Use of argon plasma to enhance softtissue integration of prosthetic components: a randomized, controlled animal study
June 14, 2017 / Categories: Digital Dentistry, Implant Dentistry

Carneiro Martins Neto, Evandro

Canullo, Luigi

Tallarico, Marco
Salata, Luiz A.
Xavier, Samuel Porfírio
Abstract
Objective
This paper aimed to assess histologically the soft- and hard-tissue changes after insertion of cleaned and activated titanium implant abutments.
Methods
Three months after tooth extractions, four implants were inserted in one side of the mandible. Before connecting the abutments to the implants, two of them were detoxified (test group), while two were left untreated (control group). The abutments were randomly placed on the two distally or on the two mesially located implants. After one month, the same procedure was repeated on the other side of the mandible. The animals were euthanized one month after the last surgery. Histological analysis was performed to identify the shoulder of the implant, the most coronal bone-to-implant contact, the top of the adjacent bony crest, the top of the periimplant mucosa (PM) and the apical termination of the junctional epithelium (AJE).
Results
All of the animals remained in good health during the experimental period. No statistically significant differences were found between the test and control sites (p > 0.05). Between the first and the second time points, no statistically significant differences between the groups were found, except for PM–AJE of the test group, with higher values observed two months after implant placement. However, a trend of better marginal bone levels was found in the test group, compared with the control group, at the second time point.
Conclusion
Although differences between the test and control groups failed to reach significance, a trend of better marginal bone levels was found at the test sites compared with the control sites.
Keywords
Argon plasma, soft-tissue adhesion, animal study, titanium abutment.
Introduction
Periimplant soft- and hard-tissue stability is critical for the success of an implant-supported restoration, from a functional and esthetic point of view.1Buser D, Martin W, Belser U. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations.
→ Int J Oral Maxillofac Implants. 2004;19 Suppl:43–61. It has been described that the relationship between the implant-abutment connection and surrounding hard and soft tissue plays an important role in establishing such mechanical and biological stability.2Abrahamsson I, Berglundh T, Wennström J, Lindhe J. The peri-implant hard and soft tissues at different implant systems. A comparative study in the dog.
→ Clin Oral Implant Res. 1996 Sep;7(3):212–9.3Pozzi A, Tallarico M, Moy PK. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with different prosthetic interfaces and design in partially posterior edentulous mandibles.
→ Eur J Oral Implantol. 2014 Spring;7(1):47–61.
In fact, the literature has demonstrated that, when an implant is exposed to the oral environment after the connection of a prosthetic component, periimplant hard-tissue level changes may occur4Hermann JS, Cochran DL, Nummikoski PV, Buser D. Crestal bone changes around titanium implants. A radiographic evaluation of unloaded nonsubmerged and submerged implants in the canine mandible.
→ J Periodontol . 1997 Nov;68(11):1117–30. and that the amount of bone remodeling, characterized by circumferential (horizontal and vertical) bone loss, should remain stable after one year.5Manz MC. Factors associated with radiographic vertical bone loss around implants placed in a clinical study.
→ Ann Periodontol. 2000 Dec;5(1):137–51. Several factors and, in particular, disruptions occurring after prosthetic connections may affect periimplant resorption,6Molina A, Sanz-Sánchez I, Martín C, Blanco J, Sanz M. The effect of one-time abutment placement on interproximal bone levels and peri-implant soft tissues: a prospective randomized clinical trial.
→ Clin Oral Implants Res. 2017 Apr;28(4):443–52. doi:10.1111/clr.12818. Epub 2016 Mar 25. since the bacterial contamination of the implant-abutment junction from the oral cavity has been shown to trigger a hard-tissue response.7Cochran DL, Hermann JS, Schenk RK, Higginbottom FL, Buser D. Biologic width around titanium implants. A histometric analysis of the implanto-gingival junction around unloaded and loaded nonsubmerged implants in the canine mandible.
→ J Periodontal. 1997 Feb;68(2):186–98.
Many strategies have been advocated to minimize the effect of this contamination clinically: mechanical improvement of the implant-abutment connection stability,8Schmitt CM, Nogueira-Filho G, Tenenbaum HC, Lai JY, Brito C, Döring H, Nonhoff J. Performance of conical abutment (Morse Taper) connection implants: a systematic review.
→ J Biomed Mater Res A. 2014 Feb;102(2):552–74. implant abutment microgap shifting from the vital bone,9Degidi M, Iezzi G, Scarano A, Piattelli A. Immediately loaded titanium implant with a tissue-stabilizing/maintaining design (‘beyond platform switch’) retrieved from man after 4 weeks: a histological and histomorphometrical evaluation. A case report.
→ Clin Oral Implants Res. 2008 Mar;19(3):276–82.10Vigolo P, Givani A. Platform-switched restorations on wide-diameter implants: a 5-year clinical prospective study.
→ Int J Oral Maxillofac Implants. 2009 Jan-Feb;24(1):103–9.11Canullo L, Fedele GR, Iannello G, Jepsen S. Platform switching and marginal bone-level alterations: the results of a randomized-controlled trial.
→ Clin Oral Implants Res. 2010 Jan;21(1):115–21.12Pozzi A, Agliardi EL, Tallarico M, Barlattani A. Clinical and radiological outcomes of two implants with different prosthetic interfaces and neck configurations: randomized, controlled, split-mouth clinical trial.
→ Clin Implant Dent Relat Res. 2014 Feb;16(1):96–106. and reducing the number of abutment dis and reconnections.13Molina A, Sanz-Sánchez I, Martín C, Blanco J, Sanz M. The effect of one-time abutment placement on interproximal bone levels and peri-implant soft tissues: a prospective randomized clinical trial.
→ Clin Oral Implants Res. 2017 Apr;28(4):443–52. doi:10.1111/clr.12818. Epub 2016 Mar 25. Nevertheless, minimal bone resorption (0.5 mm) has been observed in longitudinal analysis.14Annibali S, Bignozzi I, Cristalli MP, GrazianiF, La Monaca G, Polimeni A. Peri-implant marginal bone level: a systematic review and meta-analysis of studies comparing platform switching versus conventionally restored implants.
→ J Clin Periodontol. 2012 Nov;39(11):1097–113.
Bone resorption might be related to the contaminants (bacteria, wear microparticles and pollution from laboratory procedures) present on the abutment at the time of implant abutment connection. In fact, the presence of contaminants on the abutment surface can still be observed after the steam cleaning protocol after technical laboratory procedures.15Canullo L, Micarelli C, Lembo-Fazio L, Iannello G, Clementini M. Microscopical and microbiologic characterization of customized titanium abutments after different cleaning procedures.
→ Clin Oral Implant Res. 2014 Mar;25(3):328–36. doi:10.1111/clr.12089. Epub 2012 Dec 5. Since the abutment comes into contact with both bone and connective tissue, abutment cleanliness appears to be important. In fact, the presence of contaminants at the platform-abutment level has been suggested to cause associated tissuedamaging inflammation.16Canullo L, Micarelli C, Lembo-Fazio L, Iannello G, Clementini M. Microscopical and microbiologic characterization of customized titanium abutments after different cleaning procedures.
→ Clin Oral Implant Res. 2014 Mar;25(3):328–36. doi:10.1111/clr.12089. Epub 2012 Dec 5. Titanium wear microparticles have been demonstrated to activate osteoclastogenesis.17Mishra PK, Wu W, Rozo C, Hallab NJ, Benevenia J, Gause WC. Micrometer-sized titanium particles can induce potent th2-type responses through TLR4-independent pathways.
→ J Immunol. 2011 Dec;187(12):6491–8. Additionally, it has been shown how interactions between cellular components and implant-abutment materials influence the healing process around implants and how these interactions are regulated by the state of the surface.18Piattelli A, Pontes AE, Degidi M, Iezzi G. Histologic studies on osseointegration: soft tissues response to implant surfaces and components. A review.
→ Dent Mater. 2011 Jan;27(1):53–60.
In order to protect abutments against such pollutants, plasma cleaning of customized abutments has recently been advocated.19Canullo L, Micarelli C, Iannello G. Microscopical and chemical surface characterization of the gingival portion and connection of an internal hexagon abutment before and after different technical stages of preparation.
→ Clin Oral Implants Res. 2013 Jun;24(6):606–11. Plasma cleaning has been demonstrated in vitro to have a triple effect on titanium: cleaning, corrosion protection and increased surface energy.20Tavares JC, Cornélio DA, da Silva NB, de Moura CE, de Queiroz JD, Sá JC, Alves C Jr, de Medeiros SR. Effect of titanium surface modified by plasma energy source on genotoxic response in vitro.
→ Toxicology. 2009 Aug;262(2):138–45. 21Canullo L, Genova T, Tallarico M, Gautier G, Mussano F, Botticelli D. Plasma of argon affects the earliest biological response of different implant surfaces: an in vitro comparative study.
→ J Dent Res. 2016 May;95(5):566–73. However, there is a lack of evidence in the literature regarding the clinical relevance of a plasma cleaning procedure performed on dental implant abutments.
Although there are certain differences in the inflammatory response and in the bacterial population, the beagle dog model has been extensively used in experimental study because of its size and its extremely cooperative nature. Although some major differences exist between dogs and humans, all periodontal tissues and the size of the teeth are quite similar to those observed in humans. Furthermore, they are a very inbred type of animal with very limited anatomical differences between the various dogs.
The aim of this animal study was to assess histologically soft and hard-tissue adaptation after insertion of cleaned and activated titanium implant-abutments. The null hypothesis was that argon plasma cleaning treatment of abutments does not have any positive or detrimental effect on periimplant bone remodeling and soft-tissue adhesion.
Materials and methods
Subjects
This study followed the ARRIVE guidelines.22Kilkenny C, Browne W, Cuthill IC, Emerson M, Altman DG; National Centre for the Replacement, Refinement and Reduction of Animals in Research. Animal research: reporting in vivo experiments—the ARRIVE guidelines.
→ J Cereb Blood Flow Metab. 2011 Apr;31(4):991–3. The research protocol was approved by the local ethics committee for animal research at the University of São Paulo, Ribeirão Preto, Brazil.
Eight beagle dogs were used for the experiment. The animals were pre-anesthetized for all surgical procedures with Acepran 0.2% (0.05 mg/kg; Univet-vetnil, São Paulo, Brazil) and sedated with Zoletil (10 mg/kg; Virbac, St. Louis, Mo. U.S.), and the maintenance of the anesthesia was performed with inhalation of Forane (Baxter Hospitalar, São Paulo, Brazil).
All mandibular premolars and the first molars were extracted bilaterally and after three months, a crestal incision was performed in the premolar–molar region of one randomly selected side of the mandible. Full-thickness mucoperiosteal flaps were elevated, and four experimental sites were selected in the edentulous alveolar ridges of the mandible, two in the anterior and two in the distal regions. The surgical preparation of the sites was performed according to the manual of the implant system used. Twist drills were used to prepare each recipient site. Four implants (Premium, Sweden & Martina, Due Carrare, Italy), 7 mm long and 3.3 mm wide, were subsequently inserted. Before connection, two of the four abutments were detoxified (test group), while two were left untreated (control group). One abutment of each group was placed on to one of the two mesially and one of the two distally located implants, respectively, according to the randomization allocation. The flaps were sutured to allow nonsubmerged healing. After one month of healing, the surgical procedures were applied on the other side of the mandible, again following a randomization protocol.
After every surgery, the animals underwent antibiotic treatment for ten days (Stomorgyl 10, one tablet/10 kg daily; Merial Saúde Animal, Paulinia, Brazil) and received anti-inflammatory drugs for five days (Maxicam 2 mg, one tablet/20 kg daily; Ourofino Saúde Animal, Cravinhos, Brazil) and an analgesic for three days (Tramal 50 mg, 4 mg/kg, subcutaneous; every 8 h; União Química Farmacêutica Nacional, Pouso Alegre, Brazil).
The animals were kept in kennels at the university’s field laboratory with free access to water and feed of moistened balanced dogfood. Daily inspection of the wounds for clinical signs of complications and cleaning of the healing abutments were performed. The animals were euthanized one month after the last surgery by applying an overdose of thiopental (Cristália, Campinas, Brazil) and 25 meq of potassium chloride IV.
-
- Fig. 1
-
- Fig. 2
-

- Fig. 3
-

- Fig. 4
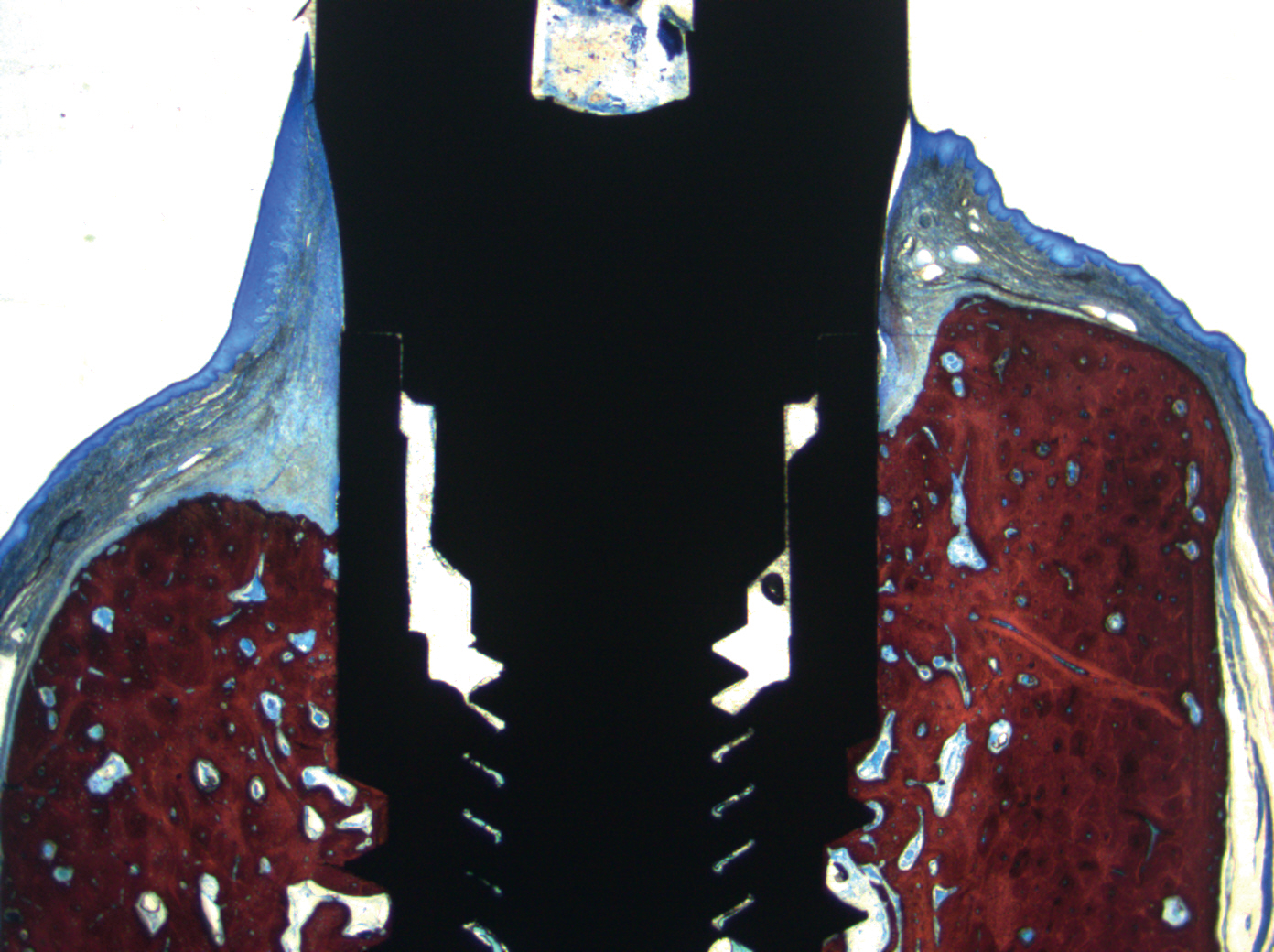
Fig. 1
Ground section illustrating the results of healing after one month at a test site. 16× magnification. Alizarin red and Stevenel’s blue stain.
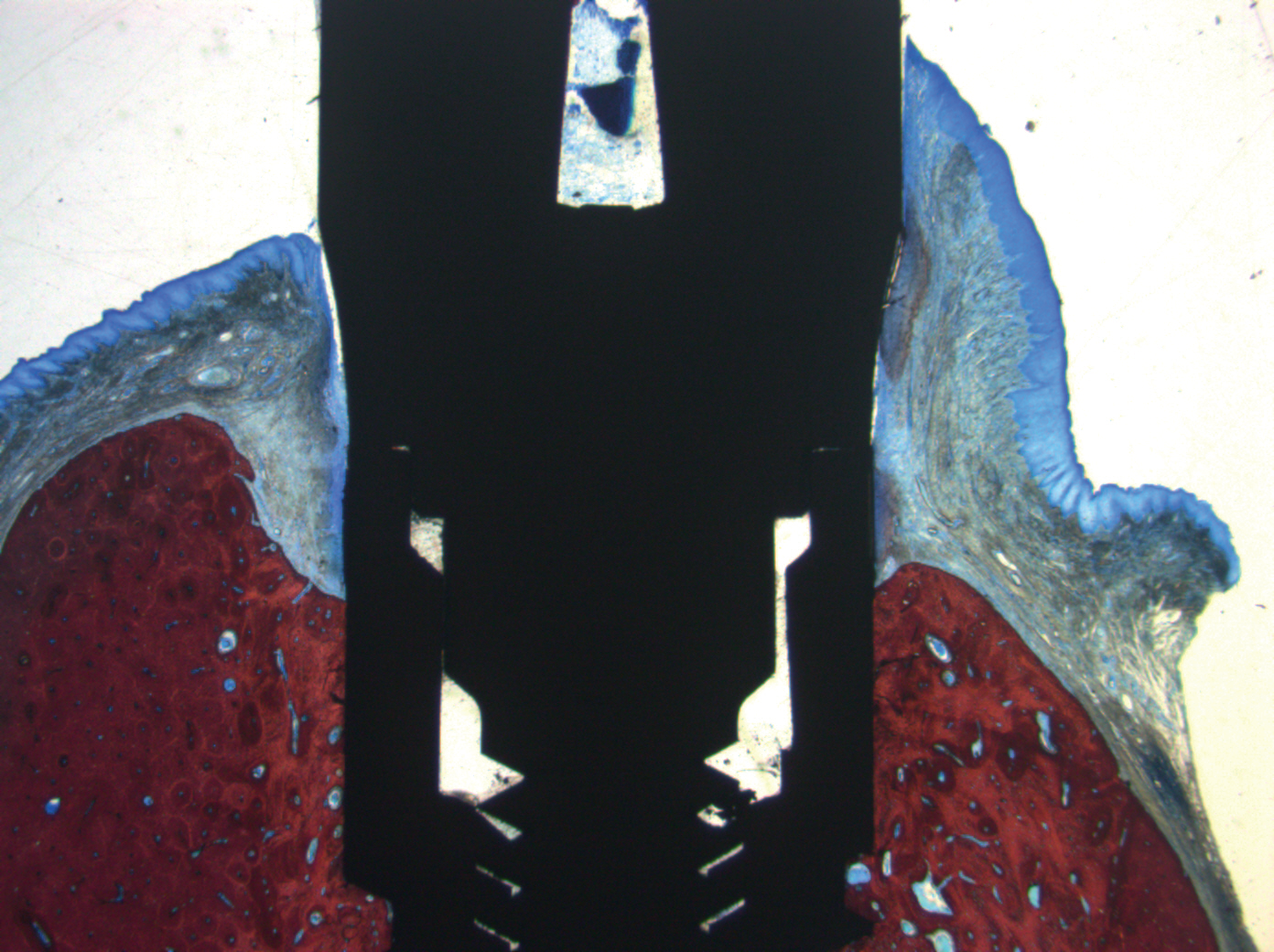
Fig. 2
Ground section illustrating the results of healing after one month at a control site. 16× magnification. Alizarin red and Stevenel’s blue stain.
Fig. 3
Ground section illustrating the results of healing after two months at a test site. 16× magnification. Alizarin red and Stevenel’s blue stain.
Fig. 4
Ground section illustrating the results of healing after two months at a control site. 16× magnification. Alizarin red and Stevenel’s blue stain.
Abutment preparation
The control group abutments, after being milled and polished, were cleaned by steam for 30 s (VAP 1; Zhermack, Cologne, Germany) before delivery. The test group abutments, after being milled, polished and cleaned for 30 s (VAP 1), underwent argon plasma treatment (75 W power and -10 MPa pressure for 12 min at room temperature) in a plasma reactor (Diener electronic, Jettingen, Germany) present in the same clinical facility, but in a different room.
Histological preparation
Individual bone blocks containing one implant each and the surrounding soft and hard tissue were fixed in a 4% formaldehyde solution. The blocks were dehydrated in a series of graded alcohol solutions and finally embedded in resin (LR White, hard grade; London Resin Company, Berkshire, U.K.). The blocks were cut in a buccolingual plane using a diamond band saw fitted in a precision slicing machine (EXAKT Apparatebau, Norderstedt, Germany) and then reduced to a thickness of about 50–60 μm using a cutting– grinding device (EXAKT Apparatebau). The histological slides were stained with alizarin red and Stevenel’s blue and examined under a standard light microscope for histometric analysis.
Histological analysis
In a microscope at 100× magnification, the following landmarks were identified: the shoulder of the implant (IS), the most coronal bone- toimplant contact (B), the top of the adjacent bony crest (C), the top of the periimplant mucosa (PM) and the apical termination of the junctional epithelium (AJE). The following linear measurements were performed parallel to the long axis of the implant: the vertical distances between (i) IS and B (IS–B), (ii) IS and C (IS–C), (iii) PM and C (PM–C), and (iv) PM and AJE (PM–AJE).
Randomization procedure
The dogs randomly received implants in the right or left side of the mandible in the first surgery and in the other side in the next surgery. Immediately after implant placement, untreated (as they come from industry; control group) or detoxified abutments (argon plasma; test group) were randomly assigned to the implant sites. A balanced random permuted block approach was used to prepare the randomization tables to prevent an unequal balance between the two groups. A blinded statistician generated the allocation sequence and assigned abutments to sites. Assignment was performed using opaque envelopes containing the generated unique randomization code opened immediately after implant placement.
Statistical analysis
Mean values and standard deviations were calculated for each outcome variable. Measurements of the buccal and lingual aspects were performed, with an accuracy of 0.01 mm. Mean values between the buccal and lingual aspects were obtained.
Median and interquartile values were also calculated in order to give a better description of the data set (25th, 50th [median] and 75th percentiles). All measurements were rounded to the nearest decimal. Data were pooled for abutment treatment (cleaned or activated titanium implant abutments). The primary variables were IS–C and IS–B. Differences between the test and control sites were analyzed using the nonparametric Mann–Whitney U test. Comparisons between each time point were made by paired tests in order to detect any changes in marginal periimplant bone levels. All statistical comparisons were conducted at the 0.05 level of signi ficance.
Results
In total, 64 implants were placed in eight beagle dogs. All of the animals remained in good health during the experimental period and no complications occurred during the healing period. An n = 8 was reached at the one-month period, while an n = 7 was reached at the two-month period because one dog lost implants in the control group.
After one month of healing (Table 1), in the test group, at the buccal aspect, IS–B was 1.43 ± 0.99 mm, IS–C was 0.67 ± 0.53 mm, PM–C was 2.61 ± 0.37 mm and PM–AJE was 2.39 ± 0.33 mm. In the control group, IS–B was 1.61 ± 0.74 mm, IS–C was 0.50 ± 0.59 mm, PM–C was 2.59 ± 0.36 mm and PM–AJE was 2.59 ± 0.41 mm. No statistically significant differences were found between the groups (p > 0.05; Table 1). The median and interquartile values are reported in Table 1.
After two months of healing (Table 2), in the test group, IS–B was 1.72 ± 0.70 mm, IS–C was 0.50 ± 0.48 mm, PM–C was 2.59 ± 0.27 mm and PM–AJE was 2.78 ± 0.44 mm. In the control group, IS–B was 2.18 ± 0.71 mm, IS–C was 0.91 ± 0.64 mm, PM–C was 2.86 ± 0.84 mm and PM–AJE was 2.42 ± 0.64 mm. No statistically significant differences were found between the groups (p > 0.05; Table 2). The median and interquartile values are reported in Table 2.
The results between the first and the second time points showed no statistically significant differences between the test and control groups, except for PM–AJE of the test group, with higher values observed two months after implant placement (Table 3).
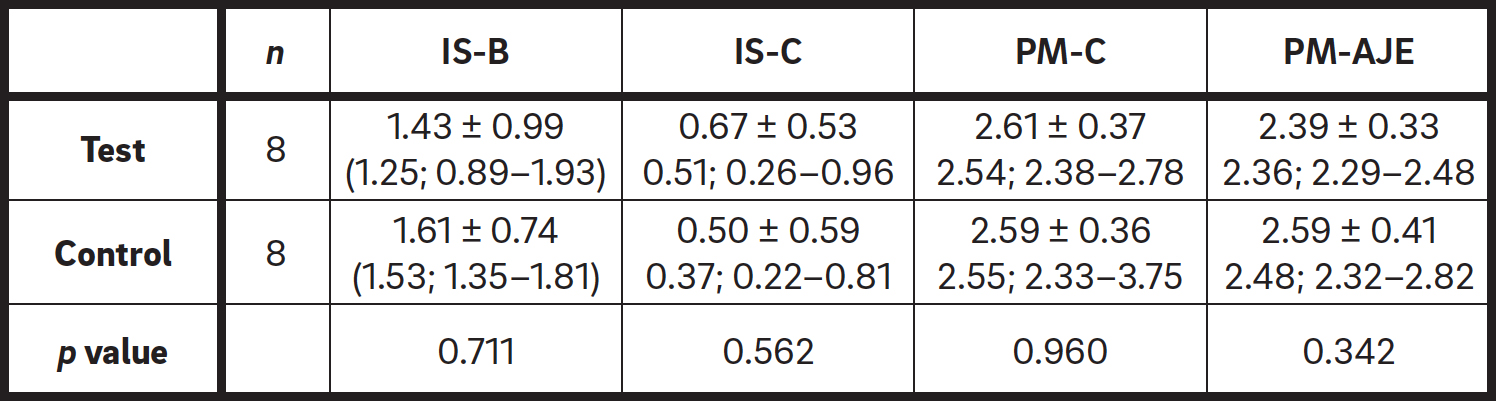
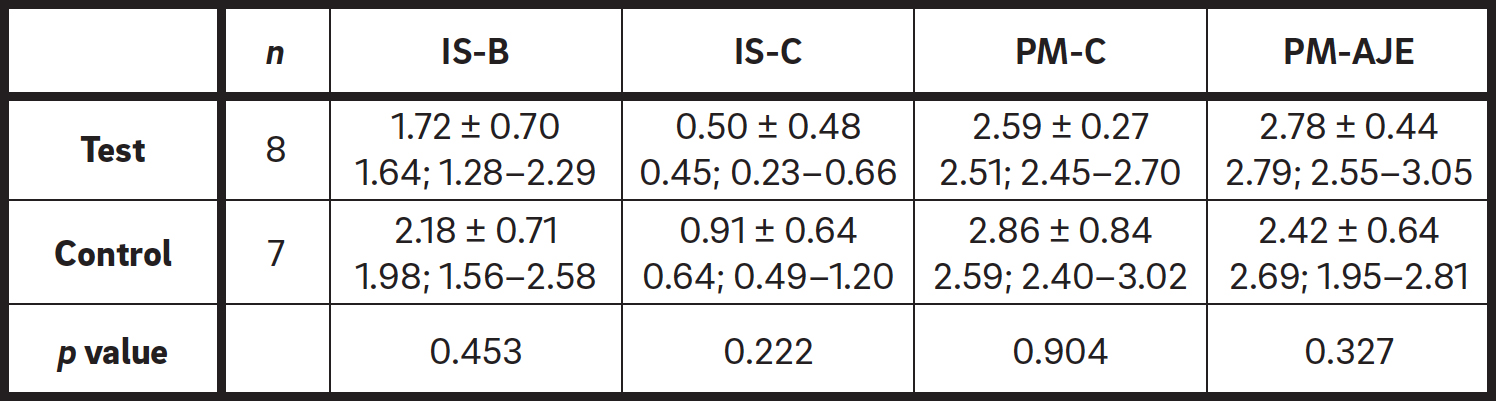
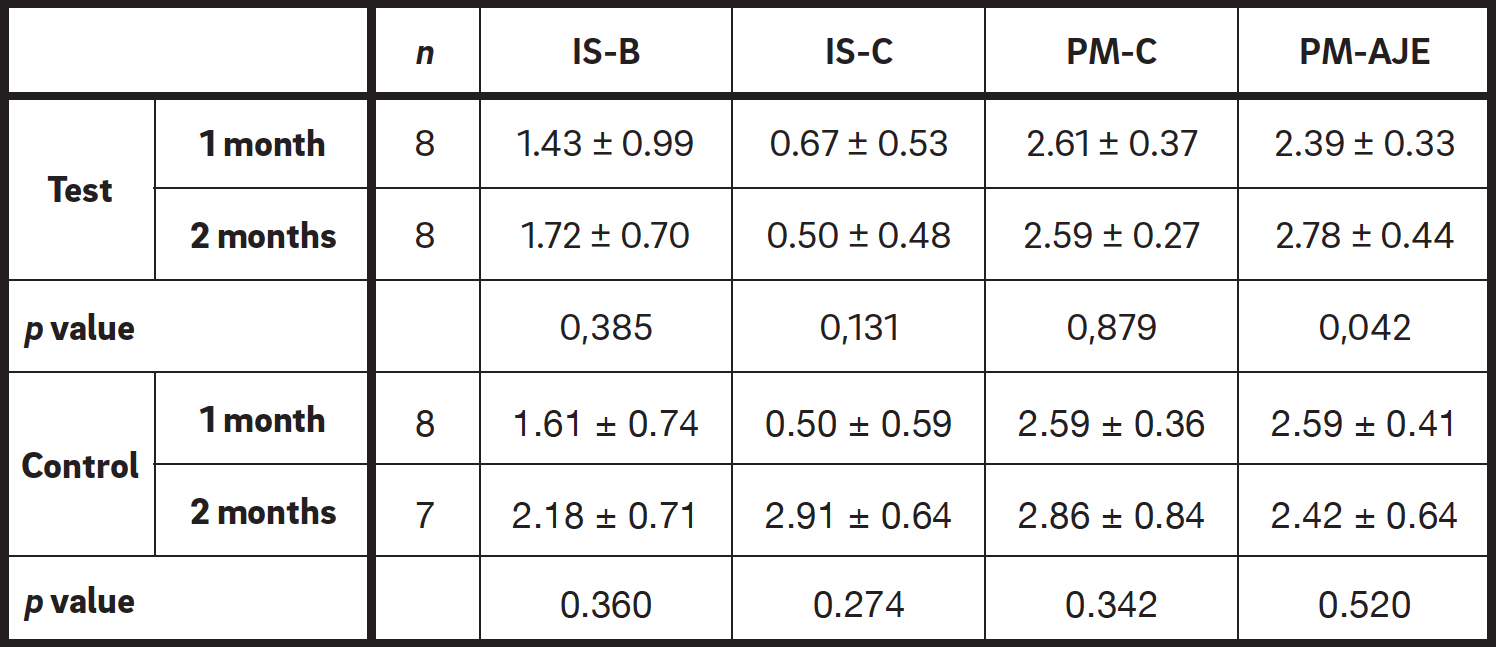
Table 1
Comparison between test and control groups one month after implant placement. Data are presented in mm as mean ± standard deviation (Median; IRQ 25th–75th mm).
Table 2
Comparison between test and control groups two months after implant placement. Data are presented in mm as mean ± standard deviation (Median; IRQ 25th–75th mm).
Table 3
Comparison between one and two months timepoints. Data are presented in mm.
Discussion
Although cleaning procedures (cleansing with alcohol, soap or steam vapor) at the end of the laboratory phase should be carried out according to law in the U.S.,23Cleveland JL, Bonito AJ, Corley TJ, Foster M, Barker L, Gordon Brown G, Lenfestey N, Lux L. Advancing infection control in dental care settings: factors associated with dentists’ implementation of guidelines from the Centers for Disease Control and Prevention.
→ J Am Dent Ass. 2012 Oct:143(10):1127–38. Europe (EN ISO 17664:2004) and Australia (ADA’s Guidelines for Infection Control, 2015), several microscopic impurities can be detected on the abutment surface even after these treatments. Microscopic impurities on the abutment surface due to industrial processes can often be detected also after industrial prepackaging procedures.24Sawase T, Wennerberg A, Hallgren C, Albrektsson T, Baba K. Chemical and topographical surface analysis of five different implant abutments.
→ Clin Oral Implants Res. 2000 Feb;11(1):44–50. Additional metallic microparticles mixed with lubricant and oxide layers can be produced during the laboratory workflow and adsorbed contaminants can be accumulated during delivery.25Canullo L, Micarelli C, Iannello G. Microscopical and chemical surface characterization of the gingival portion and connection of an internal hexagon abutment before and after different technical stages of preparation.
→ Clin Oral Implants Res. 2013 Jun;24(6):606–11. Such pollution and oxide layers can directly and indirectly trigger a soft and hard-tissue inflammatory response or at least alter the interaction with the soft and hard-tissue environments.26Mishra PK, Wu W, Rozo C, Hallab NJ, Benevenia J, Gause WC. Micrometer-sized titanium particles can induce potent th2-type responses through TLR4-independent pathways.
→ J Immunol. 2011 Dec;187(12):6491–8.
A very important area of research is the development of efficient high-vacuum technologies able to clean and functionalize surfaces to replace conventional methods of cleaning metallic or polymeric surfaces. In this context, cold plasma technology represents an efficient alternative and has been the subject of increasing attention.
Low-temperature plasma equipment works within a vacuum chamber in which atmospheric gases have been evacuated typically below 0.1 torr. This low pressure allows for a relatively long free path of accelerated electrons and ions. Since the ions and neutral particles are at or near ambient temperatures and the electrons, which are at high-temperature or electronvolt levels, have relatively few collisions with molecules at this pressure, the reaction remains at low temperature.With appropriate plasma parameters, argon plasma removes all chemical traces of previous treatments, in effect producing cleaner and better controlled surfaces than with conventional preparation methods.27Moisan M, Barbeau J, Crevier MC, Pelletier J, Philip N, Saoudi N. Plasma sterilization. Methods and mechanisms.
→ Pure Appl Chem. 2002 Jan;74(3):349–58.
Furthermore, the advantages of plasma cleaning can be exploited to enhance the softtissue response during the prosthetic implant phase. Change in the surface wettability of commercial pure titanium, in fact, might determine the functional response of fibroblasts and is therefore a critical factor for the adhesion of soft tissue to the titanium abutment.
In the present study, no differences were found between the test and control groups for the first time point (one month of healing). However, at the second time point (two months), despite the absence of statistically significant differences, a trend showing slightly better marginal bone levels in the test group, compared with the control group, was observed. This may explain why a previously published study showed statistically significantly better radiographic bone level maintenance in humans after two- and five-year follow-up at the treated sites.28Canullo L, Tallarico M, Peñarrocha-Oltra D, Monje A, Wang HL, Peñarrocha-Diago M. Implant abutment cleaning by plasma of argon: 5-year follow-up of a randomized controlled trial.
→ J Periodontal. 2016 Apr;87(4):434–42. This may suggest that, in a longer followup, statistical significance could also be reached in experimental studies.
Although a recently published in vitro study presented no quantitative differences in terms of cell adhesion between plasma-cleaned or only sterilized titanium disks after 8 h, the same study reported qualitative differences in terms of cell spreading.29Canullo L, Cassinelli C, Gotz W, Tarnow D. Plasma of argon accelerates murine fibroblast adhesion in early stages of titanium disk colonization.
→ Int J Oral Maxillofac Implants. 2013 Jul-Aug;28(4):957–62. This may suggest that a shorter analysis time frame may only show differences at the microscopical level.
It can be speculated that the differences in terms of IS–B, IS–C and PM–C between the test and control groups, although they did not reach significant levels, could be the early expression of better organization of periimplant soft tissue due to a more “proactive” abutment. This speculation could be supported by the dissimilar outcomes reported by two studies with different time points. In fact, while Canullo et al. reported an absence of histological differences after one week,30Canullo L, Dehner JF, Penarrocha D, Checchi V, Mazzoni A, Breschi L. Soft tissue response to titanium abutments with different surface treatment: preliminary histologic report of a randomized controlled trial.
→ Biomed Res Int. 2016;2016:2952530. doi:10.1155/2016/2952530. Epub 2016 Jun 6. Garcia et al. observed significantly better outcomes after two weeks in terms of connective cell adhesion and soft-tissue arrange ment around abutments cleaned by plasma compared with sterile abutments.31Garcia B, Camacho F, Peñarrocha D, Tallarico M, Perez S, Canullo L. Influence of plasma cleaning procedure on the interaction between soft tissue and abutments: a randomized controlled histologic study.
→ Clin Oral Implants Res. 2016 Aug 23. doi:10.1111/clr.12953.
Epub ahead of print] For this reason, the outcomes of the present investigation should be taken with caution owing to the short follow-up that may have failed to disclose differences.
Conclusion
Within the limitations of the present study, although differences between the test and control groups failed to reach significance, a trend of better marginal bone levels was found at the test sites compared with the control sites. This might suggest that the use of argon plasma might improve the soft-tissue integration of titanium abutments.
Acknowledgments
The authors wish to express their appreciation of the skills and commitment of Dr. Audrenn Gautier in the supervision of the study. Special thanks are given to Mr. Sebastião Bianco (University of São Paulo, Ribeirão Preto, Brazil) for his practical support.
This study was supported by a grant (number 2014/04371-6) from the São Paulo Research Foundation; nevertheless, the authors designed and executed the statistical analysis and manuscript preparation independently, and they have sole responsibility for the writing and content of this article.
Competing interests
The authors declare that they have no competing interests.
Interview
with Martins Neto
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Buser D, Martin W, Belser U. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. → Int J Oral Maxillofac Implants. 2004;19 Suppl:43–61. |
| 2. | ↑ | Abrahamsson I, Berglundh T, Wennström J, Lindhe J. The peri-implant hard and soft tissues at different implant systems. A comparative study in the dog. → Clin Oral Implant Res. 1996 Sep;7(3):212–9. |
| 3. | ↑ | Pozzi A, Tallarico M, Moy PK. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with different prosthetic interfaces and design in partially posterior edentulous mandibles. → Eur J Oral Implantol. 2014 Spring;7(1):47–61. |
| 4. | ↑ | Hermann JS, Cochran DL, Nummikoski PV, Buser D. Crestal bone changes around titanium implants. A radiographic evaluation of unloaded nonsubmerged and submerged implants in the canine mandible. → J Periodontol . 1997 Nov;68(11):1117–30. |
| 5. | ↑ | Manz MC. Factors associated with radiographic vertical bone loss around implants placed in a clinical study. → Ann Periodontol. 2000 Dec;5(1):137–51. |
| 6, 13. | ↑ | Molina A, Sanz-Sánchez I, Martín C, Blanco J, Sanz M. The effect of one-time abutment placement on interproximal bone levels and peri-implant soft tissues: a prospective randomized clinical trial. → Clin Oral Implants Res. 2017 Apr;28(4):443–52. doi:10.1111/clr.12818. Epub 2016 Mar 25. |
| 7. | ↑ | Cochran DL, Hermann JS, Schenk RK, Higginbottom FL, Buser D. Biologic width around titanium implants. A histometric analysis of the implanto-gingival junction around unloaded and loaded nonsubmerged implants in the canine mandible. → J Periodontal. 1997 Feb;68(2):186–98. |
| 8. | ↑ | Schmitt CM, Nogueira-Filho G, Tenenbaum HC, Lai JY, Brito C, Döring H, Nonhoff J. Performance of conical abutment (Morse Taper) connection implants: a systematic review. → J Biomed Mater Res A. 2014 Feb;102(2):552–74. |
| 9. | ↑ | Degidi M, Iezzi G, Scarano A, Piattelli A. Immediately loaded titanium implant with a tissue-stabilizing/maintaining design (‘beyond platform switch’) retrieved from man after 4 weeks: a histological and histomorphometrical evaluation. A case report. → Clin Oral Implants Res. 2008 Mar;19(3):276–82. |
| 10. | ↑ | Vigolo P, Givani A. Platform-switched restorations on wide-diameter implants: a 5-year clinical prospective study. → Int J Oral Maxillofac Implants. 2009 Jan-Feb;24(1):103–9. |
| 11. | ↑ | Canullo L, Fedele GR, Iannello G, Jepsen S. Platform switching and marginal bone-level alterations: the results of a randomized-controlled trial. → Clin Oral Implants Res. 2010 Jan;21(1):115–21. |
| 12. | ↑ | Pozzi A, Agliardi EL, Tallarico M, Barlattani A. Clinical and radiological outcomes of two implants with different prosthetic interfaces and neck configurations: randomized, controlled, split-mouth clinical trial. → Clin Implant Dent Relat Res. 2014 Feb;16(1):96–106. |
| 14. | ↑ | Annibali S, Bignozzi I, Cristalli MP, GrazianiF, La Monaca G, Polimeni A. Peri-implant marginal bone level: a systematic review and meta-analysis of studies comparing platform switching versus conventionally restored implants. → J Clin Periodontol. 2012 Nov;39(11):1097–113. |
| 15, 16. | ↑ | Canullo L, Micarelli C, Lembo-Fazio L, Iannello G, Clementini M. Microscopical and microbiologic characterization of customized titanium abutments after different cleaning procedures. → Clin Oral Implant Res. 2014 Mar;25(3):328–36. doi:10.1111/clr.12089. Epub 2012 Dec 5. |
| 17, 26. | ↑ | Mishra PK, Wu W, Rozo C, Hallab NJ, Benevenia J, Gause WC. Micrometer-sized titanium particles can induce potent th2-type responses through TLR4-independent pathways. → J Immunol. 2011 Dec;187(12):6491–8. |
| 18. | ↑ | Piattelli A, Pontes AE, Degidi M, Iezzi G. Histologic studies on osseointegration: soft tissues response to implant surfaces and components. A review. → Dent Mater. 2011 Jan;27(1):53–60. |
| 19, 25. | ↑ | Canullo L, Micarelli C, Iannello G. Microscopical and chemical surface characterization of the gingival portion and connection of an internal hexagon abutment before and after different technical stages of preparation. → Clin Oral Implants Res. 2013 Jun;24(6):606–11. |
| 20. | ↑ | Tavares JC, Cornélio DA, da Silva NB, de Moura CE, de Queiroz JD, Sá JC, Alves C Jr, de Medeiros SR. Effect of titanium surface modified by plasma energy source on genotoxic response in vitro. → Toxicology. 2009 Aug;262(2):138–45. |
| 21. | ↑ | Canullo L, Genova T, Tallarico M, Gautier G, Mussano F, Botticelli D. Plasma of argon affects the earliest biological response of different implant surfaces: an in vitro comparative study. → J Dent Res. 2016 May;95(5):566–73. |
| 22. | ↑ | Kilkenny C, Browne W, Cuthill IC, Emerson M, Altman DG; National Centre for the Replacement, Refinement and Reduction of Animals in Research. Animal research: reporting in vivo experiments—the ARRIVE guidelines. → J Cereb Blood Flow Metab. 2011 Apr;31(4):991–3. |
| 23. | ↑ | Cleveland JL, Bonito AJ, Corley TJ, Foster M, Barker L, Gordon Brown G, Lenfestey N, Lux L. Advancing infection control in dental care settings: factors associated with dentists’ implementation of guidelines from the Centers for Disease Control and Prevention. → J Am Dent Ass. 2012 Oct:143(10):1127–38. |
| 24. | ↑ | Sawase T, Wennerberg A, Hallgren C, Albrektsson T, Baba K. Chemical and topographical surface analysis of five different implant abutments. → Clin Oral Implants Res. 2000 Feb;11(1):44–50. |
| 27. | ↑ | Moisan M, Barbeau J, Crevier MC, Pelletier J, Philip N, Saoudi N. Plasma sterilization. Methods and mechanisms. → Pure Appl Chem. 2002 Jan;74(3):349–58. |
| 28. | ↑ | Canullo L, Tallarico M, Peñarrocha-Oltra D, Monje A, Wang HL, Peñarrocha-Diago M. Implant abutment cleaning by plasma of argon: 5-year follow-up of a randomized controlled trial. → J Periodontal. 2016 Apr;87(4):434–42. |
| 29. | ↑ | Canullo L, Cassinelli C, Gotz W, Tarnow D. Plasma of argon accelerates murine fibroblast adhesion in early stages of titanium disk colonization. → Int J Oral Maxillofac Implants. 2013 Jul-Aug;28(4):957–62. |
| 30. | ↑ | Canullo L, Dehner JF, Penarrocha D, Checchi V, Mazzoni A, Breschi L. Soft tissue response to titanium abutments with different surface treatment: preliminary histologic report of a randomized controlled trial. → Biomed Res Int. 2016;2016:2952530. doi:10.1155/2016/2952530. Epub 2016 Jun 6. |
| 31. | ↑ | Garcia B, Camacho F, Peñarrocha D, Tallarico M, Perez S, Canullo L. Influence of plasma cleaning procedure on the interaction between soft tissue and abutments: a randomized controlled histologic study. → Clin Oral Implants Res. 2016 Aug 23. doi:10.1111/clr.12953. Epub ahead of print] |





Leave a Reply
Be the First to Comment!