Evaluation of the effect of supervised plaque control after the surgical removal of partially erupted mandibular third molars on the periodontal condition distal to second molars affected by localized periodontal disease: A randomized blind clinical study
October 2, 2015 / Categories: Digital Dentistry, Implant Dentistry

Pipkorn, Anne-Sofie

Serino, Giovanni

Turri, Alberto

Mir Taramsari, Maryam
The objective of this study was to evaluate the effect of supervised plaque control on the periodontal condition distal to the second molars after the extraction of partially erupted mandibular third molars.
Introduction
Population studies have suggested that the visible presence of a third molar increases the risk of periodontal inflammatory disease at second molars1Elter JR, Cuomo CJ, Offenbacher S, White RP Jr. Third molars associated with periodontal pathology in the Third National Health and Nutrition Examination Survey. → J Oral Maxillofac Surg. 2004 Apr;62(4):440–5.2Moss KL, Oh ES, Fisher E, Beck JD, Offenbacher S, White RP Jr. Third molars and periodontal pathologic findings in middle-age and older Americans. → J Oral Maxillofac Surg. 2009 Dec;67(12):2592–8.3Blakey GH, Gelesko S, Marciani RD, Haug RH, Offenbacher S, Phillips C, White RP Jr. Third molars and periodontal pathology in American adolescents and young adults: a prevalence study. → J Oral Maxillofac Surg. 2010 Feb;68(2):325–9. adjacent to both symptomatic and asymptomatic third molars.4Marciani RD. Is there pathology associated with asymptomatic third molars? → J Oral Maxillofac Surg. 2012 Sep;70(9 Suppl 1):S15–9.5Dicus-Brookes C, Partrick M, Blakey GH 3rd, Faulk-Eggleston J, Offenbacher S, Phillips C, White RP Jr. Removal of symptomatic third molars may improve periodontal status of remaining dentition. → J Oral Maxillofac Surg. 2013 Oct;71(10):1639–46. This was also the case in young subjects (18–40 years of age) with low severity of periodontal disease in the overall dentition.6Elter JR, Cuomo CJ, Offenbacher S, White RP Jr. Third molars associated with periodontal pathology in the Third National Health and Nutrition Examination Survey. → J Oral Maxillofac Surg. 2004 Apr;62(4):440–5.7Blakey GH, Gelesko S, Marciani RD, Haug RH, Offenbacher S, Phillips C, White RP Jr. Third molars and periodontal pathology in American adolescents and young adults: a prevalence study. → J Oral Maxillofac Surg. 2010 Feb;68(2):325–9.8Dicus-Brookes C, Partrick M, Blakey GH 3rd, Faulk-Eggleston J, Offenbacher S, Phillips C, White RP Jr. Removal of symptomatic third molars may improve periodontal status of remaining dentition. → J Oral Maxillofac Surg. 2013 Oct;71(10):1639–46.
In young subjects, when the early stages of periodontal pathology are detected in the third molar region, the removal of third molars may improve the periodontal status at the distal sites of second molars.9Blakey GH, Parker DW, Hull DJ, White RP Jr, Offenbacher S, Phillips C, Haug RH. Impact of removal of asymptomatic third molars on periodontal pathology. → J Oral Maxillofac Surg. 2009 Feb;67(2):245–50.10Montero J, Mazzaglia G. Effect of removing an impacted mandibular third molar on the periodontal status of the mandibular second molar. → J Oral Maxillofac Surg. 2011 Nov;69(11):2691–7. Studies also indicate that the removal of third molars in younger individuals compared with older subjects decreases the time needed for the extraction and decreases the risk of complications. The age of 25 appears to be critical, after which complications increase more rapidly.11Pogrel MA. What is the effect of timing of removal on the incidence and severity of complications? → J Oral Maxillofac Surg. 2012 Sep;70(9 Suppl 1):S37–40.
In a retrospective study of 215 patients, Kugelberg et al. found that two years after the surgical removal of impacted mandibular third molars, 43.3% of the cases exhibited a probing pocket depth (PPD) of > 7 mm and 32.1% showed intrabony defects of > 4 mm distal to the mandi – bular second molars.12Kugelberg CF, Ahlström U, Ericson S, Hugoson A. Periodontal healing after impacted lower third molar surgery. A retrospective study. → Int J Oral Surg. 1985 Feb;14(1):29–40. The postoperative plaque control score indicated that in most of the partici – pants the level of plaque control at the distal surface of the second molar was not optimal. Leung et al. showed that a regime of strict plaque control prevented residual pockets at periodontally involved second molars six months after the removal of the third molar.13Leung WK, Corbet EF, Kan KW, Lo EC, Liu JK. A regimen of systematic periodontal care after removal of impacted mandibular third molars manages periodontal pockets associated with the mandibular second molars. → J Clin Periodontol. 2005 Jul;32(7):725–31. Kan et al. investigated the periodontal condition distal to mandibular second molars 6–36 months after routine surgical extraction of adjacent impacted third molars in 158 subjects under 40 years of age.14Kan WK, Liu JK, Lo, EC, Corbet EF, Leung WK. Residual periodontal defects distal to the mandibular second molar 6–36 months after impacted third molar extraction. A retrospective cross-sectional study of young adults. → J Clin Periodontol. 2002 Nov;29(11):1004–11. Three possible risk indicators were associated with localized increased PPD at the distal surface of the mandibular second molar: third molar mesioangular impaction; pre-extraction signs of bone loss; and inadequate post-extraction local plaque control.15Kan WK, Liu JK, Lo, EC, Corbet EF, Leung WK. Residual periodontal defects distal to the mandibular second molar 6–36 months after impacted third molar extraction. A retrospective cross-sectional study of young adults. → J Clin Periodontol. 2002 Nov;29(11):1004–11.
The aim of the current study was to evaluate the effect of supervised plaque control after the extraction of partially erupted mandibular third molars on the periodontal condition distal to the second molars.
Materials & methods
Patient recruitment
The subjects involved in this study were selected from consecutive patients referred to the department of oral surgery at Södra Älvsborg Hospital (Borås, Sweden) for extraction of mandibular third molars. The protocol of the study was approved by the Central Ethical Review Board at the University of Gothenburg (Sweden). The patients who met the inclusion criteria were informed about the diagnosis and treatment plan. They were also informed of the purpose of the study and gave their consent for participation.
In order to be included in the study, the patients had to be 18 years of age or older, have a partially erupted third molar in need of extraction, present with bone loss distal to the adjacent second molar of > 2 mm (as measured from available radiographs) and a PPD of ≥ 6 mm, but otherwise be healthy from a periodontal perspective (i.e., no bone loss of > 1 mm and no PPD of ≥ 5 mm at the residual dentition; Fig. 1a). Patients with medical conditions that could compromise healing at the extraction site were excluded.
Clinical examination
The following clinical variables were recorded at the baseline examination by one examiner (ASP) at the distal surface of the second molars:
Plaque index (PI): The presence or absence of plaque was determined after staining with disclosing solution (Rondell Blue, Nordenta, Enköping, Sweden) at the distal sites of the second molars.
Bleeding/suppuration on probing (BoP/Sup): The presence or absence of bleeding/suppuration up to 15 s after probing was determined.
PPD: Pocket depth was measured in millimeters with a manual PCP-15 periodontal probe (Hu- Friedy, Leimen, Germany) to the nearest milli – meter at the distobuccal, distal and distolingual surfaces of the second molars.
Radiographic bone loss: The presence of bone loss distal to the second molar of > 2 mm was assessed on available digital bitewing or periapical radiographs (Fig. 1b).

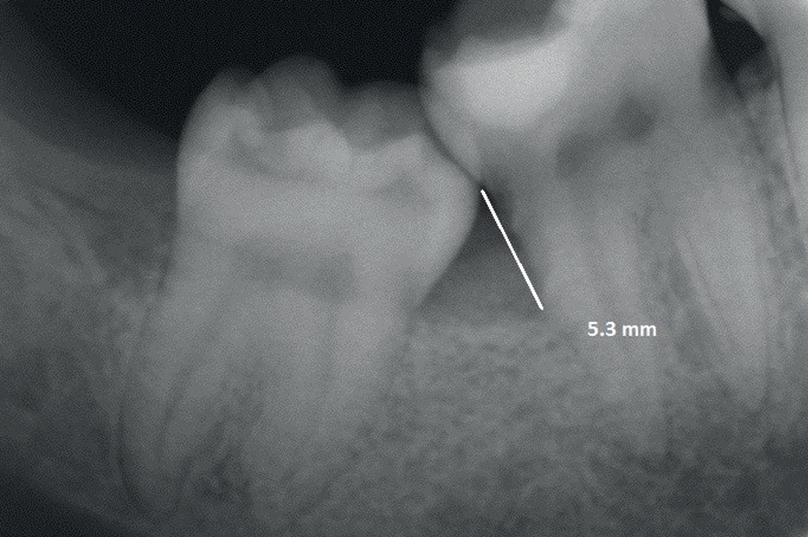
Partially erupted third molar in a patient without periodontal disease except distal to the second molar (a).
The bone-level measurement before extraction of the third molar (b).
Treatment
Surgical phase
All of the patients received an analgesic prior to surgery (1 g Alvedon, AstraZeneca, Mölndal, Sweden). The treatment was performed under aseptic conditions. After local anesthetic had been administered, a mucoperiosteal incision was placed using a #15 Bard-Parker blade according to the technique described by Nordenram.16Nordenram Å. Lambåteknik vid exstirpation av den retinerade tredje molaren I underkäken. En kritisk värdering och redovisning av en speciell metod [Flap technique in the extraction of the impacted lower third molar. A critical assessment and account of a special method]. → Sven Tandlak Tidskr. 1970 Oct;63(10):687–94. Swedish. Bone removal and sectioning of the third molar were performed with a low-speed rotary instrument under constant irrigation with sterile saline. After tooth extraction, the granulation tissue and follicular remnants were removed from the extraction alveolus. Correction of the anatomical architecture of the bone was performed under saline irrigation. The distal surface of the second molar was carefully scaled with hand instruments. After saline irrigation, the flap was repositioned in order to cover the alveolus and sutured with two (occasionally three) sutures (VICRYL, Ethicon, Somerville, N.J., U.S.).
After the surgery, the patients were randomly assigned to a test group or a control group by opening closed envelopes containing the group assignment.
Postoperative adverse events
Two patients came to the clinic before the suture removal because of postoperative pain. At this point, the extraction alveoli were rinsed with sterile saline and a prescription for stronger analgesics was given, but there was no need for the prescription of antibiotics.
Postoperative treatment
The sutures were removed seven days after the surgery. After suture removal, the patients in the control group did not receive any specific information or treatment. However, the patients in the test group were informed about the importance of good oral hygiene, especially distal to the mandibular second molars; furthermore, they were instructed on how to use a special toothbrush (Compact Tuft, Tepe Munhygienprodukter, Malmö, Sweden) to clean distal to the second molars.
At the one-month examination, the patients in the test group were recalled by a dental hygienist at the Department of Periodontology, who was not aware of the aim of the study. The patients received supra- and subgingival scaling and oral hygiene reinstruction and motivation if needed. Plaque and gingival bleeding at the distal sites of the mandibular second molars were also recorded in the following way:
PI: The presence or absence of plaque was determined in the same manner as at the baseline examination.
Gingival bleeding index (GI):The presence or absence of bleeding was determined after running the probe in the gingival sulcus distal to the second molars.17Ainamo J, Bay I. Problems and proposal for recording gingivitis and plaque. → Int Dent J. 1975 Dec;25(4):229–35.
Six-month re-evaluation
At six months, all of the patients were recalled for a control visit. This visit was performed by a perio – dontist (GS), who was not aware of the group assignment. At this time, the following parameters were recorded:
PI: The presence or absence of plaque was determined in the same manner as at the baseline examination.
BoP/Sup: The presence or absence of bleeding/suppuration was determined in the same manner as at the baseline examination.
PPD: Pocket depth was measured in the same manner as at the baseline examination (Fig. 2a).

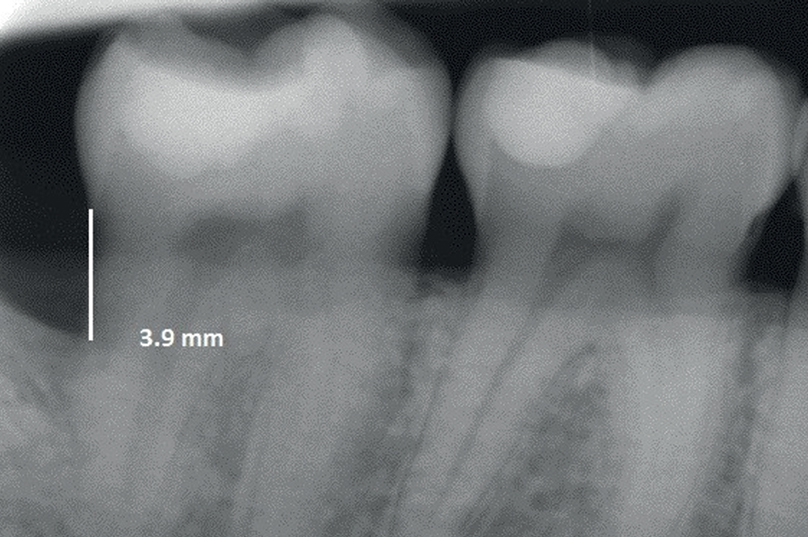
Six-month control. Clinically healthy gingival condition distal to the second molar, with a PPD of 3 mm (a).
Bone-level measurements (b).
A radiograph, aiming to control the area distal to the mandibular second molars after extraction, was also taken at this appointment using the paralleling technique.18Eggen S. [Simplification and standardization of intraoral radiography technics]. → Quintessenz. 1969 Jul;20(7):109–12. German.
Clinical criteria for healthy or diseased sites after treatment
At the re-evaluations, the surface distal to the second molars was considered healthy if there was a PPD of ≤ 4 mm without BoP/Sup. The presence of periodontal disease was determined based on a PPD of ≥ 5 mm with BoP/Sup.
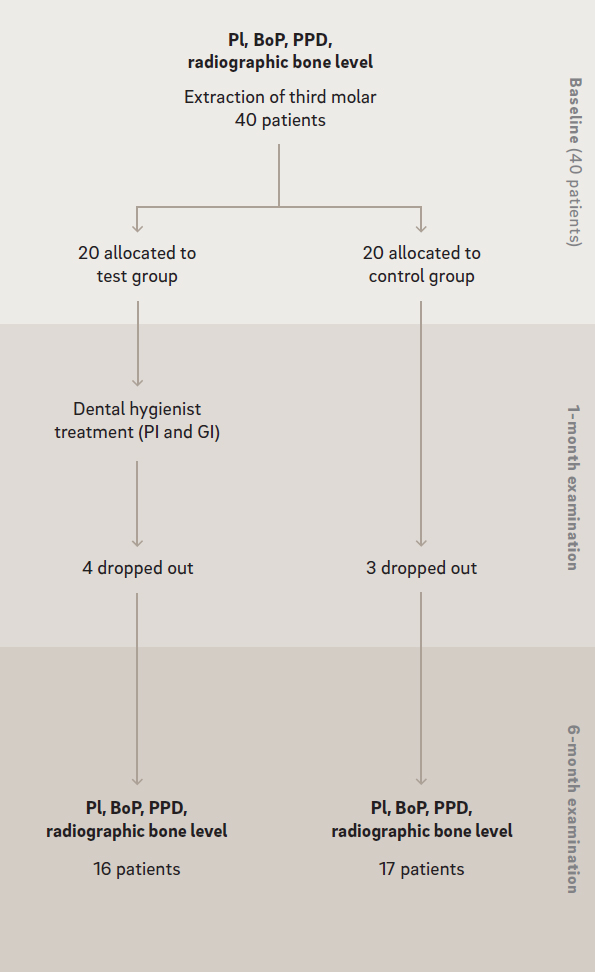 Fig. 3
Fig. 3Flowchart of the study.
Baseline and six-month radiographic measurements
The radiographs were evaluated by a second periodontist (AT), who was not aware of the study design. The bone loss distal to the second molar at baseline and at the six-month examination was measured. Thus, the distance between the cemento-enamel junction and the most coronal level along the root surfaces at which the periodontal space was considered to have a normal width19Björn H, Halling A, Thyberg H. Radiographic assessment of marginal bone loss. → Odontol Revy. 1969; 20(2):165–79. was measured using a program for digital radiographic images (Planmeca Romexis, Helsinki, Finland) with 10× magnifying power and a precision of 0.1 mm (Fig. 2b). The presence or absence of an alveolar bone defect (i.e., a bony defect 2 mm wide and 2 mm deep) was also recorded.
Data analyses
Each mandibular second molar was regarded as an independent observation. The Wilcoxon signed-rank test and Mann–Whitney U test were applied to test the difference in PPD and radiographic bone loss within and between the two groups at baseline and the six-month examination. The Fisher exact probability test was applied to assess differences in treatment outcome in the test and control groups. A p-value of < 0.05 was considered to be statistically significant.
Sample size calculation
Based on an anticipated difference in mean PPD of 1.0 mm between the test and control groups and calculated standard deviation of 1.1 mm from previous studies20Leung WK, Corbet EF, Kan KW, Lo EC, Liu JK. A regimen of systematic periodontal care after removal of impacted mandibular third molars manages periodontal pockets associated with the mandibular second molars. → J Clin Periodontol. 2005 Jul;32(7):725–31.21Kan WK, Liu JK, Lo, EC, Corbet EF, Leung WK. Residual periodontal defects distal to the mandibular second molar 6–36 months after impacted third molar extraction. A retrospective cross-sectional study of young adults. → J Clin Periodontol. 2002 Nov;29(11):1004–11. Type I error and 80% power, the calculated sample size was 20 subjects per group.
Dropout
During the study period, four patients in the test group and three in the control group dropped out from the study; one moved and the others did not attend the six-month examination (Fig. 3).
| Test | Control | All | ||||||
| Number of patients | 16 (5 female) | 17 (9 female) | 33 (14 female) | |||||
| Age | 21–48 (mean 30.1, S.D. ± 8.9) |
19–36 (mean 24.8, S.D. ± 5.0) |
19–48 (mean 27.3, S.D. ± 7.8) |
|||||
| Smokers | 1 | 2 | 3 | |||||
| Number of teeth #48 | 9 | 11 | 20 | |||||
| Number of teeth #38 | 7 | 6 | 13 | |||||
|
8 | 6 | 14 | |||||
| 8 | 10 | 18 | ||||||
| 0 | 1 | 1 | ||||||
| 0 | 0 | 0 |
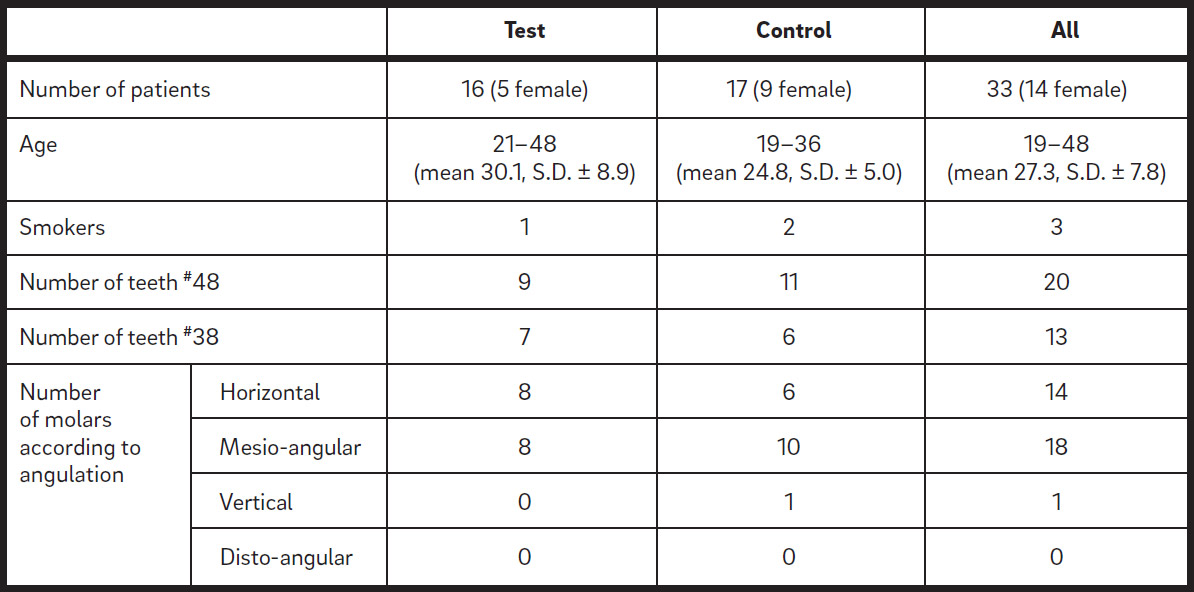
Clinical features of patients and teeth included in the study.
Results
Baseline examination
The 33 subjects (14 females and 19 males) who completed the study had a mean age of 27.4 (S.D. ± 7.8; range: 19–48). Sixteen subjects were allocated to the test group and 17 to the control group. No difference in age was noted between the test and control groups. Only three were smokers, one in the test group and two in the control group (Table 1).
A total of 33 mandibular third molars (20 on the right and 13 on the left side) were examined. The majority had a mesio-angular or horizontal position (Table 1). The presence of plaque was noted at all distal sites of the second molars, and 29 of these sites had BoP (Tables 2a & b). The mean PPD at the distal sites of the second molars, based on the deepest value measured at three points (distobuccal, distal and disto – lingual), was 7.4 mm (S.D. ± 1.5), with no difference between the test and control groups (Table 2c).
The radiographic measurements at the baseline examination showed that 26 molars had bone loss of up to one-third of the root length, and 7 molars between one-third and two-thirds, while bone loss exceeding two-thirds of the root length was not recorded in any molars (Table 2e). The mean (± S.D.)/median bone loss was 4.9 (2.4)/3.6 mm for the test group and 4.5 (0.9)/4.2 mm for the control group, and no statistically significant difference was noted in this respect between the two groups (Table 2d).
One-month examination
At one month after the extraction of the third molars, only 4 of the 16 (25%) distal sites of the second molars presented with plaque (Table 2a) and 5 showed bleeding after running the probe in the gingival sulcus.
Six-month examination
At six months after extraction, 5 out of the 16 (31%) distal sites of the second molars presented with plaque in the test group, compared with 9 out of 17 (53%) in the control group, with a reduction of 69% and 47%, respectively, from the baseline value (Table 2a). The presence of BoP was recorded at 6 out of 16 (38%) in the test group, compared with 8 out of 17 (47%) in the control group (Table 2b). The mean PPD measured at the distal sites of the second molars was 4.1 mm (S.D. ± 1.1) in the test group and 3.8 mm (S.D. ± 1.4) in the control group. None of these measurements were statistically significantly different between the two groups (Table 2c). The PPD reduction with respect to the baseline value was 3.4 mm in the test group and 3.5 mm in the control group. Both values were statistically significantly different from the baseline values (p < 0.001). No difference in the healing pattern was observed between the test and control groups with respect to the presence of a PPD of < 5 mm without BoP/Sup. Only one pocket distal to the second molar with a PPD of 6 mm with bleeding was recorded in a patient in the control group.
| Plaque | Plaque | 1 month | 6 months |
|---|---|---|---|
| Test (16) | 16 | 4 | 8 |
| Control (17) | 17 | 0 | 9 |
| All (33) | 33 | 0 | 14 |
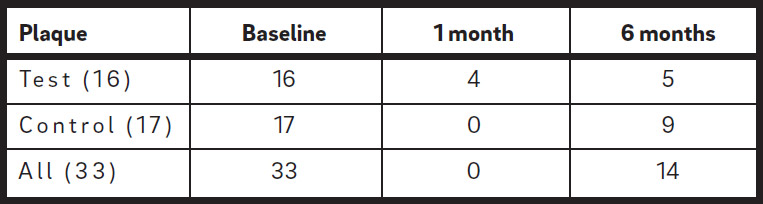
Table 2a
| BoP | Baseline | 6 months |
|---|---|---|
| Test (16) | 14 | 6 |
| Control (17) | 15 | 8 |
| All (33) | 29 | 14 |
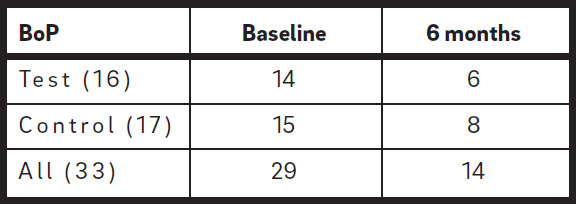
Table 2b
| PPD | Baseline | 6 months |
|---|---|---|
| Test (16) | 7.5 (1.5)/7 | 4.1 (1.1)/4 |
| Control (17) | 7.3 (1.5)/7.5 | 3.8 (1.4)/4.5 |
| All (33) | 7.4 (1.5)/7 | 4.0 (1.2)/4 |
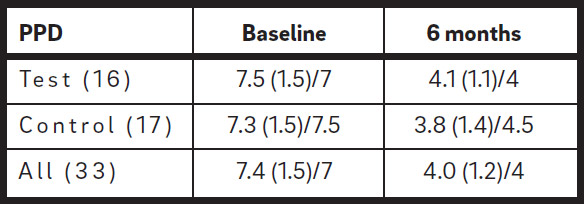
Table 2c
| Bone loss | Baseline | 6 months |
|---|---|---|
| Test (16) | 4.9 (2.4)/3.6 | 3.5 (1.6)/2.9 |
| Control (17) | 4.5 (0.9)/4.2 | 3.1 (1.4)/3.3 |
| All (33) | 4.4 (1.6)/4.1 | 3.2 (1.5)/3.3 |
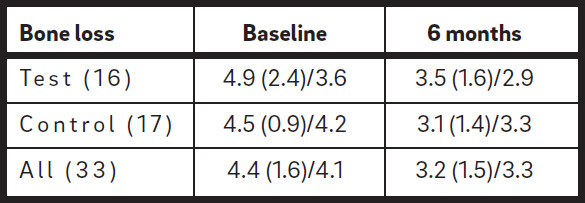
Table 2d
| Baseline | 6 months | |||||
|---|---|---|---|---|---|---|
| Bone loss ≤ 1/3 |
Bone loss 1/3–2/3 |
Bone loss > 2/3 |
Bone loss ≤ 1/3 |
Bone loss 1/3–2/3 |
Bone loss > 2/3 |
|
| Test (16) | 13 | 3 | 0 | 15 | 1 | 0 |
| Control (17) | 13 | 4 | 0 | 16 | 1 | 0 |
| All (33) | 26 | 7 | 0 | 31 | 2 | 0 |
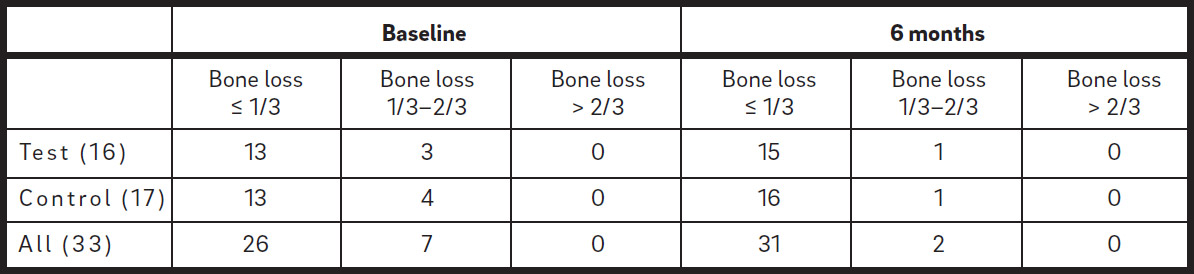
Table 2e
The radiographic measurements found no bone loss in either group. The bone level (mean/ median) at six months was 3.5/2.9 mm in the test group and 3.1/3.3 mm in the control group, with a gain of 0.7 mm in the test group and 0.8 mm in the control group with respect to the baseline value (Table 2d; Figs. 4a & b).
Discussion
The results of the present study showed that in subjects presenting with localized periodontal disease distal to mandibular second molars the periodontal condition improved at six months after extraction of the adjacent partially erupted third molars and subgingival plaque debridement. All of the distal sites of the second molars showed a clinically significant reduction in PPD and the radiographic measurements indicated bone gain distal to the second molars for both the test and control groups.
The presence of periodontal disease at the second molars adjacent to third molars in subjects with low severity of periodontal disease in the overall dentition has been reported in other studies.22Elter JR, Cuomo CJ, Offenbacher S, White RP Jr. Third molars associated with periodontal pathology in the Third National Health and Nutrition Examination Survey. → J Oral Maxillofac Surg. 2004 Apr;62(4):440–5.23Blakey GH, Gelesko S, Marciani RD, Haug RH, Offenbacher S, Phillips C, White RP Jr. Third molars and periodontal pathology in American adolescents and young adults: a prevalence study. → J Oral Maxillofac Surg. 2010 Feb;68(2):325–9.24Dicus-Brookes C, Partrick M, Blakey GH 3rd, Faulk-Eggleston J, Offenbacher S, Phillips C, White RP Jr. Removal of symptomatic third molars may improve periodontal status of remaining dentition. → J Oral Maxillofac Surg. 2013 Oct;71(10):1639–46. None of the patients included in our study had signs of periodontal attachment or bone loss at the dentition except distal to the second molar. However, considering the young age of the sample (mean age of 27.4, S.D. ± 7.8) and the radiographic mean bone loss distal to the second molar of 4.9 mm (S.D. ± 2.4), the annual rate of bone loss distal to the second molar (if calculated from the age of 17) was approximately 0.4 mm/year. This rate is comparable to the annual bone loss (> 0.2 mm/year) in subjects with rapid disease progression described in longitudinal epidemiological studies.25Löe H, Ånerud Å, Boysen H, Morrison E. Natural history of periodontal disease in man. Rapid, moderate and no loss of attachment in Sri Lankan laborers 14 to 46 years of age. → J Clin Periodontol. 1986 May;13(5):431–45.26Papapanou PN, Wennström JL. A 10-year retrospective study of periodontal disease progression. Clinical characteristics of subjects with pronounced and minimal disease development. → J Clin Periodontol. 1990 Feb;17(2):78–84.27Hugoson A, Laurell L. A prospective longitudinal study on periodontal bone height changes in a Swedish population. → J Clin Periodontol. 2000 Sep;27(9):665–74.
When early stages of periodontal path – ology are detected, the removal of third molars may improve the periodontal status at the distal sites of second molars.28Blakey GH, Parker DW, Hull DJ, White RP Jr, Offenbacher S, Phillips C, Haug RH. Impact of removal of asymptomatic third molars on periodontal pathology. → J Oral Maxillofac Surg. 2009 Feb;67(2):245–50.29Montero J, Mazzaglia G. Effect of removing an impacted mandibular third molar on the periodontal status of the mandibular second molar. → J Oral Maxillofac Surg. 2011 Nov;69(11):2691–7. In our study, both the test and control groups showed relatively good plaque control distal to the second molars after the removal of the third molars. This may be related to easier access for self-performed plaque control distal to the second molars once the third molars had been extracted. The test group, who received the dental hygienist treatment at one month after the extraction, presented with a lower number of sites with plaque and sulcular gingival bleeding compared with the control group, but the differences did not reach statistical significance.

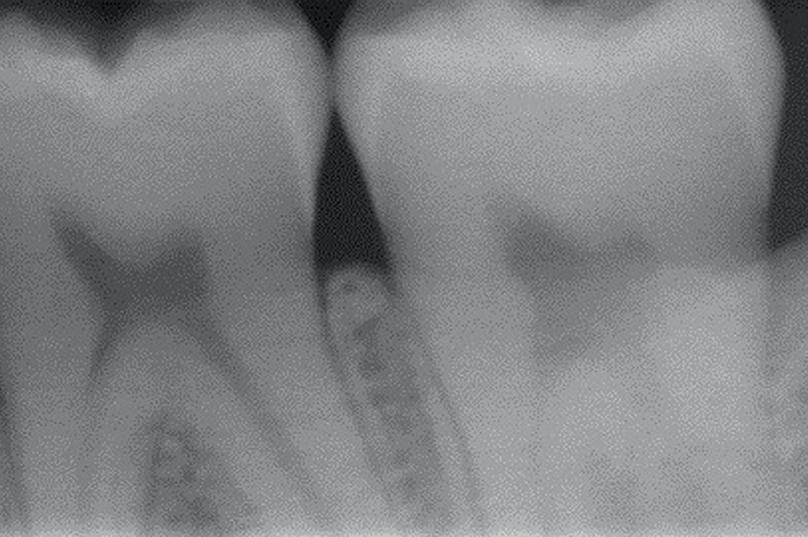
Radiographic images before and six months after the extraction of tooth #38. The bone healing distal to tooth #37 is noticeable.
At the six-month evaluation, both groups had a clinically relevant PPD reduction distal to the second molars, and only one patient (in the control group) presented with a PPD of 6 mm. Thus, no additional surgical periodontal treatment was needed, except in one patient. In this respect, it should be underlined that, after the extraction of the third molars, meticulous debridement distal to the second molars was performed, together with removal of the granulation tissue. In a literature review, Aloy-Prósper et al. also concluded that debridement of the distal radicular surface of the second molars, together with oral hygiene control, reduced PPD values after the extraction of third molars.30Aloy-Prósper A, García-Mira B, Larrazabal-Morón C, Peñarrocha- Diago M. Distal probing depth and attachment level of lower second molars following surgical extraction of lower third molars: a literature review. → Med Oral Patol Oral Cir Bucal. 2010 Sep;(15)5:755–9. Leung et al., in their clinical study, concluded that plaque control prevented residual pockets at periodontally involved second molars six months after the removal of the adjacent third molar.31Leung WK, Corbet EF, Kan KW, Lo EC, Liu JK. A regimen of systematic periodontal care after removal of impacted mandibular third molars manages periodontal pockets associated with the mandibular second molars. → J Clin Periodontol. 2005 Jul;32(7):725–31.
In our study, no bone loss distal to the second molars was recorded. In a study evaluating the adjunctive effect of guided tissue regeneration in conjunction with surgical removal of an impacted third molar, Karapataki et al. concluded that an intrabony defect distal to the second molars would depend on the existing amount of periodontal ligament of the second molar and whether this was affected by perio – dontal disease before surgery.32Karapataki S, Hugoson A, Kugelberg CF. Healing following GTR treatment of bone defects distal to mandibular 2nd molars after surgical removal of impacted 3rd molars. → J Clin Periodontol. 2000 May;27(5):325–32. Thus, un – diagnosed periodontal lesions and the presence of bacteria on the root surface of second molars might affect wound healing in the area and develop into a persistent intrabony defect. These defects require surgical treatment at a later time.33Karapataki S, Hugoson A, Falk H, Laurell L, Kugelberg CF. Healing following GTR treatment of intrabony defects distal to mandibular 2nd molars using resorbable and non-resorbable barriers. → J Clin Periodontol. 2000 May;27(5)333–40. In our study, the periodontal condition distal to the second molars in all of the patients (except one in the control group) at the six-month evaluation did not require additional periodontal surgical treatment.
Kan et al. investigated the periodontal condition distal to mandibular second molars 6–36 months after routine surgical extraction of adjacent impacted third molars in 158 subjects under 40 years of age.34Kan WK, Liu JK, Lo, EC, Corbet EF, Leung WK. Residual periodontal defects distal to the mandibular second molar 6–36 months after impacted third molar extraction. A retrospective cross-sectional study of young adults. → J Clin Periodontol. 2002 Nov;29(11):1004–11. Three possible risk indicators were associated with localized increased PPD: third molar mesio-angular impaction; pre-extraction signs of bone loss; and inadequate post-extraction local plaque control. 35Kan WK, Liu JK, Lo, EC, Corbet EF, Leung WK. Residual periodontal defects distal to the mandibular second molar 6–36 months after impacted third molar extraction. A retrospective cross-sectional study of young adults. → J Clin Periodontol. 2002 Nov;29(11):1004–11.
In our study, the majority of the patients (76%) were under 30 years of age, without compromised general condition, only three were smokers and none had periodontal disease, except at the distal sites of their second molars. Furthermore, 79% of the subjects had bone loss distal to the second molars not exceeding one-third of the root length and no patient presented with bone loss exceeding twothirds of the root length. All of these factors could have had a positive effect on the healing pattern. The moderate bone loss distal to the second molars at baseline could also have had a positive effect on the soft-tissue healing, preventing concavity in the gingiva, which could have been a retaining factor for plaque.
In the interpretation of similar studies, it is important to distinguish between those reporting results on totally impacted and on partially erupted third molars. Moss et al. reported results from 7,000 subjects (mean age of 62) and found that the PPD at the first or second molars was significantly higher when partially erupted third molars were present, compared with totally impacted third molars.36Moss KL, Oh ES, Fisher E, Beck JD, Offenbacher S, White RP Jr. Third molars and periodontal pathologic findings in middle-age and older Americans. → J Oral Maxillofac Surg. 2009 Dec;67(12):2592–8. Similarly, in 52- to 74-year-old patients in the Dental Atherosclerosis Risk in Communities Study, the presence of visible third molars was associated with a 50% increased probability of a PPD of > 5 mm at adjacent second molars.37Elter JR, Offenbacher S, White RP Jr, Beck JD. Third molars associated with periodontal pathology in older Americans. → J Oral Maxillofac Surg. 2005 Feb;63(2):179–84. This finding has also been confirmed in a group of 5,831 young adults (18–34 years old) in the U.S. Third National Health and Nutrition Examination Survey, where the presence of visible third molars was associated with twice the probability of a PPD of > 5 mm at the adjacent second molars.38Elter JR, Cuomo CJ, Offenbacher S, White RP Jr. Third molars associated with periodontal pathology in the Third National Health and Nutrition Examination Survey. → J Oral Maxillofac Surg. 2004 Apr;62(4):440–5.
Regarding postoperative events, only two patients in our study came to the clinic before suture removal because of postoperative pain. At this time, the extraction alveoli were rinsed with sterile saline and a prescription for stronger analgesics was given, but there was no need for any antibiotic prescription. This confirms the findings that the removal of third molars in younger subjects compared with older subjects decreases the risk of complications; the age of 25 appears to be critical, after which complications increase more rapidly.39Pogrel MA. What is the effect of timing of removal on the incidence and severity of complications? → J Oral Maxillofac Surg. 2012 Sep;70(9 Suppl 1):S37–40. It should be underlined that in our study the removal of third molars was performed by an experienced dentist in this area of dentistry (ASP), who meticulously removed the plaque and calculus accumulated at the distal sites of the second molars.
Conclusion
In the presence of localized periodontal disease distal to second molars, early diagnosis, extraction of the third molar and debridement at the distal site of the second molar were an effective treatment of localized periodontal disease, because no additional surgical periodontal treatment was needed at the six-month follow-up.
Competing interests
The authors declare that they have no com peting interests.
Acknowledgments
This project was supported by grants #VGFOUSA-P-289301 and VGFOUSAP 152431 from the research and development unit for primary care and dental services, Southern Älvsborg County (Borås, Sweden).
References
| 1, 6, 22, 38. | ↑ | Elter JR, Cuomo CJ, Offenbacher S, White RP Jr. Third molars associated with periodontal pathology in the Third National Health and Nutrition Examination Survey. → J Oral Maxillofac Surg. 2004 Apr;62(4):440–5. |
| 2, 36. | ↑ | Moss KL, Oh ES, Fisher E, Beck JD, Offenbacher S, White RP Jr. Third molars and periodontal pathologic findings in middle-age and older Americans. → J Oral Maxillofac Surg. 2009 Dec;67(12):2592–8. |
| 3, 7, 23. | ↑ | Blakey GH, Gelesko S, Marciani RD, Haug RH, Offenbacher S, Phillips C, White RP Jr. Third molars and periodontal pathology in American adolescents and young adults: a prevalence study. → J Oral Maxillofac Surg. 2010 Feb;68(2):325–9. |
| 4. | ↑ | Marciani RD. Is there pathology associated with asymptomatic third molars? → J Oral Maxillofac Surg. 2012 Sep;70(9 Suppl 1):S15–9. |
| 5, 8, 24. | ↑ | Dicus-Brookes C, Partrick M, Blakey GH 3rd, Faulk-Eggleston J, Offenbacher S, Phillips C, White RP Jr. Removal of symptomatic third molars may improve periodontal status of remaining dentition. → J Oral Maxillofac Surg. 2013 Oct;71(10):1639–46. |
| 9, 28. | ↑ | Blakey GH, Parker DW, Hull DJ, White RP Jr, Offenbacher S, Phillips C, Haug RH. Impact of removal of asymptomatic third molars on periodontal pathology. → J Oral Maxillofac Surg. 2009 Feb;67(2):245–50. |
| 10, 29. | ↑ | Montero J, Mazzaglia G. Effect of removing an impacted mandibular third molar on the periodontal status of the mandibular second molar. → J Oral Maxillofac Surg. 2011 Nov;69(11):2691–7. |
| 11, 39. | ↑ | Pogrel MA. What is the effect of timing of removal on the incidence and severity of complications? → J Oral Maxillofac Surg. 2012 Sep;70(9 Suppl 1):S37–40. |
| 12. | ↑ | Kugelberg CF, Ahlström U, Ericson S, Hugoson A. Periodontal healing after impacted lower third molar surgery. A retrospective study. → Int J Oral Surg. 1985 Feb;14(1):29–40. |
| 13, 20, 31. | ↑ | Leung WK, Corbet EF, Kan KW, Lo EC, Liu JK. A regimen of systematic periodontal care after removal of impacted mandibular third molars manages periodontal pockets associated with the mandibular second molars. → J Clin Periodontol. 2005 Jul;32(7):725–31. |
| 14, 15, 21, 34, 35. | ↑ | Kan WK, Liu JK, Lo, EC, Corbet EF, Leung WK. Residual periodontal defects distal to the mandibular second molar 6–36 months after impacted third molar extraction. A retrospective cross-sectional study of young adults. → J Clin Periodontol. 2002 Nov;29(11):1004–11. |
| 16. | ↑ | Nordenram Å. Lambåteknik vid exstirpation av den retinerade tredje molaren I underkäken. En kritisk värdering och redovisning av en speciell metod [Flap technique in the extraction of the impacted lower third molar. A critical assessment and account of a special method]. → Sven Tandlak Tidskr. 1970 Oct;63(10):687–94. Swedish. |
| 17. | ↑ | Ainamo J, Bay I. Problems and proposal for recording gingivitis and plaque. → Int Dent J. 1975 Dec;25(4):229–35. |
| 18. | ↑ | Eggen S. [Simplification and standardization of intraoral radiography technics]. → Quintessenz. 1969 Jul;20(7):109–12. German. |
| 19. | ↑ | Björn H, Halling A, Thyberg H. Radiographic assessment of marginal bone loss. → Odontol Revy. 1969; 20(2):165–79. |
| 25. | ↑ | Löe H, Ånerud Å, Boysen H, Morrison E. Natural history of periodontal disease in man. Rapid, moderate and no loss of attachment in Sri Lankan laborers 14 to 46 years of age. → J Clin Periodontol. 1986 May;13(5):431–45. |
| 26. | ↑ | Papapanou PN, Wennström JL. A 10-year retrospective study of periodontal disease progression. Clinical characteristics of subjects with pronounced and minimal disease development. → J Clin Periodontol. 1990 Feb;17(2):78–84. |
| 27. | ↑ | Hugoson A, Laurell L. A prospective longitudinal study on periodontal bone height changes in a Swedish population. → J Clin Periodontol. 2000 Sep;27(9):665–74. |
| 30. | ↑ | Aloy-Prósper A, García-Mira B, Larrazabal-Morón C, Peñarrocha- Diago M. Distal probing depth and attachment level of lower second molars following surgical extraction of lower third molars: a literature review. → Med Oral Patol Oral Cir Bucal. 2010 Sep;(15)5:755–9. |
| 32. | ↑ | Karapataki S, Hugoson A, Kugelberg CF. Healing following GTR treatment of bone defects distal to mandibular 2nd molars after surgical removal of impacted 3rd molars. → J Clin Periodontol. 2000 May;27(5):325–32. |
| 33. | ↑ | Karapataki S, Hugoson A, Falk H, Laurell L, Kugelberg CF. Healing following GTR treatment of intrabony defects distal to mandibular 2nd molars using resorbable and non-resorbable barriers. → J Clin Periodontol. 2000 May;27(5)333–40. |
| 37. | ↑ | Elter JR, Offenbacher S, White RP Jr, Beck JD. Third molars associated with periodontal pathology in older Americans. → J Oral Maxillofac Surg. 2005 Feb;63(2):179–84. |





Leave a Reply
Be the First to Comment!