Improved fully digital workflow to rehabilitate an edentulous patient with an implant overdenture in 4 appointments: A case report
September 18, 2017 / Categories: Digital Dentistry, Implant Dentistry

Tallarico, Marco

Schiappa, Danilo

Schipani, Franco

Cocchi, Fabio

Annucci, Marco

Xhanari, Erta
Abstract
Background
The digital revolution is changing the world, and dentistry is no exception. Through the development of new equipment and workflows, the diagnosis and treatment of patients are becoming simpler and more efficient. However, a fully digital approach to treating edentulous patients may be a challenge and time-consuming, because edentulous sites are often flat and smooth, with few features.
Case presentation
This clinical case presentation demonstrates step by step a fully digital workflow to rehabilitate a 67-year-old edentulous patient with a removable complete dental prosthesis. Treatment included cone beam computed tomography scan taken according to a modified double-scan protocol, existing removable complete dental prosthesis digitalization, computer-guided template-assisted implant placement, an optical impression taken with a modified template, a CAD/CAM titanium bar and a cobalt–chromium, friction fit superstructure framework.
Conclusion
A fully digital workflow was effective in restoring function and esthetics in an edentulous male patient treated with an overdenture fully supported by four implants and a CAD/CAM titanium bar with a low-profile attachment system.
Keywords
Intraoral scanner, digital impression, guided surgery, accuracy, dental implants, overdenture.
Introduction
Prosthetic-driven implant placement is a key factor for successful implant therapy.1Tallarico M, Meloni SM, Canullo L, Xhanari E, Polizzi G. Guided surgery for single-implant placement: a critical review.
→ J Oral Science Rehabilitation. 2016 Dec;2(4):8–14.2Polizzi G, Cantoni T, Pasini E, Tallarico M. Immediate loading of variable-thread expanding tapered-body implants placed into maxillary post-extraction or healed sites using a guided surgery approach: an up-to-five year retrospective analysis.
→ J Oral Science Rehabilitation. 2016 Sep;2(3):50–60.3Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. Five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery.
→ Clin Implant Dent Relat Res. 2016 Oct;18(5):965–72.4Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial.
→ Eur J Oral Implantol. 2014 Autumn;7(3):229–42. Hence, computer-assisted template-based implant placement has become increasingly popular owing to improved planning and the higher transfer accuracy of the virtual plan to the surgical site compared with freehand insertion or freehand final drilling.5Vermeulen J. The accuracy of implant placement by experienced surgeons: guided vs freehand approach in a simulated plastic model.
→ Int J Oral Maxillofac Implants. 2017 Mar-Apr;32(3):617–24. Nevertheless, the accuracy of computer-assisted template-based implant placement depends on several factors, from data set acquisition to the surgical procedure. Originally, guided surgery protocols advocated a dual-scan protocol.6Van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, Wendelhag I. Computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicentre study.
→ Clin Implant Dent Relat Res. 2005;7 Suppl 1:S111–20. Today, the continuous technological progress in both computer-based development and the dental manufacturing process offers additional instruments for treatment planning, surgical placement and prosthetic rehabilitation in an interdisciplinary team approach.
An accurate fit of the implant master cast affects the passive fit of an implant-supported fixed complete dental prosthesis.7Jemt T, Hjalmarsson L. In vitro measurements of precision of fit of implant-supported frameworks: a comparison between “virtual” and “physical” assessments of fit using two different techniques of measurements.
→ Clin Implant Dent Relat Res. 2012 May;14 Suppl 1:e175–82. Thus, an accurate implant impression is a prerequisite for fabricating an accurate master cast and therefore an accurately fitting prosthesis.8Pozzi A, Tallarico M, Mangani F, Barlattani A. Different implant impression techniques for edentulous patients treated with CAD/ CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading.
→ Eur J Oral Implantol. 2013 Winter;6(4):325–40. There are various implant impression techniques that have been utilized to fabricate a definitive cast for the production of an accurately fitting implant-supported fixed complete dental prosthesis.9Pozzi A, Tallarico M, Mangani F, Barlattani A. Different implant impression techniques for edentulous patients treated with CAD/ CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading.
→ Eur J Oral Implantol. 2013 Winter;6(4):325–40.10Papaspyridakos P, Chen CJ, Gallucci GO, Doukoudakis A, Weber HP, Chronopoulos V. Accuracy of implant impressions for partially and completely edentulous patients: a systematic review.
→ Int J Oral Maxillofac Implants. 2014 Jul-Aug;29(4):836–45. In a recent randomized controlled trial, it was concluded that the clinical outcome of plaster impressions for completely edentulous patients was found to be the same as for splinted polyvinyl siloxane impressions.11Pozzi A, Tallarico M, Mangani F, Barlattani A. Different implant impression techniques for edentulous patients treated with CAD/ CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading.
→ Eur J Oral Implantol. 2013 Winter;6(4):325–40. Today, there is no doubt about the potential of recent intraoral optical impression systems available on the market regarding diagnosis and treatment planning, as well as for the fabrication of fixed dental prostheses. Their accuracy compares well with traditional impression taking.12Amin S, Weber HP, Finkelman M, El Rafie K, Kudara Y, Papaspyridakos P. Digital vs. conventional full-arch implant impressions: a comparative study.
→ Clin Oral Implants Res. 2016 Dec 31. doi:10.1111/clr.12994. [Epub ahead of print]. Moreover, intraoral scanners have been successfully used in the fabrication of partial13Kattadiyil MT, Mursic Z, AlRumaih H, Goodacre CJ. Intraoral scanning of hard and soft tissues for partial removable dental prosthesis fabrication.
→ J Prosthet Dent. 2014 Sep;112(3):444–8.14Wu J, Li Y, Zhang Y. Use of intraoral scanning and 3-dimensional printing in the fabrication of a removable partial denture for a patient with limited mouth opening.
→ J Am Dent Assoc. 2017 May;148(5):338–41. and removable complete dental prostheses.15Fang JH, An X, Jeong SM, Choi BH. Development of complete dentures based on digital intraoral impressions—case report.
→ J Prosthodont Res. 2017 Jun 15. pii: S1883-1958(17)30049-X. doi:10.1016/j.jpor.2017.05.005. [Epub ahead of print]. However, scanning edentulous areas with intraoral scanners may be difficult and time-consuming because edentulous sites are smooth and devoid of features. Thus, the fabrication of complete-arch restorations remains a challenge when data are directly acquired with an intraoral scanner.
The aim of the present study is to present a fully digital pathway in a model-free approach to rehabilitate a maxillary edentulous patient with an implant overdenture. A newly developed technique to take an accurate intraoral optical impression of edentulous patient is described.
Case report
A partially edentulous 67-year-old man with a removable complete dental prosthesis in the upper jaw and a removable complete partial prosthesis in the lower jaw was referred to a private center in Rome, Italy, for a possible maxillary implant-supported rehabilitation. The patient had been edentulous in the upper jaw for years. Nevertheless, he had never been comfortable with his maxillary removable complete dental prosthesis, and he stated that he was interested in an implant-supported fixed dental prosthesis.
First clinical appointment
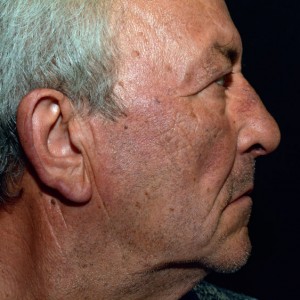
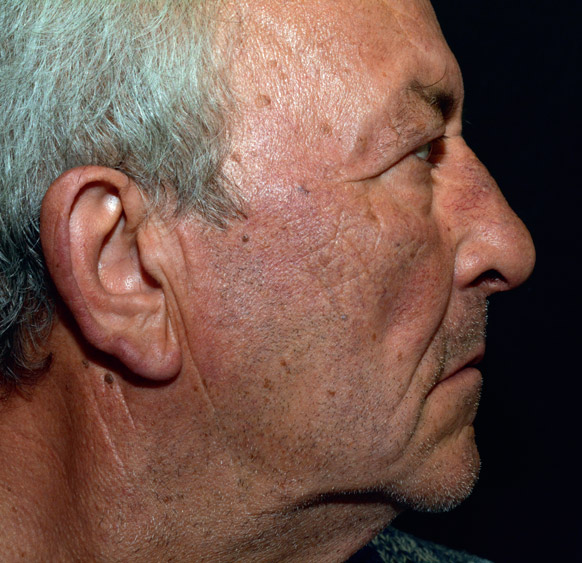
The patient’s medical history was collected and preoperative photographs, radiographs, periodontal screening and model casts were obtained for initial evaluation. During the clinical examination, the existing removable complete dental prosthesis and functional and esthetic aspects were evaluated, with particular attention to the fit of the prosthesis, vertical dimension of occlusion, facial support and lip position. Extraoral examination of the patient without the existing removable complete dental prosthesis showed a wide nasolabial angle and insufficient lip support (Figs. 1 & 2). All treatment options were then discussed and evaluated together with the patient. An implant-supported fixed dental prosthesis was excluded because of the need for facial support. Hence, a maxillary implant-supported overdenture was considered the only possible therapeutic option.
-

- Fig. 1

-
- Fig. 2
The prosthetic-driven planning workflow started with a modified double-scan protocol, with 4–6 drops of flowable composite added to the existing removable complete dental prosthesis, instead of spherical gutta-percha markers (Fig. 3).16Van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, Wendelhag I. Computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicentre study.
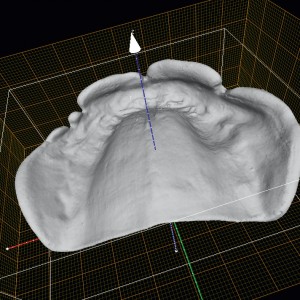
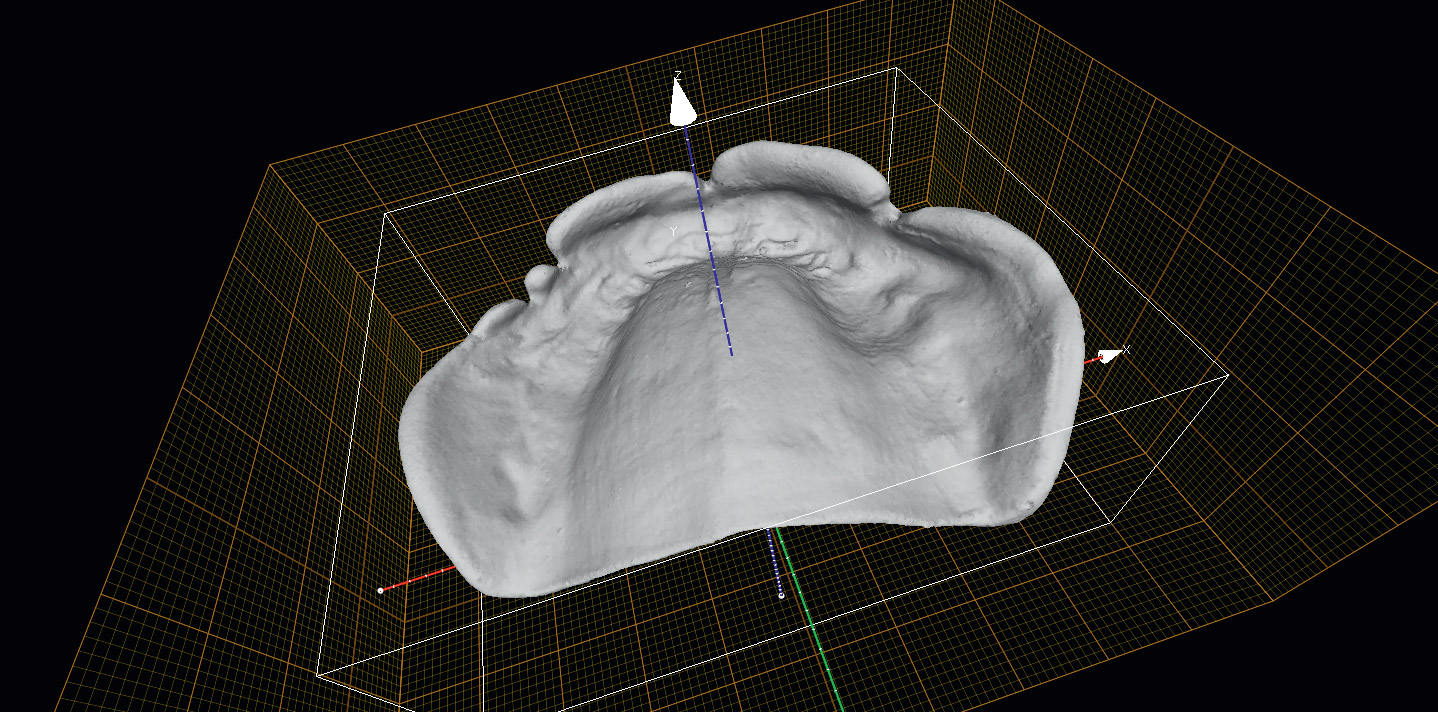
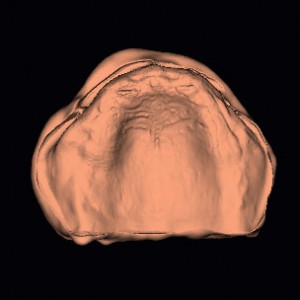
→ Clin Implant Dent Relat Res. 2005;7 Suppl 1:S111–20. In this technique, the first scan was a cone beam computed topography (CBCT) scan (CRANEX 3Dx, SOREDEX, Tuusula, Finland) of the patient wearing the existing removable complete dental prosthesis. A wax bite was used to separate the dental arches (Fig. 3). The second scan was only of the existing removable complete dental prosthesis, performed using an optical intraoral scanner (Carestream Dental, Atlanta, Ga., U.S.) to allow the merging of the DICOM data with the STL file (Figs. 4 & 5). Using reverse engineering, a virtual model was achieved (Fig. 6).
-

- Fig. 3

-

- Fig. 4

-
- Fig. 5
-
- Fig. 6

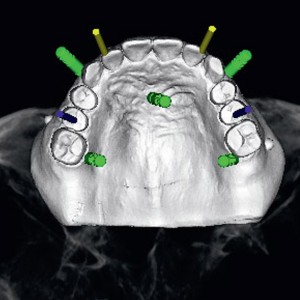
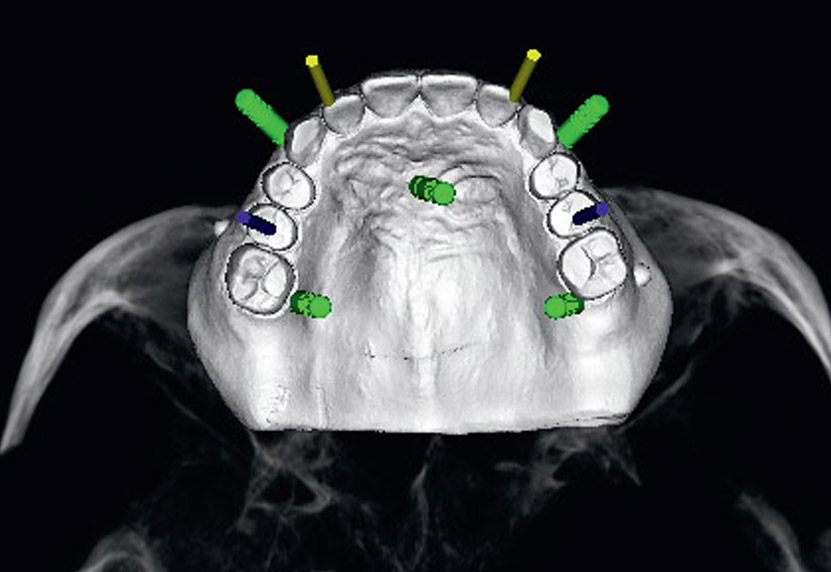
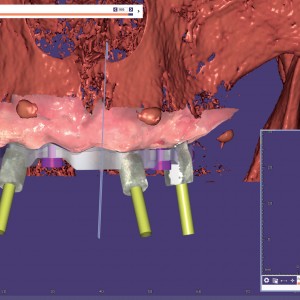
The STL and DICOM data were imported into a 3-D software planning program (3Diagnosys, Version 4.2, 3DIEMME, Cantù, Italy). The reprocessed surface extrapolated from the DICOM data and the surface of the existing removable complete dental prosthesis generated by the scanning process were merged with the best-fitting repositioning tools of the software (3Diagnosys). At this point, four prosthetic-driven implants with a diameter of 3.5 or 4.5 mm and a length of 13.0 mm (Osstem TSIII, Osstem, Seoul, South Korea) were planned, taking into account the bone quality and quantity, soft-tissue thickness, anatomical landmarks, and the type, volume and shape of the final restoration (New Ancorvis, Bargellino, Italy; Fig. 7). After careful functional and esthetic evaluation and final verification, the prosthetic-driven plan was approved, and a stereolithographic surgical template was fabricated with a newer rapid prototyping technology (New Ancorvis; Fig. 8).
-
- Fig. 7
-

- Fig. 8

Second clinical appointment
One hour before implant placement, the patient underwent professional oral hygiene, used a prophylactic antiseptic containing 0.2% chlorhexidine (CURASEPT, Curaden Healthcare, Saronno, Italy) for one min and received prophylactic antibiotic therapy (2 g of amoxicillin or 600 mg of clindamycin if allergic to penicillin). The accurate fit of the surgical templates was tried directly in the patient’s mouth (Fit Checker, GC, Tokyo, Japan). The patient was treated under local anesthesia using articaine with 1:100,000 epinephrine, administered 20 min before surgery. The surgical template was stabilized using a silicone surgical index, derived from the virtual plane, and five preplanned anchor pins (New Ancorvis). Planned implants (Osstem TSIII) were placed flapless using dedicate drills (OsstemGuide Kit, Osstem; Fig. 9). All of the implants were inserted with a minimum insertion torque of 35 N cm according to previously published protocols.17Tallarico M, Meloni SM. Open-cohort prospective study on early implant failure and physiological marginal remodeling expected using sandblasted and acid-etched bone level implants featuring an 11° Morse taper connection within one year after loading.
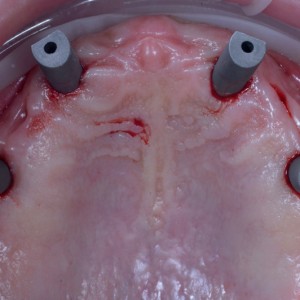
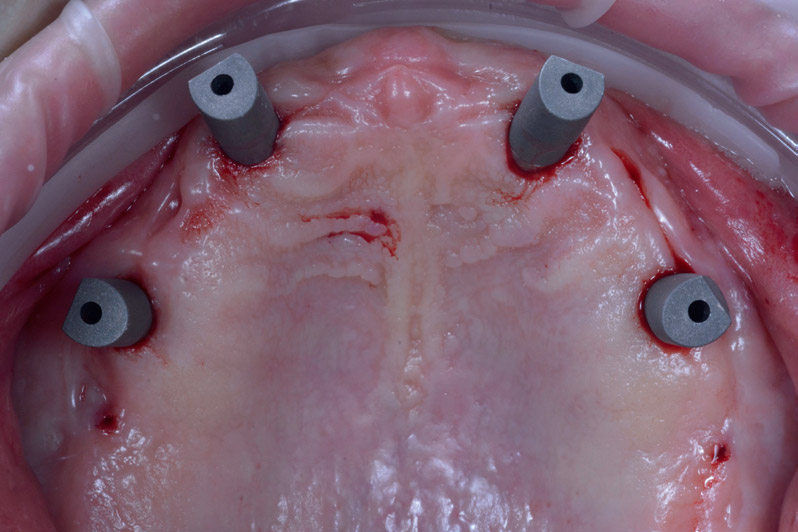
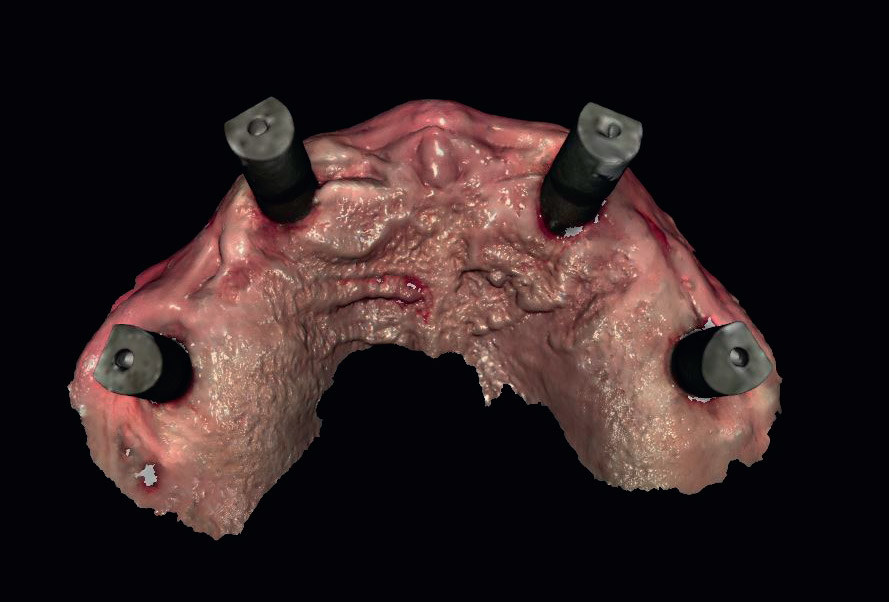
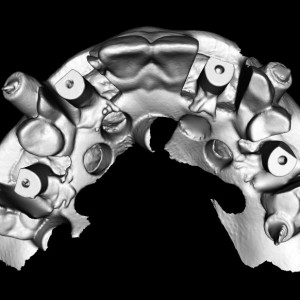
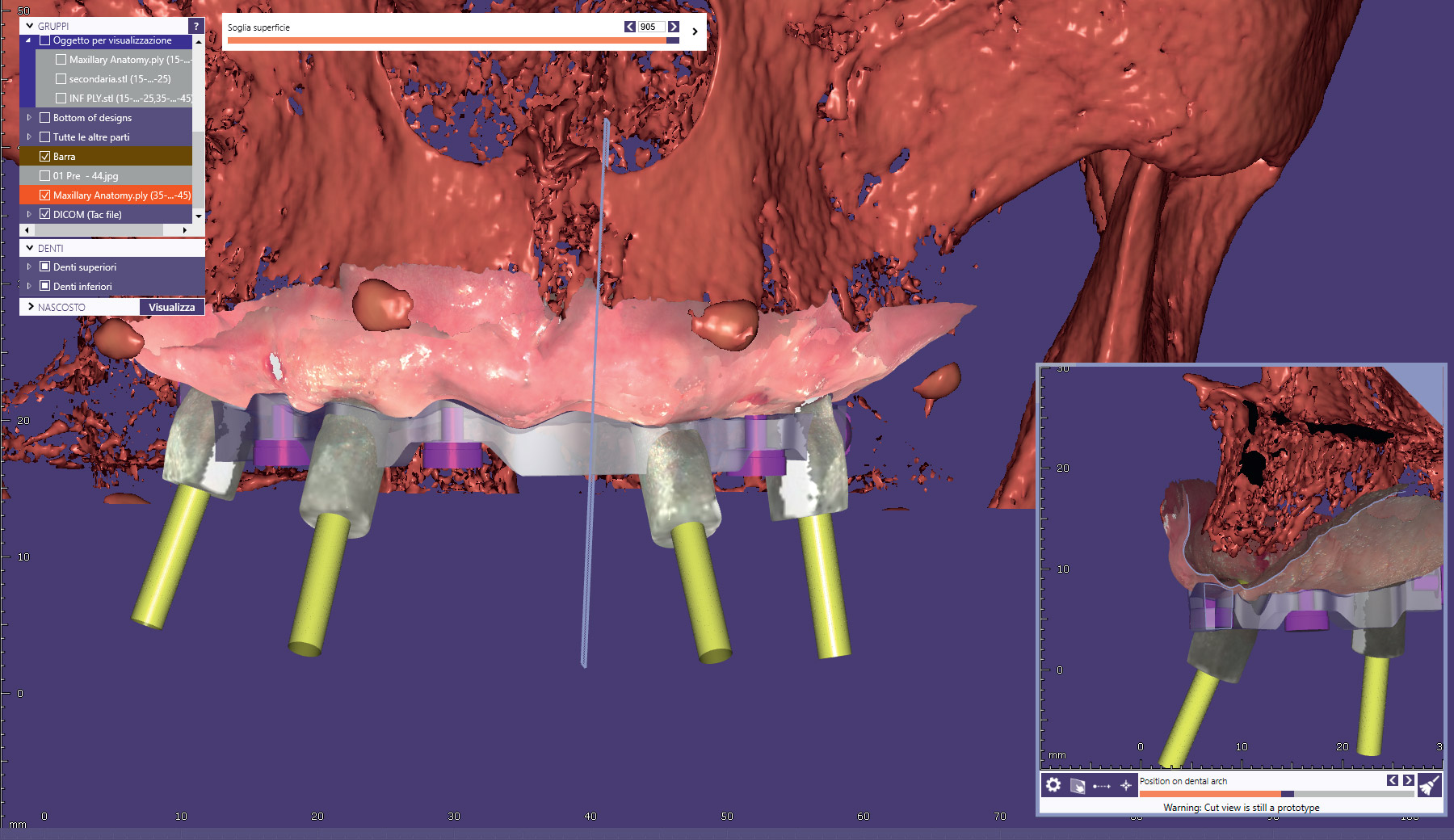
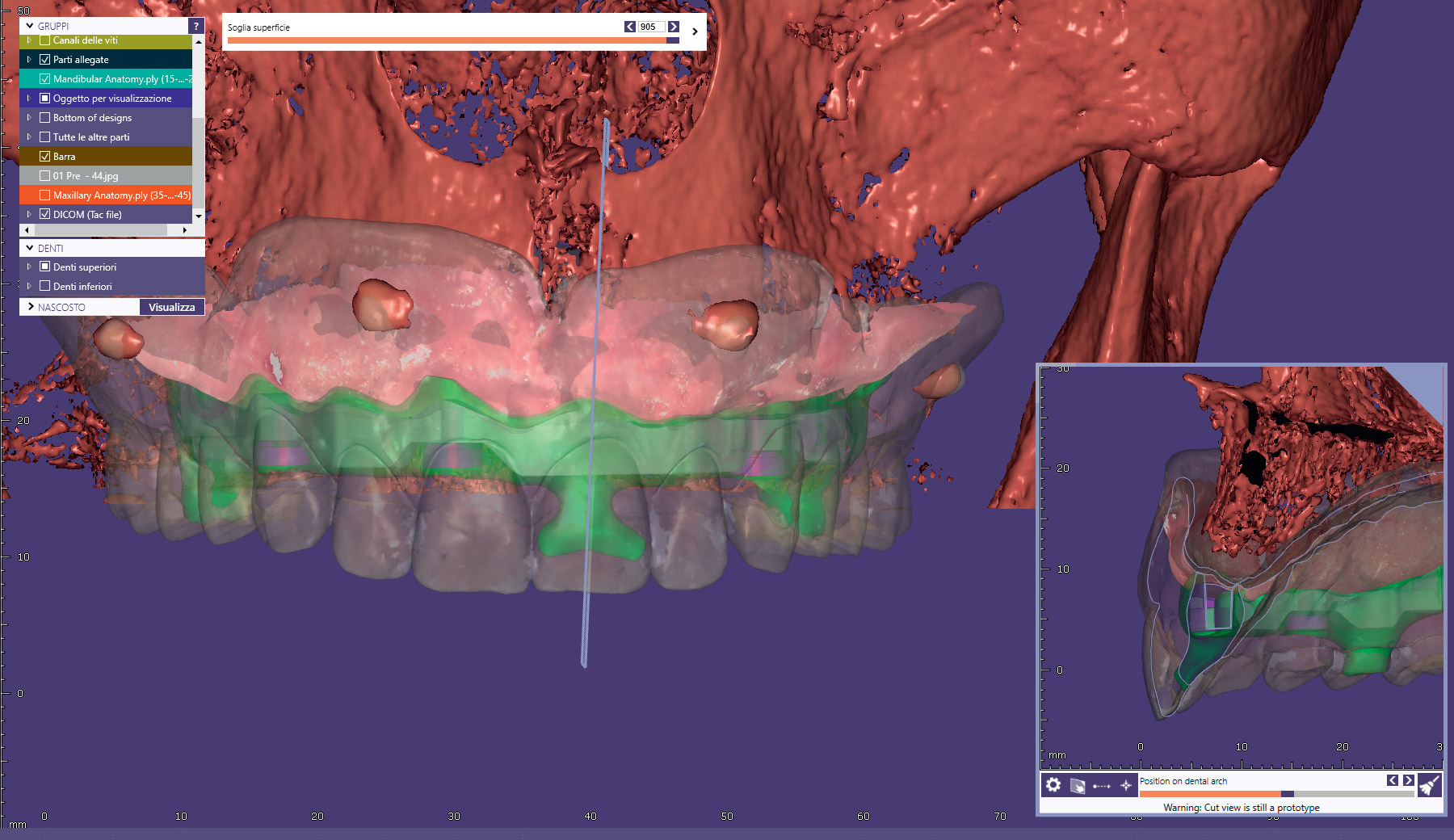
→ J Oral Science Rehabilitation. 2017 Mar;3(1):68–79. Preplanned multiunit abutments were immediately screwed on to the implants (New Ancorvis) and never removed. Immediately after implant placement, the patient received a digital impression (CS 3600 intraoral scanner, Carestream Dental), taken at abutment level, using dedicate scan abutments (Type AQ, New Ancorvis; Figs. 10a & b). In order to improve the accuracy of the digital impression in a fully edentulous patient, a second digital impression was taken using a dedicate opaque template, made by virtual planning, that was stabilized in the patient’s mouth using the same anchor pin positions of the surgical guide. This template was customized to maintain the tooth design, but allow the screwing of the scan abutments (Type AQ; Fig. 11) so that the new STL file could be superimposed with the previous planning (Fig. 12). Finally, the multiunit abutments were covered with dedicate caps, and the existing removable complete denture was relined at chairside with a autopolymerizing resin (Hydro-Cast, Sultan Healthcare, York, Pa., U.S.), thereby ensuring no pressure on the healing abutments. After implant placement, the patient received oral and written recommendations about medication, oral hygiene maintenance and diet.
-

- Fig. 9

-
- Fig. 10a
-

- Fig. 10b
-

- Fig. 11

-
- Fig. 12

A CAD/CAM titanium bar was anatomically designed by an experienced dental technician and CAD designer (MA) according to the implant position and the shape and volume of the existing removable complete dental prosthesis (exocad DentalCAD, Engine Build 6136, exocad, Darmstadt, Germany; Fig. 13).18Tallarico M, Xhanari E, Kadiu B, Scrascia R. Implant rehabilitation of extremely atrophic mandibles (Cawood and Howell Class VI) with a fixed-removable solution supported by four implants: one-year results from a preliminary prospective case series study.
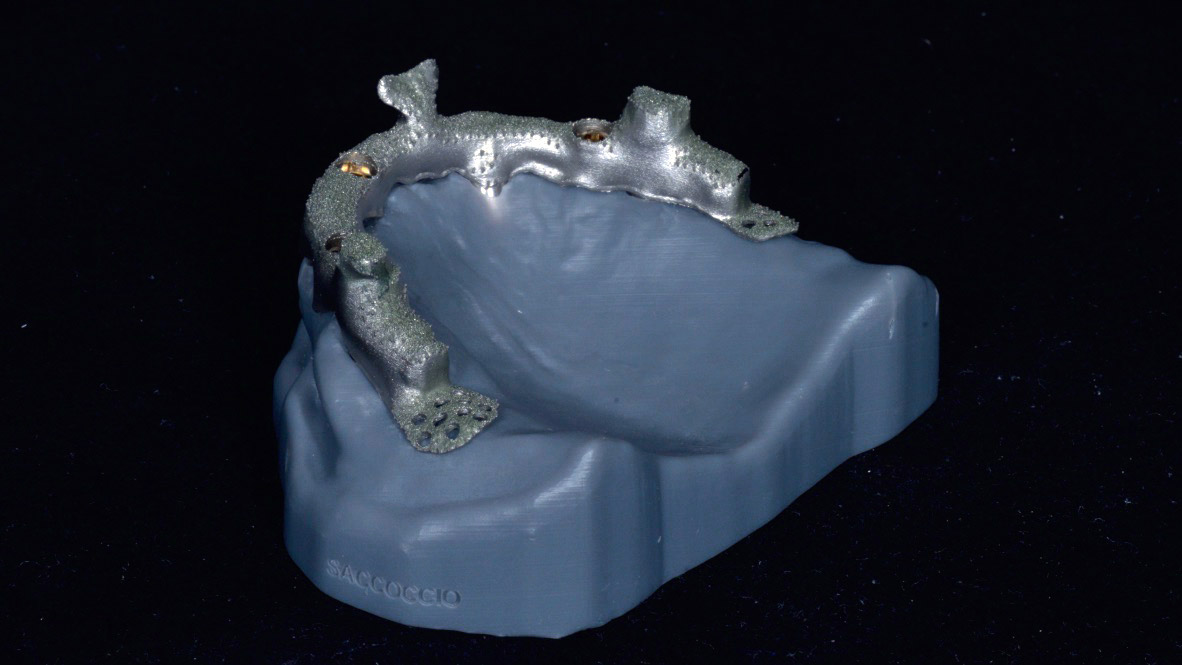
→ J Oral Science Rehabilitation.2017 Jun;3(1):32–40. Three threadable low-profile attachments (OT Equator, Rhein’83, Bologna, Italy) and two spheres (Rhein’83) were planned along the implant bar (Fig. 14). A cobalt–chromium alloy framework was then directly designed on to the CAD/CAM titanium bar project (Fig. 15) according to the existing tooth setup (exocad Partial Framework CAD, Version 0.x, exocad). The designs of the virtual bar and the superstructure framework were transmitted to the production center (New Ancorvis), where a one-piece titanium bar was milled from a homogenous solid block of medical titanium alloy (Ti6Al4V), while the cobalt– chromium, friction fit superstructure framework was laser melted (Fig. 16).
-
- Fig. 13
-

- Fig. 14

-
- Fig. 15
-

- Fig. 16
Third clinical appointment
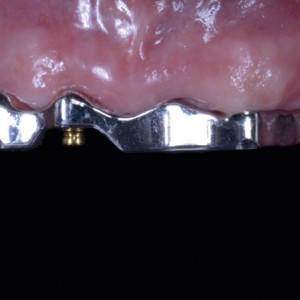
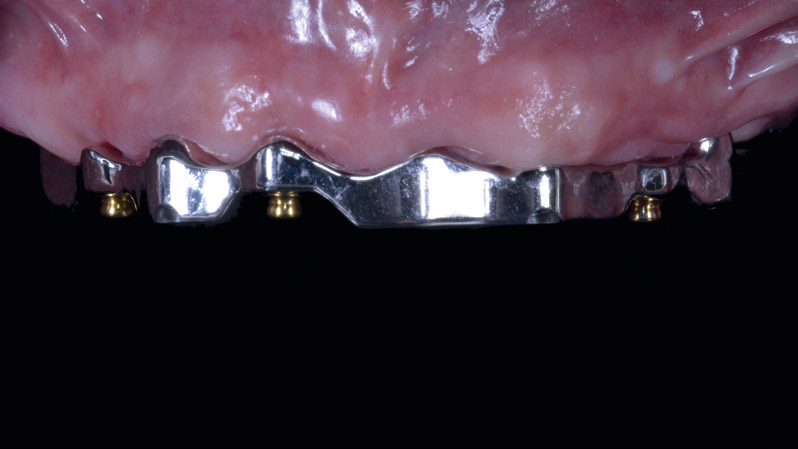
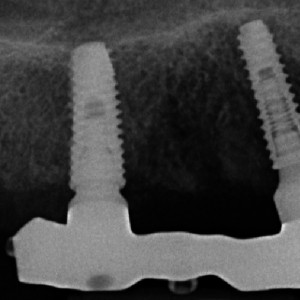
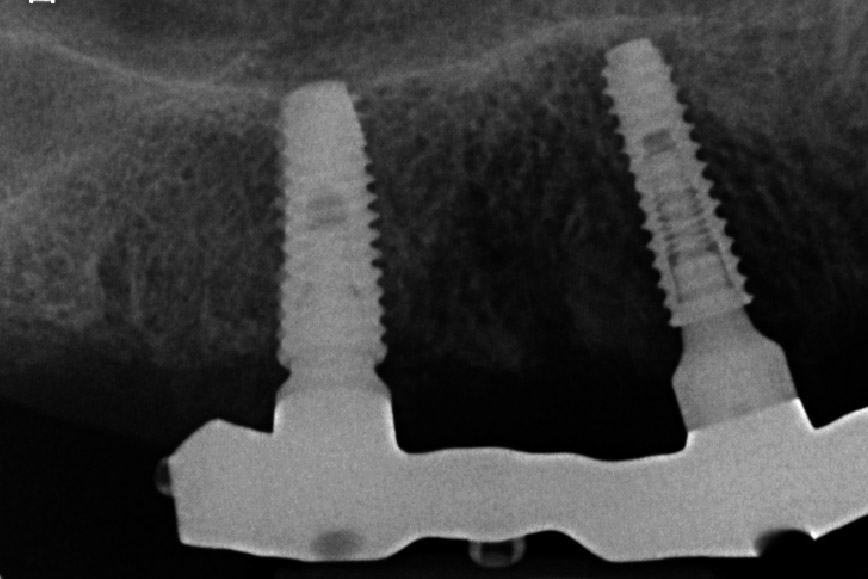
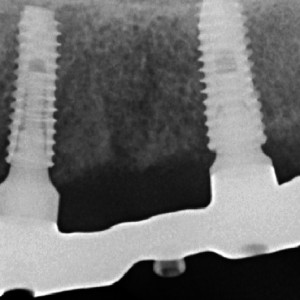
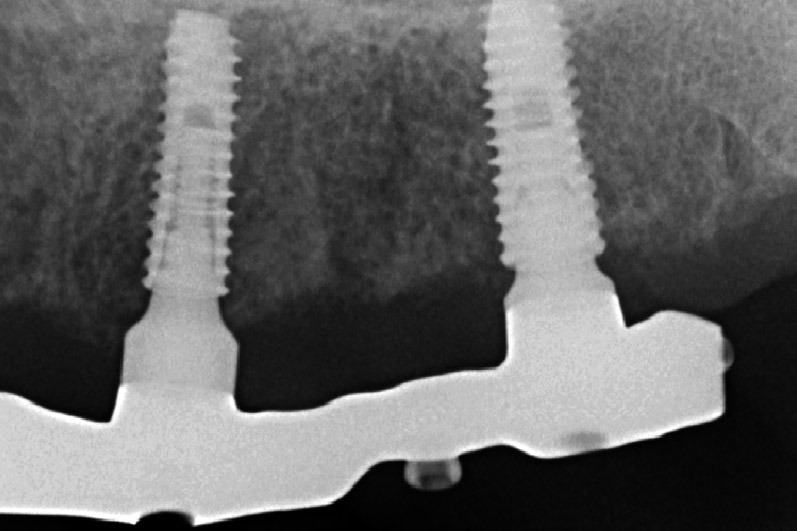
The fit of the implant bar and the superstructure framework was clinically and radiographically tested in the patient’s mouth according to established criteria (Figs. 17 & 18).19Abduo J, Bennani V, Waddell N, Lyons K, Swain M. Assessing the fit of implant fixed prostheses: a critical review.
→ Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):506–15.20Eisenmann E, Mokabberi A, Walter MH, Freesmeyer WB. Improving the fit of implant-supported superstructures using the spark erosion technique.
→ Int J Oral Maxillofac Implants. 2004 Nov-Dec;19(6):810–8. An interocclusal record was taken in centric relation, and master models, fabricated using rapid prototyping techniques, with specially designed implant replicas, were mounted in a fully adjustable articulator (PROTARevo 7, KaVo Dental, Biberach, Germany; Fig. 19). Digital analysis of movement was performed using the ARCUSdigma device (KaVo Dental) to ascertain and document all the settings required for programming the articulator (e.g., condylar inclination, Bennett angle, immediate side shift and shift angle). Finally, the overdenture was finished using a silicone index derived from the existing removable complete dental prosthesis as tooth reference, and the borders sealed to minimize food impaction, and saliva or air leakage.
-
- Fig. 17
-
- Fig. 18a
-
- Fig. 18b
-

- Fig. 19

-

- Fig. 20

-

- Fig. 21

Fourth clinical appointment
The titanium bar was screwed at the abutment level according to the manufacturer’s instructions and the implant overdenture was delivered 6 weeks after the first visit (Figs. 20 & 21). The patient was enrolled in a standard implant recall program. Oral hygiene maintenance was checked and radiographs were taken early after final prosthesis delivery. Occlusion was checked at every appointment.
Interview
with Tallarico Marco
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Tallarico M, Meloni SM, Canullo L, Xhanari E, Polizzi G. Guided surgery for single-implant placement: a critical review. → J Oral Science Rehabilitation. 2016 Dec;2(4):8–14. |
| 2. | ↑ | Polizzi G, Cantoni T, Pasini E, Tallarico M. Immediate loading of variable-thread expanding tapered-body implants placed into maxillary post-extraction or healed sites using a guided surgery approach: an up-to-five year retrospective analysis. → J Oral Science Rehabilitation. 2016 Sep;2(3):50–60. |
| 3. | ↑ | Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. Five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery. → Clin Implant Dent Relat Res. 2016 Oct;18(5):965–72. |
| 4. | ↑ | Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial. → Eur J Oral Implantol. 2014 Autumn;7(3):229–42. |
| 5. | ↑ | Vermeulen J. The accuracy of implant placement by experienced surgeons: guided vs freehand approach in a simulated plastic model. → Int J Oral Maxillofac Implants. 2017 Mar-Apr;32(3):617–24. |
| 6, 16. | ↑ | Van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, Wendelhag I. Computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicentre study. → Clin Implant Dent Relat Res. 2005;7 Suppl 1:S111–20. |
| 7. | ↑ | Jemt T, Hjalmarsson L. In vitro measurements of precision of fit of implant-supported frameworks: a comparison between “virtual” and “physical” assessments of fit using two different techniques of measurements. → Clin Implant Dent Relat Res. 2012 May;14 Suppl 1:e175–82. |
| 8, 9, 11. | ↑ | Pozzi A, Tallarico M, Mangani F, Barlattani A. Different implant impression techniques for edentulous patients treated with CAD/ CAM complete-arch prostheses: a randomised controlled trial reporting data at 3 year post-loading. → Eur J Oral Implantol. 2013 Winter;6(4):325–40. |
| 10. | ↑ | Papaspyridakos P, Chen CJ, Gallucci GO, Doukoudakis A, Weber HP, Chronopoulos V. Accuracy of implant impressions for partially and completely edentulous patients: a systematic review. → Int J Oral Maxillofac Implants. 2014 Jul-Aug;29(4):836–45. |
| 12. | ↑ | Amin S, Weber HP, Finkelman M, El Rafie K, Kudara Y, Papaspyridakos P. Digital vs. conventional full-arch implant impressions: a comparative study. → Clin Oral Implants Res. 2016 Dec 31. doi:10.1111/clr.12994. [Epub ahead of print]. |
| 13. | ↑ | Kattadiyil MT, Mursic Z, AlRumaih H, Goodacre CJ. Intraoral scanning of hard and soft tissues for partial removable dental prosthesis fabrication. → J Prosthet Dent. 2014 Sep;112(3):444–8. |
| 14. | ↑ | Wu J, Li Y, Zhang Y. Use of intraoral scanning and 3-dimensional printing in the fabrication of a removable partial denture for a patient with limited mouth opening. → J Am Dent Assoc. 2017 May;148(5):338–41. |
| 15. | ↑ | Fang JH, An X, Jeong SM, Choi BH. Development of complete dentures based on digital intraoral impressions—case report. → J Prosthodont Res. 2017 Jun 15. pii: S1883-1958(17)30049-X. doi:10.1016/j.jpor.2017.05.005. [Epub ahead of print]. |
| 17. | ↑ | Tallarico M, Meloni SM. Open-cohort prospective study on early implant failure and physiological marginal remodeling expected using sandblasted and acid-etched bone level implants featuring an 11° Morse taper connection within one year after loading. → J Oral Science Rehabilitation. 2017 Mar;3(1):68–79. |
| 18. | ↑ | Tallarico M, Xhanari E, Kadiu B, Scrascia R. Implant rehabilitation of extremely atrophic mandibles (Cawood and Howell Class VI) with a fixed-removable solution supported by four implants: one-year results from a preliminary prospective case series study. → J Oral Science Rehabilitation.2017 Jun;3(1):32–40. |
| 19. | ↑ | Abduo J, Bennani V, Waddell N, Lyons K, Swain M. Assessing the fit of implant fixed prostheses: a critical review. → Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):506–15. |
| 20. | ↑ | Eisenmann E, Mokabberi A, Walter MH, Freesmeyer WB. Improving the fit of implant-supported superstructures using the spark erosion technique. → Int J Oral Maxillofac Implants. 2004 Nov-Dec;19(6):810–8. |





Leave a Reply
Be the First to Comment!