Comparison of hard- and soft- tissue changes using a superimposition technique: A prospective case series study
September 21, 2016 / Categories: Digital Dentistry, Implant Dentistry

Xhanari, Erta

Pisano, Milena
This prospective case series study reports on a novel comprehensive method using digitized model casts and a superimposition technique to allow an objective evaluation of the hard- and soft-tissue parameters.
Introduction
Esthetic outcomes and patient satisfaction have become the main focus of interest in esthetically sensitive areas.1Chen ST, Buser D. Clinical and esthetic outcomes of implants placed in postextraction sites.
→ Int J Oral Maxillofac Implants. 2009;24 Suppl:186–217.2Den Hartog L, Slater JJ, Vissink A, Meijer HJ, Raghoebar GM. Treatment outcome of immediate, early and conventional single-tooth implants in the aesthetic zone: a systematic review to survival, bone level, soft-tissue, aesthetics and patient satisfaction.
→ J Clin Periodontol. 2008 Dec;35(12):1073–86. The level and thickness of the soft tissue, as well as its color and texture, are decisive for the natural appearance of an implant-supported restoration.3Chang M, Wennström JL, Ödman P, Andersson B. Implant supported single-tooth replacements compared to contralateral natural teeth. Crown and soft tissue dimensions.
→ Clin Oral Implants Res. 1999 Jun;10(3):185–94.
Over the last 20 years, the evaluation of the success of tooth and implant-supported restorations has shifted from judging only the survival rate of the restoration itself to additionally assessing whether an esthetic appearance similar to the adjacent teeth has been achieved. Today, the main concern is whether the surrounding bone architecture and soft-tissue texture and color can precisely and biomimetically emulate nature.4Bazos P, Magne P. Bio-emulation: biomimetically emulating nature utilizing a histoanatomic approach; structural analysis. → Eur J Esthet Dent. 2011 Spring;6(1):8–19. Assessment of esthetically successful treatment outcomes is validated clinically by several objective periodontal and esthetic parameters.5Meijer HJ, Stellingsma K, Meijndert L, Raghoebar GM. A new index for rating aesthetics of implant-supported single crowns and adjacent soft tissues—The Implant Crown Aesthetic Index.
→ Clin Oral Implants Res. 2005 Dec;16(6):645–9.6Gehrke P, Degidi M, Lulay-Saad Z, Dhom G. Reproducibility of the implant crown aesthetic index—Rating aesthetics of single-implant crowns and adjacent soft tissues with regard to observer dental specialization.
→ Clin Implant Dent Relat Res. 2009 Sep;11(3):201–13.7Fürhauser R, Florescu D, Benesch T, Mailath G, Watzek G. Evaluation of soft tissue around single-tooth implant crowns: the Pink Esthetic Score.
→ Clin Oral Implants Res. 2005 Dec;16(6):639–44.However, there is still a lack of clinical comparative studies in the current literature regarding objective outcome evaluation from an esthetic perspective.8Kois JC. Predictable single tooth peri-implant esthetics: five diagnostic keys.
→ Compend Contin Educ Dent. 2001 Mar;22(3):199–206; quiz 208.9Evans CD, Chen ST. Esthetic outcomes of immediate implant placements.
→ Clin Oral Implants Res. 2008 Jan;19(1):73–80.10Kan JY, Rungcharassaeng K, Umezu K, Kois JC. Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans.
→ J Periodontol. 2003 Apr;74(4):557–62.11Belser UC, Schmid B, Higginbottom F, Buser D. Outcome analysis of implant restorations located in the anterior maxilla: a review of the recent literature.
→ Int J Oral Maxillofac Implants. 2004;19 Suppl:30–42.12Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations.
→ Int J Oral Maxillofac Implants. 2004;19 Suppl:43–61.13Chen ST, Darby IB, Reynolds EC. A prospective clinical study of non-submerged immediate implants: clinical outcomes and esthetic results.
→ Clin Oral Implants Res. 2007 Oct;18(5):552–62.
In 2004, the International Team for Implantology presented a treatment guide to provide clinicians with practical and evidence-based clinical instructions for implant restorations in the esthetic zone.14Buser D, Belser U, Higginbottom F. Consensus statements and recommended clinical procedures regarding esthetics in implant dentistry.
→ In: Buser D, Belser U, Wismeijer D, editors. ITI treatment guide. Vol. 1, Implant therapy in the esthetic zone for single-tooth replacements.
Berlin: Quintessence; 2004. p. 73–4. Successful tissue integration and pleasing esthetic outcomes after the application of this treatment protocol have been reported in retrospective15Belser UC, Grütter L, Vailati F, Bornstein MM, Weber HP, Buser D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: a cross-sectional, retrospective study in 45 patients with a 2 to 4 year follow-up using pink and white esthetic scores.
→ J Periodontol. 2009 Jan;80(1):140–51. and prospective16 case series studies. Jemt proposed an index, termed the Papilla Index, to assess the size and volume of the interproximal papillae adjacent to a single tooth. The index defines five distinct levels, ranging from the complete absence of papillary tissue (index score of 0) to hyperplastic papillae (index score of 4).16Jemt T. Regeneration of gingival papillae after single-implant treatment.
→ Int J Periodontics Restorative Dent. 1997 Aug;17(4):326–33. Meijer et al. published the Implant Crown Aesthetic Index, which stipulates criteria related to the implant restoration itself and those associated with the surrounding soft tissue.5 Fürhauser et al. proposed an index, termed the Pink Esthetic Score (PES), focusing essentially on the soft-tissue aspects associated with an anterior single implant supported restoration.17Fürhauser R, Florescu D, Benesch T, Mailath G, Watzek G. Evaluation of soft tissue around single-tooth implant crowns: the Pink Esthetic Score.
→ Clin Oral Implants Res. 2005 Dec;16(6):639–44. Seven distinct soft tissue parameters are considered: the presence or absence of mesial and distal papillae, the level and curvature of the line of emergence of the implant restoration from the mucosa at the facial aspect, the facial soft-tissue convexity (in analogy to a root eminence), and the color and texture of the facial marginal periimplant mucosa.Each parameter score can range from 0 to 2, which results in a maximum score of 14. Finally, Belser et al. proposed a five-variable index, termed the White Esthetic Score (WES), focusing on the visible part of the implant restoration itself and usable in combination with the previously reported PES.18Belser UC, Grütter L, Vailati F, Bornstein MM, Weber HP, Buser D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: a cross-sectional, retrospective study in 45 patients with a 2 to 4 year follow-up using pink and white esthetic scores.
→ J Periodontol. 2009 Jan;80(1):140–51.
The aim of this prospective case series study was to propose a novel comprehensive method using digitized model casts and a superimposition technique to allow an objective evaluation of the hard and soft-tissue parameters for both tooth and implant-supported restorations.
Materials and methods
Fig. 1
Preoperative views revealing worn maxillary anterior teeth.
Fig. 2
Diagnostic wax-up.
Fig. 3
Direct acrylic mock-up.
Fig. 4
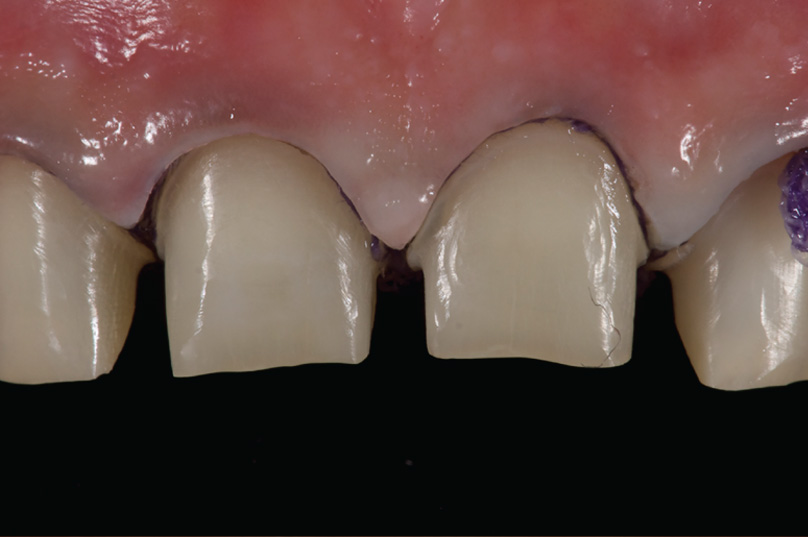
Minimally invasive tooth preparation.
Fig. 5
One-year postoperative intra-oral view.
Any patients requiring all-ceramic restoration of the anterior maxillary teeth were recruited and treated between January 2014 and December 2014. All of the patients were treated in a private dental center in Rome, Italy, by the same clinician (EX). No inclusion or exclusion criteria were considered. Initial photographs and radiographs were taken (Fig. 1). Diagnostic casts were obtained from polyvinyl siloxane impressions (Aquasil Putty DECA and Aquasil Ultra LV/ XLV Regular Set, DENTSPLY International, Milford, Del., U.S.) taken with customized lightcuring acrylic impression trays (Elite LC Tray, Zhermack, Badia Polesine, Italy) fabricated from preliminary casts.
A diagnostic wax-up was performed(Fig. 2) and used to fabricate a silicone guide. Acrylic duplication of the wax-up was performed directly in the patient’s mouth, using the silicone guide (direct mock-up; Fig. 3) in order to test the function and esthetics of the envisioned restorations. Dental preparation was carried out according to a minimally invasive approach (Fig. 4) based on the silicone guide, to avoid over-reducing areas of the teeth. A new cast was obtained for the fabrication of the all-ceramic veneer restorations. The all-ceramic veneer restorations were bonded according to a previously published technique.19Pozzi A, Tallarico M, Barlattani A. Monolithic lithium disilicate full-contour crowns bonded on CAD/CAM zirconia complete-arch implant bridges with 3 to 5 years of follow-up.
→ J Oral Implantol. 2013 Nov;41(4):450–8. One year after delivery of the definitive restorations
(Fig. 5), a new polyvinyl siloxane impression was taken for each patient to allow direct comparison with the pre-treatment scenario.Pre and post-treatment model casts were poured using a conventional single-pouring technique. Vacuum-mixed, low-expansion (0.09%) Type IV dental stone was vibrated into the impression
(CAM-base, Dentona, Dortmund, Germany). The stone casts were allowed to set for 2 h before separation from the impressions.
-

- Fig.1
-

- Fig.2
-

- Fig.3
-
- Fig.4
-

- Fig.5
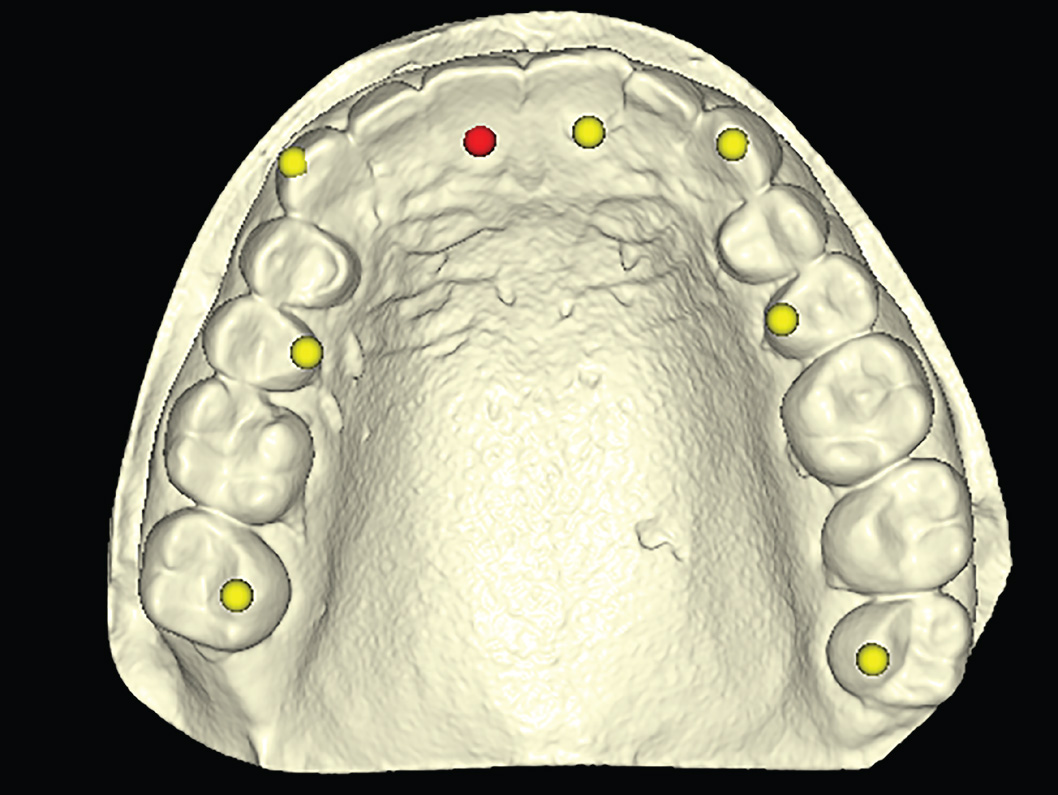
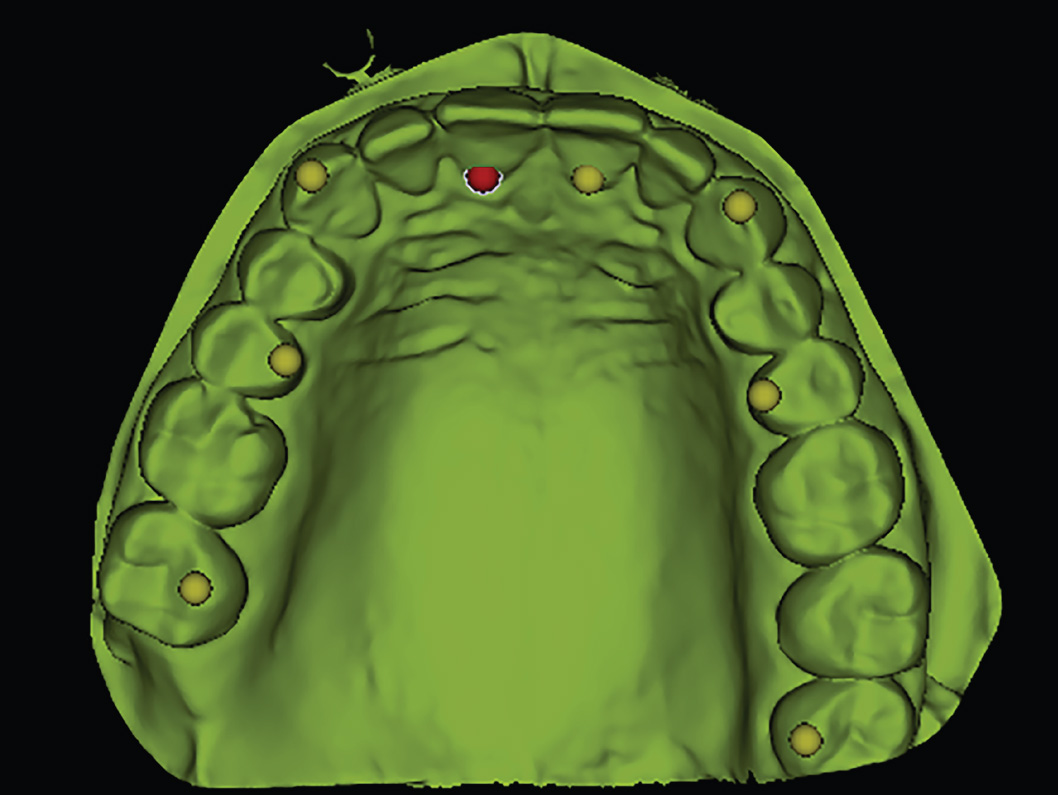
Figs. 6a & 6b
Corresponding points in the DICOM (a) and STL (b) data during superimposition.
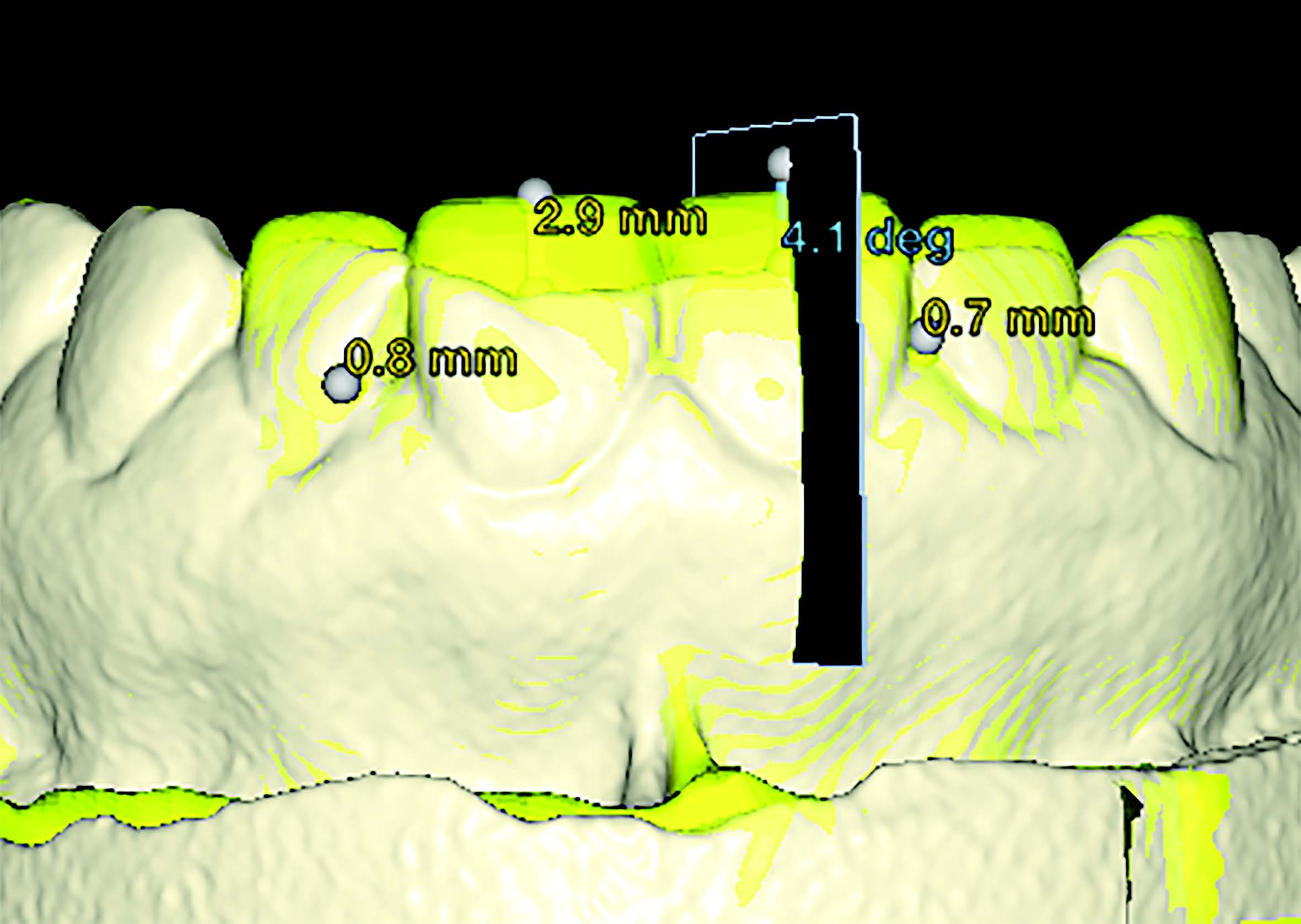
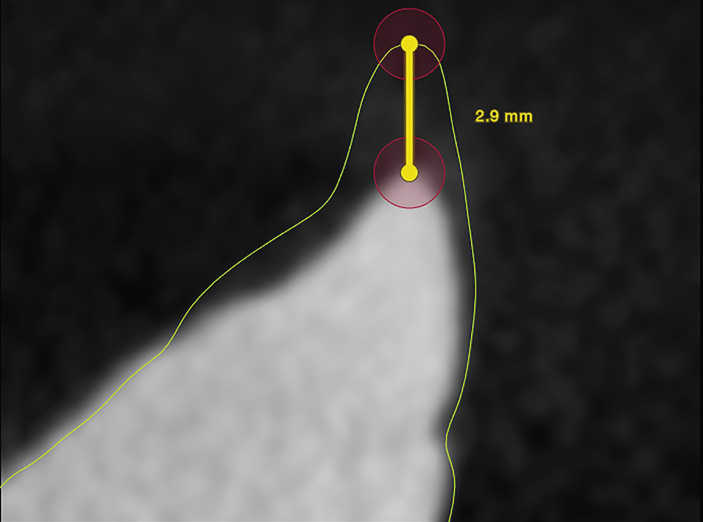
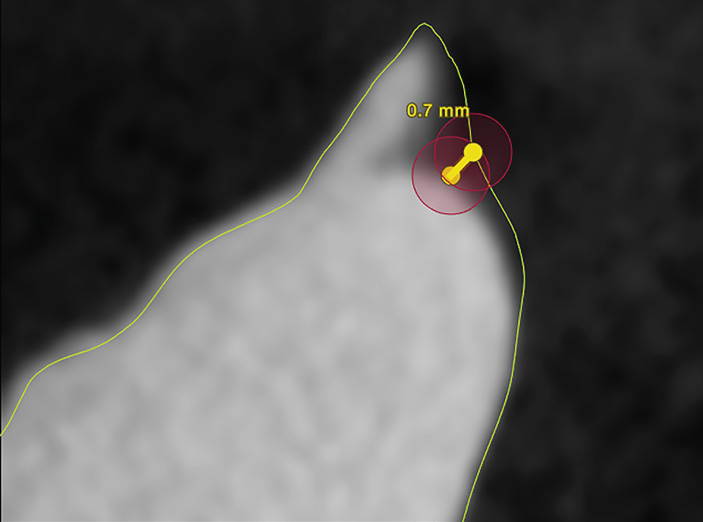
Figs. 7a – 7d
Hard- and soft-tissue measurements of the di erences between the two digitized model casts, calculated on 2-D sections (a) taken along the long axes of the restored teeth
(b & c) and along the papillae (d).
The model casts were then scanned using both a cone beam computed tomography (CBCT) scanner (CRANEX 3D, SOREDEX, Tuusula, Finland) with a 1 mm copper filter and a dental scanner based on conoscopic holography technology (NobelProcera Scanner, Nobel Biocare, Kloten, Switzerland), coupled with dedicated software (NobelProcera).
The DICOM and STL files were imported into NobelClinician Software (Nobel Biocare) to perform the superimposition of the two data sets. The DICOM and STL data were automatically matched based on the adjacent teeth and manually checked for a complete match using SmartFusion technology (Figs. 6a & b). The hard and soft-tissue differences between the two digitized model casts were calculated on 2-D sections taken along the long axes of the restored teeth and along the papillae (Figs. 7a–d).20Kan JY, Rungcharassaeng K, Umezu K, Kois JC. Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans.
→ J Periodontol.2003 Apr;74(4):557–62. An independent assessor, not previously involved in the study, scanned and measured all of the model casts.
-
- Fig.6 a
-
- Fig.6 b
-
- Fig.7 a
-
- Fig.7. b
-

- Fig.7 c
-
- Fig.7 d
Results
Overall, eight patients (two men and six women) with a total of 34 all-ceramic veneer restorations placed in the esthetically sensitive area of the maxilla (between the canines) were followed for at least one year after delivery of the final restorations. Of these, 16 replaced the central incisors, 14 the lateral incisors, and four the canines. One year after delivery of the definitive restorations, no complications were observed (fracture, wear, chipping or debonding). Mean soft-tissue levels improved between bonding and the one-year follow-up examination. The mean height of the mesial and distal papillary changes was 0.64 ± 0.31 and 0.47 ± 0.28, respectively.
Discussion
The present clinical study examined a new objective technique to assess the hard- and soft- tissue changes in natural and artificial dentition. The present technique is not intended to replace previously established methods developed to evaluate the esthetic success of a dental treatment. Conversely, the superimposition of CAD model casts may complement techniques that use subjective methods, such as standardized clinical photographs.
The main limitation of the present technique is the spatial resolution of the scanners and that it does not evaluate color. Nevertheless, the study cast evaluation involved a PES/WES evaluation, facilitating the objective appreciation of crown outline, as well as hard and soft-tissue changes. Esthetics are subjective and linked to the patient, but this technique aims to evaluate the thickness and level of the hard and soft tissue, which is also useful in pre and postoperative comparison (e.g., bone reconstruction and socket preservation).
The results of the present study showed a mean soft-tissue increase at the level of both the mesial and distal papillae between the pre and post-treatment situations. A possible explanation could be the reestablishment of the correct contact points and the renewed instructions on proper oral hygiene.
All of the reference studies21Meijer HJ, Stellingsma K, Meijndert L, Raghoebar GM. A new index for rating aesthetics of implant-supported single crowns and adjacent soft tissues—The Implant Crown Aesthetic Index.
→ Clin Oral Implants Res. 2005 Dec;16(6):645–9.
22Gehrke P, Degidi M, Lulay-Saad Z, Dhom G. Reproducibility of the implant crown aesthetic index—Rating aesthetics of single-implant crowns and adjacent soft tissues with regard to observer dental specialization.
→ Clin Implant Dent Relat Res. 2009 Sep;11(3):201–13.23Fürhauser R, Florescu D, Benesch T, Mailath G, Watzek G. Evaluation of soft tissue around single-tooth implant crowns: the Pink Esthetic Score.
→ Clin Oral Implants Res. 2005 Dec;16(6):639–44. use subjective indexes and require the capture of a series of photographs to compare the di erences between follow-up examinations. If clinical photographs are to provide an accurate record of pre- and postoperative patient appearance, the relative positions of the patient and camera must be kept constant. Perspective distortion may be an un- acceptable drawback, especially in comparison of pre- and post-treatment clinical photographs.24Ahmad I. Digital dental photography. Part 1: an overview.
→ Br Dent J. 2009 Apr;206(8):403–7.
CBCT scanning ensures a comprehensive, high-precision scan of both impressions and plaster casts, delivering accurate 3-D models, which can be used immediately or stored for later use. The scanned 3-D model can be exported as a DICOM set or superimposed onto CBCT data to provide an artifact-free model of the patient’s dentition, including the bone, crowns and soft tissue. The DICOM and STL files can be superimposed too, helping the clinician with clinical and treatment planning, as well as allow- ing for pre- and post-treatment comparison. A straightforward DICOM to STL conversion is easily possible.
Conoscopic holography scanning technology is a valid option for the laboratory digitization of model casts.25Holst S, Persson A, Wichmann M, Karl M. Digitizing implant position locators on master casts: comparison of a noncontact scanner and a contact-probe scanner.
→ Int J Oral Maxillofac Implants. 2012 Jan-Feb;27(1):29–35. This technology projects and reflects light beams from the shape of a complex scanned object along the same linear pathway. This collinearity measures steep angles and deep cavities for precision scanning. Furthermore, it allows, in a few minutes, a full simultaneous digitization of a model cast in a single work session without any manual user intervention.
Superimposition of digitized data using a voxel- based registration method has already been explored in the literature.26Maes F, Collignon A, Vandermeulen D, Marchal G, Suetens P. Multimodality image registration by maximization of mutual information.
→ IEEE Trans Med Imaging. 1997 Apr;16(2):187–98.27Caneva M, Botticelli D, Morelli F, Cesaretti G, Beolchini M, Lang NP. Alveolar process preservation at implants installed immediately into extraction sockets using deproteinized bovine bone mineral—an experimental study in dogs.
→ Clin Oral Implants Res. 2012 Jul;23(7):789–96.28Kim ES, Moon SY, Kim SG, Park HC, Oh JS. Three-dimensional volumetric analysis after sinus grafts.
→ Implant Dent. 2013 Apr;22(2):170–4.29Meloni SM, Tallarico M, Lolli FM, Deledda A, Pisano M, Jovanovic SA. Postextraction socket preservation using epithelial connective tissue graft vs porcine collagen matrix. 1-year results of a randomised controlled trial.
→ Eur J Oral Implantol. 2015 Spring;8(1):39–48.30Szathvary I, Caneva M, Caneva M, Bressan E, Botticelli D, Meneghello R. A volumetric 3-D digital analysis of dimensional changes to the alveolar process at implants placed immediately into extraction sockets.
→ J Oral Science Rehabilitation. 2015 Sep;1(1):62–9. The main advantage is the generation of digital archive of patients for several purposes, including esthetic analysis.
Conclusion
The technique presented o ers an objective evaluation of the hard and soft-tissue changes over time. This technique could complement previously established methods.
Competing interests
The authors declare that they have no competing interests related to this study.
Interview
with Dr. Erta Xhanari
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Chen ST, Buser D. Clinical and esthetic outcomes of implants placed in postextraction sites. → Int J Oral Maxillofac Implants. 2009;24 Suppl:186–217. |
| 2. | ↑ | Den Hartog L, Slater JJ, Vissink A, Meijer HJ, Raghoebar GM. Treatment outcome of immediate, early and conventional single-tooth implants in the aesthetic zone: a systematic review to survival, bone level, soft-tissue, aesthetics and patient satisfaction. → J Clin Periodontol. 2008 Dec;35(12):1073–86. |
| 3. | ↑ | Chang M, Wennström JL, Ödman P, Andersson B. Implant supported single-tooth replacements compared to contralateral natural teeth. Crown and soft tissue dimensions. → Clin Oral Implants Res. 1999 Jun;10(3):185–94. |
| 4. | ↑ | Bazos P, Magne P. Bio-emulation: biomimetically emulating nature utilizing a histoanatomic approach; structural analysis. → Eur J Esthet Dent. 2011 Spring;6(1):8–19. |
| 5, 21. | ↑ | Meijer HJ, Stellingsma K, Meijndert L, Raghoebar GM. A new index for rating aesthetics of implant-supported single crowns and adjacent soft tissues—The Implant Crown Aesthetic Index. → Clin Oral Implants Res. 2005 Dec;16(6):645–9. |
| 6, 22. | ↑ | Gehrke P, Degidi M, Lulay-Saad Z, Dhom G. Reproducibility of the implant crown aesthetic index—Rating aesthetics of single-implant crowns and adjacent soft tissues with regard to observer dental specialization. → Clin Implant Dent Relat Res. 2009 Sep;11(3):201–13. |
| 7, 17, 23. | ↑ | Fürhauser R, Florescu D, Benesch T, Mailath G, Watzek G. Evaluation of soft tissue around single-tooth implant crowns: the Pink Esthetic Score. → Clin Oral Implants Res. 2005 Dec;16(6):639–44. |
| 8. | ↑ | Kois JC. Predictable single tooth peri-implant esthetics: five diagnostic keys. → Compend Contin Educ Dent. 2001 Mar;22(3):199–206; quiz 208. |
| 9. | ↑ | Evans CD, Chen ST. Esthetic outcomes of immediate implant placements. → Clin Oral Implants Res. 2008 Jan;19(1):73–80. |
| 10. | ↑ | Kan JY, Rungcharassaeng K, Umezu K, Kois JC. Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans. → J Periodontol. 2003 Apr;74(4):557–62. |
| 11. | ↑ | Belser UC, Schmid B, Higginbottom F, Buser D. Outcome analysis of implant restorations located in the anterior maxilla: a review of the recent literature. → Int J Oral Maxillofac Implants. 2004;19 Suppl:30–42. |
| 12. | ↑ | Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. → Int J Oral Maxillofac Implants. 2004;19 Suppl:43–61. |
| 13. | ↑ | Chen ST, Darby IB, Reynolds EC. A prospective clinical study of non-submerged immediate implants: clinical outcomes and esthetic results. → Clin Oral Implants Res. 2007 Oct;18(5):552–62. |
| 14. | ↑ | Buser D, Belser U, Higginbottom F. Consensus statements and recommended clinical procedures regarding esthetics in implant dentistry. → In: Buser D, Belser U, Wismeijer D, editors. ITI treatment guide. Vol. 1, Implant therapy in the esthetic zone for single-tooth replacements. Berlin: Quintessence; 2004. p. 73–4. |
| 15, 18. | ↑ | Belser UC, Grütter L, Vailati F, Bornstein MM, Weber HP, Buser D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: a cross-sectional, retrospective study in 45 patients with a 2 to 4 year follow-up using pink and white esthetic scores. → J Periodontol. 2009 Jan;80(1):140–51. |
| 16. | ↑ | Jemt T. Regeneration of gingival papillae after single-implant treatment. → Int J Periodontics Restorative Dent. 1997 Aug;17(4):326–33. |
| 19. | ↑ | Pozzi A, Tallarico M, Barlattani A. Monolithic lithium disilicate full-contour crowns bonded on CAD/CAM zirconia complete-arch implant bridges with 3 to 5 years of follow-up. → J Oral Implantol. 2013 Nov;41(4):450–8. |
| 20. | ↑ | Kan JY, Rungcharassaeng K, Umezu K, Kois JC. Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans. → J Periodontol.2003 Apr;74(4):557–62. |
| 24. | ↑ | Ahmad I. Digital dental photography. Part 1: an overview. → Br Dent J. 2009 Apr;206(8):403–7. |
| 25. | ↑ | Holst S, Persson A, Wichmann M, Karl M. Digitizing implant position locators on master casts: comparison of a noncontact scanner and a contact-probe scanner. → Int J Oral Maxillofac Implants. 2012 Jan-Feb;27(1):29–35. |
| 26. | ↑ | Maes F, Collignon A, Vandermeulen D, Marchal G, Suetens P. Multimodality image registration by maximization of mutual information. → IEEE Trans Med Imaging. 1997 Apr;16(2):187–98. |
| 27. | ↑ | Caneva M, Botticelli D, Morelli F, Cesaretti G, Beolchini M, Lang NP. Alveolar process preservation at implants installed immediately into extraction sockets using deproteinized bovine bone mineral—an experimental study in dogs. → Clin Oral Implants Res. 2012 Jul;23(7):789–96. |
| 28. | ↑ | Kim ES, Moon SY, Kim SG, Park HC, Oh JS. Three-dimensional volumetric analysis after sinus grafts. → Implant Dent. 2013 Apr;22(2):170–4. |
| 29. | ↑ | Meloni SM, Tallarico M, Lolli FM, Deledda A, Pisano M, Jovanovic SA. Postextraction socket preservation using epithelial connective tissue graft vs porcine collagen matrix. 1-year results of a randomised controlled trial. → Eur J Oral Implantol. 2015 Spring;8(1):39–48. |
| 30. | ↑ | Szathvary I, Caneva M, Caneva M, Bressan E, Botticelli D, Meneghello R. A volumetric 3-D digital analysis of dimensional changes to the alveolar process at implants placed immediately into extraction sockets. → J Oral Science Rehabilitation. 2015 Sep;1(1):62–9. |





Leave a Reply
Be the First to Comment!