Success, survival and failure rates of dental implants: a cross-sectional study
June 14, 2017 / Categories: Digital Dentistry, Implant Dentistry

Bandeira de Almeida, Amanda

Prado Maia, Luciana

Demoner Ramos, Umberto

Luís Scombatti de Souza, Sérgio

Bazan Palioto, Daniela
Abstract
Objective
The purpose of the present study was to evaluate the success, survival and failure rates of dental implants placed in the Implantology Clinic at the School of Dentistry of Ribeirão Preto of the University of São Paulo, Ribeirão Preto, Brazil.
Materials and methods
The cross-sectional study included only patients who had undergone prosthetic rehabilitation. The following criteria were evaluated by interview and dental record analysis: age, sex, presence of systemic disease, history of smoking, area in which the implant was placed, implant diameter and height, and type of prosthesis seated on the implant. The following parameters were clinically analyzed: pain, mobility, probing depth, bleeding on probing, and presence or absence of exudate. The amount of bone loss was assessed radiographically. The study included 35 implants placed in 19 patients.
Results
There was a success rate of 74% after definitive prosthetic rehabilitation, while six implants showed bone loss of between 2 and 4 mm, being classified as satisfactory survival. There was no relationship between the success and/or survival rate and any of the parameters evaluated. Four implants presented with periimplant mucositis, while periimplantitis was observed in two implants. Regarding the definitive restorations, 17 prostheses were classified as successful, while there were complications in eight prostheses.
Conclusion
Success and survival rates of 74% and 100%, respectively, were observed. Within the limitations of this cross-sectional study, the data suggest that the implant success rate does not seem to be related to factors like age, sex, habits, systemic disease, macroscopic characteristics or area in which the implant was placed.
Keywords
Dental implants, periodontics, periimplantitis.
Introduction
The use of dental implants is considered a revolution in modern dentistry.1Pimentel GH, Martins LD, Ramos MB, Lorenzoni FC, Queiroz AC. Perda óssea Peri-implantar e diferentes sistemas de implantes [Peri-implant bone loss and different implant systems].
→ Innov Implant J Biomater Esthet. 2010; 5(2):75–81. Italian.
However, there are differences between professional and patient objectives.2Pimentel GH, Martins LD, Ramos MB, Lorenzoni FC, Queiroz AC. Perda óssea Peri-implantar e diferentes sistemas de implantes [Peri-implant bone loss and different implant systems].
→ Innov Implant J Biomater Esthet. 2010; 5(2):75–81. Italian. While the patient is usually concerned with esthetics and function, dental professionals expect success regarding biological and mechanical stability and the facilitation of oral hygiene.3Pietrokovski J. The bony residual ridge in man.
→ J Prosthet Dent. 1975 Oct;34(4):456–62.
There is consensus among authors that the success of dental implant treatment depends on the presence and maintenance of surrounding bone, mainly in the bone crest area. However, one of the major challenges encountered in implantology is the process of bone resorption around the implant after insertion or during its use. In the literature, bone resorption of approximately 1.2 mm in height during the first year of function is reported, with 0.1 mm more resorption for every subsequent year.4Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw.
→ Int J Oral Surg. 1981 Dec;10(6):387–416. This loss with a V or U shape has been called saucerization.5Wyatt CC, Zarb GA. Bone level changes proximal to oral implants supporting fixed partial prostheses.
→ Clin Oral Implants Res. 2002 Apr;13(2):162–8.
In 1986, Albrektsson et al. established the following criteria for implant success:6Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success.
→ Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. The implant should have no mobility and demonstrate no radiolucent areas radiographically, annual vertical bone loss after the first year should be less than 0.2 mm, and there should be no persistent and/or irreversible symptoms. The most common parameter used in clinical reports is the survival rate, indicating whether the dental implant is physically in the mouth or has been removed.7Ten Bruggenkate C, van der Kwast WA, Oosterbeek HS. Success criteria in oral implantology. A review of the literature.
→ Int J Oral Implantol. 1990;7(1):45–51. However, with this method, implants that should be removed owing to pain or illness may be retained and erroneously considered successful.
In 1993, an implant quality of health scale was created by James and developed by Misch.8Misch CE. Implant success or failure: clinical assessment in implant dentistry.
→ In: Misch CE, editor. Contemporary implant dentistry. St Louis, MO: Mosby; 1993. p. 33–66.9Misch CE. The implant quality scale: a clinical assessment of the health–disease continuum.
→ Oral Health. 1998 Jul;88(7):15–20, 23–6; quiz 25–6. This scale was later modified at the Interna tional Congress of Oral Implantologists’ Pisa Consensus Conference in 2007, presenting four clinical categories that contain conditions of success, survival and failure of the implant. Survival can be divided into two categories: satisfactory survival, which describes implants with less than ideal conditions, but for which there is no need for clinical intervention; and compromised survival, which includes implants with less than ideal conditions requiring clinical treatment to reduce the risk of implant failure. Implant failure is the term used for implants that require removal or that have been lost. Implant success is a term used to describe clinical conditions and must include at least a 12-month period for implants serving as prosthetic abutments. Early success is suggested for implants that are retained for a period of one to three years, intermediate success for three to seven years and long-term success for a period longer than seven years. In this new approach, pain, mobility, radiographic bone loss, probing depth and periimplant disease are evaluated.10Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz-Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference.
→ Implant Dent. 2008 Mar;17(1):5–15.
Regarding periimplant disease, since the bone loss caused by stress or bacteria leads to the deepening of the sulcular gap and decreases oxygen tension, anaerobic bacteria become the primary promoter of continuous bone loss.11Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz-Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference.
→ Implant Dent. 2008 Mar;17(1):5–15. Exudate or an abscess around an implant indicates exacerbation of periimplant disease and possibly accelerated bone loss. Exudate persisting for more than one or two weeks normally requires surgical intervention in the periimplant area to eliminate the etiological factors.12Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz-Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference.
→ Implant Dent. 2008 Mar;17(1):5–15. The reduced bone height after the exudate episode exposes the implant to secondary occlusal trauma. The dentist should re-evaluate and reduce the stress factors for the new bone condition to improve the performance in the long term.13Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz-Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference.
→ Implant Dent. 2008 Mar;17(1):5–15.
Considering the importance of maintenance of the crestal bone around dental implants, the aim of this study was to evaluate the success, survival and failure rates of implants placed over three years based on the implant quality of health scale of the Pisa Consensus Conference.
Materials and methods
This study included 19 patients who received implants and prostheses on implants in the Implantology Clinic at the School of Dentistry of Ribeirão Preto of the University of São Paulo, Ribeirão Preto, Brazil, between 2007 and 2013. The patients were recalled for clinical and radiographic examinations from three to six years after implant placement.
The following criteria were evaluated by interview and dental record analysis: age, sex, presence of systemic disease, history of smoking, area in which the implant was placed, implant diameter and height, and type of prosthesis seated. For the analysis of implant diameter, the following classification was used: narrow when the diameter was less than 3.5 mm, regular when the diameter was 4.0–4.8 mm, and wide when the diameter was greater than 5.0 mm. Regarding height, implants were classified as short when they were less than 10 mm, regular when 10–12 mm, and long when greater than 12 mm.
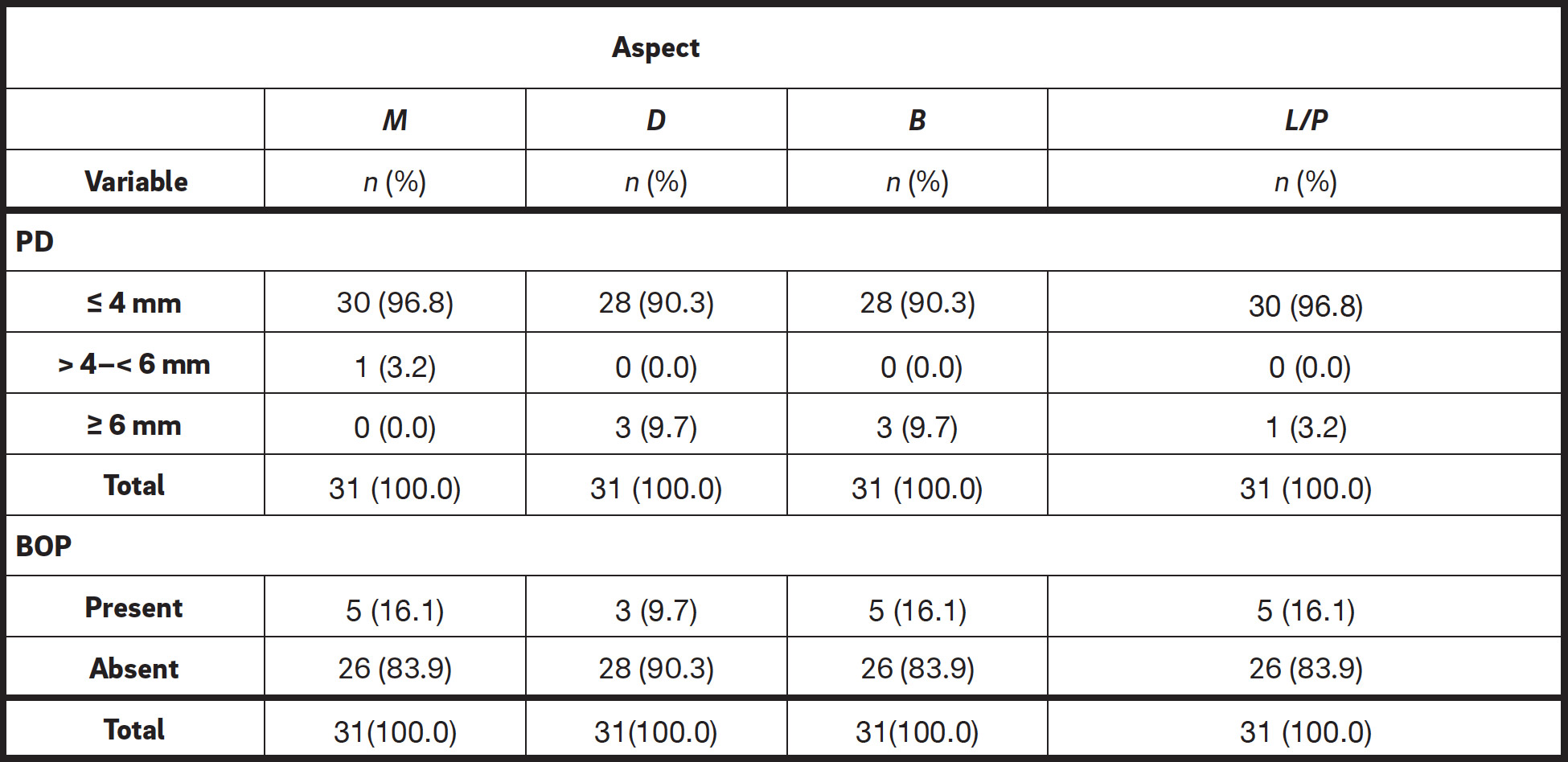
The success and survival rates of the implants were analyzed based on the criteria of the Pisa Consensus Conference, according to the following clinical parameters: pain (absent, absent in function, sensitivity in function, pain in function), mobility (present or absent), probing depth (PD), bleeding on probing (BOP), exudate (absent, with exudate history, with uncontrolled exudate) and radiographic bone loss. The PD and BOP measurements were taken at four aspects of each implant: mesial (M), distal (D), buccal (B) and lingual/palatal (L/P).
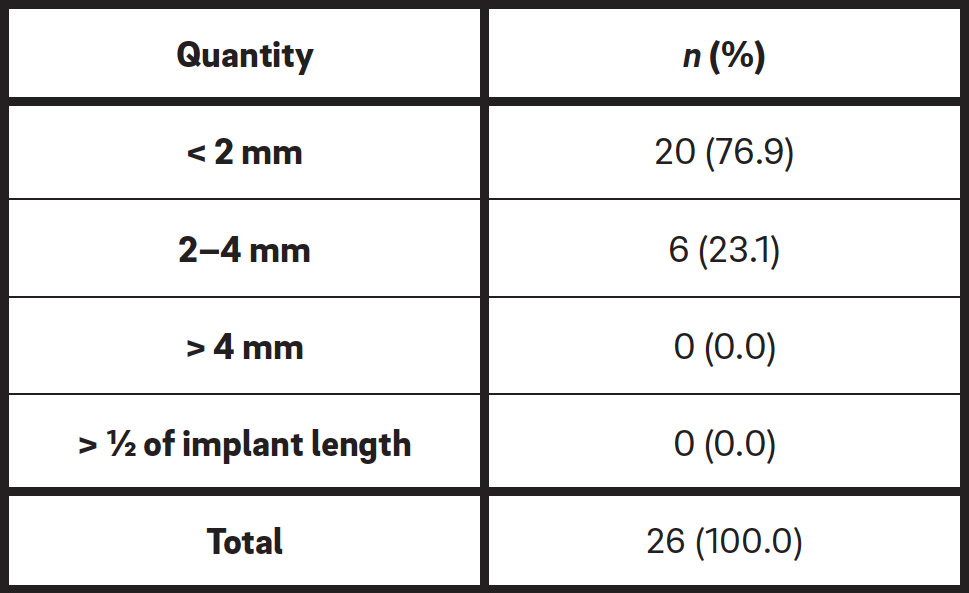
For the assessment of radiographic bone loss, a periapical radiograph using the bisecting angle technique was performed at the time of patient recall. The radiographs were digitalized and analyzed using the Image Tool software (Trophy-Radiologie, Vincennes, France) to verify and determine the resulting linear distance between the implant shoulder and bone crest. The average values for the M and D aspects were used as a single measurement for each implant. From this analysis, the implants were divided into the following categories: bone loss of less than 2 mm; bone loss of between 2 and 4 mm; bone loss of more than 4 mm, but less than half of the implant body; and bone loss greater than half of the length of the implant. According to these criteria, the implants were classified as successful, having satisfactory survival, having impaired survival or failed.
Biological and prosthetic complications, such as periimplant mucositis, periimplantitis, abscesses or fistulas, or any mechanical and prosthetic complications, such as fracture of the implant and/or of any prosthetic component, were also evaluated. Patients with BOP or positive suppuration, a PD of greater than 5 mm and radiographic bone loss were diagnosed as having periimplantitis.14Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5.
Results
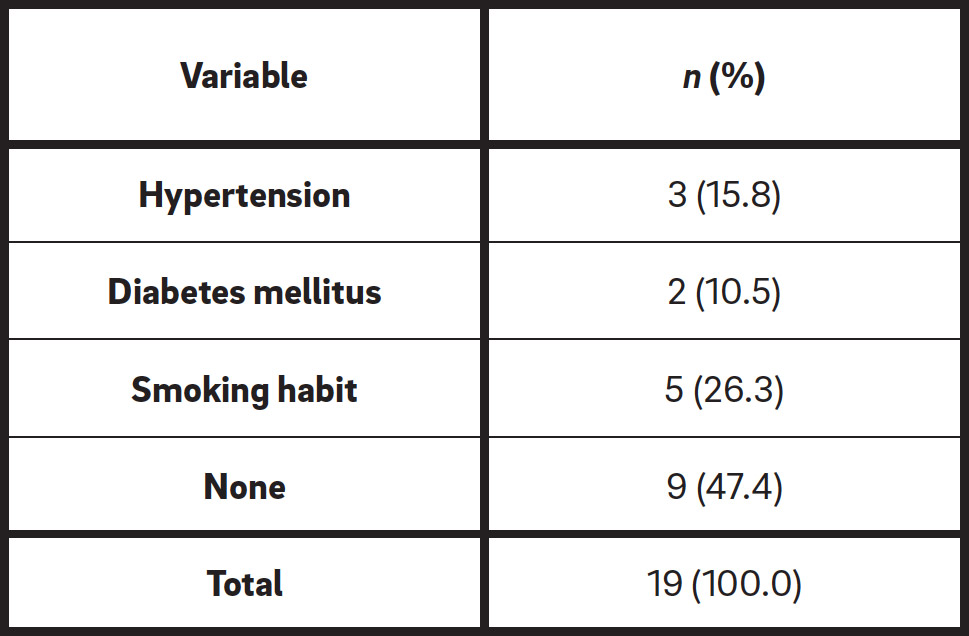
The study included 35 implants placed in 19 patients, six men and 13 women, with the following age distribution: two patients aged between 30 and 39, six patients between 40 and 49, seven patients between 50 and 59, three patients between 60 and 69, and one patient between 70 and 79. The prevalence of systemic disease and a smoking habit was assessed by interview and the results are presented in Table 1.
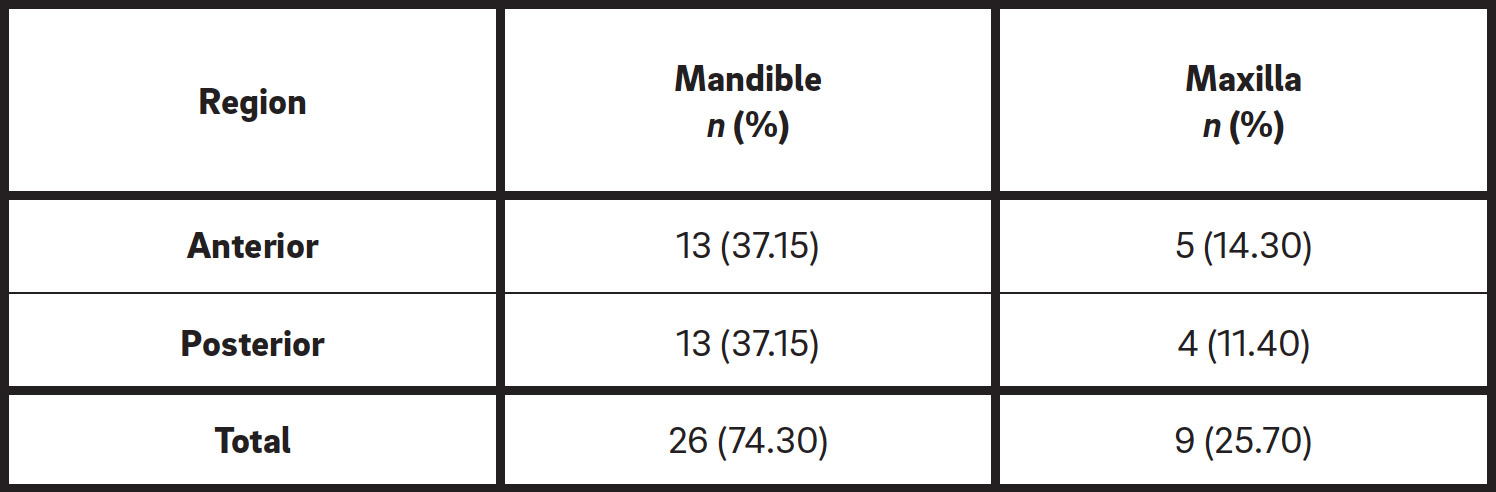
The implants were classified according to the placement area: mandible and maxilla and anterior and posterior (Table 2). Three patients were rehabilitated with full-arch fixed prostheses supported by osseointegrated implants, 20 received single prostheses and two received an overdenture.
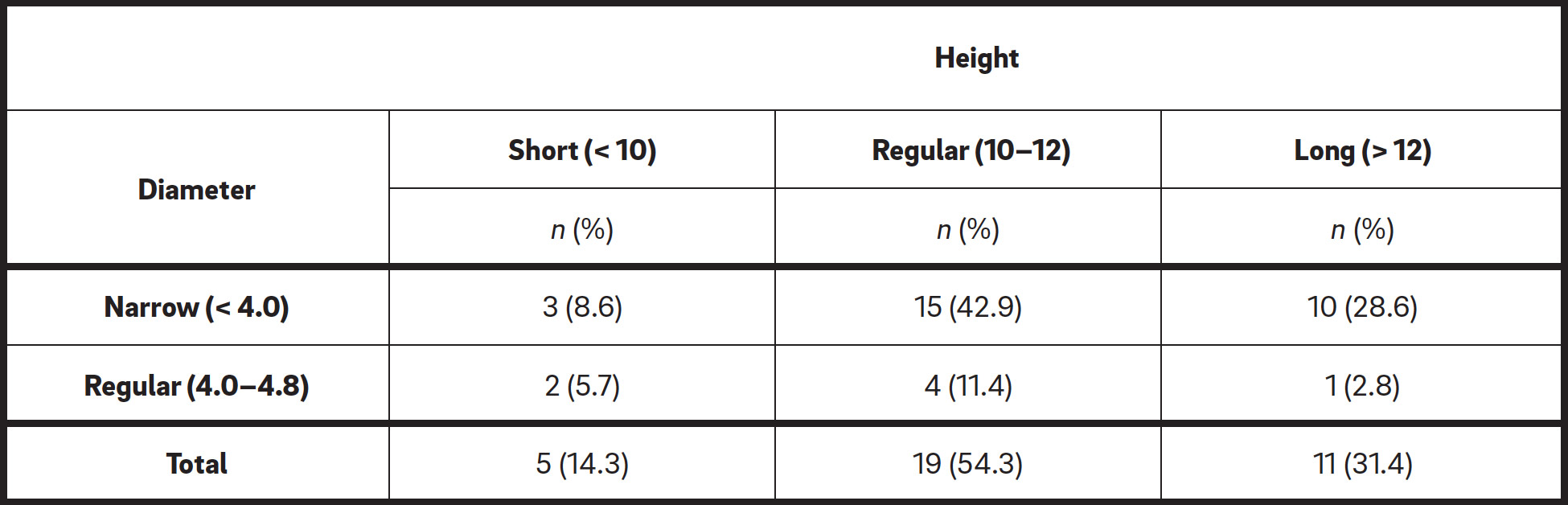
Concerning the implant diameter, 80% of the implants were classified as narrow and 20% as regular (Table 3). Regarding the implant height, 14.28% of the implants were classified as short, 54.28% as regular and 31.46% as long (Table 3). A higher frequency of implants of 11 mm in height and less than 4 mm in diameter was observed.
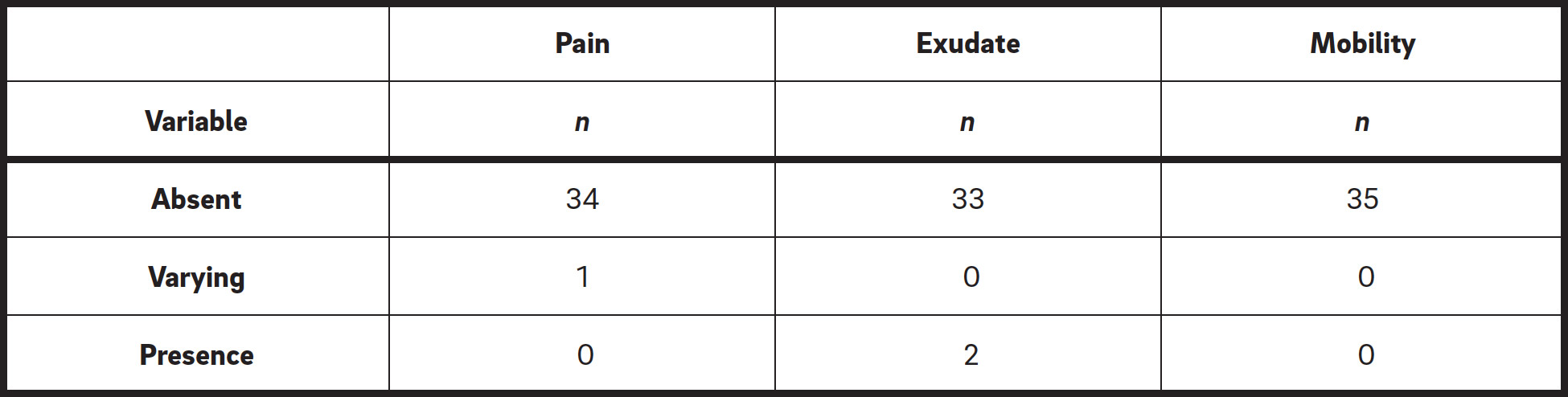
Regarding the presence of clinical signs associated with the implants, such as pain, exudate and mobility, 18 patients (who received 34 implants) reported no pain. The presence of pain in function occurred in only one implant and the presence of exudate in two implants (Table 4).
In general, PDs of less than 4 mm were observed in most cases. Only one implant showed a PD of 5 mm at the M aspect, while a PD of 6 mm and BP were observed at one implant at the L/P aspect and at three implants at the D and B aspects. BOP was present at five implants at the M, B and L/P aspects, and at three implants at the D aspect (Table 5). Four implants could not be evaluated owing to the presence of a protocol-type prosthesis.
Twenty-six of the 35 implants were evaluated in periapical radiographs by measuring the linear distance between the implant shoulder and bone crest. Only 17.1% of the implants showed bone loss of between 2 and 4 mm, while the remaining implants presented with less than 2 mm (Table 6).
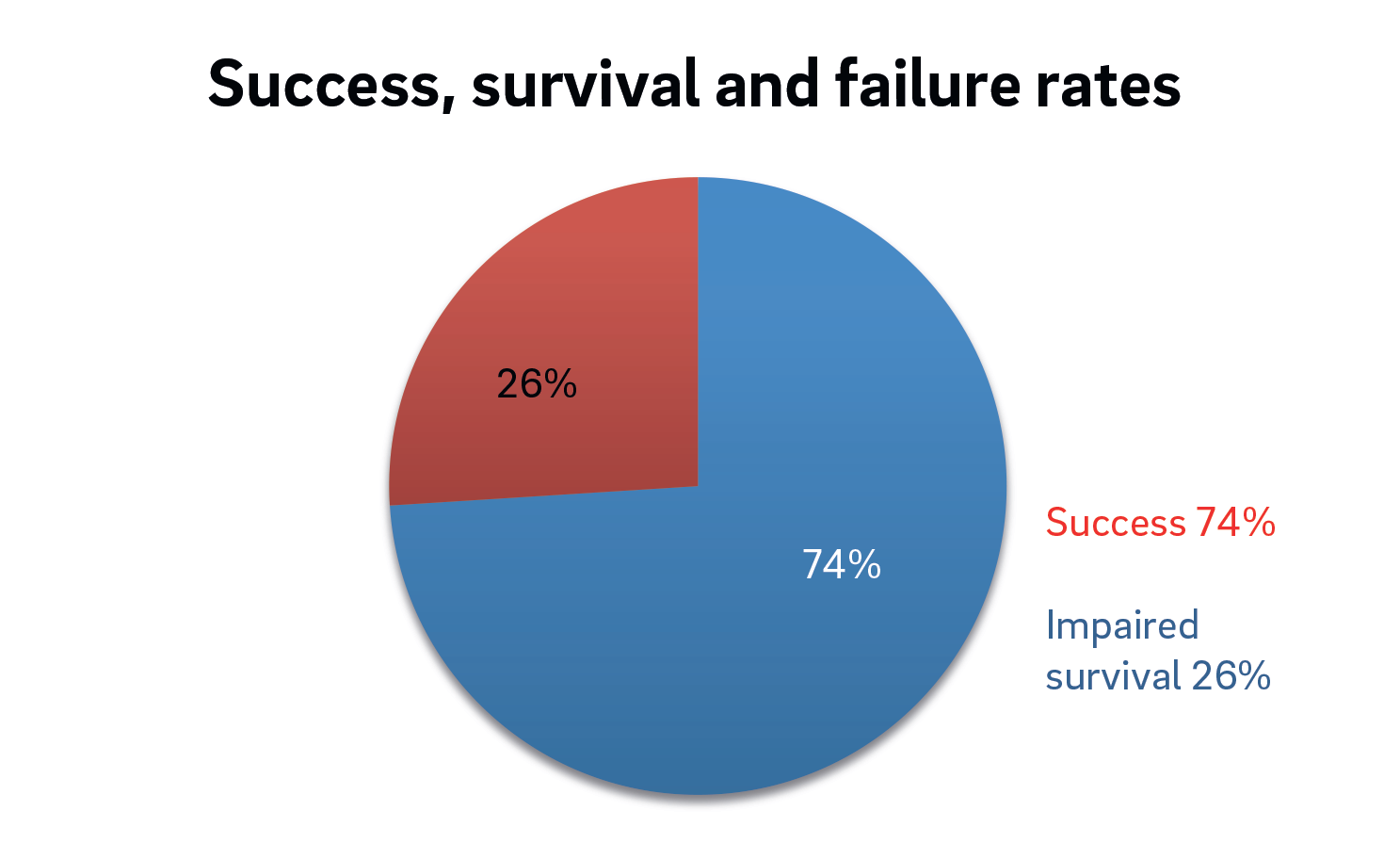
Analyzing all of the parameters established a success rate of 74% (20 implants), while 26% of the implants (six implants) were classified as having impaired survival (Fig. 1). The implants that had impaired survival showed different characteristics regarding location, size and PD. Regarding the height of these implants, three were longer than 12 mm, two were 10–12 mm in height and one less than 10 mm in height. Concerning the diameter, four of these implants were narrow and two were regular. Around the six implants classified as having impaired survival, a PD of greater than 4 mm was observed. Of all of the implants evaluated, four presented with periimplant mucositis (11.4%) and two with periimplantitis (5.7%), diagnosed by the presence of BOP or suppuration and radiographic bone loss.
-
- Fig. 1
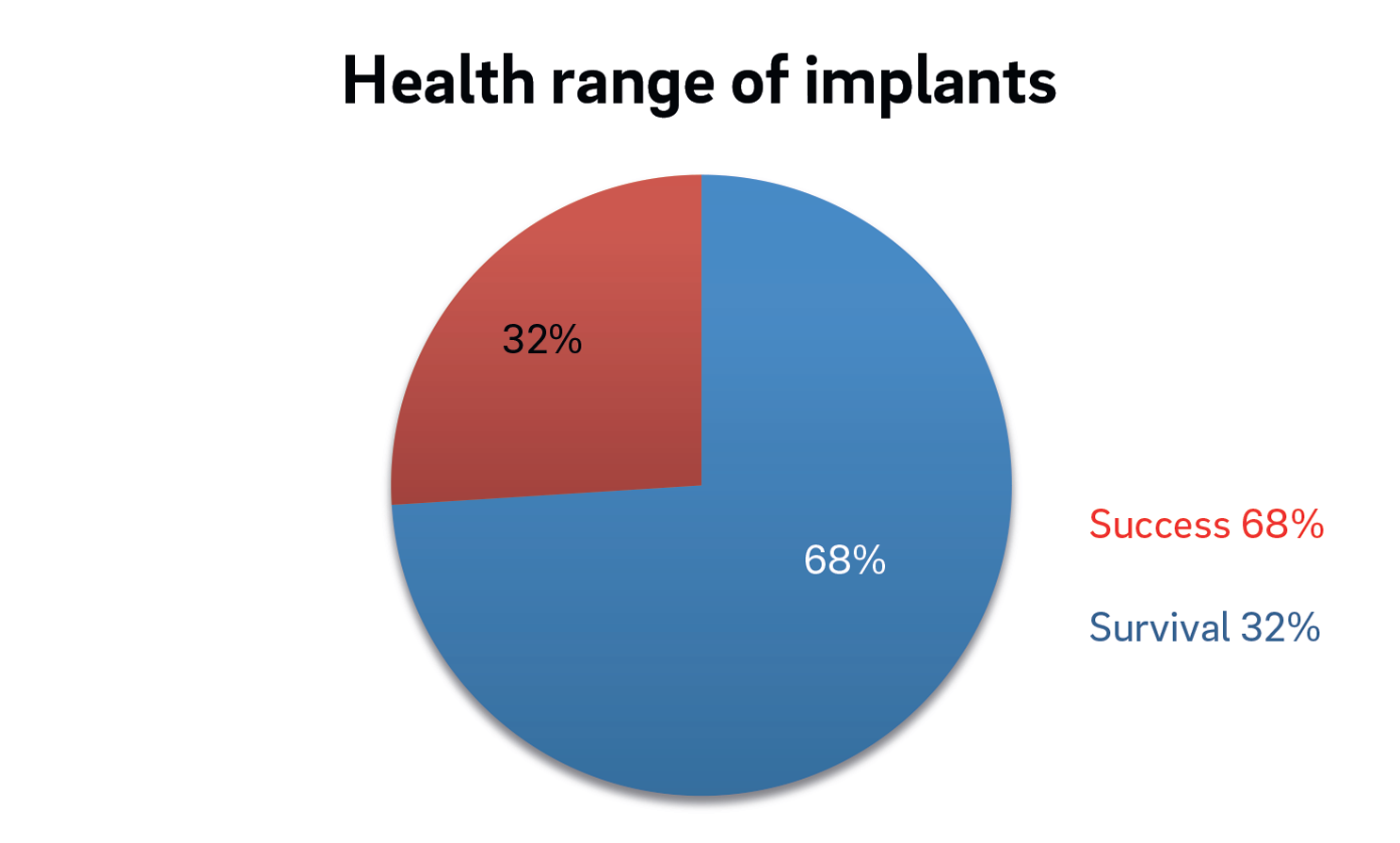
Regarding the definitive rehabilitation, 17 prostheses were classified as successful, while prosthetic complications were observed in eight implants (splinter or porcelain fracture, fracture of the prosthetic components, failure of the cement or screw loosing), resulting in a 68% success rate and a 32% survival rate of the prosthetic restorations (Fig. 2).
-
- Fig. 2
Discussion
This study aimed to evaluate the success, survival and failure rates of implants based on the implant quality of health scale developed at the Pisa Consensus Conference. The success category describes optimal conditions; the survival category describes functional implants, but not in an ideal condition, and is divided into satisfactory and impaired survival; and the failure category includes implants that should or could be removed.
In this study, one patient reported pain on function and implant mobility was observed in a second one. In both cases, the factor that caused such impairment was the presence of an unsatisfactory prosthesis. Misch et al. state that pain should not be associated with the implant after healing, and when it is observed, it is associated with an improper prosthetic component or with pressure on the tissue owing to seating of the prosthesis, suggesting that the prosthetic component can contribute to the instability of the implant.15Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz-Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference.
→ Implant Dent. 2008 Mar;17(1):5–15.
BOP was found in eight implants and increased PD (> 4 mm) in five implants. The occurrence of BOP after insertion of a probe with light pressure reveals the presence of an inflammatory lesion in the gingiva around the tooth. With respect to the mucosa around the implant, the accuracy of the diagnostic role of BOP seems to be greater than around natural teeth.16Luterbacher S, Mayfield L, Brägger U, Lang NP. Diagnostic characteristics of clinical and microbiological tests for monitoring periodontal and peri-implant mucosal tissue conditions during supportive periodontal therapy (SPT).
→ Clin Oral Implants Res. 2000 Dec;11(6):521–9. In the present study, 58% of the periimplant tissue was considered healthy.
In addition to these criteria, other factors may be related to the rate of success or failure of the implant, such as age, sex, systemic disease, smoking, area of implant placement, implant diameter and height, additional surgery and bone resorption. In the present study, the success and survival rates were similar among the age groups, corroborating with the findings in the literature that the age of the patient is not related to the implant success rate.17Sussman HI. Endodontic pathology leading to implant failure—a case report.
→ J Oral Implantol. 1997;23(3):112–5; discussion 115–6.18Zarb GA, Schmitt A. Implant therapy alternatives for geriatric edentulous patients.
→ Gerodontology. 1993 Jul;10(1):28–32.19Bryant SR, Zarb GA. Osseointegration of oral implants in older and younger adults.
→ Int J Oral Maxillofac Implants. 1998 Jul-Aug;13(4):492–9. Five patients with systemic disease and five with a smoking habit were included in the study. Regarding systemic disease, studies have shown that there is no obvious difference in the quality of periimplant tissue,20Mombelli A, Cionca N. Systemic diseases affecting osseointegration therapy.
→ Clin Oral Implants Res. 2006 Oct;17 Suppl 2:97–103. and this was observed in our study too, since implants in patients with diabetes were successful. However, in smoking patients, there is evidence that the habit has an important influence on the periimplant tissue, regarding both the healing after implant placement and the implants’ long-term prognosis.21Galindo-Moreno P, Fauri M, Avila-Ortiz G, Fernandez-Barbero JE, Cabrera-Leon A, Sanchez-Fernandez E. Influence of alcohol and tobacco habits on peri-implant marginal bone loss: a prospective study.
→ Clin Oral Implants Res. 2005 Oct;16(5):579–86.22Sánchez-Pérez A, Moya-Villaescusa MJ, Caffesse RG. Tobacco as a risk factor for survival of dental implants.
→ J Periodontol. 2007 Feb;78(2):351–9.23Francsson C, Wennstrom J, Berglundh T. Clinical characteristics at implants with a history of progressive bone loss.
→ Clin Oral Implants Res. 2008 Feb;19(2):142–7.24Strietzel FP, Reichart PA, Kale A, Kulkarni M, Wegner B, Kuchler I. Smoking interferes with the prognosis of dental implant treatment: a systematic review and meta-analysis.
→ J Clin Periodontol. 2007 Jun;34(6):523–44. There is a higher risk of inflammation and periimplant bone loss in smokers compared with nonsmokers.16–19 In our study, the implants placed in smokers did not fail, but 60% of them had bone loss of 2–4 mm, which can be seen as a dubious or even unfavorable prognosis, considering the follow-up period after implant placement.
The literature shows a lower success rate of implants placed in the maxilla compared with the mandible,25Adell R, Eriksson B, Lekholm U, Brånemark PI, Jemt T. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws.
→ Int J Oral Maxillofac Implants. 1990 Winter;5(4):347–59. a fact that is related to the lower density of the maxillary bone. The residual bone height becomes insufficient owing to the loss of alveolar bone. However, the molar area in both the maxilla and mandible displays substantial bone deficiency owing to increased occlusal forces, increasing the failure rate of implants in this area.26Adell R, Eriksson B, Lekholm U, Brånemark PI, Jemt T. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws.
→ Int J Oral Maxillofac Implants. 1990 Winter;5(4):347–59. In Type IV bone, the cortical bone is very thin, and the lack of dense bone makes it difficult to achieve adequate stability. The mandibular retromolar area and the maxillary molar region are formed by low-quality bone, while implants placed in the anterior mandible area have high success rates owing to increased cortical bone. In this study, there was no difference between implants placed in different regions of the jaws regarding their success or survival, corroborating the findings of Kim et al.27Kim YK, Kim SG, Kim JH, Yi YJ, Yun PY. Prospective study of tapered resorbable blasting media surface implant stability in the maxillary posterior area.
→ Oral Surg Oral Med Oral Pathol Oral Radiol. 2012 Jul;114(1):e19–24. It is necessary to consider that the study was conducted with a small number of patients and that probably in a larger sample these differences would be evident.
In our study, various implant systems were analyzed without differences in the success rate or acceptable survival rate, corroborating the findings of Ferrigno et al.28Ferrigno N, Laureti M, Fanali S, Grippaudo G. A long-term follow-up study of non-submerged ITI implants in the treatment of totally edentulous jaws. Part I: ten-year life table analysis of a prospective multicenter study with 1286 implants.
→ Clin Oral Implants Res. 2002 Jun;13(3):260–73. and Telleman et al.,29Telleman G, Meijer HJ, Raghoebar GM. Long-term evaluation of hollow screw and hollow cylinder dental implants: clinical and radiographic results after 10 years.
→ J Periodontol. 2006 Feb;77(2):203–10. who found similar results for the survival of different types of implant designs. In a literature review, Opperman et al. also concluded that, regarding implant survival, there are no types, surfaces or implant systems that present clear advantages over others.30Oppermann RV, Gomes SC, Fiorini T. Epidemiologia e fatores de risco para as doenças periimplantares [Epidemiology and risk factors for peri-implant diseases]. Portuguese.
→ Periodontia. 2008 Dec;18(4):14–21.
In summary, in the present study, 74% of the implants examined were classified as successful, with excellent prognoses, while 26% of the implants were classified as having impaired survival. Therefore, success and survival rates of 74% and 100%, respectively, were observed. It is important to highlight that only patients who had undergone definitive prosthetic rehabilitation were evaluated and maybe that is why no failure was observed, since Jeong et al. reported that failure usually occurs before seating of the definitive prosthesis.31Jeong SM, Choi BH, Kim J, Xuan F, Lee DH, Mo DY, Lee CU, Wonju, Korea. A 1-year prospective clinical study of soft tissue conditions and marginal bone changes around dental implants after flapless implant surgery.
→ Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Jan;111(1):41–6.
Conclusion
Within the limitations of this cross-sectional study, the data suggest that the implant success rate does not seem to be related to factors like age, sex, habits, systemic disease, macroscopic characteristics or area in which the implant was placed. This study can be considered preliminary and provides the basis for the design of further studies.
Author contributions
ABA, UDR and LPM made substantial contributions to conception and design, acquisition of data, and analysis and interpretation of data, and wrote substantial parts of the manuscript. ABA, LPM and UDR were involved in drafting the manuscript, participated in the data analysis and interpretation of the results, and revised critically for important intellectual content.
Acknowledgments
This study was supported by a grant (number 2012/25447-5) from the São Paulo Research Foundation.
Interview
with Amanda Bandeira de Almeida
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 2. | ↑ | Pimentel GH, Martins LD, Ramos MB, Lorenzoni FC, Queiroz AC. Perda óssea Peri-implantar e diferentes sistemas de implantes [Peri-implant bone loss and different implant systems]. → Innov Implant J Biomater Esthet. 2010; 5(2):75–81. Italian. |
| 3. | ↑ | Pietrokovski J. The bony residual ridge in man. → J Prosthet Dent. 1975 Oct;34(4):456–62. |
| 4. | ↑ | Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. → Int J Oral Surg. 1981 Dec;10(6):387–416. |
| 5. | ↑ | Wyatt CC, Zarb GA. Bone level changes proximal to oral implants supporting fixed partial prostheses. → Clin Oral Implants Res. 2002 Apr;13(2):162–8. |
| 6. | ↑ | Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. → Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. |
| 7. | ↑ | Ten Bruggenkate C, van der Kwast WA, Oosterbeek HS. Success criteria in oral implantology. A review of the literature. → Int J Oral Implantol. 1990;7(1):45–51. |
| 8. | ↑ | Misch CE. Implant success or failure: clinical assessment in implant dentistry. → In: Misch CE, editor. Contemporary implant dentistry. St Louis, MO: Mosby; 1993. p. 33–66. |
| 9. | ↑ | Misch CE. The implant quality scale: a clinical assessment of the health–disease continuum. → Oral Health. 1998 Jul;88(7):15–20, 23–6; quiz 25–6. |
| 10, 11, 12, 13, 15. | ↑ | Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz-Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. → Implant Dent. 2008 Mar;17(1):5–15. |
| 14. | ↑ | Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. |
| 16. | ↑ | Luterbacher S, Mayfield L, Brägger U, Lang NP. Diagnostic characteristics of clinical and microbiological tests for monitoring periodontal and peri-implant mucosal tissue conditions during supportive periodontal therapy (SPT). → Clin Oral Implants Res. 2000 Dec;11(6):521–9. |
| 17. | ↑ | Sussman HI. Endodontic pathology leading to implant failure—a case report. → J Oral Implantol. 1997;23(3):112–5; discussion 115–6. |
| 18. | ↑ | Zarb GA, Schmitt A. Implant therapy alternatives for geriatric edentulous patients. → Gerodontology. 1993 Jul;10(1):28–32. |
| 19. | ↑ | Bryant SR, Zarb GA. Osseointegration of oral implants in older and younger adults. → Int J Oral Maxillofac Implants. 1998 Jul-Aug;13(4):492–9. |
| 20. | ↑ | Mombelli A, Cionca N. Systemic diseases affecting osseointegration therapy. → Clin Oral Implants Res. 2006 Oct;17 Suppl 2:97–103. |
| 21. | ↑ | Galindo-Moreno P, Fauri M, Avila-Ortiz G, Fernandez-Barbero JE, Cabrera-Leon A, Sanchez-Fernandez E. Influence of alcohol and tobacco habits on peri-implant marginal bone loss: a prospective study. → Clin Oral Implants Res. 2005 Oct;16(5):579–86. |
| 22. | ↑ | Sánchez-Pérez A, Moya-Villaescusa MJ, Caffesse RG. Tobacco as a risk factor for survival of dental implants. → J Periodontol. 2007 Feb;78(2):351–9. |
| 23. | ↑ | Francsson C, Wennstrom J, Berglundh T. Clinical characteristics at implants with a history of progressive bone loss. → Clin Oral Implants Res. 2008 Feb;19(2):142–7. |
| 24. | ↑ | Strietzel FP, Reichart PA, Kale A, Kulkarni M, Wegner B, Kuchler I. Smoking interferes with the prognosis of dental implant treatment: a systematic review and meta-analysis. → J Clin Periodontol. 2007 Jun;34(6):523–44. |
| 25, 26. | ↑ | Adell R, Eriksson B, Lekholm U, Brånemark PI, Jemt T. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. → Int J Oral Maxillofac Implants. 1990 Winter;5(4):347–59. |
| 27. | ↑ | Kim YK, Kim SG, Kim JH, Yi YJ, Yun PY. Prospective study of tapered resorbable blasting media surface implant stability in the maxillary posterior area. → Oral Surg Oral Med Oral Pathol Oral Radiol. 2012 Jul;114(1):e19–24. |
| 28. | ↑ | Ferrigno N, Laureti M, Fanali S, Grippaudo G. A long-term follow-up study of non-submerged ITI implants in the treatment of totally edentulous jaws. Part I: ten-year life table analysis of a prospective multicenter study with 1286 implants. → Clin Oral Implants Res. 2002 Jun;13(3):260–73. |
| 29. | ↑ | Telleman G, Meijer HJ, Raghoebar GM. Long-term evaluation of hollow screw and hollow cylinder dental implants: clinical and radiographic results after 10 years. → J Periodontol. 2006 Feb;77(2):203–10. |
| 30. | ↑ | Oppermann RV, Gomes SC, Fiorini T. Epidemiologia e fatores de risco para as doenças periimplantares [Epidemiology and risk factors for peri-implant diseases]. Portuguese. → Periodontia. 2008 Dec;18(4):14–21. |
| 31. | ↑ | Jeong SM, Choi BH, Kim J, Xuan F, Lee DH, Mo DY, Lee CU, Wonju, Korea. A 1-year prospective clinical study of soft tissue conditions and marginal bone changes around dental implants after flapless implant surgery. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Jan;111(1):41–6. |





Leave a Reply
Be the First to Comment!