Three-year clinical and radiographic outcomes of patients treated according to the All-on-4 concept in the daily practice: A prospective observational study on implants and prosthesis survival rates and complications
June 27, 2016 / Categories: Digital Dentistry, Implant Dentistry

Tallarico, Marco

Meloni, Silvio Mario

Xhanari, Erta

Canullo, Luigi
All-on-4 treatment concept is widely applied for complete-arch rehabilitations. Nevertheless, minor technical and biological complications can occur. The objective of this study was to evaluate the three-year clinical and radiographic data of complete-arch fixed dental prostheses supported by four implants according to the All-on-4 protocol.
Introduction
Complete edentulism is associated with decreased masticatory function, as well as unfavorable esthetics due to the loss of support for the facial musculature, decreased vertical dimension and speech impairment.1Polzer I, Schimmel M, Müller F, Biffar R. Edentulism as part of the general health problems of elderly adults. → Int Dent J. 2010 Jun;60(3):143–55.2Emami E, de Souza RF, Kabawat M, Feine JS. The impact of edentulism on oral and general health. → Int J Dent. 2013;2013:498305. doi: 10.1155/2013/498305. Epub 2013 May 8.3Slade GD, Akinkugbe AA, Sanders AE. Projections of U.S. edentulism prevalence following 5 decades of decline. → J Dent Res. 2014 Oct;93(10):959–65. The conventional method for treating edentulous patients is to rehabilitate them with a complete removable denture.
However, the denture must be adjusted over time to compensate for the progressive tissue changes associated with denture wearing.4Felton D, Cooper L, Duqum I, Minsley G, Guckes A, Haug S, Meredith P, Solie C, Avery D, Chandler ND; American College of Prosthodontists; Academy of General Dentistry; American Dental Association Council on Scientific Affairs; American Dental Hygienists’ Association; National Association of Dental Laboratories; GlaxoSmithKline Consumer Healthcare. Evidence-based guidelines for the care and maintenance of complete dentures: a publication of the American College of Prosthodontists. → J Am Dent Assoc. 2011 Feb;142 Suppl 1:1S–20S.’ 5Carlsson GE. Clinical morbidity and sequelae of treatment with complete dentures. → J Prosthet Dent. 1998 Jan;79(1):17–23. Advances in implant dentistry have allowed a shift from a complete removable denture to an implant-supported overdenture for the oral rehabilitation of edentulous patients.6Batenburg RH, Meijer HJ, Raghoebar GM, Vissink A. Treatment concept for mandibular overdentures supported by endosseous implants: a literature review. → Int J Oral Maxillofac Implants. 1998 Jul;13(4):539–45. The McGill consensus statement in 20027Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S, Head T, Heydecke G, Lund JP, MacEntee M, Mericske-Stern R, Mojon P, Morais JA, Naert I, Payne AG, Penrod J, Stoker GT, Tawse-Smith A, Taylor TD, Thomason JM, Wismeijer D. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. → Gerodontology. 2002 Jul;19(1):3–4.’ 8Thomason JM, Kelly SA, Bendkowski A, Ellis JS. Two implant retained overdentures –A review of the literature supporting theMcGill and York consensus statements. → J Dent. 2012 Jan;40(1):22–34. and some independent studies9Harris D, Höfer S, O’Boyle CA, Sheridan S, Marley J, Benington IC, Clifford T, Houston F, O’Connell B. A comparison of implant-retained mandibular overdentures and conventional dentures on quality of life in edentulous patients: a randomized, prospective, within-subject controlled clinical trial. → Clin Oral Implants Res. 2013 Jan;24(1):96–103.10Emami E, Heydecke G, Rompré PH, De Grandmont P, Feine JS. Impact of implant support for mandibular dentures on satisfaction, oral and general health-related quality of life: a meta-analysis of randomized-controlled trials. → Clin Oral Implants Res. 2009 Jun;20(6):533–44.)11Krennmair G, Seemann R, Fazekas A, Ewers R,Piehslinger E. Patient preference and satisfaction with implant-supported mandibular overdentures retained with ball or locator attachments: a crossover clinical trial. → Int J Oral Maxillofac Implants. 2012 Nov-Dec;27(6):1560–8. state that mandibular two-implant overdentures are the gold standard for edentulous patients. However, technical and biological complications can occur.12Jemt T. Failures and complications in 391 consecutively inserted fixed prostheses supported by Brånemark implants in edentulous jaws: a study of treatment from the time of prosthesis placement to the first annual checkup. → Int J Oral Maxillofac Implants. 1991 Fall;6(3):270–6.13Jemt T, Book K, Lindén B, Urde G. Failures and complications in 92 consecutively inserted overdentures supported by Brånemark implants in severely resorbed edentulous maxillae: a study from prosthetic treatment to first annual check-up. → Int J Oral Maxillofac Implants. 1992 Summer;7(2):162–7.14French D, Tallarico M. Eight-year clinical and radiologic results of maxillary and mandibular implant-retained bar overdentures carried out on oxidized (TiUnite™) replace select implants placed in regenerated bone: a clinical case. → Quintessence Int. 2014 Feb;45(2):135–40.15Babbush CA, Tallarico M. Twelve-year clinical and radiological results of maxillary and mandibular implant-retained bar overdentures carried out on oxidized (TiUnite) replace select implants: a clinical case. → J Oral Implantol. 2013 Dec;39(6):737–42.
In two pilot retrospective studies, Maló et al. presented a planning protocol for the rehabilitation of the edentulous mandible and maxilla using four implants (All-on-4, Nobel Biocare, Kloten, Switzerland) to overcome anatomical limitations in the mandible that make it challenging to treat without the use of more complex techniques.16Maló P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:2–9.’ 17Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark System® implants for completely edentulous maxillae: a 1-year retrospective clinical study. → Clin Implant Dent Relat Res. 2005 Jun;7 Suppl 1:S88–94. The two most anterior implants are placed axially, and the posterior implants are placed in an angled position to maximize implant length and avoid anatomical structures (i.e., the mental nerve and anterior border of the maxillary sinus). The All-on-4 treatment concept seems to be a safe, effective and efficient surgical and prosthetic procedure on both jaws after ten years in function.18Malo P, de Araújo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. → J Am Dent Assoc. 2011 Mar;142(3):310–20.’ 19Maló P, de Araújo Nobre M, Lopes A, Francischone C, Rigolizzo M. “All-on-4” immediate-function concept for completely edentulous maxillae: a clinical report on the medium (3 years) and long-term (5 years) outcomes. → Clin Implant Dent Relat Res. 2012 May;14 Suppl 1:e139–50. However, as confirmed in a recent systematic review, few independent uncontrolled prospective and retrospective studies have confirmed these preliminary results.20Patzelt SB, Bahat O, Reynolds MA, Strub JR. The all-on-four treatment concept: a systematic review. → Clin Implant Dent Relat Res. 2014 Dec;16(6):836–55.
The purpose of this prospective observational study was to evaluate the three-year clinical and radiographic outcomes of implant-supported complete-arch fixed dental prostheses (FDPs) delivered on four implants placed according to the All-on-4 protocol in edentulous or partially edentate patients with a preference for an implant-supported restoration. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.21Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. → J Clin Epidemiol. 2008 Apr;61(4):344–9.
Materials and methods
This prospective observational study was designed to evaluate patients treated according to the All-on-4 protocol in the mandible or maxilla. The patients were selected and treated in two private centers in Rome and Sassari, between January 2008 and December 2011.
The inclusion criteria were a healthy patient aged 18 years or older at the time of implant placement, able to give her or his informed consent for participation, with a residual alveolar crest, distal to the first premolar, of ≤ 5 mm in height and ≤ 4 mm in width, assessed by computed tomography (CT) or scans, and refusal of a conventional bone augmentation procedure; partially edentate patient with hopeless dentition based on multiple risk factors, including endodontic22Zitzmann NU, Krastl G, Hecker H, Walter C, Weiger R. Endodontics or implants? A review of decisive criteria and guidelines for single tooth restorations and full arch reconstructions. → Int Endod J. 2009 Sep;42(9):757–74. and periodontal criteria,23Becker W, Berg L, Becker BE. The long term evaluation of periodontal treatment and maintenance in 95 patients. → Int J Periodontics Restorative Dent. 1984;4(2)54–71. prosthetic restorability of the tooth, cost–benefit ratio and patient preference in terms of refusing any major bone augmentation procedures.
The exclusion criteria were general medical (American Society of Anesthesiologists Physical Status Class III or IV) and/or psychiatric contraindications; pregnancy or nursing; any interfering medication, such as steroid therapy or bisphosphonate therapy; alcohol or drug abuse; heavy smoking (> 10 cigarettes/day); radiation therapy to the head or neck region within five years; high or moderate parafunctional activity; untreated periodontitis; poor oral hygiene and motivation, defined as full-mouth bleeding on probing and a full-mouth plaque index of ≥ 25%; known allergic or adverse reactions to the restorative material; and unavailability for regular follow-ups.
This investigation was conducted according to the principles embodied in the Declaration of Helsinki of 1975 for biomedical research involving human subjects, as amended in 2008. All of patients were duly informed about the nature of the study and gave their written consent.
Before implant placement, all of the patients underwent CT or CBCT scan according to a double-scan protocol.24Van Steenberghe D, Naert I, Andersson M, Brajnovic I, Van Cleynenbreugel J, Suetens P. A custom template and definitive prosthesis allowing immediate implant loading in the maxilla: a clinical report. → Int J Oral Maxillofac Implants. 2002 Sep-Oct;17(5):663–70. In the case of immediately post-extraction implants, a previously reported two-piece radiographic guide was used for the diagnostic study and for virtual implant planning.25Polizzi G, Cantoni T. Five-year follow-up of immediate fixed restorations of maxillary implants inserted in both fresh extraction and healed sites using the NobelGuide™ system. → Clin Implant Dent Relat Res. 2015 Apr;17(2):221–33.’ 26Cantoni T, Giovanni P. Implant treatment planning in fresh extraction sockets: use of a novel radiographic guide and CAD/CAM technology. → Quintessence Int. 2009 Oct;40(9):773–81. If the operator decided to wait for healing of the post-extraction socket, the implant sites had to heal for at least three months before radiographic examination (Figs. 1–2).
DICOM data of the two sets of scans were transferred to a 3-D software planning program (NobelGuide, Nobel Biocare) and matched to each other. Four implants were planned for the rehabilitation of each participant in post-extraction or healed sockets, according to the All-on-4 protocol.27Maló P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:2–9.’ 28Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark System® implants for completely edentulous maxillae: a 1-year retrospective clinical study. → Clin Implant Dent Relat Res. 2005 Jun;7 Suppl 1:S88–94. Planning data of the patients who required template-guided surgery were sent to a milling center (NobelProcera, Nobel Biocare), where stereolithographic surgical templates with hollow metallic cylinders to guide implant placement in the virtually planned position were fabricated. Patients received professional oral hygiene prior to the surgery and were instructed to rinse with a 0.2% chlorhexidine mouthwash for 1 min, starting two days prior to the intervention.
-

- Fig. 1 Pretreatment intra-oral photograph.
-

- Fig. 2 Intra-oral photograph three months after tooth extractions.
-

- Fig. 3 Try-in of the dental set-up modeled on the established vertical dimension of occlusion according to functional and esthetic parameters.
-

- Fig. 4 Screw-retained temporary restoration.
-

- Fig. 5 Intra-oral photograph of the temporary restoration screwed onto the implants.
-

- Fig. 6 Intra-oral photograph five days after flapless implant placement.
 Fig. 7 Periapical radiographs five days after implant placement.
Fig. 7 Periapical radiographs five days after implant placement.Surgical protocol
An antibiotic (2 g of amoxicillin and clavulanic acid or 600 mg clindamycin if allergic to penicillin) was administered 1 h prior to surgery and continued for six days (1 g amoxicillin and clavulanic acid or 300 mg clindamycin b.i.d.) after surgery. Local anesthesia was induced using a 4% articaine solution with 1:100,000 epinephrine (Ubistesin; 3M Italia, Milan, Italy). Implants were placed in the planned anatomical sites either conventionally or using a fully guided approach. A flapless or a flap approach was performed in order to maintain an adequate residual band of keratinized mucosa around the implants. When the alveolar crest was too thin (knife edge) to place the implant, the alveolar crest was remodeled using piezoelectric bone surgery under copious irrigation with sterile saline to obtain a flat bony crest. Each patient received four NobelSpeedy Groovy implants (Nobel Biocare), featuring a flat-to-flat matched implant-abutment interface with a 0.7 mm tall external hexagonal prosthetic connection and a rough, highly crystalline and phosphate-enriched titanium oxide surface (TiUnite, Nobel Biocare). All of the implants were placed according to the surgical and prosthetic protocols recommended by the manufacturer (IFU 73494 Manual 2/All-on-4 and IFU 71286), with no deviations from the original protocol. The drilling sequence was chosen according to the manufacturer’s instructions in relation to the bone quality, achieving an insertion torque at implant placement ranging from 35 to 45 N cm in the mandible or from 35 to 55 N cm in the maxilla, measured using a surgical unit (OsseoCare Pro Drill Motor Set, Nobel Biocare). In the post-extraction sites, the gaps between the implants and the surrounding socket walls were filled with 0.25–1 mm granules of deproteinized bovine bone (Geistlich Bio-Oss or Geistlich Bio-Oss Collagen, Geistlich Pharma, Wolhusen, Switzerland), hydrated using the patient’s blood mixed with antibiotic solution (Rifocin 250 mg/10 mL, Sanofi-aventis, Milan, Italy).
Seventeen- or thirty-degree angled multi-unit abutments (Nobel Biocare) were immediately connected to the distal implants for better orientation of the screw access hole. Straight multi-unit abutments (Nobel Biocare) were used in the anterior implants if needed.
A prefabricated screw-retained acrylic resin provisional restoration without any cantilever was delivered immediately after surgery (Figs. 3–5). All of the patients received oral and written recommendations regarding medication, oral hygiene maintenance and diet. Post-surgical analgesic treatment was provided with ibuprofen 600 mg, administered every 8 h for two days after the surgery, and later on if needed. The patients were instructed to rinse the mouth with a 0.2% chlorhexidine mouthwash t.i.d. without brushing the implant area (Figs. 6 & 7).
Prosthetic protocol
After three to four months of healing, a definitive impression was taken at the implant or abutment level according to a previously reported protocol.29Pozzi A, Tallarico M, Mangani F, Barlattani A. Different implant impression techniques for edentulous patients treated with CAD/CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading. → Eur J Oral Implantol. 2013 Winter;6(4):325–40. Definitive prostheses with titanium or zirconia frameworks, fabricated using CAD/CAM technology (NobelProcera), were screwed on at either the implant or abutment level according to the manufacturer’s instructions three to five months after implant placement (in the mandible and the maxilla, respectively). The definitive implant-supported complete-arch FDP was designed with (hybrid design) or without pink material in the cervical region (crown design) and veneered with ceramic, acrylic or composite according to the patients’ needs (Figs. 8a–c). Clinical accuracy of the framework (strain-free screwing and absence of an open margin upon clinical and radiographic examination) was evaluated before prosthesis delivery.30Abduo J, Bennani V, Waddell N, Lyons K, Swain M. Assessing the fit of implant fixed prostheses: a critical review. → Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):506–15.31Eisenmann E, Mokabberi A, Walter MH, Freesmeyer WB. Improving the fit of implant-supported superstructures using the spark erosion technique. → Int J Oral Maxillofac Implants. 2004 Nov-Dec;19(6):810–8.32Katsoulis J, Mericske-Stern R, Rotkina L, Zbären C, Enkling N, Blatz MB. Precision of fit of implant-supported screw-retained 10-unit computer-aided-designed and computeraided- manufactured frameworks made from zirconium dioxide and titanium: an in vitro study. → Clin Oral Implants Res. 2014 Feb;25(2):165–74. The occlusion was adjusted avoiding any premature contacts. Mutually protected occlusion with anterior guidance or balanced occlusion was used in cases of opposing natural dentition or an FDP and complete removable denture, respectively. Follow-up visits were scheduled at one and six months and then annually up to five years of function. The patients underwent a professional cleaning by a dental hygienist every four to six months (Figs. 9a–c). Panoramic and periapical radiographs were obtained annually after definitive prosthesis delivery (Fig. 10).






Figs. 9a-c Lateral (a & c) and frontal (b) intra-oral photographs of the definitive prosthesis taken three years after implant placement.
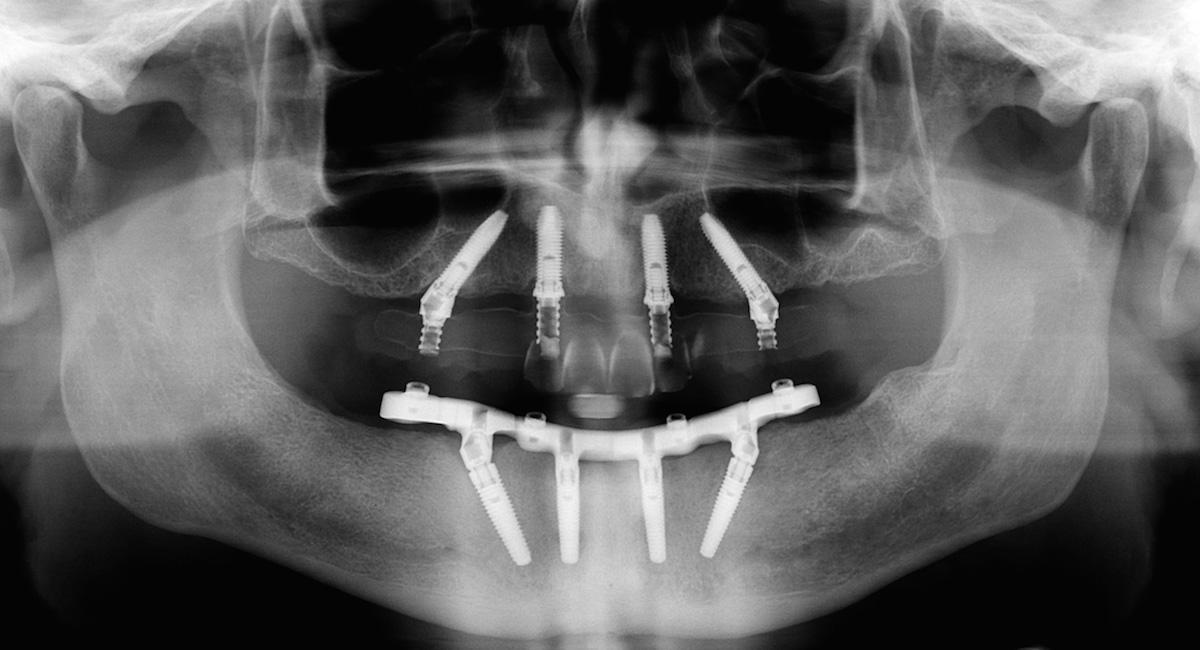 Fig. 10 Panoramic radiograph three years after implant placement.
Fig. 10 Panoramic radiograph three years after implant placement.The primary outcome measures were as follows:
- An implant was classified as “successful” when the following criteria33Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: a systematic review. → J Dent Res. 2012 Mar;91(3):242–8. were fulfilled: did not cause pain or suppuration, did not show any mobility, did not show any signs of radiolucency, and did not show periimplant bone loss of > 1.5 mm during the first year and then > 0.2 mm yearly.
- An implant was classified as “surviving” when the implant remained in the jaw and was stable after the prosthesis was removed, even though all of the success criteria were not fulfilled.
- An implant-supported complete-arch FDP was defined as “successful” when the dental prosthesis remained in function and the esthetic evaluation, assessed by the dentist and the patient, was satisfactory during the study period.
- An implant-supported complete-arch FDP was considered as “surviving” when the dental prosthesis remained in function, even though all of the success criteria were not fulfilled.
The secondary outcome measures were as follows:
- Any technical (fracture of the framework and/ or the veneering material, screw loosening, etc.) and/or biological (pain, swelling, suppuration, etc.) complications were considered.
- The distance from the most coronal margin of the implant collar and the most coronal point of bone-to-implant contact was taken as the marginal bone level. This level was evaluated on intra-oral digital radiographs taken with the paralleling technique using a film holder (Rinn XCP, DENTSPLY, Elgin, Ill., U.S.) at implant placement (baseline) and then yearly up to three years of function. Radiographs were accepted or rejected for evaluation based on the clarity of the implant threads. All readable radiographs were displayed in image analysis software (Digora for Windows 2.8, SOREDEX, Tuusula, Finland) that was calibrated for every single image using the known measure of the implant thread pitch. Measurements of the mesial and distal bony crest level adjacent to each implant were made to the nearest 0.1 mm and averaged at the patient level.
- Patient satisfaction was evaluated with a questionnaire one month after delivery of the final prosthesis and at the three-year follow-up examination, provided by independent and blinded outcome assessors. The assessor asked the following questions: Are you satisfied with the function of your implant-supported prosthesis? Are you satisfied with the esthetic outcome of your implant-supported prosthesis? Would you undergo the same therapy again?
An independent assessor evaluated the implant and prosthesis survival and success rates. Complications were assessed and treated by the same clinicians. The marginal bone loss was evaluated by an independent radiologist.
Statistical Analysis
Patient data were collected in an Excel spreadsheet (Microsoft). Finally, all of the data were exported into IBM SPSS Statistics for Macintosh (Version 22.0; IBM, Armonk, N.Y., U.S.) for statistical analysis. A bio-statistician with expertise in dentistry analyzed the data using PASW Statistics for Windows (Version 18.0; SPSS, Chicago, Ill., U.S.). Descriptive analysis was performed for numeric parameters using mean ± standard deviation (median; 95% CI). Dichotomous and continuous outcomes were compared using the chisquared test and one-way analysis of variance, respectively. Differences in the proportions of patients with implant failures, prosthesis failures and complications (dichotomous outcomes) were compared between the subgroups using the Fisher exact test. Patient was the statistical unit of the analyses. All statistical comparisons were conducted at a 0.05 level of significance.
Results
Thirty-two patients were screened for eligibility. Two patients were not enrolled in the trial, because of refusal to sign the informed consent. A total of 120 NobelSpeedy Groovy implants were placed using either computer-assisted template-guided (n = 15) or conventional freehand surgery (n = 15) in 30 consecutive patients (18 females and 12 males) with a mean age of 67.4 ± 6.9 (range of 51–87). Thirty CAD/CAM screw-retained implant-supported complete-arch FDPs (18 in the mandible and 12 in the maxilla) were delivered. No patients dropped out of the study within three years after implant placement and no deviation from the original protocol occurred. All of the patients were followed up for a minimum period of three years (mean of 53.8 months; range of 36–84 months). Data collected were included in the statistical analysis. The main patients’ and interventions’ characteristics are summarized in Table 1. At the three-year follow-up examination, one out of 120 implants (0.8%) had failed, resulting in a cumulative implant survival rate of 99.2%. The only implant failure occurred in one patient two months after placement, before delivery of the final prosthesis. The affected implant had an infectious etiology (pain, swelling and suppuration) and it was 11.5 mm long in position 16, placed using guided surgery in a healed site. The implant was replaced three months after bone healing. The temporary prosthesis was shortened, but not replaced by a conventional complete removable denture, and the patient was adequately informed and instructed to pay attention and follow a soft diet. At the three-year follow-up examination, no definitive prostheses had failed, resulting in a cumulative prosthesis survival rate of 100%.
Eleven patients experienced one technical or biological complication each, resulting in eight technical and three biological complications reported during the entire follow-up period. Six technical and one biological complication were reported during the healing period with temporary prostheses, while two technical and two biological complications were reported after definitive prosthesis delivery. All of the complications were successfully resolved.
Three prosthetic screws loosened in the temporary prostheses (in three patients) during the healing period, and this was resolved by retightening the screws, stabilizing the occlusion and advising the patients not to overload the prostheses (not to ingest food that may require significant masticatory effort). Three fractures of the provisional acrylic prostheses occurred (in three patients) during the healing period. The temporary prosthesis was adjusted chairside, the occlusion was stabilized and a night guard was delivered for each patient. Fracture of the composite veneering material of the definitive implant-supported cross-arch FDP occurred in one patient two years after loading, most likely due to occasional parafunctional habits. These situations were resolved by adjusting the definitive prosthesis chairside, stabilizing the occlusion and a delivering a night guard.
The first biological complication was reported six weeks after implant placement in an 11.5 mm long implant placed in position 45, using guided surgery in a healed site. The patient reported pain and swelling without suppuration. The temporary abutment was replaced with a healing abutment. The temporary prosthesis was shortened to the right canine. The implant was left to heal for four months according to a conventional loading protocol. The other two complications were periimplantitis, consisting of a mean mesiodistal periimplant bone loss of 2.6 and 2.8 mm, reported at the one-year follow-up examination. The first case of periimplantitis developed around a 15 mm long implant in position 35, placed using conventional freehand surgery in a healed site. The second case developed around a 13 mm long implant in position 32, placed using guided surgery in a healed site and immediately loaded. No other technical or biological complications occurred during the entire follow-up period.
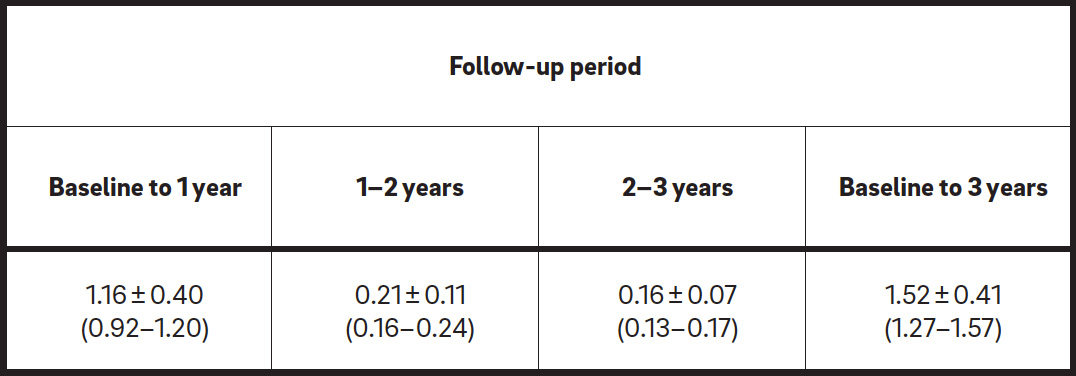
After an initial mean marginal bone loss of 1.16 ± 0.40 mm (1.06 mm; 95% CI: 0.92–1.20), all of the implants lost a mean of 0.21 ± 0.11 mm (0.20 mm; 95% CI: 0.16–0.24) between the oneand two-year follow-ups, and 0.16 ± 0.07 mm (0.15 mm; 95% CI: 0.13–0.17) between the twoand three-year follow-ups. At the three-year follow-up, the mean marginal bone loss was 1.52 ± 0.41 mm (1.42 mm; 95% CI: 1.27–1.57). The radiographic data are shown in Table 2.
All of the patients were fully satisfied with the function and esthetics of their definitive prostheses, and all of the patients declared that they would undergo the same treatment again.
Maxilla versus mandible
Twelve patients were treated in the maxilla, while 18 patients were treated in the mandible. There were no statistically significant differences between centers for the number of patients who had failed implants (1/12 vs. 0/18; risk ratio = NA; p = 0.399) or complications (3/12 vs. 8/18; risk ratio = 0.5625; 95% CI: 0.19–1.70; p = 0.442). At the three-year follow-up examination, the mean marginal bone loss was 1.49 ± 0.34 mm (1.42 mm; 95% CI: 1.23–1.61) in the maxilla versus 1.54 ± 0.46 mm (1.38 mm; 95% CI: 1.17–1.59) in the mandible (p = 0.756). The radiographic data are shown in Table 3.
Guided versus conventional freehand surgery
Fifteen patients were treated using computer-assisted template-based surgery and 15 with conventional freehand surgery. There were no statistically significant differences between centers for the number of patients who had failed implants (1/15 vs. 0/15; risk ratio = NA; p = 0.999) or complications (4/15 vs. 7/15; risk ratio = 0.5714; 95% CI: 0.21–1.55; p = 0.449). At the three-year follow-up examination, the mean marginal bone loss was 1.48 ± 0.47 mm (1.33 mm; 95% CI: 1.09–1.57) in the guided surgery group versus 1.55 ± 0.34 mm (1.46 mm; 95% CI: 1.29–1.63) in the conventional freehand surgery group (p = 0.365). The radiographic data are shown in Table 3.

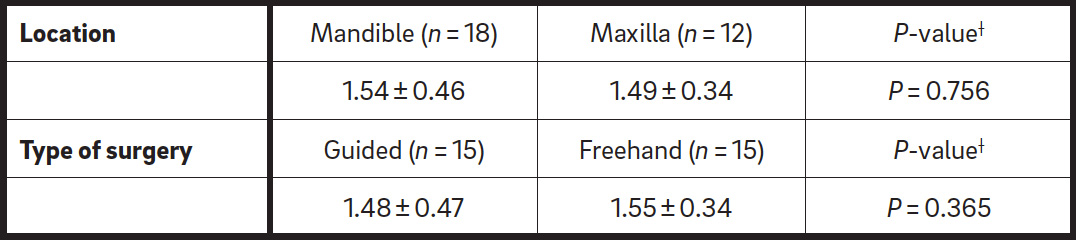
† Unpaired t-test assuming normal distribution.
Discussion
The present study reported data on 30 implant-supported restorations delivered according to the All-on-4 protocol and followed for at least three years after implant placement. Because it was designed as a single-cohort prospective study, the main limitation of the present research was the lack of a control group and the small sample size. Another limitation of the present study was the variability within the cohort of patients. In the present study, the three-year implant (99.2%) and prosthesis success rates (100.0%), as well as the mean bone loss of 1.52 ± 0.41 mm, indicate that the All-on-4 treatment concept is a promising treatment modality. Furthermore, the results of this prospective observational study are consistent with other studies investigating the same topic.
A recent systematic review by Patzelt et al., which included 4,804 implants, demonstrated a mean cumulative implant and prosthesis survival rate at three years of 99.0 ± 1.0% and 99.9 ± 0.3%, respectively.34Patzelt SB, Bahat O, Reynolds MA, Strub JR. The all-on-four treatment concept: a systematic review. → Clin Implant Dent Relat Res. 2014 Dec;16(6):836–55. The mean bone loss at three years amounted to 1.3 ± 0.4 mm. However, 12 out of the 13 included studies were considered to be highly biased. Most of the studies included (69%) in the systematic review derived from a limited number of investigators in Italy and Portugal, which may limit the generalizability of the findings, and only 31 % of the studies reported a completed follow-up period of three years.
Malo et al. retrospectively reported a cumulative patient-related success rate of 93.8% up to ten years of follow-up in the mandible and a prosthesis survival rate of 99.2%.35Malo P, de Araújo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. → J Am Dent Assoc. 2011 Mar;142(3):310–20. In the maxilla, a five-year survival rate of 93% was reported, and the survival rate of the prostheses was 100%.36Maló P, de Araújo Nobre M, Lopes A, Francischone C, Rigolizzo M. “All-on-4” immediate-function concept for completely edentulous maxillae: a clinical report on the medium (3 years) and long-term (5 years) outcomes. → Clin Implant Dent Relat Res. 2012 May;14 Suppl 1:e139–50. The mean marginal bone loss was 1.52 ± 0.30 mm after three years. Similar results were reported by Browaeys et al., who highlighted unacceptable ongoing bone loss in 49.2% of the patients.37Browaeys H, Dierens M, Ruyffelaert C, Matthijs C, De Bruyn H, Vandeweghe S. Ongoing crestal bone loss around implants subjected to computer-guided flapless surgery and immediate loading using the All-on-4® concept. → Clin Implant Dent Relat Res. 2015 Oct;17(5):831–43.
Balshi et al. retrospectively analyzed the outcomes of 200 arches (800 implants) treated according to the All-on-4 protocol.38Balshi TJ, Wolfinger GJ, Slauch RW, Balshi SF. A retrospective analysis of 800 Brånemark System implants following the All-on-Four™ protocol. → J Prosthodont. 2014 Feb;23(2):83–8. Twenty percent (168 implants out of 800) of the implants analyzed had a follow-up period of three years or more. Cumulative implant and prosthesis survival rates amounted to 97.3% and 99.0%, respectively.
Grandi et al. analyzed 47 patients treated with 188 immediately loaded implants placed in the mandible according to the All-on-4 protocol in post-extraction sites.39Grandi T, Guazzi P, Samarani R, Grandi G. Immediate loading of four (All-on-4) post-extractive implants supporting mandibular cross-arch fixed prostheses: 18-month follow-up from a multicentre prospective cohort study. → Eur J Oral Implantol. 2012 Autumn;5(3):277–85. At the 18-month follow- up, no implant had failed and all of the restorations were stable. However, three patients experienced fracture of the provisional restoration. No significant differences in bone loss were found between axially placed and tilted implants at the 18-month follow-up.
Babbush et al. retrospectively examined 165 patients treated according to the All-on-4 protocol.40Babbush CA, Kutsko GT, Brokloff J. The All-on-Four immediate function treatment concept with NobelActive implants: a retrospective study. → J Oral Implantol. 2011 Aug;37(4):431–45. The cumulative implant survival rate was 99.6% (99.3% in the maxilla and 100.0% in the mandible) for up to 29 months of loading. The definitive prosthesis survival rate was 100%. Recently, the same authors retrospectively analyzed the patient-centered outcomes, including the cost of treatment, length of the treatment period and comfort provided by the provisional restoration, in patients treated according to the All-on-4 protocol and compared these results to a historical control group, which included complete- arch FDPs supported by natural teeth or implants and implant-supported overdentures.41Babbush CA, Kanawati A, Kotsakis GA, Hinrichs JE. Patient-related and financial outcomes analysis of conventional full-arch rehabilitation versus the All-on-4 concept: a cohort study. → Implant Dent. 2014 Apr;23(2):218–24. This study demonstrated that the cost, length of treatment and comfort provided by the provisional restoration significantly favored the All-on-4 treatment modality.
In the present study, the overall percentage of complications experienced was large (36.6 %). Nevertheless, this result did not differ from those normally encountered in oral rehabilitation in which implants are used as support for an FDP (33.6% at five years).42Schwarz F, Hegewald A, Becker J. Impact of implant-abutment connection and positioning of the machined collar/microgap on crestal bone level changes: a systematic review. → Clin Oral Implants Res. 2014 Apr;25(4):417–25. Moreover, most of these complications were reported on the temporary restoration, during healing. The clinicians who carried out the procedures addressed all of the complications chairside. Furthermore, the condition of the patients remained stable up to the completion of the three-year follow-up period. In order to minimize the incidence of complications, dental clinicians should exert great effort in selecting patients, respecting the original protocols, and choosing reliable components and materials for implant-supported complete-arch FDPs.
Patients with untreated periodontitis were not included in the study. Implant therapy in patients with a history of chronic periodontitis and generalized aggressive periodontitis might be considered a viable treatment with similar survival outcomes to those reported for healthy patients. Periodontally compromised patients were included after being treated to reduce the inflammation and halt the disease progression, before tooth extraction and implant placement. According to Donos et al., it is necessary to treat and control the periodontal disease, regardless of its progression pattern and subtype, before implant therapy is initiated in order to improve the overall implant success and achieve a more favorable bone resorption pattern.((Donos N, Laurell L, Mardas N. Hierarchical decisions on teeth vs. implants in the periodontitis-susceptible patient: the modern dilemma. → Periodontol 2000. 2012 Jun;59(1):89–110. Nevertheless, a comprehensive implant maintenance program has to be encouraged and continued in order to identify periimplant bone loss early on, particularly in patients with a history of periodontal disease.
Conclusion
Within the limitations of the present study, the All-on-4 concept is a predictable and minimally invasive treatment concept for the complete-arch rehabilitation of both jaws, regardless of jaw location and type of surgery. It may decrease the overall treatment time and re-establish adequate function in a cost-effective way. Further longterm prospective data (five years and more) and outcomes beyond cumulative survival rates are needed.
Competing interests
The authors declare that they have no competing interests. This study was completely self-financed and no funding was sought or obtained, not even in the form of free materials.
References
| 1. | ↑ | Polzer I, Schimmel M, Müller F, Biffar R. Edentulism as part of the general health problems of elderly adults. → Int Dent J. 2010 Jun;60(3):143–55. |
| 2. | ↑ | Emami E, de Souza RF, Kabawat M, Feine JS. The impact of edentulism on oral and general health. → Int J Dent. 2013;2013:498305. doi: 10.1155/2013/498305. Epub 2013 May 8. |
| 3. | ↑ | Slade GD, Akinkugbe AA, Sanders AE. Projections of U.S. edentulism prevalence following 5 decades of decline. → J Dent Res. 2014 Oct;93(10):959–65. |
| 4. | ↑ | Felton D, Cooper L, Duqum I, Minsley G, Guckes A, Haug S, Meredith P, Solie C, Avery D, Chandler ND; American College of Prosthodontists; Academy of General Dentistry; American Dental Association Council on Scientific Affairs; American Dental Hygienists’ Association; National Association of Dental Laboratories; GlaxoSmithKline Consumer Healthcare. Evidence-based guidelines for the care and maintenance of complete dentures: a publication of the American College of Prosthodontists. → J Am Dent Assoc. 2011 Feb;142 Suppl 1:1S–20S. |
| 5. | ↑ | Carlsson GE. Clinical morbidity and sequelae of treatment with complete dentures. → J Prosthet Dent. 1998 Jan;79(1):17–23. |
| 6. | ↑ | Batenburg RH, Meijer HJ, Raghoebar GM, Vissink A. Treatment concept for mandibular overdentures supported by endosseous implants: a literature review. → Int J Oral Maxillofac Implants. 1998 Jul;13(4):539–45. |
| 7. | ↑ | Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S, Head T, Heydecke G, Lund JP, MacEntee M, Mericske-Stern R, Mojon P, Morais JA, Naert I, Payne AG, Penrod J, Stoker GT, Tawse-Smith A, Taylor TD, Thomason JM, Wismeijer D. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. → Gerodontology. 2002 Jul;19(1):3–4. |
| 8. | ↑ | Thomason JM, Kelly SA, Bendkowski A, Ellis JS. Two implant retained overdentures –A review of the literature supporting theMcGill and York consensus statements. → J Dent. 2012 Jan;40(1):22–34. |
| 9. | ↑ | Harris D, Höfer S, O’Boyle CA, Sheridan S, Marley J, Benington IC, Clifford T, Houston F, O’Connell B. A comparison of implant-retained mandibular overdentures and conventional dentures on quality of life in edentulous patients: a randomized, prospective, within-subject controlled clinical trial. → Clin Oral Implants Res. 2013 Jan;24(1):96–103. |
| 10. | ↑ | Emami E, Heydecke G, Rompré PH, De Grandmont P, Feine JS. Impact of implant support for mandibular dentures on satisfaction, oral and general health-related quality of life: a meta-analysis of randomized-controlled trials. → Clin Oral Implants Res. 2009 Jun;20(6):533–44.)((Krennmair G, Seemann R, Fazekas A, Ewers R,Piehslinger E. Patient preference and satisfaction with implant-supported mandibular overdentures retained with ball or locator attachments: a crossover clinical trial. → Int J Oral Maxillofac Implants. 2012 Nov-Dec;27(6):1560–8. |
| 11. | ↑ | Krennmair G, Seemann R, Fazekas A, Ewers R,Piehslinger E. Patient preference and satisfaction with implant-supported mandibular overdentures retained with ball or locator attachments: a crossover clinical trial. → Int J Oral Maxillofac Implants. 2012 Nov-Dec;27(6):1560–8. state that mandibular two-implant overdentures are the gold standard for edentulous patients. However, technical and biological complications can occur.((Jemt T. Failures and complications in 391 consecutively inserted fixed prostheses supported by Brånemark implants in edentulous jaws: a study of treatment from the time of prosthesis placement to the first annual checkup. → Int J Oral Maxillofac Implants. 1991 Fall;6(3):270–6. |
| 12. | ↑ | Jemt T. Failures and complications in 391 consecutively inserted fixed prostheses supported by Brånemark implants in edentulous jaws: a study of treatment from the time of prosthesis placement to the first annual checkup. → Int J Oral Maxillofac Implants. 1991 Fall;6(3):270–6.((Jemt T, Book K, Lindén B, Urde G. Failures and complications in 92 consecutively inserted overdentures supported by Brånemark implants in severely resorbed edentulous maxillae: a study from prosthetic treatment to first annual check-up. → Int J Oral Maxillofac Implants. 1992 Summer;7(2):162–7. |
| 13. | ↑ | Jemt T, Book K, Lindén B, Urde G. Failures and complications in 92 consecutively inserted overdentures supported by Brånemark implants in severely resorbed edentulous maxillae: a study from prosthetic treatment to first annual check-up. → Int J Oral Maxillofac Implants. 1992 Summer;7(2):162–7.((French D, Tallarico M. Eight-year clinical and radiologic results of maxillary and mandibular implant-retained bar overdentures carried out on oxidized (TiUnite™) replace select implants placed in regenerated bone: a clinical case. → Quintessence Int. 2014 Feb;45(2):135–40. |
| 14. | ↑ | French D, Tallarico M. Eight-year clinical and radiologic results of maxillary and mandibular implant-retained bar overdentures carried out on oxidized (TiUnite™) replace select implants placed in regenerated bone: a clinical case. → Quintessence Int. 2014 Feb;45(2):135–40.((Babbush CA, Tallarico M. Twelve-year clinical and radiological results of maxillary and mandibular implant-retained bar overdentures carried out on oxidized (TiUnite) replace select implants: a clinical case. → J Oral Implantol. 2013 Dec;39(6):737–42. |
| 15. | ↑ | Babbush CA, Tallarico M. Twelve-year clinical and radiological results of maxillary and mandibular implant-retained bar overdentures carried out on oxidized (TiUnite) replace select implants: a clinical case. → J Oral Implantol. 2013 Dec;39(6):737–42.
In two pilot retrospective studies, Maló et al. presented a planning protocol for the rehabilitation of the edentulous mandible and maxilla using four implants (All-on-4, Nobel Biocare, Kloten, Switzerland) to overcome anatomical limitations in the mandible that make it challenging to treat without the use of more complex techniques.((Maló P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:2–9. |
| 16. | ↑ | Maló P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:2–9.’ ((Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark System® implants for completely edentulous maxillae: a 1-year retrospective clinical study. → Clin Implant Dent Relat Res. 2005 Jun;7 Suppl 1:S88–94. |
| 17. | ↑ | Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark System® implants for completely edentulous maxillae: a 1-year retrospective clinical study. → Clin Implant Dent Relat Res. 2005 Jun;7 Suppl 1:S88–94. The two most anterior implants are placed axially, and the posterior implants are placed in an angled position to maximize implant length and avoid anatomical structures (i.e., the mental nerve and anterior border of the maxillary sinus). The All-on-4 treatment concept seems to be a safe, effective and efficient surgical and prosthetic procedure on both jaws after ten years in function.((Malo P, de Araújo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. → J Am Dent Assoc. 2011 Mar;142(3):310–20. |
| 18. | ↑ | Malo P, de Araújo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. → J Am Dent Assoc. 2011 Mar;142(3):310–20.’ ((Maló P, de Araújo Nobre M, Lopes A, Francischone C, Rigolizzo M. “All-on-4” immediate-function concept for completely edentulous maxillae: a clinical report on the medium (3 years) and long-term (5 years) outcomes. → Clin Implant Dent Relat Res. 2012 May;14 Suppl 1:e139–50. |
| 19. | ↑ | Maló P, de Araújo Nobre M, Lopes A, Francischone C, Rigolizzo M. “All-on-4” immediate-function concept for completely edentulous maxillae: a clinical report on the medium (3 years) and long-term (5 years) outcomes. → Clin Implant Dent Relat Res. 2012 May;14 Suppl 1:e139–50. However, as confirmed in a recent systematic review, few independent uncontrolled prospective and retrospective studies have confirmed these preliminary results.((Patzelt SB, Bahat O, Reynolds MA, Strub JR. The all-on-four treatment concept: a systematic review. → Clin Implant Dent Relat Res. 2014 Dec;16(6):836–55. |
| 20. | ↑ | Patzelt SB, Bahat O, Reynolds MA, Strub JR. The all-on-four treatment concept: a systematic review. → Clin Implant Dent Relat Res. 2014 Dec;16(6):836–55.
The purpose of this prospective observational study was to evaluate the three-year clinical and radiographic outcomes of implant-supported complete-arch fixed dental prostheses (FDPs) delivered on four implants placed according to the All-on-4 protocol in edentulous or partially edentate patients with a preference for an implant-supported restoration. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.((Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. → J Clin Epidemiol. 2008 Apr;61(4):344–9. |
| 21. | ↑ | Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. → J Clin Epidemiol. 2008 Apr;61(4):344–9.
Materials and methodsThis prospective observational study was designed to evaluate patients treated according to the All-on-4 protocol in the mandible or maxilla. The patients were selected and treated in two private centers in Rome and Sassari, between January 2008 and December 2011. The inclusion criteria were a healthy patient aged 18 years or older at the time of implant placement, able to give her or his informed consent for participation, with a residual alveolar crest, distal to the first premolar, of ≤ 5 mm in height and ≤ 4 mm in width, assessed by computed tomography (CT) or scans, and refusal of a conventional bone augmentation procedure; partially edentate patient with hopeless dentition based on multiple risk factors, including endodontic((Zitzmann NU, Krastl G, Hecker H, Walter C, Weiger R. Endodontics or implants? A review of decisive criteria and guidelines for single tooth restorations and full arch reconstructions. → Int Endod J. 2009 Sep;42(9):757–74. |
| 22. | ↑ | Zitzmann NU, Krastl G, Hecker H, Walter C, Weiger R. Endodontics or implants? A review of decisive criteria and guidelines for single tooth restorations and full arch reconstructions. → Int Endod J. 2009 Sep;42(9):757–74. and periodontal criteria,((Becker W, Berg L, Becker BE. The long term evaluation of periodontal treatment and maintenance in 95 patients. → Int J Periodontics Restorative Dent. 1984;4(2)54–71. |
| 23. | ↑ | Becker W, Berg L, Becker BE. The long term evaluation of periodontal treatment and maintenance in 95 patients. → Int J Periodontics Restorative Dent. 1984;4(2)54–71. prosthetic restorability of the tooth, cost–benefit ratio and patient preference in terms of refusing any major bone augmentation procedures.
The exclusion criteria were general medical (American Society of Anesthesiologists Physical Status Class III or IV) and/or psychiatric contraindications; pregnancy or nursing; any interfering medication, such as steroid therapy or bisphosphonate therapy; alcohol or drug abuse; heavy smoking (> 10 cigarettes/day); radiation therapy to the head or neck region within five years; high or moderate parafunctional activity; untreated periodontitis; poor oral hygiene and motivation, defined as full-mouth bleeding on probing and a full-mouth plaque index of ≥ 25%; known allergic or adverse reactions to the restorative material; and unavailability for regular follow-ups. This investigation was conducted according to the principles embodied in the Declaration of Helsinki of 1975 for biomedical research involving human subjects, as amended in 2008. All of patients were duly informed about the nature of the study and gave their written consent. Before implant placement, all of the patients underwent CT or CBCT scan according to a double-scan protocol.((Van Steenberghe D, Naert I, Andersson M, Brajnovic I, Van Cleynenbreugel J, Suetens P. A custom template and definitive prosthesis allowing immediate implant loading in the maxilla: a clinical report. → Int J Oral Maxillofac Implants. 2002 Sep-Oct;17(5):663–70. |
| 24. | ↑ | Van Steenberghe D, Naert I, Andersson M, Brajnovic I, Van Cleynenbreugel J, Suetens P. A custom template and definitive prosthesis allowing immediate implant loading in the maxilla: a clinical report. → Int J Oral Maxillofac Implants. 2002 Sep-Oct;17(5):663–70. In the case of immediately post-extraction implants, a previously reported two-piece radiographic guide was used for the diagnostic study and for virtual implant planning.((Polizzi G, Cantoni T. Five-year follow-up of immediate fixed restorations of maxillary implants inserted in both fresh extraction and healed sites using the NobelGuide™ system. → Clin Implant Dent Relat Res. 2015 Apr;17(2):221–33. |
| 25. | ↑ | Polizzi G, Cantoni T. Five-year follow-up of immediate fixed restorations of maxillary implants inserted in both fresh extraction and healed sites using the NobelGuide™ system. → Clin Implant Dent Relat Res. 2015 Apr;17(2):221–33.’ ((Cantoni T, Giovanni P. Implant treatment planning in fresh extraction sockets: use of a novel radiographic guide and CAD/CAM technology. → Quintessence Int. 2009 Oct;40(9):773–81. |
| 26. | ↑ | Cantoni T, Giovanni P. Implant treatment planning in fresh extraction sockets: use of a novel radiographic guide and CAD/CAM technology. → Quintessence Int. 2009 Oct;40(9):773–81. If the operator decided to wait for healing of the post-extraction socket, the implant sites had to heal for at least three months before radiographic examination (Figs. 1–2).
DICOM data of the two sets of scans were transferred to a 3-D software planning program (NobelGuide, Nobel Biocare) and matched to each other. Four implants were planned for the rehabilitation of each participant in post-extraction or healed sockets, according to the All-on-4 protocol.((Maló P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:2–9. |
| 27. | ↑ | Maló P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:2–9.’ ((Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark System® implants for completely edentulous maxillae: a 1-year retrospective clinical study. → Clin Implant Dent Relat Res. 2005 Jun;7 Suppl 1:S88–94. |
| 28. | ↑ | Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark System® implants for completely edentulous maxillae: a 1-year retrospective clinical study. → Clin Implant Dent Relat Res. 2005 Jun;7 Suppl 1:S88–94. Planning data of the patients who required template-guided surgery were sent to a milling center (NobelProcera, Nobel Biocare), where stereolithographic surgical templates with hollow metallic cylinders to guide implant placement in the virtually planned position were fabricated. Patients received professional oral hygiene prior to the surgery and were instructed to rinse with a 0.2% chlorhexidine mouthwash for 1 min, starting two days prior to the intervention.
Fig. 7 Periapical radiographs five days after implant placement.Surgical protocolAn antibiotic (2 g of amoxicillin and clavulanic acid or 600 mg clindamycin if allergic to penicillin) was administered 1 h prior to surgery and continued for six days (1 g amoxicillin and clavulanic acid or 300 mg clindamycin b.i.d.) after surgery. Local anesthesia was induced using a 4% articaine solution with 1:100,000 epinephrine (Ubistesin; 3M Italia, Milan, Italy). Implants were placed in the planned anatomical sites either conventionally or using a fully guided approach. A flapless or a flap approach was performed in order to maintain an adequate residual band of keratinized mucosa around the implants. When the alveolar crest was too thin (knife edge) to place the implant, the alveolar crest was remodeled using piezoelectric bone surgery under copious irrigation with sterile saline to obtain a flat bony crest. Each patient received four NobelSpeedy Groovy implants (Nobel Biocare), featuring a flat-to-flat matched implant-abutment interface with a 0.7 mm tall external hexagonal prosthetic connection and a rough, highly crystalline and phosphate-enriched titanium oxide surface (TiUnite, Nobel Biocare). All of the implants were placed according to the surgical and prosthetic protocols recommended by the manufacturer (IFU 73494 Manual 2/All-on-4 and IFU 71286), with no deviations from the original protocol. The drilling sequence was chosen according to the manufacturer’s instructions in relation to the bone quality, achieving an insertion torque at implant placement ranging from 35 to 45 N cm in the mandible or from 35 to 55 N cm in the maxilla, measured using a surgical unit (OsseoCare Pro Drill Motor Set, Nobel Biocare). In the post-extraction sites, the gaps between the implants and the surrounding socket walls were filled with 0.25–1 mm granules of deproteinized bovine bone (Geistlich Bio-Oss or Geistlich Bio-Oss Collagen, Geistlich Pharma, Wolhusen, Switzerland), hydrated using the patient’s blood mixed with antibiotic solution (Rifocin 250 mg/10 mL, Sanofi-aventis, Milan, Italy). Seventeen- or thirty-degree angled multi-unit abutments (Nobel Biocare) were immediately connected to the distal implants for better orientation of the screw access hole. Straight multi-unit abutments (Nobel Biocare) were used in the anterior implants if needed. A prefabricated screw-retained acrylic resin provisional restoration without any cantilever was delivered immediately after surgery (Figs. 3–5). All of the patients received oral and written recommendations regarding medication, oral hygiene maintenance and diet. Post-surgical analgesic treatment was provided with ibuprofen 600 mg, administered every 8 h for two days after the surgery, and later on if needed. The patients were instructed to rinse the mouth with a 0.2% chlorhexidine mouthwash t.i.d. without brushing the implant area (Figs. 6 & 7). Prosthetic protocolAfter three to four months of healing, a definitive impression was taken at the implant or abutment level according to a previously reported protocol.((Pozzi A, Tallarico M, Mangani F, Barlattani A. Different implant impression techniques for edentulous patients treated with CAD/CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading. → Eur J Oral Implantol. 2013 Winter;6(4):325–40. |
| 29. | ↑ | Pozzi A, Tallarico M, Mangani F, Barlattani A. Different implant impression techniques for edentulous patients treated with CAD/CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading. → Eur J Oral Implantol. 2013 Winter;6(4):325–40. Definitive prostheses with titanium or zirconia frameworks, fabricated using CAD/CAM technology (NobelProcera), were screwed on at either the implant or abutment level according to the manufacturer’s instructions three to five months after implant placement (in the mandible and the maxilla, respectively). The definitive implant-supported complete-arch FDP was designed with (hybrid design) or without pink material in the cervical region (crown design) and veneered with ceramic, acrylic or composite according to the patients’ needs (Figs. 8a–c). Clinical accuracy of the framework (strain-free screwing and absence of an open margin upon clinical and radiographic examination) was evaluated before prosthesis delivery.((Abduo J, Bennani V, Waddell N, Lyons K, Swain M. Assessing the fit of implant fixed prostheses: a critical review. → Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):506–15. |
| 30. | ↑ | Abduo J, Bennani V, Waddell N, Lyons K, Swain M. Assessing the fit of implant fixed prostheses: a critical review. → Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):506–15.((Eisenmann E, Mokabberi A, Walter MH, Freesmeyer WB. Improving the fit of implant-supported superstructures using the spark erosion technique. → Int J Oral Maxillofac Implants. 2004 Nov-Dec;19(6):810–8. |
| 31. | ↑ | Eisenmann E, Mokabberi A, Walter MH, Freesmeyer WB. Improving the fit of implant-supported superstructures using the spark erosion technique. → Int J Oral Maxillofac Implants. 2004 Nov-Dec;19(6):810–8.((Katsoulis J, Mericske-Stern R, Rotkina L, Zbären C, Enkling N, Blatz MB. Precision of fit of implant-supported screw-retained 10-unit computer-aided-designed and computeraided- manufactured frameworks made from zirconium dioxide and titanium: an in vitro study. → Clin Oral Implants Res. 2014 Feb;25(2):165–74. |
| 32. | ↑ | Katsoulis J, Mericske-Stern R, Rotkina L, Zbären C, Enkling N, Blatz MB. Precision of fit of implant-supported screw-retained 10-unit computer-aided-designed and computeraided- manufactured frameworks made from zirconium dioxide and titanium: an in vitro study. → Clin Oral Implants Res. 2014 Feb;25(2):165–74. The occlusion was adjusted avoiding any premature contacts. Mutually protected occlusion with anterior guidance or balanced occlusion was used in cases of opposing natural dentition or an FDP and complete removable denture, respectively. Follow-up visits were scheduled at one and six months and then annually up to five years of function. The patients underwent a professional cleaning by a dental hygienist every four to six months (Figs. 9a–c). Panoramic and periapical radiographs were obtained annually after definitive prosthesis delivery (Fig. 10).
Figs. 9a-c Lateral (a & c) and frontal (b) intra-oral photographs of the definitive prosthesis taken three years after implant placement. Fig. 10 Panoramic radiograph three years after implant placement.The primary outcome measures were as follows:
|
| 33. | ↑ | Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: a systematic review. → J Dent Res. 2012 Mar;91(3):242–8. were fulfilled: did not cause pain or suppuration, did not show any mobility, did not show any signs of radiolucency, and did not show periimplant bone loss of > 1.5 mm during the first year and then > 0.2 mm yearly.
The secondary outcome measures were as follows:
An independent assessor evaluated the implant and prosthesis survival and success rates. Complications were assessed and treated by the same clinicians. The marginal bone loss was evaluated by an independent radiologist. Statistical AnalysisPatient data were collected in an Excel spreadsheet (Microsoft). Finally, all of the data were exported into IBM SPSS Statistics for Macintosh (Version 22.0; IBM, Armonk, N.Y., U.S.) for statistical analysis. A bio-statistician with expertise in dentistry analyzed the data using PASW Statistics for Windows (Version 18.0; SPSS, Chicago, Ill., U.S.). Descriptive analysis was performed for numeric parameters using mean ± standard deviation (median; 95% CI). Dichotomous and continuous outcomes were compared using the chisquared test and one-way analysis of variance, respectively. Differences in the proportions of patients with implant failures, prosthesis failures and complications (dichotomous outcomes) were compared between the subgroups using the Fisher exact test. Patient was the statistical unit of the analyses. All statistical comparisons were conducted at a 0.05 level of significance. ResultsThirty-two patients were screened for eligibility. Two patients were not enrolled in the trial, because of refusal to sign the informed consent. A total of 120 NobelSpeedy Groovy implants were placed using either computer-assisted template-guided (n = 15) or conventional freehand surgery (n = 15) in 30 consecutive patients (18 females and 12 males) with a mean age of 67.4 ± 6.9 (range of 51–87). Thirty CAD/CAM screw-retained implant-supported complete-arch FDPs (18 in the mandible and 12 in the maxilla) were delivered. No patients dropped out of the study within three years after implant placement and no deviation from the original protocol occurred. All of the patients were followed up for a minimum period of three years (mean of 53.8 months; range of 36–84 months). Data collected were included in the statistical analysis. The main patients’ and interventions’ characteristics are summarized in Table 1. At the three-year follow-up examination, one out of 120 implants (0.8%) had failed, resulting in a cumulative implant survival rate of 99.2%. The only implant failure occurred in one patient two months after placement, before delivery of the final prosthesis. The affected implant had an infectious etiology (pain, swelling and suppuration) and it was 11.5 mm long in position 16, placed using guided surgery in a healed site. The implant was replaced three months after bone healing. The temporary prosthesis was shortened, but not replaced by a conventional complete removable denture, and the patient was adequately informed and instructed to pay attention and follow a soft diet. At the three-year follow-up examination, no definitive prostheses had failed, resulting in a cumulative prosthesis survival rate of 100%. Eleven patients experienced one technical or biological complication each, resulting in eight technical and three biological complications reported during the entire follow-up period. Six technical and one biological complication were reported during the healing period with temporary prostheses, while two technical and two biological complications were reported after definitive prosthesis delivery. All of the complications were successfully resolved. Three prosthetic screws loosened in the temporary prostheses (in three patients) during the healing period, and this was resolved by retightening the screws, stabilizing the occlusion and advising the patients not to overload the prostheses (not to ingest food that may require significant masticatory effort). Three fractures of the provisional acrylic prostheses occurred (in three patients) during the healing period. The temporary prosthesis was adjusted chairside, the occlusion was stabilized and a night guard was delivered for each patient. Fracture of the composite veneering material of the definitive implant-supported cross-arch FDP occurred in one patient two years after loading, most likely due to occasional parafunctional habits. These situations were resolved by adjusting the definitive prosthesis chairside, stabilizing the occlusion and a delivering a night guard. The first biological complication was reported six weeks after implant placement in an 11.5 mm long implant placed in position 45, using guided surgery in a healed site. The patient reported pain and swelling without suppuration. The temporary abutment was replaced with a healing abutment. The temporary prosthesis was shortened to the right canine. The implant was left to heal for four months according to a conventional loading protocol. The other two complications were periimplantitis, consisting of a mean mesiodistal periimplant bone loss of 2.6 and 2.8 mm, reported at the one-year follow-up examination. The first case of periimplantitis developed around a 15 mm long implant in position 35, placed using conventional freehand surgery in a healed site. The second case developed around a 13 mm long implant in position 32, placed using guided surgery in a healed site and immediately loaded. No other technical or biological complications occurred during the entire follow-up period. After an initial mean marginal bone loss of 1.16 ± 0.40 mm (1.06 mm; 95% CI: 0.92–1.20), all of the implants lost a mean of 0.21 ± 0.11 mm (0.20 mm; 95% CI: 0.16–0.24) between the oneand two-year follow-ups, and 0.16 ± 0.07 mm (0.15 mm; 95% CI: 0.13–0.17) between the twoand three-year follow-ups. At the three-year follow-up, the mean marginal bone loss was 1.52 ± 0.41 mm (1.42 mm; 95% CI: 1.27–1.57). The radiographic data are shown in Table 2. All of the patients were fully satisfied with the function and esthetics of their definitive prostheses, and all of the patients declared that they would undergo the same treatment again. Maxilla versus mandibleTwelve patients were treated in the maxilla, while 18 patients were treated in the mandible. There were no statistically significant differences between centers for the number of patients who had failed implants (1/12 vs. 0/18; risk ratio = NA; p = 0.399) or complications (3/12 vs. 8/18; risk ratio = 0.5625; 95% CI: 0.19–1.70; p = 0.442). At the three-year follow-up examination, the mean marginal bone loss was 1.49 ± 0.34 mm (1.42 mm; 95% CI: 1.23–1.61) in the maxilla versus 1.54 ± 0.46 mm (1.38 mm; 95% CI: 1.17–1.59) in the mandible (p = 0.756). The radiographic data are shown in Table 3. Guided versus conventional freehand surgeryFifteen patients were treated using computer-assisted template-based surgery and 15 with conventional freehand surgery. There were no statistically significant differences between centers for the number of patients who had failed implants (1/15 vs. 0/15; risk ratio = NA; p = 0.999) or complications (4/15 vs. 7/15; risk ratio = 0.5714; 95% CI: 0.21–1.55; p = 0.449). At the three-year follow-up examination, the mean marginal bone loss was 1.48 ± 0.47 mm (1.33 mm; 95% CI: 1.09–1.57) in the guided surgery group versus 1.55 ± 0.34 mm (1.46 mm; 95% CI: 1.29–1.63) in the conventional freehand surgery group (p = 0.365). The radiographic data are shown in Table 3.
Table 1. Patients’ and interventions’ characteristics.
Table 2. Mean marginal bone loss ± standard deviation (mm) (95% CI) between follow-up examinations.
Table 3. Three-year marginal bone loss ± standard deviation (mm) according to the jaw location and type of surgery.
† Unpaired t-test assuming normal distribution. DiscussionThe present study reported data on 30 implant-supported restorations delivered according to the All-on-4 protocol and followed for at least three years after implant placement. Because it was designed as a single-cohort prospective study, the main limitation of the present research was the lack of a control group and the small sample size. Another limitation of the present study was the variability within the cohort of patients. In the present study, the three-year implant (99.2%) and prosthesis success rates (100.0%), as well as the mean bone loss of 1.52 ± 0.41 mm, indicate that the All-on-4 treatment concept is a promising treatment modality. Furthermore, the results of this prospective observational study are consistent with other studies investigating the same topic. A recent systematic review by Patzelt et al., which included 4,804 implants, demonstrated a mean cumulative implant and prosthesis survival rate at three years of 99.0 ± 1.0% and 99.9 ± 0.3%, respectively.((Patzelt SB, Bahat O, Reynolds MA, Strub JR. The all-on-four treatment concept: a systematic review. → Clin Implant Dent Relat Res. 2014 Dec;16(6):836–55. |
| 34. | ↑ | Patzelt SB, Bahat O, Reynolds MA, Strub JR. The all-on-four treatment concept: a systematic review. → Clin Implant Dent Relat Res. 2014 Dec;16(6):836–55. The mean bone loss at three years amounted to 1.3 ± 0.4 mm. However, 12 out of the 13 included studies were considered to be highly biased. Most of the studies included (69%) in the systematic review derived from a limited number of investigators in Italy and Portugal, which may limit the generalizability of the findings, and only 31 % of the studies reported a completed follow-up period of three years.
Malo et al. retrospectively reported a cumulative patient-related success rate of 93.8% up to ten years of follow-up in the mandible and a prosthesis survival rate of 99.2%.((Malo P, de Araújo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. → J Am Dent Assoc. 2011 Mar;142(3):310–20. |
| 35. | ↑ | Malo P, de Araújo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. → J Am Dent Assoc. 2011 Mar;142(3):310–20. In the maxilla, a five-year survival rate of 93% was reported, and the survival rate of the prostheses was 100%.((Maló P, de Araújo Nobre M, Lopes A, Francischone C, Rigolizzo M. “All-on-4” immediate-function concept for completely edentulous maxillae: a clinical report on the medium (3 years) and long-term (5 years) outcomes. → Clin Implant Dent Relat Res. 2012 May;14 Suppl 1:e139–50. |
| 36. | ↑ | Maló P, de Araújo Nobre M, Lopes A, Francischone C, Rigolizzo M. “All-on-4” immediate-function concept for completely edentulous maxillae: a clinical report on the medium (3 years) and long-term (5 years) outcomes. → Clin Implant Dent Relat Res. 2012 May;14 Suppl 1:e139–50. The mean marginal bone loss was 1.52 ± 0.30 mm after three years. Similar results were reported by Browaeys et al., who highlighted unacceptable ongoing bone loss in 49.2% of the patients.((Browaeys H, Dierens M, Ruyffelaert C, Matthijs C, De Bruyn H, Vandeweghe S. Ongoing crestal bone loss around implants subjected to computer-guided flapless surgery and immediate loading using the All-on-4® concept. → Clin Implant Dent Relat Res. 2015 Oct;17(5):831–43. |
| 37. | ↑ | Browaeys H, Dierens M, Ruyffelaert C, Matthijs C, De Bruyn H, Vandeweghe S. Ongoing crestal bone loss around implants subjected to computer-guided flapless surgery and immediate loading using the All-on-4® concept. → Clin Implant Dent Relat Res. 2015 Oct;17(5):831–43.
Balshi et al. retrospectively analyzed the outcomes of 200 arches (800 implants) treated according to the All-on-4 protocol.((Balshi TJ, Wolfinger GJ, Slauch RW, Balshi SF. A retrospective analysis of 800 Brånemark System implants following the All-on-Four™ protocol. → J Prosthodont. 2014 Feb;23(2):83–8. |
| 38. | ↑ | Balshi TJ, Wolfinger GJ, Slauch RW, Balshi SF. A retrospective analysis of 800 Brånemark System implants following the All-on-Four™ protocol. → J Prosthodont. 2014 Feb;23(2):83–8. Twenty percent (168 implants out of 800) of the implants analyzed had a follow-up period of three years or more. Cumulative implant and prosthesis survival rates amounted to 97.3% and 99.0%, respectively.
Grandi et al. analyzed 47 patients treated with 188 immediately loaded implants placed in the mandible according to the All-on-4 protocol in post-extraction sites.((Grandi T, Guazzi P, Samarani R, Grandi G. Immediate loading of four (All-on-4) post-extractive implants supporting mandibular cross-arch fixed prostheses: 18-month follow-up from a multicentre prospective cohort study. → Eur J Oral Implantol. 2012 Autumn;5(3):277–85. |
| 39. | ↑ | Grandi T, Guazzi P, Samarani R, Grandi G. Immediate loading of four (All-on-4) post-extractive implants supporting mandibular cross-arch fixed prostheses: 18-month follow-up from a multicentre prospective cohort study. → Eur J Oral Implantol. 2012 Autumn;5(3):277–85. At the 18-month follow- up, no implant had failed and all of the restorations were stable. However, three patients experienced fracture of the provisional restoration. No significant differences in bone loss were found between axially placed and tilted implants at the 18-month follow-up.
Babbush et al. retrospectively examined 165 patients treated according to the All-on-4 protocol.((Babbush CA, Kutsko GT, Brokloff J. The All-on-Four immediate function treatment concept with NobelActive implants: a retrospective study. → J Oral Implantol. 2011 Aug;37(4):431–45. |
| 40. | ↑ | Babbush CA, Kutsko GT, Brokloff J. The All-on-Four immediate function treatment concept with NobelActive implants: a retrospective study. → J Oral Implantol. 2011 Aug;37(4):431–45. The cumulative implant survival rate was 99.6% (99.3% in the maxilla and 100.0% in the mandible) for up to 29 months of loading. The definitive prosthesis survival rate was 100%. Recently, the same authors retrospectively analyzed the patient-centered outcomes, including the cost of treatment, length of the treatment period and comfort provided by the provisional restoration, in patients treated according to the All-on-4 protocol and compared these results to a historical control group, which included complete- arch FDPs supported by natural teeth or implants and implant-supported overdentures.((Babbush CA, Kanawati A, Kotsakis GA, Hinrichs JE. Patient-related and financial outcomes analysis of conventional full-arch rehabilitation versus the All-on-4 concept: a cohort study. → Implant Dent. 2014 Apr;23(2):218–24. |
| 41. | ↑ | Babbush CA, Kanawati A, Kotsakis GA, Hinrichs JE. Patient-related and financial outcomes analysis of conventional full-arch rehabilitation versus the All-on-4 concept: a cohort study. → Implant Dent. 2014 Apr;23(2):218–24. This study demonstrated that the cost, length of treatment and comfort provided by the provisional restoration significantly favored the All-on-4 treatment modality.
In the present study, the overall percentage of complications experienced was large (36.6 %). Nevertheless, this result did not differ from those normally encountered in oral rehabilitation in which implants are used as support for an FDP (33.6% at five years).((Schwarz F, Hegewald A, Becker J. Impact of implant-abutment connection and positioning of the machined collar/microgap on crestal bone level changes: a systematic review. → Clin Oral Implants Res. 2014 Apr;25(4):417–25. |
| 42. | ↑ | Schwarz F, Hegewald A, Becker J. Impact of implant-abutment connection and positioning of the machined collar/microgap on crestal bone level changes: a systematic review. → Clin Oral Implants Res. 2014 Apr;25(4):417–25. Moreover, most of these complications were reported on the temporary restoration, during healing. The clinicians who carried out the procedures addressed all of the complications chairside. Furthermore, the condition of the patients remained stable up to the completion of the three-year follow-up period. In order to minimize the incidence of complications, dental clinicians should exert great effort in selecting patients, respecting the original protocols, and choosing reliable components and materials for implant-supported complete-arch FDPs.
Patients with untreated periodontitis were not included in the study. Implant therapy in patients with a history of chronic periodontitis and generalized aggressive periodontitis might be considered a viable treatment with similar survival outcomes to those reported for healthy patients. Periodontally compromised patients were included after being treated to reduce the inflammation and halt the disease progression, before tooth extraction and implant placement. According to Donos et al., it is necessary to treat and control the periodontal disease, regardless of its progression pattern and subtype, before implant therapy is initiated in order to improve the overall implant success and achieve a more favorable bone resorption pattern.((Donos N, Laurell L, Mardas N. Hierarchical decisions on teeth vs. implants in the periodontitis-susceptible patient: the modern dilemma. → Periodontol 2000. 2012 Jun;59(1):89–110. |





Leave a Reply
Be the First to Comment!