Influence of the position of implants placed immediately into extraction sockets: An experimental study in dogs
March 11, 2016 / Categories: Digital Dentistry, Implant Dentistry

De Santis, Enzo
Salata, Luiz A.
Pereira, Flávia Priscila
Ferraris, Sara
Pantani, Fabio
Favero, Giacomo

Botticelli, Daniele
The objective of this study was to evaluate the influence of implant positioning within an extraction socket on the depth of the implant at the time of surgery and on the buccal supracrestal exposure of the implant surface after healing.
Introduction
After tooth extraction, the immediate placement of an implant into an alveolus is considered a predictable procedure, even though a higher loss of implants has been reported.1Chrcanovic BR, Albrektsson T, Wennerberg A. Dental implants inserted in fresh extraction sockets versus healed sites: a systematic review and meta-analysis. → J Dent. 2015 Jan;43(1):16–41.
Moreover, it has been shown that an implant placed into an extraction socket will not avoid bone resorption at the coronal aspect of the walls of the alveolus.2Botticelli D, Berglundh T, Lindhe J. Hardtissue alterations following immediate implant placement in extraction sites. → J Clin Periodontol. 2004 Oct;31(10):820–8.3Araújo MG, Sukekava F, Wennström JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. → J Clin Periodontol. 2005 Jun;32(6):645–52.
One of the most important aspects to be considered is the position of the implant within the extraction socket in relation to the buccolingual walls of the alveolus. It has been shown that a buccal placement will produce, after healing, higher supracrestal exposure of the implant at the buccal aspect compared with a lingual positioning. 4Caneva M, Salata LA, de Souza SS, Baffone G, Lang NP, Botticelli D. Influence of implant positioning in extraction sockets on osseointegration: histomorphometric analyses in dogs. → Clin Oral Implants Res. 2010 Jan;21(1):43–9.5Tomasi C, Sanz M, Cecchinato D, Pjetursson B, Ferrus J, Lang NP, Lindhe J. Bone dimensional variations at implants placed in fresh extraction sockets: a multilevel multivariate analysis. → Clin Oral Implants Res. 2010 Jan;21(1):30–6.6Favero G, Lang NP, Favero G, León IG, Salata LA, Botticelli D. Role of teeth adjacent to implants installed immediately into extraction sockets: an experimental study in the dog. → Clin Oral Implants Res. 2012 Apr;23(4):402–8.7Favero G, Botticelli D, Rea M, Pantani F, León IG, Lang NP. Influence of presence or absence of teeth adjacent to implants installed immediately into extraction sockets on peri-implant hard tissue levels: an experimental study in the dog. → Clin Oral Implants Res. 2013 Mar;24(3):262–9. This may be explained by the higher resorption of the buccal bone plates compared with the lingual bone plates during healing after tooth extraction so that a slope will be formed, being higher at the lingual aspect compared with the buccal aspect.8 This, in turn, means that the closer the implant is to the lingual aspect and the farther from the buccal aspect, the lesser the exposure of the implant body above the bony crest will be.
Owing to anatomical, functional and esthetic reasons, in a clinical situation, the axis of an implant placed into an extraction socket will be more lingually located compared with the tooth axis. This is explained by the presence of residual defects between the implant body and the walls of the extraction socket that will be larger and more likely to occur at the buccal aspect compared with the lingual aspect.8Botticelli D, Berglundh T, Lindhe J. Hard- tissue alterations following immediate implant placement in extraction sites. → J Clin Periodontol. 2004 Oct;31(10):820–8. When an implant is placed into an extraction socket, the recipient site will generally be prepared with a lingual bodily displacement, maintaining more or less the same axis of the alveolus. However, it has been suggested that, owing to the different projection, if the axis of the implant is tilted in a lingual direction, the implant will be located deeper within the extraction socket than it would have been had the same axis as that of the alveolus been maintained,9Favero G, Botticelli D, Favero G, García B, Mainetti T, Lang NP. Alveolar bony crest preservation at implants installed immediately after tooth extraction: an experimental study in the dog. → Clin Oral Implants Res. 2013 Jan;24(1):7–12. even though the margin will be located at the same level as the buccal bone crest.
The concept of implant positioning needs to be further clarified. Hence, the aim of the present experiment is to evaluate the influence of implant positioning within an extraction socket on the depth of the implant at the time of surgery and on the buccal supracrestal exposure of the implant surface after healing.
Materials & methods
The research protocol was submitted to and approved by the ethics committee for animal research at the Universidad Estadual Paulista (Araçatuba, Brazil). Eight Labrador dogs were included in the study. The animals had a mean weight of approximately 30 kg and a mean age of 2 years and were housed in kennels on concrete runs at the university’s field laboratory with free access to water and moistened balanced dog food.
Clinical procedures
At each surgery, the animals were first pre-anesthetized with Acepran (0.05 mg/kg; Univet- Vetnil, São Paulo, Brazil) and then anesthetized with Zoletil (10 mg/kg; Virbac, São Paulo, Brazil) and Xilazina (1 mg/kg; Cristália, São Paulo, Brazil), supplemented with ketamine (1⁄4 of the dose of 10 mg/kg; Cristália, São Paulo, Brazil). Before the surgical procedure, the pulp of the mesial roots of the fourth mandibular premolars was removed on both sides of the mandible, and the root canals were filled with gutta-percha and root canal cement (Mtwo, Endopocket, Epfill, Sweden & Martina). The crowns were afterward restored with composite (Adonis, Sweden & Martina).
The surgical procedure began with an incision performed within the sulcus. The flaps were elevated and the buccal and lingual alveolar bone plates were exposed. The fourth premolars were first hemisectioned and the distal roots removed, together with the corresponding portion of the crowns. The distal alveoli were subsequently prepared at the apex for implant placement. However, randomly, the drill was tilted buccally at one site and lingually at the other. Implants 11.5 mm in length and 3.5 mm in diameter (Alvim CM, Neodent, Curitiba, Brazil) and with a rough surface (sand-blasted and acid etched) were placed with the shoulder flush with the buccal bone (Figs. 1a & b). At one site, the implant was placed in a buccal position (B-sites), in contact with the buccal wall of the alveolus, while in the opposite jaw, the implant was placed lingually (L-sites), in contact with the lingual wall of the alveolus (Figs. 2a & b).
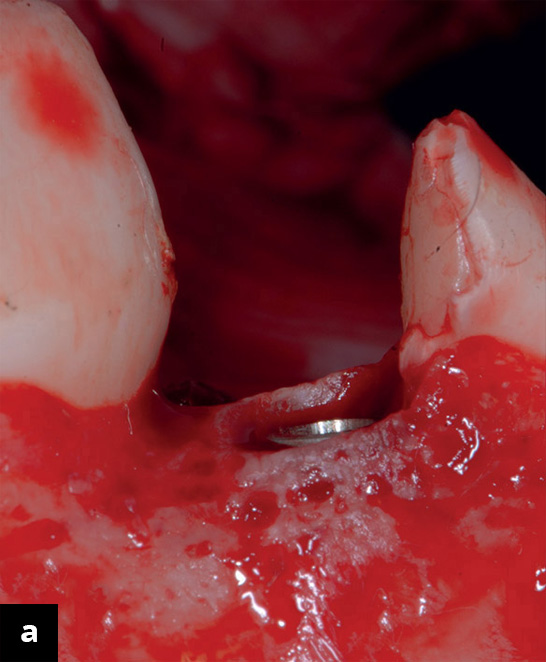
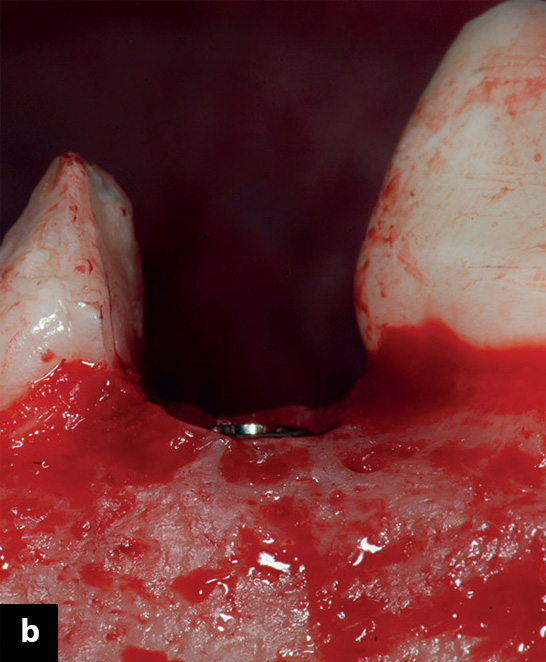
Clinical buccal view. Implants placed into the distal alveoli of the fourth premolars in a (a) lingual and (b) buccal position. Note that the implant in the lingual position was deeper in relation to the lingual bone crest compared with the implant placed buccally.
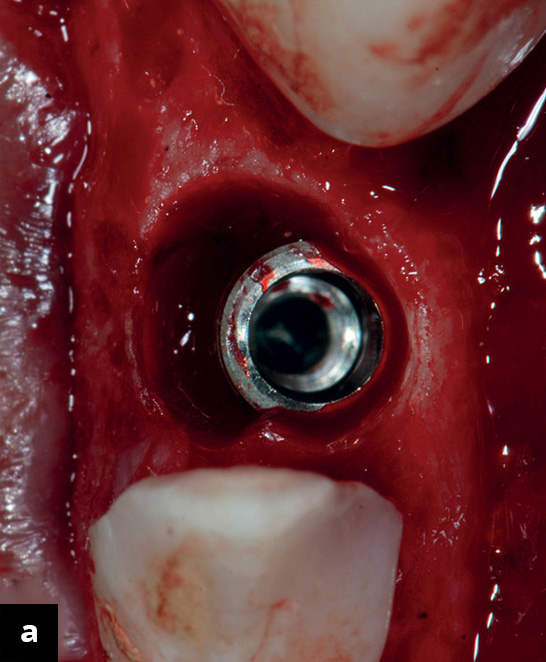
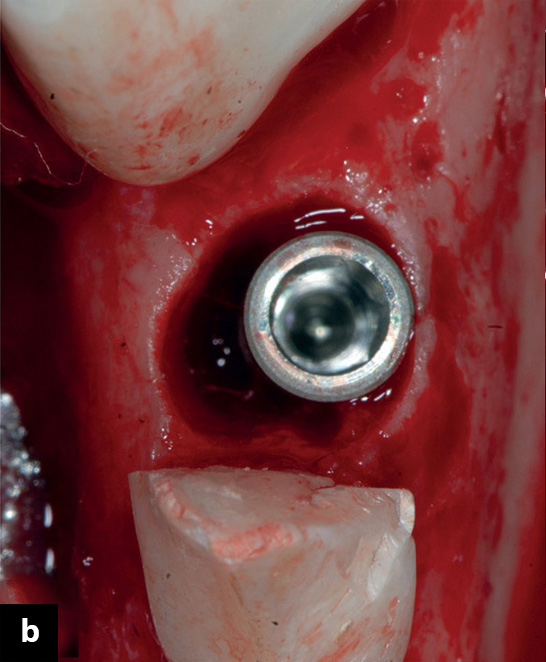
Figs 2 a & b:
Clinical occlusal view. Implants placed into the distal alveoli of the fourth premolars in a (a) lingual and (b) buccal position.
Using a #15 UNC probe (Hu-Friedy, Chicago, Ill., U.S.), the horizontal and vertical dimensions of the remaining buccal or lingual defects were measured, as well as the vertical distance between the top of the bony crest and the implant shoulder at the lingual aspect. Abutments of appropriate length were attached to the implants and sutures were applied to allow nonsubmerged healing.
After completion of the surgery, the animals were given a vitamin compound (Potenay, Fort Dodge Animal Health, Campinas, Brazil), an anti-inflammatory and analgesic drug (Banamine, Schering-Plough Animal Health, Campinas, Brazil) and an antibiotic (Penta-biótico, Fort Dodge Animal Health, Campinas, Brazil). Three times per week for the first two weeks after surgery, the wounds were inspected for clinical signs of complications and the implant abutments were cleaned and disinfected with chlorhexidine. Afterward, cleaning was performed three times per week. The animals were euthanatized four months after the surgery, with overdoses of thiopental (Cristália, Itapira, Brazil) and then perfused with a fixative (4% formaldehyde solution) through the carotid arteries.
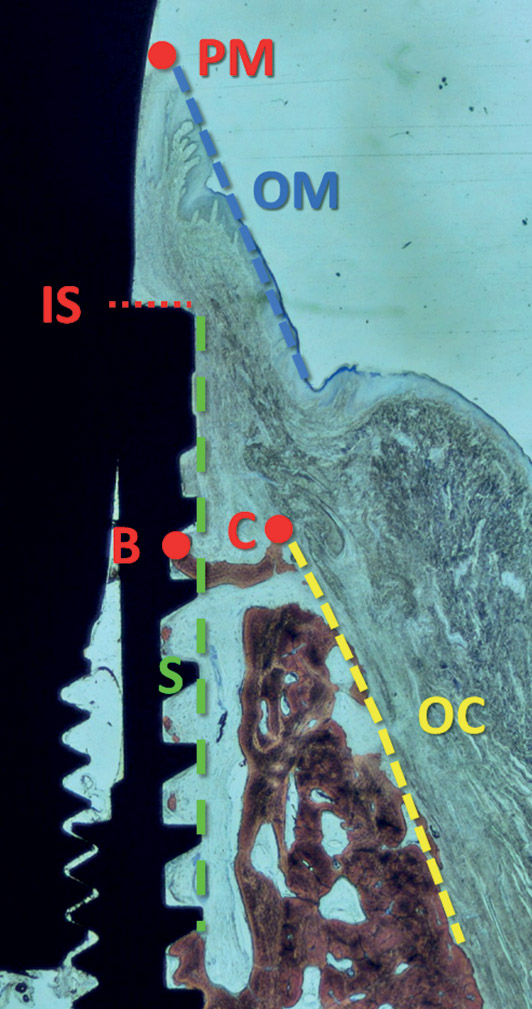
Fig 3. Landmarks used for histomorphometric analyses: IS: implant shoulder; C: top of the adjacent bony crest; B: most coronal point of contact between the bone and implant; PM: top of the mucosal margin; S (dashed green line): the surface of the implant at the top of the threads; OC (dashed yellow line): the outer contour of the bony crest; OM (dashed blue line): the outer contour of the periimplant mucosa.
Histological preparation
Individual blocks containing the implant and the surrounding hard and soft tissue were collected from the mandible and fixed in a 4% formaldehyde solution. The specimens were subsequently dehydrated in a series of graded ethanol solutions and finally embedded in resin (LR White, hard grade, London Resin, Reading, UK). The blocks were cut along the buccolingual plane using a diamond band saw fitted in a precision slicing machine (EXAKT 300, EXAKT Advanced Technologies, Norderstedt, Germany) and then reduced to a thickness of approximately 60 μm using a cutting and grinding device (EXAKT 400, EXAKT Advanced Technologies). The histological slides were stained with Stevenel’s blue and alizarin red and examined under a standard light microscope for histometric analysis.
Histological evaluation
Under an Eclipse Ci microscope (Nikon, Tokyo, Japan), connected to a computer through a video camera (Nikon Digital DS-Fi2, Nikon), the following landmarks were identified (Fig. 3): the implant shoulder (IS), the top of the adjacent bony crest (C), the most coronal point of contact between the bone and implant (B), the top of the mucosal margin (PM), the surface of the implant at the top of the threads (S), the outer contour of the bony crest (OC) and the outer contour of the periimplant mucosa (OM). The following measurements were performed using NIS-Elements software (Version 4.1; Nikon, Tokyo, Japan) under 40× magnification: the vertical distance between IS and C, IS and B, as well as PM and IS. PM–B was calculated from the data available.
Under 40× magnification, the width of the alveolar bony crest was measured from S to OC at the IS level (0 mm) and then apical to it at each subsequent millimeter, up to 5 mm (Fig. 3). The width of the periimplant mucosa was measured at the IS level (0 mm) and then up to 3 mm coronal to the abutment surface and up to 3 mm apical to it, from S. Under 100× magnification, the percentage of bone-to-implant contact (BIC%) was evaluated from the IS to the apical extension of the implant, both buccally and lingually.
Data Analysis
Mean values and standard deviations, as well as the 25th, 50th (median) and 75th percentiles, were calculated for each outcome variable. Differences between buccally (B-sites) and lingually (L-sites) positioned implants were analysed using the Wilcoxon signed-rank test for paired observations using IBM SPSS Statistics for Windows (Version 19.0; IBM Corp., Armonk, N.Y., U.S.). The vertical level of the bony crest and osseointegration (IS–C and IS–B) were the main outcome variables. The level of significance was set at α = 0.05.
Results
In one animal, a fracture of the buccal wall of the alveolus occurred during extraction and the animal was excluded entirely from analysis. No artifacts were generated during histological processing, nor were any tissue blocks destroyed. Hence, the B- and L-sites yielded n = 7. In the text, mean values ± standard deviations are reported, and in the tables, the medians and the 25th and 75th percentiles are included too.
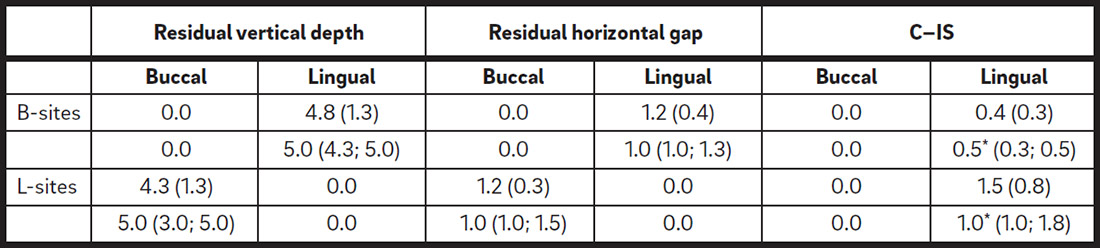
Clinical dimensions (mm) of the residual bone defects after implant placement (n = 7). Mean values (standard deviations) and medians (25th; 75th percentiles) are reported.
C: top of the adjacent bony crest; IS: implant shoulder. No statistically significant differences (p < 0.05) were found between the lingual defects at B-sites and the buccal defects at L-sites for vertical depth and horizontal gap. *p < 0.05 between B-sites and L-sites for C–IS at buccal and lingual aspects.

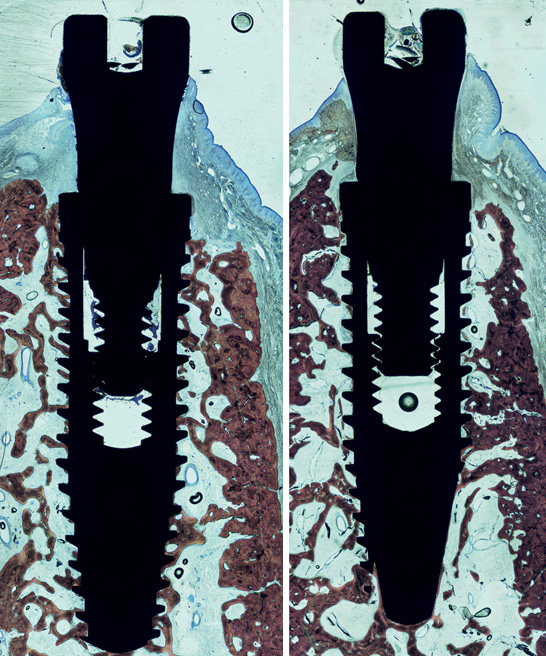
Figs. 4 & 5
Ground sections illustrating the histological healing after four months at the B-sites (20× magnification; Stevenel’s blue and alizarin red stain).
Fig. 5
Ground sections illustrating the histological healing after four months at the L-sites (20× magnification; Stevenel’s blue and alizarin red stain).
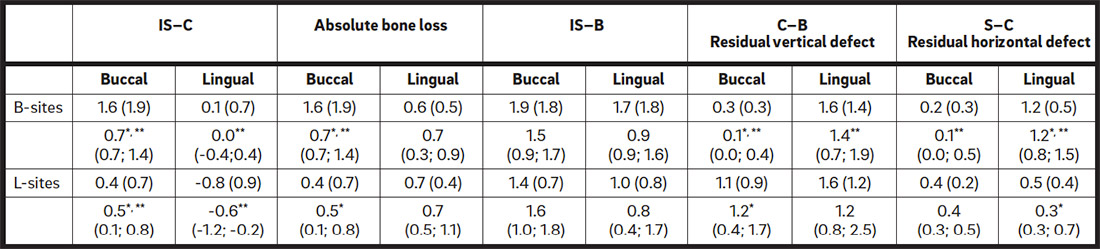
IS: implant shoulder; C: top of the adjacent bony crest; B: most coronal point of contact between the bone and implant; S: surface of the implant at the top of the threads. *p < 0.05 between B-sites and L-sites. **p < 0.05 between buccal and lingual aspects.
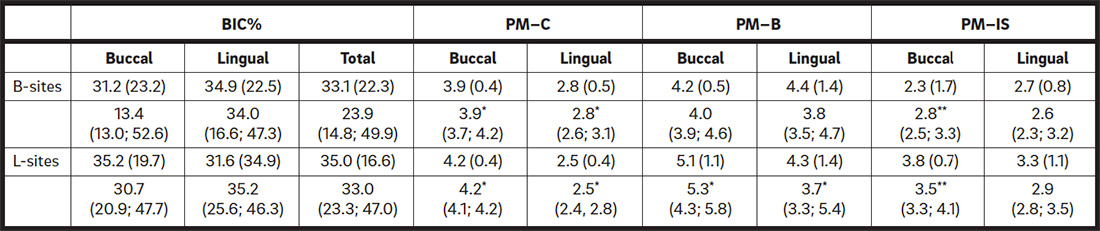
PM: top of the mucosal margin; C: top of the adjacent bony crest; B: most coronal point of contact between the bone and implant; IS: implant shoulder. *p < 0.05 between buccal and lingual aspects. **p < 0.05 between B-sites and L-sites.
Clinical evaluation (Table1)
Table 2. Histological hard-tissue dimensions (mm; n = 7). Mean values (standard deviations) and medians (25th; 75th percentiles) are reported.
Table 3. Histological soft-tissue dimensions (mm) and BIC% (n = 7). Mean values (standard deviation) and medians (25th; 75th percentiles) are reported.
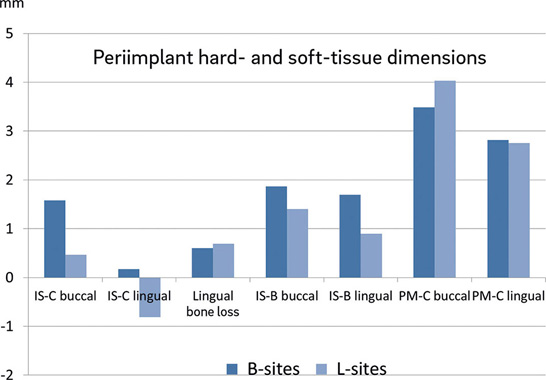
Fig. 6. Graphic showing the mean values of the dimensions of the periimplant hard and soft tissue. IS: implant shoulder; C: top of the adjacent bony crest; B: most coronal point of contact between the bone and implant; PM: top of the mucosal margin.
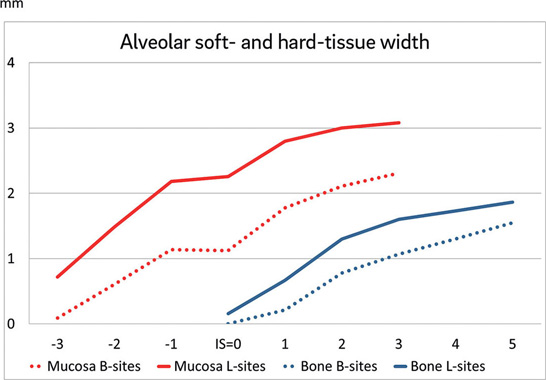
Fig. 7. Graphic showing the mean values of the alveolar soft- and hard-tissue width at the buccal aspect after four months of healing. The continuous lines represent the width of the tissue at the L-sites, and the dotted lines represent the width at the B-sites. Red and blue lines represent the mucosal and bone widths, respectively. IS: implant shoulder.
After implant placement, residual marginal bone defects were observed that were 4.8 ± 1.3 mm deep and 1.2 ± 0.4 mm wide at the lingual aspect of the B-sites and 4.3 ± 1.3 mm deep and 1.2 ± 0.3 mm wide at the buccal aspect of the L-sites. The distance between the lingual bone crest and the implant shoulder was 0.4 ± 0.3 mm at the B-sites and 1.5 ± 0.8 mm at the L-sites, the difference being statistically significant (p = 0.017). This indicates that, despite the implant margin being placed flush with the buccal bone crest at both the B- and L-sites, the implant was approximately 1.1 mm deeper with respect to the lingual bony crest when positioned lingually within the extraction socket compared with buccal positioning.
Histological evaluation
Ground sections showing examples of healing at the B-sites are illustrated in Figure 4 and of healing at the L-sites in Figure 5.
Hard-tissue dimensions (Table 2; Fig. 6)
IS–C at the buccal aspect was 1.6 ± 1.9 mm at the B-sites and 0.4 ± 0.7 mm at the L-sites. The difference was statistically significant. At the lingual aspect, IS–C was 0.1 ± 0.7 mm and -0.8 ± 0.9 mm at the B-and L-sites, respectively. When the absolute instead of the relative values were taken into account, the bone crest resorption at the lingual aspect was 0.6 ± 0.5 mm at the B-sites and 0.7 ± 0.4 mm at the L-sites. None of the differences between the B-sites and L-sites for relative and absolute values at the lingual aspect were statistically significant.
IS–B at the buccal aspect was 1.9 ± 1.8 mm at the B-sites and 1.4 ± 0.7 mm at the L-sites. At the lingual aspect, it was 1.7 ± 1.8 mm and 1.0 ± 0.8 mm at the B- and L-sites, respectively. None of the differences were statistically significant. At the B-sites, after healing, marginal bone defects were noted. The dimensions of the defects were smaller at the buccal (0.3 mm high and 0.2 mm wide) compared with the lingual (1.6 mm high and 1.2mm wide) aspects. When the implants were placed lingually (L-sites), vertical bone defects were found both at the buccal (1.1 ± 0.9 mm) and at the lingual (1.6 ± 1.2 mm) aspects. It has to be considered, however, that the coronal aspect of the defect was included in the abutment region given that IS was located apical to C by approximately 0.8 mm. These defects were narrow (≤ 0.5 mm). BIC% was similar at both sites, as well as buccolingually, and ranged between 31.2% and 35.2% (Table 3).
The width of the buccal bone ridge (OC–S) was larger at the L-sites compared with the B-sites. However, the difference was statistically significant only at the 1 mm level (Fig. 7).
Soft-tissue dimensions (Table 3; Fig. 6)
PM–C and PM–B at the buccal aspect were 3.9 ± 0.4mm and 4.2 ± 0.5 mm at the B-sites and 4.2 ± 0.4 mm and 5.1 ± 1.1 mm at the L-sites. None of the differences were statistically significant.The periimplant mucosa was located more coronally at the L-sites (3.8 ± 0.7 mm) compared with the B-sites (2.3 ± 1.7 mm), the difference being statistically significant. The width of the periimplant mucosa was greater at the L-sites compared with the B-sites. The differences were statistically significant at all levels considered (Fig. 7).
Discussion
The first aim of the present study was to evaluate the influence of implant positioning within an extraction socket on the depth of the implant. The apex of the alveolus was used as apical point for preparation and the drills were tilted toward either the buccal or the lingual aspects. No bodily displacements were applied. The implants were, consequently, placed in contact with the buccal or the lingual walls of the extraction sockets. Clinically, the lingual positioning of the implant is mainly achieved by a bodily displacement. However, a slight angulation of the implant may be applied toward the lingual bone wall when necessary for anatomical or prosthetic reasons. In the present experiment, the final position was obtained by changing the angulation in relation to the axis of the extraction socket. The procedure applied in the present experiment exaggerated the difference in angulations of the implants between the two groups, B- and L-sites, allowing the limits to be tested. It was shown that placing the implant lingually resulted in the implant shoulder being deeper with respect to the lingual bone crest compared with a buccal position, even though the implant margin was placed at the same level as the buccal bone crest. This was due to the rotation of the projection that occurred when the surgeon placed the implant flush with the buccal wall of the extraction socket, as described previously in another experiment in dogs.10Favero G, Botticelli D, Favero G, García B, Mainetti T, Lang NP. Alveolar bony crest preservation at implants installed immediately after tooth extraction: an experimental study in the dog. → Clin Oral Implants Res. 2013 Jan;24(1):7–12. From a clinical perspective, if a lingual tilting of the implant is included in the procedure, a deeper positioning of the implant can be expected compared with an implant placed following the axis of the alveolus or in a buccal position. This should be taken into account if the buccal bone crest of the alveolus is used as the reference level to judge the depth of the recipient implant site.
In the present experiment, the placement of an implant in a lingual position resulted in reduced supracrestal exposure of the implant compared with a buccal positioning. This is in complete agreement with other studies that showed similar results.11Caneva M, Salata LA, de Souza SS, Baffone G, Lang NP, Botticelli D. Influence of implant positioning in extraction sockets on osseointegration: histomorphometric analyses in dogs. → Clin Oral Implants Res. 2010 Jan;21(1):43–9.12Tomasi C, Sanz M, Cecchinato D, Pjetursson B, Ferrus J, Lang NP, Lindhe J. Bone dimensional variations at implants placed in fresh extraction sockets: a multilevel multivariate analysis. → Clin Oral Implants Res. 2010 Jan;21(1):30–6.13Favero G, Lang NP, Favero G, León IG, Salata LA, Botticelli D. Role of teeth adjacent to implants installed immediately into extraction sockets: an experimental study in the dog. → Clin Oral Implants Res. 2012 Apr;23(4):402–8.14Favero G, Botticelli D, Rea M, Pantani F, León IG, Lang NP. Influence of presence or absence of teeth adjacent to implants installed immediately into extraction sockets on peri-implant hard tissue levels: an experimental study in the dog. → Clin Oral Implants Res. 2013 Mar;24(3):262–9. In an experiment in dogs,15Caneva M, Salata LA, de Souza SS, Baffone G, Lang NP, Botticelli D. Influence of implant positioning in extraction sockets on osseointegration: histomorphometric analyses in dogs. → Clin Oral Implants Res. 2010 Jan;21(1):43–9. implants placed immediately into extraction sockets were placed in the center of the alveoli at the control sites, and placed lingually and 0.8 mm deeper at the test sites. The supracrestal exposure of the implants was higher at the centrally compared with the lingually positioned implants. In another experiment in dogs,16Favero G, Lang NP, Favero G, León IG, Salata LA, Botticelli D. Role of teeth adjacent to implants installed immediately into extraction sockets: an experimental study in the dog. → Clin Oral Implants Res. 2012 Apr;23(4):402–8.’ 17Favero G, Botticelli D, Rea M, Pantani F, León IG, Lang NP. Influence of presence or absence of teeth adjacent to implants installed immediately into extraction sockets on peri-implant hard tissue levels: an experimental study in the dog. → Clin Oral Implants Res. 2013 Mar;24(3):262–9. the implants were placed in a central position of the extraction sockets of third premolars and lingually in the alveoli of fourth premolars. After three months of healing, higher supracrestal exposure was found at the implants placed in the center of the alveoli. These results were also validated by a multivariate multilevel analysis on implants placed into sockets immediately after tooth extraction.18Tomasi C, Sanz M, Cecchinato D, Pjetursson B, Ferrus J, Lang NP, Lindhe J. Bone dimensional variations at implants placed in fresh extraction sockets: a multilevel multivariate analysis. → Clin Oral Implants Res. 2010 Jan;21(1):30–6. The reason for this outcome may be explained by the fact that the buccal wall of the extraction socket undergoes higher resorption than the lingual wall does.19Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. → J Clin Periodontol. 2005 Feb;32(2):212–8.’ 20Pietrokovski J, Massler M. Alveolar ridge resorption following tooth extraction. → J Prosthet Dent. 1967 Jan;17(1):21–7. The healing at an implant placed into an extraction socket immediately after tooth extraction will be affected by this resorption. The more buccal the implant placement, the greater the supracrestal exposure of the buccal surface of the implant will be. This assumption has been further corroborated by other experimental studies on implants placed immediately into extraction sockets.21Caneva M, Salata LA, de Souza SS, Bressan E, Botticelli D, Lang NP. Hard tissue formation adjacent to implants of various size and configuration immediately placed into extraction sockets: an experimental study in dogs. → Clin Oral Implants Res 2010 Sep;21(9):885–90.’ 22Caneva M, Botticelli D, Rossi F, Cardoso LC, Pantani F, Lang NP. Influence of implants with different sizes and configurations installed immediately into extraction sockets on peri-implant hard and soft tissues: an experimental study in dogs. → Clin Oral Implants Res. 2012 Apr;23(4):396–401. In these experiments in dogs, wide implants with the same coronal dimensions as the extraction sockets were placed on one side, and implants narrower than the extraction sockets were used on the other side. In the latter, a gap resulted between the buccal bone wall and the implant. Higher buccal bone resorption was observed at the wide compared with the narrow implants.
Factors such as the thickness of the buccal bone and the size of the horizontal defects present at the time of implant placement may influence ridge alterations.23Ferrus J, Cecchinato D, Pjetursson EB, Lang NP, Sanz M, Lindhe J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. → Clin Oral Implants Res. 2010 Jan;21(1):22–9. It was shown that buccal bone crests of ≤ 1 mm and residual buccal gaps of ≤ 1 mm presented higher vertical and horizontal resorption compared with buccal bone crests of > 1 mm and residual buccal gaps of > 1 mm.24Ferrus J, Cecchinato D, Pjetursson EB, Lang NP, Sanz M, Lindhe J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. → Clin Oral Implants Res. 2010 Jan;21(1):22–9. This may indicate that the distance between the outer contour of the bone crest at the buccal aspect and the surface of the implant plays the most important role. This, in turn, means that the closer the implant is placed into an extraction socket with respect to the outer contour of the bone crest, the greater the supracrestal exposure of the buccal surface of the implant will be.
After four months of healing, the top of the bone crest at the lingual aspect was located 0.1 mm below the implant shoulder at the B-sites and 0.8 mm above the implant shoulder at the L-sites. However, this does not mean that higher resorption occurred at the lingual crest at the B-sites compared with the L-sites. In fact, owing to the different angulation of the implants with respect to the axis of the alveolus, the implants at the L-sites were located deeper with respect to the lingual bone crest at the time of placement compared with the implants at the B-sites. When the original position of the implants was taken into account, similar absolute values of lingual bone crest resorption were found.
At the time of placement, defects were present opposite the implants. At the B-sites, lingual defects with mean values of 1.6 mm in depth and 1.2 mm in width were still present after four months of healing. At the L-sites, residual defects were also present at both the buccal (1.1 mm) and the lingual (1.6 mm) aspects. At the buccal aspect, the defects lay entirely between the implant surface and the bone wall, while at the lingual aspect, the residual defects were opposite the implant surface in the apical part and opposite the abutment in the coronal part. In a clinical situation, the implant is generally placed in a lingual position and residual defects may be present after healing. However, their presence may not be detected clinically if they are very narrow (≤ 0.5 mm). BIC% was similar at the buccal and lingual aspects, both at the B- and the L-sites, demonstrating that the position of the implants within the extraction sockets did not affect the degree of osseointegration. The lingual position affected the height of the periimplant mucosa, which was more coronal with respect to the implant shoulder at the L-sites compared with the B-sites.
Conclusion
In conclusion, at implants placed immediately into extraction sockets, smaller buccal exposure above the bone crest will occur when implants are placed in a lingual compared with a buccal position. Moreover, implants placed lingually will be located deeper within the extraction sockets compared with those placed buccally when the implants are tilted lingually or buccally, respectively, in relation to the axis of the alveolus.
Acknowledgements
This study was supported by a grant from the Ariminum Research and Dental Education Center, Ariminum Odontologica (Rimini, Italy). The implants were provided by Neodent (Curitiba, Brazil). The competent contributions of Mr. Sebastião Bianco, Ribeirão Preto, Brazil, in the histological processing are highly appreciated.
References
| 1. | ↑ | Chrcanovic BR, Albrektsson T, Wennerberg A. Dental implants inserted in fresh extraction sockets versus healed sites: a systematic review and meta-analysis. → J Dent. 2015 Jan;43(1):16–41. |
| 2. | ↑ | Botticelli D, Berglundh T, Lindhe J. Hardtissue alterations following immediate implant placement in extraction sites. → J Clin Periodontol. 2004 Oct;31(10):820–8. |
| 3. | ↑ | Araújo MG, Sukekava F, Wennström JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. → J Clin Periodontol. 2005 Jun;32(6):645–52. |
| 4, 11, 15. | ↑ | Caneva M, Salata LA, de Souza SS, Baffone G, Lang NP, Botticelli D. Influence of implant positioning in extraction sockets on osseointegration: histomorphometric analyses in dogs. → Clin Oral Implants Res. 2010 Jan;21(1):43–9. |
| 5, 12, 18. | ↑ | Tomasi C, Sanz M, Cecchinato D, Pjetursson B, Ferrus J, Lang NP, Lindhe J. Bone dimensional variations at implants placed in fresh extraction sockets: a multilevel multivariate analysis. → Clin Oral Implants Res. 2010 Jan;21(1):30–6. |
| 6, 13, 16. | ↑ | Favero G, Lang NP, Favero G, León IG, Salata LA, Botticelli D. Role of teeth adjacent to implants installed immediately into extraction sockets: an experimental study in the dog. → Clin Oral Implants Res. 2012 Apr;23(4):402–8. |
| 7, 14, 17. | ↑ | Favero G, Botticelli D, Rea M, Pantani F, León IG, Lang NP. Influence of presence or absence of teeth adjacent to implants installed immediately into extraction sockets on peri-implant hard tissue levels: an experimental study in the dog. → Clin Oral Implants Res. 2013 Mar;24(3):262–9. |
| 8. | ↑ | Botticelli D, Berglundh T, Lindhe J. Hard- tissue alterations following immediate implant placement in extraction sites. → J Clin Periodontol. 2004 Oct;31(10):820–8. |
| 9, 10. | ↑ | Favero G, Botticelli D, Favero G, García B, Mainetti T, Lang NP. Alveolar bony crest preservation at implants installed immediately after tooth extraction: an experimental study in the dog. → Clin Oral Implants Res. 2013 Jan;24(1):7–12. |
| 19. | ↑ | Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. → J Clin Periodontol. 2005 Feb;32(2):212–8. |
| 20. | ↑ | Pietrokovski J, Massler M. Alveolar ridge resorption following tooth extraction. → J Prosthet Dent. 1967 Jan;17(1):21–7. |
| 21. | ↑ | Caneva M, Salata LA, de Souza SS, Bressan E, Botticelli D, Lang NP. Hard tissue formation adjacent to implants of various size and configuration immediately placed into extraction sockets: an experimental study in dogs. → Clin Oral Implants Res 2010 Sep;21(9):885–90. |
| 22. | ↑ | Caneva M, Botticelli D, Rossi F, Cardoso LC, Pantani F, Lang NP. Influence of implants with different sizes and configurations installed immediately into extraction sockets on peri-implant hard and soft tissues: an experimental study in dogs. → Clin Oral Implants Res. 2012 Apr;23(4):396–401. |
| 23, 24. | ↑ | Ferrus J, Cecchinato D, Pjetursson EB, Lang NP, Sanz M, Lindhe J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. → Clin Oral Implants Res. 2010 Jan;21(1):22–9. |





Leave a Reply
Be the First to Comment!