Comprehensive rehabilitation and natural esthetics with implant and orthodontics (CRANIO):
An interdisciplinary approach to missing maxillary lateral incisors
March 22, 2017 / Categories: Digital Dentistry, Implant Dentistry

Tallarico, Marco

Luzi, Cesare

Galasso, Giorgia

Lione, Roberta

Cozza, Paola
The absence of the maxillary lateral incisors creates a functional and esthetic problem that can be managed with different treatment modalities.
Introduction
Congenital tooth agenesis is a common dental anomaly, with reported incidences of 2.7% to 12.2%, excluding third molars.
In the permanent dentition, maxillary lateral incisors are the most commonly affected,1Kiliaridis S, Sidira M, Kirmanidou Y, Michalakis K. Treatment options for congenitally missing lateral incisors.
→ Eur J Oral Implantol. 2016;9 Suppl 1:S5–24. with a prevalence rate of between 1% and 4%2Muller TP, Hill IN, Peterson AC, Blayney JR. A survey of congenitally missing permanent teeth.
→ J Am Dent Assoc. 1970 Jul;81(1):101–7. and a female predominance of approximately 2:1 compared with males.3Stamatiou J, Symons AL. Agenesis of the permanent lateral incisor: distribution, number and sites.
→ J Clin Pediatr Dent. 1991 Summer;15(4):244–6.This anomaly is not usually an isolated phenomenon, but is associated with other dental anomalies, such as peg-shaped contralateral incisors.4Kiliaridis S, Sidira M, Kirmanidou Y, Michalakis K. Treatment options for congenitally missing lateral incisors.
→ Eur J Oral Implantol. 2016;9 Suppl 1:S5–24. Therefore, the concurrence of several dental anomalies in the same subject results in functional and esthetic problems, which may in turn affect the patient’s self-confidence and social relationships from a very young age.
Treatment options for missing lateral incisors include space opening, followed by the placement of a conventional fixed bridge or a single- unit implant-supported crown, and orthodontic space closure with anatomical recontouring of the canines.5Andrade DC, Loureiro CA, Araújo VE, Riera R, Atallah AN. Treatment for agenesis of maxillary lateral incisors: a systematic review.
→ Orthod Craniofac Res. 2013 Aug;16(3):129–36. Selecting the most appropriate therapy is still a challenge. Numerous clinical characteristics must be analyzed, such as the patient’s age, occlusal relationships, profile, smile line, presence or absence of third molars, and size, shape and color of the canines.6Silveira GS, Mucha JN. Agenesis of maxillary lateral incisors: treatment involves much more than just canine guidance.
→ Open Dent J. 2016 Feb;10:19–27.
In order to maximize the esthetic and functional results, an interdisciplinary approach involving an orthodontist, an oral surgeon and a restorative dentist has become essential. Comprehensive rehabilitation and natural esthetics with implant and orthodontics (CRANIO) is a philosophy based on interdisciplinary treatments to achieve stable occlusion and healthy hard and soft tissue and to enhance the natural esthetic appearance and subsequent patient satisfaction.
The aim of the present study was to describe an interdisciplinary approach to a clinical case presenting with a missing maxillary lateral incisor treated in two phases: orthodontic space opening, followed by placement of a narrow 3 mm diameter implant and restored with a screw-retained lithium disilicate crown veneered on a zirconia abutment.
Case report
A 24-year-old Caucasian female was referred to our private clinic to seek a second opinion for treatment, with the chief complaint of an unattractive smile and the mobility of the primary maxillary right canine. Clinical examination and radiographs confirmed the advanced root resorption of the primary maxillary right canine, the agenesis of the permanent maxillary right lateral incisor, with the presence of the permanent canine in place of the lateral incisor, and microdontia of the maxillary left lateral incisor (Figs. 1a–c). Intraoral observation revealed an Angle Class II relationship of the molars and canine, an increased overjet, a normal overbite and a lower dental midline that was displaced 3 mm to the left compared with the upper midline.
-

- Fig. 1a

-

- Fig. 1b

-

- Fig. 1c

Preoperative intraoral view: frontal (a), right (b) and left (c).
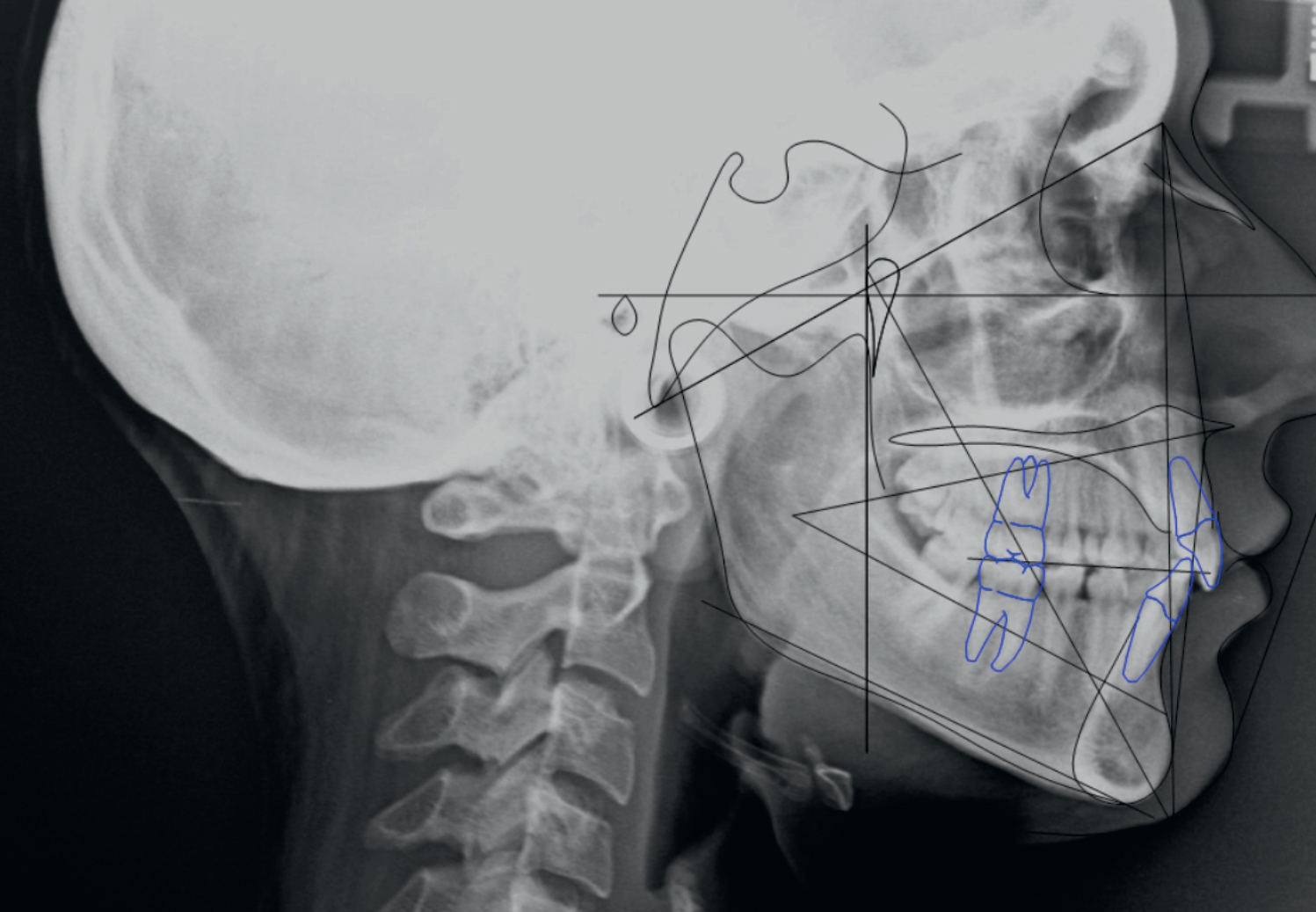
Figs. 2
Cephalometric analysis.
Cephalometric analysis (Dolphin Imaging 11.7, Dolphin Imaging and Management Solutions, Chatsworth, Calif., U.S.) highlighted a mesofacial facial pattern, with a Class II sagittal skeletal relationship (Fig. 2). The patient presented with a symmetrical and proportional face and flat facial profile, with the upper lip positioned 4 mm and the lower lip 2 mm behind the Ricketts E-line.
-
- Fig. 2
The previously proposed treatment was extraction of the primary canine with space maintenance for a future implant rehabilitation and canine substitution with a veneer restoration. In contrast to this, the alternative treatment proposed was extraction of the primary canine, followed by orthodontic space recovery for implant placement in the lateral incisal area, with alignment and leveling of the dental arches. The option of correcting the Class II relationship would have required orthognathic surgery, which was refused by the patient.
The patient was initially very skeptical toward such a comprehensive treatment option. However, after discussion with both the orthodontist (CL) and implantologist (MT) of the advantages and disadvantages of all of the available treatment options, it became clear to the patient that the overall advantages of the proposed interdisciplinary treatment, involving orthodontic treatment, implant placement and prosthetic rehabilitation, would provide improved esthetic and functional results.
The disadvantages of the proposed treatment were related to costs and a longer treatment time.
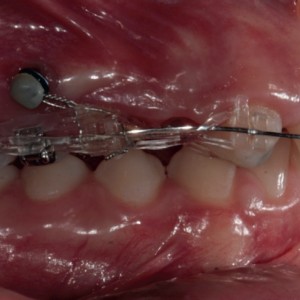
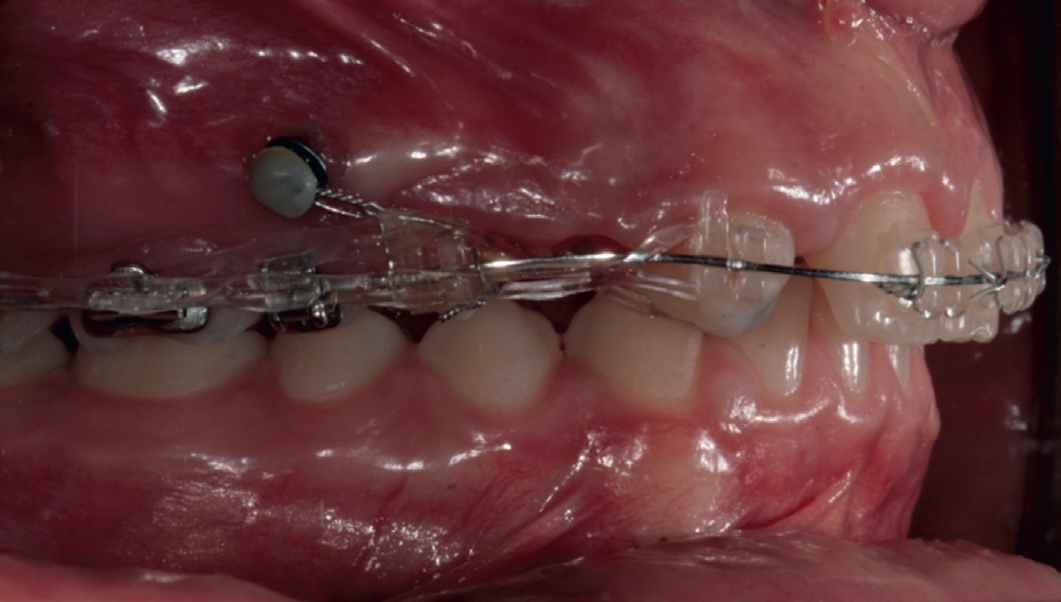
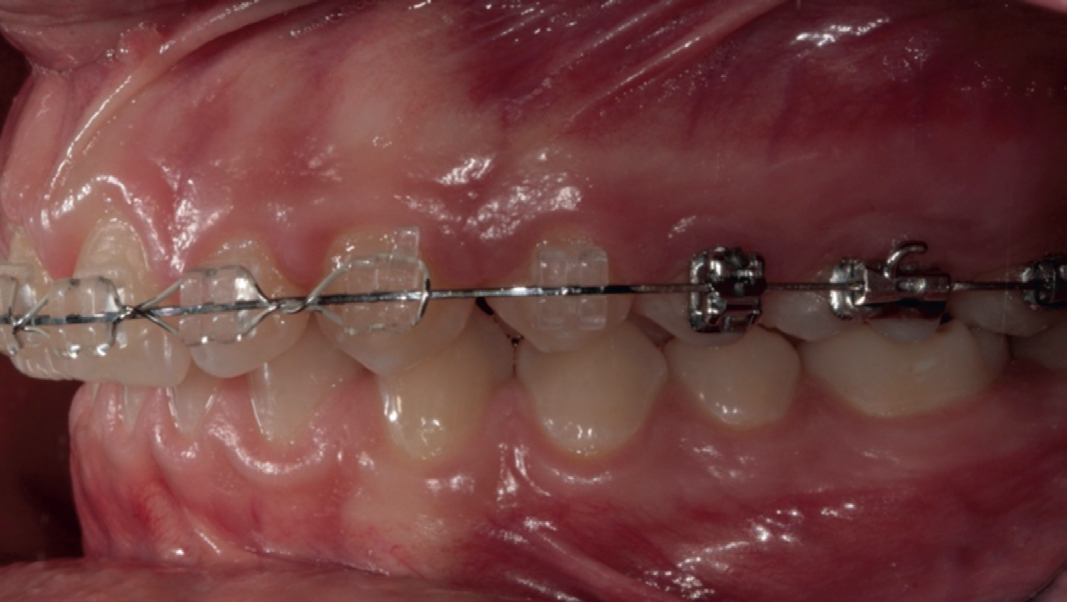
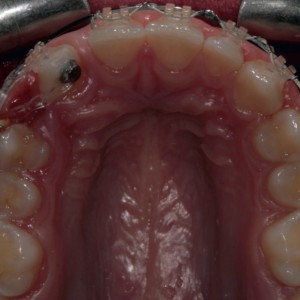
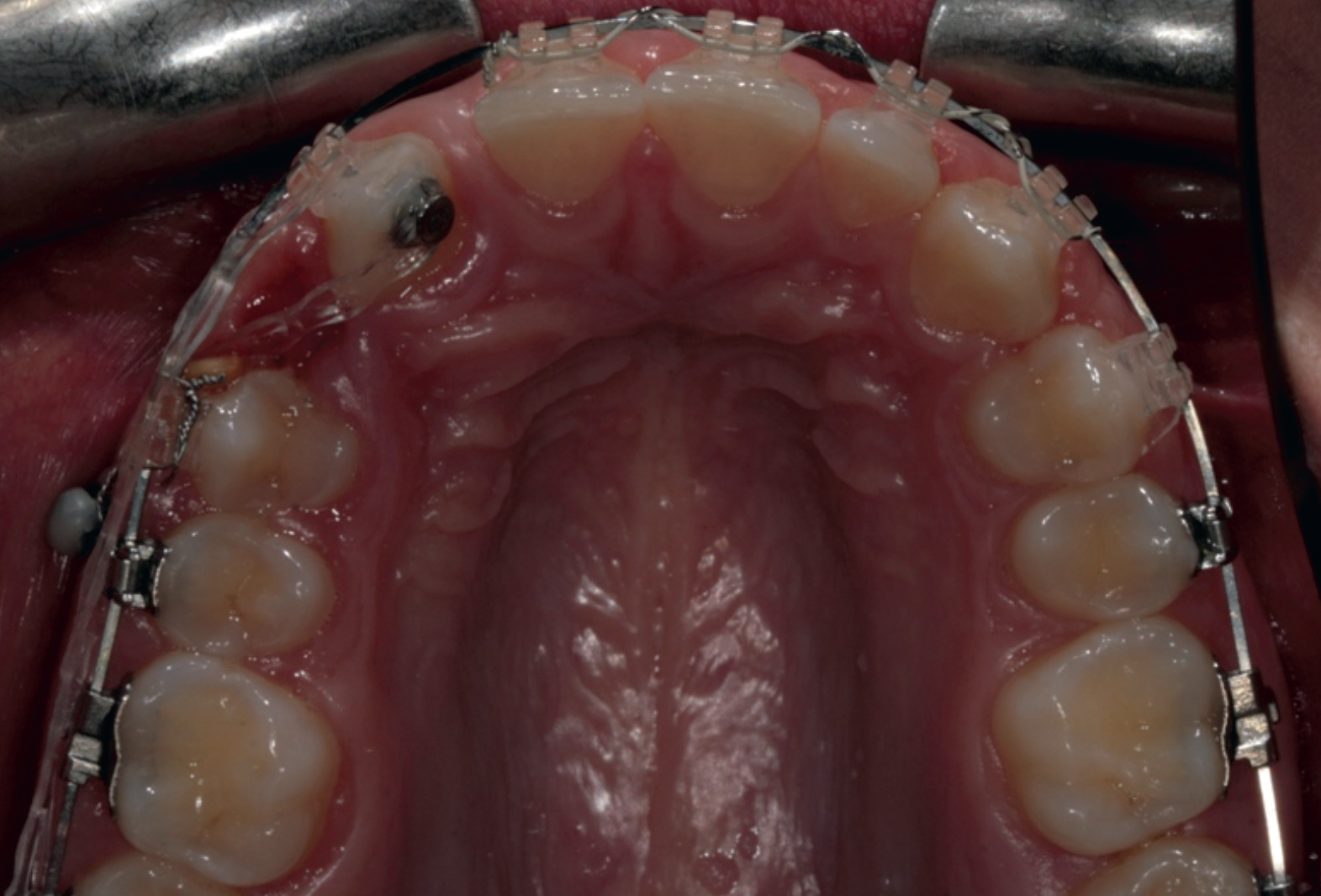
The orthodontic treatment lasted 18 months. After the extraction of the primary canine, fullarch bonding with a fixed esthetic multibracket appliance was performed, and the maxillary right canine was strategically bonded with a mesial tip back to enhance root control. Skeletal anchorage by means of an orthodontic miniscrew (Aarhus System, American Orthodontics, Sheboygan, Wisconsin, U.S.; 1.5 mm diameter, 6.0 mm thread length) was used during canine retraction with sliding mechanics to avoid side effects (i.e., worsening of the molar relationship). Both direct and indirect traction to the miniscrew were used with derotation elastomeric chains for enhanced control of the final crown and root position (Figs. 3 & 4a–c). The finishing phase was accomplished with braided multistrand stainless-steel 0.018 × 0.025 in. arch wires and intermaxillary elastics. An upper Hawley plate was used for retention after appliance removal in the maxillary arch, and a mandibular fixed retainer was bonded in the mandibular anterior segment.
-
- Fig. 3
-
- Fig. 4a
-

- Fig. 4b
-
- Fig. 4c
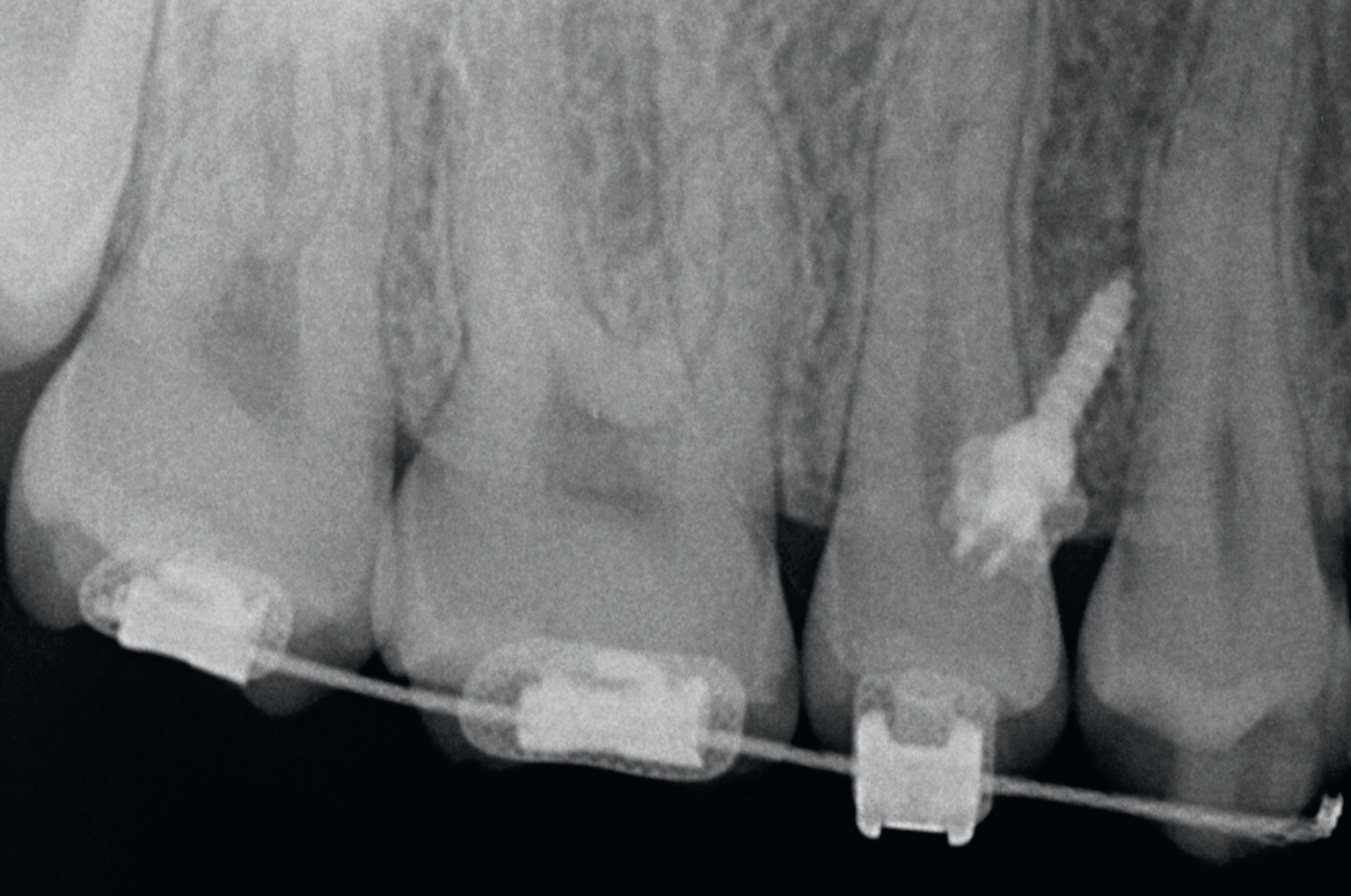
Periapical radiograph showing the orthodontic miniscrew.
Figs. 4a-c
Orthodontic treatment: right (a), left (b) and occlusal (c) view.
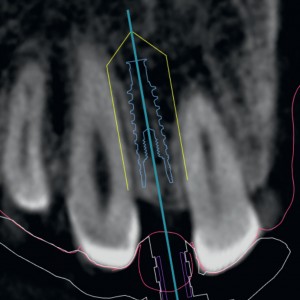
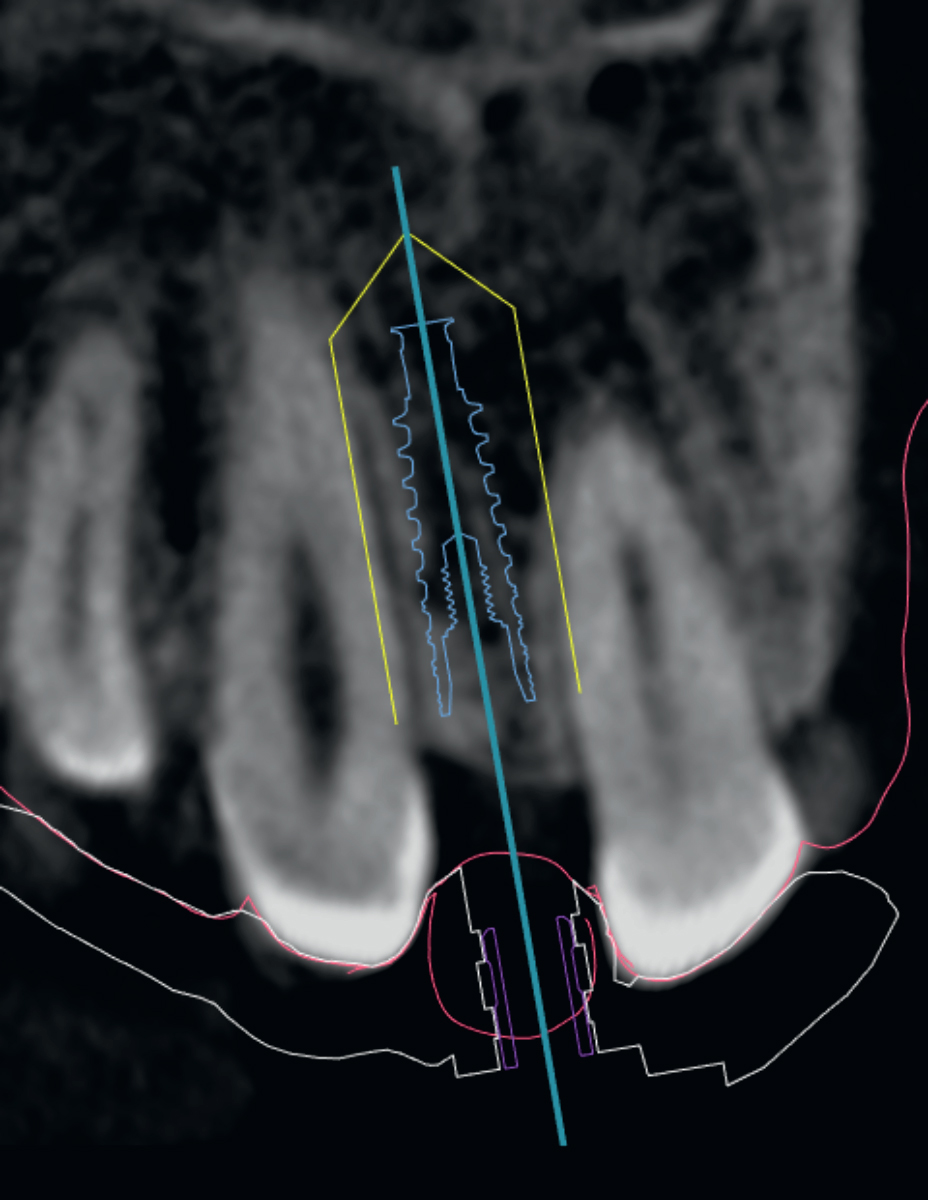
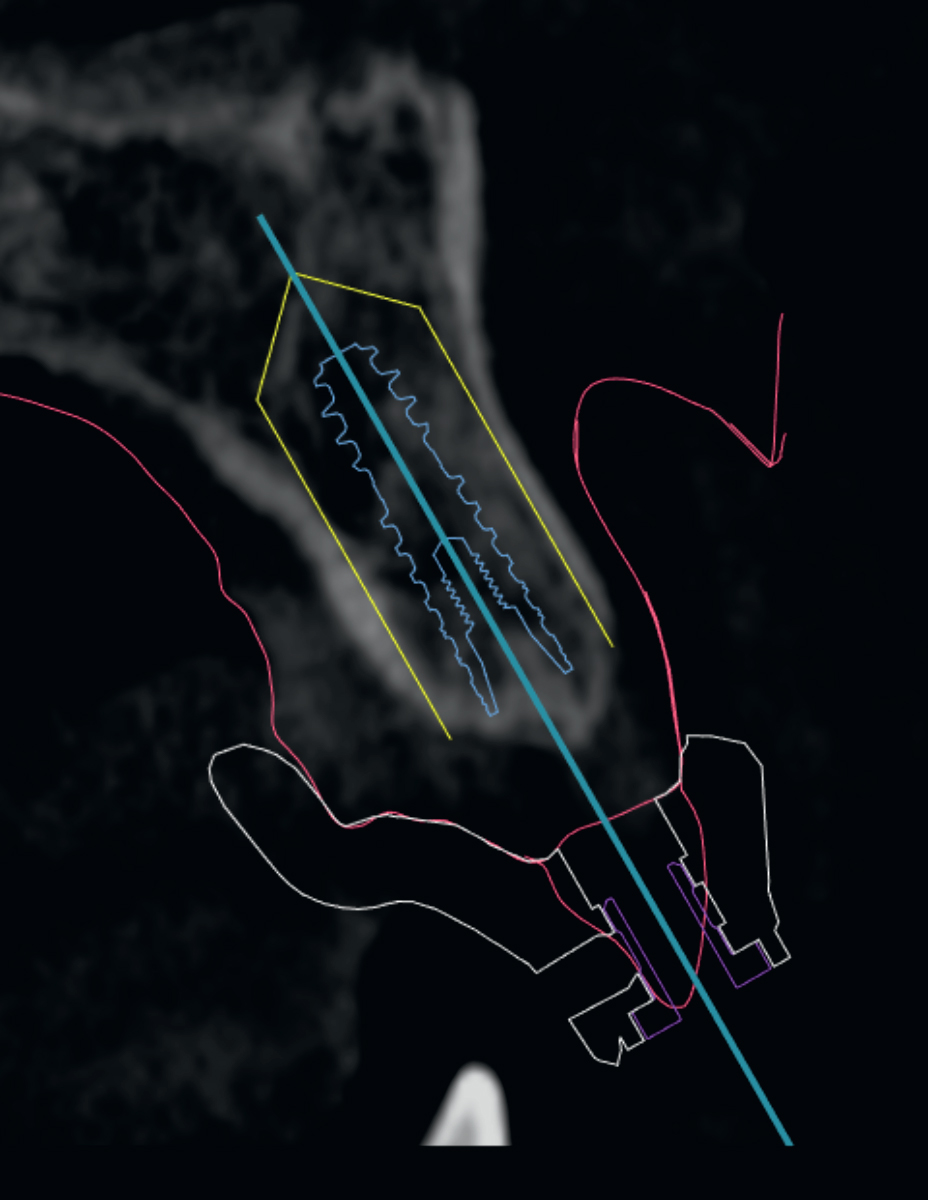
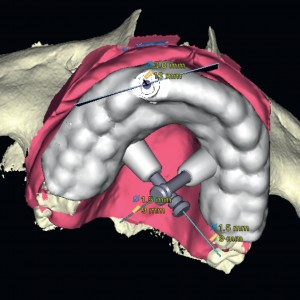
After orthodontic treatment, the patient underwent a preoperative cone beam computed tomography (CBCT; CRANEX 3Dx, SOREDEX, Tuusula, Finland) scan, and diagnostic impressions were taken using a polyether material (Impregum, 3M ESPE, Seefeld, Germany) with a custom open tray (Diatray Top, Dental Kontor, Stockelsdorf, Germany). Furthermore, model casts were poured in Type IV stone (Techim Super Stone, Techim Group, Milan, Italy) and a diagnostic wax-up was made. The STL files derived from the scanned model and wax-up were merged with the DICOM data derived from the CBCT scan in the same virtual implant planning software (NobelClinician, Nobel Biocare, Kloten, Switzerland). Virtual planning was completed by defining a prosthetically driven implant placement. Owing to the reduced space between adjacent roots, a 3.0 mm implant was planned (Osstem TSIII, Osstem, Seoul, South Korea). After careful functional and esthetic evaluation and final verification, the approved virtual plan was transmitted to a milling center (Nobel Biocare) for the production of a stereolithographic surgical template (Figs. 5a–c).
-
- Fig. 5a
-

- Fig. 5b
-
- Fig. 5c

Virtual plan: frontal (a) and sagittal views (b); virtual stereolithographic surgical template (c).
Before implant placement, the stereolithographic surgical template was adapted to the master cast.
The patient underwent professional oral hygiene and received prophylactic antiseptic (0.2% chlorhexidine for 1 min) and antibiotic therapy (2 g of amoxicillin and clavulanic acid). Local anesthetic was administered with a 4% articaine solution with epinephrine 1:100 000 (Ubistein, 3M ESPE). The surgical template was placed intraorally in relation to the opposing arch using the silicone surgical index derived from the mounted casts and stabilized with two anchor pins. A flapless guided pilot drill was employed using the surgical template, and the continuity of the implant site was evaluated with the aid of a periodontal probe (PCPUNC156, Hu-Friedy, Milan, Italy). The implant was placed freehand in the planned anatomical site according to a one-stage approach, without tissue grafting. The final insertion torque was 37.5 N cm (iChiro Pro, Bien-Air Dental, Biel, Switzerland).
A new definitive impression of the maxilla was made using a polyether material (Impregum) and poured in Type IV stone (Techim Super Stone).
This master cast was cross-mounted in a semi-adjustable articulator and a temporary acrylic restoration was fabricated using a temporary titanium abutment (Osstem). The temporary restoration was screwed to the implant with prosthetic screws tightened according to the manufacturer’s instructions (30 N cm) 24 h after implant placement, as directed by an immediate loading protocol. The prefabricated temporary acrylic restoration was trimmed and polished chairside.
A nonoccluding occlusal scheme was delivered (Fig. 6). After implant placement, the patient received oral and written instructions regarding medication, oral hygiene maintenance and diet. A periapical radiograph was taken with the paralleling technique in order to exclude radiolucency or other complications.
-
- Fig. 6
Immediately loaded temporary restoration.
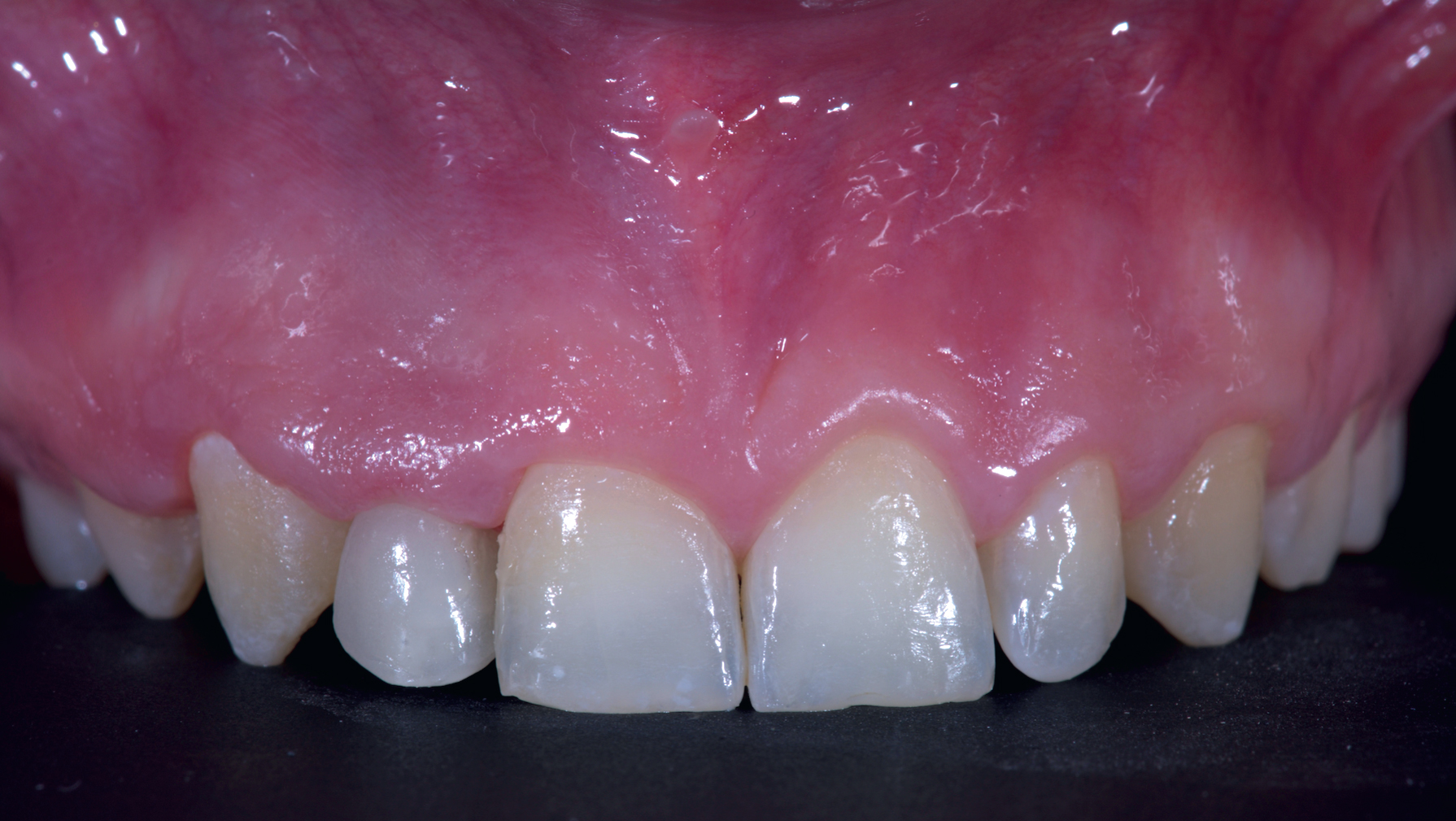
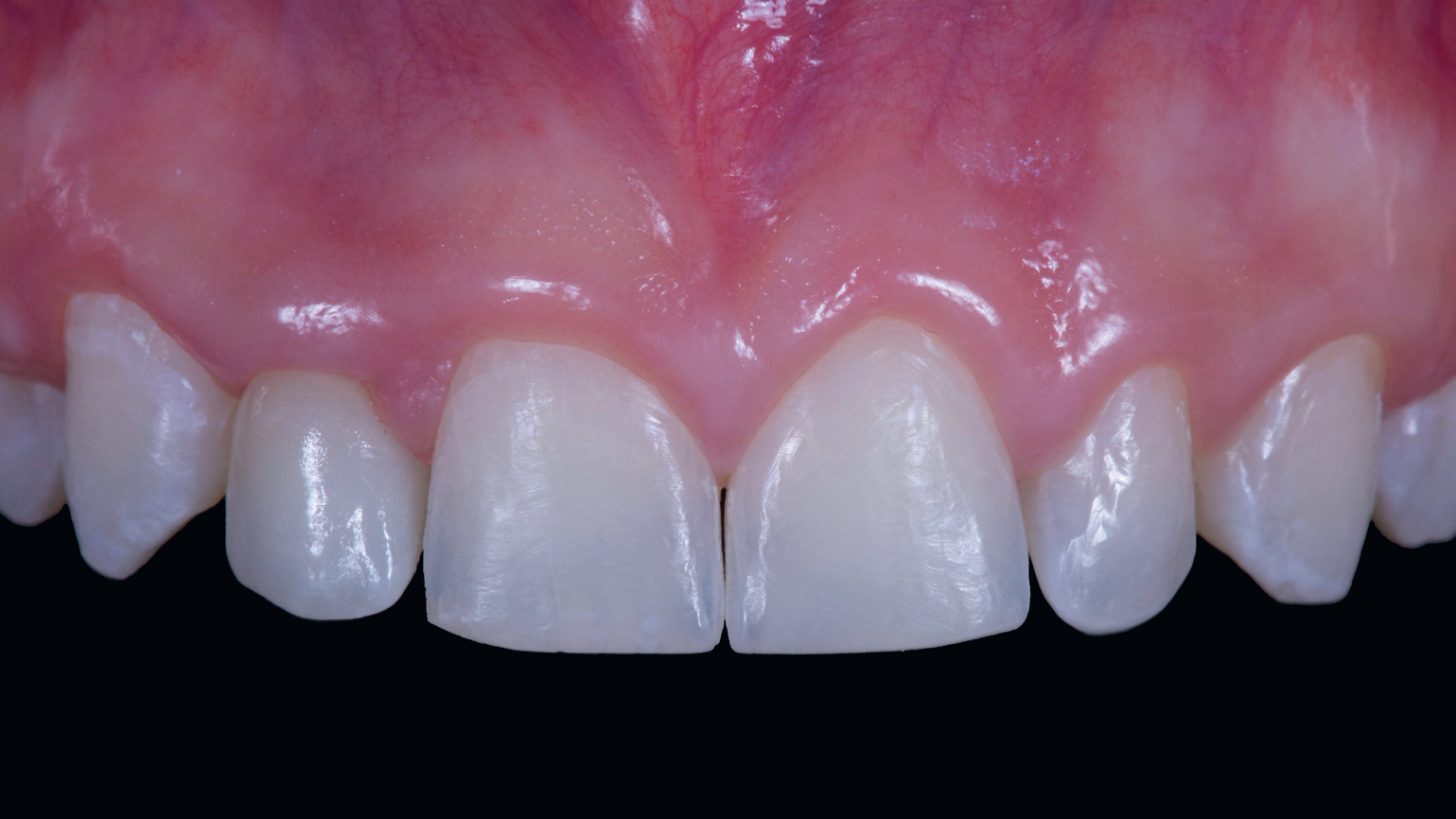
The final restoration was delivered three months after implant placement. The zirconia framework was fabricated using CAD/CAM technology (New Ancorvis, Bargellino, Italy) and veneered with ceramic. The screw-retained definitive restoration was finally attached at the torque setting recommended by the manufacturer (30 N cm; Figs. 7 & 8). The occlusion was carefully adjusted and the patient was recalled every 4 months for hygiene maintenance and annually for occlusal adjustment (Figs. 9 &10).
-

- Fig. 7

-

- Fig. 8

-

- Fig. 9
-
- Fig. 10

Definitive restoration.
Figs. 8
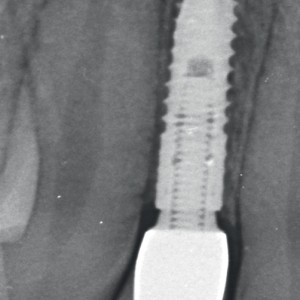
Periapical radiograph.
Figs. 9
Definitive restoration 1 year after implant placement.
Figs. 10
Periapical radiograph 1 year after implant placement.
Discussion
In the present report, the case was treated successfully with orthodontic space opening and prosthetic replacement of the missing lateral incisor with a single implant-supported crown. This case report aimed to describe the novel Osstem TSIII 3.0 mm (Osstem) implant used, which allows for the replacement of maxillary lateral incisors and mandibular incisors. Prompt diagnosis and an interdisciplinary approach, guided by functional and esthetic demands, are essential for the proper management of such complex cases. Teenagers with late mixed dentition or newly developed permanent dentition often seek treatment for the congenital absence of maxillary lateral incisors, because, during this period, the esthetic problem becomes more evident.
When maxillary lateral incisors are missing, there are several factors to consider before treatment with space opening or closure. These factors include the type of malocclusion, crowing/spacing, tooth size relationships, canine position, shape and color of the canines, and upper lip length.7Thordarson A, Zachrisson BU, Mjor IA. Remodeling of canines to the shape of lateral incisors by grinding: a long-term clinical and radiographic evaluation.
→ Am J Orthod Dentofacial Orthop. 1991 Aug;100(2):123–32.8Kokich VO Jr. Congenitally missing teeth: orthodontic management in the adolescent patient.
→ Am J Orthod Dentofacial Orthop. 2002 Jun;121(6):594–5.9Robertsson S, Mohlin B. The congenital missing upper lateral incisor. A retrospective study of orthodontic space closure versus restorative treatment.
→ Eur J Orthod. 2000 Dec;22(6):697–710. The choice between these two modalities of treatment should not be made empirically. In most instances, the presence or absence of major occlusal problems serves as the primary criterion for either space closure or space opening. 10Zachrisson BU. Improving orthodontic results in cases with maxillary incisors missing.
→ Am J Orthod. 1978 Mar;73(3):274–89. Lateral incisal spaces should be closed in cases in which malocclusions require the extraction of permanent mandibular teeth.11Andrade DC, Loureiro CA, Araújo VE, Riera R, Atallah AN. Treatment for agenesis of maxillary lateral incisors: a systematic review.
→ Orthod Craniofac Res. 2013 Aug;16(3):129–36. Mandibular extractions may be indicated to relieve anterior or posterior arch length deficiency, to reduce mandibular dentoalveolar protrusion or to compensate for a Class II molar relationship. Some orthodontic patients may be missing several permanent teeth, including maxillary lateral incisors. If teeth have been missing for several years, the remaining teeth may have drifted. In these patients, orthodontists and restorative dentists may not know what the restorative requirements are or what the eventual restorative treatment plan should be. For these types of patients, it is suggested to predetermine the final occlusal and restorative outcomes by creating diagnostic wax setups.12Kokich VG, Spear FM. Guidelines of managing the orthodontic-restorative patient.
→ Semin Orthod. 1997 Mar;3(1):3–20. In addition, the trial setup will allow identification of tooth surfaces that require functional and esthetic reduction so that equilibration may be initiated either at the beginning of or during the orthodontic treatment.
The diagnosis and treatment of growing children with missing lateral incisors can be a problem for many clinicians. If the patient and his or her parents plan on him or her undergoing implant treatment in the future, it is important that the majority of vertical facial growth and tooth eruption be completed before implant placement.13Kokich VO Jr. Congenitally missing teeth: orthodontic management in the adolescent patient.
→ Am J Orthod Dentofacial Orthop. 2002 Jun;121(6):594–5. After completion of growth in body height, sequential cephalometric or hand–wrist radiographs verify the cessation of facial growth over a time frame of approximately six months to one year. The sequence of treatment in cases of agenesis of anterior teeth must be carefully explained to both the patient and his or her parents. They must realize that the orthodontic treatment is the beginning of the process, which is to be followed by the scheduling of periodontal therapy and final restorations. It is crucial that all of the treatment options be discussed with the interdisciplinary team, just as all of the options are explained in the orthodontic treatment phase.
Space closure is recommended for missing lateral incisors in subjects with long faces, as it is the preferred treatment for preserving arch anchorage and avoiding clockwise rotation of the lower jaw. In addition, it is the treatment of choice in subjects with bimaxillary dental protrusion in order to avoid worsening of the profile or in cases of early treatment in adolescents. Space closure can also be considered with two types of malocclusions: a mandibular anterior with severe dental crowding and a Class I malocclusion, for which the first premolars and canines are extracted to achieve mesialization (thus obtaining a molar and canine Class I), as well as a Class II malocclusion without crowding and mandibular protrusion. Furthermore, space closure may benefit patients with a specific anterior relationship, specifically those with an increased overjet and reduced overbite. Lastly, the presence of third molars is an additional factor that would be supported by space closure mechanics. The color of the natural canine should be approximately that of the central incisor. It is not uncommon for the canine to be more saturated with color, resulting in a tooth that is one to two shades darker than the central incisor.
Space opening (between the canine and central incisor) is the second therapeutic option in the treatment of missing lateral incisors. Space opening and prosthodontic intervention are indicated in low-angle subjects and those with retruded profiles in order to improve the labial sagittal relationship. It is also the treatment of choice in patients with molar Class I or III tendency in order to preserve an ideal occlusal anterior and posterior relationship. Space opening is also of benefit in cases with a reduced overjet and increased overbite. As mentioned previously, an important factor that clinicians should consider when deciding on treatment is the patient’s age. Space opening is not recommended before the age of 13 years in order to prevent the relapse and progression of bone atrophy.11 In the case of unilateral tooth agenesis, space opening is often recommended in order to improve the esthetics and preserve smile symmetry.14Rosa M, Zachrisson BU. The space-closure alternative for missing maxillary lateral incisors: an update.
→ J Clin Orthod. 2010 Sep;44(9):540–9; quiz 561.
According to Magne and Belser, there are various subjective and objective criteria for the assessment of an ideal smile.15Magne P, Belser U. Bonded porcelain restorations in the anterior dentition: a biomimetic approach.
→ Chicago: Quintessence. 2002. 406 p. The midline is an imaginary line located at the center of the face, perpendicular to the interpupillary line. In a totally symmetrical face, the dental midline and the facial midline should coincide, but this is often not the case.16Pinho S, Ciriaco C, Faber J, Lenza MA. Impact of dental asymmetries on the perception of smile esthetics.
→ Am J Orthod Dentofacial Orthop. 2007 Dec;132(6):748–53. According to Spear et al., a midline deviation greater than 4 mm can be detected by the general public,17Spear FM, Kokich VG, Mathews DP. Interdisciplinary management of anterior dental aesthetics.
→ J Am Dent Assoc. 2006 Feb;137(2):160–9. whereas a midline deviation of 2 mm remains undetectable by laypersons.18Pinho S, Ciriaco C, Faber J, Lenza MA. Impact of dental asymmetries on the perception of smile esthetics.
→ Am J Orthod Dentofacial Orthop. 2007 Dec;132(6):748–53.
Given these considerations, the choice of opening space for the implant in our patient was especially influenced by the presence of microdontia of the maxillary left lateral incisor and the midline deviation of over 3 mm.
When examining the esthetics of the anterior teeth and overall smile, the clinician should be aware of the morphology of the gingival contours, tooth contacts, tooth morphology and tooth size problems. In order to obtain ideal esthetic results, worn incisal edges, tooth shape, incisal contact, the contours of the gingival margins, and black triangles should be considered before starting orthodontic treatment. The decision to reshape or add tooth structure should be evaluated in light of the width-to-length ratios of the golden proportion.19Ricketts RM. The biologic significance of the divine proportion and Fibonacci series.
→ Am J Orthod. 1982 May;81(5):351–70. It appears clinically that long, tapered triangular maxillary incisors have thin, arched gingival tissue with a longer, delicate papilla and thin bone with a smaller incisal contact point. In contrast, rectangular- shaped incisors tend to have thicker gingiva with a flatter, wider free gingival margin. Furthermore, these latter teeth have broad contacts. Generally speaking, the more rectangular the teeth, the thicker the alveolus and the gingiva that house them.20Ricketts RM. The biologic significance of the divine proportion and Fibonacci series.
→ Am J Orthod. 1982 May;81(5):351–70.
Present-day demands and expectations of esthetic dentistry are growing. In order to provide esthetic anterior tooth shape and correct agenesis, patients must be informed of their total dental needs, not just those associated with a limited specialty. In order to integrate and coordinate treatment, patients need to be offered a total treatment approach that maximizes function, esthetics and oral health. In many common dental malocclusions, orthodontic treatment alone may not be enough.21Kavadia S, Papadiochou S, Papadiochos I, Zafiriadis L. Agenesis of maxillary lateral incisors: a global overview of the clinical problem.
→ Orthodontics (Chic.). 2011 Winter;12(4):296–317.
Computer-assisted, template-based implant placement may help clinicians to perform successful implant therapy, avoiding elevation of large flaps or even eliminating flaps completely and thereby causing less pain and discomfort to patients, particularly in complex cases.22Tallarico M, Meloni SM, Canullo L, Polizzi G. Guided surgery for single-implant placement: a critical review.
→ J Oral Science Rehabilitation. 2016 Dec;2(4):8–14.23Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. Five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery.
→ Clin Implant Dent Relat Res. 2016 Oct;18(5):965–72. doi:10.1111/cid.12380. Epub 2015 Oct 7.24Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial.
→ Eur J Oral Implantol. 2014 Autumn;7(3):229–42.25Pozzi A, Tallarico M, Mangani F, Barlattani A. Different implant impression techniques for edentulous patients treated with CAD/ CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading.
→ Eur J Oral Implantol. 2013 Winter;6(4):325–40. Correct estimation of the bone condition and the implant position and precise drilling into the bone according to the preoperative planning may be essential in ensuring the successful placement of an implant.
Conclusion
Comprehensive interdisciplinary rehabilitation according to the CRANIO philosophy was effective in successfully restoring function and esthetics in a young female patient affected by congenitally missing maxillary lateral incisor.
Competing interests
The first author (MT) is the Research and Scientific Project Manager at Osstem AIC, Italy. Osstem, Seoul, South Korea, the manufacturer of the implant system evaluated in this investigation, kindly donated the implant placed. However, the data remained that of the authors and in no manner did the manufacturer interfere with the conduct of the trial or the publication of the results.
References
| 1, 4. | ↑ | Kiliaridis S, Sidira M, Kirmanidou Y, Michalakis K. Treatment options for congenitally missing lateral incisors. → Eur J Oral Implantol. 2016;9 Suppl 1:S5–24. |
| 2. | ↑ | Muller TP, Hill IN, Peterson AC, Blayney JR. A survey of congenitally missing permanent teeth. → J Am Dent Assoc. 1970 Jul;81(1):101–7. |
| 3. | ↑ | Stamatiou J, Symons AL. Agenesis of the permanent lateral incisor: distribution, number and sites. → J Clin Pediatr Dent. 1991 Summer;15(4):244–6. |
| 5, 11. | ↑ | Andrade DC, Loureiro CA, Araújo VE, Riera R, Atallah AN. Treatment for agenesis of maxillary lateral incisors: a systematic review. → Orthod Craniofac Res. 2013 Aug;16(3):129–36. |
| 6. | ↑ | Silveira GS, Mucha JN. Agenesis of maxillary lateral incisors: treatment involves much more than just canine guidance. → Open Dent J. 2016 Feb;10:19–27. |
| 7. | ↑ | Thordarson A, Zachrisson BU, Mjor IA. Remodeling of canines to the shape of lateral incisors by grinding: a long-term clinical and radiographic evaluation. → Am J Orthod Dentofacial Orthop. 1991 Aug;100(2):123–32. |
| 8, 13. | ↑ | Kokich VO Jr. Congenitally missing teeth: orthodontic management in the adolescent patient. → Am J Orthod Dentofacial Orthop. 2002 Jun;121(6):594–5. |
| 9. | ↑ | Robertsson S, Mohlin B. The congenital missing upper lateral incisor. A retrospective study of orthodontic space closure versus restorative treatment. → Eur J Orthod. 2000 Dec;22(6):697–710. |
| 10. | ↑ | Zachrisson BU. Improving orthodontic results in cases with maxillary incisors missing. → Am J Orthod. 1978 Mar;73(3):274–89. |
| 12. | ↑ | Kokich VG, Spear FM. Guidelines of managing the orthodontic-restorative patient. → Semin Orthod. 1997 Mar;3(1):3–20. |
| 14. | ↑ | Rosa M, Zachrisson BU. The space-closure alternative for missing maxillary lateral incisors: an update. → J Clin Orthod. 2010 Sep;44(9):540–9; quiz 561. |
| 15. | ↑ | Magne P, Belser U. Bonded porcelain restorations in the anterior dentition: a biomimetic approach. → Chicago: Quintessence. 2002. 406 p. |
| 16, 18. | ↑ | Pinho S, Ciriaco C, Faber J, Lenza MA. Impact of dental asymmetries on the perception of smile esthetics. → Am J Orthod Dentofacial Orthop. 2007 Dec;132(6):748–53. |
| 17. | ↑ | Spear FM, Kokich VG, Mathews DP. Interdisciplinary management of anterior dental aesthetics. → J Am Dent Assoc. 2006 Feb;137(2):160–9. |
| 19, 20. | ↑ | Ricketts RM. The biologic significance of the divine proportion and Fibonacci series. → Am J Orthod. 1982 May;81(5):351–70. |
| 21. | ↑ | Kavadia S, Papadiochou S, Papadiochos I, Zafiriadis L. Agenesis of maxillary lateral incisors: a global overview of the clinical problem. → Orthodontics (Chic.). 2011 Winter;12(4):296–317. |
| 22. | ↑ | Tallarico M, Meloni SM, Canullo L, Polizzi G. Guided surgery for single-implant placement: a critical review. → J Oral Science Rehabilitation. 2016 Dec;2(4):8–14. |
| 23. | ↑ | Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. Five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery. → Clin Implant Dent Relat Res. 2016 Oct;18(5):965–72. doi:10.1111/cid.12380. Epub 2015 Oct 7. |
| 24. | ↑ | Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial. → Eur J Oral Implantol. 2014 Autumn;7(3):229–42. |
| 25. | ↑ | Pozzi A, Tallarico M, Mangani F, Barlattani A. Different implant impression techniques for edentulous patients treated with CAD/ CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading. → Eur J Oral Implantol. 2013 Winter;6(4):325–40. |





Leave a Reply
Be the First to Comment!