Retrospective analysis of periimplantitis therapy of 158 implants
March 20, 2017 / Categories: Digital Dentistry, Implant Dentistry

Wiegner, Jörg-Ulf
Klinsmann, Hermann
Kömmling, Toralf
The objective of the retrospective analysis was to evaluate the efficacy of periimplantitis treatment up to a five-year observation period.
Introduction
Implant therapy is a well-established method to restore missing teeth. However, periimplant tissue infections due to biofilm formation may compromise implant survival. The term “periimplantitis” describes an inflammatory process in the periimplant mucosa with additional signs of bone loss.1Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant diseases.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):286–91. Periimplantitis occurs in around 10% of implants and 20% of patients.2Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant diseases.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):286–91.3Atieh MA, Alsabeeha NH, Faggion CM Jr, uncan WJ. The frequency of peri-implant diseases: a systematic review and meta-analysis.
→ J Periodontol. 2013 Nov;84(11):1586–98.4Mombelli A, Muller N, Cionca N. The epidemiology of peri-implantitis.
→ Clin Oral Implants Res. 2012 Oct;23 Suppl 6:67–76. A very recent meta-analysis reported a mean prevalence of 22% (CI: 14–30%) for periimplantitis.5Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology.
→ J Clin Periodontol. 2015 Apr;42 Suppl 16:S158–71.
Risk factors for periimplantitis are poor plaque control, history of periodontitis, smoking, uncontrolled diabetes, periimplant cement residue, genetic factors, occlusal overload and history of periimplantitis.6American Academy of Periodontology. Peri-implant mucositis and periimplantitis: a current understanding of their diagnoses and clinical implications.
→ J Periodontol. 2013 Apr;84(4):436–43.7Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. Current strategies for periimplantitis therapy include a pretreatment phase with professional tooth cleaning, optimization of plaque control with prosthesis adjustment if necessary and nonsurgical debridement.8Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review.
→ Int J Oral Maxillofac Implants. 2014;29 Suppl:325–45.9Heitz-Mayfield LJ, Needleman I, Salvi GE, Pjetursson BE. Consensus statements and clinical recommendations for prevention and management of biologic and technical implant complications.
→ Int J Oral Maxillofac Implants. 2014;29 Suppl:346–50.
10Meyle J. Mechanical, chemical and laser treatments of the implant surface in the presence of marginal bone loss around implants.
→ Eur J Oral Implantol. 2012;5 Suppl:S71–81. Afterward, in the surgical phase, a full-thickness flap is prepared and the contaminated implant surface is thoroughly cleaned. Intraosseous defects can be filled using a bone substitute or tissue graft material with or without a resorbable membrane. The postsurgical protocol includes systemic antibiotic therapy and chlorhexidine rinsing during the healing phase, followed by the maintenance phase with regular recall visits, ranging from three to six months.
Regenerative surgical therapy has been shown to predictably obtain partial to full defect fill,11Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis.
→ Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94. although the outcome may be influenced by the defect morphology 12Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis.
→ J Clin Periodontol. 2010 May;37(5):449–55. and implant surface.13Roccuzzo M, Bonino F, Bonino L, Dalmasso P. Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: comparative results of a prospective study on two different implant surfaces.
→ J Clin Periodontol. 2011 Aug;38(8):738–45. According to the concept of guided bone regeneration (GBR), the use of a deproteinized bovine bone mineral (DBBM) either with or without a native bilayer collagen membrane (NBCM) has been evaluated in various clinical studies and demonstrated marked short-term clinical improvements and promising long-term results.14Roccuzzo M, Bonino F, Bonino L, Dalmasso P. Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: comparative results of a prospective study on two different implant surfaces.
→ J Clin Periodontol. 2011 Aug;38(8):738–45.15Aghazadeh A, Rutger Persson G, Renvert S. A single-centre randomized controlled clinical trial on the adjunct treatment of intra-bony defects with autogenous bone or a xenograft: results after 12 months.
→ J Clin Periodontol. 2012 Jul;39(7):666–73.)16Froum SJ, Froum SH, Rosen PS. Successful management of peri-implantitis with a regenerative approach: a consecutive series of 51 treated implants with 3- to 7.5-year follow-up.
→ Int J Periodontics Restorative Dent. 2012 Feb;32(1):11–20.17Matarasso S, Iorio Siciliano V, Aglietta M, Andreuccetti G, Salvi GE. Clinical and radiographic outcomes of a combined resective and regenerative approach in the treatment of peri-implantitis: a prospective case series.
→ Clin Oral Implants Res. 2014 Jul;25(7):761–7.18Roccuzzo M, Gaudioso L, Lungo M, Dalmasso P. Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with 10% collagen.
→ J Clin Periodontol. 2016 Mar;43(3):311–8. The aim of our retrospective evaluation was to analyze the efficacy of the periimplantitis treatment with or without bone augmentation in patients over a long-term observation period up to five years post-therapy.
Materials and methods
Study population
The retrospective evaluation included 107 patients with 158 implants that were treated for periimplantitis between 2009 and 2015. Implants had been inserted between 1993 and 2014 by the same surgeon (JUW) according to the manufacturers’ instructions. Implant systems included Steri-Oss (Nobel Biocare, Zurich, Switzerland), CAMLOG implant system (Cylinder Line, Screw Cylinder Line, Root-Line, SCREW-LINE, SCREW-LINE Promote plus, iSy, CAMLOG Biotechnologies, Basel, Switzerland), ITI and Straumann implants (Straumann, Basel, Switzerland), FRIALIT 2 (Dentsply Sirona, Mannheim, Germany), XiVE (Dentsply Sirona), ASTRA TECH OsseoSpeed (Dentsply Sirona), IMZ Twin- Plus (Dentsply Sirona) and ANKYLOS (Dentsply Sirona). If necessary, bone augmentation procedures were performed before or during the implantation. After completion of the healing phase, the patients were referred back to their dentists or prosthodontists for further prosthetic treatment and follow-up. Later on, some of those patients were referred to our practice again because of periimplantitis.
Therapy
Defect classes and treatment protocol according to Schwarz et al.19Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs.
→ Clin Oral Implants Res. 2007 Apr;18(2):161–70.20Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study.
→ J Clin Periodontol. 2011 Mar;38(3):276–84.
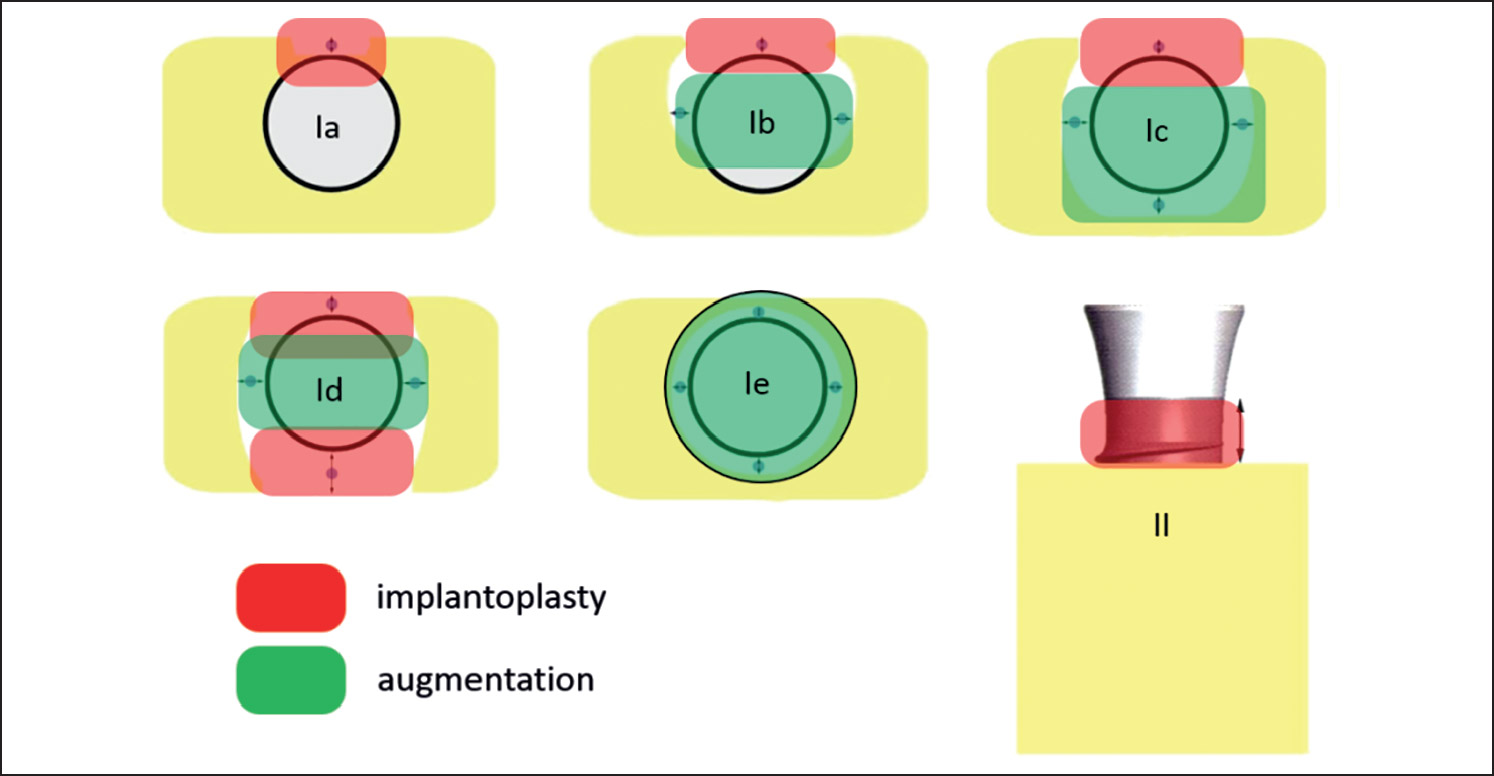
Ia (buccal vertical bone dehiscence),
Ib (buccal dehiscence and semicircular bone defect to the middle of the implant body),
Ic (buccal dehiscence, circular bone defect, maintained lingual solid bone),
Id (buccal and lingual dehiscence defects),
Ie (circular bone resorption, buccal and oral compacta maintained),
II (supra-alveolar circumferential bone loss).
Before periimplantitis treatment, clinical and radiographic evaluation took place. In the case of acute inflammation, anti-inflammatories were locally applied. Patients underwent professional tooth cleaning and periodontal therapy in the case of generalized periodontitis.
Periimplantitis was classified and treated in accordance with Schwarz et al. (Fig. 1).21Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs.
→ Clin Oral Implants Res. 2007 Apr;18(2):161–70.22Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study.
→ J Clin Periodontol. 2011 Mar;38(3):276–84. After exposing the defects and removing granulation tissue, implantoplasty was performed using diamonds rotary instruments and Arkansas stones finishing burs. Defects were cleaned with sterile saline. Intraosseous defects (defect Classes Ib, c, d and e; Fig. 1) were augmented according to the treatment protocol using a DBBM (Geistlich Bio-Oss spongiosa granules, Geistlich Pharma, Wolhusen, Switzerland) and an NBCM (Geistlich Bio-Gide Perio, Geistlich Pharma). The surgical area was carefully closed, a periodontal wound dressing applied (Coe-Pak, GC Europe, Leuven, Belgium) and a radiographic evaluation performed. Patients were advised to rinse cautiously with chlorhexamed 0.2% (GSK, London, U.K.) from the first day postsurgery for one week. Antibiotics were given at the discretion of the surgeon starting 24 h before surgery until suture removal eight days postsurgery. Patients were followed up according to a strict recall schedule in our practice. If necessary, supplementary therapy, such as gingivectomy or implantoplasty, was performed during the follow-up phase.
Analysis
Both hopeless implants extracted before the periimplantitis therapy and implants treated by a different dentist with incomplete data were not included in our evaluation. Data for the clinical evaluation were retrieved retrospectively from the patient files in our practice and included plaque index, full-mouth bleeding on probing (BOP) and probing pocket depth (PPD). PPD was measured from the mucosal margin to the bottom of the probeable pocket mesially, distally, orally and vestibularly at the start of the periimplantitis therapy and during recall visits in our practice at 3, 6, 9, 12, 24, 36, 48 and 49 to 56 months. In order to evaluate possible risk factors for periimplantitis, signs of prosthetic deficiencies at the start of the therapy were analyzed, as was history of periimplantitis. Additionally, patient files were analyzed to identify smoking, bisphosphonate intake and diabetic patients at the time of implantation.
In order to analyze the prevalence of periimplantitis per indication, implants were allocated to one of the following indication classes as defined at the consensus conference of the BDIZ EDI, DGI, DGMKG, DGZI and BDO (national German dental associations) on Oct. 8, 2014:
- Ia: single-tooth replacement in the anterior area;
- Ib: single-tooth replacement in the posterior area;
- IIa: interdental space;
- IIb: free-end situation;
- IIc: greatly reduced residual dentition; and
- III: edentulous jaw.
In an additional subanalysis, implants inserted between 1993 and 2014 were evaluated for primary indication classes and the rate of explantations.
Statistic alanalysis
The following exploratory tests were performed:
- To test the null hypothesis of no association between indication class and the need for implant therapy, the approximate chi-squared test for association was used. The significance level was set at 5%.
- All pairs of indication classes were tested against each other using the same chi-squared tests. In order to avoid inflation of Type I error due to multiple testing, all p-values were multiplied by the number of such comparisons (15; Bonferroni correction).
- Each indication class was compared to all other indication classes pooled using the chisquared tests already mentioned above. Since there were six comparisons, p-values were multiplied by six (Bonferroni correction) to account for multiple testing.
Results
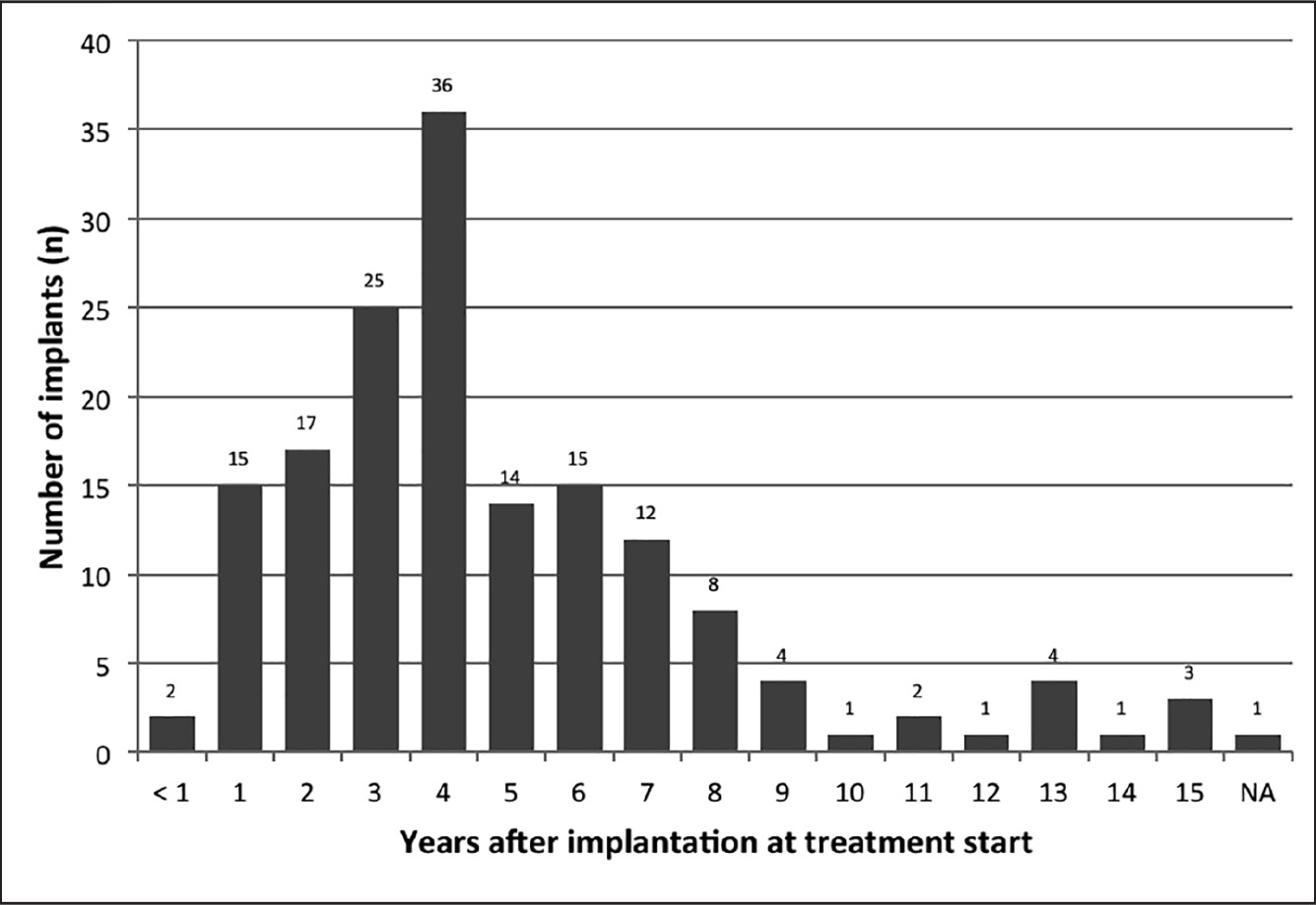
Time after implantation in years at start of periimplantitis therapy. (NA = unknown; n = 158).Figs. 3a & b
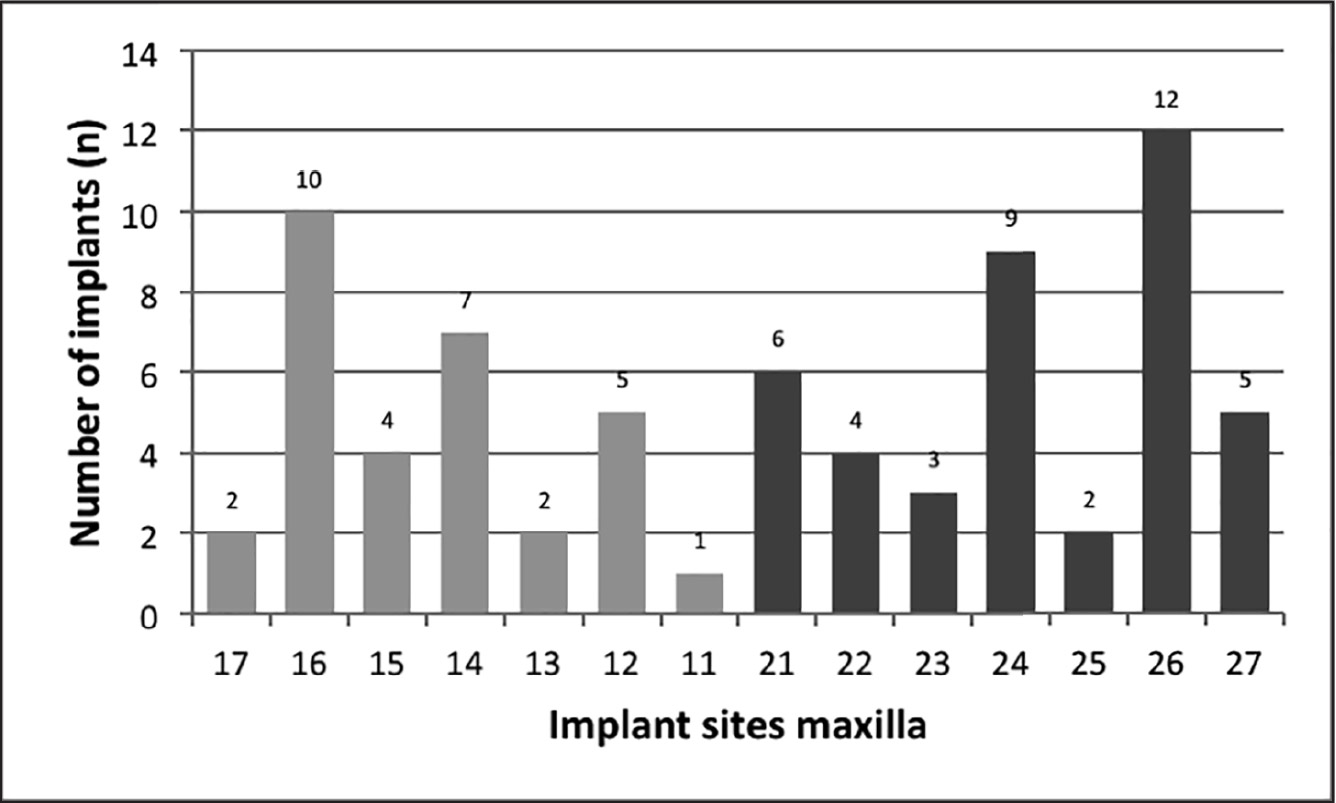
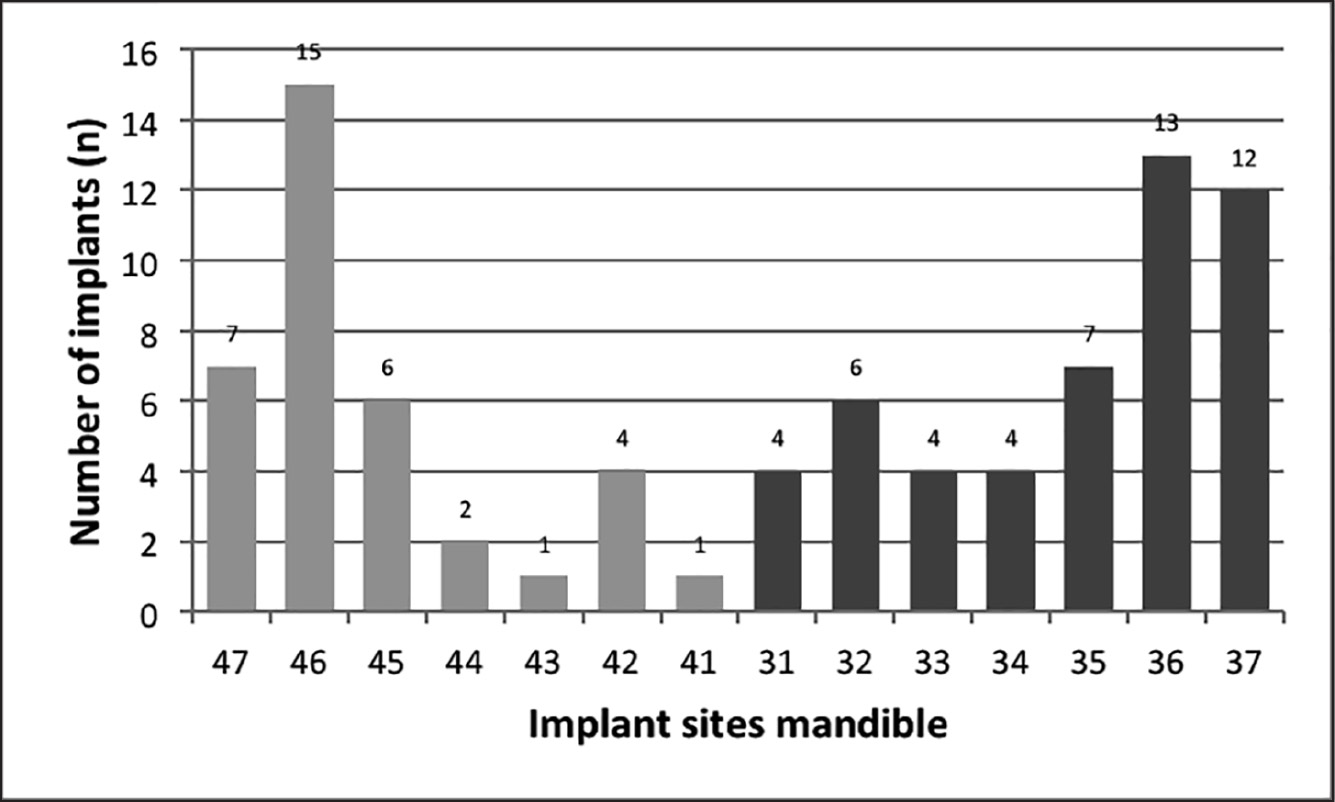
Number of affected implants per site: (a) maxilla (b) mandible. (n = 158).
Between 1993 and 2014, a total of 22,724 implants were inserted in 9,429 patients in our practice and patients were then referred back to their prosthodontists or treating dentists for prostheses. During the observation period of our evaluation (2009–2015), 516 of those patients with a total of 637 implants were referred back to our practice owing to periimplantitis. Of these, 471 implants were deemed hopeless and extracted immediately (73.9%). Eight implants for which periimplantitis therapy was planned had to be extracted at the start of the treatment phase. Thus, periimplantitis therapy was initiated for 158 implants in 107 patients (24.8%). Analysis of the original patient files established that cemented reconstructions were used in 128 implants (77.6%) and screw-retained reconstructions in 37 implants (22.4%). The 158 implants had been in place for nine months to 15 years (Fig. 2). Most of the periimplantitis infections had occurred within the first five years after implant insertion (108 implants; 68.4%). In one implant, this period was retrospectively not clearly determinable. Seventy-two implants treated with periimplantitis therapy were located in the maxilla (45.6%) and 86 in the mandible (54.4%). The distribution of the implantation sites is shown in Figures 3a and b. Before the observation period of our evaluation, 17 implants had been explanted owing to periimplantitis and replaced (10.8%). The newly inserted implants developed periimplantitis again.
Of the patients referred back to our practice and treated for periimplantitis, 41 were male (38.3%) and 66 were female (61.7%). The mean age of the 107 patients at the start of the periimplantitis therapy was 58 ± 11 (23–85) years. At the time of implantation, 18 of the 107 patients were smokers (16.8%), three had received bisphosphonate treatment (3.80%), five had diabetes mellitus (4.67%) and 81 did present any conspicuous medical findings (75.7%), based on the original patient files. The following prosthetic deficiencies of the implants were identified in 25 of the 107 patients (36%): formation of marginal gaps, overcontouring, overload, insufficient biological width, unnecessary splinting and cement residue.
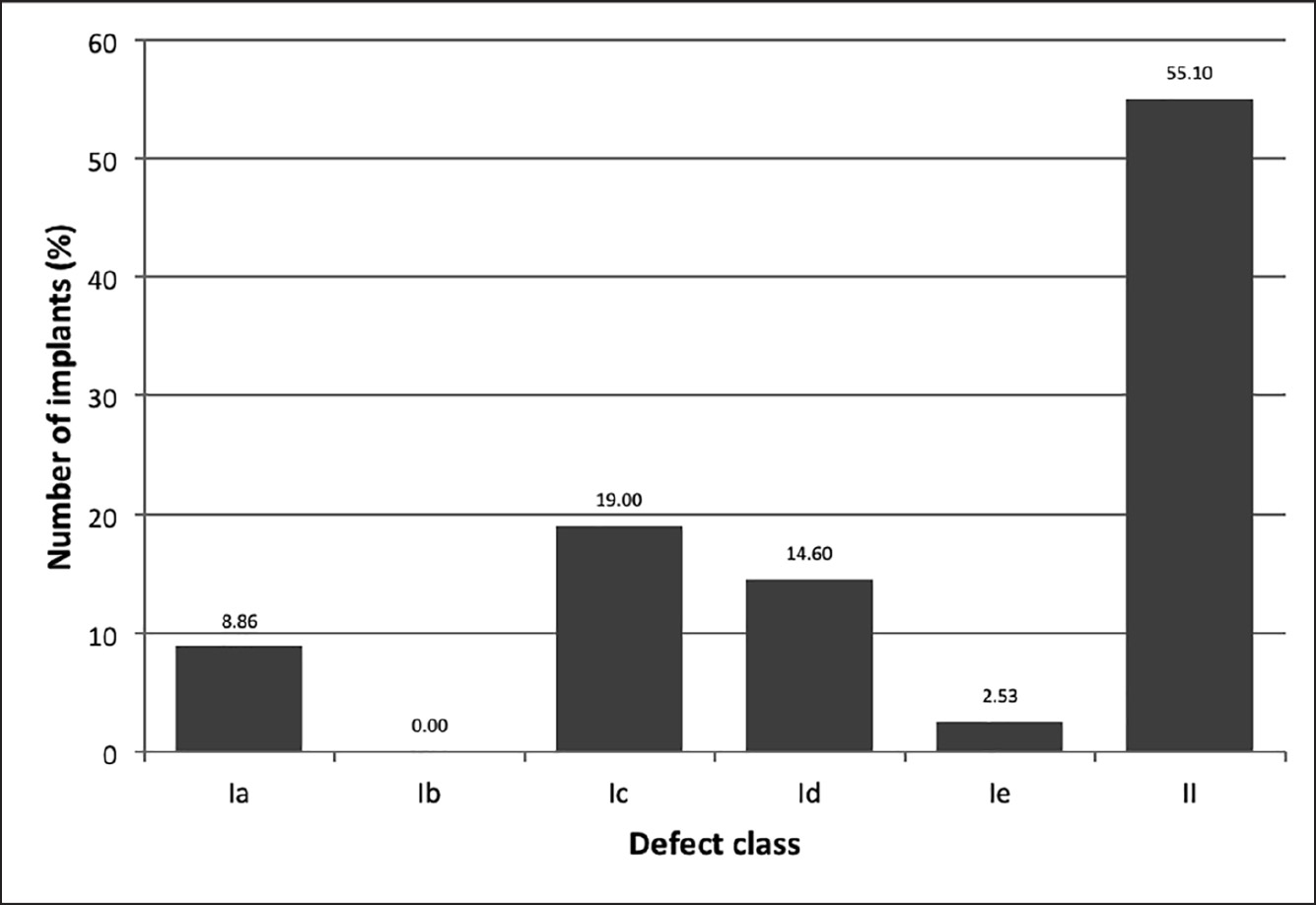
Defect classes at the start of periimplantitis therapy according to Schwarz et al.23Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs.
→ Clin Oral Implants Res. 2007 Apr;18(2):161–70.24Schwarz F, Sahm N, Becker J. Impact of the outcome of guided bone regeneration in dehiscence-type defects on the long-term stability of peri-implant health: clinical observations at 4 years.
→ Clin Oral Implants Res. 2012 Feb;23(2):191–6.
In 52 of the 107 patients (48.6%), generalized periodontitis was diagnosed for 79 implants (50.0%) and treated accordingly. The distribution of the periimplantitis defect classes is shown in Figure 4. In 45 implants (28.5%), the therapy included GBR using a DBBM and an NBCM. The remaining 113 implants underwent professional tooth cleaning and were treated according to the implantoplasty protocol. At the start of the periimplantitis therapy, the BOP of the 158 implants was 100.0% and the plaque index was on average 48.5 ± 26.6% (n = 88).
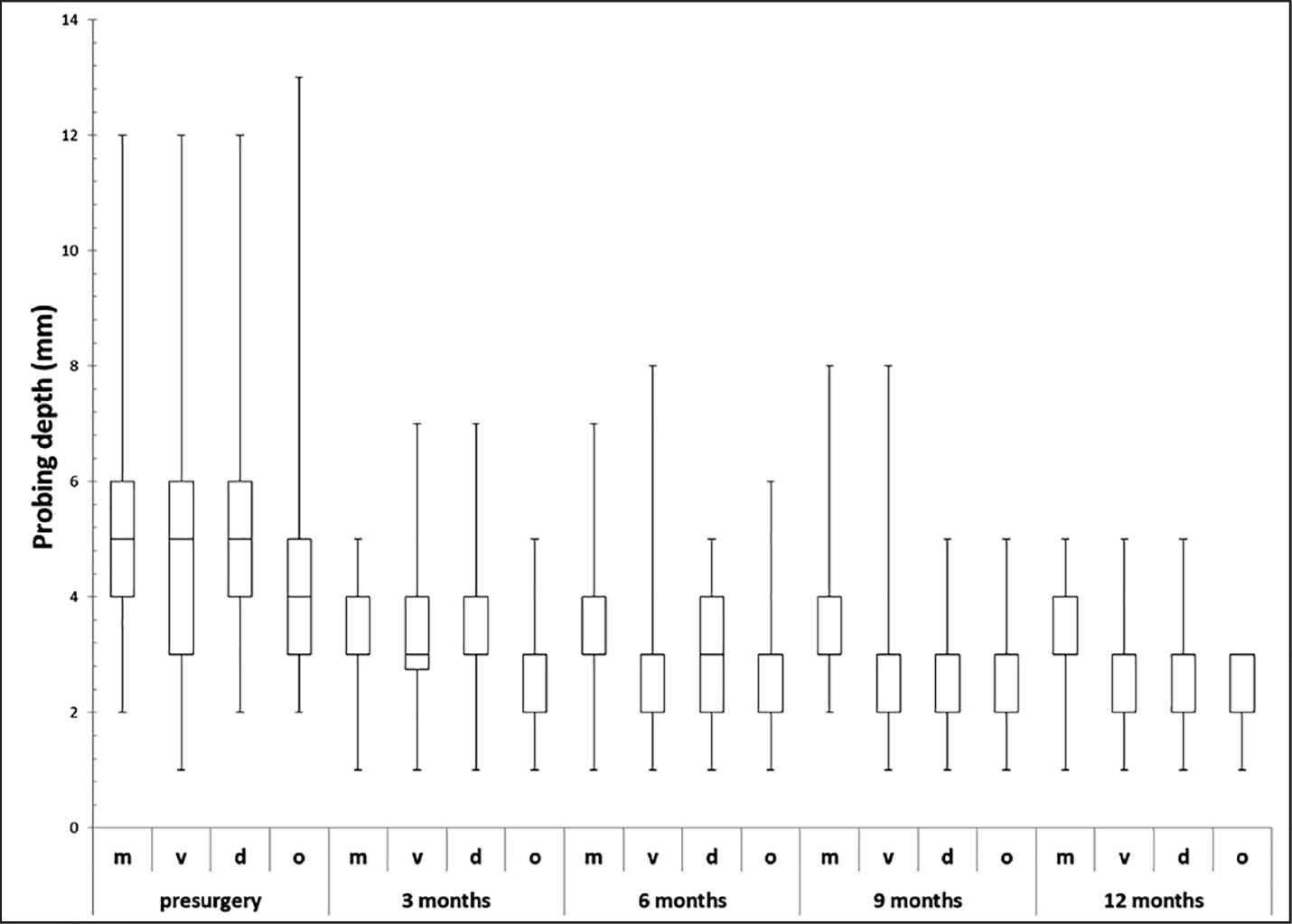
(a) Box plot of pocket depth preoperatively and three, six, nine and 12 months after the start of periimplantitis therapy. (m = mesial; v = vestibular; d = distal; o = oral; n = 123–158).
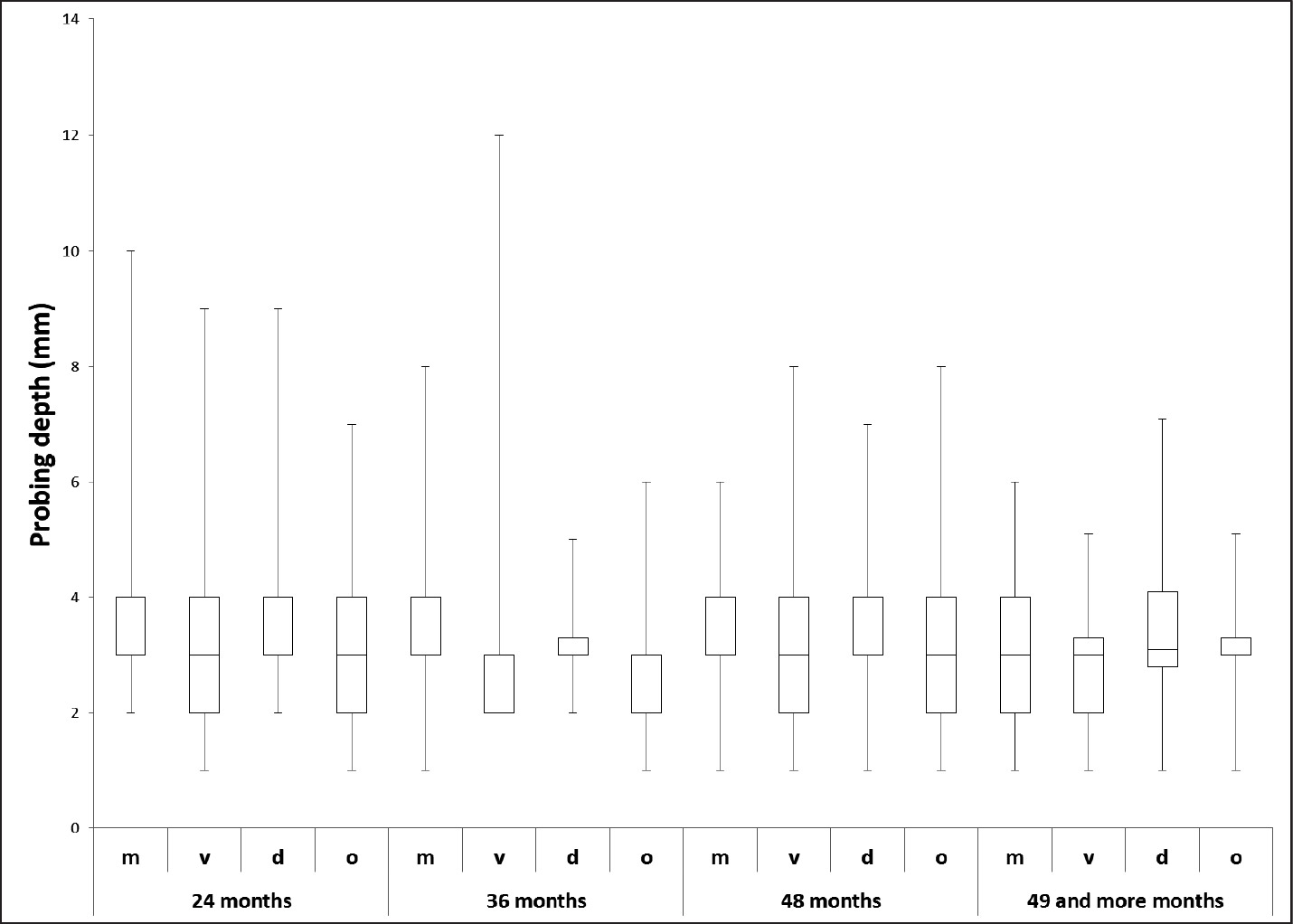
(b) Box plot of pocket depth after 24, 36, 48, and 49 and more months after the start of periimplantitis therapy. (m = mesial; v = vestibular; d = distal; o = oral; n = 16–158).
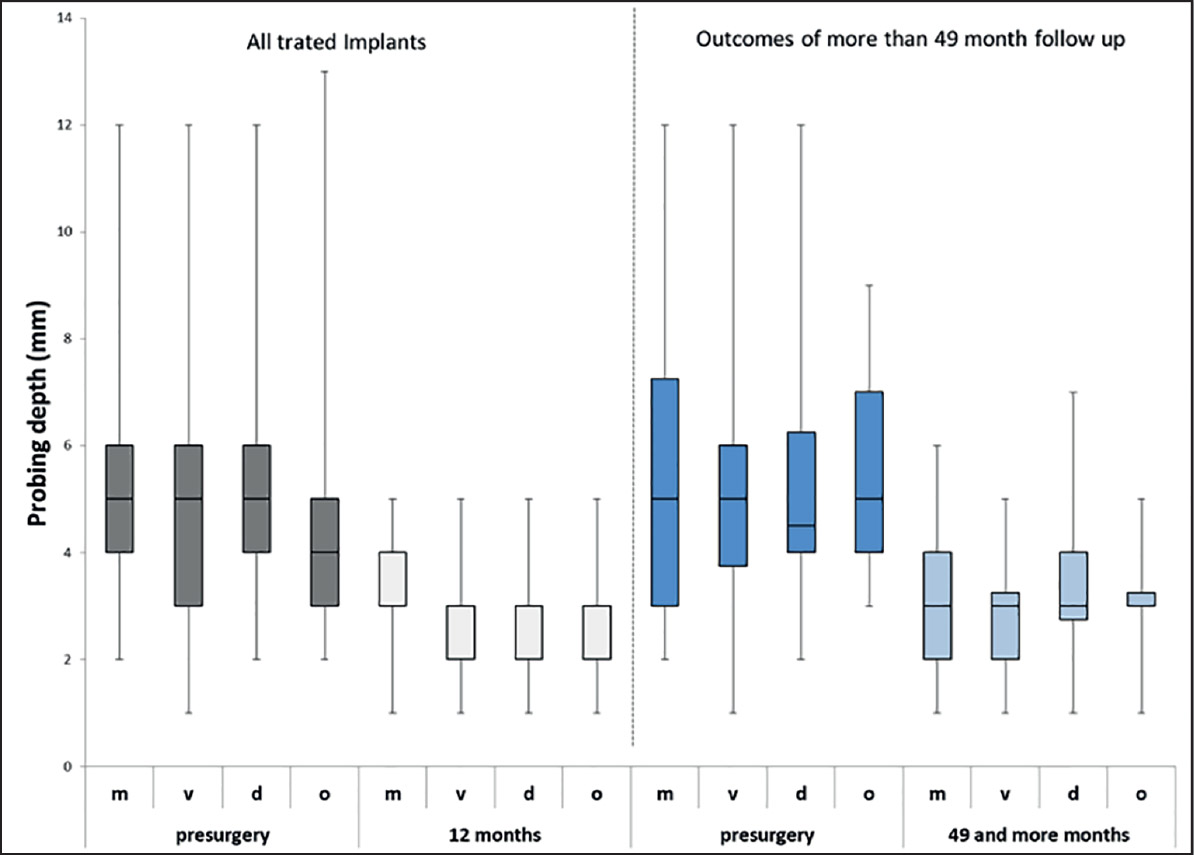
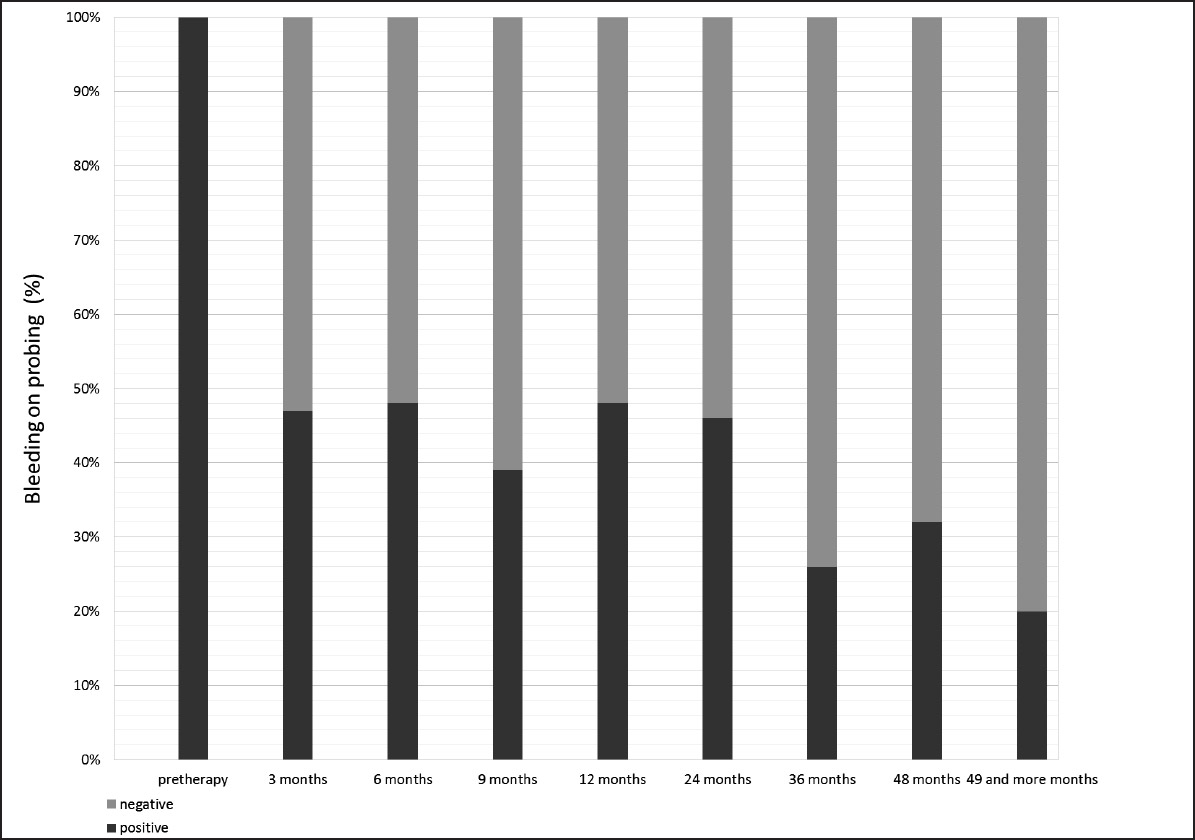
After initiation of the periimplantitis therapy, the mean vestibular PPD of the 158 implants was reduced from 4.93 ± 1.94 mm to 2.67 ± 0.88 mm after 12 months (n = 123) and 2.71 ± 0.30 mm after 49–56 months (n = 32; Figs. 5a & b), therefore on average below the level stated for the definition of periimplantitis.9 Stable PPD reduction was also found for implants with long-term follow-up data 49–56 months post-therapy (Fig. 6). BOP was absent in 50.0% of 58 analyzed implants at 12 months after the periimplantitis therapy and in 73.1% of 26 implants evaluated with long-term data available 49–56 months post-therapy (Fig. 7).
During the follow-up period, one treated implant had to undergo additional gingivectomy and eight repeated implantoplasties. Despite treatment, 15 implants had to be explanted during the follow-up period (9.49%), three of these in patients with diabetes, one in a smoker and two in which the therapy included an intraosseous defect treatment.
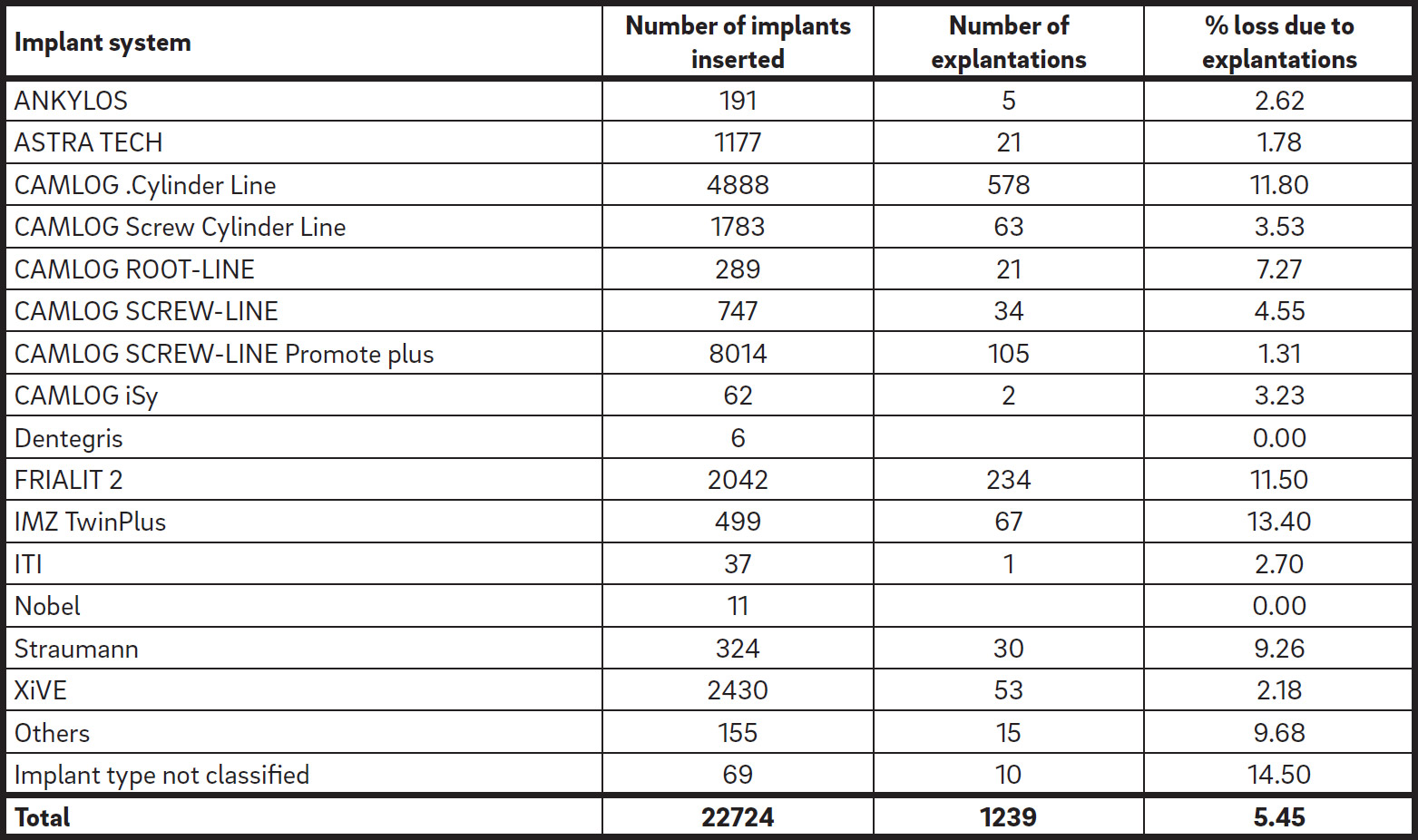
Distribution of implant systems: overall inserted implants and implants affected by periimplantitis between 1993 to 2014.
Evaluation of the original data files for the 158 treated implants established that bone augmentation procedures using a DBBM and an NBCM had been performed in 20 implants (12.7%) before or simultaneously with the implantation. Autologous bone had been used additionally for one of these. No initial augmentation had been performed in 127 implants (80.4%), while this information was not available for 11 implants (6.96%). The augmentation rate of all 22,724 implants inserted between 1993 and 2014 was 31%. In an additional subanalysis, for all 22,724 implants, the explantation rate was evaluated per implant system (Table 1). Of these, 1,239 implants were explanted owing to periimplantitis (5.45%). The highest rates of explantations were noted for the CAMLOG
Cylinder Line, FRIALIT 2 and IMZ TwinPlus.
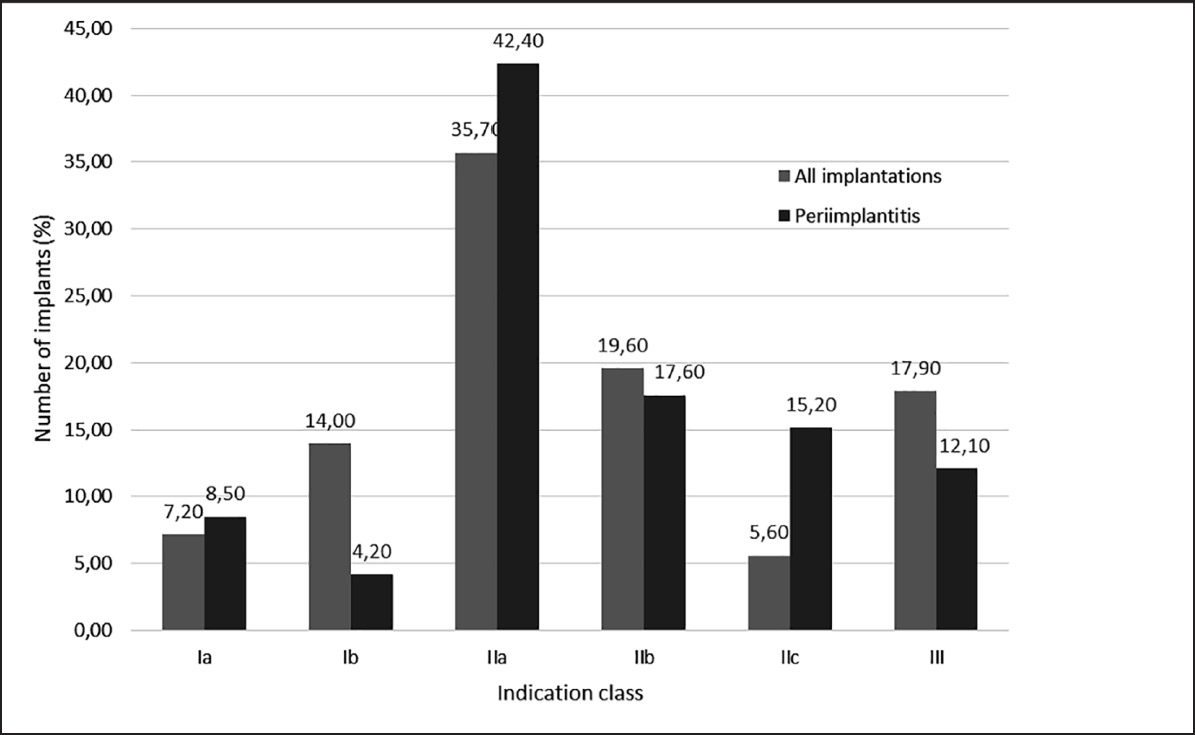
Distribution per indication class at the time of implantation for implants treated for periimplantitis compared with all inserted implants. (All implants: n = 22,724; periimplantitis-affected implants: n = 158).
Statistical analysis of the null hypothesis of no association between indication class and the need for implant therapy applying the chisquared test yielded a p-value of 0.0056. Thus, at the 5% level of significance, the hypothesis of no differences across indication classes with respect to the need for periimplantitis therapy might be withdrawn. Comparing the implant indication classes between all 22,724 implants and the 158 implants that underwent periimplantitis therapy, free-end situations (indication Class IIb) tended to be more frequent in the periimplantitis group (p = 0.07), while interdental spaces (indication Class IIa) were significantly less frequent (p = 0.02). The frequencies of all other indication classes were not significantly different between all inserted implants and implants that underwent periimplantitis therapy (Fig. 8). However, in 2,728 of all 22,724 inserted implants (12%), the indication class could not be evaluated retrospectively.
Discussion
The retrospective evaluation presented here focused on the treatment of patients with implants placed between 1993 and 2014 in our practice and later treated again owing to periimplantitis. Of the implants that received periimplantitis therapy with or without GBR, treatment was successful in terms of stable reduction in PPD and BOP and implant survival of 90.5%, as only 15 of the 158 implants had to be extracted despite periimplantitis therapy over the observation period of our evaluation.
Our findings are in accordance with several reviews reporting successful surgical therapy of periimplantitis despite disease progression or recurrence.25Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review.
→ Int J Oral Maxillofac Implants. 2014;29 Suppl:325–45.26Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis.
→ Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94.27Chan HL, Lin GH, Suarez F, MacEachern M, Wang HL. Surgical management of peri-implantitis: a systematic review and meta-analysis of treatment outcomes.
→ J Periodontol. 2014 Aug;85(8):1027–41.28Figuero E, Graziani F, Sanz I, Herrera D, Sanz M. Management of peri-implant mucositis and peri-implantitis.
→ Periodontol 2000. 2014 Oct;66(1):255–73. A recent meta-analysis compared the results for PPD reduction and radiographic bone fill for different surgical approaches. 29Chan HL, Lin GH, Suarez F, MacEachern M, Wang HL. Surgical management of peri-implantitis: a systematic review and meta-analysis of treatment outcomes.
→ J Periodontol. 2014 Aug;85(8):1027–41. Greater PPD reduction and radiographic bone fill were found when grafting materials and membranes were applied compared with procedures that used access flaps, debridement and resection. In another meta-analysis, greater PPD reduction and gain of clinical attachment were found when bone grafts and membranes were applied compared with a nonsurgical therapy. 30Faggion CM Jr, Chambrone L, Listl S, Tu YK. Network meta-analysis for evaluating interventions in implant dentistry: the case of peri-implantitis treatment.
→ Clin Implant Dent Relat Res. 2013 Aug;15(4):576–88. However, regenerative therapy has been shown to be more effective in contained, circumferential intrabony defects than in defects with buccal dehiscences or a predominantly suprabony component.31Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis.
→ J Clin Periodontol. 2010 May;37(5):449–55. Therefore, in our evaluation, a treatment concept considering defect morphology according to the classification of Schwarz et al. was applied.32Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs.
→ Clin Oral Implants Res. 2007 Apr;18(2):161–70.33Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study.
→ J Clin Periodontol. 2011 Mar;38(3):276–84. Interestingly, 36.1% of the implants with periimplantitis presented with a defect morphology allowing bone augmentation procedures. For financial reasons, in only 28.5% of the implants did periimplantitis therapy include bone augmentation. This included defect Classes Ib, c, d and e. The defect morphology of the remaining implants treated for periimplantitis corresponded to 55.0% Class II and 8.9% Class Ia defects. These defect types were therefore treated by anti-infective, resective therapy only.
For the regenerative treatment of intraosseous defects, we applied a DBBM and an NBCM. Our findings are in accordance with other reports that found encouraging results of periimplantitis treatment using a DBBM with or without an NBCM. In a case series of 51 consecutively treated patients who presented with periimplantitis, Froum et al. used enamel matrix protein, a combination of a platelet-derived growth factor with anorganic bovine bone or mineralized freezedried bone and an NBCM.34Froum SJ, Froum SH, Rosen PS. Successful management of peri-implantitis with a regenerative approach: a consecutive series of 51 treated implants with 3- to 7.5-year follow-up.
→ Int J Periodontics Restorative Dent. 2012 Feb;32(1):11–20. Bone level measured by periapical radiographs or bone sounding increased and remained stable up to 7.5 years after periimplantitis therapy. Positive results in terms of PPD reduction and radiographic bone fill after one year were also found using a DBBM and an NBCM in intrabony defects with a PPD > 5 mm.35Matarasso S, Iorio Siciliano V, Aglietta M, Andreuccetti G, Salvi GE. Clinical and radiographic outcomes of a combined resective and regenerative approach in the treatment of peri-implantitis: a prospective case series.
→ Clin Oral Implants Res. 2014 Jul;25(7):761–7. Using a DBBM, Aghazadeh et al. reported reduced PPD after 12 months and a higher likelihood of radiographic defect fill compared with autogenous bone.36Aghazadeh A, Rutger Persson G, Renvert S. A single-centre randomized controlled clinical trial on the adjunct treatment of intra-bony defects with autogenous bone or a xenograft: results after 12 months.
→ J Clin Periodontol. 2012 Jul;39(7):666–73. In two other studies, a significant defect reduction was achieved using a DBBM in implants with crater-like defects at the one-year follow-up.37Roccuzzo M, Bonino F, Bonino L, Dalmasso P. Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: comparative results of a prospective study on two different implant surfaces.
→ J Clin Periodontol. 2011 Aug;38(8):738–45.38Roccuzzo M, Gaudioso L, Lungo M, Dalmasso P. Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with 10% collagen.
→ J Clin Periodontol. 2016 Mar;43(3):311–8. These results, together with the data of our retrospective evaluation, demonstrate that periimplantitis treatment using a DBBM and an NBCM in defects with suitable defect morphologies may be clinically effective.
In our retrospective evaluation, only a quarter of the implants affected by periimplantitis underwent therapy while all other implants were regarded as hopeless and explanted. We support recommendations of other authors to include patients with implants in a strict maintenance program 39Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review.
→ Int J Oral Maxillofac Implants. 2014;29 Suppl:325–45.40Heitz-Mayfield LJ, Needleman I, Salvi GE, Pjetursson BE. Consensus statements and clinical recommendations for prevention and management of biologic and technical implant complications.
→ Int J Oral Maxillofac Implants. 2014;29 Suppl:346–50. as poor oral hygiene is a well-known risk factor for periimplantitis.41Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. However, this was probably not ensured in many of the cases included in our evaluation, as almost half of the patients presented with generalized periodontitis at the start of the periimplantitis treatment. Therefore, periimplantitis may have proceeded in many implants to a stage that required explantation. In fact, a recent analysis demonstrated that implants provided with prostheses delivered by general practitioners were at higher risk of moderate and severe periimplantitis.42Derks J, Schaller D, Hakansson J, Wennstrom JL, Tomasi C, Berglundh T. Effectiveness of implant therapy analyzed in a Swedish population: prevalence of peri-implantitis.
→ J Dent Res. 2016 Jan;95(1):43–9. Dentists who follow up on implant patients should be sensitized and should be instructed to establish strict maintenance programs according to consensus statements, especially regarding diagnosis of mucositis. Regular clinical monitoring with professional plaque removal and reinforcement of oral hygiene may also have been a main factor of the long-term success of the 158 implants that received periimplantitis therapy in our evaluation.
Simultaneous bone augmentation procedures at the time of implantation may bear higher risk of periimplantitis.43Karbach J, Callaway A, Kwon YD, d’Hoedt B, Al-Nawas B. Comparison of five parameters as risk factors for peri-mucositis.
→ Int J Oral Maxillofac Implants. 2009 May-Jun;24(3):491–6.44Canullo L, Tallarico M, Radovanovic S, Delibasic B, Covani U, Rakic M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered peri-implantitis.
→ Clin Oral Implants Res. 2016 Oct;27(10):1243–50. The results of our retrospective evaluation, however, established that only 12.7% of the implants that received periimplantitis therapy had initially been inserted together with bone augmentation. Bone augmentation in all 22,724 inserted implants was 31%. The results indicate that implants in augmented sites are not more susceptible to periimplant infection than implants inserted without bone augmentation. Nevertheless, clear conclusions must first be drawn in clinical studies including both hopeless implants and implants suitable for periimplantitis therapy.
Various clinical studies have found smokers to be at higher risk of developing periimplant infections.45Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5.46Turri A, Rossetti PH, Canullo L, Grusovin MG, Dahlin C. Prevalence of peri-implantitis in medically compromised patients and smokers: a systematic review.
→ Int J Oral Maxillofac Implants. 2016 Jan-Feb;31(1):111–8. A meta-analysis by Atieh et al. found a significantly higher frequency of periimplant disease in smokers (36%).47Atieh MA, Alsabeeha NH, Faggion CM Jr, uncan WJ. The frequency of peri-implant diseases: a systematic review and meta-analysis.
→ J Periodontol. 2013 Nov;84(11):1586–98. This is in accordance with the results of our retrospective evaluation, in which 16.8% of the patients who underwent periimplantitis therapy were smokers and 16.7% of the smokers had already undergone explantation and re-implantation previously. Uncontrolled diabetes and the intake of bisphosphonates are two additional risk factors for periimplantitis.48Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5.49Turri A, Rossetti PH, Canullo L, Grusovin MG, Dahlin C. Prevalence of peri-implantitis in medically compromised patients and smokers: a systematic review.
→ Int J Oral Maxillofac Implants. 2016 Jan-Feb;31(1):111–8. In our retrospective evaluation, 4.67% of the patients were diabetic and 3.80% received bisphosphonates at the time of implantation. Lindhe et al. demonstrated that 5% of the patients that had undergone periimplantitis therapy and 23% of the patients in which explantations were performed despite the therapy had diabetes.50Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. These results support the conclusion that implant patients with diabetes are at higher risk and should be informed accordingly. Similarly, bisphosphonates have been found to increase the risk of implant failure due to impaired implant osseointegration. However, a review has shown that successful long-term results of implant therapy can be achieved in patients despite bisphosphonate intake.((Javed F, Almas K. Osseointegration of dental implants in patients undergoing bisphosphonate treatment: a literature review.
→ J Periodontol. 2010 Apr;81(4):479–84. Our retrospective evaluation, however, does not provide a clear conclusion for negative effects of bisphosphonate intake or diabetes mellitus on the long-term survival of implants.
In an additional subanalysis, the overall explantation rate of implants placed between 1993 and 2014 was calculated to be 5.45%. Three implant systems presented with a failure rate of more than 10%. However, the number of periimplantitis patients who were not referred back and treated elsewhere is not known. Therefore, the analysis does not allow for definitive conclusions of the prevalence of periimplantitis affecting implants inserted in our practice.
Conclusion
In our retrospective evaluation, data from patients who were referred for periimplantitis treatment were analyzed. Using a treatment approach that included a hygiene phase and that considered defect morphology, PPD and BOP were improved and remained stable over more than four years post-therapy. Retreatments or explantations may be necessary and should be considered part of periimplantitis therapy. The results of our evaluation demonstrated that periimplantitis can be treated successfully and with good long-term results if a treatment approach is chosen based on defect morphology and on consensus recommendations and if patients are enrolled in a strict maintenance program. However, owing to the retrospective character of this evaluation, it is recommended that scientifically sound clinical trials be performed to further evaluate the efficacy of the periimplantitis treatment described here.
Competing interests
The expenses for statistical data analysis and description were covered by Geistlich Pharma, Wolhusen, Switzerland. Other than that, the authors declare that they have no competing interests.
References
| 1, 2. | ↑ | Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant diseases. → J Clin Periodontol. 2008 Sep;35(8 Suppl):286–91. |
| 3. | ↑ | Atieh MA, Alsabeeha NH, Faggion CM Jr, uncan WJ. The frequency of peri-implant diseases: a systematic review and meta-analysis. → J Periodontol. 2013 Nov;84(11):1586–98. |
| 4. | ↑ | Mombelli A, Muller N, Cionca N. The epidemiology of peri-implantitis. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:67–76. |
| 5. | ↑ | Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. → J Clin Periodontol. 2015 Apr;42 Suppl 16:S158–71. |
| 6. | ↑ | American Academy of Periodontology. Peri-implant mucositis and periimplantitis: a current understanding of their diagnoses and clinical implications. → J Periodontol. 2013 Apr;84(4):436–43. |
| 7. | ↑ | Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. |
| 8. | ↑ | Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:325–45. |
| 9. | ↑ | Heitz-Mayfield LJ, Needleman I, Salvi GE, Pjetursson BE. Consensus statements and clinical recommendations for prevention and management of biologic and technical implant complications. → Int J Oral Maxillofac Implants. 2014;29 Suppl:346–50. |
| 10. | ↑ | Meyle J. Mechanical, chemical and laser treatments of the implant surface in the presence of marginal bone loss around implants. → Eur J Oral Implantol. 2012;5 Suppl:S71–81. |
| 11. | ↑ | Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94. |
| 12. | ↑ | Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. → J Clin Periodontol. 2010 May;37(5):449–55. |
| 13, 14. | ↑ | Roccuzzo M, Bonino F, Bonino L, Dalmasso P. Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: comparative results of a prospective study on two different implant surfaces. → J Clin Periodontol. 2011 Aug;38(8):738–45. |
| 15. | ↑ | Aghazadeh A, Rutger Persson G, Renvert S. A single-centre randomized controlled clinical trial on the adjunct treatment of intra-bony defects with autogenous bone or a xenograft: results after 12 months. → J Clin Periodontol. 2012 Jul;39(7):666–73.)((Froum SJ, Froum SH, Rosen PS. Successful management of peri-implantitis with a regenerative approach: a consecutive series of 51 treated implants with 3- to 7.5-year follow-up. → Int J Periodontics Restorative Dent. 2012 Feb;32(1):11–20. |
| 16. | ↑ | Froum SJ, Froum SH, Rosen PS. Successful management of peri-implantitis with a regenerative approach: a consecutive series of 51 treated implants with 3- to 7.5-year follow-up. → Int J Periodontics Restorative Dent. 2012 Feb;32(1):11–20.((Matarasso S, Iorio Siciliano V, Aglietta M, Andreuccetti G, Salvi GE. Clinical and radiographic outcomes of a combined resective and regenerative approach in the treatment of peri-implantitis: a prospective case series. → Clin Oral Implants Res. 2014 Jul;25(7):761–7. |
| 17. | ↑ | Matarasso S, Iorio Siciliano V, Aglietta M, Andreuccetti G, Salvi GE. Clinical and radiographic outcomes of a combined resective and regenerative approach in the treatment of peri-implantitis: a prospective case series. → Clin Oral Implants Res. 2014 Jul;25(7):761–7.((Roccuzzo M, Gaudioso L, Lungo M, Dalmasso P. Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with 10% collagen. → J Clin Periodontol. 2016 Mar;43(3):311–8. |
| 18. | ↑ | Roccuzzo M, Gaudioso L, Lungo M, Dalmasso P. Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with 10% collagen. → J Clin Periodontol. 2016 Mar;43(3):311–8. The aim of our retrospective evaluation was to analyze the efficacy of the periimplantitis treatment with or without bone augmentation in patients over a long-term observation period up to five years post-therapy. Materials and methodsStudy populationThe retrospective evaluation included 107 patients with 158 implants that were treated for periimplantitis between 2009 and 2015. Implants had been inserted between 1993 and 2014 by the same surgeon (JUW) according to the manufacturers’ instructions. Implant systems included Steri-Oss (Nobel Biocare, Zurich, Switzerland), CAMLOG implant system (Cylinder Line, Screw Cylinder Line, Root-Line, SCREW-LINE, SCREW-LINE Promote plus, iSy, CAMLOG Biotechnologies, Basel, Switzerland), ITI and Straumann implants (Straumann, Basel, Switzerland), FRIALIT 2 (Dentsply Sirona, Mannheim, Germany), XiVE (Dentsply Sirona), ASTRA TECH OsseoSpeed (Dentsply Sirona), IMZ Twin- Plus (Dentsply Sirona) and ANKYLOS (Dentsply Sirona). If necessary, bone augmentation procedures were performed before or during the implantation. After completion of the healing phase, the patients were referred back to their dentists or prosthodontists for further prosthetic treatment and follow-up. Later on, some of those patients were referred to our practice again because of periimplantitis. TherapyFig. 1 Defect classes and treatment protocol according to Schwarz et al.((Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. → Clin Oral Implants Res. 2007 Apr;18(2):161–70. |
| 19. | ↑ | Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. → Clin Oral Implants Res. 2007 Apr;18(2):161–70.((Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study. → J Clin Periodontol. 2011 Mar;38(3):276–84. |
| 20. | ↑ | Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study. → J Clin Periodontol. 2011 Mar;38(3):276–84. Ia (buccal vertical bone dehiscence), Ib (buccal dehiscence and semicircular bone defect to the middle of the implant body), Ic (buccal dehiscence, circular bone defect, maintained lingual solid bone), Id (buccal and lingual dehiscence defects), Ie (circular bone resorption, buccal and oral compacta maintained), II (supra-alveolar circumferential bone loss). Before periimplantitis treatment, clinical and radiographic evaluation took place. In the case of acute inflammation, anti-inflammatories were locally applied. Patients underwent professional tooth cleaning and periodontal therapy in the case of generalized periodontitis. Periimplantitis was classified and treated in accordance with Schwarz et al. (Fig. 1).((Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. |
| 21. | ↑ | Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. → Clin Oral Implants Res. 2007 Apr;18(2):161–70.((Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study. → J Clin Periodontol. 2011 Mar;38(3):276–84. |
| 22. | ↑ | Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study. → J Clin Periodontol. 2011 Mar;38(3):276–84. After exposing the defects and removing granulation tissue, implantoplasty was performed using diamonds rotary instruments and Arkansas stones finishing burs. Defects were cleaned with sterile saline. Intraosseous defects (defect Classes Ib, c, d and e; Fig. 1) were augmented according to the treatment protocol using a DBBM (Geistlich Bio-Oss spongiosa granules, Geistlich Pharma, Wolhusen, Switzerland) and an NBCM (Geistlich Bio-Gide Perio, Geistlich Pharma). The surgical area was carefully closed, a periodontal wound dressing applied (Coe-Pak, GC Europe, Leuven, Belgium) and a radiographic evaluation performed. Patients were advised to rinse cautiously with chlorhexamed 0.2% (GSK, London, U.K.) from the first day postsurgery for one week. Antibiotics were given at the discretion of the surgeon starting 24 h before surgery until suture removal eight days postsurgery. Patients were followed up according to a strict recall schedule in our practice. If necessary, supplementary therapy, such as gingivectomy or implantoplasty, was performed during the follow-up phase.
Fig. 1
AnalysisBoth hopeless implants extracted before the periimplantitis therapy and implants treated by a different dentist with incomplete data were not included in our evaluation. Data for the clinical evaluation were retrieved retrospectively from the patient files in our practice and included plaque index, full-mouth bleeding on probing (BOP) and probing pocket depth (PPD). PPD was measured from the mucosal margin to the bottom of the probeable pocket mesially, distally, orally and vestibularly at the start of the periimplantitis therapy and during recall visits in our practice at 3, 6, 9, 12, 24, 36, 48 and 49 to 56 months. In order to evaluate possible risk factors for periimplantitis, signs of prosthetic deficiencies at the start of the therapy were analyzed, as was history of periimplantitis. Additionally, patient files were analyzed to identify smoking, bisphosphonate intake and diabetic patients at the time of implantation. In order to analyze the prevalence of periimplantitis per indication, implants were allocated to one of the following indication classes as defined at the consensus conference of the BDIZ EDI, DGI, DGMKG, DGZI and BDO (national German dental associations) on Oct. 8, 2014:
In an additional subanalysis, implants inserted between 1993 and 2014 were evaluated for primary indication classes and the rate of explantations. Statistic alanalysisThe following exploratory tests were performed:
ResultsFig. 2
Time after implantation in years at start of periimplantitis therapy. (NA = unknown; n = 158).Figs. 3a & b Number of affected implants per site: (a) maxilla (b) mandible. (n = 158). Between 1993 and 2014, a total of 22,724 implants were inserted in 9,429 patients in our practice and patients were then referred back to their prosthodontists or treating dentists for prostheses. During the observation period of our evaluation (2009–2015), 516 of those patients with a total of 637 implants were referred back to our practice owing to periimplantitis. Of these, 471 implants were deemed hopeless and extracted immediately (73.9%). Eight implants for which periimplantitis therapy was planned had to be extracted at the start of the treatment phase. Thus, periimplantitis therapy was initiated for 158 implants in 107 patients (24.8%). Analysis of the original patient files established that cemented reconstructions were used in 128 implants (77.6%) and screw-retained reconstructions in 37 implants (22.4%). The 158 implants had been in place for nine months to 15 years (Fig. 2). Most of the periimplantitis infections had occurred within the first five years after implant insertion (108 implants; 68.4%). In one implant, this period was retrospectively not clearly determinable. Seventy-two implants treated with periimplantitis therapy were located in the maxilla (45.6%) and 86 in the mandible (54.4%). The distribution of the implantation sites is shown in Figures 3a and b. Before the observation period of our evaluation, 17 implants had been explanted owing to periimplantitis and replaced (10.8%). The newly inserted implants developed periimplantitis again.
Fig. 2
Fig. 3a
Fig. 3b
Of the patients referred back to our practice and treated for periimplantitis, 41 were male (38.3%) and 66 were female (61.7%). The mean age of the 107 patients at the start of the periimplantitis therapy was 58 ± 11 (23–85) years. At the time of implantation, 18 of the 107 patients were smokers (16.8%), three had received bisphosphonate treatment (3.80%), five had diabetes mellitus (4.67%) and 81 did present any conspicuous medical findings (75.7%), based on the original patient files. The following prosthetic deficiencies of the implants were identified in 25 of the 107 patients (36%): formation of marginal gaps, overcontouring, overload, insufficient biological width, unnecessary splinting and cement residue. Fig. 4 Defect classes at the start of periimplantitis therapy according to Schwarz et al.((Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. → Clin Oral Implants Res. 2007 Apr;18(2):161–70. |
| 23. | ↑ | Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. → Clin Oral Implants Res. 2007 Apr;18(2):161–70.((Schwarz F, Sahm N, Becker J. Impact of the outcome of guided bone regeneration in dehiscence-type defects on the long-term stability of peri-implant health: clinical observations at 4 years. → Clin Oral Implants Res. 2012 Feb;23(2):191–6. |
| 24. | ↑ | Schwarz F, Sahm N, Becker J. Impact of the outcome of guided bone regeneration in dehiscence-type defects on the long-term stability of peri-implant health: clinical observations at 4 years. → Clin Oral Implants Res. 2012 Feb;23(2):191–6. In 52 of the 107 patients (48.6%), generalized periodontitis was diagnosed for 79 implants (50.0%) and treated accordingly. The distribution of the periimplantitis defect classes is shown in Figure 4. In 45 implants (28.5%), the therapy included GBR using a DBBM and an NBCM. The remaining 113 implants underwent professional tooth cleaning and were treated according to the implantoplasty protocol. At the start of the periimplantitis therapy, the BOP of the 158 implants was 100.0% and the plaque index was on average 48.5 ± 26.6% (n = 88).
Fig. 4
Figs. 5a & b
(a) Box plot of pocket depth preoperatively and three, six, nine and 12 months after the start of periimplantitis therapy. (m = mesial; v = vestibular; d = distal; o = oral; n = 123–158). (b) Box plot of pocket depth after 24, 36, 48, and 49 and more months after the start of periimplantitis therapy. (m = mesial; v = vestibular; d = distal; o = oral; n = 16–158). After initiation of the periimplantitis therapy, the mean vestibular PPD of the 158 implants was reduced from 4.93 ± 1.94 mm to 2.67 ± 0.88 mm after 12 months (n = 123) and 2.71 ± 0.30 mm after 49–56 months (n = 32; Figs. 5a & b), therefore on average below the level stated for the definition of periimplantitis.9 Stable PPD reduction was also found for implants with long-term follow-up data 49–56 months post-therapy (Fig. 6). BOP was absent in 50.0% of 58 analyzed implants at 12 months after the periimplantitis therapy and in 73.1% of 26 implants evaluated with long-term data available 49–56 months post-therapy (Fig. 7). During the follow-up period, one treated implant had to undergo additional gingivectomy and eight repeated implantoplasties. Despite treatment, 15 implants had to be explanted during the follow-up period (9.49%), three of these in patients with diabetes, one in a smoker and two in which the therapy included an intraosseous defect treatment.
Fig. 5a
Fig. 5b
Fig. 6
Fig. 7
Table 1
Distribution of implant systems: overall inserted implants and implants affected by periimplantitis between 1993 to 2014. Evaluation of the original data files for the 158 treated implants established that bone augmentation procedures using a DBBM and an NBCM had been performed in 20 implants (12.7%) before or simultaneously with the implantation. Autologous bone had been used additionally for one of these. No initial augmentation had been performed in 127 implants (80.4%), while this information was not available for 11 implants (6.96%). The augmentation rate of all 22,724 implants inserted between 1993 and 2014 was 31%. In an additional subanalysis, for all 22,724 implants, the explantation rate was evaluated per implant system (Table 1). Of these, 1,239 implants were explanted owing to periimplantitis (5.45%). The highest rates of explantations were noted for the CAMLOG
Table 1
Fig. 8
Distribution per indication class at the time of implantation for implants treated for periimplantitis compared with all inserted implants. (All implants: n = 22,724; periimplantitis-affected implants: n = 158). Statistical analysis of the null hypothesis of no association between indication class and the need for implant therapy applying the chisquared test yielded a p-value of 0.0056. Thus, at the 5% level of significance, the hypothesis of no differences across indication classes with respect to the need for periimplantitis therapy might be withdrawn. Comparing the implant indication classes between all 22,724 implants and the 158 implants that underwent periimplantitis therapy, free-end situations (indication Class IIb) tended to be more frequent in the periimplantitis group (p = 0.07), while interdental spaces (indication Class IIa) were significantly less frequent (p = 0.02). The frequencies of all other indication classes were not significantly different between all inserted implants and implants that underwent periimplantitis therapy (Fig. 8). However, in 2,728 of all 22,724 inserted implants (12%), the indication class could not be evaluated retrospectively.
Fig. 8
DiscussionThe retrospective evaluation presented here focused on the treatment of patients with implants placed between 1993 and 2014 in our practice and later treated again owing to periimplantitis. Of the implants that received periimplantitis therapy with or without GBR, treatment was successful in terms of stable reduction in PPD and BOP and implant survival of 90.5%, as only 15 of the 158 implants had to be extracted despite periimplantitis therapy over the observation period of our evaluation. Our findings are in accordance with several reviews reporting successful surgical therapy of periimplantitis despite disease progression or recurrence.((Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review. |
| 25. | ↑ | Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:325–45.((Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94. |
| 26. | ↑ | Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94.((Chan HL, Lin GH, Suarez F, MacEachern M, Wang HL. Surgical management of peri-implantitis: a systematic review and meta-analysis of treatment outcomes. → J Periodontol. 2014 Aug;85(8):1027–41. |
| 27. | ↑ | Chan HL, Lin GH, Suarez F, MacEachern M, Wang HL. Surgical management of peri-implantitis: a systematic review and meta-analysis of treatment outcomes. → J Periodontol. 2014 Aug;85(8):1027–41.((Figuero E, Graziani F, Sanz I, Herrera D, Sanz M. Management of peri-implant mucositis and peri-implantitis. → Periodontol 2000. 2014 Oct;66(1):255–73. |
| 28. | ↑ | Figuero E, Graziani F, Sanz I, Herrera D, Sanz M. Management of peri-implant mucositis and peri-implantitis. → Periodontol 2000. 2014 Oct;66(1):255–73. A recent meta-analysis compared the results for PPD reduction and radiographic bone fill for different surgical approaches. ((Chan HL, Lin GH, Suarez F, MacEachern M, Wang HL. Surgical management of peri-implantitis: a systematic review and meta-analysis of treatment outcomes. → J Periodontol. 2014 Aug;85(8):1027–41. |
| 29. | ↑ | Chan HL, Lin GH, Suarez F, MacEachern M, Wang HL. Surgical management of peri-implantitis: a systematic review and meta-analysis of treatment outcomes. → J Periodontol. 2014 Aug;85(8):1027–41. Greater PPD reduction and radiographic bone fill were found when grafting materials and membranes were applied compared with procedures that used access flaps, debridement and resection. In another meta-analysis, greater PPD reduction and gain of clinical attachment were found when bone grafts and membranes were applied compared with a nonsurgical therapy. ((Faggion CM Jr, Chambrone L, Listl S, Tu YK. Network meta-analysis for evaluating interventions in implant dentistry: the case of peri-implantitis treatment. → Clin Implant Dent Relat Res. 2013 Aug;15(4):576–88. |
| 30. | ↑ | Faggion CM Jr, Chambrone L, Listl S, Tu YK. Network meta-analysis for evaluating interventions in implant dentistry: the case of peri-implantitis treatment. → Clin Implant Dent Relat Res. 2013 Aug;15(4):576–88. However, regenerative therapy has been shown to be more effective in contained, circumferential intrabony defects than in defects with buccal dehiscences or a predominantly suprabony component.((Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. → J Clin Periodontol. 2010 May;37(5):449–55. |
| 31. | ↑ | Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. → J Clin Periodontol. 2010 May;37(5):449–55. Therefore, in our evaluation, a treatment concept considering defect morphology according to the classification of Schwarz et al. was applied.((Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. → Clin Oral Implants Res. 2007 Apr;18(2):161–70. |
| 32. | ↑ | Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. → Clin Oral Implants Res. 2007 Apr;18(2):161–70.((Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study. → J Clin Periodontol. 2011 Mar;38(3):276–84. |
| 33. | ↑ | Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study. → J Clin Periodontol. 2011 Mar;38(3):276–84. Interestingly, 36.1% of the implants with periimplantitis presented with a defect morphology allowing bone augmentation procedures. For financial reasons, in only 28.5% of the implants did periimplantitis therapy include bone augmentation. This included defect Classes Ib, c, d and e. The defect morphology of the remaining implants treated for periimplantitis corresponded to 55.0% Class II and 8.9% Class Ia defects. These defect types were therefore treated by anti-infective, resective therapy only. For the regenerative treatment of intraosseous defects, we applied a DBBM and an NBCM. Our findings are in accordance with other reports that found encouraging results of periimplantitis treatment using a DBBM with or without an NBCM. In a case series of 51 consecutively treated patients who presented with periimplantitis, Froum et al. used enamel matrix protein, a combination of a platelet-derived growth factor with anorganic bovine bone or mineralized freezedried bone and an NBCM.((Froum SJ, Froum SH, Rosen PS. Successful management of peri-implantitis with a regenerative approach: a consecutive series of 51 treated implants with 3- to 7.5-year follow-up. |
| 34. | ↑ | Froum SJ, Froum SH, Rosen PS. Successful management of peri-implantitis with a regenerative approach: a consecutive series of 51 treated implants with 3- to 7.5-year follow-up. → Int J Periodontics Restorative Dent. 2012 Feb;32(1):11–20. Bone level measured by periapical radiographs or bone sounding increased and remained stable up to 7.5 years after periimplantitis therapy. Positive results in terms of PPD reduction and radiographic bone fill after one year were also found using a DBBM and an NBCM in intrabony defects with a PPD > 5 mm.((Matarasso S, Iorio Siciliano V, Aglietta M, Andreuccetti G, Salvi GE. Clinical and radiographic outcomes of a combined resective and regenerative approach in the treatment of peri-implantitis: a prospective case series. → Clin Oral Implants Res. 2014 Jul;25(7):761–7. |
| 35. | ↑ | Matarasso S, Iorio Siciliano V, Aglietta M, Andreuccetti G, Salvi GE. Clinical and radiographic outcomes of a combined resective and regenerative approach in the treatment of peri-implantitis: a prospective case series. → Clin Oral Implants Res. 2014 Jul;25(7):761–7. Using a DBBM, Aghazadeh et al. reported reduced PPD after 12 months and a higher likelihood of radiographic defect fill compared with autogenous bone.((Aghazadeh A, Rutger Persson G, Renvert S. A single-centre randomized controlled clinical trial on the adjunct treatment of intra-bony defects with autogenous bone or a xenograft: results after 12 months. → J Clin Periodontol. 2012 Jul;39(7):666–73. |
| 36. | ↑ | Aghazadeh A, Rutger Persson G, Renvert S. A single-centre randomized controlled clinical trial on the adjunct treatment of intra-bony defects with autogenous bone or a xenograft: results after 12 months. → J Clin Periodontol. 2012 Jul;39(7):666–73. In two other studies, a significant defect reduction was achieved using a DBBM in implants with crater-like defects at the one-year follow-up.((Roccuzzo M, Bonino F, Bonino L, Dalmasso P. Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: comparative results of a prospective study on two different implant surfaces. → J Clin Periodontol. 2011 Aug;38(8):738–45. |
| 37. | ↑ | Roccuzzo M, Bonino F, Bonino L, Dalmasso P. Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: comparative results of a prospective study on two different implant surfaces. → J Clin Periodontol. 2011 Aug;38(8):738–45.((Roccuzzo M, Gaudioso L, Lungo M, Dalmasso P. Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with 10% collagen. → J Clin Periodontol. 2016 Mar;43(3):311–8. |
| 38. | ↑ | Roccuzzo M, Gaudioso L, Lungo M, Dalmasso P. Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with 10% collagen. → J Clin Periodontol. 2016 Mar;43(3):311–8. These results, together with the data of our retrospective evaluation, demonstrate that periimplantitis treatment using a DBBM and an NBCM in defects with suitable defect morphologies may be clinically effective. In our retrospective evaluation, only a quarter of the implants affected by periimplantitis underwent therapy while all other implants were regarded as hopeless and explanted. We support recommendations of other authors to include patients with implants in a strict maintenance program ((Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review. |
| 39. | ↑ | Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:325–45.((Heitz-Mayfield LJ, Needleman I, Salvi GE, Pjetursson BE. Consensus statements and clinical recommendations for prevention and management of biologic and technical implant complications. → Int J Oral Maxillofac Implants. 2014;29 Suppl:346–50. |
| 40. | ↑ | Heitz-Mayfield LJ, Needleman I, Salvi GE, Pjetursson BE. Consensus statements and clinical recommendations for prevention and management of biologic and technical implant complications. → Int J Oral Maxillofac Implants. 2014;29 Suppl:346–50. as poor oral hygiene is a well-known risk factor for periimplantitis.((Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. |
| 41. | ↑ | Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. However, this was probably not ensured in many of the cases included in our evaluation, as almost half of the patients presented with generalized periodontitis at the start of the periimplantitis treatment. Therefore, periimplantitis may have proceeded in many implants to a stage that required explantation. In fact, a recent analysis demonstrated that implants provided with prostheses delivered by general practitioners were at higher risk of moderate and severe periimplantitis.((Derks J, Schaller D, Hakansson J, Wennstrom JL, Tomasi C, Berglundh T. Effectiveness of implant therapy analyzed in a Swedish population: prevalence of peri-implantitis. → J Dent Res. 2016 Jan;95(1):43–9. |
| 42. | ↑ | Derks J, Schaller D, Hakansson J, Wennstrom JL, Tomasi C, Berglundh T. Effectiveness of implant therapy analyzed in a Swedish population: prevalence of peri-implantitis. → J Dent Res. 2016 Jan;95(1):43–9. Dentists who follow up on implant patients should be sensitized and should be instructed to establish strict maintenance programs according to consensus statements, especially regarding diagnosis of mucositis. Regular clinical monitoring with professional plaque removal and reinforcement of oral hygiene may also have been a main factor of the long-term success of the 158 implants that received periimplantitis therapy in our evaluation. Simultaneous bone augmentation procedures at the time of implantation may bear higher risk of periimplantitis.((Karbach J, Callaway A, Kwon YD, d’Hoedt B, Al-Nawas B. Comparison of five parameters as risk factors for peri-mucositis. |
| 43. | ↑ | Karbach J, Callaway A, Kwon YD, d’Hoedt B, Al-Nawas B. Comparison of five parameters as risk factors for peri-mucositis. → Int J Oral Maxillofac Implants. 2009 May-Jun;24(3):491–6.((Canullo L, Tallarico M, Radovanovic S, Delibasic B, Covani U, Rakic M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered peri-implantitis. → Clin Oral Implants Res. 2016 Oct;27(10):1243–50. |
| 44. | ↑ | Canullo L, Tallarico M, Radovanovic S, Delibasic B, Covani U, Rakic M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered peri-implantitis. → Clin Oral Implants Res. 2016 Oct;27(10):1243–50. The results of our retrospective evaluation, however, established that only 12.7% of the implants that received periimplantitis therapy had initially been inserted together with bone augmentation. Bone augmentation in all 22,724 inserted implants was 31%. The results indicate that implants in augmented sites are not more susceptible to periimplant infection than implants inserted without bone augmentation. Nevertheless, clear conclusions must first be drawn in clinical studies including both hopeless implants and implants suitable for periimplantitis therapy. Various clinical studies have found smokers to be at higher risk of developing periimplant infections.((Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. |
| 45. | ↑ | Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5.((Turri A, Rossetti PH, Canullo L, Grusovin MG, Dahlin C. Prevalence of peri-implantitis in medically compromised patients and smokers: a systematic review. → Int J Oral Maxillofac Implants. 2016 Jan-Feb;31(1):111–8. |
| 46. | ↑ | Turri A, Rossetti PH, Canullo L, Grusovin MG, Dahlin C. Prevalence of peri-implantitis in medically compromised patients and smokers: a systematic review. → Int J Oral Maxillofac Implants. 2016 Jan-Feb;31(1):111–8. A meta-analysis by Atieh et al. found a significantly higher frequency of periimplant disease in smokers (36%).((Atieh MA, Alsabeeha NH, Faggion CM Jr, uncan WJ. The frequency of peri-implant diseases: a systematic review and meta-analysis. → J Periodontol. 2013 Nov;84(11):1586–98. |
| 47. | ↑ | Atieh MA, Alsabeeha NH, Faggion CM Jr, uncan WJ. The frequency of peri-implant diseases: a systematic review and meta-analysis. → J Periodontol. 2013 Nov;84(11):1586–98. This is in accordance with the results of our retrospective evaluation, in which 16.8% of the patients who underwent periimplantitis therapy were smokers and 16.7% of the smokers had already undergone explantation and re-implantation previously. Uncontrolled diabetes and the intake of bisphosphonates are two additional risk factors for periimplantitis.((Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. |
| 48. | ↑ | Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5.((Turri A, Rossetti PH, Canullo L, Grusovin MG, Dahlin C. Prevalence of peri-implantitis in medically compromised patients and smokers: a systematic review. → Int J Oral Maxillofac Implants. 2016 Jan-Feb;31(1):111–8. |
| 49. | ↑ | Turri A, Rossetti PH, Canullo L, Grusovin MG, Dahlin C. Prevalence of peri-implantitis in medically compromised patients and smokers: a systematic review. → Int J Oral Maxillofac Implants. 2016 Jan-Feb;31(1):111–8. In our retrospective evaluation, 4.67% of the patients were diabetic and 3.80% received bisphosphonates at the time of implantation. Lindhe et al. demonstrated that 5% of the patients that had undergone periimplantitis therapy and 23% of the patients in which explantations were performed despite the therapy had diabetes.((Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. |
| 50. | ↑ | Lindhe J, Meyle J; Group D of the European Workshop on Periodontology. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. → J Clin Periodontol. 2008 Sep;35(8 Suppl):282–5. These results support the conclusion that implant patients with diabetes are at higher risk and should be informed accordingly. Similarly, bisphosphonates have been found to increase the risk of implant failure due to impaired implant osseointegration. However, a review has shown that successful long-term results of implant therapy can be achieved in patients despite bisphosphonate intake.((Javed F, Almas K. Osseointegration of dental implants in patients undergoing bisphosphonate treatment: a literature review. → J Periodontol. 2010 Apr;81(4):479–84. |





Leave a Reply
Be the First to Comment!