Immediate dentoalveolar restoration
November 26, 2019 / Categories: Digital Dentistry, Implant Dentistry

da Silva Brum, Igor
Ferreira Natal, Renan
da Silva Pires, Jorge Luís
Gonçalo Pinto dos Santos, Paulo
Alencar de Carvalho, Marco Antonio
José de Carvalho, Jorge
Abstract
Background
The replacement of an anterior tooth with an implant has become frequent in the daily routine of an implantologist. This procedure is an enormous challenge because of its esthetic potential and possibility of implant failure. In this article, we report a case of immediate dentoalveolar restoration, based on the 1-stage protocol proposed by José Carlos Martins da Rosa.
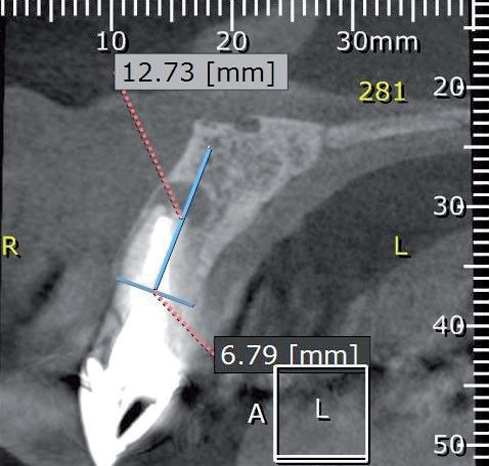
A 57-year-old female patient presented with pain and a fractured root with mobility of the crown. After analysis of the cone beam computed tomography scan, fracture of the maxillary left central incisor was confirmed and periapical inflammatory lesions affecting both central incisors could be seen. A cross-sectional image revealed substantial loss of the buccal bone wall and confirmed the 7 mm probing depth.
The treatment entailed atraumatic extraction of both central incisors, curettage and preparation of the sockets. Two provisional crowns were fabricated previously using composite, simulating the implants’ position on the cast. The implants and abutments were placed. The crowns were adjusted. A cortical triangular bone graft was removed from the maxillary tuberosity and inserted into the socket of the left central incisor. After that, the provisional restorations were reinserted to seal the gingival margin. After 1 week, the patient showed no postoperative pain or swelling. No mobility of the crowns or implants was observed. Periodic follow-ups were necessary to assess bone formation in the grafted area and to check whether the gingival profile had been maintained.
Conclusion
The technique proved to be clinically effective for esthetic edentulous areas and showed significant predictability of results. Throughout the follow-up, the stability of the hard and soft tissue had been observed.
Keywords
Dental implant; fresh socket; immediate provisionalization; immediate loading; maxillary tuberosity; autologous bone graft.
Introduction
Periapical infections caused by periodontal disease, fractures, endodontic lesions or root resorption may directly promote severe alveolar bone resorption and soft-tissue loss surrounding the tooth. When such infections are present, more surgical procedures may be needed to regenerate and prepare the tissue to receive the implant.1Muhamad AH, Georges C, Azzaldeen A. Immediate Implants Placed Into Infected Sockets: Clinical Update with 3-Year Follow-Up. → J Dent Med Sci. 2017, 16, pp.0853-160109105111. The lack of a buccal bone wall to support the attached gingiva can cause recession and papillary loss, influencing the esthetic characteristics. Furthermore, further reconstructive stages such as bone and soft-tissue grafts may be needed.
Owing to the evolution of implantology, techniques are being improved and the period of healing between surgery and prosthetic restoration is being reduced. Several authors have described success rates of higher than 90% for implants placed immediately after tooth extraction and immediately loaded using provisional crowns. The technique is indicated for low-stress areas and when initial stability has been achieved. Some papers have shown that certain forces are important for triggering a series of biological reactions that accelerate the bone repair process, thus supporting 1-stage implant treatment.2Esposito M, Trullenque-Eriksson A, Blasone R, Malaguti G, Gaffuri C, Caneva M, Minciarelli A, Luongo G. Clinical evaluation of a novel dental implant system as single implants under immediate loading conditions— 4-month post-loading results from a multicentre randomised controlled trial. → Eur J Oral Implantol. 2016;9(4):367–79.

Fig. 1
Immediate implant placement followed by immediate loading can provide numerous advantages, such as reduced treatment time and procedures, a potentially lower cost and a smaller number of provisional crown adjustments. Furthermore, the esthetic benefits are the maintenance of the gingival architecture and a reduced loss of bone volume. If correctly planned and executed, the procedure promotes really impressive results, though there are requisites that must be followed for clinical safety. Among them are initial implant stability, adequate bone volume to accommodate the implant, no gingival recession, and proximity to vital structures.3De Molon RS, de Avila ED, Cirelli JA, Mollo F de A Jr, de Andrade MF, Filho LA, Barros LA. A combined approach for the treatment of resorbed fresh sockets allowing immediate implant restoration: a 2-year followup. → J Oral Implantol. 2015 Dec;41(6):712–8.
The immediate dentoalveolar restoration (IDR) technique was created to enhance the clinical efficacy and esthetics in these kinds of clinical cases. Furthermore, it reduces the treatment time and promote superior results. To achieve the expected esthetic results, careful surgical and prosthetic protocols are of great importance.4De Molon RS, de Avila ED, de Barros-Filho LA, Ricci WA, Tetradis S, Cirelli JA, Borelli de Barros LA. Reconstruction of the alveolar buccal bone plate in compromised fresh socket after immediate implant placement followed by immediate provisionalization. → J Esthet Restor Dent. 2015 May–Jun;27(3):122–35.
-
- Fig. 2a
-
- Fig. 2b
-

- Fig. 2c
Case report
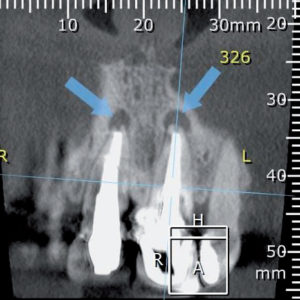
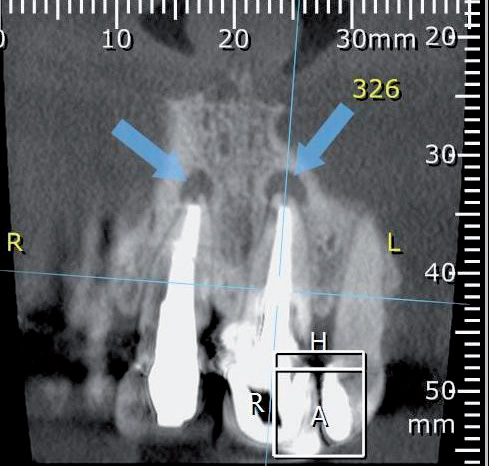
A 57-year-old woman was referred to the department of implantology for treatment of her maxillary central incisors. The patient complained of pain and a fractured root with mobility of the crown. She had no relevant medical history and denied deleterious habits such as smoking or alcohol consumption. Her oral hygiene was satisfactory. During the clinical examination, the left central incisor presented class I mobility and a probing depth of 7 mm in the buccal region, indicating a vertical bone defect (Fig. 1). A cone beam computed tomography (CBCT) scan was captured, from which fracture of the left central incisor was confirmed and periapical inflammatory lesions affecting both central incisors could be seen (Figs. 2a–c).
-
- Fig. 3a
-
- Fig. 3b
-
- Fig. 4a
-
- Fig. 4b
-
- Fig. 4c
-

- Fig. 4d
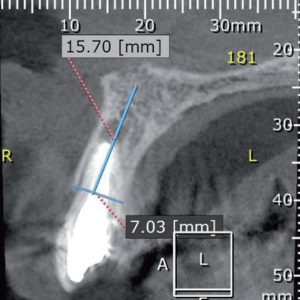
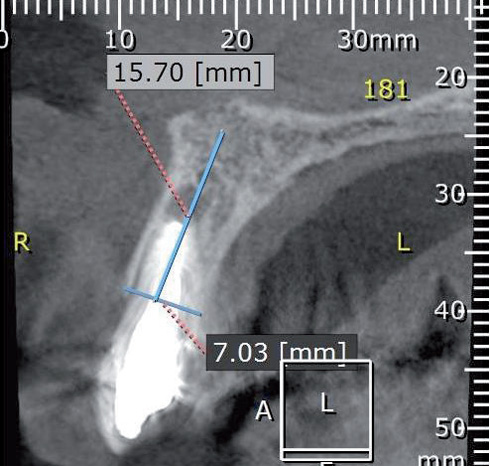
A cross section on the CBCT scan showed substantial loss of the buccal bone wall, which accounted for the deep probing depth at that aspect of the tooth. The maxillary right central incisor presented a recurrent periapical inflammatory lesion. Both maxillary central incisors had large metal core buildups. The mentioned features confirmed the need to extract the incisors. Subsequently, planning was performed based on the IDR technique, and the procedures to be performed were explained to the patient. The informed consent form was signed and a blood analysis was done to evaluate the patient’s general health. The results permitted us to proceed with the surgical procedure.
Pharmacological protocol
Antibiotic therapy (amoxicillin, 1 g) was administered 1 h before the surgical procedure, and antibiotic doses (500 mg) 3 times a day for 7 days after the procedure were prescribed. Dexamethasone (4 mg, 2 tablets) was administered 1 h before the surgical procedure and continued twice a day for 3 days. Ibuprofen (600 mg, 1 tablet) 3 times a day for 5 days after the procedure was prescribed.
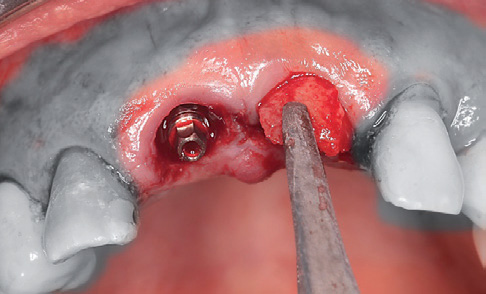
Fig. 5
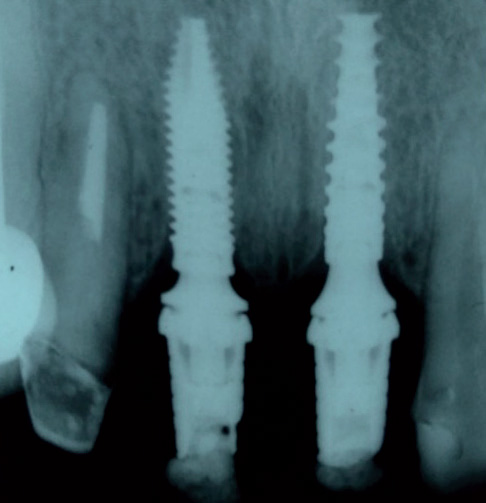
Fig. 6a

Fig. 6b
Technique
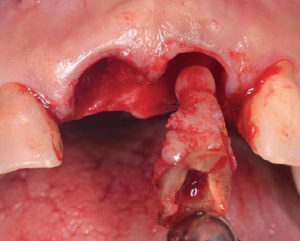
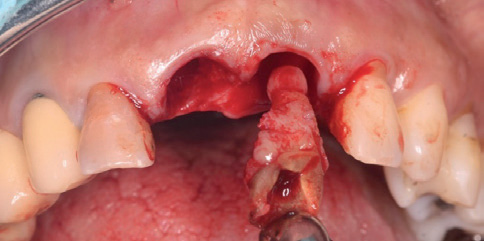
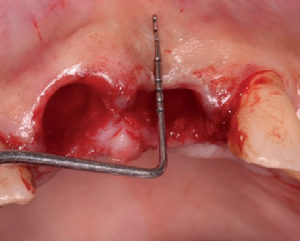
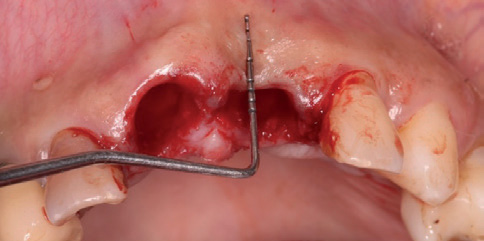
Local infiltration of anesthetic near the roots of the maxillary central incisors and a block of the nasopalatine nerve were done. Afterward, an intrasulcular incision was made following the contour of the incisors. Furthermore, periotomes and a manual root extractor were used to realize the minimally invasive procedure and avoid the necessity of flap creation. During the extraction, the inflammatory lesions came out attached to the roots (Fig. 3a). After the tooth removal, socket curettage was performed to remove any granulomatous tissue and the remains of the periodontal ligament. The fresh socket was evaluated using a millimeter probe to confirm the buccal bone defect observed on the CBCT scan (Fig. 3b).
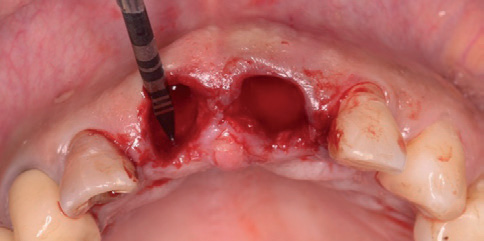
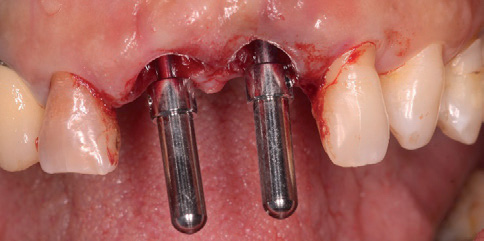
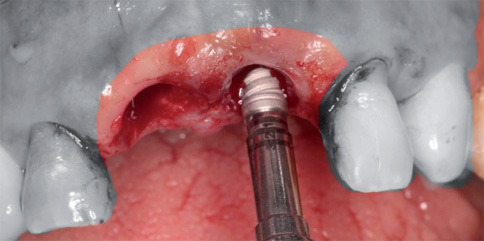
The preparation of the sockets for the implants was performed approaching the palatal bone. Two Systhex implants were placed (Attract and Attract ts; Figs. 4a–d). Both implants were 3.5 mm in diameter and 12.0 mm in height, had a Morse taper connection and had undergone the same surface treatment. The initial torque achieved was approximately 45 N cm. The provisional crowns were fabricated using composite before the procedure and adjusted to the ideal emergence profile and vestibular-palatal angle. It is important to note the necessity of 3 mm in height, from the bone crest to the contact point, to stimulate coronal growth of the papilla. This distance extends from the bone crest to the contact point.
Anesthesia of the maxillary tuberosity was then administered and the triangular bone graft removed. The cortical bone fragment was positioned between the vestibular plate and the implant placed in the left central incisor region (Fig. 5). The right central implant did not need any grafting. The occlusion was adjusted for both incisors, and any occlusal contact was avoided. Thereafter, the provisional crowns were polished and reinserted. Finally, the tissue was sutured with simple stitches.
After the procedure, the patient was instructed to avoid any loading on the area for 3 months, as also spitting over 3 days. Application of a 0.12% chlorhexidine gluconate topical gel (Perioxidin, Gross) once a day before bedtime was recommended. Follow-ups were done once a week for 1 month and continued every 15 days for 1 month. After 1 week, the patient showed amazing results, with no complaint of postoperative pain or swelling. No mobility of the crowns or implants was observed. Periodic clinical monitoring is necessary to assess whether there has been bone formation in the grafted area and whether the gingival profile has been maintained over the years.
After 6 months, the period of bone remodeling and soft-tissue healing was done, and the periimplant tissue analyzed. Furthermore, a periapical radiograph was performed to evaluate the final aspect of the healing and bone–implant contact (Figs. 6a & b). The results showed complete adaptation of the periimplant tissue without any sign of inflammation.
Final restoration
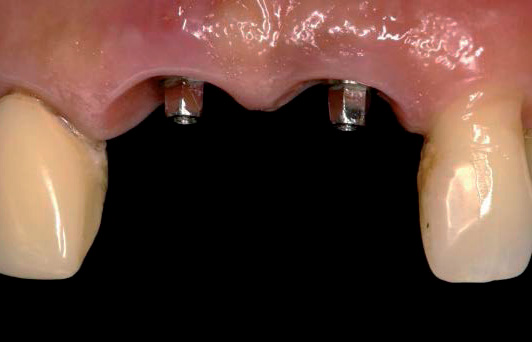
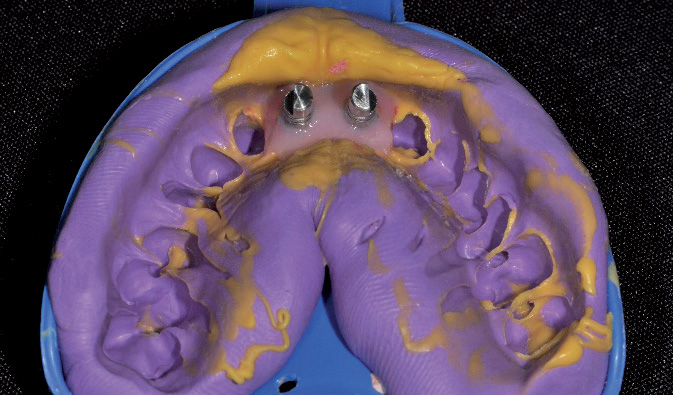
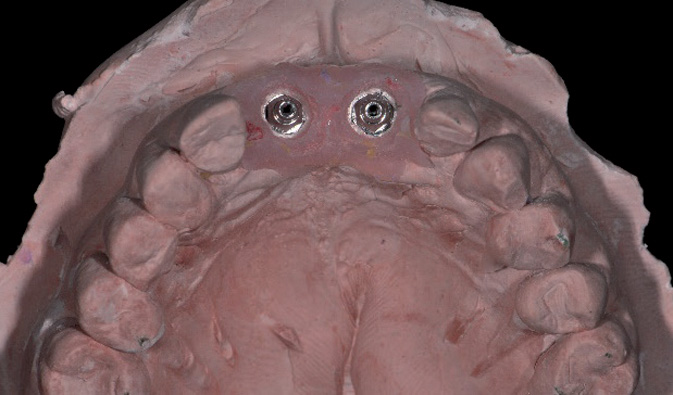
Prosthetic procedures were started with a transfer impression of the esthetic abutments. A final impression was carefully performed using autopolymerizing resin to copy the emergence profiles (Figs. 7a & b) and addition silicone for the impression (Figs. 8a–c). The working cast was sent to the laboratory for production of the metal superstructure and porcelain application. Monolithic ceramic crowns were prepared, adjusted and screwed onto the abutments (Figs. 9a–c). In both steps, periapical radiographs were taken to evaluate the adaptation level. Additionally, features such as emergence profile, contact point and esthetic were analyzed.
-
- Fig. 7a
-

- Fig. 7b
-
- Fig. 8a
-
- Fig. 8b
-

- Fig. 8c
Discussion
The IDR technique in compromised sockets of anterior teeth has been proved to be a complex clinical challenge. Immediate loading of implants placed immediately after extraction has been very well documented in the literature in cases where the supporting tissue is undamaged.5Rosa AC, Francischone CE, Cardoso Mde A, Alonso AC, Filho LC, Da Rosa JC. Post-traumatic treatment of maxillary incisors by immediate dentoalveolar restoration with long-term follow-up. → Compend Contin Educ Dent. 2015 Feb;36(2):130–4. Furthermore, for the initial stability, the biological changes that occur when immediate loading is performed are of great importance in the repair process.6Rosa JC, Rosa AC, Francischone CE, Sotto-Maior BS. Esthetic outcomes and tissue stability of implant placement in compromised sockets following immediate dentoalveolar restoration: results of a prospective case series at 58 months follow-up. → Int J Periodontics Restorative Dent. 2014 Mar–Apr;34(2):199–208. The maintenance of the tissue is more predictable than the re-covering of the buccal bone wall and the emergence profile.
-

- Fig. 9a
-

- Fig. 9b
-

- Fig. 9c
According to Zhang, their analysis of patients who had received immediate, early or conventional loading showed that the patients who had undergone immediate loading had reduced marginal bone level changes in comparison with those who had not received immediate loading. Although, some factors, such as the loading protocol for non immediate loading, implant number and location, type of prosthesis, loading concept and follow-up time, could modify these results.7Zhang S, Wang S, Song Y. Immediate loading for implant restoration compared with early or conventional loading: A meta-analysis. → J Craniomaxillofac Surg. 2017 Jun;45(6):793–803. doi: 10.1016/j.jcms.2016.05.002. Epub 2016 May 14. Marginal bone level is a surrogate measurement for the esthetic outcome.8Da Rosa JC, Rosa AC, da Rosa DM, Zardo CM. Immediate dentoalveolar restoration of compromised sockets: a novel technique. → Eur J Esthet Dent. 2013 Autumn;8(3):432–43.
The cosmetology assessment has been used in some papers to analyze the clinical outcomes of treatment with dental implants. This index is of great importance and should be evaluated in further studies. When comparing immediate and non immediate loading, some authors9Crespi R, Capparè P, Gherlone E, Romanos GE. Immediate occlusal loading of implants placed in fresh sockets after tooth extraction. → Int J Oral Maxillofac Implants. 2007 Nov–Dec;22(6):955–62.,10Vandamme K, Naert I, Geris L, Sloten JV, Puers R, Duyck J. Histodynamics of bone tissue formation around immediately loaded cylindrical implants in the rabbit. → Clinical oral implants research. 2007;18(4):471–80. found that the ideal gingival margin was achieved in more cases of immediate loading than in cases of conventional loading.11Rojas-Vizcaya F. Rehabilitation of the maxillary arch with implant-supported fixed restorations guided by the most apical buccal bone level in the esthetic zone: A clinical report. → The Journal of prosthetic dentistry. 2012. 107(4);213–20.,12De Rouck T, Collys K, Cosyn J. Single-tooth replacement in the anterior maxilla by means of immediate implantation and provisionalization: a review. → Int J Oral Maxillofac Implants. 2008 Sep–Oct;23(5):897–904.
The loss of tooth support greatly increases the risk of poor esthetics reducing the predictability of results. Implants inserted in association with bone grafts or membranes are indicated for procedures on the esthetic zone, but function is restored only after the healing period.13Grandi T, Guazzi P, Samarani R, Grandi G. Clinical outcome and bone healing of implants placed with high insertion torque: 12-month results from a multicenter controlled cohort study. → International journal of oral and maxillofacial surgery. 2013. 42(4);516–20. Many types of grafts have been used to restore bone and gingival defects. The maxillary tuberosity is one of the important donor areas mentioned in many papers14Balasubramaniam AS, Raja SV, Thomas LJ. Peri-implant esthetics assessment and management. → Dent Res J (Isfahan). 2013 Jan;10(1):7–14. doi: 10.4103/1735-3327.111757.,15Silva DB, Neves LC, Querino E, Rosa JC, Barreto MA. Behavior of peri-implant tissues in immediate implant with provisionalization: A literature review. → Dent Press Implantol. 2013 Jul–Sep;7(3):41–51. for correcting socket defects in esthetic areas. This kind of graft has shown some advantages, such as bone malleability facilitating adaptation to the defect, greater speed of graft repair, the ease of harvesting and excellent postoperative recovery; however, the disadvantages are low bone quality, limited quantity of material and difficult surgical access.16Slagter KW, den Hartog L, Bakker NA, Vissink A, Meijer HJ, Raghoebar GM. Immediate placement of dental implants in the esthetic zone: a systematic review and pooled analysis. → J Periodontol. 2014 Jul;85(7):e241–50. doi: 10.1902/jop.2014.130632.
In the present study, there was total adaptation of the soft tissue in relation to the metal-free zirconia prostheses. According to papers 17Barwacz CA, Brogden KA, Stanford CM, Dawson DV, Recker EN, Blanchette D. Comparison of proinflammatory cytokines and bone metabolism mediators around titanium and zirconia dental implant abutments following a minimum of 6 months of clinical function. → Clin Oral Implants Res. 2015 Apr;26(4):e35–41. doi: 10.1111/clr.12326. comparing the cell infiltration and expression of pro-inflammatory cytokines (lymphocytes, plasma cells) between titanium and zirconia implant abutments, higher rates were found around the titanium abutments, and our clinical results showed the same.
In the present study, we can observe that the physical properties of zirconia, like those of other ceramics, can deteriorate over time; however, a long period is necessary for this deterioration to appear, so it is very safe to predict long-lasting results for customized zirconia crowns supported on implants.18Studart AR, Filser F, Kocher P, Gauckler LJ. In vitro lifetime of dental ceramics under cyclic loading in water. → Biomaterials. 2007 Jun;28(17):2695–705.
Conclusion
The proposed technique, as described in the literature, has proved clinically effective for esthetic edentulous areas and shown significant predictability of results. The immediate reconstruction of the buccal plate with an autologous graft was an efficient procedure for recovering lost anatomical structure. Throughout the follow-up, the stability of hard and soft tissue was observed. Despite the positive outcomes, there is a need for further research to improve the technique and compare the results between different types of grafts for use in this type of case.
Competing interests
The authors declare that they have no competing interests.
Legends
Fig. 1 – Initial clinical condition.
Figs. 2a–c – Confirmation of fracture and inflammatory lesions on the CBCT scan.
Fig. 3a – Inflammatory lesion attached to the fractured tooth.
Fig. 3b – Confirmation of the probing depth and buccal bone loss.
Figs. 4a–d – Socket preparation and placement of the dental implants.
Fig. 5 – Maxillary tuberosity graft positioned between the vestibular plate and the implant.
Figs. 6a & b – Final aspect after 6 months of healing.
Figs. 7a & b – Copying the emergence profiles.
Figs. 8a–c – Final impression and working cast.
Figs. 9a–c – Final prosthesis.
Interview
with Dr. Igor da Silva Brum
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Muhamad AH, Georges C, Azzaldeen A. Immediate Implants Placed Into Infected Sockets: Clinical Update with 3-Year Follow-Up. → J Dent Med Sci. 2017, 16, pp.0853-160109105111. |
| 2. | ↑ | Esposito M, Trullenque-Eriksson A, Blasone R, Malaguti G, Gaffuri C, Caneva M, Minciarelli A, Luongo G. Clinical evaluation of a novel dental implant system as single implants under immediate loading conditions— 4-month post-loading results from a multicentre randomised controlled trial. → Eur J Oral Implantol. 2016;9(4):367–79. |
| 3. | ↑ | De Molon RS, de Avila ED, Cirelli JA, Mollo F de A Jr, de Andrade MF, Filho LA, Barros LA. A combined approach for the treatment of resorbed fresh sockets allowing immediate implant restoration: a 2-year followup. → J Oral Implantol. 2015 Dec;41(6):712–8. |
| 4. | ↑ | De Molon RS, de Avila ED, de Barros-Filho LA, Ricci WA, Tetradis S, Cirelli JA, Borelli de Barros LA. Reconstruction of the alveolar buccal bone plate in compromised fresh socket after immediate implant placement followed by immediate provisionalization. → J Esthet Restor Dent. 2015 May–Jun;27(3):122–35. |
| 5. | ↑ | Rosa AC, Francischone CE, Cardoso Mde A, Alonso AC, Filho LC, Da Rosa JC. Post-traumatic treatment of maxillary incisors by immediate dentoalveolar restoration with long-term follow-up. → Compend Contin Educ Dent. 2015 Feb;36(2):130–4. |
| 6. | ↑ | Rosa JC, Rosa AC, Francischone CE, Sotto-Maior BS. Esthetic outcomes and tissue stability of implant placement in compromised sockets following immediate dentoalveolar restoration: results of a prospective case series at 58 months follow-up. → Int J Periodontics Restorative Dent. 2014 Mar–Apr;34(2):199–208. |
| 7. | ↑ | Zhang S, Wang S, Song Y. Immediate loading for implant restoration compared with early or conventional loading: A meta-analysis. → J Craniomaxillofac Surg. 2017 Jun;45(6):793–803. doi: 10.1016/j.jcms.2016.05.002. Epub 2016 May 14. |
| 8. | ↑ | Da Rosa JC, Rosa AC, da Rosa DM, Zardo CM. Immediate dentoalveolar restoration of compromised sockets: a novel technique. → Eur J Esthet Dent. 2013 Autumn;8(3):432–43. |
| 9. | ↑ | Crespi R, Capparè P, Gherlone E, Romanos GE. Immediate occlusal loading of implants placed in fresh sockets after tooth extraction. → Int J Oral Maxillofac Implants. 2007 Nov–Dec;22(6):955–62. |
| 10. | ↑ | Vandamme K, Naert I, Geris L, Sloten JV, Puers R, Duyck J. Histodynamics of bone tissue formation around immediately loaded cylindrical implants in the rabbit. → Clinical oral implants research. 2007;18(4):471–80. |
| 11. | ↑ | Rojas-Vizcaya F. Rehabilitation of the maxillary arch with implant-supported fixed restorations guided by the most apical buccal bone level in the esthetic zone: A clinical report. → The Journal of prosthetic dentistry. 2012. 107(4);213–20. |
| 12. | ↑ | De Rouck T, Collys K, Cosyn J. Single-tooth replacement in the anterior maxilla by means of immediate implantation and provisionalization: a review. → Int J Oral Maxillofac Implants. 2008 Sep–Oct;23(5):897–904. |
| 13. | ↑ | Grandi T, Guazzi P, Samarani R, Grandi G. Clinical outcome and bone healing of implants placed with high insertion torque: 12-month results from a multicenter controlled cohort study. → International journal of oral and maxillofacial surgery. 2013. 42(4);516–20. |
| 14. | ↑ | Balasubramaniam AS, Raja SV, Thomas LJ. Peri-implant esthetics assessment and management. → Dent Res J (Isfahan). 2013 Jan;10(1):7–14. doi: 10.4103/1735-3327.111757. |
| 15. | ↑ | Silva DB, Neves LC, Querino E, Rosa JC, Barreto MA. Behavior of peri-implant tissues in immediate implant with provisionalization: A literature review. → Dent Press Implantol. 2013 Jul–Sep;7(3):41–51. |
| 16. | ↑ | Slagter KW, den Hartog L, Bakker NA, Vissink A, Meijer HJ, Raghoebar GM. Immediate placement of dental implants in the esthetic zone: a systematic review and pooled analysis. → J Periodontol. 2014 Jul;85(7):e241–50. doi: 10.1902/jop.2014.130632. |
| 17. | ↑ | Barwacz CA, Brogden KA, Stanford CM, Dawson DV, Recker EN, Blanchette D. Comparison of proinflammatory cytokines and bone metabolism mediators around titanium and zirconia dental implant abutments following a minimum of 6 months of clinical function. → Clin Oral Implants Res. 2015 Apr;26(4):e35–41. doi: 10.1111/clr.12326. |
| 18. | ↑ | Studart AR, Filser F, Kocher P, Gauckler LJ. In vitro lifetime of dental ceramics under cyclic loading in water. → Biomaterials. 2007 Jun;28(17):2695–705. |





Leave a Reply
Be the First to Comment!