Open-healing approach to avoid flap mobilization and subsequent morbidity
January 6, 2017 / Categories: Digital Dentistry, Implant Dentistry

Taffet, Georg
This retrospective analysis evaluated the outcome of bone regeneration using membranes in an open-healing approach.
Introduction
The aim of implant therapy is to ensure an optimal functional and esthetic outcome as well as good long-term results. The use of regenerative techniques is often necessary to maintain or augment sufficient bone and soft-tissue for implant placement.
Among the bone substitutes, a deproteinized bovine bone mineral (DBBM) has been shown to be effective in bone augmentation1Von Arx T, Buser D. Horizontal ridge augmentation using autogenous block grafts and the guided bone regeneration technique with collagen membranes: a clinical study with 42 patients.
→ Clin Oral Implants Res. 2006;17(4):359–66.2Jensen T, Schou S, Stavropoulos A, Terheyden H, Holmstrup P. Maxillary sinus floor augmentation with Bio-Oss or Bio-Oss mixed with autogenous bone as graft: a systematic review.
→ Clin Oral Implants Res. 2012;23(3):263–73.3Urban IA, Nagursky H, Lozada JL, Nagy K. Horizontal ridge augmentation with a collagen membrane and a combination of particulated autogenous bone and anorganic bovine bone-derived mineral: a prospective case series in 25 patients.
→ Int J Periodontics Restorative Dent. 2013;33(3):299–307.4Chen ST, Darby IB, Reynolds EC. A prospective clinical study of non-submerged immediate implants: clinical outcomes and esthetic results.
→ Clin Oral Implants Res. 2007;18(5):552–62. and ridge preservation procedures.5Ackermann KL. Extraction site management using a natural bone mineral containing collagen: rationale and retrospective case study.
→ Int J Periodontics Restorative Dent. 2009;29(5):489–97.6Nevins M, Camelo M, De Paoli S, Friedland B, Schenk RK, Parma-Benfenati S, Simion M, Tinti C, Wagenberg B. A study of the fate of the buccal wall of extraction sockets of teeth with prominent roots.
→ Int J Periodontics Restorative Dent. 2006;26(1):19–29.7Perelman-Karmon M, Kozlovsky A, Liloy R, Artzi Z. Socket site preservation using bovine bone mineral with and without a bioresorbable collagen membrane.
→ Int J Periodontics Restorative Dent. 2012;32(4):459–65.8Cardaropoli D, Tamagnone L, Roffredo A, Gaveglio L, Cardaropoli G. Socket preservation using bovine bone mineral and collagen membrane: a randomized controlled clinical trial with histologic analysis.
→ Int J Periodontics Restorative Dent. 2012;32(4):421–30. Studies with long-term follow-ups have shown that the regenerated bone is maintained over time.9Jung RE, Fenner N, Hämmerle CH, Zitzmann NU. Long-term outcome of implants placed with guided bone regeneration (GBR) using resorbable and non-resorbable membranes after 12-14 years.
→ Clin Oral Implants Res. 2013;24(10):1065–73.10Buser D, Chappuis V, Bornstein MM, Wittneben JG, Frei M, Belser UC. Long-term stability of contour augmentation with early implant placement following single tooth extraction in the esthetic zone: a prospective, cross-sectional study in 41 patients with a 5- to 9-year follow-up.
→ J Periodontol. 2013;84(11):1517–27. Histological analyses have indicated that the slow resorption rate of DBBM is responsible for the long-term stability of the augmented bone volume.11Jensen SS, Bosshardt DD, Gruber R, Buser D. Long-term stability of contour augmentation in the esthetic zone: histologic and histomorphometric evaluation of 12 human biopsies 14 to 80 months after augmentation.
→ J Periodontol. 2014;85(11):1549–56.
DBBM is often used in combination with a semipermeable membrane. According to the principle of guided bone regeneration (GBR), the membrane is used to exclude epithelial cells from
the bone defect, thereby allowing bone formation. 12Hammerle CH, Jung RE. Bone augmentation by means of barrier membranes.
→ Periodontol 2000. 2003;33:36–53. In the early days of GBR, nonresorbable ePTFE (expanded polytetrafluoroethylene) barriers were successfully used to cover bone defects. 13Dahlin C, Andersson L, Linde A. Bone augmentation at fenestrated implants by an osteopromotive membrane technique. A controlled clinical study.
→ Clin Oral Implants Res. 1991;2(4):159–65.14Dahlin C, Lekholm U, Linde A. Membraneinduced bone augmentation at titanium implants. A report on ten fixtures followed from 1 to 3 years after loading.
→ Int J Periodontics Restorative Dent. 1991;11(4):273–81. However, postoperative wound dehiscence occurred frequently. It was often associated with infections that required early membrane removal and impaired bone regeneration.15Simion M, Baldoni M, Rossi P, Zaffe D. A comparative study of the effectiveness of e-PTFE membranes with and without early exposure during the healing period.
→ Int J Periodontics Restorative Dent. 1994;14(2):166–80.16Zitzmann NU, Naef R, Scharer P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration.
→ Int J Oral Maxillofac Implants. 1997;12(6):844–52.17Machtei EE. The effect of membrane exposure on the outcome of regenerative procedures in humans: a meta-analysis.
→ J Periodontol. 2001;72(4):512–6. doi:10.1902/ jop.2001.72.4.512. A resorbable native bilayer collagen membrane (NBCM) was shown to reduce the risk of membrane exposure and achieve comparable results to the ePTFE barriers with regard to bone regeneration. 18Zitzmann NU, Naef R, Scharer P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration.
→ Int J Oral Maxillofac Implants. 1997;12(6):844–52. If wound dehiscence occurred with the NBCM, healing was uneventful. Other studies have confirmed the promising healing characteristics of this membrane.19Tal H, Kozlovsky A, Artzi Z, Nemcovsky CE, Moses O. Long-term bio-degradation of cross-linked and non-cross-linked collagen barriers in human guided bone regeneration.
→ Clin Oral Implants Res. 2008;19(3):295–302. doi:10.1111/j.1600-0501.2007.01424.x.20Becker J, Al-Nawas B, Klein MO, Schliephake H, Terheyden H, Schwarz F. Use of a new cross-linked collagen membrane for the treatment of dehiscence-type defects at titanium implants: a prospective, randomized-controlled double-blinded clinical multicenter study.
→ Clin Oral Implants Res. 2009;20(7):742–9. doi:10.1111/j.1600-0501.2008.01689.x.
In general, it is recommended to achieve complete, but tension-free, primary wound closure over the collagen membrane. However, when bone augmentation procedures are performed, closing the flap without tension may become challenging. Splitting of the periosteum and extensive soft-tissue mobilization may then be necessary. This may increase morbidity, swelling and the rate of wound dehiscence because of impaired blood supply in a thinned flap. In addition, an insufficient vestibular depth, lack of keratinized tissue or scars may compromise the esthetic results and require additional surgical interventions.
Materials and methods
Evaluation included patients from a private practice who were treated between August 2005 and June 2014 using an open-healing approach. Patients underwent implant therapy to replace hopeless or missing teeth. Surgical interventions were performed as well as preand postoperative care administered according to our standard procedures. Membranes were applied in ridge preservation and in bone augmentation procedures, which were performed simultaneously with or before implant placement.
In ridge preservation procedures, hopeless teeth were extracted atraumatically. The extraction socket was cleaned and all granulation tissue was removed carefully. A DBBM (Geistlich Bio-Oss, Geistlich Pharma, Wolhusen, Switzerland) was applied into the socket according to the manufacturer’s instructions and covered with a membrane. In three-wall defects, that is, if the buccal bone wall was partially or completely missing, and if the defect was narrow and deep, a soft-tissue pond was prepared and the ice-cream cone technique21Tan-Chu JH, Tuminelli FJ, Kurtz KS, Tarnow DP. Analysis of buccolingual dimensional changes of the extraction socket using the “ice cream cone” flapless grafting technique.
→ Int J Periodontics Restorative Dent. 2014;34(3):399–403. doi:10.11607/prd.1605. was used.
In patients with missing teeth, a reduced full-thickness flap was prepared. If sufficient primary stability could be ensured, implants were placed immediately according to the manufacturers’ instructions. Bone augmentation was performed using DBBM or autogenous bone harvested from the drill hole. If the defect was large or if several bone walls were missing, mechanical stability was ensured using a titanium mesh (Synthes, Umkirch, Germany). A membrane was applied overlapping the defect. Membrane margins were placed under the flap and the flap was sutured tension-free, leaving the membrane partially exposed.
The following membrane materials were used:
- Geistlich Bio-Gide (NBCM; Geistlich Pharma)
- Jason membrane (JM; botiss biomaterials, Berlin, Germany)
- Socket Repair Membrane (SRM; Zimmer Biomet, Freiburg, Germany)
- DynaMatrix (DM; Keystone Dental, Alfter, Germany)
- Geistlich Mucograft Seal (CMXs; Geistlich Pharma)
- Histoacryl (HIA; B. Braun Medical, Melsungen, Germany).
Antibiotics were prescribed in accordance with current guidelines, that is, in patients at higher risk, such as valvular heart disease or inflammation due to tooth fracture prior to tooth extraction. Suture removal took place after two weeks. In order to allow maturation of bone and soft tissue, sites were allowed to heal for at least six months before implant placement or secondary augmentation procedures were performed. A typical clinical case is shown in Figures 1a–n.
-

- Fig. 1 a

-

- Fig. 1 b

-
- Fig. 1 c
-
- Fig. 1 d
-
- Fig. 1 e

-

- Fig. 1 f

-

- Fig. 1 g
-

- Fig. 1 h

-

- Fig. 1 i
-

- Fig. 1 j

-
- Fig. 1 k
-

- Fig. 1 l

-
- Fig. 1 m
-

- Fig. 1 n
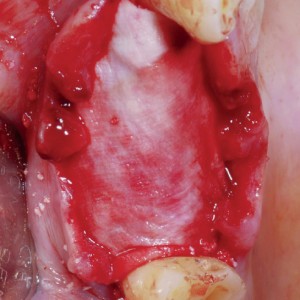
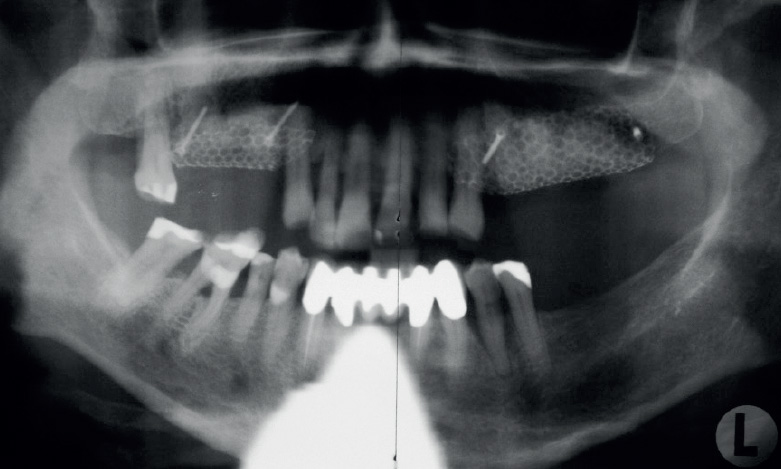
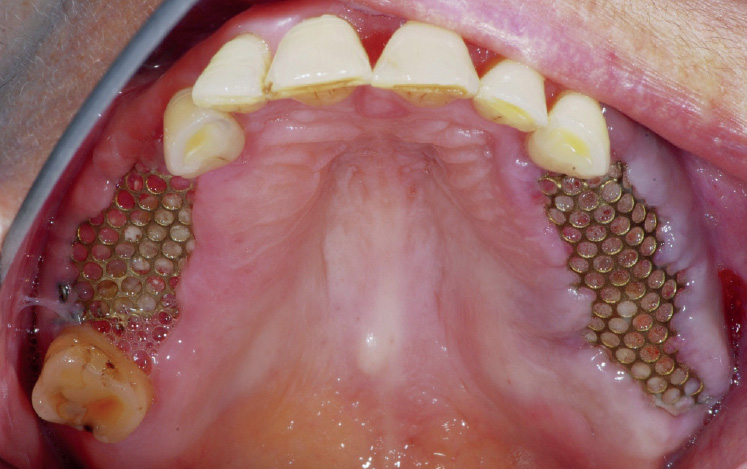
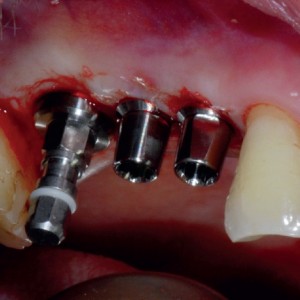
Fig. 1 a-n
Initial (a) clinical and (b) radiographic situation prior to tooth extraction. Owing to periodontal bone loss, teeth in the upper and lower jaws were extracted.
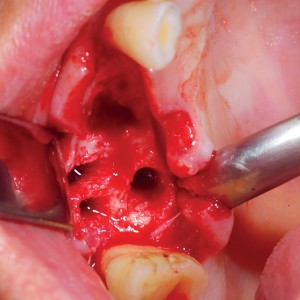
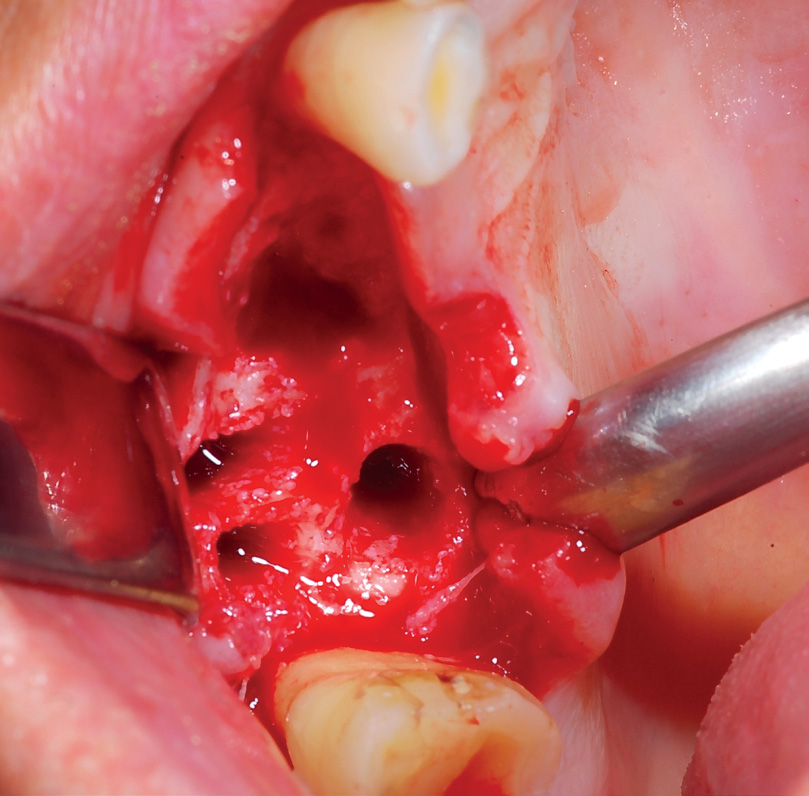
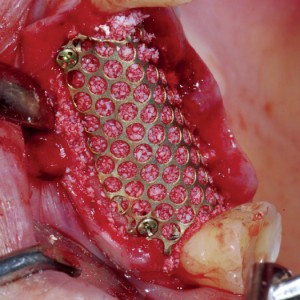
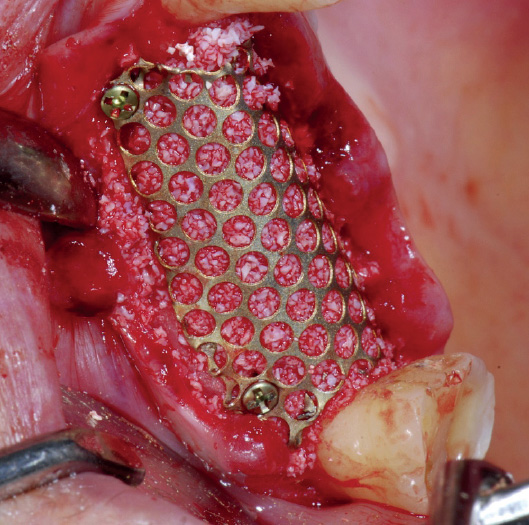
Intraoperative view:
(c) Ridge situation after atraumatic extraction and reduced flap elevation. (d) The extraction sites were filled with DBBM, and titanium nets were placed bilaterally to stabilize the augmented volume (first quadrant is shown here). (e) Placement of a native bilayer collagen membrane (NBCM) over the titanium mesh. The flap was sutured without tension, leaving the NBCM exposed. (f) Clinical situation two days after surgery. (g) Radiographic situation two weeks after surgery.
During healing:
(h) Nine days and (i) three weeks after surgery. The membrane had resorbed and the titanium mesh was visible. (j) After three months, the titanium mesh was removed.
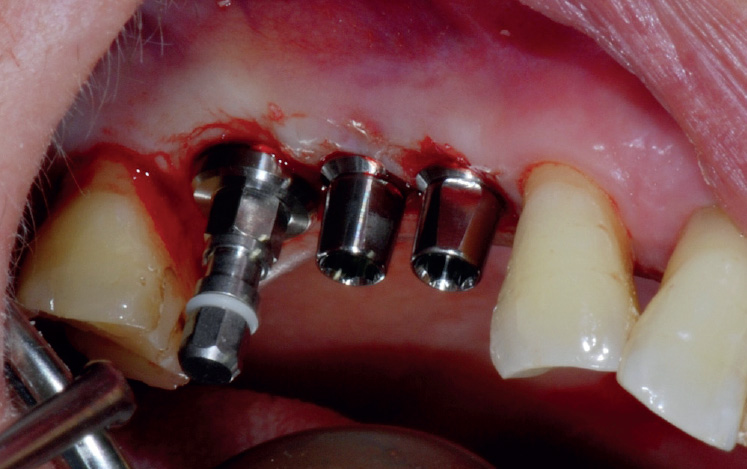
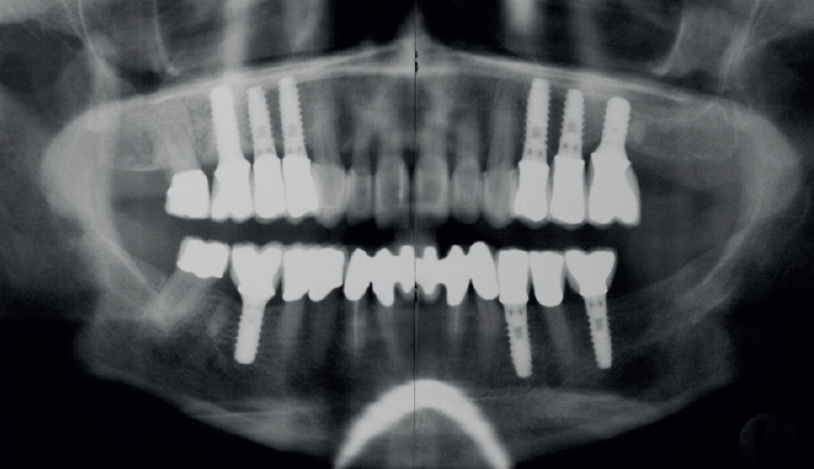
After healing: (k) Six months after surgery, implants were placed using minimally invasive surgery. (l) Final restoration and (m) radio graphic view after 15 months. (n) Stable clinical situation five years after augmentation.
Evaluation
In many cases, one membrane was used to cover multiple neighboring defects. These sites were defined as one surgical area. The data were retrospectively analyzed for defect morphology (number of remaining bone walls), size of surgical area (number of neighboring sites), indication, complications during healing, loss of graft material, possibility of performing flapless implantation and need for follow-up augmentation procedures (none, planned or unplanned). The primary outcome parameter was the need to perform an unplanned augmentation during the implant procedure. The secondary outcome parameter was complication rate during wound healing. In addition, the data were analyzed to determine whether unfavorable defect morphology might increase the frequency of healing complications and whether the membranes differed with regard to healing complications.
Statistics
Explorative analysis of the data was performed using R (Version 3.2.2; R Foundation Vienna, Austria). A possible correlation between healing complications and membrane type or defect morphology (number of bone walls) was evaluated using the exact chi-squared test or Fisher exact test for general frequency tables at the 5% level of significance. Additionally, a Spearman rank correlation coefficient was calculated for healing cpmplications and defect morphology. The univariate results were confirmed by a multivariate logistic regression using healing complications as the main variable and defect morphology and membrane type as co-variables.
Results
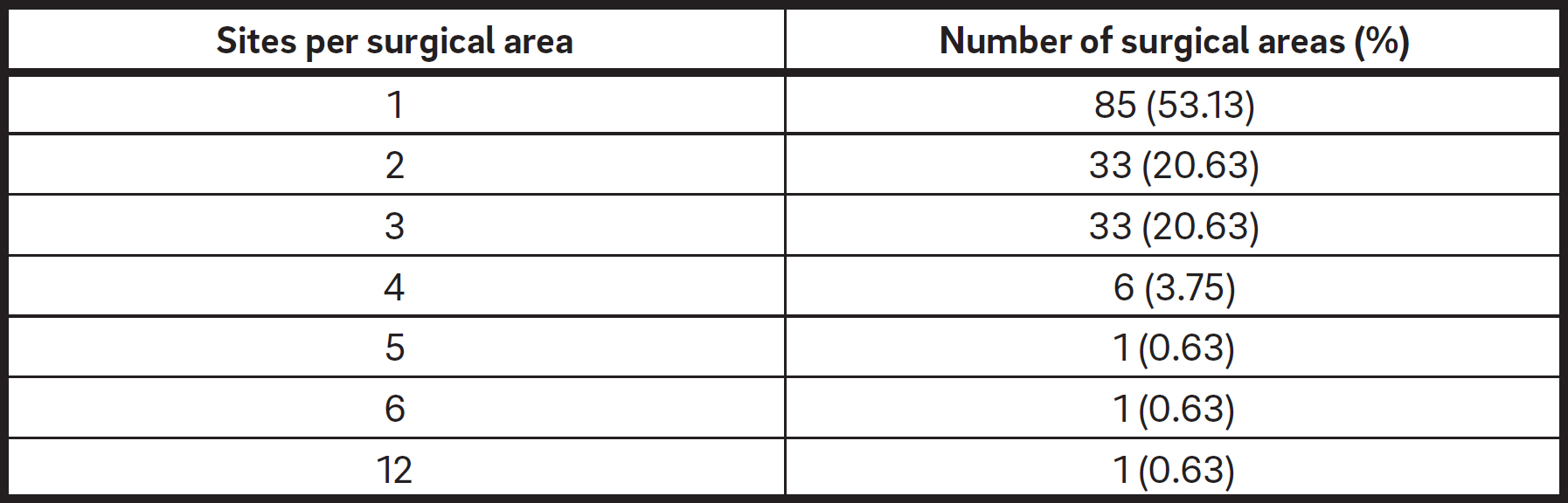
During the observation period, a total of 127 patients with 171 surgical areas were treated using the open-healing approach. Eight patients were lost to follow-up because they did not show up for implant placement. Therefore, the analysis included 160 surgical areas in 119 patients. Of the patients, 49.6% were male and 50.4% female. Mean patient age was 54.3 ± 13.0 years (aged 29–88 years). The maximum number of surgical areas per patient was four. A surgical area contained 1.89 ± 1.26 sites on average (Table 1). The number of missing bone walls per surgical area is shown in Table 2.

Surgical area contained sites with one, two, three and four bone wall defects.
‡ Surgical area contained sites with two and three bone wall defects.
§ Surgical area contained sites with three and four bone wall defects.
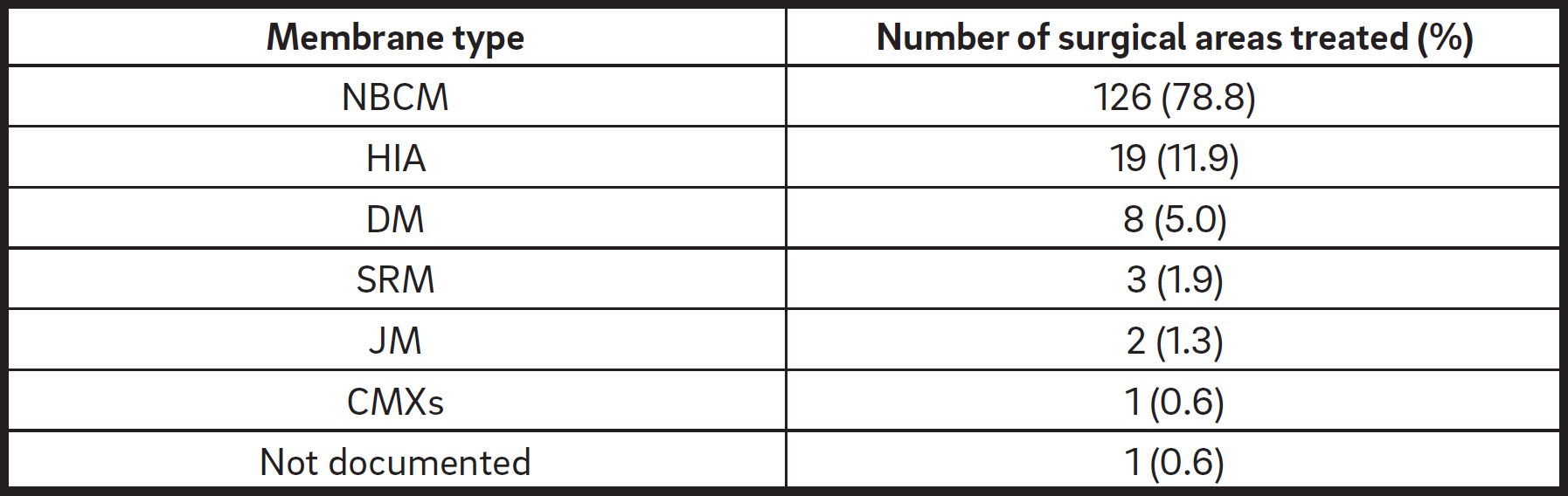
DBBM was used in 98.1% and autogenous bone in 1.9% of the surgical areas. In 78.8% of the surgical areas, NBCM was used (Table 3). A titanium mesh was additionally applied in 11.3% of the surgical areas. Of these surgical areas, 88.9% were covered with NBCM, 5.55% with JM and 5.55% with DM.
Bone augmentation procedures were performed in 33.1% of the surgical areas. They included bone splitting, horizontal, and/or vertical bone augmentation and sinus floor elevation. Ridge preservation alone was performed in 41.9% of the surgical areas. In 13.1%, ridge preservation was combined with bone augmentation. The ice-cream cone technique was used in 14% of the surgical areas (26% of all areas undergoing ridge preservation). In 1.25% of the surgical areas, bone defects were treated owing to implant removal.
A total of 32.5% of the surgical areas included an extraction site in which immediate implant placement was performed. In 10.6% of the surgical areas, implants were placed into healed bone simultaneously with the augmentation procedure.
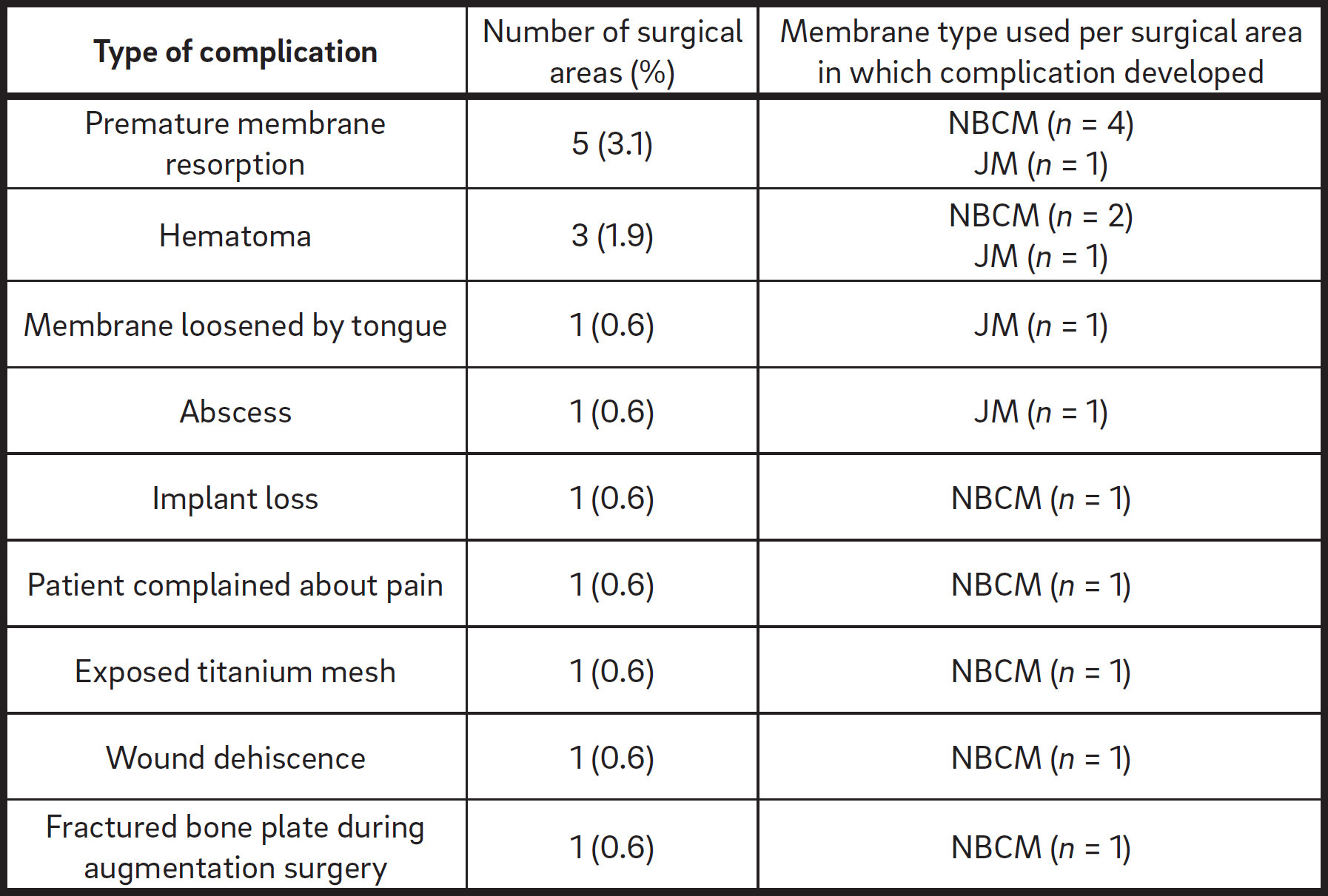
Healing was uneventful in 90.6% of the surgical areas. Complications during healing occurred in 15 areas (9.4%; Table 4). Five of these areas had undergone ridge preservation, three areas ridge preservation combined with bone augmentation and seven areas augmentation procedures. The complications included premature membrane resorption (five areas: four covered with NBCM; one covered with JM), hematoma (three areas: two covered with NBCM; one covered with JM) and membrane loosened by tongue (one area covered with NBCM). One patient developed an abscess (area covered with JM), one implant was lost (area covered with NBCM) and another patient complained about pain six weeks after surgery (area covered with NBCM). The patient was successfully treated with antibiotics. Other complications were an exposed titanium mesh (one area covered with NBCM), wound dehiscence (one area covered with NBCM) and a fractured bone plate during the augmentation surgery (one area covered with NBCM). The graft was partially lost in three surgical areas (1.9%; one area covered with JM; two areas covered with NBCM).
The number of complications per defect morphology type is given in Table 5. The number of morphology categories was too large to test for a correlation between the number of present bone walls and frequency of healing complications. When only the two most frequent defect morphologies, that is, three- and four-wall defects, were compared with each other, no clear indication of a correlation was found. In both morphology types, the percentage of healing problems was very similar. When defect morphology was coded as a figure (e.g., 2–3 was 2.5), a rank correlation of -0.052 was calculated. This indicated that defects with a higher number of bone walls slightly tended to have fewer healing complications. Healing complications occurred in 9.52% of the surgical areas covered with NBCM and in 8.82% of the areas covered with a different membrane type. The data did not indicate any correlation between membrane type and healing complications.

Implantationor secondary augmentation
The average healing phase until implantation and/or secondary augmentation was 5.2 ± 8.1 months (0–58 months). Implants could be inserted as planned in a two-stage procedure in all but one surgical area. Flapless implantation was possible in 58.8% of the surgical areas. In 86.88% of the surgical areas, no secondary augmentation was necessary (Table 6). Secondary augmentation procedures were performed according to the treatment plan in 12.5% of the surgical areas. They ranged from minor to extensive interventions and included sinus floor augmentation in nine surgical areas (three internal sinus lifts), bone spreading in three and bone splitting in two. There was only one surgical area in which an abscess required an unplanned re-augmentation and implant insertion was there fore not possible as planned.

† Re-augmentation.
Discussion
In this analysis, different collagen membranes and matrices, as well as tissue glue, were used in ridge preservation and augmentation procedures in an open-healing approach in a variety of indications and defect types. The clinical outcomes were evaluated retrospectively. The primary outcome parameter was the necessity to perform unplanned augmentation since this was regarded to be a partial failure of the regenerative treatment. The treatment was judged to be successful if no re-augmentation had to be performed or if an additional bone augmentation could be performed as planned at the time point of the first intervention. There was just one case in which an unplanned re-augmentation had to be performed owing to an abscess. Therefore, the surgical approach using open healing was successful according to the criterion of no unplanned re-augmentation being required in 99.4% of the surgical areas.
However, owing to the retrospective and uncontrolled nature of this study, it is not known whether a closed-healing approach might have resulted in improved bone regeneration or might have reduced the extent of a planned secondary augmentation. Exposure of resorbable membranes may be associated with premature membrane degradation and a shortened barrier function. 22Becker J, Al-Nawas B, Klein MO, Schliephake H, Terheyden H, Schwarz F. Use of a new cross-linked collagen membrane for the treatment of dehiscence-type defects at titanium implants: a prospective, randomized-controlled double-blinded clinical multicenter study.
→ Clin Oral Implants Res. 2009;20(7):742–9. doi:10.1111/j.1600-0501.2008.01689.x. Various studies have shown controversial results regarding the effect of secondary wound dehiscence occurring during healing. Moses et al. evaluated bone healing of buccal periimplant bone dehiscence defects with or without membrane exposure.23Moses O, Pitaru S, Artzi Z, Nemcovsky CE. Healing of dehiscence-type defects in implants placed together with different barrier membranes: a comparative clinical study.
→ Clin Oral Implants Res. 2005;16(2):210–9. doi:10.1111/j.1600-0501.2004.01100.x. Using NBCM, they found a mean defect reduction of 95% in the case of uneventful healing, while defect resolution was significantly reduced to 53% when the membrane was exposed. In a dog study, a significant negative effect of membrane exposure on defect fill was found too.24Oh TJ, Meraw SJ, Lee EJ, Giannobile WV, Wang HL. Comparative analysis of collagen membranes for the treatment of implant dehiscence defects.
→ Clin Oral Implants Res. 2003;14(1):80–90. In contrast, other studies demonstrated only a slight, nonsignificant reduction in defect fill if exposed membrane sites were compared to nonexposed ones.25Zitzmann NU, Naef R, Scharer P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration.
→ Int J Oral Maxillofac Implants. 1997;12(6):844–52.26Becker J, Al-Nawas B, Klein MO, Schliephake H, Terheyden H, Schwarz F. Use of a new cross-linked collagen membrane for the treatment of dehiscence-type defects at titanium implants: a prospective, randomized-controlled double-blinded clinical multicenter study.
→ Clin Oral Implants Res. 2009;20(7):742–9. doi:10.1111/j.1600-0501.2008.01689.x.
In ridge preservation, positive results using the membrane in an open-healing approach have been described before. Filipek et al. compared open and closed healing in extraction sites in 40 patients.27Filipek D, Koszowski R, Smieszek-Wilczewska J. A comparative clinical study on human tooth extractions: flap vs flapless buccal surgery.
→ Quintessence Int. 2012;43(10):887–9. When analyzing the dimensions of the alveolar ridge six months after tooth extraction, they did not find any significant difference between open and closed healing. In another study, Cardaropoli et al. achieved good results using open healing with regard to ridge dimension.28Cardaropoli D, Tamagnone L, Roffredo A, Gaveglio L, Cardaropoli G. Socket preservation using bovine bone mineral and collagen membrane: a randomized controlled clinical trial with histologic analysis.
→ Int J Periodontics Restorative Dent. 2012;32(4):421–30. However, the control treatment was spontaneous extraction socket healing and there was no control treatment with closed healing.
Owing to its retrospective nature and the lack of a control group, the current analysis does not allow drawing of clear conclusions on whether open healing may have a certain negative effect on the outcome of the regenerative procedure. The positive result regarding the low necessity of re-augmentation indicates that open healing may be a suitable clinical procedure. However, prospective studies should compare the outcome of open and closed healing under standardized clinical conditions.
In this study, the second outcome parameter was the incidence of complications during healing. Healing was uneventful in 90.6% of the surgical areas. In 2.5% of the surgical areas, the complications were associated with the surgical intervention (hematoma and one broken bone plate). In 6.9% of the areas, the complications may have been related to the open-healing approach. These complications were premature resorption, membrane loosening by tongue, exposed titanium mesh and wound dehiscence. A certain rate of healing complications has been reported with closed healing too. In a study using NBCM in periimplant defects, Zitzmann et al. found wound dehiscences in 16% of the defects at the time point of suture removal.29Zitzmann NU, Naef R, Scharer P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration.
→ Int J Oral Maxillofac Implants. 1997;12(6):844–52. Von Arx and Buser reported a complication rate of 9.5% during healing in horizontal ridge augmentation.30Von Arx T, Buser D. Horizontal ridge augmentation using autogenous block grafts and the guided bone regeneration technique with collagen membranes: a clinical study with 42 patients.
→ Clin Oral Implants Res. 2006;17(4):359–66. The sites re-epithelized spontaneously within two to four weeks and the authors concluded that the membrane did not cause infections when exposed.
Moses et al. found wound dehiscences in 39% of patients treated with cross-linked collagen membranes.31Moses O, Pitaru S, Artzi Z, Nemcovsky CE. Healing of dehiscence-type defects in implants placed together with different barrier membranes: a comparative clinical study.
→ Clin Oral Implants Res. 2005;16(2):210–9. doi:10.1111/j.1600-0501.2004.01100.x. In a multicenter randomized, controlled clinical trial, bone augmentation procedures using DBBM and NBCM were applied in 90% of 208 patients undergoing immediate implant placement with transmucosal healing.32Lang NP, Tonetti MS, Suvan JE, Pierre Bernard J, Botticelli D, Fourmousis I, Hallund M, Jung R, Laurell L, Salvi GE, Shafer D, Weber HP; European Research Group on Periodontology. Immediate implant placement with transmucosal healing in areas of aesthetic priority. A multicentre randomized-controlled clinical trial I. Surgical outcomes.
→ Clin Oral Implants Res. 2007;18(2):188–96. doi:10.1111/j.1600-0501.2006.01371.x. After one week, flap dehiscences were noted in 12% of the cases. After two weeks, the percentage had decreased to 6.0% and after six weeks to 1.5%, indicating proper secondary healing even in the case of membrane exposure. In the retrospective analysis presented here, the overall complication rate of 9.4% indicates that open healing is not associated with an increased risk of healing complications compared with closed healing. Studies have indicated that native collagen membranes may facilitate angiogenesis.33Schwarz F, Rothamel D, Herten M, Wüstefeld M, Sager M, Ferrari D, Becker J. Immunohistochemical characterization of guided bone regeneration at a dehiscencetype defect using different barrier membranes: an experimental study in dogs.
→ Clin Oral Implants Res. 2008;19(4):402–15. doi:10.1111/j.1600-0501.2007.01486.x. and allow for less compromised wound healing in comparison with cross-linked collagen materials. 34Becker J, Al-Nawas B, Klein MO, Schliephake H, Terheyden H, Schwarz F. Use of a new cross-linked collagen membrane for the treatment of dehiscence-type defects at titanium implants: a prospective, randomized-controlled double-blinded clinical multicenter study.
→ Clin Oral Implants Res. 2009;20(7):742–9. doi:10.1111/j.1600-0501.2008.01689.x. Therefore, native collagen may promote uneventful soft-tissue healing under openhealing conditions too. Apart from materialrelated wound dehiscence, iatrogenic factors like suture technique may play an even more important role, but to our knowledge, no study has reported on the rate and effect of tensionless wound closure compared with flaps under tension. However, further studies are needed to investigate wound healing when the flap is not closed over the membrane.
Owing to the large variety of defect morphologies, no clear correlation could be found between defect morphology and healing complications, although there was a small trend for a higher complication rate in defects with a higher number of missing bone walls. However, the positive outcomes for all defect morphologies indicate that open healing is not limited to a certain defect type.
While NBCM was applied in most of the areas, a few other materials were used too. The number was too small to draw a clear conclusion on possible differences in healing between these different membrane types. Further studies are necessary to compare the suitability of various membranes for open healing.
Conclusion
The retrospective analysis of patients treated in a private practice indicates that open healing using suitable membrane materials allows uneventful healing and sufficient bone formation. Thereby, soft-tissue problems associated with extensive flap mobilization and tension may be avoided. There was no control group and the data set included different indications, defect morphologies and defect sizes. While this limits the power of the study, it reflects the situation in private practice. Furthermore, if open healing allows for achieving good results in a nonuniform patient group, one may conclude that it could have the potential to become a general clinical option. Prospective studies with control groups are needed to further investigate this surgical approach.
Competing interests
The author declares that he has no competing interests.
Interview
with Dr. Taffet Georg
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 30. | ↑ | Von Arx T, Buser D. Horizontal ridge augmentation using autogenous block grafts and the guided bone regeneration technique with collagen membranes: a clinical study with 42 patients. → Clin Oral Implants Res. 2006;17(4):359–66. |
| 2. | ↑ | Jensen T, Schou S, Stavropoulos A, Terheyden H, Holmstrup P. Maxillary sinus floor augmentation with Bio-Oss or Bio-Oss mixed with autogenous bone as graft: a systematic review. → Clin Oral Implants Res. 2012;23(3):263–73. |
| 3. | ↑ | Urban IA, Nagursky H, Lozada JL, Nagy K. Horizontal ridge augmentation with a collagen membrane and a combination of particulated autogenous bone and anorganic bovine bone-derived mineral: a prospective case series in 25 patients. → Int J Periodontics Restorative Dent. 2013;33(3):299–307. |
| 4. | ↑ | Chen ST, Darby IB, Reynolds EC. A prospective clinical study of non-submerged immediate implants: clinical outcomes and esthetic results. → Clin Oral Implants Res. 2007;18(5):552–62. |
| 5. | ↑ | Ackermann KL. Extraction site management using a natural bone mineral containing collagen: rationale and retrospective case study. → Int J Periodontics Restorative Dent. 2009;29(5):489–97. |
| 6. | ↑ | Nevins M, Camelo M, De Paoli S, Friedland B, Schenk RK, Parma-Benfenati S, Simion M, Tinti C, Wagenberg B. A study of the fate of the buccal wall of extraction sockets of teeth with prominent roots. → Int J Periodontics Restorative Dent. 2006;26(1):19–29. |
| 7. | ↑ | Perelman-Karmon M, Kozlovsky A, Liloy R, Artzi Z. Socket site preservation using bovine bone mineral with and without a bioresorbable collagen membrane. → Int J Periodontics Restorative Dent. 2012;32(4):459–65. |
| 8, 28. | ↑ | Cardaropoli D, Tamagnone L, Roffredo A, Gaveglio L, Cardaropoli G. Socket preservation using bovine bone mineral and collagen membrane: a randomized controlled clinical trial with histologic analysis. → Int J Periodontics Restorative Dent. 2012;32(4):421–30. |
| 9. | ↑ | Jung RE, Fenner N, Hämmerle CH, Zitzmann NU. Long-term outcome of implants placed with guided bone regeneration (GBR) using resorbable and non-resorbable membranes after 12-14 years. → Clin Oral Implants Res. 2013;24(10):1065–73. |
| 10. | ↑ | Buser D, Chappuis V, Bornstein MM, Wittneben JG, Frei M, Belser UC. Long-term stability of contour augmentation with early implant placement following single tooth extraction in the esthetic zone: a prospective, cross-sectional study in 41 patients with a 5- to 9-year follow-up. → J Periodontol. 2013;84(11):1517–27. |
| 11. | ↑ | Jensen SS, Bosshardt DD, Gruber R, Buser D. Long-term stability of contour augmentation in the esthetic zone: histologic and histomorphometric evaluation of 12 human biopsies 14 to 80 months after augmentation. → J Periodontol. 2014;85(11):1549–56. |
| 12. | ↑ | Hammerle CH, Jung RE. Bone augmentation by means of barrier membranes. → Periodontol 2000. 2003;33:36–53. |
| 13. | ↑ | Dahlin C, Andersson L, Linde A. Bone augmentation at fenestrated implants by an osteopromotive membrane technique. A controlled clinical study. → Clin Oral Implants Res. 1991;2(4):159–65. |
| 14. | ↑ | Dahlin C, Lekholm U, Linde A. Membraneinduced bone augmentation at titanium implants. A report on ten fixtures followed from 1 to 3 years after loading. → Int J Periodontics Restorative Dent. 1991;11(4):273–81. |
| 15. | ↑ | Simion M, Baldoni M, Rossi P, Zaffe D. A comparative study of the effectiveness of e-PTFE membranes with and without early exposure during the healing period. → Int J Periodontics Restorative Dent. 1994;14(2):166–80. |
| 16, 18, 25, 29. | ↑ | Zitzmann NU, Naef R, Scharer P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration. → Int J Oral Maxillofac Implants. 1997;12(6):844–52. |
| 17. | ↑ | Machtei EE. The effect of membrane exposure on the outcome of regenerative procedures in humans: a meta-analysis. → J Periodontol. 2001;72(4):512–6. doi:10.1902/ jop.2001.72.4.512. |
| 19. | ↑ | Tal H, Kozlovsky A, Artzi Z, Nemcovsky CE, Moses O. Long-term bio-degradation of cross-linked and non-cross-linked collagen barriers in human guided bone regeneration. → Clin Oral Implants Res. 2008;19(3):295–302. doi:10.1111/j.1600-0501.2007.01424.x. |
| 20, 22, 26, 34. | ↑ | Becker J, Al-Nawas B, Klein MO, Schliephake H, Terheyden H, Schwarz F. Use of a new cross-linked collagen membrane for the treatment of dehiscence-type defects at titanium implants: a prospective, randomized-controlled double-blinded clinical multicenter study. → Clin Oral Implants Res. 2009;20(7):742–9. doi:10.1111/j.1600-0501.2008.01689.x. |
| 21. | ↑ | Tan-Chu JH, Tuminelli FJ, Kurtz KS, Tarnow DP. Analysis of buccolingual dimensional changes of the extraction socket using the “ice cream cone” flapless grafting technique. → Int J Periodontics Restorative Dent. 2014;34(3):399–403. doi:10.11607/prd.1605. |
| 23, 31. | ↑ | Moses O, Pitaru S, Artzi Z, Nemcovsky CE. Healing of dehiscence-type defects in implants placed together with different barrier membranes: a comparative clinical study. → Clin Oral Implants Res. 2005;16(2):210–9. doi:10.1111/j.1600-0501.2004.01100.x. |
| 24. | ↑ | Oh TJ, Meraw SJ, Lee EJ, Giannobile WV, Wang HL. Comparative analysis of collagen membranes for the treatment of implant dehiscence defects. → Clin Oral Implants Res. 2003;14(1):80–90. |
| 27. | ↑ | Filipek D, Koszowski R, Smieszek-Wilczewska J. A comparative clinical study on human tooth extractions: flap vs flapless buccal surgery. → Quintessence Int. 2012;43(10):887–9. |
| 32. | ↑ | Lang NP, Tonetti MS, Suvan JE, Pierre Bernard J, Botticelli D, Fourmousis I, Hallund M, Jung R, Laurell L, Salvi GE, Shafer D, Weber HP; European Research Group on Periodontology. Immediate implant placement with transmucosal healing in areas of aesthetic priority. A multicentre randomized-controlled clinical trial I. Surgical outcomes. → Clin Oral Implants Res. 2007;18(2):188–96. doi:10.1111/j.1600-0501.2006.01371.x. |
| 33. | ↑ | Schwarz F, Rothamel D, Herten M, Wüstefeld M, Sager M, Ferrari D, Becker J. Immunohistochemical characterization of guided bone regeneration at a dehiscencetype defect using different barrier membranes: an experimental study in dogs. → Clin Oral Implants Res. 2008;19(4):402–15. doi:10.1111/j.1600-0501.2007.01486.x. |





Leave a Reply
Be the First to Comment!