3):308–10. |
| 19, 40. | ↑ | Kim DH, Won SY, Choi DY, Kim HS, Jung UW, Kim HJ, Hu KS. Topography of the submental artery that should be considered in bleeding during dentoalveolar surgery. → J Craniofac Surg. 2012 Sep;23(5):1453–56. |
| 20, 39. | ↑ | Liang X, Jacobs R, Lambrichts I, Vandewalle G. Lingual foramina on the mandibular midline revisited: a macroanatomical study. → Clin Anat. 2007 Apr;20(3):246–51. |
| 22. | ↑ | Wang YC, Liao YF, Li HY, Chen YR. Genial tubercle position and dimensions by cone-beam computerized tomography in a Taiwanese sample. → Oral Surg Oral Med Oral Pathol Oral Radiol. 2012 Jun;113(6):e46–50. |
| 23. | ↑ | La’porte SJ, Juttla JK, Lingam RK. Imaging the floor of the mouth and the sublingual space. → Radiographics. 2011 Sep-Oct;31(5):1215–30. |
| 25, 38. | ↑ | Katsumi Y, Tanaka R, Hayashi T, Koga T, Takagi R, Ohshima H. Variation in arterial supply to the floor of the mouth and assessment of relative hemorrhage risk in implant surgery. → Clin Oral Implants Res. 2013 Apr;24(4):434–40. |
| 26, 29. | ↑ | Kilic E, Doganay S, Ulu M, Çelebi N, Yikilmaz A, Alkan A. Determination of lingual vascular canals in the interforaminal region before implant surgery to prevent life-threatening bleeding complications. → Clin Oral Implants Res. 2014 Feb;25(2):e90–3. |
| 27, 30. | ↑ | Tagaya A, Matsuda Y, Nakajima K, Seki K, Okano T. Assessment of the blood supply to the lingual surface of the mandible for reduction of bleeding during implant surgery. → Clin Oral Implants Res. 2009 Apr;20(4):351–5. |
| 28, 31, 34. | ↑ | Katakami K, Mishima A, Kuribayashi A, Shimoda S, Hamada Y, Kobayashi K. Anatomical characteristics of the mandibular lingual foramina observed on limited cone-beam CT images. → Clin Oral Implants Res. 2009 Apr;20(4):386–90. |
| 32, 41. | ↑ | Loukas M, Kinsella CR, Kapos T, Tubbs RS, Ramachandra S. Anatomical variation in arterial supply of the mandible with special regard to implant placement. → Int J Oral Maxillofac Surg. 2008 Apr;37(4):367–71. |
| 44. | ↑ | Parnia F, Fard EM, Mahboub F, Hafezeqoran A, Gavgani FE. Tomographic volume evaluation of submandibular fossa in patients requiring dental implants. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Jan;109(1):e32–6. |
| 45. | ↑ | Yildiz S, Bayar GR, Guvenc I, Kocabiyik N, Cömert A, Yazar F. Tomographic evaluation on bone morphology in posterior mandibular region for safe placement of dental implant. → Surg Radiol Anat. 2014 Mar;37(2):167–73. |
| 46, 52. | ↑ | Mardinger O, Manor Y, Mijiritsky E, Hirshberg A. Lingual perimandibular vessels associated with life-threatening bleeding: an anatomic study. → Int J Oral Maxillofac Surg. 2007 Jan-Feb;22(1):127–31. |
| 47. | ↑ | Bidra AS. Management of pain and sublingual hematoma caused by suture irritation after implant surgery: a clinical report. → J Prosthet Dent. 2015 May;113(5):360–5. |
| 48. | ↑ | Gowgiel JM. The position and course of the mandibular canal. → J Oral Implantol. 1992;18(4):383–5. |
| 49. | ↑ | Peñarrocha Diago M, Maestre Ferrín L, Peñarrocha Oltra D, Canullo L, Calvo Guirado JL, Peñarrocha Diago M. Tilted implants for the restoration of posterior mandibles with horizontal atrophy: an alternative treatment. → J Oral Maxillofac Surg. 2013 May;71(5):856–64. |
| 53. | ↑ | Correa LR, Spin-Neto R, Stavropoulos A, Schropp L, da Silveira HED, Wenzel A. Planning of dental implant size with digital panoramic radiographs, CBCT-generated panoramic images, and CBCT cross- sectional images. → Clin Oral Implants Res. 2014 Jun;25(6):690–5. |
| 54, 58. | ↑ | Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:25–42. |
| 55. | ↑ | Cushen SE, Turkyilmaz I. Impact of operator experience on the accuracy of implant placement with stereolithographic surgical templates: an in vitro study. → J Prosthet Dent. 2013 Apr;109(4):248–54. |
| 56. | ↑ | Behneke A, Burwinkel M, Knierim K, Behneke N. Accuracy assessment of cone beam computed tomography-derived laboratory-based surgical templates on partially edentulous patients. → Clin Oral Implants Res. 2012 Feb;23(2):137–43. |
| 57. | ↑ | Vasak C, Strbac GD, Huber CD, Lettner S, Gahleitner A, Zechner W. Evaluation of three different validation procedures regarding the accuracy of template-guided implant placement: an in vitro study. → Clin Implant Dent Relat Res. 2015 Feb;17(1):142–9. Epub 2013 May 16. |
| 59. | ↑ | Lekholm U, Zarb G. Patient selection and preparation. → In: Brånemark P-I, Zarb GA, Albrektsson T, editors. Tissue-integrated prostheses: Osseointegration in clinical dentistry. Chicago: Quintessence Publishing; 1985. p. 199–209. |





Leave a Reply
Be the First to Comment!