The clinical effects of insertion torque for implants placed in healed ridges: A two-year randomized controlled clinical trial
January 6, 2017 / Categories: Digital Dentistry, Implant Dentistry

Alfonsi, Fortunato

Borgia, Valentina

Barbato, Luigi

Tonelli, Paolo

Giammarinaro, Enrica

Marconcini, Simone

Romeggio, Stefano

Barone, Antonio
Several factors are involved in the achievement of implant primary stability, such as the insertion torque, the implant’s macrogeometry, the surgical technique, and the bone quality and quantity. Implant primary stability is considered one of the key factors for osseointegration and is associated with insertion torque.
Introduction
Several studies have suggested that insertion torque values of 25–45 N cm could prevent micromovements that could impair the bone healing around the implants. The aim of the present randomized clinical trial was to evaluate and compare the clinical outcome for implants placed with a high insertion torque (50–100 N cm) and a regular insertion torque (within 50 N cm) in healed ridges after two years.
The use of dental implants is considered a safe and reliable procedure for replacing missing teeth. Several factors are involved in the achievement of implant primary stability, such as the insertion torque, the implant’s macrogeometry, the surgical technique, and the bone quality and quantity. Primary stability is regarded as one of the main factors for the achievement of osseointegration, that is, secondary stability.1Campos FE, Jimbo R, Bonfante EA, Barbosa DZ, Oliveira MT, Janal MN, Coelho PG. Are insertion torque and early osseointegration proportional? A histologic evaluation.
→ Clin Oral Implants Res. 2015 Nov;26(11):1256–60. It has been observed that micromovements > 50–150 μm have a detrimental effect on bone formation around the implant surface, leading to the formation of fibrous tissue and consequently implant failure.2Szmukler-Moncler S, Salama H, Reingewirtz Y, Dubruille JH. Timing of loading and effect of micromotion on bone-dental implant interface: review of experimental literature.
→ J Biomed Mater Res. 1998 Summer;43(2):192–203. With implant primary stability being related to the mechanical connection between the implant and the bone, it could be influenced by the implant’s design, the bone quality and quantity, and the surgical site preparation. 3Duyck J, Roesems R, Cardoso MV, Ogawa T, De Villa Camargos G, Vandamme K. Effect of insertion torque on titanium implant osseointegration: an animal experimental study.
→ Clin Oral Implants Res. 2015 Feb;26(2):191–6.4Freitas AC Jr, Bonfante EA, Giro G, Janal MN, Coelho PG. The effect of implant design on insertion torque and immediate micromotion.
→ Clin Oral Implants Res. 2012 Jan;23(1):113–8. Inserting an implant in an undersized implant site osteotomy requires considerable force, which is referred to as the insertion torque. The bone is an elastic tissue before exceeding the yielding point: It can tolerate a certain level of strain owing to a relaxation effect.5 Jimbo R, Anchieta R, Baldassarri M, Granato R, Marin C, Teixeira HS, Tovar N, Vandeweghe S, Janal MN, Coelho PG. Histomorphometry and bone mechanical property evolution around different implant systems at early healing stages: an experimental study in dogs.
→ Implant Dent. 2013 Dec;22(6):596–603. When the strain exceeds the yielding point, bone microfractures can be observed; this could cause an ischemic necrosis6Bashutski JD, D’Silva NJ, Wang HL. Implant compression necrosis: current understanding and case report.
→ J Periodontol. 2009 Apr;80(4):700–4. and, consequently, bone resorption. High insertion torque protocols have been suggested to enhance and accelerate implant success, considered as being strictly related to the bone–implant mechanical interlocking and primary stability.7Trisi P, Perfetti G, Baldoni E, Berardi D, Colagiovanni M, Scogna G. Implant micromotion is related to peak insertion torque and bone density.
→ Clin Oral Implants Res. 2009 May;20(5):467–71. However, the compressive forces caused by a high insertion torque could delay or compromise the process of osseointegration. 8Coelho PG, Takayama T, Yoo D, Jimbo R, Karunagaran S, Tovar N, Janal MN, Yamano S. Nanometer-scale features on micrometer-scale surface texturing: a bone histological, gene expression, and nanomechanical study.
→ Bone. 2014 Aug;65:25–32. A modified thread design could significantly help to decrease the strain developed on the bone surface compared with the conventional thread design.9Jimbo R, Tovar N, Marin C, Teixeira HS, Anchieta RB, Silveira LM, Janal MN, Shibli JA, Coelho PG. The impact of modified cutting flute implant design on osseointegration.
→ Int J Oral Maxillofac Surg. 2014 Jul;43(7):883–8. Although the scientific literature is not uniform regarding the minimum insertion torque required to obtain successful osseointegration, values between 32 N cm and 50 N cm are recommended.10Ottoni JM, Oliveira ZF, Mansini R, Cabral AM. Correlation between placement torque and survival of single-tooth implants.
→ Int J Oral Maxillofac Implants. 2005 Sep-Oct;20(5):769–76. One factor affecting the esthetic outcome of implants is buccal bone thickness after the implant site preparation. In healed ridges, 2 mm thickness is recommended, although there is insufficient scientific evidence to establish a threshold for minimum buccal bone thickness.11Suaid FA, Novaes AB Jr, Queiroz AC, Muglia VA, Almeida AL, Grisi MF. Buccal bone plate remodeling, after immediate implants with or without synthetic bone grafting and flapless surgery: a histomorphometric and fluorescence study in dogs.
→ Clin Oral Implants Res. 2014 Feb;25(2):e10–21.12Teughels W, Merheb J, Quirynen M. Critical horizontal dimensions of interproximal and buccal bone around implants for optimal aesthetic outcomes: a systematic review.
→ Clin Oral Implants Res. 2009 Sep;20 Suppl 4:134–45.
The primary objective of the present study was to evaluate and compare the clinical outcomes for implants placed with a high insertion torque (50–100 N cm) and a regular insertion torque (within 50 N cm) in healed ridges, in terms of changes at the marginal bone level. The null hypothesis was that there was no difference in the marginal bone level changes between the two groups; the alternative hypothesis was that there was a difference.
The secondary objective of this study was to analyze the correlation between the residual thickness of the buccal bone after implant osteotomy preparation and the facial soft-tissue level changes. The null hypothesis was that there was no difference in the facial soft-tissue changes between the two buccal plate groups (thickness < 1 mm vs. thickness > 1 mm), against the alternative hypothesis that there was a difference. The present study was designed according to the CONSORT Statement for parallel-group randomized trials.13 Schultz KF, Altman DG, Moher D; CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials.
→ Trials [Internet]. 2010 Mar 24 [cited 2016 Nov 14];11:Article 32 [8 p.]. doi:10.1186/1745-6215-11-32.
Materials and methods
Partially edentulous patients who were 18 years old or older and able to sign an informed consent form and required at least one single implantsupported delayed restoration were considered eligible for inclusion in the trial. All of the patients were recruited from the consultation clinic at the Dentistry Department of Versilia Hospital, University of Pisa, Pisa, Italy, from July 2011 to December 2012. This study was designed as a parallel-arm randomized controlled clinical trial and consecutively treated patients were included.
The exclusion criteria were
- history of systemic diseases that would contraindicate oral surgery;
- long-term nonsteroidal anti-inflammatory drug therapy;
- intravenous and oral bisphosphonate therapy;
- lack of occluding dentition in the area intended for the restoration;
- extraction sites with less than three months of healing;
- untreated periodontal disease;
- need for bone augmentation at the time of implant surgery;
- poor oral hygiene and compliance (presence of stains, calculus and plaque before surgery);
- pregnant or nursing;
- unwillingness to return for the follow-up examination; and
- smoking more than ten cigarettes per day (subjects who smoked fewer than ten cigarettes per day were requested to stop smoking before and after surgery;
- however, their compliance could not be monitored).
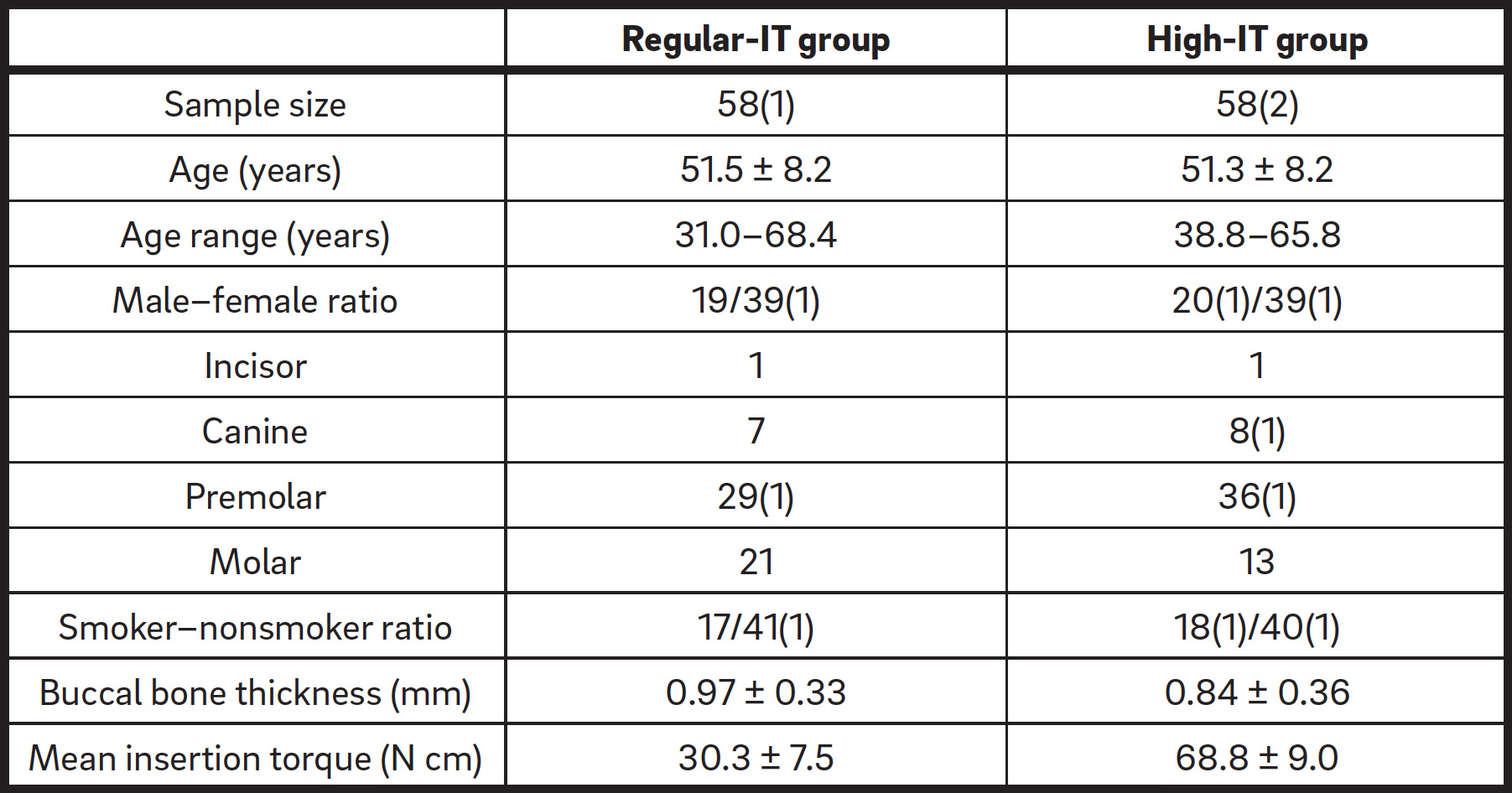
The study followed the principles outlined in the Declaration of Helsinki of 1975, as revised in 2013, on clinical research involving human subjects and was approved by the local ethics committee. Demographic data are summarized in Table 1. All of the patients received a thorough explanation and had to complete a written informed consent form prior to being enrolled in the trial. Patients included in the study were accurately evaluated by examining the clinical aspects and periapical or panoramic radiographs and underwent computed tomography scan examination, if required. After the consent form had been signed, all of the patients underwent at least one oral hygiene session in order to provide a more favorable oral environment for wound healing. Impressions of the selected jaws were taken, in order to adequately plan the prosthesis and obtain a stable occlusion.
Clinical and radiographic evaluations were performed to select patients with an amount of bone adequate for implant placement. Patient recruitment and treatment were performed by two well-trained surgeons (AB and FA), who received training before starting the study. The training included calibration for surgical, prosthetic and follow-up procedures, as well as the management of any complications.
Patients were randomly allocated by opening a sequentially numbered envelope corresponding to the patients’ recruitment numbers, either to the high insertion torque group or to the regular insertion torque group. The high insertion torque group received a self-tapping design implant (CT, Intra-Lock International, Boca Raton, Fla., U.S.), which had an insertion torque value ≥ 50 N cm. The regular insertion torque group received a modified cutting flute design implant (Blossom CT, Intra-Lock International), which had an insertion torque value < 50 N cm. The thread design of the two implants was identical, only differing regarding the cutting groove design.
A computer-generated restricted randomization list was created. One investigator (PT), who was not involved in the selection and in the clinical treatment of the patients, had access to this list and was aware of the random sequence. The information about the treatment of each patient was contained in sealed envelopes, sequentially numbered, identical and opaque. Envelopes were opened sequentially, after osteotomy prepara tion and before implant insertion. Treatment allocation was concealed to the investigators in charge of enrolling and treating the patients.
Surgical procedure
All of the patients received prophylactic antibiotic therapy (2 g of amoxicillin or 600 mg of clindamycin if allergic to penicillin 1 h prior to implant surgery). After local anesthesia (articaine with 1:100,000 epinephrine) and rinsing with a 0.2% chlorhexidine mouthwash, a crestal incision and full-thickness flap elevation were performed in all of the patients.
The implant osteotomy preparation followed the manufacturer’s recommendations. A surgical guide was used to prosthetically determine the implant position after the initial perforation of the cortical bone. A 2 mm twist drill was used with the surgical guide in order to achieve the position and angulation planned, and the osteotomy was widened according to the manufacturer’s recommendations. After the final drilling, all of the surgical sites were prepared in the coronal part to as deep as 2 mm with a countersink drill. Implants were inserted with a surgical unit (ElcoMed, W&H Dentalwerk Bürmoos, Bürmoos, Austria; Fig. 1) at a calibrated maximum torque of 40 N cm at a predetermined 30 rpm. All of the implants were positioned at the bone crest level and were seated at the final position, utilizing for the last 2 mm a digital torque gauge (BTGE 10CN, Tohnichi Torque, Northbrook, Ill., U.S.). After positioning of the cover screw, the flaps were sutured using 4-0 silk stitches.
The patients were instructed to take anti-inflammatory therapy (ibuprofen 600 mg tablets t.i.d. for as long as required) and to rinse with a 0.2% chlorhexidine mouthwash (for 1 min b.i.d. for two weeks). The patients were recommended to avoid brushing and trauma and any removable prostheses were removed. After ten days, the sutures were removed and oral hygiene instructions were given.
The implants were left to heal submerged for three months. Subsequently, the implants were exposed and impressions were taken using the ITAB transfer/abutment (Intra-Lock International) with an individual tray and polyvinyl siloxane material (Flexitime, Heraeus Kulzer, Hanu, Germany). Implant abutments were customized and definitive metal–ceramic crowns were cemented. Periapical radiographs were taken, with the parallel cone technique with a digital sensor (70 kVp, 7 mA), at baseline (immediately after implant insertion) and at three, six, 12 and 24 months after implant placement. The patients were enrolled in an oral hygiene program with recall visits every four months for the entire duration of the study and an independent observer performed all of the follow-ups.
-
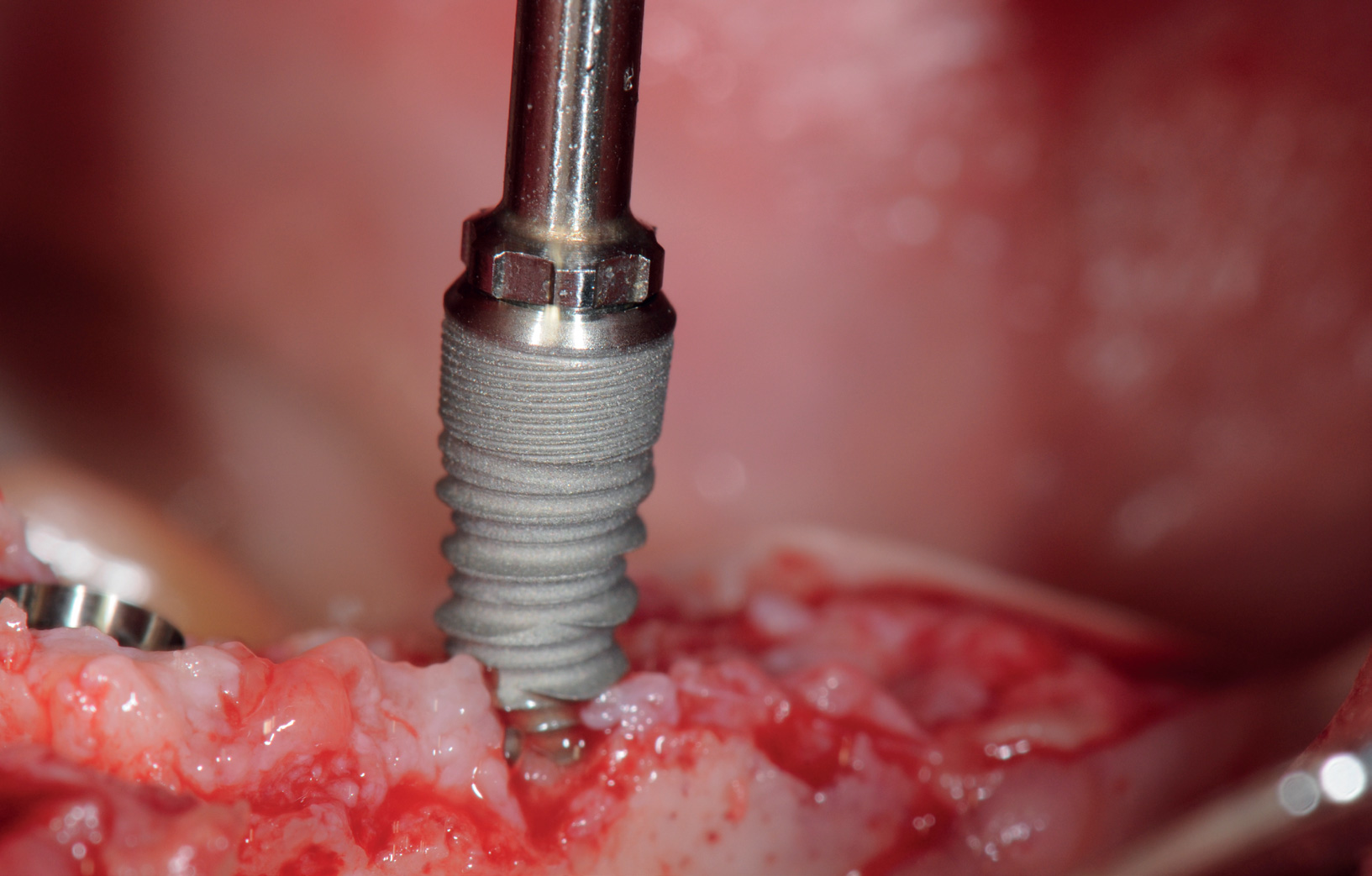
- Fig. 1
Insertion of an implant of the regular-IT group.
Variables
Sample description variables
The sample was described by the following variables: age; sex; smoking habit; location, length and insertion torque of dental implant; and thickness of the residual buccal bone plate after osteotomy. The following numerical variables were evaluated:
- Insertion torque (IT): The IT was registered at the time of surgery by a digital torque gauge (BTGE 10CN), after each turn of 90° of the implant. Subsequently, the mean IT was calculated according to the values registered and to the number of turns required to fit the implant platform to the level of the crestal bone.
- Buccal bone thickness (BBT): The residual bone thickness on the buccal aspect of the implant osteotomy preparation was measured at baseline at the midfacial level of the buccal bone plate using a surgical caliper. Two groups were identified according to the BBT: Group A with a thickness < 1 mm and Group B with a thickness ≥ 1 mm.
Outcome variables
All other measurements were acquired immediately at the time of surgery (baseline) and at three, six, 12 and 24 months after dental implant
insertion. A single well-trained clinician, who was not involved in the surgical treatment, registered all of the measurements.
The following outcome variables were registered:
- Periimplant marginal bone level (MBL) at the mesial and distal sites: The distance between the reference point and the most apical point of the MBL was evaluated on intraoral radiographs. The reference point was the fixture platform. A paralleling device and individualized bite blocks, made of polyvinyl siloxane impression material, were used for the standardization of the X-ray geometry. Calibration was performed using the known thread pitch distance of the implants (pitch = 1 mm). Previous known values, such as fixture diameter and length, were used for calibration when the threads were not clearly visible on the radiographs. Measurements were taken to the nearest millimeter using computer software (UTHSCSA Image Tool, Version 3; University of Texas Health Science Center, San Antonio, Texas, U.S.). Changes at the MBL were evaluated for all of the mesial and distal aspects by subtracting the postoperative values from the respective baseline value (nΔMBL = nMBLBaseline − nMBL, with n as mesial or distal). MBL represented the mean of the values measured at the mesial and distal aspects, and ΔMBL represented the mean of the variation in values measured at the mesial and distal aspects.
- Facial soft-tissue level (FSTL) was evaluated, measuring the distance between the level of soft tissue at the midfacial gingival level and a reference line connecting the FSTL of the adjacent teeth. Facial soft-tissue changes were calculated by subtracting the baseline value from the respective postoperative values according to the formula ΔFSTL = FSTL − FSTLBaseline.
- Implant failure, such as implant mobility and removal of implants caused by progressive bone loss or infection: The stability of each implant was evaluated at the delivery of the prosthetic restoration and one and two years after implant insertion. The stability of each crown was ascertained with two metallic handles of dental instruments. Survival and success rates were calculated according to the criteria suggested by Buser et al.14Buser D, Weber HP, Lang NP. Tissue integration of non-submerged implants. 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants.
→ Clin Oral Implants Res. 1990 Dec;1(1):33–40.
Statistical analysis
Power analysis was employed to determine the sample size using a 0.05 significance level and a power of 80%, based on the results reported in a previous study concerning periimplant marginal bone loss.15Khayat PG, Arnal HM, Tourbah BI, Sennerby L. Clinical outcome of dental implants placed with high insertion torques (up to 176 Ncm).
→ Clin Implant Dent Relat Res. 2013 Apr;15(2):227–33. Sample size estimates, ranging from 23 to 168, were generated, comparing data on regular-IT and high-IT groups at the time of loading and after two years. A primary statistical evaluation was performed with multiway analysis of variance and multiple regression analysis (Database Toolbox and Statistics Toolbox, MatLab 7.0.1, MathWorks, Natick, Mass., U.S.). Post-hoc comparisons were performed with a t-test and the confidence interval was set at 95% (Statistics Toolbox). The level of statistical significance (p-value) was set at 0.05 for all analyses.
Results
One hundred and twenty implants were considered eligible for this study. Four patients were excluded (two required bone augmentation at the time of implant insertion; one refused to attend the recall visits; and one had excessive IT at the time of implant placement, so the osteotomy had to be widened with a countersink bur before implant insertion). The remaining 116 patients were allocated to two groups (58 to the regular-IT and 58 to the high IT group), according to a randomization process. Each patient received one implant and the experimental sites were followed for two years. The patients’ mean age at the time of the surgery was 51.5 ± 8.2 years in the regular-IT group and 51.3 ± 8.2 years in the high-IT group. Implants were inserted both in the maxilla and in the mandible, showing a homogenous distribution between the lower and upper jaws. Most of the sites were located in the premolar area, both for the regular-IT (29 implants) and for the high-IT (36 implants). The mean IT registered at the time of implant insertion was 30.3 ± 7.5 N cm for the regular-IT group and 68.8 ± 9.0 N cm for the high-IT group. The implant distribution is shown in Table 1.
-

- Fig. 2

-

- Fig. 3
-
- Fig. 4

-
- Fig. 5
-

- Fig. 6

-
- Fig. 7
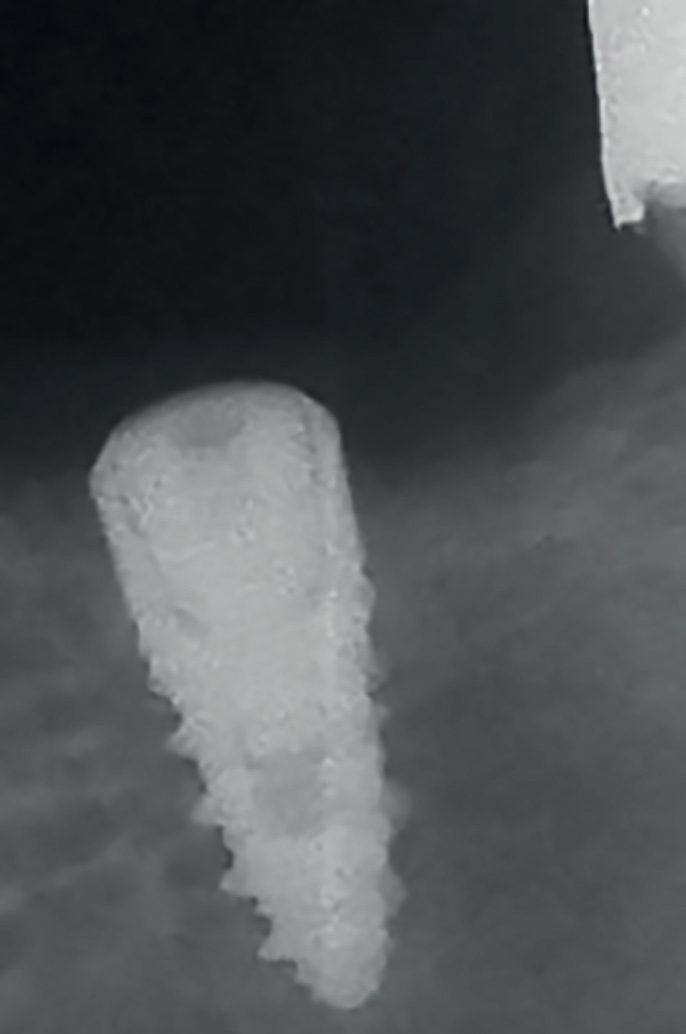
High-IT group: implant inserted in the maxilla, radiograph at baseline.Figs. 3
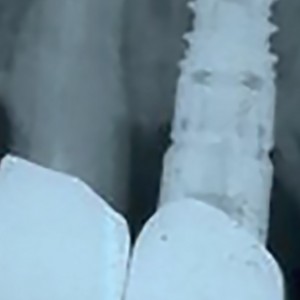
Regular-IT group: implant inserted in the mandible, radiograph at baseline.Figs. 4
High-IT group: implant inserted in the maxilla, radiograph at 12 months.Figs. 5
Regular-IT group: implant inserted in the mandible, radiograph at 12 months.
Figs. 6
High-IT group: implant inserted in the maxilla, radiograph at 24 months.
Figs. 7
Regular-IT group: implant inserted in the mandible, radiograph at 24 months.
After 24 months, one implant in the regular- IT group and three implants in the high-IT group were considered failures, since it was necessary to remove and replace the implants. The survival rate recorded in the regular-IT group was 98.2%, while in the high-IT group it was 94.8%.
The implant success rate was established according to Buser et al.,14 considering a marginal bone loss > 1.5 mm at 12 months a failure criterion. On that basis, after two years, one implant in the regular-IT group could not be considered successful, and the cumulative success rate in this group was 98.2%. In the high-IT group, the cumulative success rate was significantly lower (93.1%), since four implants did not fulfil the success criteria.
The MBL values were homogeneous at baseline between the two groups, as they depended on the final position of the implants in the healed bone ridges decided by the surgeon. The MBL values at baseline (maxilla: 0.14 ± 0.47 mm in the high-IT group and 0.12 ± 0.39 mm in the regular-IT group; mandible: 0.10 ± 0.24 mm in the high-IT group and 0.06 ± 0.17 mm in the regular-IT group) attested that the fixture platform was positioned at the bone crest level both in the maxilla and in the mandible (Figs. 2 & 3). Regarding the maxillary MBL values, after one year, the bone levels had decreased in both groups, showing a significant difference between the regular- and high-IT groups (p = 0.0045; Figs. 4 & 5). The difference between the two groups was still significant at the 24-month follow- up, being -0.79 ± 0.38 mm in the high-IT group and -0.55 ± 0.31 mm in the regular-IT group (p = 0.0056; Figs. 6 & 7). The ΔMBL emphasized the difference between the two groups after two years, being -0.93 ± 0.57 mm in the high-IT group and -0.67 ± 0.43 mm in the regular-IT group in the maxilla at the 24-month recall. In particular, the ΔMBL at 24 months in the high-IT group showed a slight increase in the MBL compared with the 12-month time point, but the difference between the high- and regular-IT groups was still significant (p = 0.0095). Differences in the effects of the IT appeared even more evident in the mandible. After one year, the MBL in the high-IT group was -1.23 ± 0.36 mm, and after 24 months, it was -1.21 ± 0.36 mm, showing that the MBL remained quite stable between the one- and the two-year recall visits. The MBL in the high-IT group had decreased to 1.31 ± 0.33 mm at the two-year follow-up; this value was similar to the ΔMBL at 12 months, attesting that the bone ridge around the implants in the high-IT group remained stable after a remarkable decrease in the first year. The MBL and ΔMBL values in the regular-IT group were completely dissimilar from the high-IT group values in the mandible. The MBL was -0.63 ± 0.31 mm at the 12-month follow-up and -0.68 ± 0.30 mm after 24 months. After the first year, the marginal bone around the implants remained stable, registering a decrease of 0.75 ± 0.28 mm at 24 months (Table 2).
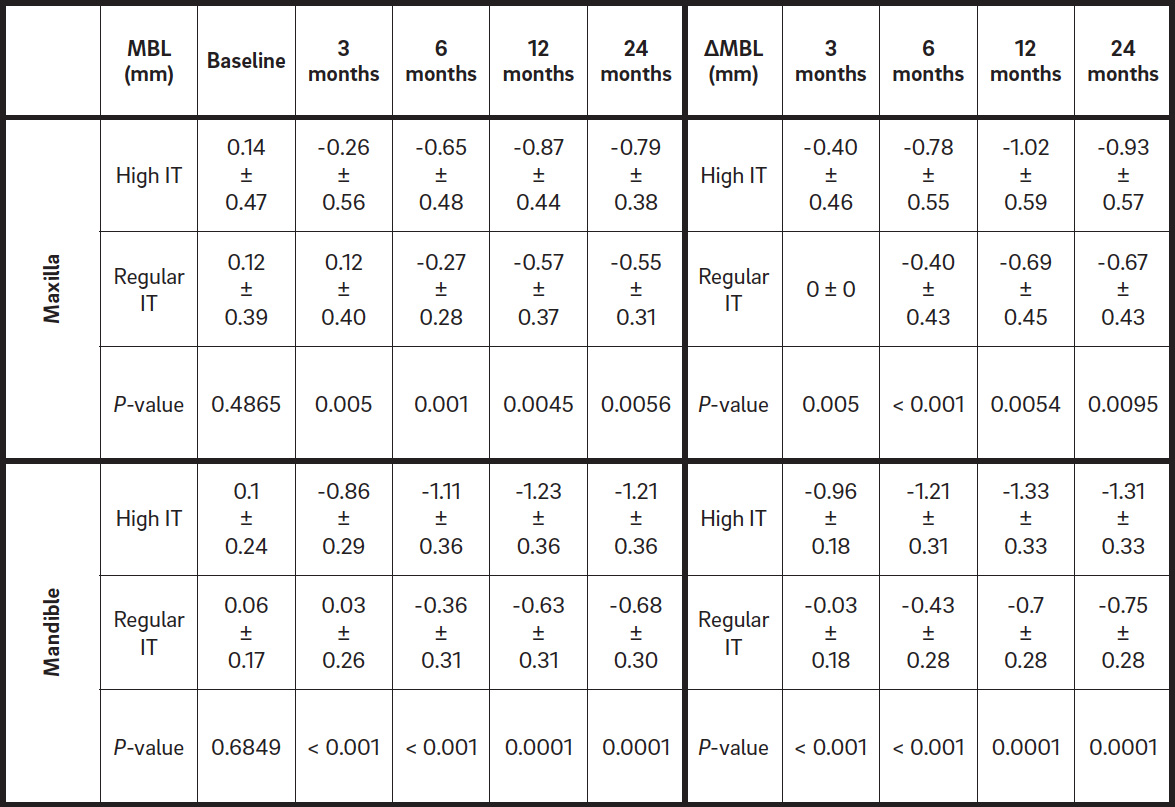
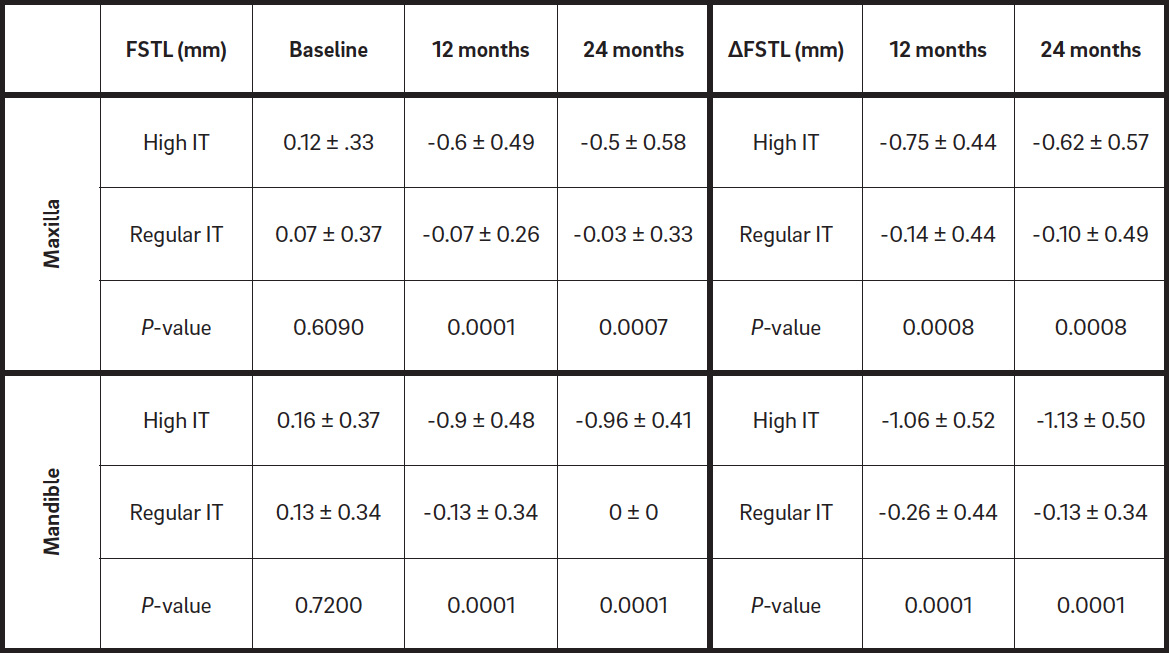
Table. 2
MBL (mean ± standard deviation) and ΔMBL at 24 months in the maxilla and mandible for the high- and regular-IT groups.
Table. 3
FSTL (mean ± standard deviation) and ΔFSTL at 24 months in the maxilla and mandible for the high- and regular-IT groups.
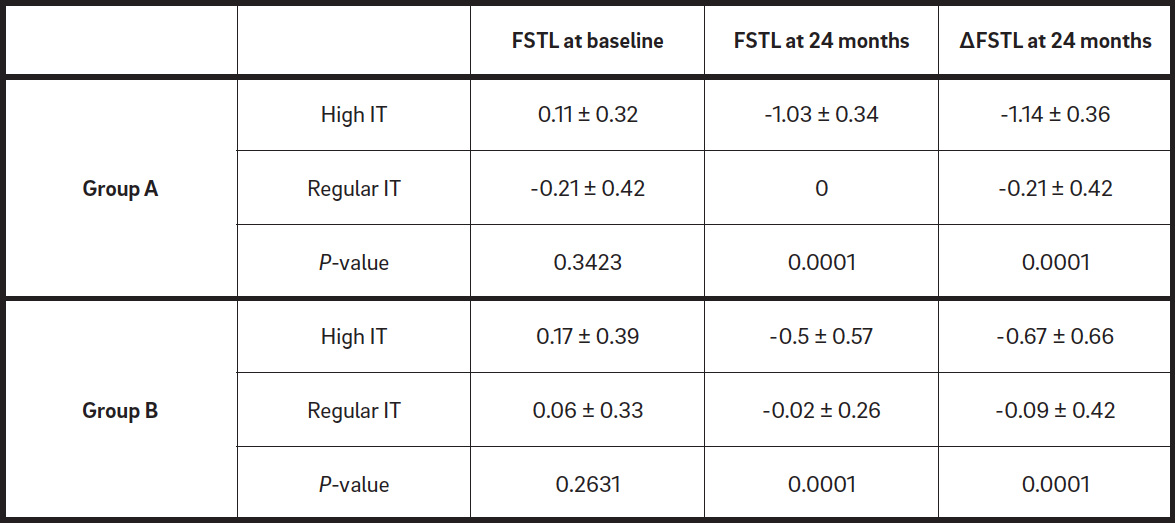
Table. 4
FSTL (mean ± standard deviation) and ΔFSTL (mean ± standard deviation) in sites with BBT < 1 mm (Group A) and BBT ≥ 1 mm (Group B) for the high- and regular-IT groups.
The FSTL values were analyzed in the mandible and maxilla in the high-IT and regular-IT groups (Table 3). In the maxilla, the FSTL values at baseline were homogeneous for the two groups. After one year, a decrease in FSTL was registered in both groups (-0.60 ± 0.49 mm in the high-IT group and -0.07 ± 0.26 mm in the regular-IT group), but at the 24-month recall, both the regular-IT group and the high-IT group showed a slight increase. Despite this, the difference between the two groups was significant at each time point. The ΔFSTL underlined the
one-year decrease and the two-year increase in the soft-tissue level, besides the clear differences between the two groups at each time point.
The FSTL values in the mandible showed a decrease in both groups after 12 months (-0.90 ± 0.48 mm in the high-IT group and -0.13 ± 0.34 mm in the regular-IT group). After two years, the high-IT group remained stable, while the regular-IT group showed an increase in FSTL. The difference in ΔFSTL between the regular-IT and high-IT groups was significant at the one-year follow-up and even more evident at the two-year follow-up.
The FSTL and ΔFSTL were also examined around implants, dividing the results into Group A and Group B according to the thickness of the buccal
bone after the osteotomy preparation, measured at the time of implant insertion (Table 4). The FSTL and ΔFSTL in the high-IT group showed differences between the values registered for Group A and in Group B. In fact, at the 24-month follow-up, the implants in Group A inserted with a high IT had greater soft-tissue recession (FSTL: -1.03 ± 0.34 mm; ΔFSTL: -1.15 ± 0.36 mm) compared with Group B (FSTL: -0.50 ± 0.57 mm; ΔFSTL: -0.67 ± 0.66 mm). Moreover, the BBT in the regular-IT group had an influence on facial soft-tissue behavior. In fact, the soft-tissue recession in Group A (-0.21 ± 0.42 mm) was greater than in Group B (-0.09 ± 0.42 mm) after two years.
Discussion
The clinical and radiographic outcome of implants inserted with a high IT (50–100 N cm) and regular IT (< 50 N cm) in healed ridges were compared in this study. The outcome variables considered were FSTL, measured clinically, and MBL, analyzed through radiographs. Also, the influence of BBT after implant osteotomy on the facial soft-tissue changes was investigated. The implant cumulative success rate was registered in each group and all experimental sites were followed for two years. Only one implant per patient was inserted, in order to exclude possible cluster effects on the implant outcome. Only nongrafted sites were included to eliminate the possible influence of a biomaterial previously grafted in the surgical sites, although implants inserted in grafted sites have been demonstrated to have survival rates similar to that of implants inserted in
nonaugmented sites.16Barone A, Orlando B, Tonelli P, Covani U. Survival rate for implants placed in the posterior maxilla with and without sinus augmentation: a comparative cohort study.
→ J Periodontol. 2011 Feb;82(2):219–26.17Needleman I, Chin S, O’Brien T, Petrie A, Donos N. Systematic review of outcome measurements and reference group(s) to evaluate and compare implant success and failure.
→ J Clin Periodontol. 2012 Feb;39 Suppl 12:122–32.
Measures were taken at baseline and at three, six, 12 and 24 months, providing the possibility of analyzing the outcomes after both the first and the second year of follow-up. This would help in studying the hard- and soft-tissue changes after implant loading.
The achievement of good primary stability when inserting an implant has been found to be important, mostly when applying an immediate loading protocol.18Degidi M, Daprile G, Piattelli A. Determination of primary stability: a comparison of the surgeon’s perception and objective measurements.
→ Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):558–61. A higher IT makes the clinician feel more comfortable while inserting an implant, as it appears to mimic implant primary stability.19Trisi P, Todisco M, Consolo U, Travaglini D. High versus low implant insertion torque: a histologic, histomorphometric, and biomechanical study in the sheep mandible.
→ Int J Oral Maxillofac Implants. 2011 Jul-Aug;26(4):837–49.20Norton MR. The influence of insertion torque on the survival of immediately placed and restored single-tooth implants.
→ Int J Oral Maxillofac Implants. 2011 Nov-Dec;26(6):1333–43.
In the present study, implants inserted with an IT that exceeded 50 N cm had more pronounced periimplant bone resorption and soft-tissue recession than implants with an IT within 50 N cm, and this result was more evident in the mandible. These findings are in line with that of other studies.21Grandi T, Garuti G, Guazzi P, Tarabini L, Forabosco A. Survival and success rates of immediately and early loaded implants; 12-month results from a multicentric randomized clinical study.
→ J Oral Implantol. 2012 Jun;38(3):239–49. In fact, implants inserted in the anterior maxilla with a high IT (ranging from 50 N cm to 80 N cm), immediately or early loaded, and followed for one year showed significant differences between the bone resorption at each time point.22 Grandi T, Garuti G, Guazzi P, Tarabini L, Forabosco A. Survival and success rates of immediately and early loaded implants; 12-month results from a multicentric randomized clinical study.
→ J Oral Implantol. 2012 Jun;38(3):239–49.
However, a recent systematic review analyzing bone resorption, implant failure and boneimplant contact found no significant differences between implants inserted with a high or low IT.23Berardini M, Trisi P, Sinjari B, Rutjes AW, Caputi S. The effects of high insertion torque versus low insertion torque on marginal bone resorption and implant failure rates: a systematic review with meta-analyses.
→ Implant Dent. 2016 Aug;25(4):532–40. The same review stated that there is poor evidence regarding the correlation between excessive bone compression and bone resorption, but there is still no clear statement about the minimum IT necessary to obtain clinical success, even when considering immediate loading.24Berardini M, Trisi P, Sinjari B, Rutjes AW, Caputi S. The effects of high insertion torque versus low insertion torque on marginal bone resorption and implant failure rates: a systematic review withmeta-analyses.
→ Implant Dent. 2016 Aug;25(4):532–40.
As the soft-tissue appearance significantly influences the esthetics of implants, its treatment is of great importance, although more research on the behavior of soft tissue around dental implants is required.
In our findings, significant differences were observed in soft-tissue changes too. In the high- IT group, the FSTL significantly decreased after one year and remained quite stable at the two-year follow-up. In the regular-IT group, the FSTL remained stable for the one year, and then it seemed to gain soft tissue, the difference between the two groups becoming more evident, both in the maxilla and in the mandible. If we consider the BBT, recession of the FSTL seemed to be significantly influenced by a BBT < 1 mm. Differences were evident within both of the experimental groups. In fact, the ΔFSTL in the high- IT group at 24 months was -1.15 ± 0.36 mm for Group A and -0.67 ± 0.66 mm for Group B. The ΔFSTL in the regular-IT group at 24 months was -0.21 ± 0.42 mm in Group A and -0.09 ± 0.42 mm in Group B.
These results are in line with that of other studies, which found 0–1 mm gingival recession at the buccal side of implants placed in post-extractive sites and restored after three weeks.23 The same studies did not observe significant recession in sites with a thick gingival biotype; therefore, the FSTL seemed to be influenced not only by the bone but also by the tissue thickness.25Lops D, Romeo E, Chiapasco M, Procopio RM, Oteri G. Behaviour of soft tissues healing around single bone-level-implants placed immediately after tooth extraction. A 1 year prospective cohort study.
→ Clin Oral Implants Res. 2013 Nov;24(11):1206–13. The implants inserted in the present study were not immediately restored.
A key point of this study is the observation period: Two years is a relatively short follow-up in which to observe the behavior not only during the osseointegration period but also after the prosthesis delivery. Also, surgical sites were strictly selected, excluding the possible influence of bone augmentation; thus, only IT and BBT were studied. IT and bone resorption were measured via software, allowing precise and reliable comparisons.
Conclusion
The present randomized clinical trial analyzed the effect of IT on MBL and FSTL after two years. The effect of BBT on MBL after the implant osteo tomy was investigated too. Implants inserted with an IT > 50 N cm showed significantly more bone resorption; this was evident after one year, but became even more marked at the two-year follow-up. The FSTL showed more evident recession in the high-IT group after two years, especially in implants with a BBT < 1 mm after osteotomy. The findings of this study suggest that inserting implants with a high IT could be detrimental to soft- and hard-tissue outcome, even though the implant success rate was similar for the high-IT and regular-IT groups. Furthermore, the clinician should pay great attention during the preparation of the implant site, as a BBT > 1 mm could positively affect the longterm behavior of soft tissue. Although the randomization process lent reliability to the results, the findings of this study should be corroborated with a longer follow-up and a greater number of patients.
Competing interests
The authors declare that they have no competing interests.

Interview
with Alfonsi, Fortunato
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Campos FE, Jimbo R, Bonfante EA, Barbosa DZ, Oliveira MT, Janal MN, Coelho PG. Are insertion torque and early osseointegration proportional? A histologic evaluation. → Clin Oral Implants Res. 2015 Nov;26(11):1256–60. |
| 2. | ↑ | Szmukler-Moncler S, Salama H, Reingewirtz Y, Dubruille JH. Timing of loading and effect of micromotion on bone-dental implant interface: review of experimental literature. → J Biomed Mater Res. 1998 Summer;43(2):192–203. |
| 3. | ↑ | Duyck J, Roesems R, Cardoso MV, Ogawa T, De Villa Camargos G, Vandamme K. Effect of insertion torque on titanium implant osseointegration: an animal experimental study. → Clin Oral Implants Res. 2015 Feb;26(2):191–6. |
| 4. | ↑ | Freitas AC Jr, Bonfante EA, Giro G, Janal MN, Coelho PG. The effect of implant design on insertion torque and immediate micromotion. → Clin Oral Implants Res. 2012 Jan;23(1):113–8. |
| 5. | ↑ | Jimbo R, Anchieta R, Baldassarri M, Granato R, Marin C, Teixeira HS, Tovar N, Vandeweghe S, Janal MN, Coelho PG. Histomorphometry and bone mechanical property evolution around different implant systems at early healing stages: an experimental study in dogs. → Implant Dent. 2013 Dec;22(6):596–603. |
| 6. | ↑ | Bashutski JD, D’Silva NJ, Wang HL. Implant compression necrosis: current understanding and case report. → J Periodontol. 2009 Apr;80(4):700–4. |
| 7. | ↑ | Trisi P, Perfetti G, Baldoni E, Berardi D, Colagiovanni M, Scogna G. Implant micromotion is related to peak insertion torque and bone density. → Clin Oral Implants Res. 2009 May;20(5):467–71. |
| 8. | ↑ | Coelho PG, Takayama T, Yoo D, Jimbo R, Karunagaran S, Tovar N, Janal MN, Yamano S. Nanometer-scale features on micrometer-scale surface texturing: a bone histological, gene expression, and nanomechanical study. → Bone. 2014 Aug;65:25–32. |
| 9. | ↑ | Jimbo R, Tovar N, Marin C, Teixeira HS, Anchieta RB, Silveira LM, Janal MN, Shibli JA, Coelho PG. The impact of modified cutting flute implant design on osseointegration. → Int J Oral Maxillofac Surg. 2014 Jul;43(7):883–8. |
| 10. | ↑ | Ottoni JM, Oliveira ZF, Mansini R, Cabral AM. Correlation between placement torque and survival of single-tooth implants. → Int J Oral Maxillofac Implants. 2005 Sep-Oct;20(5):769–76. |
| 11. | ↑ | Suaid FA, Novaes AB Jr, Queiroz AC, Muglia VA, Almeida AL, Grisi MF. Buccal bone plate remodeling, after immediate implants with or without synthetic bone grafting and flapless surgery: a histomorphometric and fluorescence study in dogs. → Clin Oral Implants Res. 2014 Feb;25(2):e10–21. |
| 12. | ↑ | Teughels W, Merheb J, Quirynen M. Critical horizontal dimensions of interproximal and buccal bone around implants for optimal aesthetic outcomes: a systematic review. → Clin Oral Implants Res. 2009 Sep;20 Suppl 4:134–45. |
| 13. | ↑ | Schultz KF, Altman DG, Moher D; CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. → Trials [Internet]. 2010 Mar 24 [cited 2016 Nov 14];11:Article 32 [8 p.]. doi:10.1186/1745-6215-11-32. |
| 14. | ↑ | Buser D, Weber HP, Lang NP. Tissue integration of non-submerged implants. 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants. → Clin Oral Implants Res. 1990 Dec;1(1):33–40. |
| 15. | ↑ | Khayat PG, Arnal HM, Tourbah BI, Sennerby L. Clinical outcome of dental implants placed with high insertion torques (up to 176 Ncm). → Clin Implant Dent Relat Res. 2013 Apr;15(2):227–33. |
| 16. | ↑ | Barone A, Orlando B, Tonelli P, Covani U. Survival rate for implants placed in the posterior maxilla with and without sinus augmentation: a comparative cohort study. → J Periodontol. 2011 Feb;82(2):219–26. |
| 17. | ↑ | Needleman I, Chin S, O’Brien T, Petrie A, Donos N. Systematic review of outcome measurements and reference group(s) to evaluate and compare implant success and failure. → J Clin Periodontol. 2012 Feb;39 Suppl 12:122–32. |
| 18. | ↑ | Degidi M, Daprile G, Piattelli A. Determination of primary stability: a comparison of the surgeon’s perception and objective measurements. → Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):558–61. |
| 19. | ↑ | Trisi P, Todisco M, Consolo U, Travaglini D. High versus low implant insertion torque: a histologic, histomorphometric, and biomechanical study in the sheep mandible. → Int J Oral Maxillofac Implants. 2011 Jul-Aug;26(4):837–49. |
| 20. | ↑ | Norton MR. The influence of insertion torque on the survival of immediately placed and restored single-tooth implants. → Int J Oral Maxillofac Implants. 2011 Nov-Dec;26(6):1333–43. |
| 21. | ↑ | Grandi T, Garuti G, Guazzi P, Tarabini L, Forabosco A. Survival and success rates of immediately and early loaded implants; 12-month results from a multicentric randomized clinical study. → J Oral Implantol. 2012 Jun;38(3):239–49. |
| 22. | ↑ | Grandi T, Garuti G, Guazzi P, Tarabini L, Forabosco A. Survival and success rates of immediately and early loaded implants; 12-month results from a multicentric randomized clinical study. → J Oral Implantol. 2012 Jun;38(3):239–49. |
| 23. | ↑ | Berardini M, Trisi P, Sinjari B, Rutjes AW, Caputi S. The effects of high insertion torque versus low insertion torque on marginal bone resorption and implant failure rates: a systematic review with meta-analyses. → Implant Dent. 2016 Aug;25(4):532–40. |
| 24. | ↑ | Berardini M, Trisi P, Sinjari B, Rutjes AW, Caputi S. The effects of high insertion torque versus low insertion torque on marginal bone resorption and implant failure rates: a systematic review withmeta-analyses. → Implant Dent. 2016 Aug;25(4):532–40. |
| 25. | ↑ | Lops D, Romeo E, Chiapasco M, Procopio RM, Oteri G. Behaviour of soft tissues healing around single bone-level-implants placed immediately after tooth extraction. A 1 year prospective cohort study. → Clin Oral Implants Res. 2013 Nov;24(11):1206–13. |





Leave a Reply
Be the First to Comment!