Spontaneous bone regeneration after removal of cysts: One-year follow-up of 336 consecutive cases
June 27, 2016 / Categories: Digital Dentistry, Implant Dentistry

Di Dio, Marco

Scarapecchia, Dario

Porcelli, Daniela

Arcuri, Claudio
The objective of this study was to assess spontaneous bone healing after enucleation of large jaw cysts without using any grafting material.
Introduction
The gold standard for the treatment of most jaw cysts is enucleation of the lesions. The cavity remaining after enucleation may heal spontaneously by the physiological appositional mechanism of bone growth. However, in larger bony defects, the use of bone grafting materials is still controversial.1Getter L, Bhaskar SN, Cutright DE, Perez B, Brady JM, Driskell TD, O’Hara MJ. Three biodegradable calcium phosphate slurry implants in bone. → J Oral Surg. 1972 Apr;30(4):263–8.2Salama R. Xenogeneic bone grafting in humans. → Clin Orthop Relat Res. 1983 Apr;(174):113–21.3Horowitz I, Bodner L. Use of xenograft bone with aspirated bone marrow for treatment of cystic defect of the jaws. → Head Neck. 1989 Nov-Dec;11(6):516–23.4Mitchell R. An evaluation of bone healing in cavities in the jaws implanted with a collagen matrix. → Br J Oral Maxillofac Surg. 1992 Jun;30(3):180–2.5Moskow BS, Gold SI, Gottsegen R. Effects of scleral collagen upon the healing of experimental osseous wounds. → J Periodontol. 1976 Oct;47(10):596–606.6Del Balso AM, Adrian JC. Collagen gel in osseous defects: a preliminary report. → Oral Surg Oral Med Oral Pathol. 1976 Nov;42(5):562–9.7Bodner L. Effect of decalcified freeze-dried bone allograft on the healing of jaw defects after cyst enucleation. → J Oral Maxillofac Surg. 1996 Nov;54(11):1282–6.8Bodner L. Osseous regeneration in the jaws using demineralized allogenic bone implants. → J Craniomaxillofac Surg. 1998 Apr;26(2):116–20.9Schepers EJ, Ducheyne P, Barbier L, Schepers S. Bioactive glass particles of narrow size range: a new material for the repair of bone defects. → Implant Dent. 1993 Fall;2(3):151–6.10Marx RE, Kline SN, Johnson RP, Malinin TI, Matthews JG 2nd, Gambill V. The use of freeze-dried allogeneic bone in oral and maxillofacial surgery. → J Oral Surg. 1981 Apr;39(4):264–74.11Spengos MN. Irradiated allogeneic bone grafts in the treatment of odontogenic cysts. → J Oral Surg. 1974 Sep;32(9):674–8.12Constantinides J, Zachariades N. Homogenous bone grafts to the mandible. → J Oral Surg. 1978 Aug;36(8):599–603.13Marble HB Jr. Homografts of freeze-dried bone in cystic defects of the jaws: a survey of ninety-one cases. → Oral Surg Oral Med Oral Pathol. 1968 Jul;26(1):118–23.
Many studies have concluded that bone grafts should be used to reduce the risk of jaw weakness.14Chiapasco M, Rossi A, Motta JJ, Crescentini M. Spontaneous bone regeneration after enucleation of large mandibular cysts: a radiographic computed analysis of 27 consecutive cases. → J Oral Maxillofac Surg. 2000 Sep;58(9):942–8.15Damante JH, Da S Guerra EN, Ferreira O Jr. Spontaneous resolution of simple bone cysts. → Dentomaxillofac Radiol. 2002 May;31(3):182–6.16Caicoya SO. Bone cavity filling with alloplastic material in maxillofacial surgery. → Rev Esp Cir Oral y Maxillofac. 2007 Jan-Feb;29(1):21–32.17Wiltfang J, Kloss FR, Kessler P, Nkenke E, Schultze-Mosgau S, Zimmermann R, Schlegel KA. Effects of platelet-rich plasma on bone healing in combination with autogenous bone and bone substitutes in critical-size defects: an animal experiment. → Clin Oral Implants Res. 2004 Apr;15(2):187–93.18Santamaría J, García AM, de Vicente JC, Landa S, López-Arranz JS. Bone regeneration after radicular cyst removal with and without guided bone regeneration: pathology. → Int J Oral Maxillofac Surg. 1998 Apr;27(2):118–20. Some researchers have supported that the remaining cystic cavities should be filled with biointegrative materials to prepare the site for implant placement.19Ihan Hren N, Miljavec M. Spontaneous bone healing of the large bone defects in the mandible. → Int J Oral Maxillofac Surg. 2008 Dec;37(12):1111–6. However, other authors have reported that spontaneous bone healing occurred without the use of bone grafts.20Pradel W, Eckelt U, Lauer G. Bone regeneration after enucleation of mandibular cysts: comparing autogenous grafts from tissue-engineered bone and iliac bone. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Mar;101(3):285–90. According to this last study, bone density can increase by 48% after 12 months and by 91% after 24 months, as seen after marsupialization of large jaw cysts. The success of spontaneous regeneration should be directly related to the size of the bony defect, anatomical features, patient’s age and other parameters, such as monocortical or bicortical defect type.21Ihan Hren N, Miljavec M. Spontaneous bone healing of the large bone defects in the mandible. → Int J Oral Maxillofac Surg. 2008 Dec;37(12):1111–6.
The objective of this retrospective clinical study was to evaluate spontaneous bone regeneration after enucleation of large jaw cysts, achieved with a conservative surgical technique, without using any filling material.
Materials and methods
This study was conducted at the Department of Oral Surgery of the San Giovanni Calibita, Fatebenefratelli Hospital, Rome, Italy, from January 2000 to July 2012. All consecutive patients requiring a Partch II surgical intervention for cyst removal were enrolled. Each patient was completely informed about the possible risks of the intervention and the surgical procedure.Preoperative analysis
Panoramic radiographs were obtained for all of the patients subjected to surgical enucleation (Fig. 1). The dimensions of the cysts were evaluated on panoramic radiographs taken just before surgical treatment. A preoperative computed tomography (CT) scan was required only in cases of very large jaw cysts with erosion of cortical plates, in order to evaluate more precisely the extent of the lesions (Fig. 2).
Surgical protocol
The surgery was conducted by one surgeon (MDD) in a single session for each patient, with standardized techniques. All of the patients received antibiotics before surgery. Local antimicrobial treatment was performed with 0.12% chlorhexidine digluconate mouth rinses t.i.d. for two weeks, starting three days before surgery, interrupted only on the first postoperative day. The majority of the surgeries (93.5%) were performed under local anesthesia with 2% mepivacaine. Only 22 (6.5%) surgical procedures were conducted under general anesthesia (in cases of cysts entering into the nasal cavity), depending on the general conditions, compliance, local and anatomical characteristics (such as the lesion extent), the site accessibility and the expected duration of the surgery. When the cysts were placed into the anterior region of the mandible, bilateral local anesthesia at Spix’s spine with 2% mepivacaine and infiltrative anesthesia with 2% mepivacaine and 1:100,000 epinephrine was administered. After the elevation of a fullthickness flap of adequate dimensions, with two lateral releasing incisions on the vestibular aspect (to preserve the lingual nerve in the mandible; Figs. 3 & 4), conservative access to the lesion was obtained using a round bur in a low-speed handpiece under irrigation with sterile saline (Fig. 5). In all of the cases, there was very little bone debris, owing to the minimally invasive surgical approach. Particular care was taken to preserve the maximum amount of bone in order to allow postoperative regeneration of the defect and to provide adequate support to the soft tissue during the healing period (bone bridging). Whenever possible, the cysts were enucleated in one piece with minimal invasion. The remaining cyst cavity was curetted to remove all residual fragments and to reduce the risk of recurrence (Fig. 6). The hopeless teeth were either extracted or endodontically treated, followed by apicectomy. In all of the cases, after the careful cleaning of the residual cavity, a primary closure was performed with a nonresorbable thread and interrupted sutures. No grafting material was placed into the residual bone sites. In all of the cases, a histological examination was performed, after fixation in a 4% formalin solution (Fig. 7).
The patients were advised to refrain from drinking and eating for 2 h after the surgical procedure and to then eat only cold and soft food for 24 h. After ten days, upon removal of the sutures, the wound was examined and controlled.
All of the patients were followed for possible complications, including hemorrhagic complications, swelling, hematoma and ecchymosis. Follow-ups entailed both clinical and radiographic evaluations in order to assess the reduction in size of the residual cavities. Clinical controls were performed ten days after surgery and radiographic assessment after 30 days and at six and 12 months postoperatively. The radiographic examinations, performed in order to evaluate the bone regeneration rate, entailed preoperative and postoperative panoramic radiographs and, in some cases, CT scans (Figs. 8 & 9). A CT dental scan was required in order to evaluate more precisely the rate of bone healing in the buccolingual dimension, using axial slices, if necessary. The findings from the panoramic radiographs were analyzed both subjectively and using the Kawai et al. radiographic classification, which evaluates the variation of the surgical site margins and the interior contents of the sites based on radiographs.22Kawai T, Murakami S, Hiranuma H, Sakuda M. Healing after removal of benign cysts and tumors of the jaws: a radiologic appraisal. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995 Apr;79(4):517–25.
-
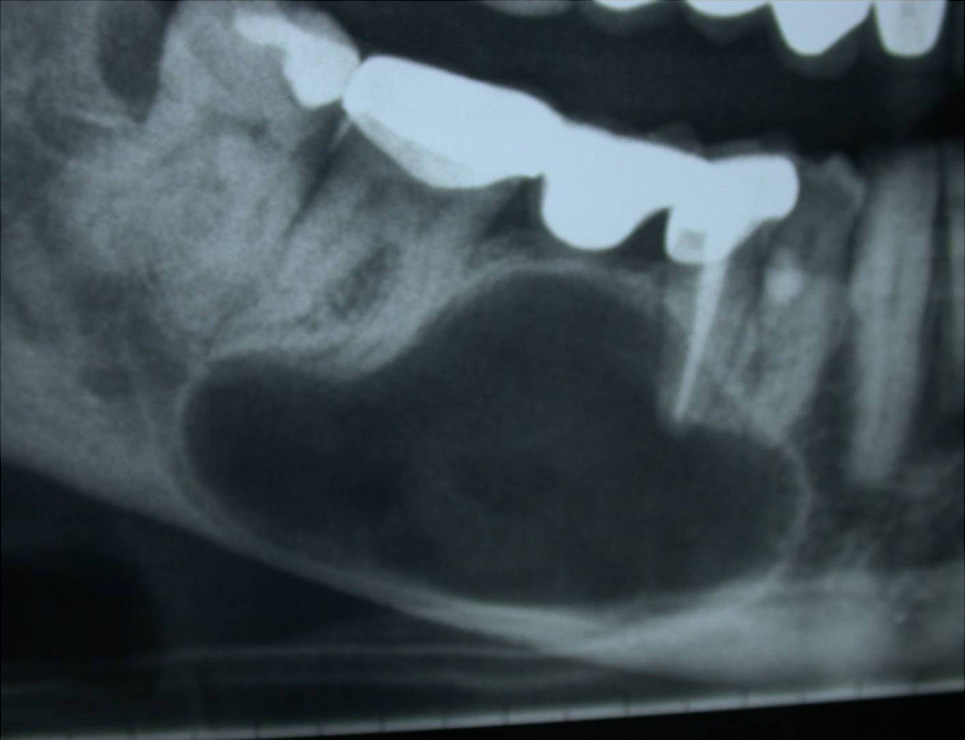
- Fig. 1 Preoperative radiographic view (2005).
-

- Fig. 2 Preoperative CT scan view (2005).
-

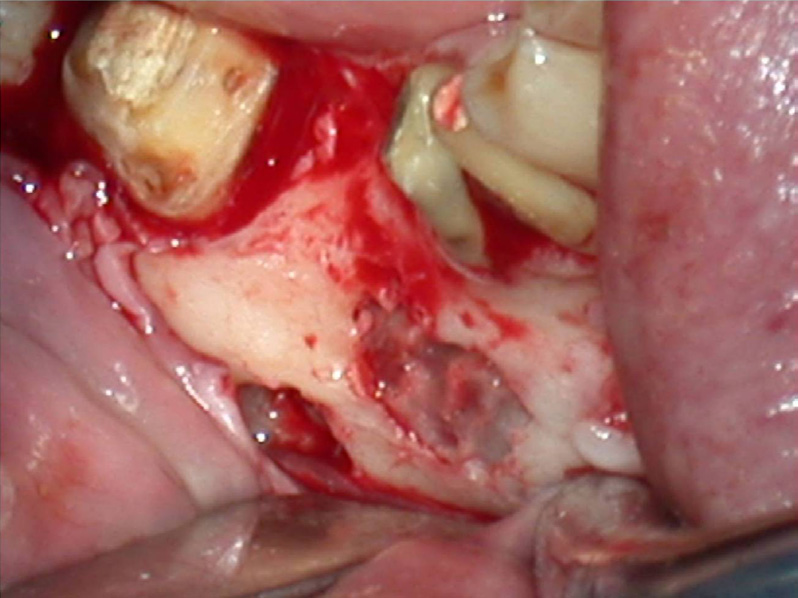
- Fig. 3 Preoperative clinical view.
-

-
Fig. 4
The surgery was performed under local anesthesia to obtain a larger working area.
-
- Fig. 5 An intra-oral view.
-
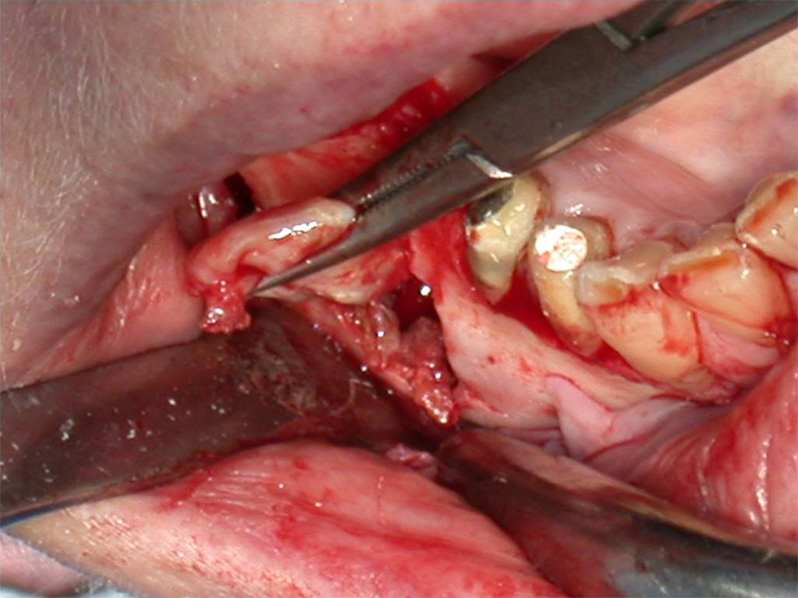
- Fig. 6 An intra-oral view during the cyst enucleation.
 Fig. 7 The cystic specimen.
Fig. 7 The cystic specimen.-
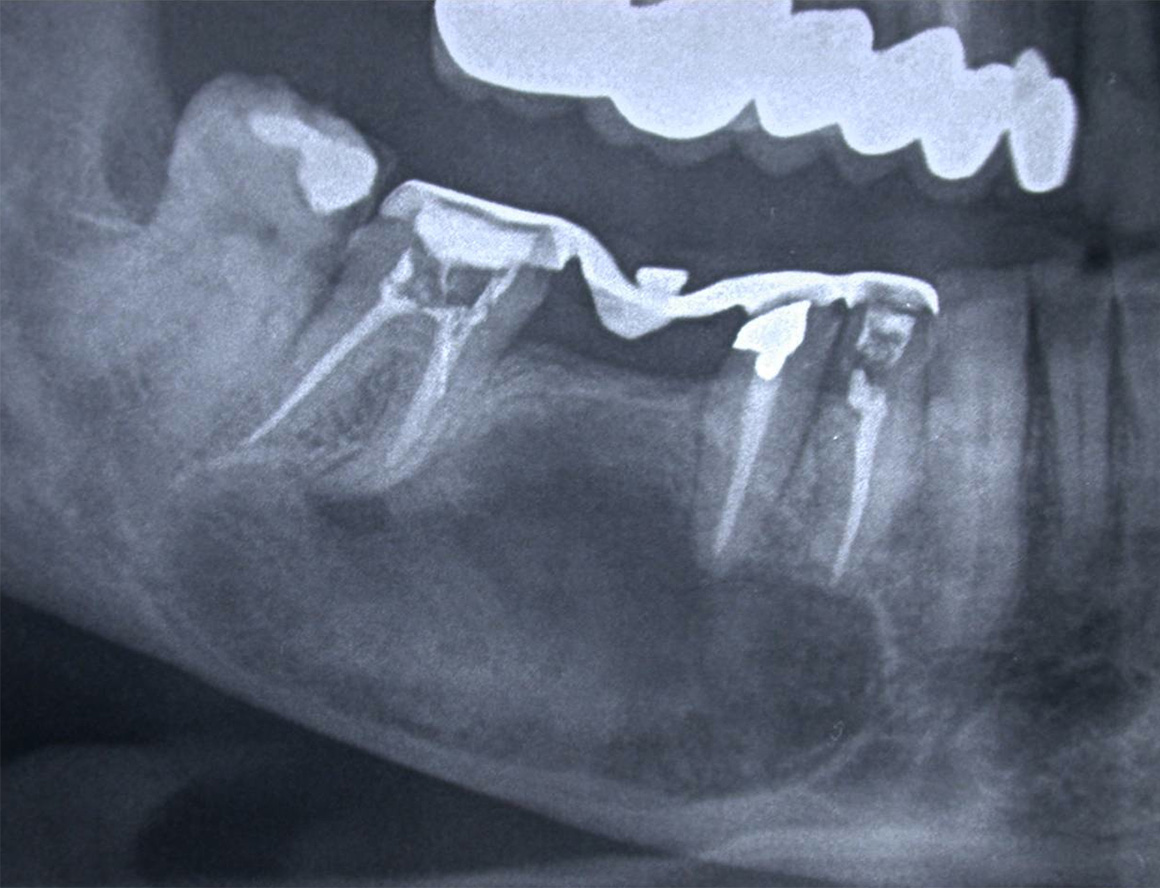
- Fig. 8 Postoperative radiographic view (six months after surgery).
-

- Fig. 9 Postoperative radiographic view (one year after surgery).
Results
The sample included 336 patients, 200 males (59.5%) and 136 females (40.5%) ranging from 10 to 83 years of age (mean age and standard deviation of 43.4 ± 16.8), as demonstrated in Table 1. No patients were lost during follow-up. The majority (68.8%) of the patients had mandibular cysts and the remainder of the sample (31.3%) had maxillary lesions.
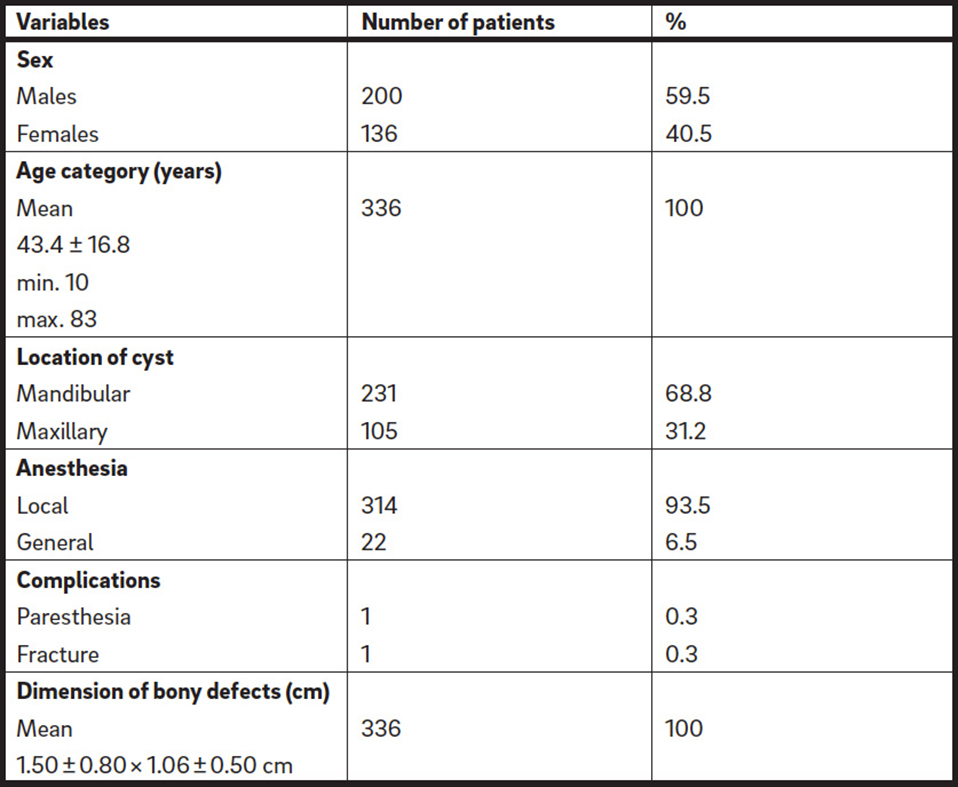
Demographic composition of the study population and clinical features.
Surgical and radiographic data
The mean dimensions of the bony defects were 1.50 ± 0.80 × 1.06 ± 0.50 cm. Primary closure was obtained in all of the cases. Minor complications (swelling, hematoma and ecchymosis were present in 85% of the cases) were reported during the first week. At the second recall, these minor complications were no longer present. No hemorrhagic complications occurred. An inferior alveolar nerve paresthesia and a compound fracture both occurred in only one patient (0.3%).
The patient with the mandibular fracture was treated with analgesics and a soft diet under close observation. No surgical intervention to reduce and stabilize the fracture was carried out. At six months postoperatively, the affected patient experienced a spontaneous full recovery of the inferior alveolar nerve paresthesia.
Clinical and radiographic evaluation performed 12 months after the surgical procedure showed complete healing of the lesions in all of the cases, with no sign of inflammation, infection or recurrence. On the basis of Kawai et al.’s criteria23Kawai T, Murakami S, Hiranuma H, Sakuda M. Healing after removal of benign cysts and tumors of the jaws: a radiologic appraisal. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995 Apr;79(4):517–25. and of the postoperative radiographic and clinical controls, all of these areas were considered healthy and showed complete bone recovery. The postoperative CT scans performed on patients with very large mandibular cysts showed complete bone regeneration and reconstitution of almost normal anatomy of the previously affected jaw segment 12 months after surgery. There were also gradual increases in bone density in both mandibular and maxillary defects. In all of the cases, the clinical healing patterns were similar.
Histological data
According to the World Health Organization classification, most of the cysts were odontogenic cysts of inflammatory origin, followed by odontogenic cysts of unspecified nature; radicular cysts (also termed periapical cysts); cystic lesions of odontogenic developmental dentigerous (or follicular) nature, unilocular and/or multilocular; unspecified granulation tissue; odontomas; periapical granulomas; ameloblastomas; keratocysts; nonodontogenic nasopalatine duct cysts; inflammatory residual cysts; and lesions due to other diseases, such as odontogenic fibromas, nonepithelial, traumatic and hemorrhagic cysts, sinus polyposis, epulis, fibrous bone dysplasia and oral melanosis. The diagnoses are reported in Table 2.
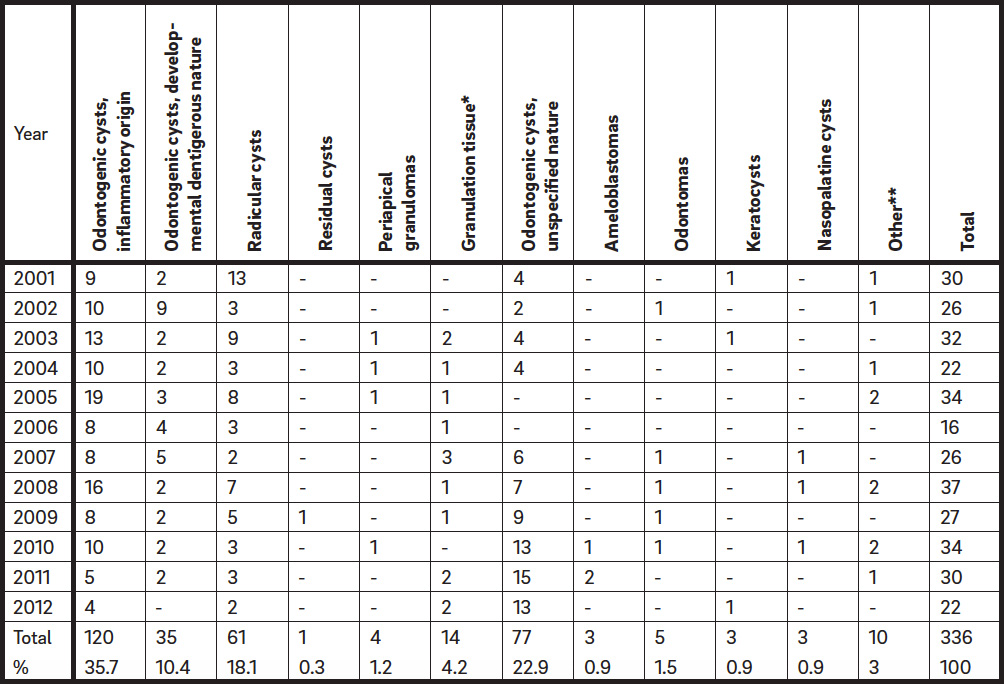
Distribution of oral cysts in the population sample.
* Unspecified.
** Such as odontogenic fibromas, nonepithelial, traumatic and hemorrhagic cysts, sinus polyposis, epulis, fibrous bone dysplasia and oral melanosis.
Discussion
Bone reconstruction has been considered an essential requirement for complete functional rehabilitation after jaw surgery. Although many studies have supported the use of different bone grafts to reduce the risk of jaw weakness,24Chiapasco M, Rossi A, Motta JJ, Crescentini M. Spontaneous bone regeneration after enucleation of large mandibular cysts: a radiographic computed analysis of 27 consecutive cases. → J Oral Maxillofac Surg. 2000 Sep;58(9):942–8.25Damante JH, Da S Guerra EN, Ferreira O Jr. Spontaneous resolution of simple bone cysts. → Dentomaxillofac Radiol. 2002 May;31(3):182–6.26Caicoya SO. Bone cavity filling with alloplastic material in maxillofacial surgery. → Rev Esp Cir Oral y Maxillofac. 2007 Jan-Feb;29(1):21–32.27Wiltfang J, Kloss FR, Kessler P, Nkenke E, Schultze-Mosgau S, Zimmermann R, Schlegel KA. Effects of platelet-rich plasma on bone healing in combination with autogenous bone and bone substitutes in critical-size defects: an animal experiment. → Clin Oral Implants Res. 2004 Apr;15(2):187–93. the present study showed that spontaneous bone regeneration occurred in all of the residual bony defects without the use of any filling material. The physiological healing process occurred with spontaneous bone regeneration even in the presence of large residual cystic cavities. The present study suggested that this type of intervention was very safe and minimally invasive, despite the increased surgical duration and technical complexity, with a complete recovery of the area occupied by jaw cysts. The bone recovery could be demonstrated with absolute accuracy only on CT scan controls, comparing on a digitalized image the preoperative and postoperative bone density. However, the main limitation of the present study was the short follow-up period. In fact, in order to confirm data from the present study, a longitudinal control (five years after surgery) would be recommended.
However, in most cases, patients with cysts in edentulous areas underwent a CT scan evaluation for the following implant-supported prosthetic rehabilitation.28Di Dio M, De Luca M, Cammarata L, Pierazzi G. Bone regeneration after removal of a mandibular cyst and following prosthetic rehabilitation with implants. Case report. → Minerva Stomatol. 2005 Jun;54(6):373–8. Morphometric analysis, similarly to Chiapasco et al.,29Chiapasco M, Rossi A, Motta JJ, Crescentini M. Spontaneous bone regeneration after enucleation of large mandibular cysts: a radiographic computed analysis of 27 consecutive cases. → J Oral Maxillofac Surg. 2000 Sep;58(9):942–8. was not performed because implant stability and survival clinically demonstrated that bone was of a good quality. These results corroborate those of Pradel et al., who concluded that the bone density increased after enucleation of large mandibular cysts without using filling material.30Pradel W, Eckelt U, Lauer G. Bone regeneration after enucleation of mandibular cysts: comparing autogenous grafts from tissue-engineered bone and iliac bone. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Mar;101(3):285–90. Similar results were obtained by Chiapasco et al.31Chiapasco M, Rossi A, Motta JJ, Crescentini M. Spontaneous bone regeneration after enucleation of large mandibular cysts: a radiographic computed analysis of 27 consecutive cases. → J Oral Maxillofac Surg. 2000 Sep;58(9):942–8.
The differential diagnosis between odontogenic cysts and ameloblastomas could be attained by analyzing the postoperative recurrence in the short term. Differences such as root resorption of adjacent teeth may aid the clinician in the preoperative differential diagnosis. In a radiographic preoperative analysis, ameloblastomas proved to have a root resorptive potential far greater than did other cystic lesions. No recurrence was noted during the entire follow-up period of the study, although the incidence was about 3%. However, ongoing follow-up examination is required and essential for management.
Conclusions
Within the limitations of this study, some observations in agreement with current literature can be made. Spontaneous bone regeneration with bone bridging outside the residual cyst cavity can occur after surgical removal of large jaw cysts without the aid of any grafting materials, according to evidence-based clinical and radiographic criteria. There was also a reduction of the risks of paresthesia and fracture in the mandible, owing to the conservative approach. This will simplify the surgical procedure, decreasing financial and biological costs and reducing the risk of postoperative complications.
Competing interests
The authors declare that they have no competing interests.
References
| 1. | ↑ | Getter L, Bhaskar SN, Cutright DE, Perez B, Brady JM, Driskell TD, O’Hara MJ. Three biodegradable calcium phosphate slurry implants in bone. → J Oral Surg. 1972 Apr;30(4):263–8. |
| 2. | ↑ | Salama R. Xenogeneic bone grafting in humans. → Clin Orthop Relat Res. 1983 Apr;(174):113–21. |
| 3. | ↑ | Horowitz I, Bodner L. Use of xenograft bone with aspirated bone marrow for treatment of cystic defect of the jaws. → Head Neck. 1989 Nov-Dec;11(6):516–23. |
| 4. | ↑ | Mitchell R. An evaluation of bone healing in cavities in the jaws implanted with a collagen matrix. → Br J Oral Maxillofac Surg. 1992 Jun;30(3):180–2. |
| 5. | ↑ | Moskow BS, Gold SI, Gottsegen R. Effects of scleral collagen upon the healing of experimental osseous wounds. → J Periodontol. 1976 Oct;47(10):596–606. |
| 6. | ↑ | Del Balso AM, Adrian JC. Collagen gel in osseous defects: a preliminary report. → Oral Surg Oral Med Oral Pathol. 1976 Nov;42(5):562–9. |
| 7. | ↑ | Bodner L. Effect of decalcified freeze-dried bone allograft on the healing of jaw defects after cyst enucleation. → J Oral Maxillofac Surg. 1996 Nov;54(11):1282–6. |
| 8. | ↑ | Bodner L. Osseous regeneration in the jaws using demineralized allogenic bone implants. → J Craniomaxillofac Surg. 1998 Apr;26(2):116–20. |
| 9. | ↑ | Schepers EJ, Ducheyne P, Barbier L, Schepers S. Bioactive glass particles of narrow size range: a new material for the repair of bone defects. → Implant Dent. 1993 Fall;2(3):151–6. |
| 10. | ↑ | Marx RE, Kline SN, Johnson RP, Malinin TI, Matthews JG 2nd, Gambill V. The use of freeze-dried allogeneic bone in oral and maxillofacial surgery. → J Oral Surg. 1981 Apr;39(4):264–74. |
| 11. | ↑ | Spengos MN. Irradiated allogeneic bone grafts in the treatment of odontogenic cysts. → J Oral Surg. 1974 Sep;32(9):674–8. |
| 12. | ↑ | Constantinides J, Zachariades N. Homogenous bone grafts to the mandible. → J Oral Surg. 1978 Aug;36(8):599–603. |
| 13. | ↑ | Marble HB Jr. Homografts of freeze-dried bone in cystic defects of the jaws: a survey of ninety-one cases. → Oral Surg Oral Med Oral Pathol. 1968 Jul;26(1):118–23. |
| 14, 24, 29, 31. | ↑ | Chiapasco M, Rossi A, Motta JJ, Crescentini M. Spontaneous bone regeneration after enucleation of large mandibular cysts: a radiographic computed analysis of 27 consecutive cases. → J Oral Maxillofac Surg. 2000 Sep;58(9):942–8. |
| 15, 25. | ↑ | Damante JH, Da S Guerra EN, Ferreira O Jr. Spontaneous resolution of simple bone cysts. → Dentomaxillofac Radiol. 2002 May;31(3):182–6. |
| 16, 26. | ↑ | Caicoya SO. Bone cavity filling with alloplastic material in maxillofacial surgery. → Rev Esp Cir Oral y Maxillofac. 2007 Jan-Feb;29(1):21–32. |
| 17, 27. | ↑ | Wiltfang J, Kloss FR, Kessler P, Nkenke E, Schultze-Mosgau S, Zimmermann R, Schlegel KA. Effects of platelet-rich plasma on bone healing in combination with autogenous bone and bone substitutes in critical-size defects: an animal experiment. → Clin Oral Implants Res. 2004 Apr;15(2):187–93. |
| 18. | ↑ | Santamaría J, García AM, de Vicente JC, Landa S, López-Arranz JS. Bone regeneration after radicular cyst removal with and without guided bone regeneration: pathology. → Int J Oral Maxillofac Surg. 1998 Apr;27(2):118–20. |
| 19, 21. | ↑ | Ihan Hren N, Miljavec M. Spontaneous bone healing of the large bone defects in the mandible. → Int J Oral Maxillofac Surg. 2008 Dec;37(12):1111–6. |
| 20, 30. | ↑ | Pradel W, Eckelt U, Lauer G. Bone regeneration after enucleation of mandibular cysts: comparing autogenous grafts from tissue-engineered bone and iliac bone. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Mar;101(3):285–90. |
| 22, 23. | ↑ | Kawai T, Murakami S, Hiranuma H, Sakuda M. Healing after removal of benign cysts and tumors of the jaws: a radiologic appraisal. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995 Apr;79(4):517–25. |
| 28. | ↑ | Di Dio M, De Luca M, Cammarata L, Pierazzi G. Bone regeneration after removal of a mandibular cyst and following prosthetic rehabilitation with implants. Case report. → Minerva Stomatol. 2005 Jun;54(6):373–8. |





Leave a Reply
Be the First to Comment!