Surgical treatment of circumferential and semicircumferential defects due to periimplantitis: A prospective case series cohort study
January 6, 2017 / Categories: Digital Dentistry, Implant Dentistry

Canullo, Luigi

Peñarrocha Diago, Maria

Pellicer Chover, Hilario

Aloy Prosper, Amparo

Tallarico, Marco

Peñarrocha Oltra, David
Different surgical treatment strategies for periimplantitis using graft material and membranes have been suggested. However, in these, the microbiological aspects of the periimplant environment were underestimated. The present preliminary study was aimed at analyzing a new clinical approach based on disinfection of the implant connection and of the implant surface, as well as the use of only a self-stabilizing graft material in the treatment of circumferential and semicircumferential bony defects resulting from periimplantitis.
Introduction
Different treatment strategies for periimplantitis have been suggested.1Muthukuru M, Zainvi A, Esplugues EO, Flemmig TF. Non-surgical therapy 0for the management of peri-implantitis: a systematic review.
→ Clin Oral Implants Res. 2012 Oct;23 Suppl 6:77–83.3Serino G, Turri A. Outcome of surgical treatment of peri-implantitis: results from a 2-year prospective clinical study in humans.
→ Clin Oral Implants Res. 2011 Nov;22(11):1214–20.2 Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis.
→ Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94.Despite the unesthetic outcomes, the resective approach was considered the only longitudinally effective strategy.4Serino G, Turri A, Lang NP. Maintenance therapy in patients following the surgical treatment of peri-implantitis: a 5-year follow-up study.
→ Clin Oral Implants Res. 2015 Aug;26(8):950–6.
However, nonsurgical (which basically consisted of simple subgingival mechanical debridement with or without systemic or local anti-infective agent delivery) and regenerative approaches were considered ineffective.5Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review.
→ Int J Oral Maxillofac Implants. 2014;29 Suppl:325–45. In fact, despite some positive short-term outcomes that have been reported in many studies,6Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis.
→ Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94.7Schwarz F, Sahm N, Schwarz K, Becker J.Impact of defect configuration on theclinical outcome following surgical regenerative therapy of peri-implantitis.
→ J Clin Periodontol. 2010 May;37(5):449–55. absence of reso lution, as well as progression or recurrence after treatment of disease, leading to the loss of implant, were also highlighted.8Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review.
→ Int J Oral Maxillofac Implants. 2014;29 Suppl:325–45. According to Graziani et al., current literature on periimplant disease prevention and treatment does not provide applicable clinical information.9Graziani F, Figuero E, Herrera D. Systematic review of quality of reporting, outcome measurements and methods to study efficacy of preventive and therapeutic approaches to peri-implant diseases.
→ J Clin Periodontol. 2012 Feb;39 Suppl 12:224–44. In fact, the lack of efficacy of the current methods for treating periimplantitis may be due to insufficient understanding of the entire biological etiology of the disease. Therapy concepts for periodontitis have been directly transferred to periimplant disease treatments, neglecting the differences between teeth and implants that may be highly relevant to periimplantitis treatment concepts. In fact, since implant surface and topology differ dramatically on the micro and macrolevel from tooth structure and shape, conventional bacterial removal and debridement cannot be effective on implants.10Pesce P, Menini M, Tealdo T, Bevilacqua M, Pera F, Pera P. Peri-implantitis: a systematic review of recently published papers.
→ Int J Prosthodont. 2014 Jan-Feb;27(1):15–25. At the same time, since implants always present the opportunity for bacterial contamination at the implant–abutment junction,often positioned at the bone level,11 Canullo L, Penarrocha-Oltra D, Soldini C, Mazzocco F, Penarrocha M, Covani U. Microbiological assessment of the implant-abutment interface in different connections: cross-sectional study after 5 years of functional loading.
→ Clin Oral Implants Res. 2015 Apr;26(4):426–34. Epub 2014 Mar 26. guided bone regeneration techniques or regenerative procedures cannot be successful (at least in the long run) owing to the recontamination of the site through the implant–abutment junction. An additional reason for low surgical outcomes might be the misunderstanding of triggering conditions for the implant disintegration process. In fact, according to Sanz and Chapple, the use of unequivocal case definitions would help in increasing the quality of research on this topic.12Sanz M, Chapple IL; Working Group 4 of the VIII European Workshop on Periodontology. Clinical research on peri-implant diseases: consensus report of Working Group 4.
→ J Clin Periodontol. 2012 Feb;39 Suppl 12:202–6. As it is easy to understand, differences in periimplant environment (soft and hard-tissue conditions, 3-D implant positioning, triggering factor of disease) could completely change the prognosis and give rise to different treatment plans. However, one of the most important factors affecting surgical outcomes, particularly in the case of regenerativeprocedures, appears to be the selection of patients, especially as regards the shape of the bone defect.13Schwarz F, Sahm N, Schwarz K, Becker J.Impact of defect configuration on theclinical outcome following surgical regenerative therapy of peri-implantitis.
→ J Clin Periodontol. 2010 May;37(5):449–55. In fact, self-containing or three-wall bone defects demonstrated a higher clinical and radiographic improvement in terms of bone regeneration.14Schwarz F, Sahm N, Schwarz K, Becker J.Impact of defect configuration on theclinical outcome following surgical regenerative therapy of peri-implantitis.
→ J Clin Periodontol. 2010 May;37(5):449–55.
Circumferential and semicircumferential intrabony defects displayed promising outcomes when treated with the application of a particulate bone material stabilized with a collagen membrane. 15 Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis.
→ Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94.
16Schwarz F, Sahm N, Schwarz K, Becker J.Impact of defect configuration on theclinical outcome following surgical regenerative therapy of peri-implantitis.
→ J Clin Periodontol. 2010 May;37(5):449–55.Besides loose particulate bone materials, alloplastic biomaterials designed to harden in situ are commonly used in dental indications.11 These resorbable materials (GUIDOR easy-graft CLASSIC, Sunstar Suisse, Étoy, Switzerland) are composed of calcium phosphate particles coated with a thin layer of PLGA, enhancing the material handling and forming a stable scaffold for regeneration within the defect site. This in situ hardening PLGA-coated biomaterial has been proven to provide excellent soft-tissue healing after socket grafting and equivalent perfor mance in terms of new bone formation has been found,17Leventis MD, Fairbairn P, Kakar A, Leventis AD, Maragaritis V, Lückerath W, Horowitz RA, Nagursky H. Minimally invasive alveolar ridge preservation utilizing an in situ hardening ?-tricalcium phosphate bone substitute: a multicenter case series.
→ Int J Dent. 2016;2016:5406736. doi:10.1155/2016/5406736. comparable to the results reported for other bovine and synthetic biomaterials.18Cordaro L, Bosshardt DD, Palattella P, Rao W, Serino G, Chiapasco M. Maxillary sinus grafting with Bio-Oss or Straumann Bone Ceramic: histomorphometric results from a randomized controlled multicenter clinical trial.
→ Clin Oral Implants Res. 2008 Aug;19(8):796–803. The aim of the present preliminary prospective study was to test the outcome of a surgical approach to treating periimplant circumferential and semicircumferential defects using only a selfstabilizing graft material.
Materials and methods
In January 2013, at the Department of Oral Surgery, University of Valencia, Valencia, Spain, a preliminary prospective clinical trial was designed to test the efficacy of a self-stabilizing graft material in the treatment of bony defects resulting from periimplantitis. Only those patients who had received implant therapy at the Department of Stomatology in the past, had a good-quality periapical baseline radiograph obtained after prosthetic rehabilitation, attended control visits, were older than 18 years, and presented with a circumferential or semicircumferential periimplant bony defect were included in the study.19Schwarz F, Sahm N, Schwarz K, Becker J.Impact of defect configuration on theclinical outcome following surgical regenerative therapy of peri-implantitis.
→ J Clin Periodontol. 2010 May;37(5):449–55. Exclusion criteria were relevant medical conditions (American Society of Anesthesiologists Physical Status Class III or IV), > 10 cigarettes/day or pipe or cigar smokers, plaque index and bleeding on probing scores > 25%, pregnant or lactating patients, and patients with a history of bisphosphonate therapy (Fig. 1).
The patients were informed about the study and the intervention and asked to sign an informed consent document in order to be involved. The investigation was conducted according to the principles embodied in the Declaration of Helsinki of 1975, as revised in 2013. All of the procedures and materials in the present prospective study were approved by the local ethics committee of the University of Valencia (H1447757419931).
-
- Fig. 1a
-
- Fig. 1b
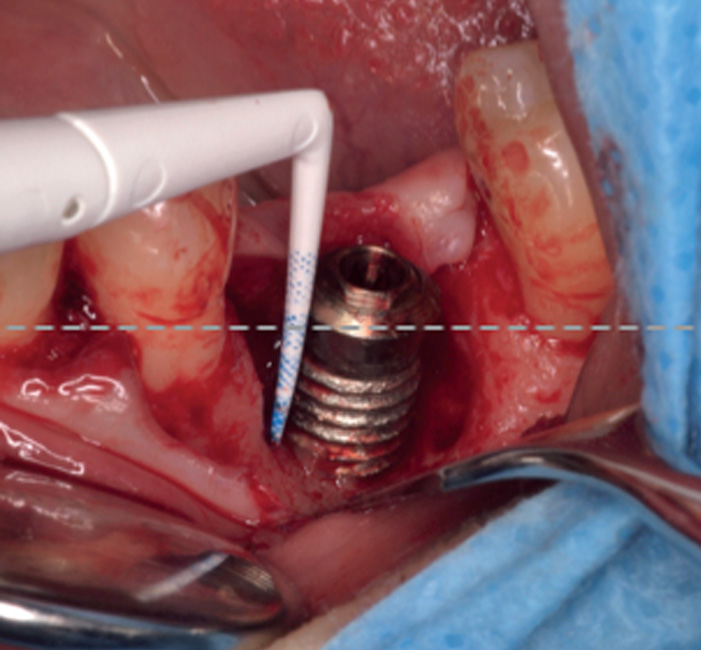
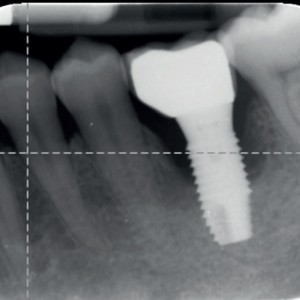
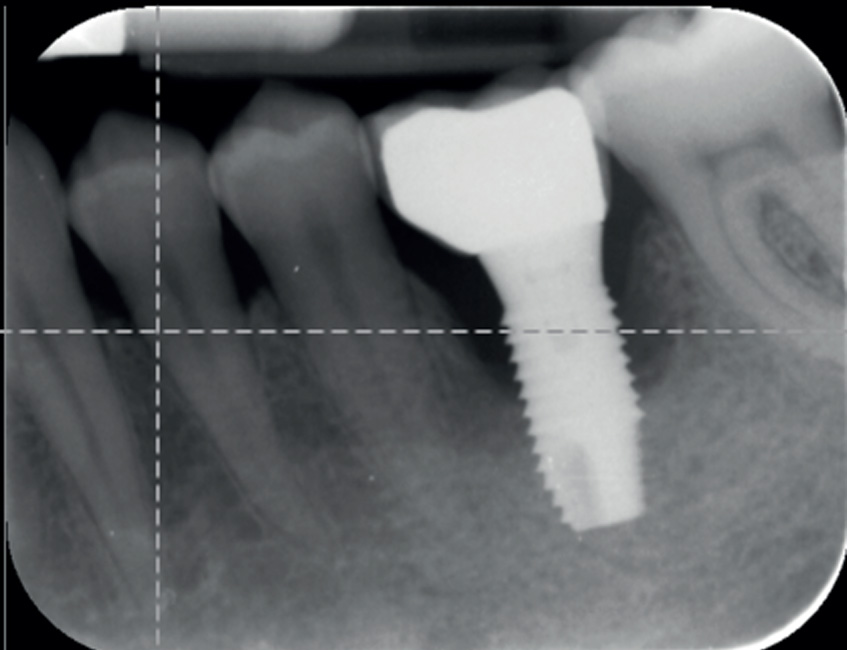
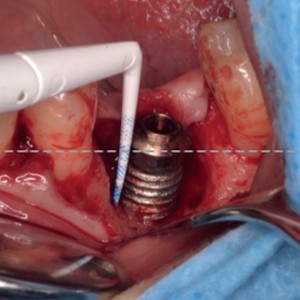
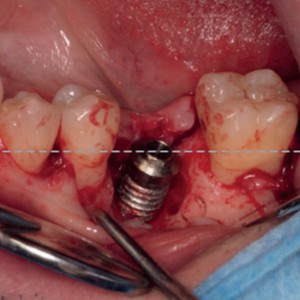
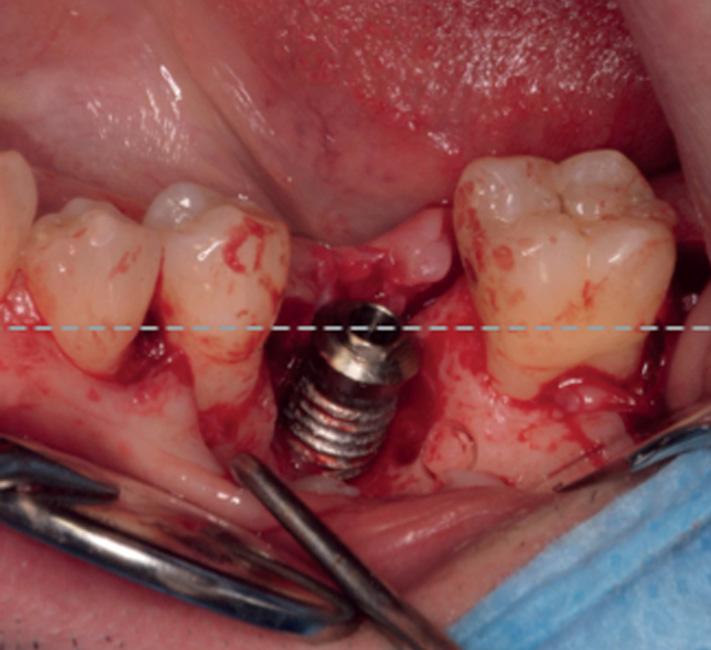
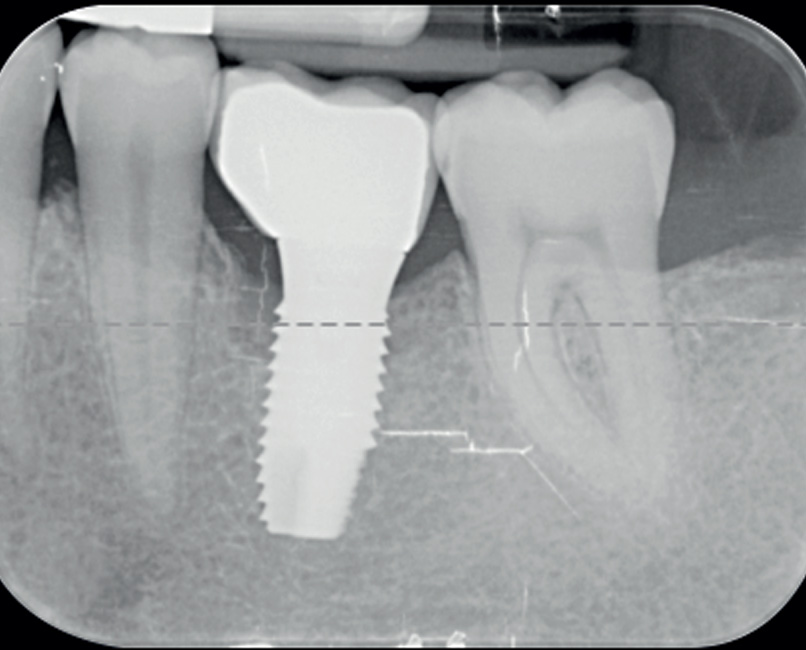
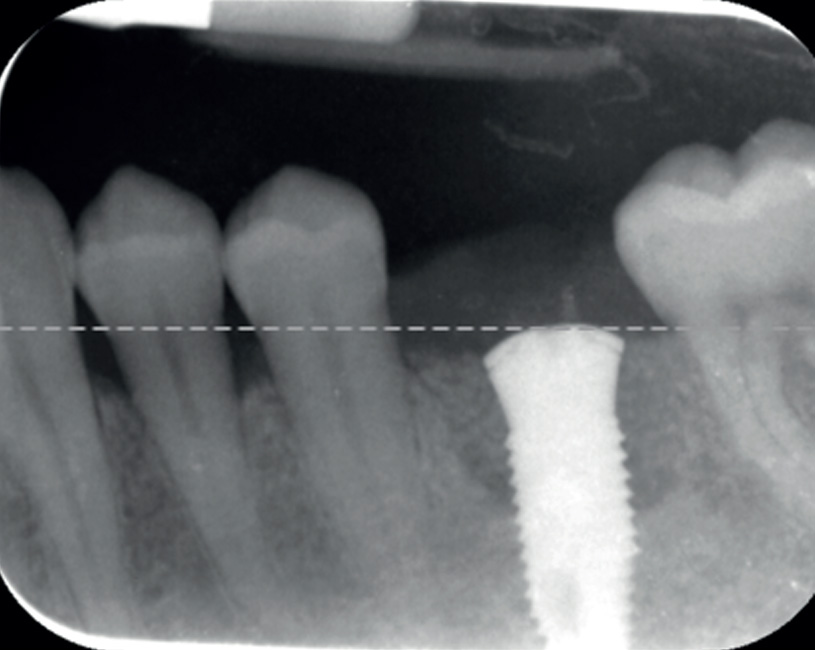
Fig. 1a & 1b
Preoperative radiograph and (b) intraoperative measurement of the bony defect.
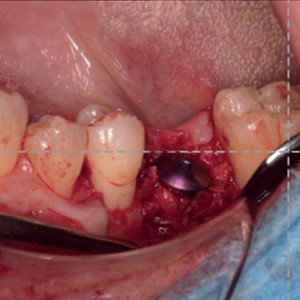
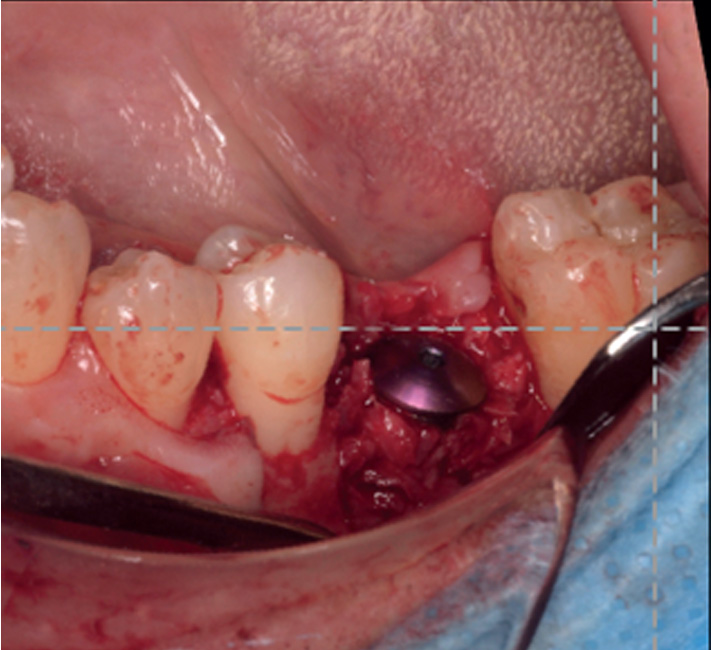
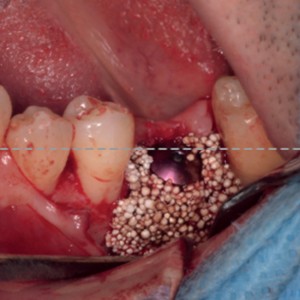
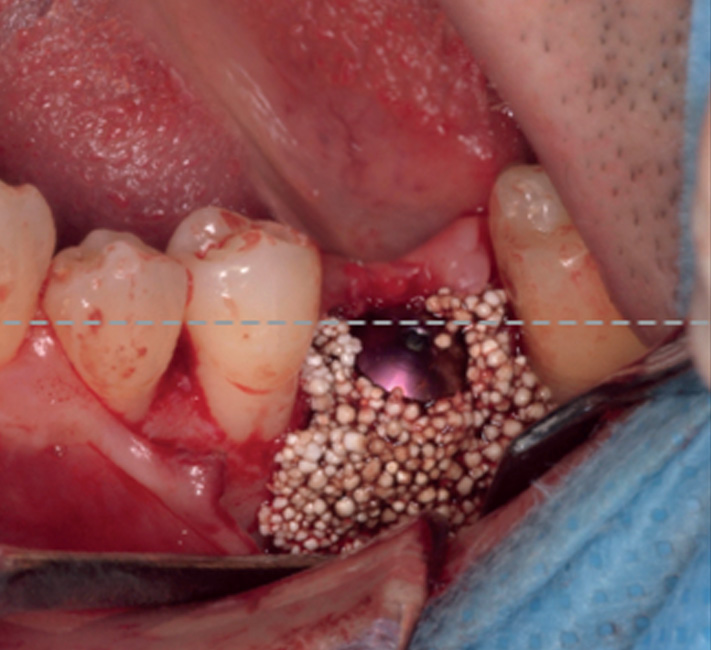
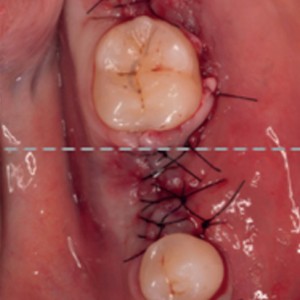
Fig. 2a-d
Surgical phases: (a) degranulation of the defect, (b) autogenous bone graft apposition, (c) easy-graft apposition and (d) primary intention flap suturing.
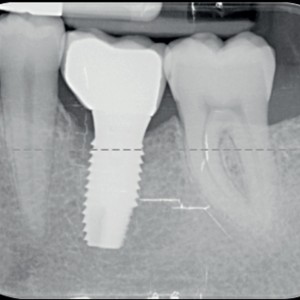
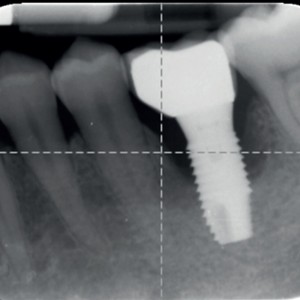
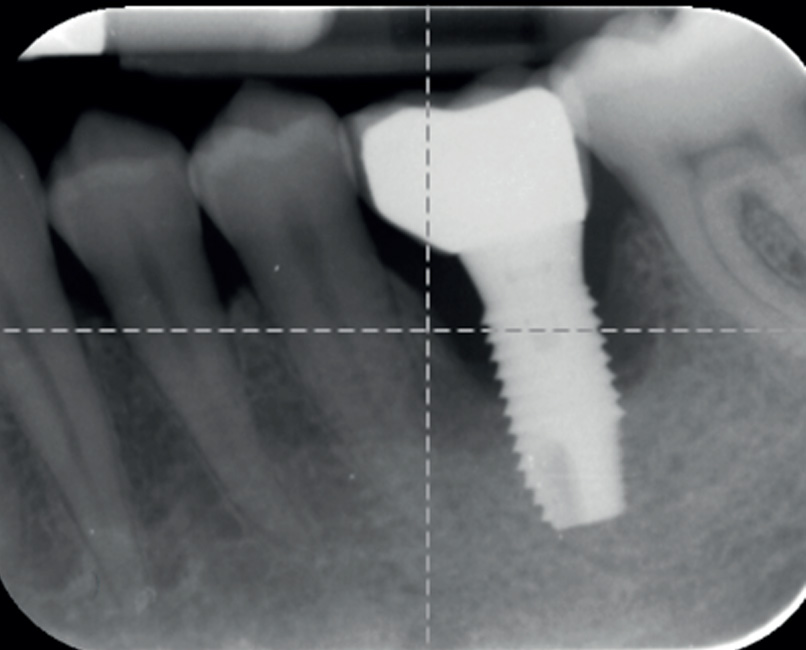
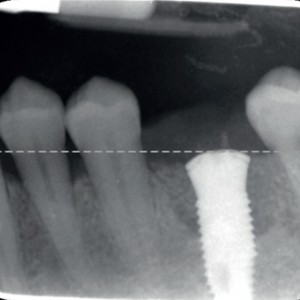
Fig. 3a-c
Radiographic sequence of the site at the time of periimplantitis detection and at the time of surgery.
Preoperative phase
Factors possibly influencing the periimplant pathology were evaluated and problems solved before the surgical phase. This included occlusal adjustment, modification or change of poorly designed prostheses, and periodontal treatment when necessary. Two weeks prior to the surgical therapy, all of the patients received professional prophylaxis (total oral district disinfection) and 0.12% chlorhexidine digluconate (rinsing b.i.d.; GUM Paroex 0.12%, Sunstar Suisse) was prescribed. Antibiotic treatment consisting of amoxicillin 850 mg and clavulanate 125 mg every 8 h was administered to all of the patients, starting two days before the surgical treatment and ending one week after the intervention.
Surgical phase
The surgical intervention was performed under local anesthesia with 4% articaine and 1:100,000 epinephrine (Laboratorios Inibsa, Barcelona, Spain). The prosthesis was removed and a full-thickness flap was elevated to allow access to the periimplant defect and the exposed implant surface.
Once the granulation tissue had been removed, the implant surface was mechanically debrided using PTFE curettes and further cleaned with a cotton pellet soaked in 0.2% chlorhexidine digluconate. The inside of the implant connection was cleaned using 0.2% chlorhexidine (GUM Paroex 0.2%, Sunstar Suisse). Perforations were performed to increase blood supply to the remaining bone and the periimplant bone defects were filled using a double-layer graft:20 Buser D, von Arx T, ten Bruggenkate C, Weingart D. Basic surgical principles with ITI implants.
→ Clin Oral Implants Res. 2000;11 Suppl 1:59–68. autologous bone on the implant surface (collected from a neighboring area using scrapers) and an alloplastic, resorbable bone graft substitute consisting of 100% beta-tricalcium phosphate (GUIDOR easy-graft CLASSIC) to fill the remaining gap and act as a stabilizing shell, that is, a tentlike structure. After defect filling, cover screws were inserted. Tensionless soft-tissue closure of the flap was performed with a 5-0 suture (Fig. 2). Sutures were removed two weeks after the intervention. Abutments and prostheses were cleaned according to Canullo et al. using ultrasound and an extraoral argon plasma device (Plasma R, Diener Electronic, Jettingen, Germany). 21Canullo L, Micarelli C, Lembo-Fazio L, Iannello G, Clementini M. Microscopical and microbiologic characterization of customized titanium abutments after different cleaning procedures.
→ Clin Oral Implants Res. 2014 Mar;25(3):328–36. Epub 2012 Dec 5. One to two months thereafter, the cleaned prosthetic components were reinserted after microsurgical reopening.
-
- Fig. 2a
-
- Fig. 2b
-
- Fig. 2c
-
- Fig. 2d

Follow-up and maintenance
Before suture removal, the patients were advised to discontinue toothbrushing and to avoid trauma at the site of surgery. After the healing phase, the patients were placed on an individually tailored maintenance care program. Motivation, reinforcement of oral hygiene instruction, supragingival instrumentation and antiseptic therapy were performed as needed All of the patients were subsequently recalled every three months for data collection and maintenance therapy. Nonsurgical treatment with ultrasound plastic instruments and air polishing and erythritol powder was repeated every three months throughout the entire follow up period (Fig. 3).
-
- Fig. 3a
-
- Fig. 3b
-
- Fig. 3c
Clinical analysis
All of the clinical analysis were performed by a single trained clinician using a predefined standard protocol. The following clinical variables were assessed at six and 12 months with the aid of a periodontal probe with a millimeter scale (Hawe Neos Probe 1395, Hawe, London, U.K.):
- plaque index;
- bleeding on probing, evaluated as present if bleeding was evident within 30 s after probing or absent if no bleeding was observed within 30 s after probing;
- probing depth, measured from the mucosal margin to the bottom of the examined pocket;
- mucosal recession, measured from the implant shoulder or restoration margin to the mucosal margin;
- clinical attachment level, measured from the implant neck to the deepest point of the periimplant pocket.
Probing depth, mucosal recession and clinical attachment level scores were recorded to the nearest millimeter at six aspects per implant.
Radiographic analysis
Radiographic changes (bone gain or loss) were evaluated using periapical radiographs obtained at baseline and at six and 12 months using paralleling rings and silicone bites to reproduce the exact film position. Periimplant marginal bone changes were evaluated with a computerized measuring technique applied to digital radiographs.
The distance from the mesial and distal margin of the implant neck to the most coronal point where the bone appeared to be in contact with the implant was measured. Evaluation of the marginal bone level around the implants was performed using image analysis software (Scion Image for Windows, Version 4.02, Scion Corp., Frederick, Md., U.S.) able to compensate for radio graphic distortion. The software calculated bone remodeling at the mesial and distal aspects of the implants. The mean of both values was used.
Microbiological analysis
Sampling for microbiological analysis was performed by a single researcher. Samples were obtained from three types of sites in each patient: (a) the periimplant sulcus of each implant; (b) the gingival sulcus of the neighboring teeth; and (c) the connection’s inside and the abutment surface of each implant.
Samples were obtained before the cleaning procedures and 12 months after treatment. Sampling was performed using the GUIDOR Perio- Implant Diagnostic Kit (Sunstar Iberia, Barcelona, Spain; provided by Institut Clinident, Aixen Provence, France), consisting of five sterile absorbent paper tips and an empty sterile 2 mL Eppendorf tube. Prior to subgingival plaque sampling, supragingival plaque was eliminated from the implants and teeth using a curette or cotton roll, without penetrating the gingival or periimplant sulcus. Cotton rolls were used for relative isolation and the sampling sites were dried with a pistol. The paper tips were inserted into the gingival or periimplant sulcus for 30 s.
One drop of RNA and DNA free water (Water Molecular Biology Reagent, code W4502, Sigma-Aldrich, St. Louis, Mo., U.S.) was placed inside the implant connection and the paper tips were inserted for 30 s. Quantitative real time polymerase chain reaction (PCR) assays were carried out for total bacterial count and for ten pathogens at Institut Clinident: Aggregatibacter actinomycetemcomitans (Aa), Porphyromonas gingivalis (Pg), Tannerella forsythia (Tf), Treponema denticola (Td), Prevotella intermedia (Pi), Peptostreptococcus micros (Pm), Fusobacterium nucleatum (Fn), Campylobacter rectus (Cr), Eikenella corrodens (Ec) and Candida albicans (Ca).
Quantitative real time PCR assays was performed in a volume of 10 μL composed of 1× QuantiFast SYBR Green PCR (Qiagen, Berlin, Germany), 2 μL of DNA extract and 1 μM of each primer. The species-specific PCR primers (Metabion, Martinsried, Germany) used in this study were provided by Institut Clinident. The bacterial primers used were derived from previously published ribosomal 16S ribosomal RNA sequences15, 16 and were adapted to the real time PCR conditions. The Ca primers used in this study were derived from 18S/28S ribosomal RNA sequences.
Assays were carried out on the Rotor-Gene Q thermal cycling system (Qiagen) with the following program: 95 °C for 5 min, followed by 40 cycles of 10 s at 95 °C, 10 s at 60 °C, and 35 s at 72 °C. A final melting curve analysis (70–95 °C in 1 °C steps for 5 s increments) was performed. Fluorescence signals were measured every cycle at the end of the extension step and continuously during the melting curve analysis. The resulting data were analyzed using Rotor-Gene Q Series Software (Qiagen).
Serial dilutions of bacterial standard DNA, provided by Institut Clinident, were used in each reaction as external standards for absolute quantification of the targeted bacterial pathogens. Standard bacterial strains used for standard DNA production were obtained from the DSMZ (Braunschweig, Germany), the Collection of Institut Pasteur (Paris, France) and from the BCCM/ LMG Bacteria Collection (Ghent, Belgium): Aa (DSM No. 8324), Pg (DSM No. 20709), Tf (CIP No. 105220), Td (DSM No. 14222), Pi (DSM No. 20706), Pm (DSM No. 20468), Fn (DSM No. 20482), Cr (LMG No. 18530) and Ec (DSM No. 8340). A Ca standard DNA (DSM No. 6659) was also used as external standard for identification and semiquantification.
Statistical analysis
The statistical analysis was performed using a commercially available software program (IBM SPSS Statistics for Windows, Version 20.0, IBM Corp., Armonk, N.Y., U.S.). Mean values and standard deviations were calculated for each variable using the implant as the statistical unit. The data rows were examined with the Kolmogorov– Smirnov test and proven to be normally distributed. For the statistical evaluation of the changes over time, the paired t-test was used. The error was set at 0.05.
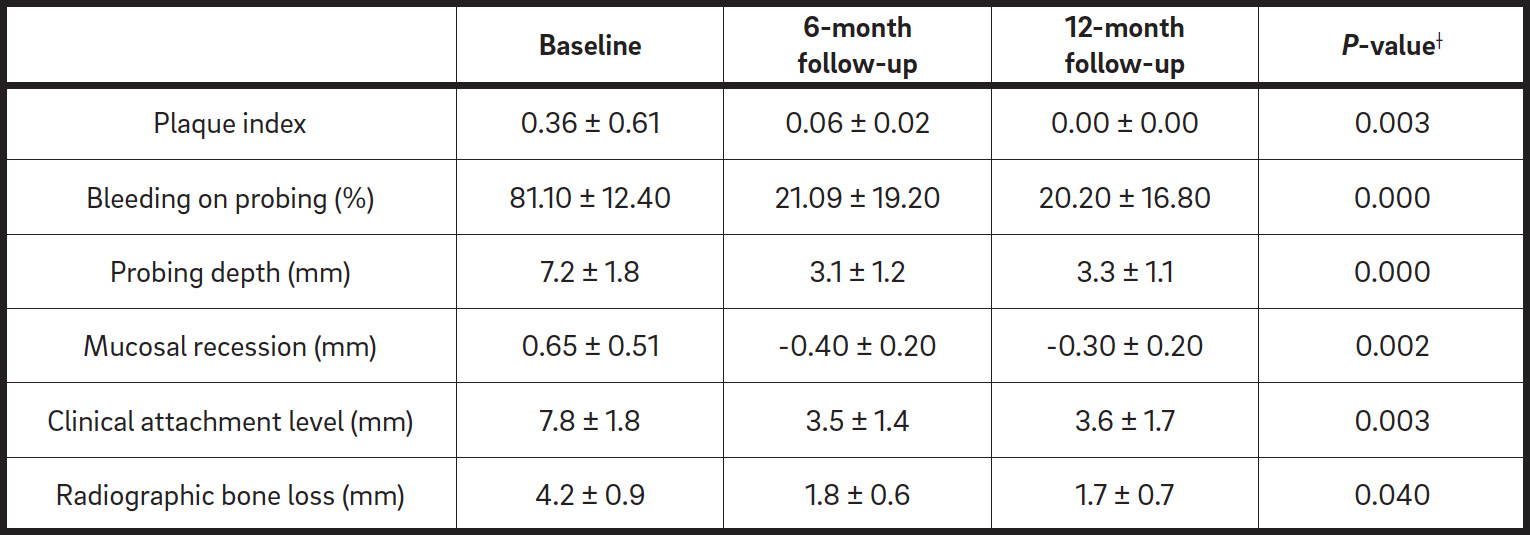
Clinical (occlusal and lateral) and radiographic view at the 12-month follow-up.Table. 1
Clinical parameters (mean ± standard deviation) at baseline and at six months and 12 months (13 implants).
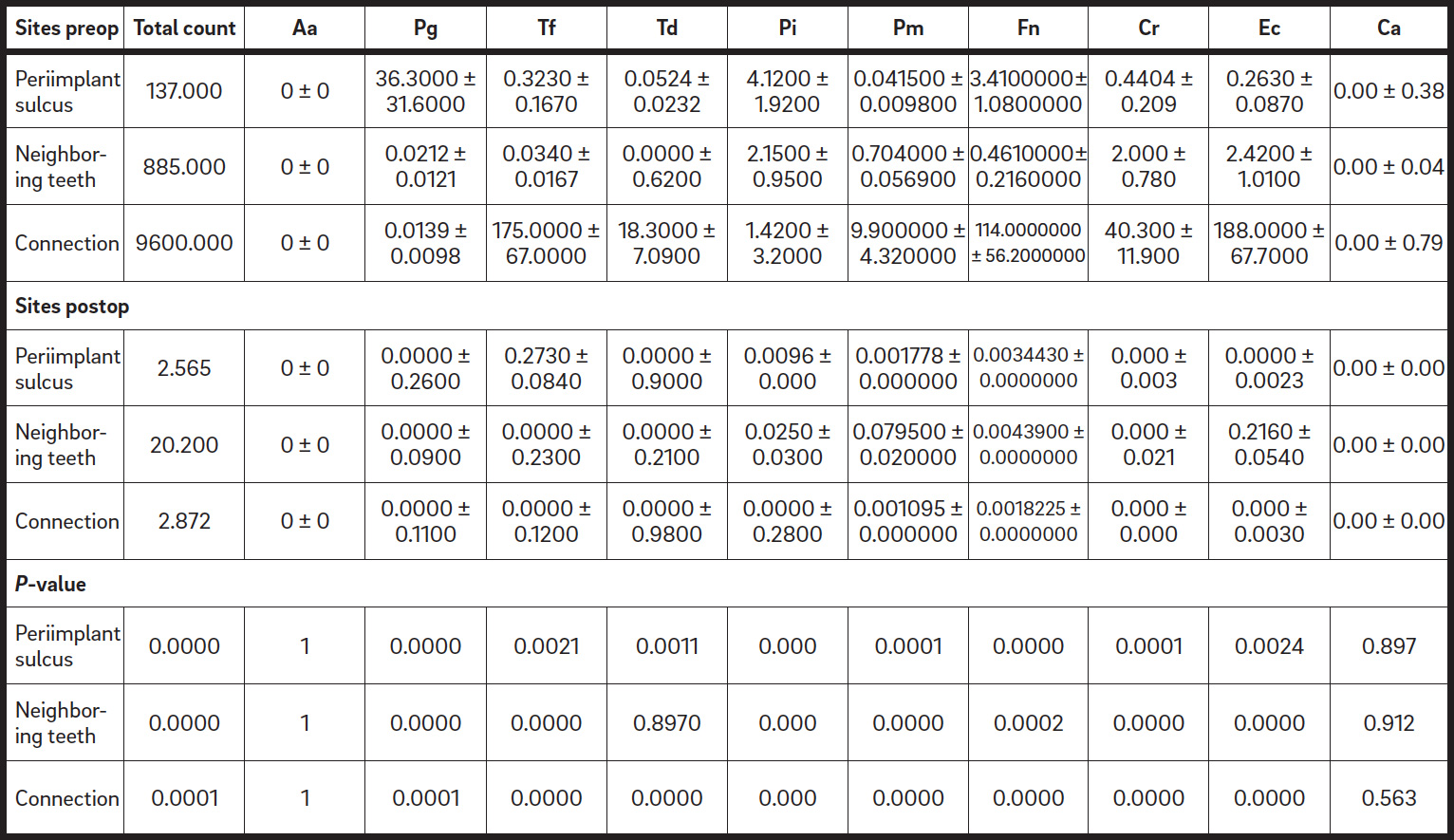
Table. 2
Bacteria counts at different sites (values expressed in millions of colony-forming units).
Results
Ten patients were included in the study. A total of 13 implants were treated. During the entire observation period of 12 months, two patients failed to attend the scheduled recall sessions and, therefore, were excluded from the study. No patient reported any sign of swelling or pain two weeks after the surgery. The clinical and radiographic data are summarized in Table 1. Essentially, mean probing depth values were significantly reduced by 4.1 mm and 3.9 mm at six and 12 months, respectively. The surgical procedure was associated with a pronounced increase in mucosal recession and clinical attachment level; however, stable periimplant conditions at six and12 months were reported. Mean bleeding on probing values were significantly reduced at six and 12 months. Before treatment, pus was present around four implants. At the end of the observation period, the tissue around the implants was in a healthy condition.
All of the patients presented with low plaque index values throughout the entire observation period. Radiographic analysis demonstrated a complete or semicomplete filling of the defect in all of the cases, with a significant bone gain at six and 12 months (Fig. 4). Microbiological analysis, in terms of total bacterial count and single pathogens, demonstrated a significant decrease of microbiological contamination in all of the test sites between baseline and the 12 months follow-up: at the sulcus, the neighboring teeth and the connection. The data are summarized in Table 2.
-

- Fig. 4a

-

- Fig. 4b

-

- Fig. 4c

Discussion
The data reported in the present study showed a good short-term resolution of periimplantitis defects using the proposed surgical approach and concomitant dental hygienic treatment. The graft material proposed is self-stabilizing in the defect, which might suggest that the use of a membrane with the bone graft substitute can be omitted. This feature helped to stabilize the bone graft substitute in situ in a tentlike structure over the autologous bone in a double-layer graft technique, thereby providing and protecting space for bone regeneration around the dental implant. Application of autogenous bone to the implant surface below the biomaterial might increase the osteopromotive capability of the technique as reported before.22Buser D, von Arx T, ten Bruggenkate C, Weingart D. Basic surgical principles with ITI implants.
→ Clin Oral Implants Res. 2000;11 Suppl 1:59–68.
In the present study, no barrier membrane was used in addition to the bone graft substitute. This was due to the previously mentioned qualities of the tested graft material. The presence of a collagen membrane might additionally prevent the invasion of connective tissue into the grafted site, but it does not provide any additional stabilization of the bone graft substitute. It must be noted, however, that the coverage with the intact periosteum might protect the graft material, allowing bone promotive cell diffusion into the grafted site.23Jensen OT, Bell W, Cotta, J. Osteoperiosteal flaps and local osteotomies for alveolar reconstruction.
→ Oral Maxillofac Surg Clin North Am. 2010 Aug;22(3):331–46, vi. For this reason, in this preliminary study, preoperative marginal soft-tissue healing through professional oral hygiene (scaling) was achieved, applied by dental hygienists to resolve periimplant mucositis before treatment. Additionally, accurate soft-tissue management during the surgical phase was provided to minimize periosteum deficiencies.
Regarding the microbiological environment at the periimplant sulcus and neighboring teeth, a significant decrease of the bacterial load in terms of total count and single pathogens was observed. At the same time, these data corroborated a significant decrease of the clinical parameters indicative of a reduction of the peri implantitis. The data suggest that a preoperative full-mouth prophylaxis, a tailored program of maintenance, recall and reinforcement of home care, represents a prerequisite for successful soft and hardtissue healing. In fact, while preoperative oral district disinfection might be involved in the most considerable improvement of microbiological contamination (essential for a good surgical plan), a tailored program of oral hygiene might represent an essential criterion for the longitudinal maintenance of the periimplant soft and hard-tissue during healing. As documented by Renvert and Polyzois and Serino et al., decreasing of home maintenance might compromise the clinically achieved outcomes in the mid-term.24Renvert S, Polyzois IN. Clinical approaches to treat peri-implant mucositis and peri-implantitis.
→ Periodontol 2000. 2015 Jun;68(1):369–404. 25Serino G, Turri A, Lang NP. Maintenance therapy in patients following the surgical treatment of peri-implantitis: a 5-year follow-up study.
→ Clin Oral Implants Res. 2015 Aug;26(8):950–6.
In the analysis of the bacterial contamination at the implant connection level, a statistically significant decrease of the total account was detected during the study. However, all of the connections still demonstrated a bacteriologically polluted environment until the end of the follow-up period. It could be speculated that more effective bacterial control at the implant connection level and in the periimplant sulcus would allow for longer protection of the defect site from the disruptive effects of bacterial presence. For this reason, a different technique providing decontamination and, therefore, maintenance of the condition might be suggested. In fact, as documented by Paolantonio et al., chlorhexidine
was demonstrated to maintain the implant connection decontamination for a period shorter than six months.26Paolantonio M, Perinetti G, D’Ercole S, Graziani F, Catamo G, Sammartino G, Piccolomini R. Internal decontamination of dental implants: an in vivo randomized microbiologic 6-month trial on the effects of a chlorhexidine gel.
→ J Periodontol. 2008 Aug;79(8):1419–25.
Limitations of the present study clearly relate to the study design itself: The short follow-up period and small sample size suggested to carefully handle the even promising reported outcomes. A further limitation is that only less challenging bone defects were included in this preliminary study; hence, the regenerative outcomes should be considered in light of this.
For this study, only contained circumferential or semicircumferential defects were included that represented the most predictive defect shape, as documented by Schwarz et al compared with two or one-wall bone defects.27Schwarz F, Sahm N, Schwarz K, Becker J.Impact of defect configuration on theclinical outcome following surgical regenerative therapy of peri-implantitis.
→ J Clin Periodontol. 2010 May;37(5):449–55. According to the literature, despite profuse efforts, massive soft-tissue shrinkage has been reported. 28Schwarz F, Sahm N, Schwarz K, Becker J.Impact of defect configuration on theclinical outcome following surgical regenerative therapy of peri-implantitis.
→ J Clin Periodontol. 2010 May;37(5):449–55. For this reason, new surgical techniques should be applied to counteract this phenomenon. For this purpose, as suggested by Schwarz et al., the use of a connective tissue graft might be effective in controlling soft-tissue architecture if adapted over the regenerated site.29 Schwarz F, Sahm N, Becker J. Combined surgical therapy of advanced periimplantitis lesions with concomitant soft tissue volume augmentation. A case series.
→ Clin Oral Implants Res. 2014 Jan;25(1):132–6. In addition, a new flap design, as reported by Zucchelli and Mounssif, might represent an alternative strategy. 30Zucchelli G, Mounssif I. Periodontal plastic surgery.
→ Periodontol 2000. 2015 Jun;68(1):333–68. Furthermore, a study with a longer followup, larger sample size and different defect types should be designed to corroborate the findings of the present study. However, it can be concluded that, within the limitations of the present preliminary study, the proposed technique, in combination with a self-stabilizing graft material, offers promising results in the treatment of circumferential and semicircumferential bone defects around implants affected by periimplantitis, without the use of a barrier membrane.
Competing interests
The authors declare that they have no competing interests.
Interview
with Luigi Canullo
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Muthukuru M, Zainvi A, Esplugues EO, Flemmig TF. Non-surgical therapy 0for the management of peri-implantitis: a systematic review. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:77–83. |
| 2. | ↑ | Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94. |
| 3. | ↑ | Serino G, Turri A. Outcome of surgical treatment of peri-implantitis: results from a 2-year prospective clinical study in humans. → Clin Oral Implants Res. 2011 Nov;22(11):1214–20. |
| 4, 25. | ↑ | Serino G, Turri A, Lang NP. Maintenance therapy in patients following the surgical treatment of peri-implantitis: a 5-year follow-up study. → Clin Oral Implants Res. 2015 Aug;26(8):950–6. |
| 5, 8. | ↑ | Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:325–45. |
| 6. | ↑ | Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94. |
| 7, 13, 14, 16, 19, 27, 28. | ↑ | Schwarz F, Sahm N, Schwarz K, Becker J.Impact of defect configuration on theclinical outcome following surgical regenerative therapy of peri-implantitis. → J Clin Periodontol. 2010 May;37(5):449–55. |
| 9. | ↑ | Graziani F, Figuero E, Herrera D. Systematic review of quality of reporting, outcome measurements and methods to study efficacy of preventive and therapeutic approaches to peri-implant diseases. → J Clin Periodontol. 2012 Feb;39 Suppl 12:224–44. |
| 10. | ↑ | Pesce P, Menini M, Tealdo T, Bevilacqua M, Pera F, Pera P. Peri-implantitis: a systematic review of recently published papers. → Int J Prosthodont. 2014 Jan-Feb;27(1):15–25. |
| 11. | ↑ | Canullo L, Penarrocha-Oltra D, Soldini C, Mazzocco F, Penarrocha M, Covani U. Microbiological assessment of the implant-abutment interface in different connections: cross-sectional study after 5 years of functional loading. → Clin Oral Implants Res. 2015 Apr;26(4):426–34. Epub 2014 Mar 26. |
| 12. | ↑ | Sanz M, Chapple IL; Working Group 4 of the VIII European Workshop on Periodontology. Clinical research on peri-implant diseases: consensus report of Working Group 4. → J Clin Periodontol. 2012 Feb;39 Suppl 12:202–6. |
| 15. | ↑ | Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:84–94. |
| 17. | ↑ | Leventis MD, Fairbairn P, Kakar A, Leventis AD, Maragaritis V, Lückerath W, Horowitz RA, Nagursky H. Minimally invasive alveolar ridge preservation utilizing an in situ hardening ?-tricalcium phosphate bone substitute: a multicenter case series. → Int J Dent. 2016;2016:5406736. doi:10.1155/2016/5406736. |
| 18. | ↑ | Cordaro L, Bosshardt DD, Palattella P, Rao W, Serino G, Chiapasco M. Maxillary sinus grafting with Bio-Oss or Straumann Bone Ceramic: histomorphometric results from a randomized controlled multicenter clinical trial. → Clin Oral Implants Res. 2008 Aug;19(8):796–803. |
| 20. | ↑ | Buser D, von Arx T, ten Bruggenkate C, Weingart D. Basic surgical principles with ITI implants. → Clin Oral Implants Res. 2000;11 Suppl 1:59–68. |
| 21. | ↑ | Canullo L, Micarelli C, Lembo-Fazio L, Iannello G, Clementini M. Microscopical and microbiologic characterization of customized titanium abutments after different cleaning procedures. → Clin Oral Implants Res. 2014 Mar;25(3):328–36. Epub 2012 Dec 5. |
| 22. | ↑ | Buser D, von Arx T, ten Bruggenkate C, Weingart D. Basic surgical principles with ITI implants. → Clin Oral Implants Res. 2000;11 Suppl 1:59–68. |
| 23. | ↑ | Jensen OT, Bell W, Cotta, J. Osteoperiosteal flaps and local osteotomies for alveolar reconstruction. → Oral Maxillofac Surg Clin North Am. 2010 Aug;22(3):331–46, vi. |
| 24. | ↑ | Renvert S, Polyzois IN. Clinical approaches to treat peri-implant mucositis and peri-implantitis. → Periodontol 2000. 2015 Jun;68(1):369–404. |
| 26. | ↑ | Paolantonio M, Perinetti G, D’Ercole S, Graziani F, Catamo G, Sammartino G, Piccolomini R. Internal decontamination of dental implants: an in vivo randomized microbiologic 6-month trial on the effects of a chlorhexidine gel. → J Periodontol. 2008 Aug;79(8):1419–25. |
| 29. | ↑ | Schwarz F, Sahm N, Becker J. Combined surgical therapy of advanced periimplantitis lesions with concomitant soft tissue volume augmentation. A case series. → Clin Oral Implants Res. 2014 Jan;25(1):132–6. |
| 30. | ↑ | Zucchelli G, Mounssif I. Periodontal plastic surgery. → Periodontol 2000. 2015 Jun;68(1):333–68. |





Leave a Reply
Be the First to Comment!