Importance of a preoperative radiographic scale for evaluating surgical difficulty of impacted mandibular third molar extraction
March 22, 2017 / Categories: Digital Dentistry, Implant Dentistry

Ribes Lainez, Natalia

Sanchis González, José Carlos

Peñarrocha Oltra, David

Sanchis Bielsa, José María
The objectives of the study were to evaluate the correlation between the degree of surgical difficulty measured by an established scale and the total surgical time, the ostectomy time and the tooth sectioning time, and to analyze which of the factors involved had a greater influence on total surgical time.
Abstract
Objective
The objectives of the study were to evaluate the correlation between the degree of surgical difficulty measured by an established scale and the total surgical time, the ostectomy time and the tooth sectioning time, and to analyze which of the factors involved had a greater influence on total surgical time.
Materials and methods
A presurgical radiographic scale was developed, based on ten parameters. Each parameter was scored from 1 to 3, and the individual scores were summed. A retrospective analysis using panoramic radiographs was performed of patients subjected to surgical extraction of a mandibular third molar, with recording of the surgical times. A statistical analysis was performed to establish correlations between the study parameters and scale and the surgical times.
Results
A greater Winter’s distance prolonged ostectomy time and, conversely, a greater distance from the mandibular ramus to the distal surface of the second molar was observed to shorten ostectomy time. Separate or dysmorphic root shape increased ostectomy time and total surgical time. Total surgical time was longer in the presence of greater coronal width and a shorter distance from the ramus to the second molar. The only variable correlated to tooth sectioning time was coronal width.
Conclusion
The final score was correlated to ostectomy time and total surgical time. Ostectomy time in turn was influenced by Winter’s distance, the distance from the mandibular ramus to the second molar, and root shape. Tooth sectioning time was influenced by the coronal width of the third molar. The parameters with the closest correlation to total surgical time were coronal width and the distance between the ramus and second molar.
Keywords
Third molar surgery, wisdom teeth, impacted mandibular third molar, third molar extraction.
Introduction
A number of classification systems have been proposed for estimating the surgical difficulty of impacted mandibular third molar extraction, based on preoperative assessment of panoramic
radiographs.The traditional classifications are those of Pell and Gregory1Pell G. Gregory B. Impacted mandibular third molars: classification and modified techniques for removal.
→ Dent Dig. 1993;39:330–8. and Winter,2Winter GB. Principles of exodontia as applied to the impacted third molar.
→ St Louis: American Medical Book Co; 1926. p.21-58. based on the depth of the third molar, the relation to the mandibular ramus and the anatomical position in relation to the longitudinal axis of the adjacent second molar. Over the years, different modifications of these scales have been proposed with the aim of improving the prediction of surgical difficulty. In this regard, Pederson proposed a modification of the scale of Pell and Gregory that contemplated an additional factor: the position of the molar.3Pederson GW. Oral surgery. Philadelphia: WB Saunders, 1988 (Cited in: Koerner KR. The removal of impacted third molarsprinciples and procedures.
→ Dent Clin North Am. 1994;38:255-78). Each variable was assigned a score of 1–4 according to its influence upon the difficulty of extraction, and these scores were then summed to yield a final score predicting surgical difficulty: 3–4 (not difficult), 5–7 (moderate difficulty) and 7–10 (great difficulty). This scale has been widely cited in the oral and maxillofacial surgical literature as an easy way to predict the surgical difficulty of impacted mandibular third molar extraction.
Cáceres Madroño et al. added further parameters to the scale of Pedersen, such as mandibular height, distal inclination of the second molar, size and shape of the dental follicle, and development of the roots.4Cáceres Madroño E, Martinez-González JM, Meníz García C, López Carriches C, Madrigal Martínez-Pereda C. Estudio del grado de dificultad en la extracción de los terceros molares inferiores en relación con la experiencia profesional; Periodo preoperatorio (Parte I).
→ Arch Odontoestomatol. 1998;14(4):229–37. Peñarrocha et al. in turn summed the scores corresponding to pericoronal radiolucency, pericoronal space, Winter’s distance and coronal area, and subdivided the size and shape of the roots into two separate parameters: the length of the root and the type of root.5Peñarrocha M, Sanchis JM, Sáez U, Gay Escoda C, Bagán JV. Escala numérica de valoración de la dificultad quirúrgica en la extracción de 190 terceros molares mandibulares incluidos.
→ Arch Odontoestomatol. 2000;16(2):96–100. Each variable was scored from 0 to 2, and the individual scores were summed to yield a final surgical difficulty score: 0–5 (not difficult), 6–10 (average difficulty) and over 10 (great difficulty). This is one of the scales involving the largest number of parameters, and higher scores have been shown to correspond to longer ostectomy times and total surgical times thereby confirming the efficacy of the classification.6Peñarrocha M, Sanchis JM, Sáez U, Gay Escoda C, Bagán JV. Escala numérica de valoración de la dificultad quirúrgica en la extracción de 190 terceros molares mandibulares incluidos.
→ Arch Odontoestomatol. 2000;16(2):96–100.
Another clinical and radiographic scale for predicting the difficulty of third molar extraction was developed by Romero-Ruiz et al., based on the classical parameters with the addition of integrity of the bone and mucosa covering the third molar.7Romero Ruiz MM. El tercer molar incluido.
→ In: Romero Ruiz MM, Gutiérrez Pérez JL, editors. El tercer molar incluido. Madrid: GSK; 2001. p. 43–69. Minimum surgical difficulty was predicted if the tooth was covered only by mucosa, while maximum difficulty corresponded to molars fully covered by bone and mucosa.
Predicting the surgical difficulty of impacted mandibular third molar extraction is essential for treatment planning and helps assess professional surgical skill, reduces complications, optimizes patient preparation, and minimizes postoperative pain and inflammation.
The present study describes a radiographic surgical difficulty scale based on a series of parameters and compares it with ostectomy time, tooth sectioning time, the presence or absence of additional ostectomy, and total surgical time. In addition, actual measurements of the radiographic parameters were taken to identify those that had the greatest impact upon surgical difficulty.
Materials and methods
A retrospective study using panoramic radiographs was conducted of patients subjected to surgical extraction of an impacted mandibular third molar in the Department of Stomatology and Maxillofacial Surgery (General University Hospital of Valencia, Valencia, Spain), with recording of the following surgical times: ostectomy time and tooth sectioning time (in seconds) and total surgical time (in minutes), calculated from the start of the incision to the last suture. A presurgical radiographic scale was developed (Figs. 1-10), based on ten parameters that were recorded by three dental students of the Faculty of Medicine and Odontology, University of Valencia, Valencia, Spain, using ImageJ software (64-bit; developed by the U.S. National Institutes of Health, Bethesda, Md.)7, with calculation of the corresponding mean values: inclination of the third molar, inclination of the second molar, pericoronal radiolucency, root radiolucency, root shape, Winter’s distance, distance between the ramus and second molar, width of the third molar, coronal area and root length.
Calibration was carried out based on the calculation of the distortion of the radiographic measurements versus the real measurements of the third molar, using radiographic measurements of the diameter and length of 15 impacted mandibular third molars, exported to ImageJ, and caliper measurements obtained after extraction of the third molar, respectively. The statistical analysis of these dual measurements (ImageJ and calipers) showed the distortion coefficient to be 0.11.
The final score was obtained by summing the individual scores for each parameter, coded as follows for statistical processing: 1 = not difficult (10–16 points), 2 = average difficulty (17– 23 points) and 3 = difficult (24–30 points). The data were processed using the SPSS statistical package (IBM SPSS Statistics for Windows, Version 21.0, IBM, Armonk, N.Y., U.S.). Normal distribution of the variables was evaluated by the Kolmogorov–Smirnov test and was confirmed in all cases. Multivariate analysis was performed, involving the estimation of a general linear multiple regression model for the selected response variable (time) as a function of the study parameters and surgical difficulty scores. The accepted level of statistical significance was 5% (α = 0.05).
-

- Fig. 1a
-
- Fig. 1b
-

- Fig. 1c
-
- Fig. 2a
-
- Fig. 2b
-

- Fig. 2c
-
- Fig. 3a
-

- Fig. 3b
-

- Fig. 3c
-
- Fig. 4a

-

- Fig. 4b

-

- Fig. 4c

-
- Fig. 5a
-

- Fig. 5b
-
- Fig. 5c
-

- Fig. 6a

-
- Fig. 6b
-
- Fig. 6c
-

- Fig. 7a

-

- Fig. 7b

-

- Fig. 7c
-

- Fig. 8a
-
- Fig. 8b
-

- Fig. 8c
Results
One hundred patients (41 men and 59 women) between 18 and 45 years of age (mean age of 24.9 ± 6.5 years) were analyzed. Mandibular left (n = 49) and right (n = 51) third molars were extracted. The maximum final score was 27 points, with a minimum final score of 13 (mean final score of 19.4 ± 2.6 points). Extraction was not difficult in 14.6% of the patients (10–16 points on the surgical difficulty scale), of average difficulty in 79.2% (17–23 points) and difficult in 6.3% (24–30 points).
The maximum ostectomy time was 180 s, with a minimum time of 10 s (mean of 54.4 ± 28.2 s). Tooth sectioning was carried out in 74 cases, with a mean duration of 73.4 ± 45.7 s (maximum of 284 s). The mean total surgical time was 10.8 ± 5.3 min (maximum of 30 min and minimum of 4 min).
The mean total surgical time was significantly longer in the case of molars with mesial inclination and in distal or horizontal presentations (p = 0.043). There were no great differences on comparing inclination of the second molar and pericoronal and root radiolucency. However, very significant differences were observed on comparing root shape with ostectomy time (p = 0.001) and total surgical time (p = 0.001; Table 1).
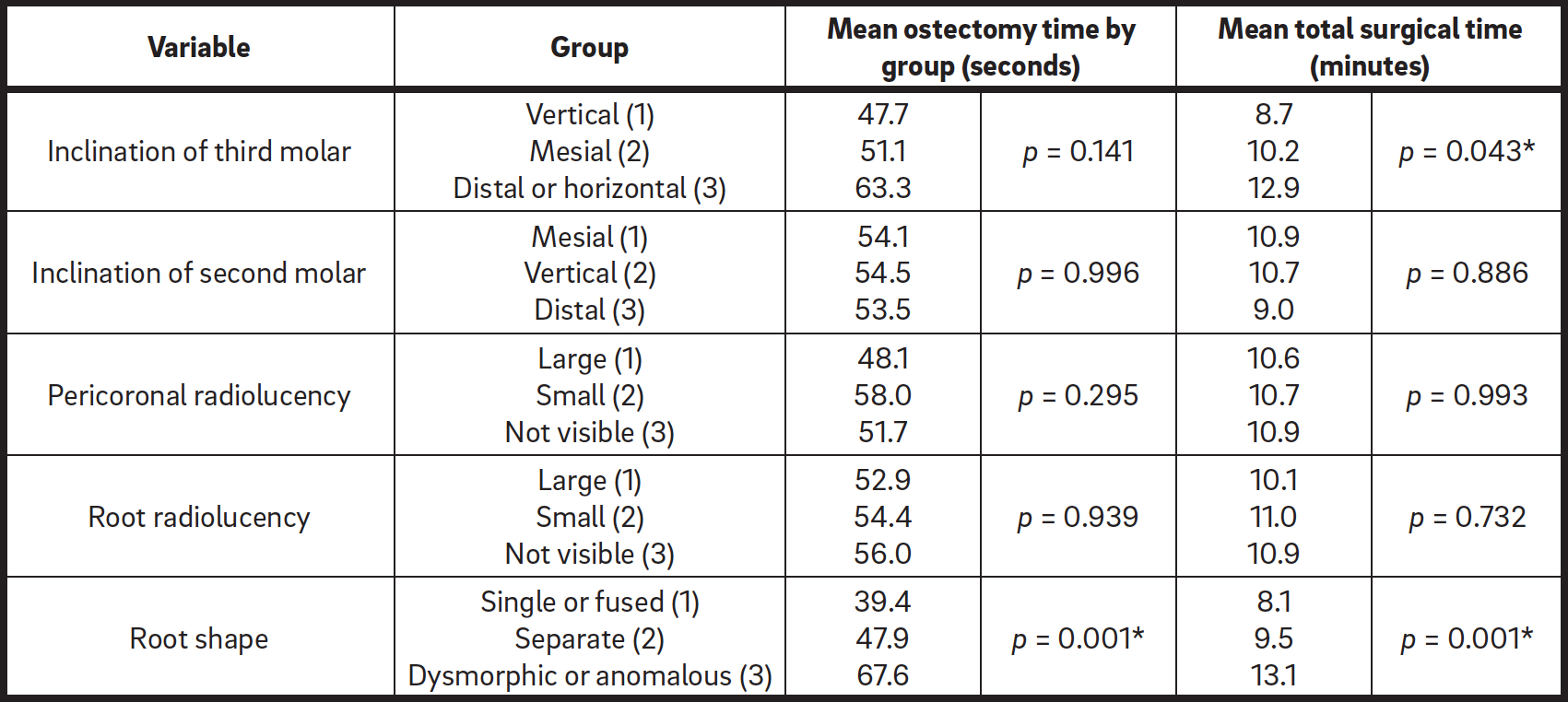
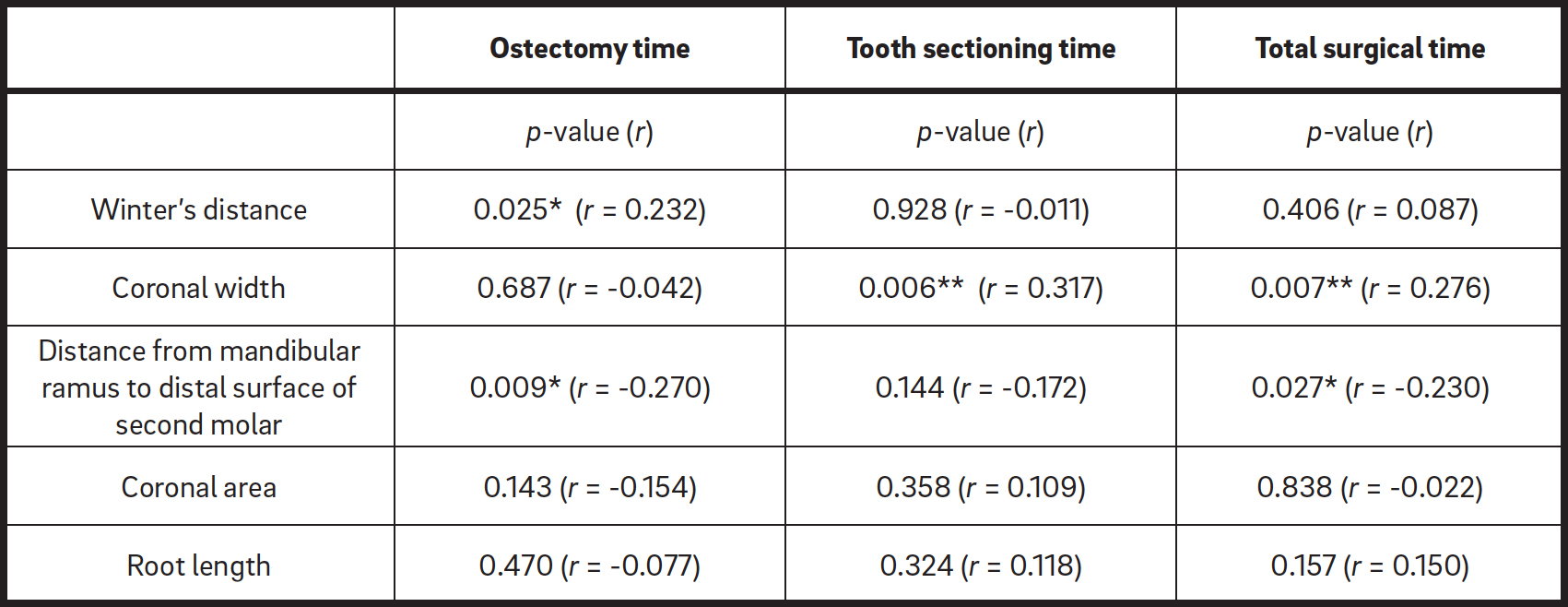
Table 1
Study parameters with the greatest influence upon surgical difficulty.
Table 2
Correlation of the quantitative parameters to the variable time according to the general linear multiple regression model.
The general linear multiple regression model showed the quantitative parameters with the greatest influence upon ostectomy time to be Winter’s distance and the distance from the ascending ramus to the second molar.
A greater Winter’s distance prolonged ostectomy time and, conversely, a greater distance from the mandibular ramus to the distal surface of the second molar was observed to shorten ostectomy time. The parameters found to be linearly correlated to total surgical time were coronal width and the distance from the ramus to the second molar.
Total surgical time was longer in the presence of greater coronal width and a shorter distance from the ramus to the second molar. The only variable correlated to tooth sectioning time was coronal width (Table 2).




According to the model, higher scores on the radiographic scale were associated with longer ostectomy time and total surgical time. For each additional point increase on the scale, the ostectomy time was seen to increase by 2.89 s, while the total surgical time increased by 0.56 s.
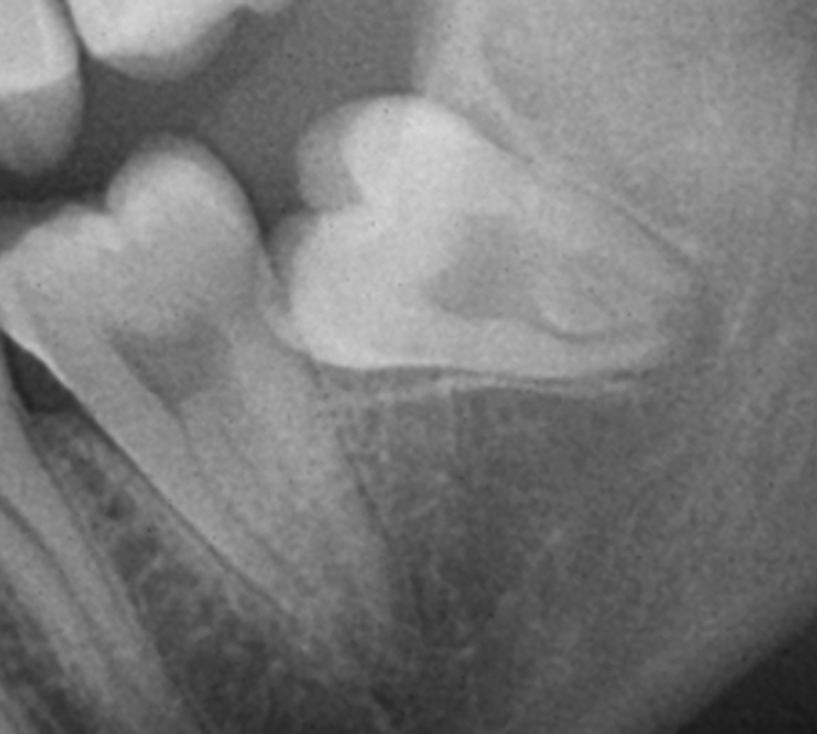
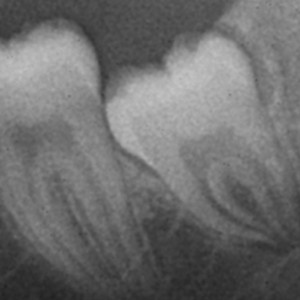
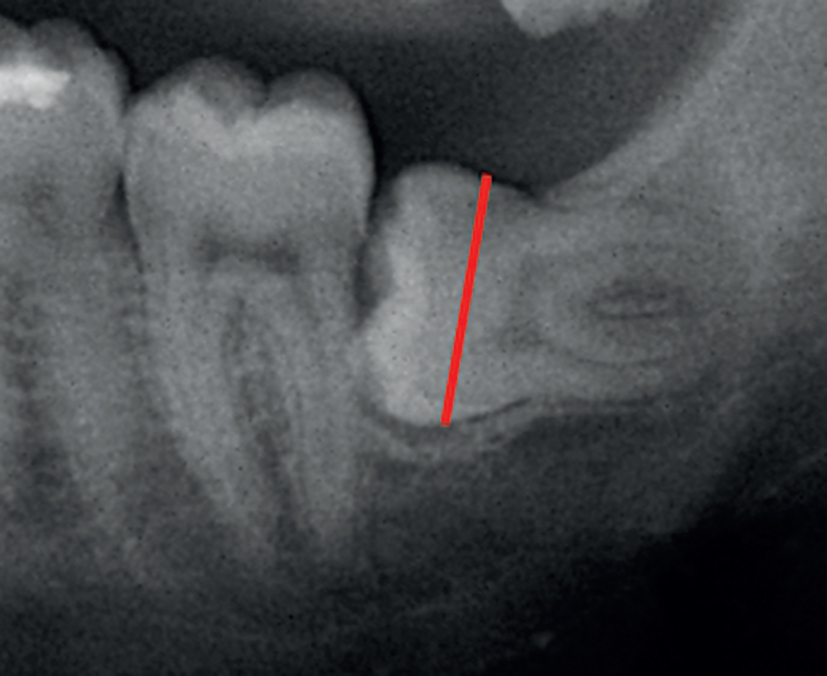
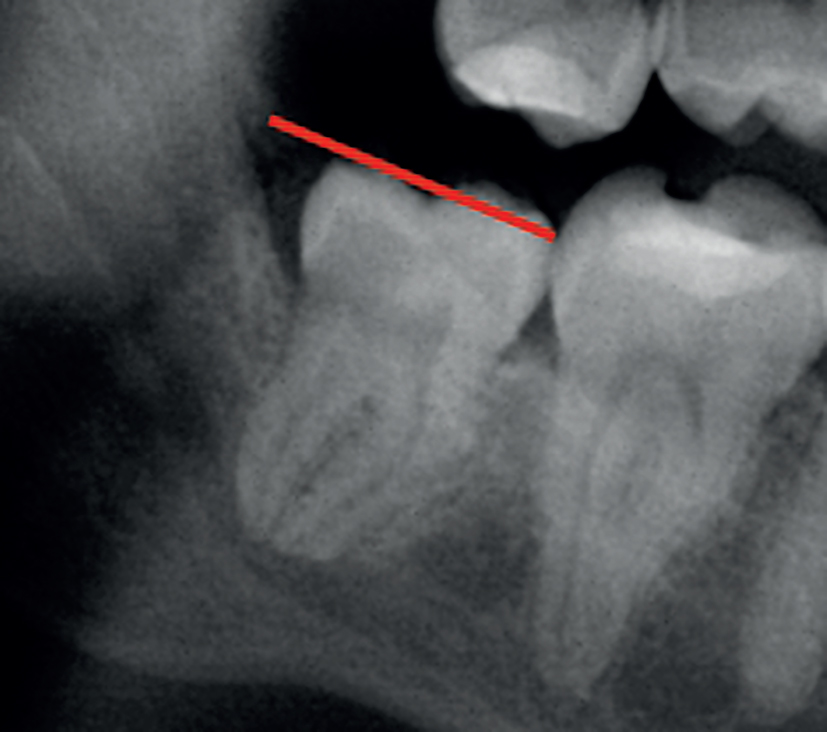
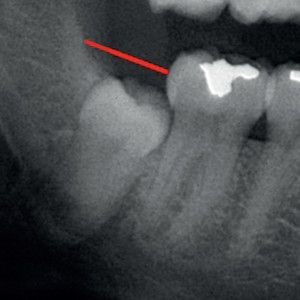
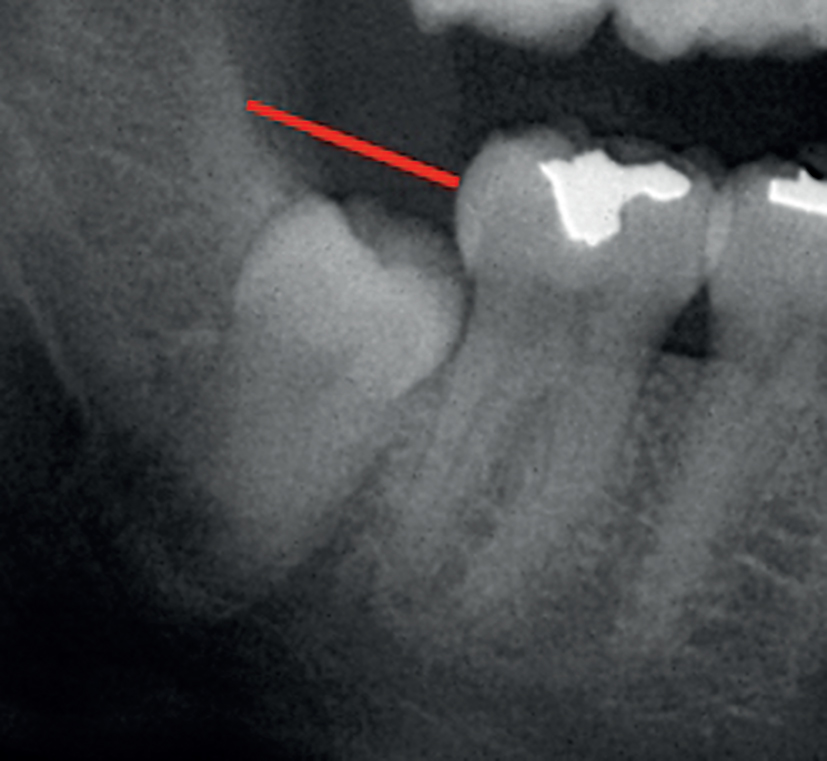
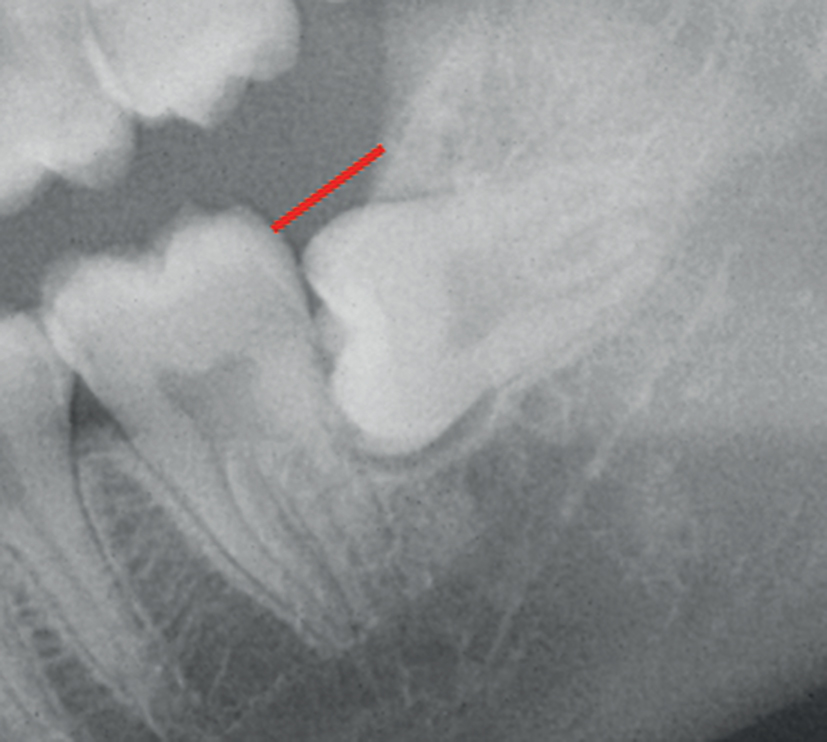
Figs. 1a-c
Inclination of third molar:
(a) vertical (1);
(b) mesial (2); and
(c) distal or horizontal (3).
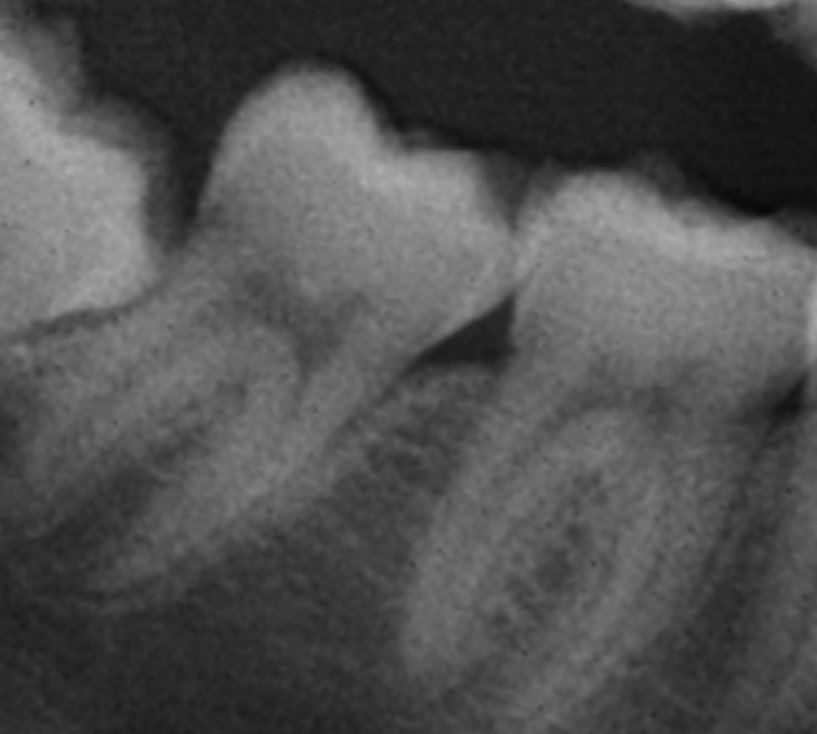
Figs. 2a-c
Inclination of second molar:
(a) mesial (1);
(b) vertical (2); and
(c) distal (3).
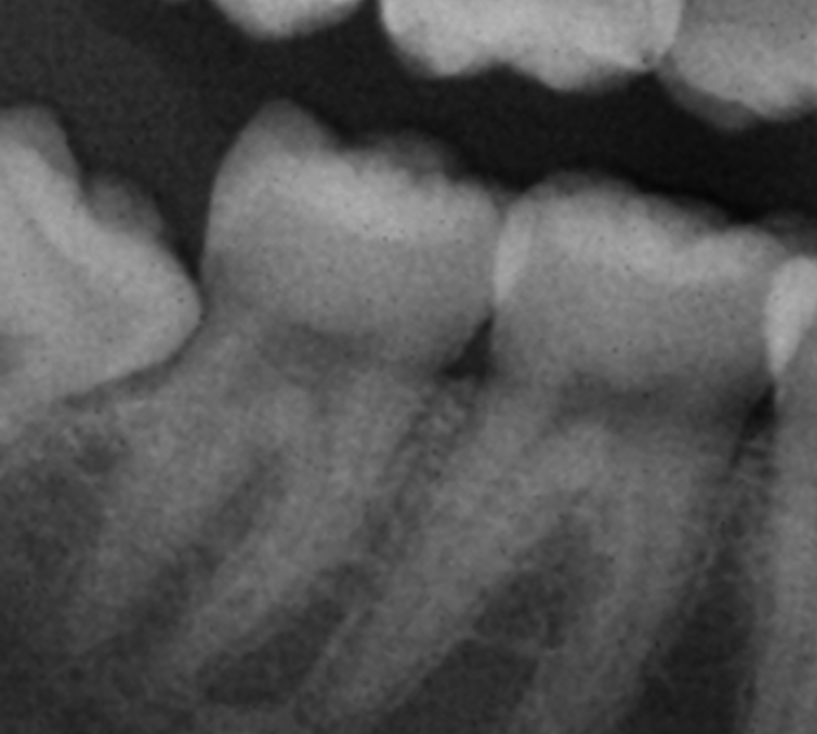
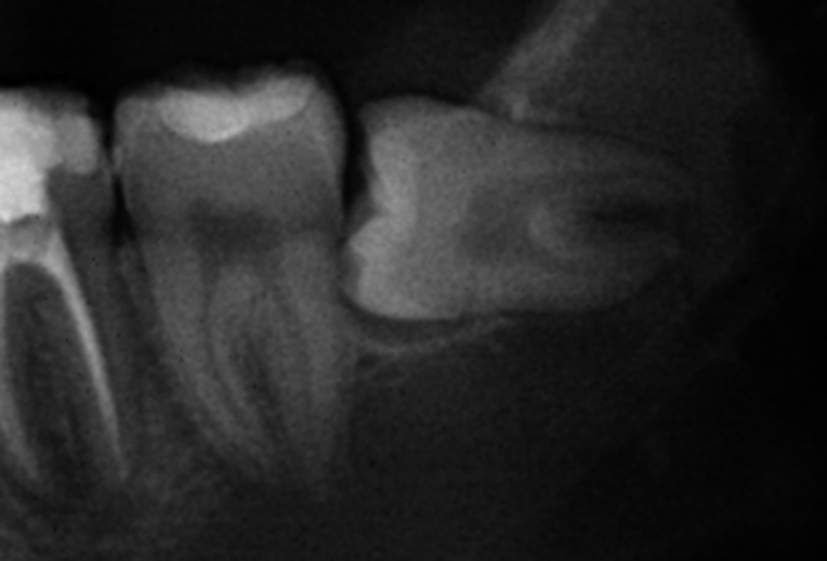
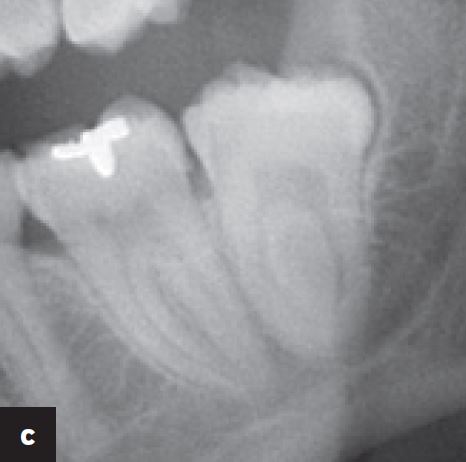
Figs. 3a-c
Pericoronal radiolucency:
(a) large (1);
(b) small (2); and
(c) not visible (3).
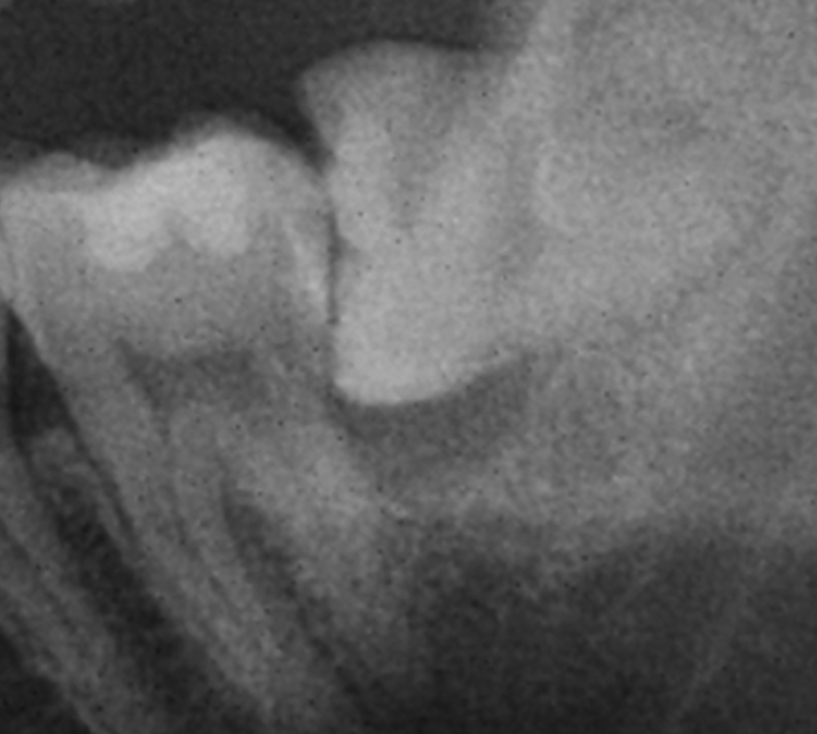
Figs. 4a-c
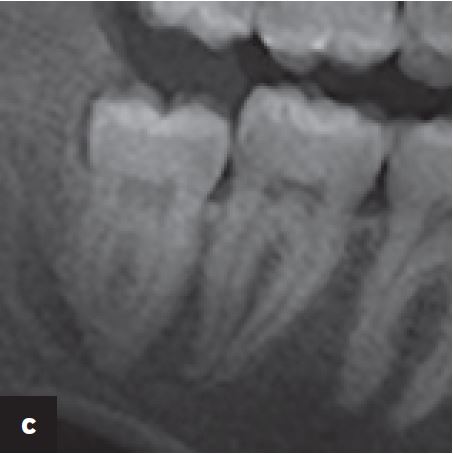
Root radiolucency:
(a) large (1);
(b) small (2); and
(c) not visible (3).
Figs. 5a-c
Root shape:
(a) single or fused (1);
(b) separate (2); and
(c) dysmorphic or
anomalous (3).
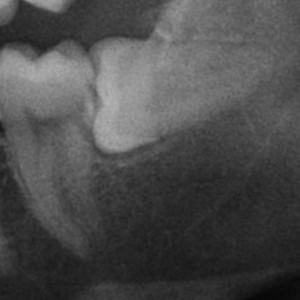
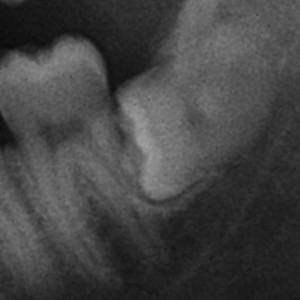
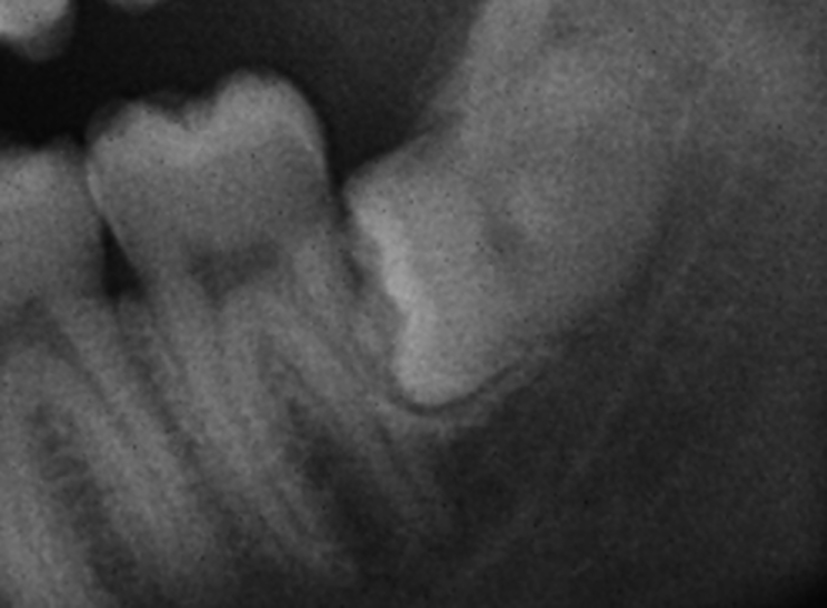
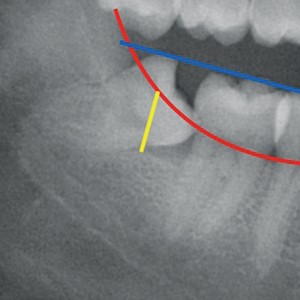
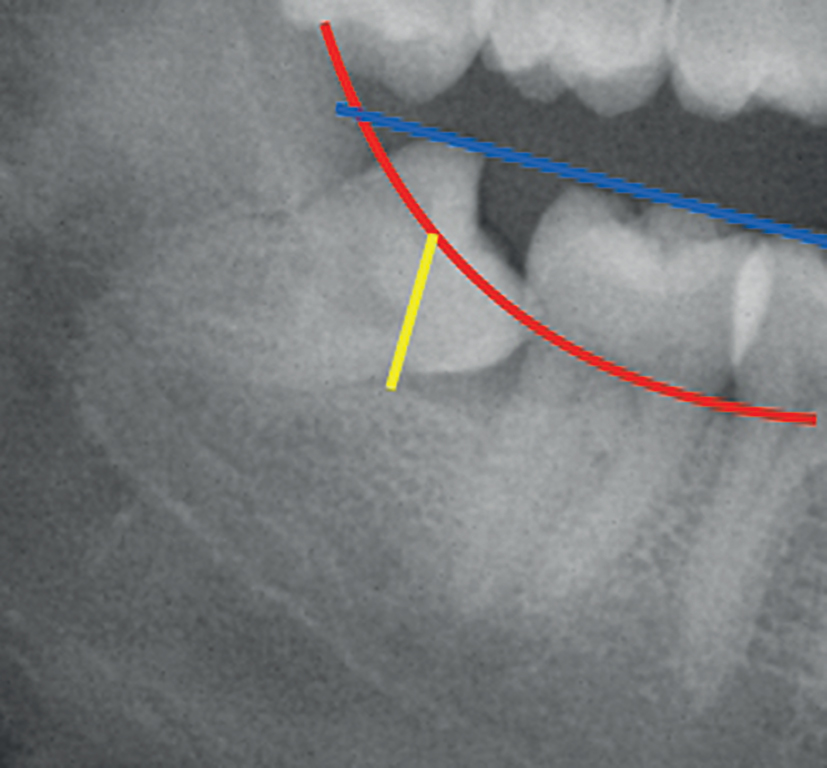
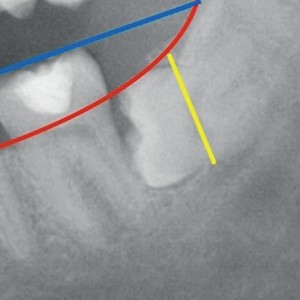
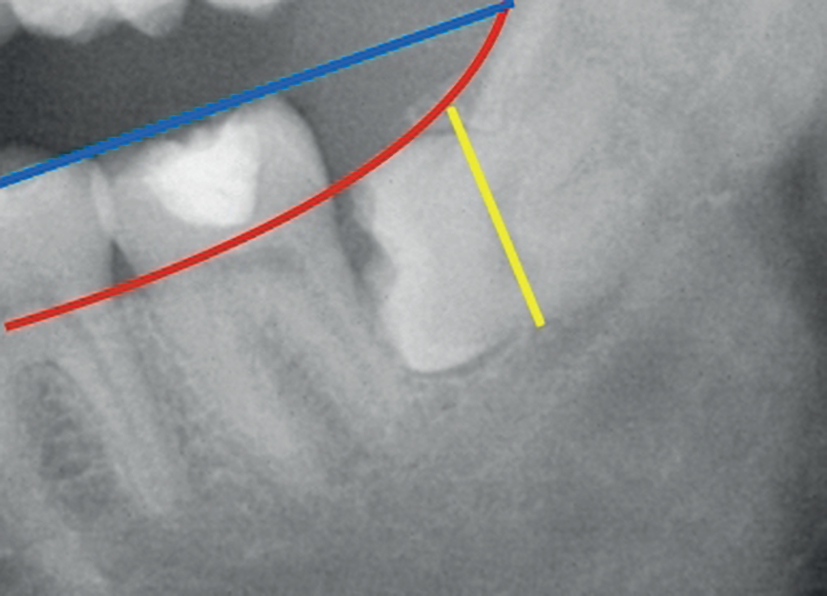
Figs. 6a-c
Winter’s distance:
(a) < 5 mm (1); (b) 5–9 mm (2); and (c) > 9 mm (3).
Figs. 7a-c
Coronal width:
(a) < 10.0 mm (1); (b) 10.0–11.5 mm (2); and (c) > 11.5 mm (3).
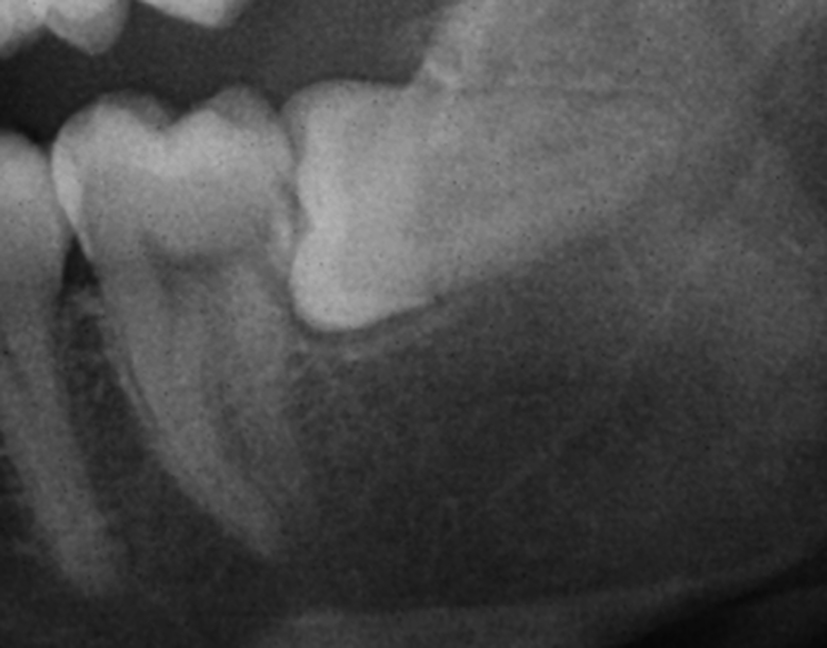
Figs. 8a-c
Distance from mandibular
ramus to distal surface of the
second molar:
(a) 10.5–14 mm (1);
(b) 8.0–10.5 mm (2); and
(c) 2.0–8.0 mm (3).
Figs. 9a-c
Coronal area:
(a) 20–75 mm2 (1);
(b) 75–90 mm2 (2); and
(c) 90–130 mm2 (3).
Figs. 10a-c
Root length:
(a) 3.0–8.0 mm (1);
(b) 8.0–9.5 mm (2); and
(c) 9.5–13.0 mm (3).
Discussion
In order to successfully predict the difficulty of impacted mandibular third molar extraction, consideration is required of the clinical and radiographic findings, which not only help to plan surgery, but also to increase patient satisfaction with the treatment received. Barreiro-Torres et al. underscored the importance of operator expertise in establishing a prior diagnosis of surgical difficulty, since an expert dental professional tends to underestimate surgery and only examine the radiographs and this in turn can lead to a failed estimation of extraction difficulty.8Barreiro-Torres J, Diniz-Freitas M, Lago-Méndez L, Gude-Sampedro F, Gándara-Rey JM, García-García A. Evaluation of the surgical difficulty in lower third molar extraction.
→ Med Oral Patol Oral Cir Bucal. 2010 Nov 1;15(6):e869–74.
The various systems developed for estimating surgical difficulty in extracting impacted mandibular third molars are based on preoperative examination of the panoramic radiographs. Although the classifications of Pell and Gregory9Pell G. Gregory B. Impacted mandibular third molars: classification and modified techniques for removal.
→ Dent Dig. 1993;39:330–8. and Winter10Winter GB. Principles of exodontia as applied to the impacted third molar.
→ St Louis: American Medical Book Co; 1926. p.21-58. have served as references, some authors, such as García-García et al.,11García-García A, Gude-Sampedro J, Gándara-Rey JM, Gándara-Vila P, Somoza-Martin M. Pell-Gregory classification is unreliable as a predictor of difficulty in extracting impacted lower third molars.
→ Br J Oral Maxillofac Surg. 2000 Dec;38(6):585–7. have found the classification of Pell and Gregory to offer low sensitivity: It failed to detect many of those cases that subsequently proved to be very difficult when classified with the scale of Parant.12Parant M. Petite Chirurgie de la Bouche. Paris: Expansion Cientifique, 1974. (Cited in: García GA. Sampedro GF, Rey GJ, Torreira GM. Trismus and pain after removal of impacted lower third molars.)
→ J Oral Maxillofac Surg. 1997;55:1223-6. This scale,13Parant M. Petite Chirurgie de la Bouche. Paris: Expansion Cientifique, 1974. (Cited in: García GA. Sampedro GF, Rey GJ, Torreira GM. Trismus and pain after removal of impacted lower third molars.)
→ J Oral Maxillofac Surg. 1997;55:1223-6. in contrast to the presurgical radiographic scale used in the present study, was designed to assess the difficulty of extraction from the clinical perspective: It is based on the need for rating from greater to lesser surgical effort, but lacks predictive value. Pedersen14Pederson GW. Oral surgery. Philadelphia: WB Saunders, 1988 (Cited in: Koerner KR. The removal of impacted third molarsprinciples and procedures.
→ Dent Clin North Am. 1994;38:255-78). added a further factor to the classification of Pell and Gregory15Pell G. Gregory B. Impacted mandibular third molars: classification and modified techniques for removal.
→ Dent Dig. 1993;39:330–8. the position of the third molar and predicted surgical difficulty from the sum of the individual scores of the scale.
With the aim of establishing a preoperative diagnosis of surgical difficulty, various investigators have proposed scales based on a series of clinical and radiographic parameters. Peñarrocha et al. added the variables of inclination of the third molar and inclination of the second molar, pericoronal radiolucency, pericoronal space, Winter’s distance, length and type of root, and coronal area to the classical variables of Pell and Gregory,16Pell G. Gregory B. Impacted mandibular third molars: classification and modified techniques for removal.
→ Dent Dig. 1993;39:330–8. producing the predictive scale with the largest number of variables to date, and adding ostectomy time as an indicator of surgical difficulty.17Peñarrocha M, Sanchis JM, Sáez U, Gay Escoda C, Bagán JV. Escala numérica de valoración de la dificultad quirúrgica en la extracción de 190 terceros molares mandibulares incluidos.
→ Arch Odontoestomatol. 2000;16(2):96–100. These authors recorded longer ostectomy times in those cases predicted to be the most difficult extractions according to their classification. 18Peñarrocha M, Sanchis JM, Sáez U, Gay Escoda C, Bagán JV. Escala numérica de valoración de la dificultad quirúrgica en la extracción de 190 terceros molares mandibulares incluidos.
→ Arch Odontoestomatol. 2000;16(2):96–100. This is consistent with the findings of the present study, in which the variables mesiodistal diameter of the third molar and root radiolucency were added to the classification of Peñarrocha et al.,19Peñarrocha M, Sanchis JM, Sáez U, Gay Escoda C, Bagán JV. Escala numérica de valoración de la dificultad quirúrgica en la extracción de 190 terceros molares mandibulares incluidos.
→ Arch Odontoestomatol. 2000;16(2):96–100. and ostectomy time, tooth sectioning time and total surgical time were also considered.
The relationship between the difficulty of extraction and the parameters evaluated by the various presurgical scales is usually appraised on the basis of the total surgical time. The results obtained in the present study point to a linear relationship between the surgical difficulty score and the total surgical time and ostectomy time. Santamaría and Arteagoitia demonstrated a relationship between the difficulty of extraction and the depth of impaction, the width of the periodontal ligament, the inclination of the third molar, its relation to the second molar, and the distance between the mandibular ramus and the second molar.20Santamaría J, Arteagoitia I. Radiologic variables of clinical significance in the extraction of impacted mandibular third molars.
→ Oral Surg Oral Med Oral Pathol Radiol Endod. 1997 Nov;84(5):469–73. According to Yuasa et al., the most important variables for assessing the difficulty of mandibular third molar extraction are depth level C, Class 3 and large roots, or the combination of these three factors all of which can be recorded from the panoramic radiographs.21Yuasa H, Kawai T, Sugiura M. Classification of surgical difficulty in extracting impacted third molars.
→ Br J Oral Maxillofac Surg. 2002 Feb;40(1):26–31. López Arranz underscored the importance of evaluating the adjacent teeth: The presence of the first and second molars, their anatomical integrity and separate roots constitute important support for extraction of the third molar.22López Arranz JS. Diagnóstico por la imagen.
→ In: López Arranz JS, editor. Cirugía oral. Madrid: Interamericana-McGraw-Hill. 1991. p. 65–118.
In the present study, the mesiodistal diameter of the third molar and the distance between the mandibular ramus and the second molar were the parameters most closely correlated to total surgical time. This was in contrast to Carvalho and do Egito Vasconcelos, who identified the number of roots and their morphology, the position of the tooth, the periodontal space, and the relation to the second molar as the only significant predictors.23Carvalho RW, do Egito Vasconcelos BC. Assessment of factors associated with surgical difficulty during removal of impacted lower third molars.
→ J Oral Maxillofac Surg. 2011 Nov;69(11):2714–21.
These authors associated the greatest surgical difficulty with Class 3 cases on the scale of Pell and Gregory.24Pell G. Gregory B. Impacted mandibular third molars: classification and modified techniques for removal.
→ Dent Dig. 1993;39:330–8.
The observations of Yuasa et al.25Yuasa H, Kawai T, Sugiura M. Classification of surgical difficulty in extracting impacted third molars.
→ Br J Oral Maxillofac Surg. 2002 Feb;40(1):26–31. and those of the present study indicate that long distances between the ascending mandibular ramus and the distal surface of the second molar (Class 3) shorten the surgical time.
Conclusion
In summary, an analysis of the surgical difficulty of impacted mandibular third molar extraction is essential for treatment planning and helps assess professional surgical skill, reduces complications, optimizes patient preparation, and minimizes postoperative pain and inflammation.
Our scale is effective, since the mandibular third molars with the highest scores were significantly correlated to longer ostectomy time and total surgical time. The strongest predictors of ostectomy time were Winter’s distance, the distance from the mandibular ramus to the second molar, and root shape, while the strongest predictor of tooth sectioning time was coronal width. The parameters that influenced total surgical time the most were coronal width, mesial and distal or horizontal inclination of the third molar, separate and dysmorphic or anomalous roots, and the distance between the mandibular ramus and the second molar.
Competing interests
The authors declare that they have no competing interests.
References
| 1, 9, 15, 16, 24. | ↑ | Pell G. Gregory B. Impacted mandibular third molars: classification and modified techniques for removal. → Dent Dig. 1993;39:330–8. |
| 2, 10. | ↑ | Winter GB. Principles of exodontia as applied to the impacted third molar. → St Louis: American Medical Book Co; 1926. p.21-58. |
| 3, 14. | ↑ | Pederson GW. Oral surgery. Philadelphia: WB Saunders, 1988 (Cited in: Koerner KR. The removal of impacted third molarsprinciples and procedures. → Dent Clin North Am. 1994;38:255-78). |
| 4. | ↑ | Cáceres Madroño E, Martinez-González JM, Meníz García C, López Carriches C, Madrigal Martínez-Pereda C. Estudio del grado de dificultad en la extracción de los terceros molares inferiores en relación con la experiencia profesional; Periodo preoperatorio (Parte I). → Arch Odontoestomatol. 1998;14(4):229–37. |
| 5, 6, 17, 18, 19. | ↑ | Peñarrocha M, Sanchis JM, Sáez U, Gay Escoda C, Bagán JV. Escala numérica de valoración de la dificultad quirúrgica en la extracción de 190 terceros molares mandibulares incluidos. → Arch Odontoestomatol. 2000;16(2):96–100. |
| 7. | ↑ | Romero Ruiz MM. El tercer molar incluido. → In: Romero Ruiz MM, Gutiérrez Pérez JL, editors. El tercer molar incluido. Madrid: GSK; 2001. p. 43–69. |
| 8. | ↑ | Barreiro-Torres J, Diniz-Freitas M, Lago-Méndez L, Gude-Sampedro F, Gándara-Rey JM, García-García A. Evaluation of the surgical difficulty in lower third molar extraction. → Med Oral Patol Oral Cir Bucal. 2010 Nov 1;15(6):e869–74. |
| 11. | ↑ | García-García A, Gude-Sampedro J, Gándara-Rey JM, Gándara-Vila P, Somoza-Martin M. Pell-Gregory classification is unreliable as a predictor of difficulty in extracting impacted lower third molars. → Br J Oral Maxillofac Surg. 2000 Dec;38(6):585–7. |
| 12, 13. | ↑ | Parant M. Petite Chirurgie de la Bouche. Paris: Expansion Cientifique, 1974. (Cited in: García GA. Sampedro GF, Rey GJ, Torreira GM. Trismus and pain after removal of impacted lower third molars.) → J Oral Maxillofac Surg. 1997;55:1223-6. |
| 20. | ↑ | Santamaría J, Arteagoitia I. Radiologic variables of clinical significance in the extraction of impacted mandibular third molars. → Oral Surg Oral Med Oral Pathol Radiol Endod. 1997 Nov;84(5):469–73. |
| 21, 25. | ↑ | Yuasa H, Kawai T, Sugiura M. Classification of surgical difficulty in extracting impacted third molars. → Br J Oral Maxillofac Surg. 2002 Feb;40(1):26–31. |
| 22. | ↑ | López Arranz JS. Diagnóstico por la imagen. → In: López Arranz JS, editor. Cirugía oral. Madrid: Interamericana-McGraw-Hill. 1991. p. 65–118. |
| 23. | ↑ | Carvalho RW, do Egito Vasconcelos BC. Assessment of factors associated with surgical difficulty during removal of impacted lower third molars. → J Oral Maxillofac Surg. 2011 Nov;69(11):2714–21. |





Leave a Reply
Be the First to Comment!