An unusual case of sublingual ranula with submandibular gland involvement
November 26, 2019 / Categories: Digital Dentistry, Implant Dentistry

Lim, Min Jim
Abstract
Background
A ranula is a diffuse swelling on the floor of the mouth resulting from extravasation of mucous secretion from salivary glands. A ranula is commonly presented as a painless, soft, mobile, slow-growing mass on the floor of the mouth. Occasionally, a ranula may present with misleading signs and symptoms. We present an unusual case of intraoral swelling associated with signs of submandibular gland involvement.
Methods
Ranulas of both the submandibular gland and the sublingual gland were suspected and excisions of both glands were planned. Surgical exploration revealed only sublingual gland swelling causing obstruction of the submandibular gland. Sublingual gland removal resulted in complete restoration of salivary flow from the submandibular gland.
Conclusion
This article highlights that misleading signs may lead to unnecessary surgery and cosmetic disfigurement, as submandibular gland excision is approached extraorally. If the pathology is suspected in both glands, an intraoral approach should be opted for first.
Keywords
Ranula; sublingual gland; submandibular gland; obstruction; sialadenitis.
Introduction
A ranula is formed mainly from extravasation of the saliva, forming cyst on the floor of the mouth. It can be derived from either the sublingual gland or the submandibular gland.1Peters E, Kola H, Doyle-Chan W. Bilateral congenital oral mucous extravasation cysts. → Pediatr Dent.
1999 Jul–Aug;21(4):285–8. The most common presentation of a ranula is as a soft, fluctuant, slow-growing mass on the floor of the mouth. If the ranula is left in situ, it may continue enlarging and thus cause compression of the nearby structures. In this paper, we report an unusual case of a ranula that originated from the sublingual gland, but presented with signs and symptoms of submandibular gland involvement.
-

- Fig. 1

-

- Fig. 2

-

- Fig. 3

Case report
A 39-year-old female patient was referred to our oral and maxillofacial surgery department for an intraoral swelling that had persisted, waxing and waning, for 2 years. The swelling had been increasing in size gradually. It was associated with discomfort on the floor of mouth and pain in the right submandibular region. The patient was otherwise in good health with no history of systemic or constitutional symptoms.
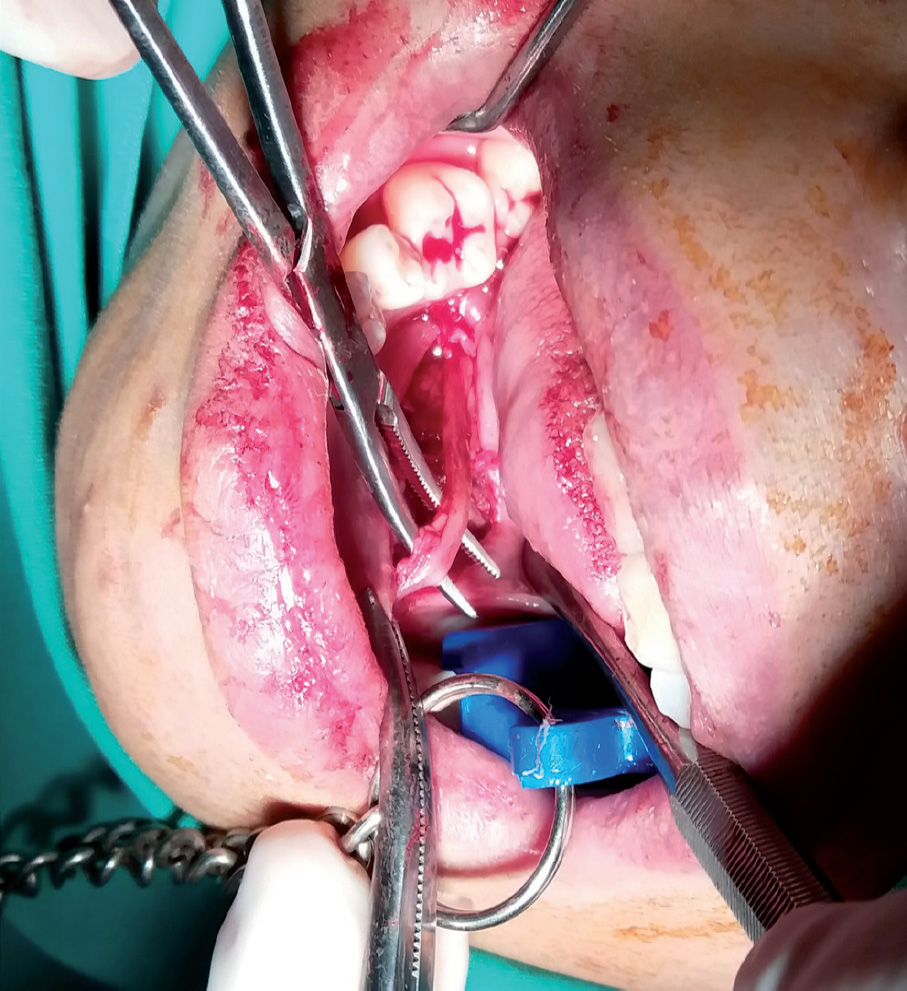
Fig. 4
There was no significant swelling in the head and neck region. However, tenderness was elicited on bimanual palpation over the left submandibular gland region. The overlying skin was normal in both color and temperature. Intraoral examination revealed a diffuse, soft, fluctuant swelling with a size of 4 × 3 cm on the right side of the floor of mouth (Fig. 1). The swelling was not tender or discolored and did not cross the midline. Posteriorly, the swelling extended up to the first molar. The right submandibular duct was not visible, unlike the contralateral duct. On milking of both submandibular glands separately, there was limited flow of saliva from the right submandibular duct opening compared with the left. Radiographic examination showed no sign of calcification (Fig. 2). An initial diagnosis of a ranula with sublingual gland and submandibular gland involvement was made, and surgery was advised.
After preparing the patient for the surgery, adequate local anesthesia was administered in the surrounding region. The lesion was approached intraorally through a mucosal incision directly above the swelling. Blunt dissection was performed carefully in the submucosal plane to reveal an enlarged sublingual gland with multiple well-encapsulated cysts attached to it. The right submandibular duct was located after careful dissection. The right submandibular duct was found to have been displaced by the swollen sublingual gland. It was positioned posteriorly and inferiorly in relation to the sublingual gland. Blunt dissection was performed around the sublingual gland to separate it from the surrounding tissue (Fig. 3). The sublingual gland with its duct was then completely excised. The right submandibular duct was checked again to ensure no dissection (Fig. 4). Immediately after the surgical site had been closed and sutured, there was significant improvement in salivary flow from the right submandibular duct. Histological examination confirmed a ranula with moderate chronic inflammatory infiltration, suggestive of sialadenitis of the sublingual gland. The subsequent follow-up showed full recovery with no complication or recurrence (Fig. 5).

Fig. 5
Discussion
A ranula is a cystic formation that develops from extravasation of saliva due to traumatic rupture of a salivary duct may lead to accumulation of saliva within the tissue. When the saliva-filled cyst herniates through the mylohyoid muscle into the submental or submandibular space, it is termed plunging ranula.2Arunachalam P, Priyadharshini N. Recurrent plunging ranula. → J Indian Assoc Pediatr Surg. 2010 Jan–Mar;15(1):36–8. However, the patient did not recall any trauma to the floor of the mouth. The decision to surgically excise the sublingual gland was made as quickly as possible owing to the fact that the patient experienced tenderness of the submandibular gland region.
The main concern for this patient was the tenderness on the right submandibular region, accompanied by reduced salivary flow from the submandibular duct. These signs indicated that there was a partial obstruction of the right submandibular duct. It was postulated that the enlargement of the sublingual gland had resulted in significant pressure on the submandibular duct. This postulation was proved intraoperatively, as the submandibular duct had been significantly displaced. A similar finding in the literature has been reported regarding a case in which the submandibular duct was compressed by a tumor originating from the sublingual gland.3Kumar VS, Prathi VS, Manne RK, Beeraka S, Natarajan K. Adenoid cystic carcinoma of sublingual salivary gland obstructing the submandibular salivary gland duct. → J Clin Imaging Sci. 2013 Oct;3(Suppl 1):10.
The partial obstruction of the submandibular duct could lead to the formation of a sialolith.4Leung AK, Choi MC, Wagner GA. Multiple sialoliths
and a sialolith of unusual size in submandibular duct: a case report. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999 Mar;87(3):331–3. In this case, the enlarged sublingual gland was compressing the submandibular duct. A sialolith is commonly formed in the submandibular gland, as it produces mainly mucous saliva with a high level of calcium and phosphate. If the surgical removal of the sublingual gland is further delayed, the submandibular duct may become fully obstructed. This may lead to the formation of a sialolith along the submandibular duct and gland, leading to sialadenitis of the submandibular gland.4 Although the occlusal radiograph did not show any radiopaque calculi in this case, it is critical to assess the salivary flow after removal of the sublingual gland. This is because 20% of sialoliths in the submandibular gland system are radiolucent. If the salivary flow is still obstructed, sialography may be required.
Conclusion
This case report highlights that misleading signs may lead to the wrong initial diagnosis. It is important to take into account the surrounding structure when treating a case of ranula. An incorrect diagnosis may lead to unnecessary surgery and cosmetic disfigurement, as submandibular gland excision is usually approached extraorally. If pathology of both glands is suspected, an intraoral approach should be opted for first.
Acknowledgment
We would like to thank the Director General of Health, Ministry of Health, Malaysia, for his permission to publish this article.
Competing interests
The author declares that he has no competing interests.
Figure legends
Fig. 1 – Intraoral swelling on the right side of the floor of the mouth.
Fig. 2 – Occlusal radiograph of the mandible shows no abnormalities.
Fig. 3 – Excision of sublingual gland.
Fig. 4 – Ensuring the right submandibular duct is intact.
Fig. 5 – Postoperative healing after 1 week. Good healing with slight inflammation.
Interview
with Dr. Lim Min Jim
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Peters E, Kola H, Doyle-Chan W. Bilateral congenital oral mucous extravasation cysts. → Pediatr Dent. 1999 Jul–Aug;21(4):285–8. |
| 2. | ↑ | Arunachalam P, Priyadharshini N. Recurrent plunging ranula. → J Indian Assoc Pediatr Surg. 2010 Jan–Mar;15(1):36–8. |
| 3. | ↑ | Kumar VS, Prathi VS, Manne RK, Beeraka S, Natarajan K. Adenoid cystic carcinoma of sublingual salivary gland obstructing the submandibular salivary gland duct. → J Clin Imaging Sci. 2013 Oct;3(Suppl 1):10. |
| 4. | ↑ | Leung AK, Choi MC, Wagner GA. Multiple sialoliths and a sialolith of unusual size in submandibular duct: a case report. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999 Mar;87(3):331–3. |





Leave a Reply
Be the First to Comment!