Transcrestal sinus floor elevation performed twice with collagen sponges and using a sonic instrument
April 4, 2016 / Categories: Digital Dentistry, Implant Dentistry

Agabiti, Ivo

Botticelli, Daniele
The objective of this study was to describe a minimally invasive transcrestal modified technique for sinus floor elevation performed twice with a sonic instrument (Sonosurgery).
Introduction
After tooth extraction, shrinkage of the alveolar process is expected that may reach 50% of the original horizontal width.1Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. → Int J Periodontics Restorative Dent. 2003 Jul-Aug;23(4):313–24.
In the posterior maxilla, the resorption of the radicular portion of the sockets that may protrude into the sinus could yield a further bone volume reduction due to sinus pneumatization. In the molar area, the resorption is greater than in the premolar area, owing to the larger volume of the extraction sockets that requires more time to be filled by newly formed bone, thus allowing the time for sinus pneumatization.2Sharan A, Madjar D. Maxillary sinus pneumatization following extractions: a radiographic study. → Int J Oral Maxillofac Implants. 2008 Jan-Feb;23(1):48–56.
The maxillary sinus floor elevation technique with a lateral approach has been well described in literature.6Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. → J Oral Surg. 1980 Aug;38(8):613–6. This surgical approach was based on a previously unpublished technique presented by Tatum at the Alabama Birmingham meeting in 1976. The safety and reliability of the technique have received large consensus by clinicians and researchers. Several modifications of the sinus floor elevation technique have been subsequently proposed for the surgical procedures and grafting materials used. Many of the sinus floor elevation techniques include the use of grafting materials to fill the subantral space, aiming to maintain the volume created.
However, clinical studies on sinus floor elevation performed concomitantly with implant placement have shown that the establishment of an isolated space between the bone wall surface and the sinus mucosa, resulted in spontaneous formation of new bone, even without the use of grafting materials.7Ellegaard B, Kølsen-Petersen J, Baelum V. Implant therapy involving maxillary sinus lift in periodontally compromised patients. → Clin Oral Implants Res. 1997 Aug;8(4):305–15.8Ellegaard B, Baelum V, Kølsen-Petersen J. Non-grafted sinus implants in periodontally compromised patients: a time-to-event analysis. → Clin Oral Implants Res. 2006 Apr;17(2):156–64.9Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. → J Oral Surg. 1980 Aug;38(8):613–6.10Lundgren S, Anderson S, Gualini F, Sennerby L. Bone reformation with sinus membrane elevation: a new surgical technique for maxillary sinus floor augmentation. → Clin Implant Dent Relat Res. 2004 Sep;6(3):165–73. Moreover, the integrity of the sinus membrane is known to be a prerequisite for success of the technique because it prevents the shift of the grafted material inside the sinus cavity; shifting of the material may favor acute or chronic infective complications and possibly compromise bone regeneration.11Barone A, Santini S, Sbordone L, Crespi R, Covani U. A clinical study of the outcomes and complications associated with maxillary sinus augmentation. → Int J Oral Maxillofac Implants. 2006 Jan-Feb;21(1):81–5. Another technique frequently adopted for sinus floor elevation requires a crestal access,12Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. → J Clin Periodontol. 2008 Sep;35(8 Suppl):216–40. first carried out with the use of osteotomes and autologous bone as filler material.13Summers RB. A new concept in maxillary implant surgery: the osteotome technique. → Compendium. 1994 Feb;15(2):152, 154–6, 158 passim; quiz 162. The crestal approach may reduce the perforation of the sinus membrane (4.7%)14Toffler M. Osteotome-mediated sinus floor elevation: a clinical report. → Int J Oral Maxillofac Implants. 2004 Mar-Apr;19(2):266–73. compared with the lateral approach (44%).15Schwartz-Arad D, Herzberg R, Dolev E. The prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. → J Periodontol. 2004 Apr;75(4):511–6.
Several modifications of the crestal approach have been subsequently proposed, aiming to elevate the sinus floor while maintaining the integrity of the Schneiderian membrane. For this purpose, a variety of osteotomes, used with or without bone fillers,16Pjetursson BE, Rast C, Brägger U, Schmidlin K, Zwahlen M, Lang NP. Maxillary sinus floor elevation using the (transalveolar) osteotome technique with or without grafting material. Part I: implant survival and patients’ perception. → Clin Oral Implants Res. 2009 Jul;20(7):667–76.’ 17Pjetursson BE, Ignjatovic D, Matuliene G, Brägger U, Schmidlin K, Lang NP. Transalveolar maxillary sinus floor elevation using osteotomes with or without grafting material. Part II: radiographic tissue remodeling. → Clin Oral Implants Res. 2009 Jul;20(7):677–83. or drills designed to avoid membrane perforation,18Cosci F, Luccioli M. A new sinus lift technique in conjunction with placement of 265 implants: a 6-year retrospective study. → Implant Dent. 2000 Winter;9(4):363–8. or the use of specific devices19Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32.’ 20Trombelli L, Franceschetti G, Stacchi C, Minenna L, Riccardi O, Di Raimondo R, Rizzi A, Farina R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or β-tricalcium phosphate: a multicenter, double-blind, randomized, controlled clinical trial. → J Clin Periodontol. 2014 Mar;41(3):311–9. Epub 2014 Jan 2. or ultrasonic instruments21Baldi D, Menini M, Pera F, Ravera G, Pera P. Sinus floor elevation using osteotomes or piezoelectric surgery. → Int J Oral Maxillofac Surg. 2011 May;40(5):497–503.’ 22Vercellotti T, De Paoli S, Nevins M. The piezoelectric bony window osteotomy and sinus membrane elevation: introduction of a new technique for simplification of the sinus augmentation procedure. → Int J Periodontics Restorative Dent. 2001 Dec;21(6):561–7. have been proposed. With the use of osteotomes, an elevation of the sinus membrane of up to 10 mm in total may be obtained without causing tearing.23Diserens V, Mericske E, Mericske-Stern R. Radiographic analysis of the transcrestal sinus floor elevation: short-term observations. → Clin Implant Dent Relat Res. 2005 Apr;7(2):70–8. Another modification of the transcrestal approach was proposed24Bruschi GB, Scipioni A, Calesini G, Bruschi E. Localized management of sinus floor with simultaneous implant placement:a clinical report. → Int J Oral Maxillofac Implants. 1998 Mar-Apr;13(2):219–26.25Winter AA, Pollack AS, Odrich RB. Placement of implants in the severely atrophic posterior maxilla using localized management of the sinus floor: a preliminary study. → Int J Oral Maxillofac Implants. 2002 Sep-Oct;17(5):687–95.26Winter AA, Pollack AS, Odrich RB. Sinus/alveolar crest tenting (SACT): a new technique for implant placement in atrophic maxillary ridges without bone grafts or membranes. → Int J Periodontics Restorative Dent. 2003 Nov-Dec;23(6):557–65. based on the principle of the edentulous ridge expansion technique.27Scipioni A, Bruschi GB, Calesini G. The edentulous ridge expansion technique: a five-year study. → Int J Periodontics Restorative Dent. 1994 Oct;14(5):451–60. This approach includes the use of a blade to perform the osteotomies and, subsequently, the use of blunt osteotomes.
The preservation of sinus walls appears to have an important role in bone formation in the sinus floor elevation procedure. In fact, in an experiment in monkeys on the early healing at elevated floor sinuses,28Scala A, Botticelli D, Rangel IG Jr, de Oliveira JA, Okamoto R, Lang NP. Early healing after elevation of the maxillary sinus floor applying a lateral access: a histological study in monkeys. → Clin Oral Implants Res. 2010 Dec;21(12):1320–6.’ 29Scala A, Botticelli D, Faeda RS, Rangel IG Jr, de Oliveira JA, Lang NP. Lack of influence of the Schneiderian membrane in forming new bone apical to implants simultaneously installed with sinus floor elevation: an experimental study in monkeys. → Clin Oral Implants Res. 2012 Feb;23(2):175–81. it was shown that new bone only originated from the bone walls and septa of the sinus. In that study, no evidence of bone formation was observed from the sinus mucosa, even though other studies have demonstrated that the Schneiderian membrane has the potential to produce bone.30Gruber R, Kandler B, Fuerst G, Fisher MB, Watzek G. Porcine sinus mucosa holds cells that respond to bone morphogenetic protein (BMP)-6 and BMP-7 with increased osteogenic differentiation in vitro. → Clin Oral Implants Res. 2004 Oct;15(5):575–80.31Srouji S, Kizhner T, Ben David D, Riminucci M, Bianco P, Livne E. The Schneiderian membrane contains osteoprogenitor cells: in vivo and in vitro study. → Calcif Tissue Int. 2009 Feb;84(2):138–45.32Srouji S, Ben-David D, Lotan R, Riminucci M, Livne E, Bianco P. The innate osteogenic potential of the maxillary sinus (Schneiderian) membrane: an ectopic tissue transplant model simulating sinus lifting. → Int J Oral Maxillofac Surg. 2010 Aug;39(8):793–801.33Srouji S, Ben-David D, Funari A, Riminucci M, Bianco P. Evaluation of the osteoconductive potential of bone substitutes embedded with Schneiderian membrane- or maxillary bone marrow- derived osteoprogenitor cells. → Clin Oral Implants Res. 2013 Dec;24(12):1288–94. A minimum height of 4–6 mm of the sinus floor has been suggested to guarantee the stability of the implant and, consequently, the success of the crestal access for sinus elevation.34Summers RB. A new concept in maxillary implant surgery: the osteotome technique. → Compendium. 1994 Feb;15(2):152, 154–6, 158 passim; quiz 162.’ 35Zitzmann NU, Schärer P. Sinus elevation procedures in the resorbed posterior maxilla: comparison of the crestal and lateral approaches. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Jan;85(1):8–17.36Chao YL, Chen HH, Mei CC, Tu YK, Lu HK. Meta-regression analysis of the initial bone height for predicting implant survival rates of two sinus elevation procedures. → J Clin Periodontol. 2010 May;37(5):456–65.37Bernardello F, Righi D, Cosci F, Bozzoli P, Soardi CM, Spinato S. Crestal sinus lift with sequential drills and simultaneous implant placement in sites with <5 mm of native bone: a multicenter retrospective study. → Implant Dent. 2011 Dec;20(6):439–44.38He L, Chang X, Liu Y. Sinus floor elevation using osteotome technique without grafting materials: a 2-year retrospective study. → Clin Oral Implants Res. 2013 Aug;24 Suppl A100:63–7.39Kang T. Sinus elevation using a staged osteotome technique for site development prior to implant placement in sites with less than 5 mm of native bone: a case report. → Int J Periodontics Restorative Dent. 2008 Jan-Feb;28(1):73–81. When the primary stability of an implant cannot be guaranteed, a two-stage approach may be followed and implant placement would have to be postponed for several months, depending on the quality of the filler material used.40Zitzmann NU, Schärer P. Sinus elevation procedures in the resorbed posterior maxilla: comparison of the crestal and lateral approaches. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Jan;85(1):8–17.41Chao YL, Chen HH, Mei CC, Tu YK, Lu HK. Meta-regression analysis of the initial bone height for predicting implant survival rates of two sinus elevation procedures. → J Clin Periodontol. 2010 May;37(5):456–65.42Bernardello F, Righi D, Cosci F, Bozzoli P, Soardi CM, Spinato S. Crestal sinus lift with sequential drills and simultaneous implant placement in sites with <5 mm of native bone: a multicenter retrospective study. → Implant Dent. 2011 Dec;20(6):439–44.43He L, Chang X, Liu Y. Sinus floor elevation using osteotome technique without grafting materials: a 2-year retrospective study. → Clin Oral Implants Res. 2013 Aug;24 Suppl A100:63–7.44Kang T. Sinus elevation using a staged osteotome technique for site development prior to implant placement in sites with less than 5 mm of native bone: a case report. → Int J Periodontics Restorative Dent. 2008 Jan-Feb;28(1):73–81. A twostage procedure has also been described for sinus floor elevation through a crestal access using blades, osteotomes and a mallet.45Bruschi GB, Scipioni A, Calesini G, Bruschi E. Localized management of sinus floor with simultaneous implant placement:a clinical report. → Int J Oral Maxillofac Implants. 1998 Mar-Apr;13(2):219–26. The aim of the present study is to describe a minimally invasive two-stage technique for sinus floor elevation through a crestal access, using in both stages a trapdoor prepared with the Sonosurgery system.
Materials & methods
The case of a patient who required oral rehabilitation by means of implants in the posterior maxillary area and presented with a widely pneumatized sinus was chosen to present the step-bystep procedure of the technique. The height of the sinus floor ranged between 2 mm and 4 mm, depending on the outline of the base of the sinus. It was not possible to guarantee implant primary stability; thus, a two-stage approach was followed (Figs. 1a–c). Micro-cone beam computed tomography (CBCT) scans (Kodak 9000, Carestream Health, Rochester, N.Y., U.S.) were taken before surgery.

First stage of sinus floor elevation
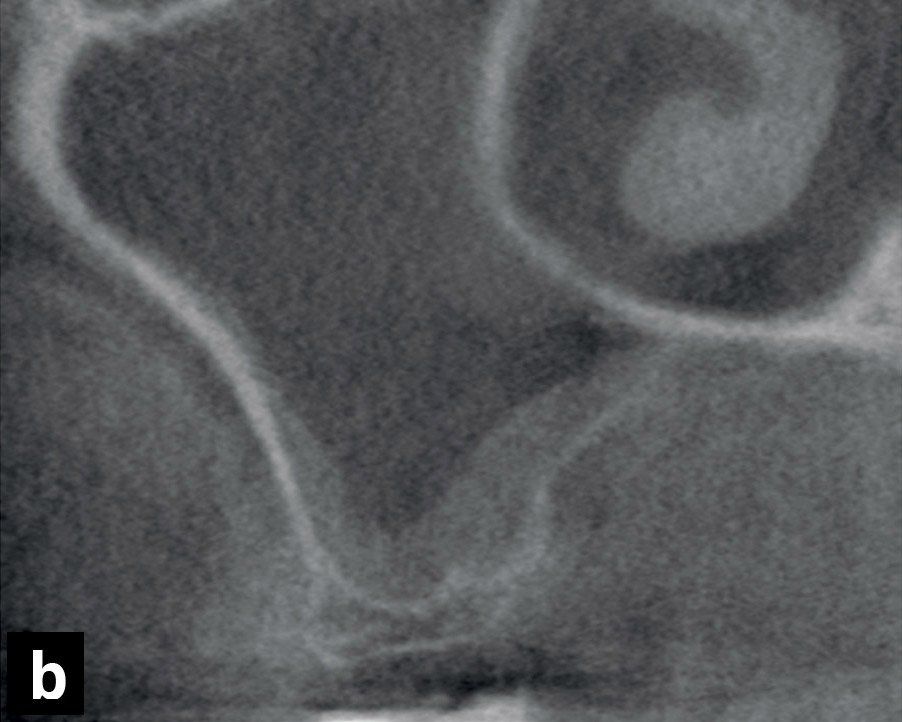
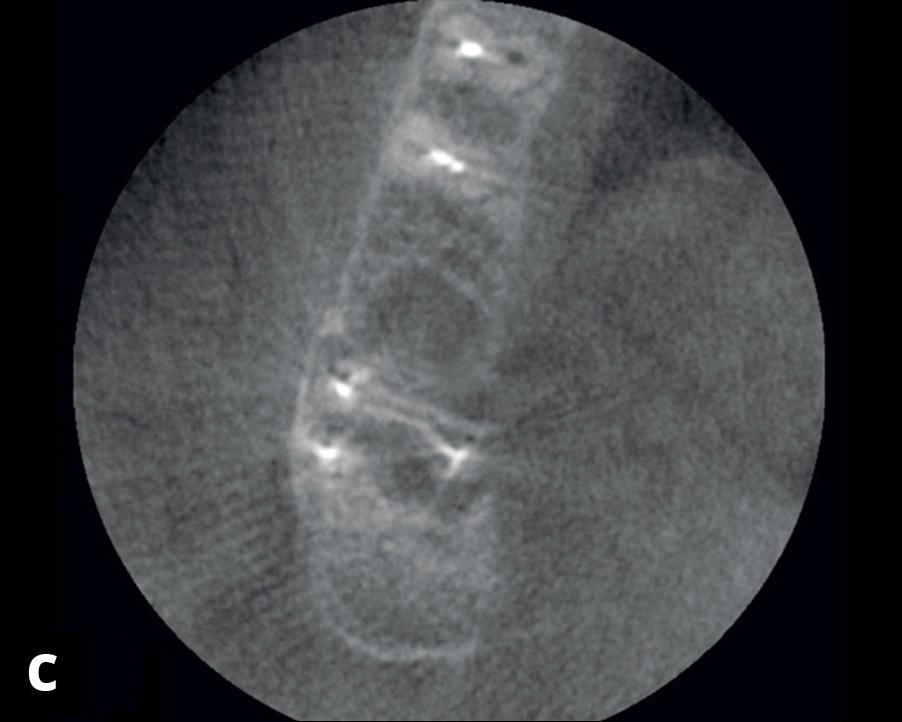
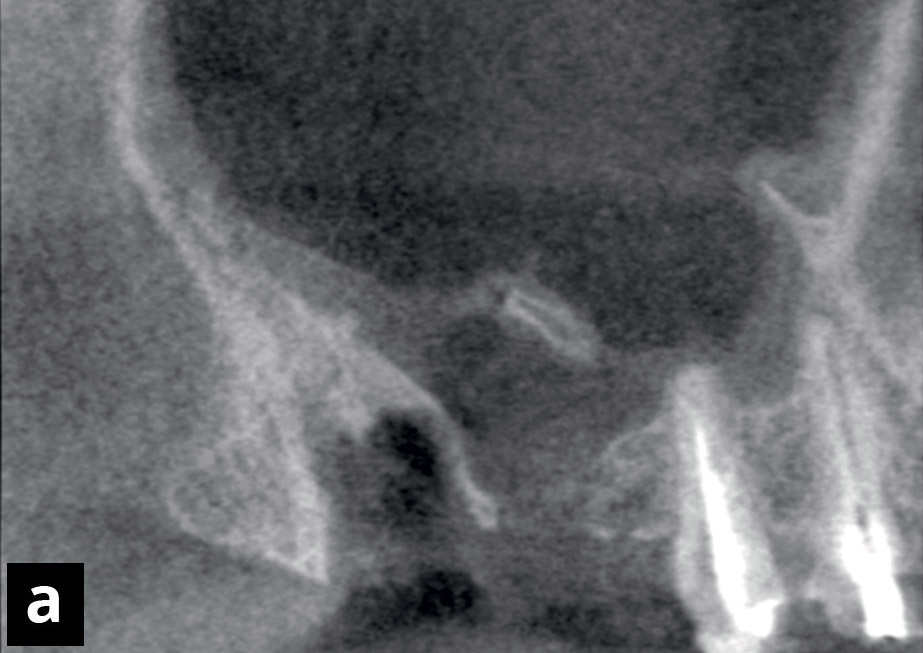
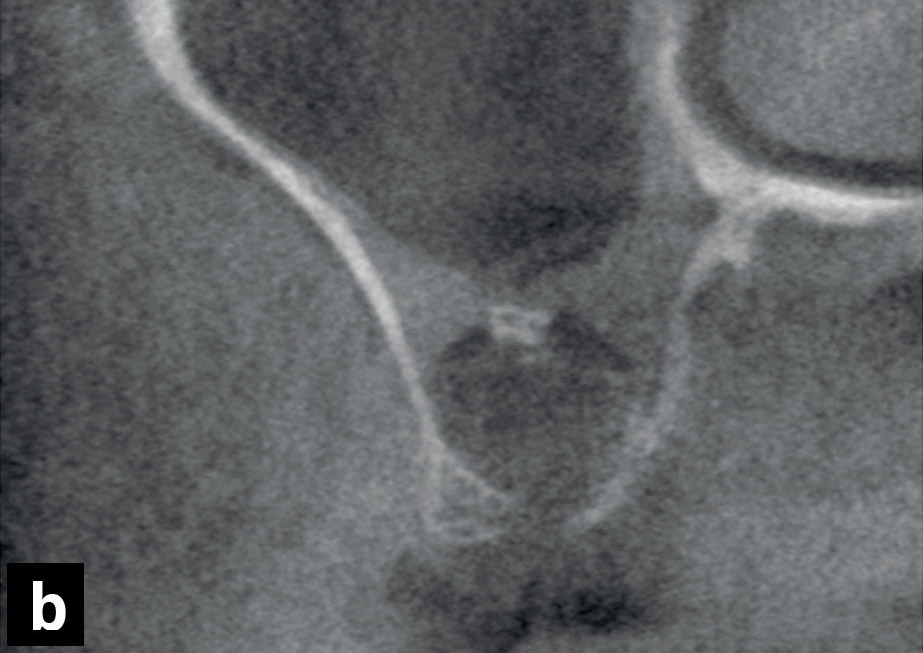
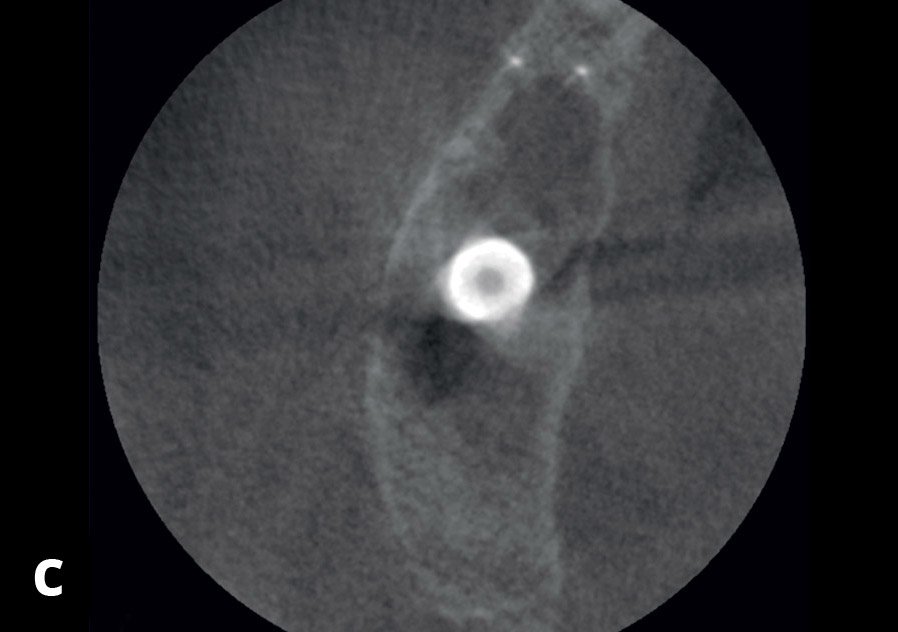
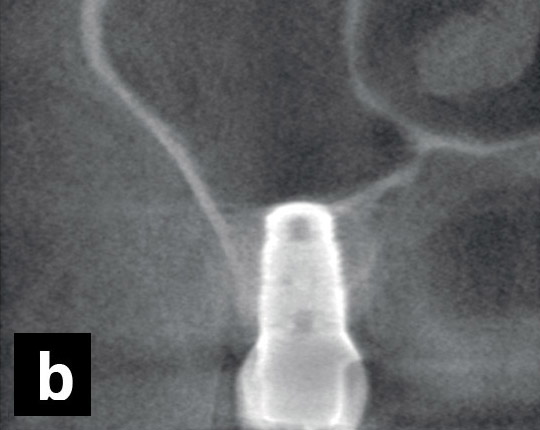
First sinus floor elevation stage in the three planes. In the initial CBCT scan, a fracture of the second molar and a periapical radiolucency were observed. The insufficient sinus floor height in the first molar position did not allow for immediate implant placement.
(a) Panoramic view.
(b) Cross-sectional view.
(c) Axial view.
Figs. 2a–f
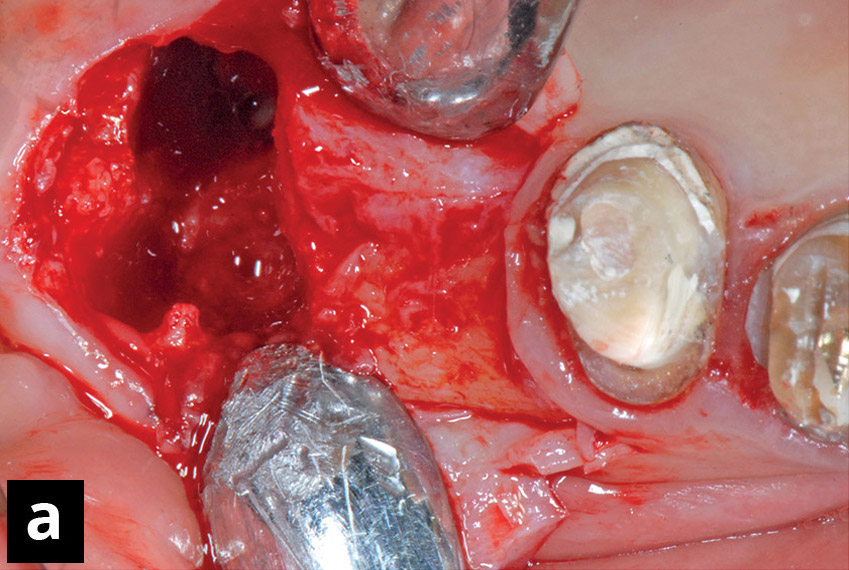
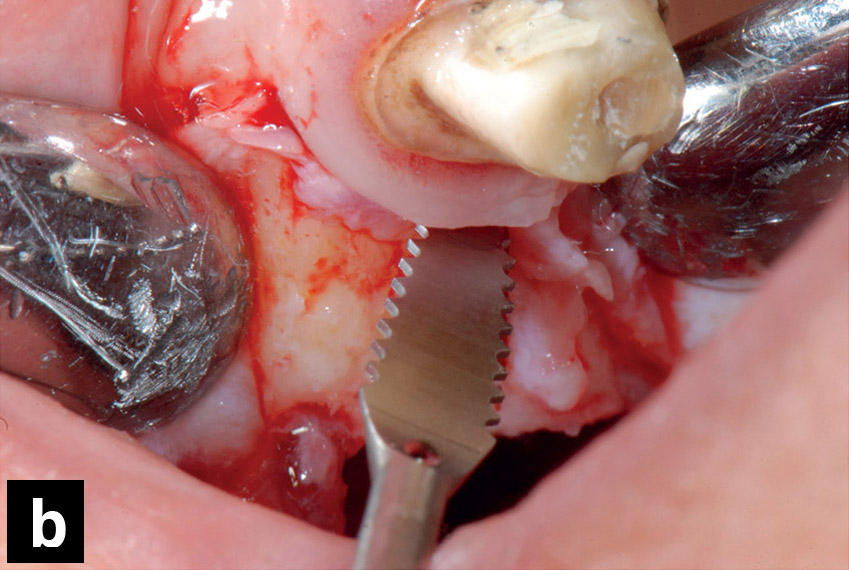
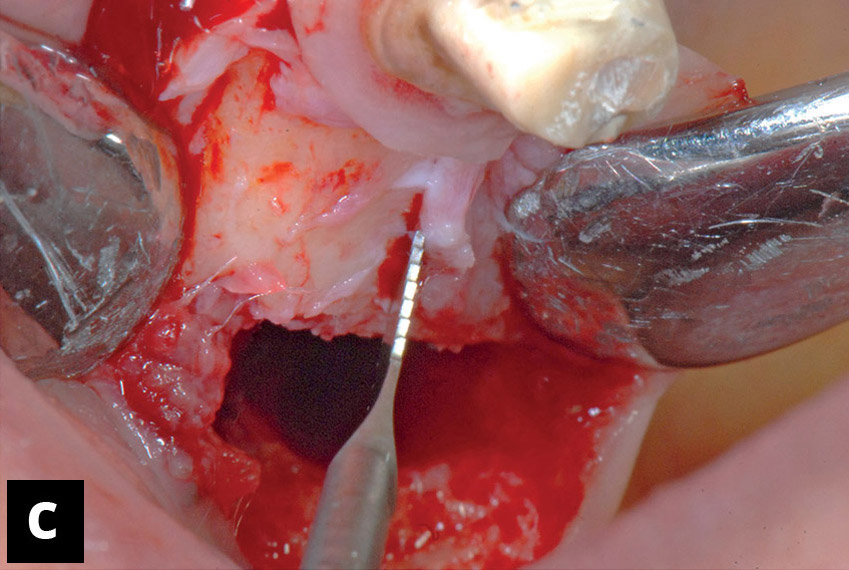
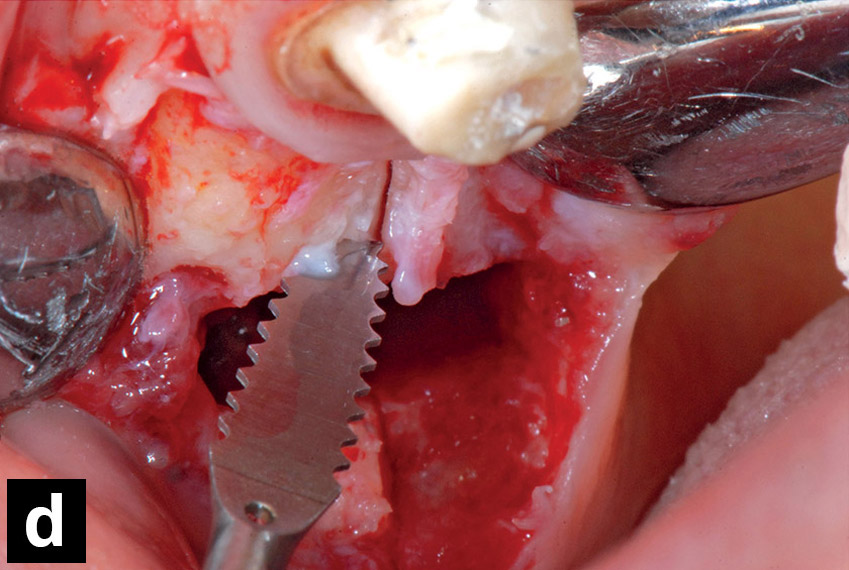
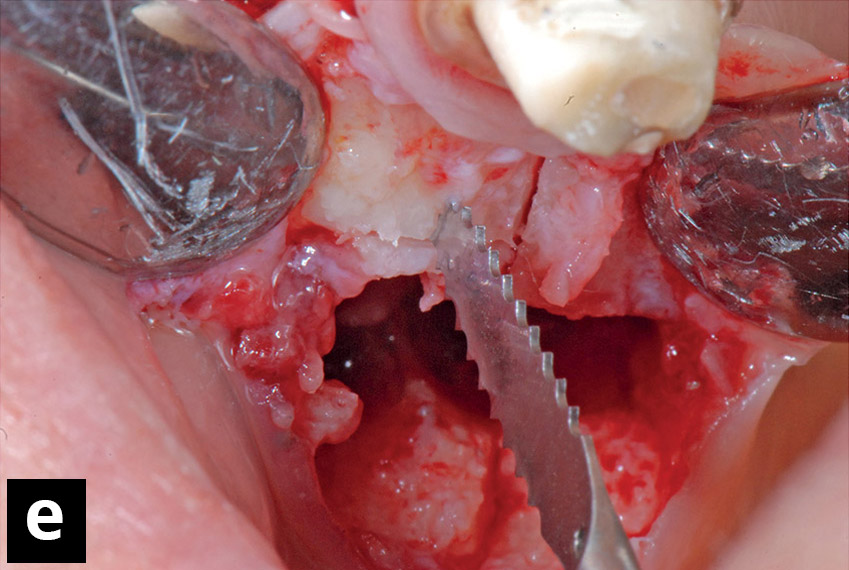
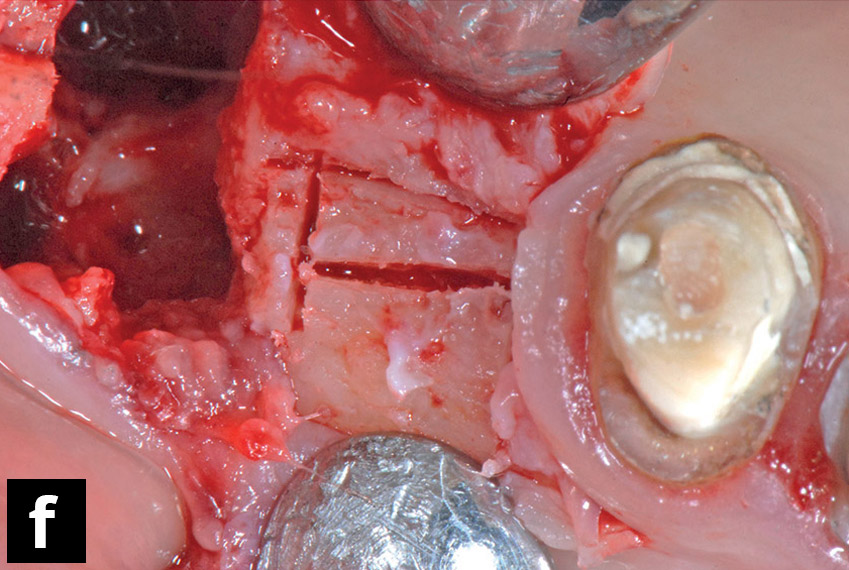
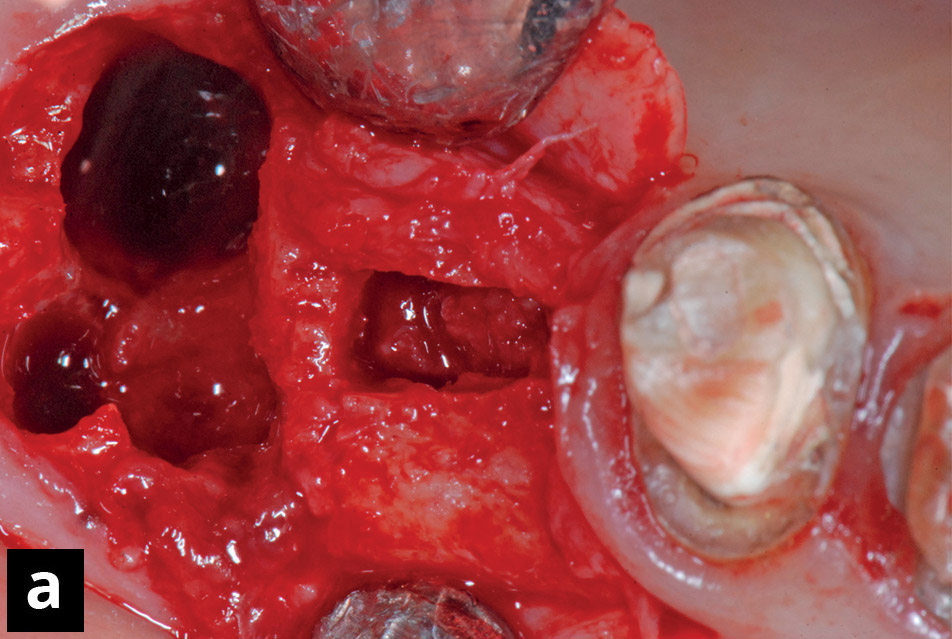
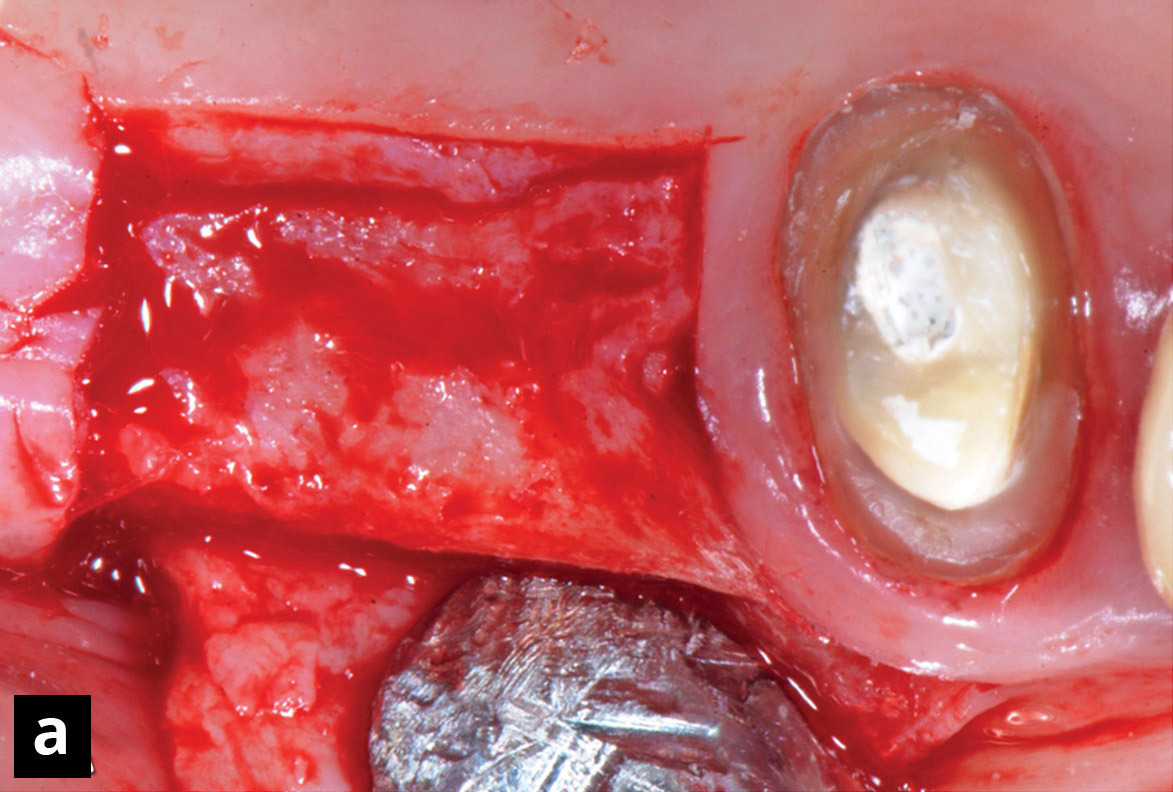
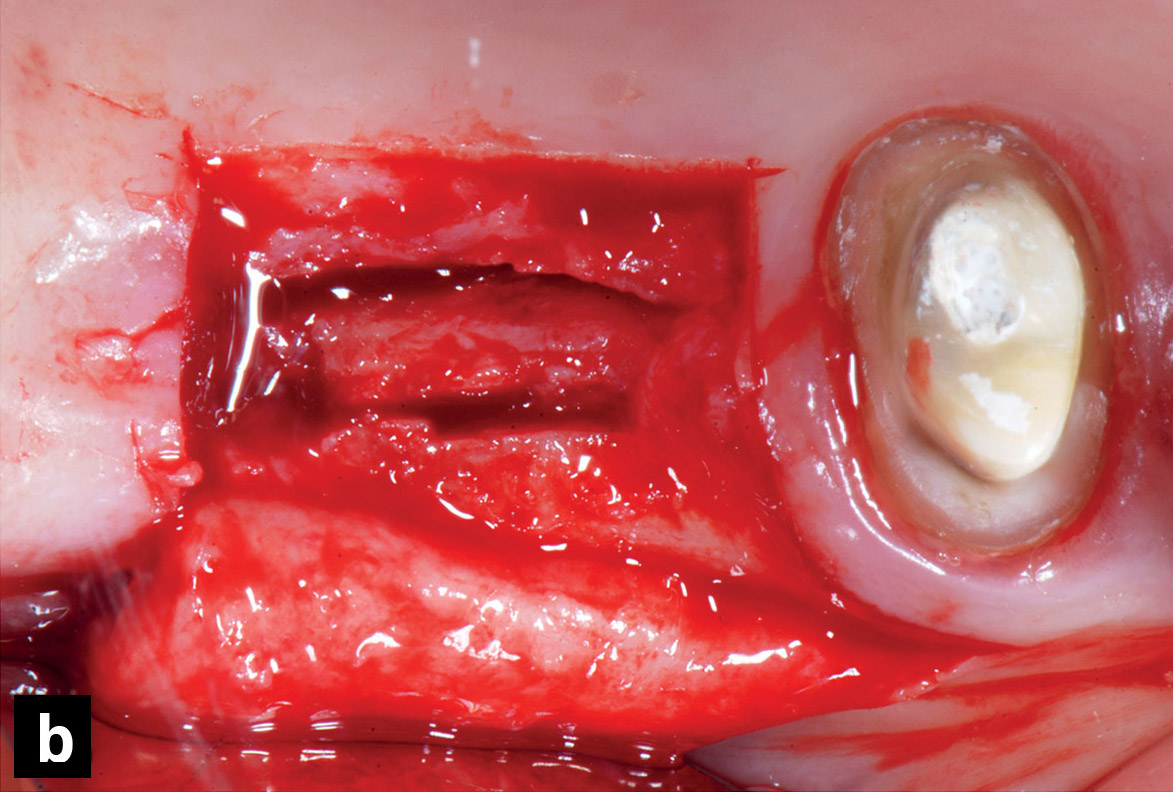
Clinical view of the surgical procedures. (a) Site after flap dissection and extraction of the first molar. The osteotomies were performed with an external bevel using a micro-saw 0.25 mm thick and exercising minimal pressure. The bevel cuts were orientated (b) mesially, (c) palatally, (d) distally, and (e) buccally, respectively. (f) The osteotomies of the trapdoor were finalized.
Figs. 3a–c
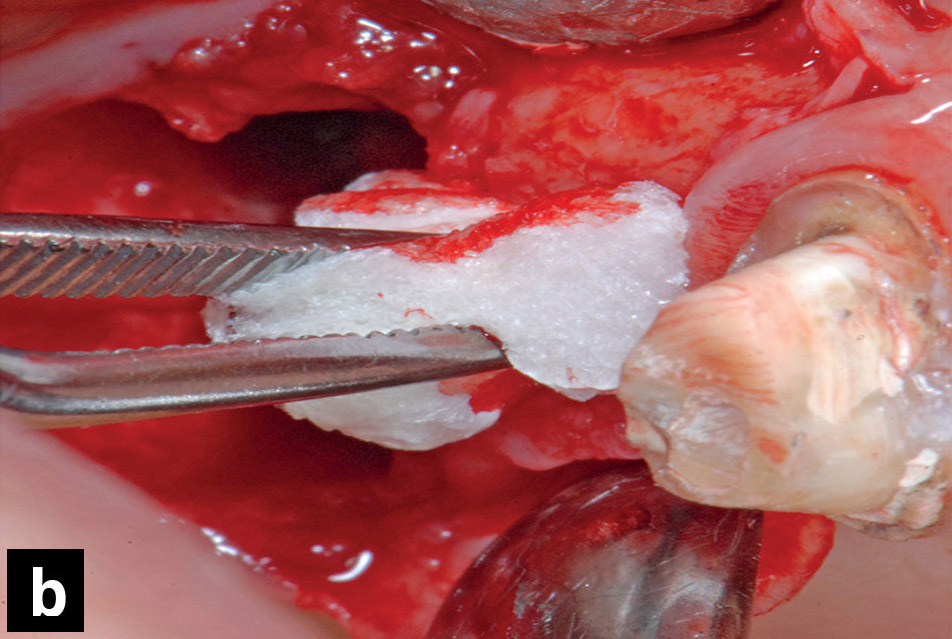
(a) The elevation of the trapdoor and of the sinus floor was performed with a surgical mallet on blunt chisels.
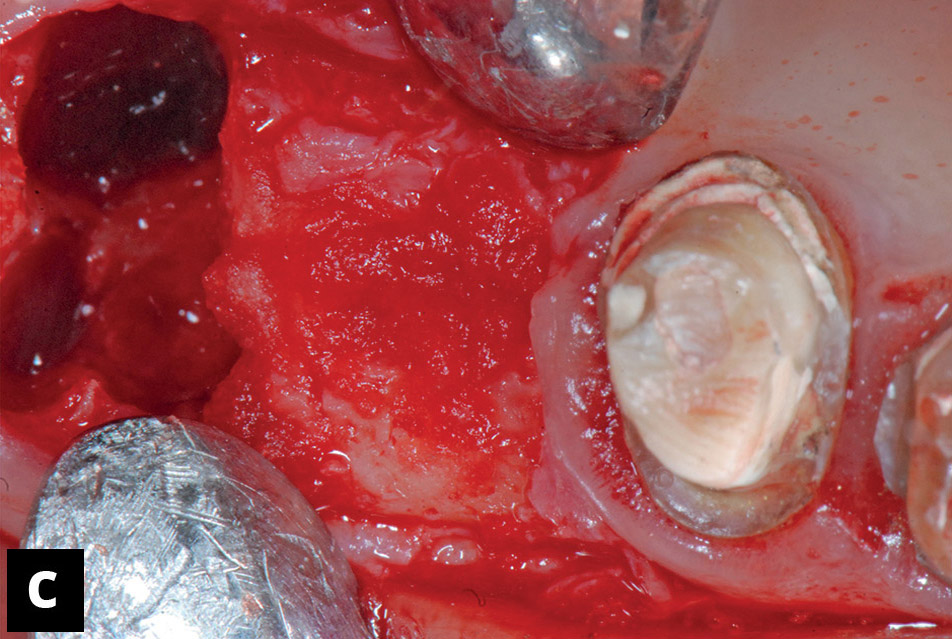
(b) Collagen sponges were placed into the space obtained, and these were subsequently pushed within the subantral space using the blunt chisels and mallet.
(c) Situation after the placement of collagen sponges.
Figs. 4a–c
A CBCT scan was taken immediately after the surgery.
(a) Panoramic view.
(b) Cross-sectional view.
(c) Axial view.
A split-thickness flap was dissected using a scalpel blade (BD Beaver 376400, BD Medical Ophthalmic Systems, Waltham, Mass., U.S.). A longitudinal incision was performed on the alveolar crest 3–4 mm palatal to the center of the crest. Short paramarginal releasing incisions were performed mesially (Fig. 2a). The dissection of the flap at the buccal aspect was extended up to the mucogingival junction, leaving only a thin layer of connective tissue on the bone surface in order to better visualize the bony crest morphology. After flap elevation, a bone trapdoor was prepared with the use of a vibrating sonic handpiece (Sonosurgery, TeKne Dental, Calenzano, Italy) into which a straight micro-saw (SFS 102, Komet Dental Gebr. Brasseler, Lemgo, Germany) had been inserted. The trapdoor was produced in the center of the alveolar crest and was < 2.5 mm wide in the buccolingual plane. The bone incision was extended in a mesiodistal direction for the entire edentulous area to be treated. However, a safe distance of about 1.5 mm from the premolar was maintained to avoid damaging the root (Figs. 2b–f).
The osteotomy of the bone trapdoor was performed with a micro-saw 0.25 mm thick and exercising minimal pressure, similar to that of a pencil when writing (a maximum of 2–3 N). These incisions on the bone were performed with an external bevel, so that the bone trapdoor had a trapezoidal cross-section, the largest base being at the cranial and the smallest at the caudal aspect of the trapdoor. A continuous movement along the incisions had to be carried out by the operator using the sonic insert, gradually penetrating into the bone, until a distinct change of material texture was perceived, indicating that the base of the sinus had been reached. After that, the trapdoor was released along the osteotomies using a surgical mallet on blunt chisels (KLS Martin Group, Umkirch, Germany) with gentle taps (Fig. 3a). Collagen sponges (Gingistat, GABA VEBAS, Rome, Italy) were placed into the space obtained in order to prevent the Schneiderian membrane from tearing, and these were subsequently pushed within the subantral space using the blunt chisels and mallet (Figs. 3b & c). The 3-D hydraulic pressure produced by the collagen soaked with blood encouraged the sinus membrane detachment from the bone walls. After sinus elevation, the buccal flap was repositioned and sutured to the palatal aspect, allowing a primary intention wound closure. A CBCT scan with a low radiation dose was taken immediately after the surgery (Figs. 4a–c). Intra-oral radiographs were taken one, two and three months after the first sinus elevation (Figs. 5a–c).
Second stage of sinus floor elevation
Four months after the first surgical session, an intra-oral radiograph was taken and assessed (Fig. 5d). The radiographs showed that the base of the sinus had gained about 3–4 mm in height compared with the original situation, yielding a total height of about 5–6 mm, which could allow for primary implant stability. No clinical signs of inflammation were observed. A surgical procedure similar to that used in the first stage was performed, including the mucosal incision. Again, a buccolingual crestal osteotomy < 2.5 mm wide was made (Figs. 6a & b).
The augmented dimensions of the sinus floor compared with the initial situation allowed the execution of deeper osteotomies with more pronounced bevels than those carried out during the previous surgical stage. Consequently, the bone trapdoor was higher and wider in the cranial regions in comparison with that prepared in the first surgical stage.
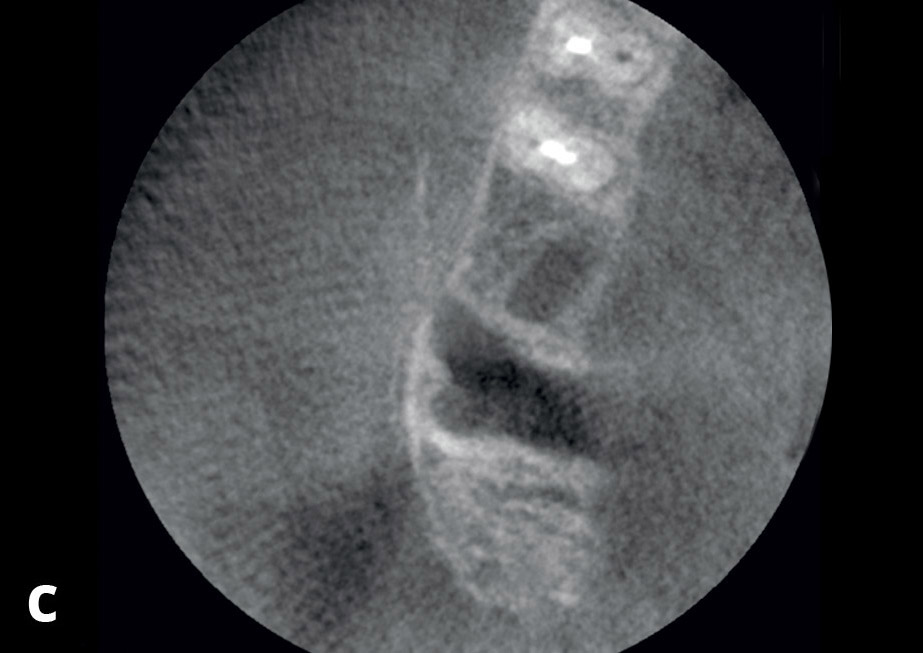
Chisels of increasing thickness were used to distract the bone toward the sinus, following the incisions made with the sonic micro-saw. This, in turn, meant that the chisels had a working direction with the same angulation as the osteotomies. Once the trapdoor had been split and mobilized by blunt chisels and a mallet, both buccally and palatally from the parent bone, collagen sponges were added and an implant with a conical shape (Pilot, Sweden & Martina, Due Carrare, Italy) was placed (Fig. 6c). The implant apex pushed the collagen and the bone further, producing an additional sinus floor elevation. Implant primary stability was obtained by means of the pressure of the implant collar on the walls of the access. The buccal and lingual flaps were sutured with apical repositioning at the buccal aspect (Fig. 6d). A low-dose CBCT scan was taken immediately after the second surgery (Figs. 7a–c).
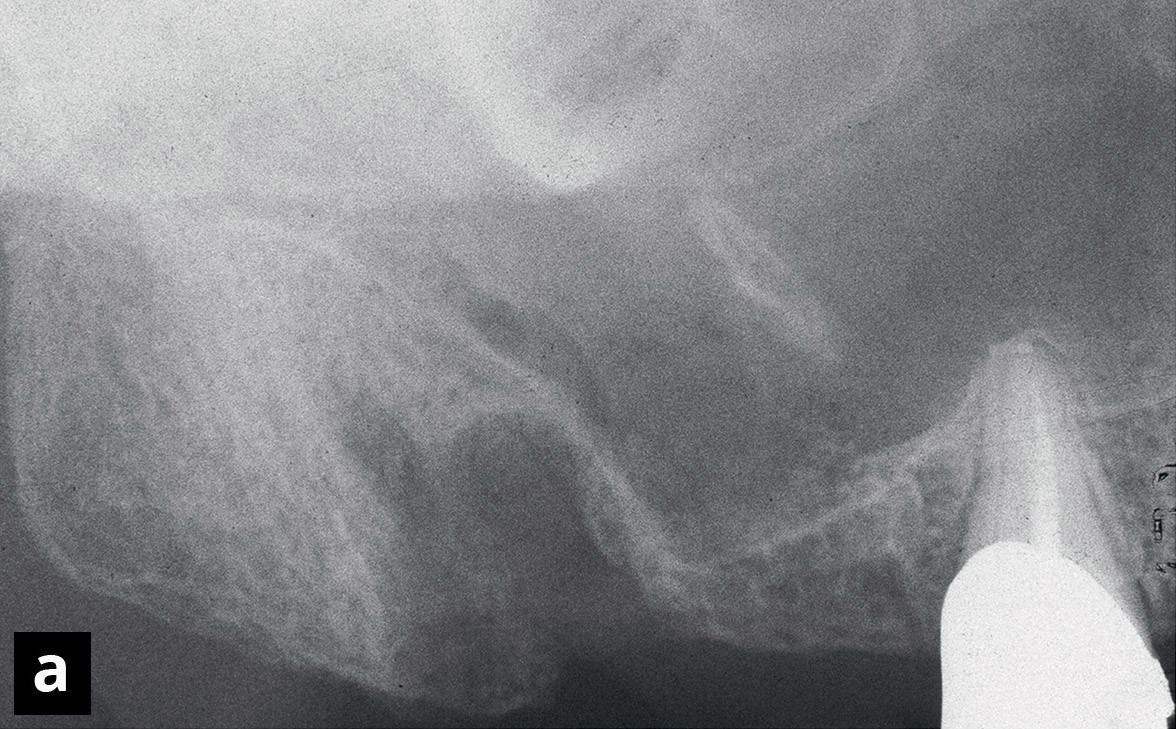
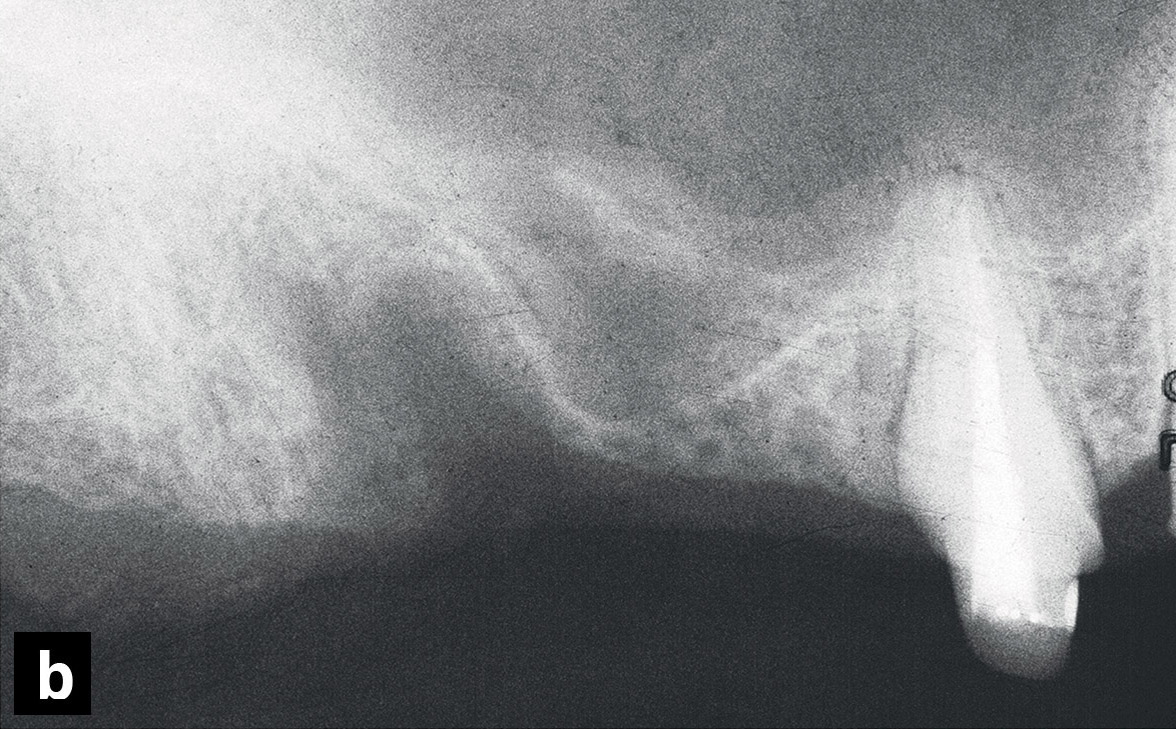
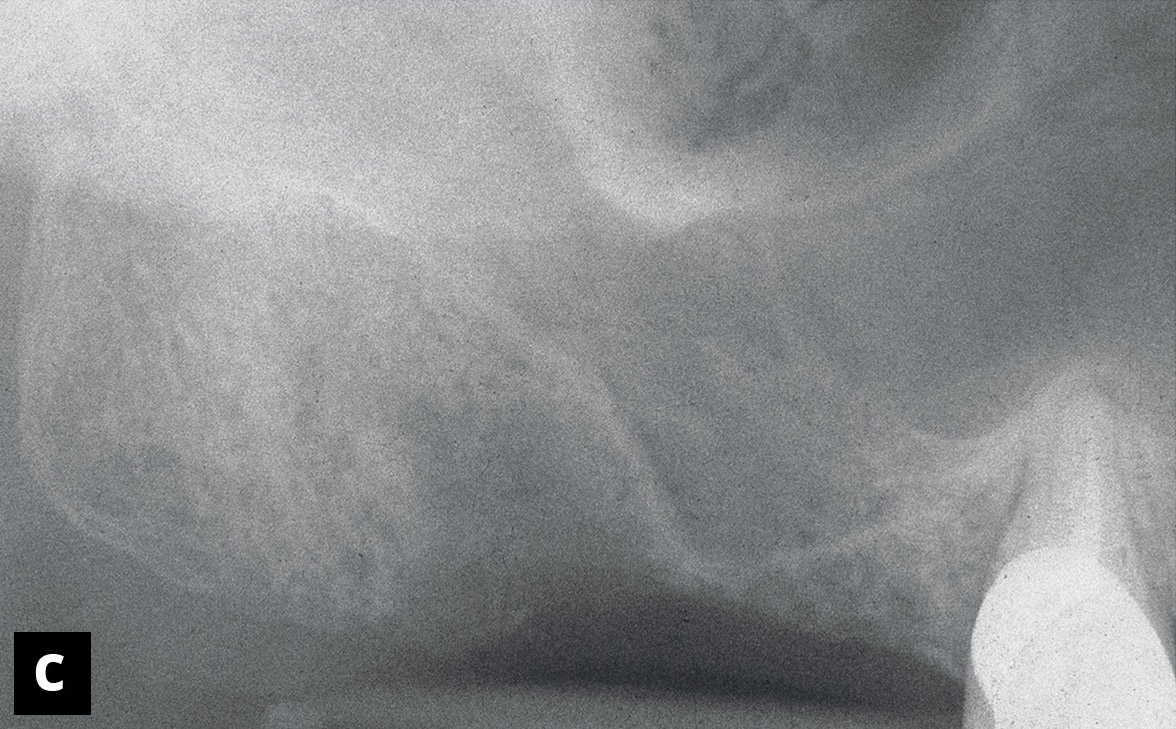
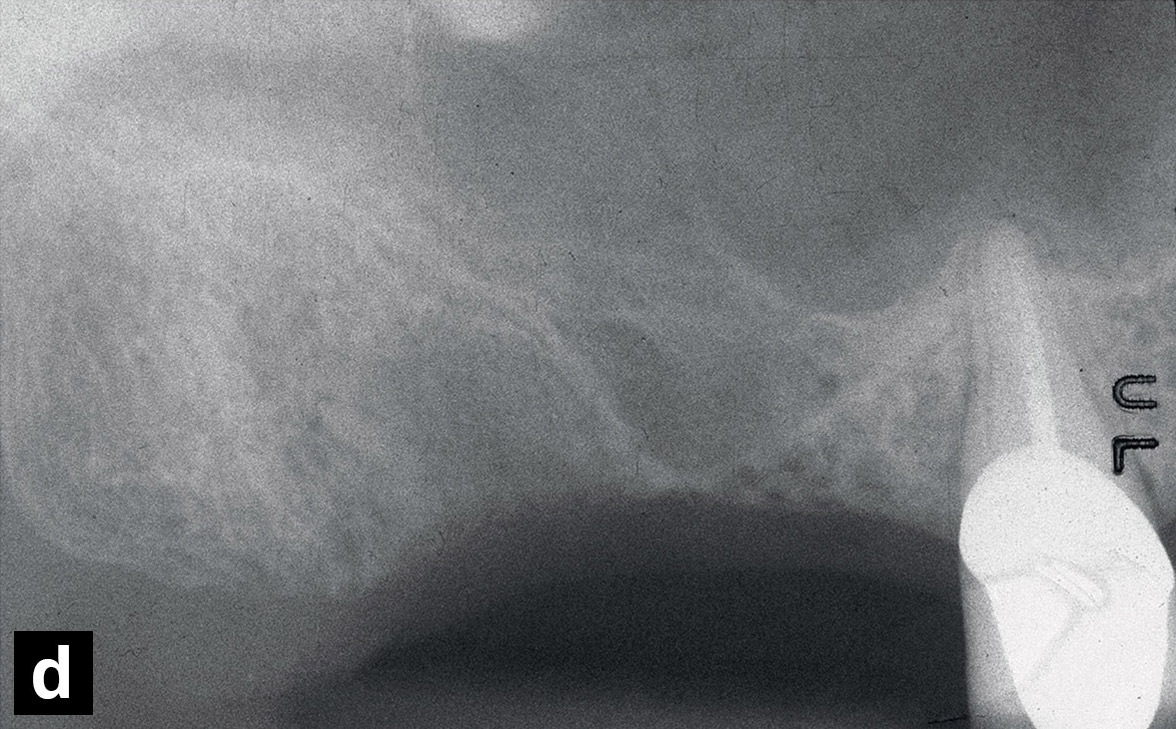
Radiographs showing the healing (a) one, (b) two, (c) three and (d) four months after the first sinus floor elevation procedure.
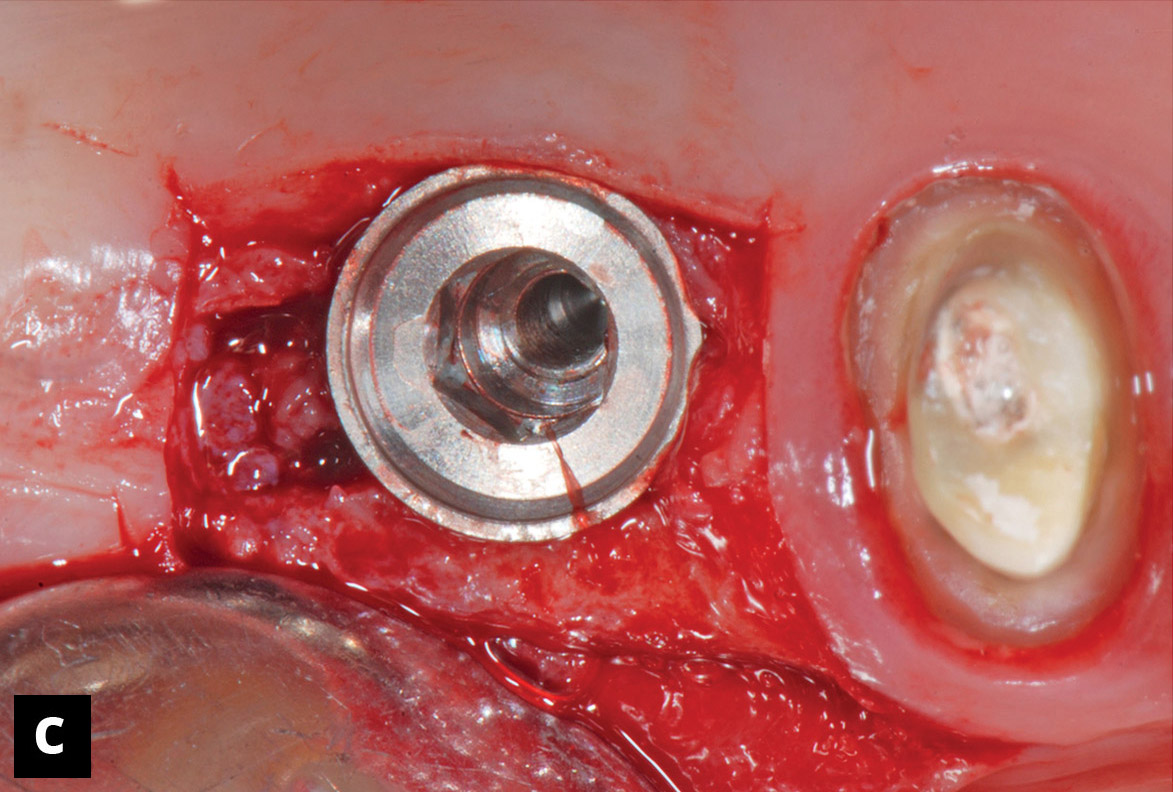
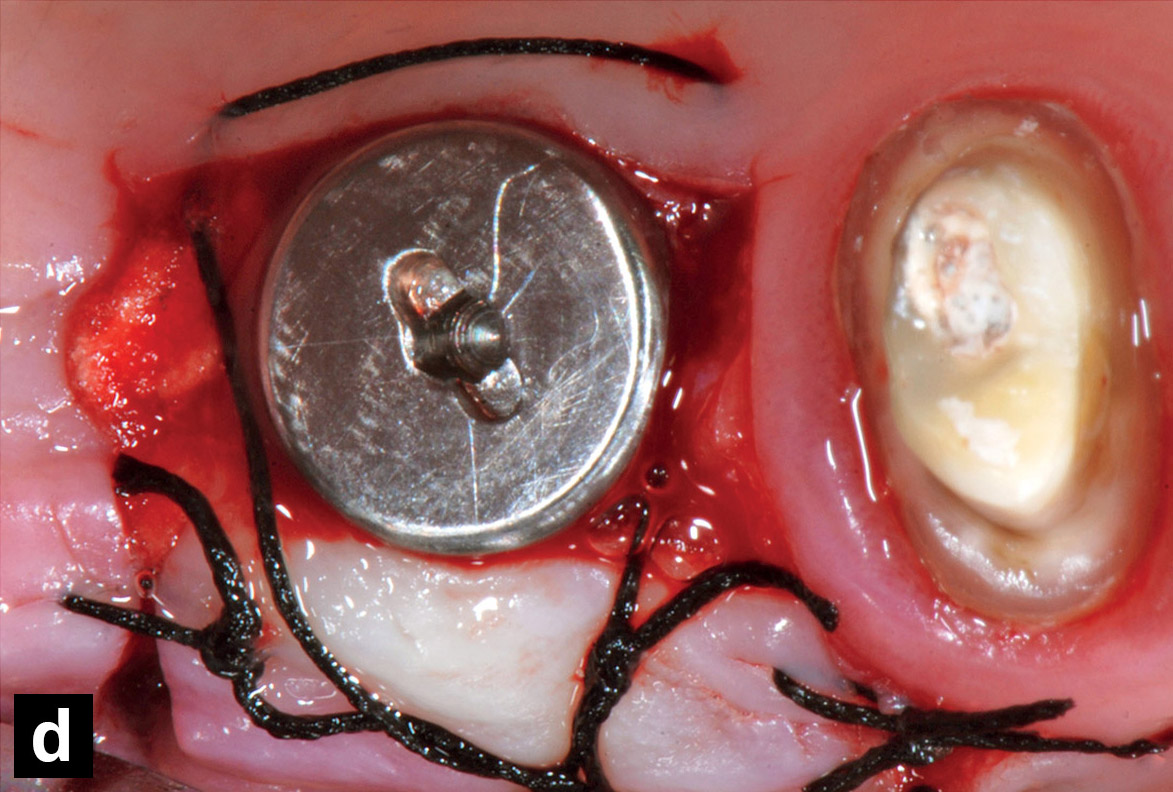
Clinical view of the surgical procedures of the second sinus floor elevation. (a) Buccal flap elevated. (b) The trapdoor was prepared, split and mobilized from the parent bone by chisels and a mallet. (c) Collagen sponges were added and an implant with a conical shape was placed. (d) The flaps were sutured with apical repositioning at the buccal aspect.
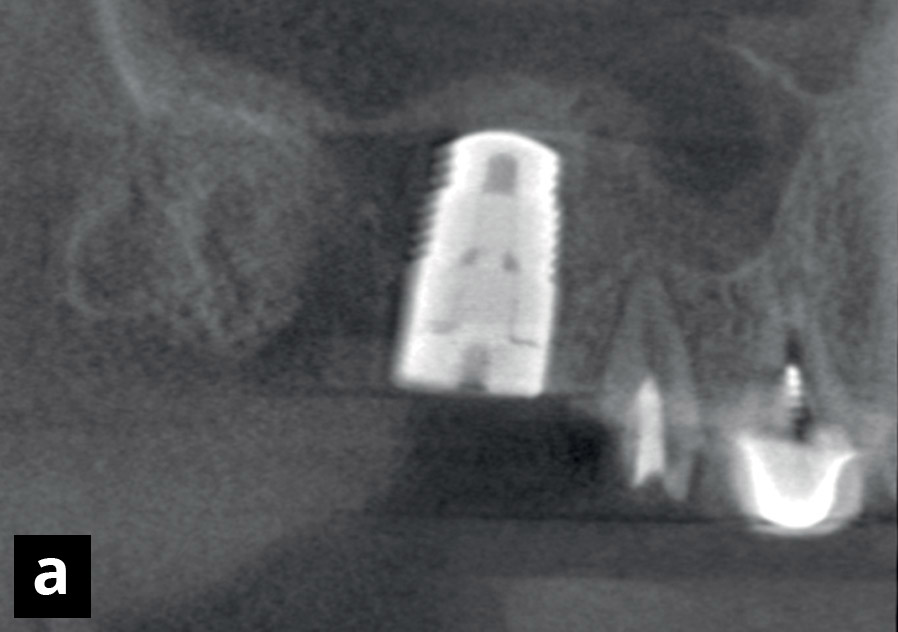
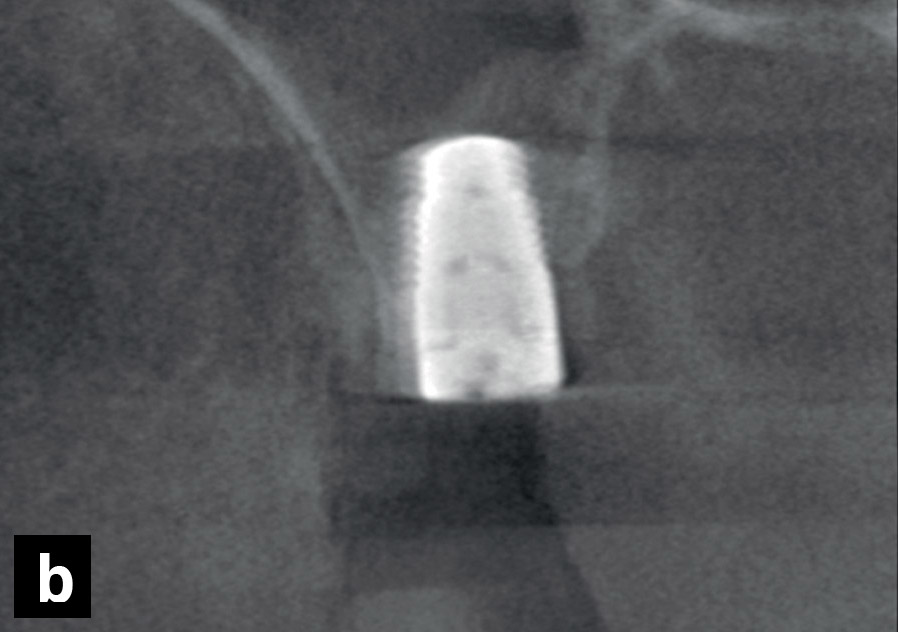
Low-dose CBCT scan taken immediately after the second surgery. (a) Panoramic view. (b) Cross-sectional view. (c) Axial view.
Prosthesis delivery and follow-up
After four months of uneventful healing, impressions were taken and a metal–ceramic crown was fabricated and seated over the implant (Figs. 8a–c). Checkups were performed during the healing period and regularly up to three years afterward. Intra-oral radiographs were taken immediately after prosthesis seating and yearly thereafter.
Results
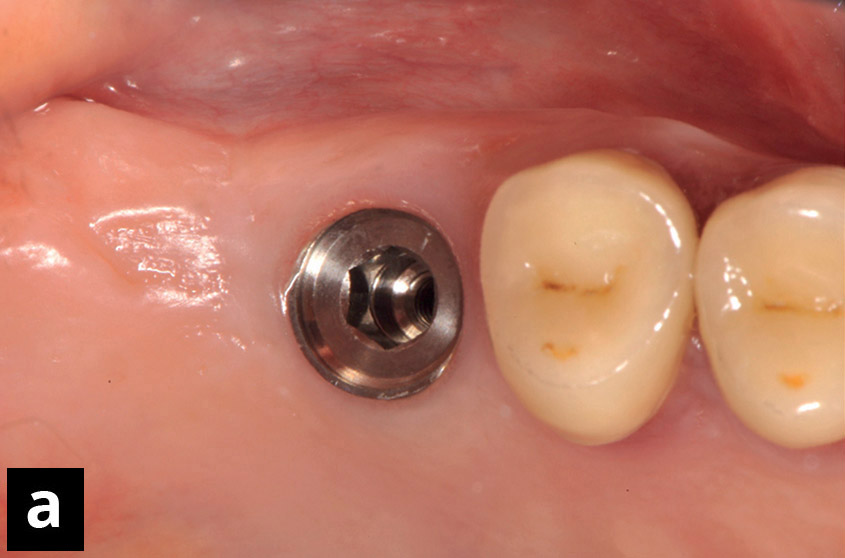
After three years, from the analyses of the CBCT scans, no marginal loss was found and bone was observed all around the implant surface. The location of the implant apex corresponded to the new sinus floor (Figs. 9a–c). No complaints were reported by the patient. At the clinical follow-ups, no clinical signs of periimplant soft-tissue inflammation and no technical complications were noted during the three-year period of observation (Fig. 9d).





Discussion
Clinical view of the outcome. (a) Implant four months after the second sinus floor elevation. (b & c) Crown just seated over the implant from the occlusal and buccal views, respectively.
Figs. 9a–d
Low-dose CBCT scan taken after three years.
(a) Panoramic view.
(b) Cross-sectional view.
(c) Axial view.
(d) Clinical view.
The surgical technique with a crestal trapdoor approach may present advantages over classical sinus floor elevation performed through a lateral window access. The crestal approach, conversely to the lateral access, avoids opening large flaps, performing long vertical releasing incisions, and strong pulling on the flaps during surgery. Moreover, it allows for easier access to the distal zones with less exposure of the surgical area.
The absence of biomaterial grafts, other than the rapidly resorbable collagen sponge, decreases the possible loss of material into the sinus and, consequently, the risk of infection in case of unexpected perforation of the sinus mucosa. Moreover, no membranes are needed to cover the access osteotomy, reducing the total biomaterial cost.46Listl S, Faggion CM Jr. An economic evaluation of different sinus lift techniques. → J Clin Periodontol. 2010 Aug;37(8):777–87. The absence of grafted material allows a more reliable radiographic evaluation of the progressive mineralization within the elevated area, whereas when a radiopaque grafting material is used, its radiopaque nature may hinder the evaluation of bone formation.
The use of a crestal access may avoid crossing the anastomosis between the posterior superior alveolar artery and the infraorbital arteries. This anastomosis may be quite large in diameter and may cause severe hemorrhages when it is unintentionally damaged and possibly compromise the blood supply of the region.47Solar P, Geyerhofer U, Traxler H, Windisch A, Ulm C, Watzek G. Blood supply to the maxillary sinus relevant to sinus floor elevation procedures. → Clin Oral Implants Res. 1999 Feb;10(1):34–44.48Elian N, Wallace S, Cho SC, Jalbout ZN, Froum S. Distribution of the maxillary artery as it relates to sinus floor augmentation. → Int J Oral Maxillofac Implants. 2005 Sep-Oct;20(5):784–7.49Rosano G, Taschieri S, Gaudy JF, Weinstein T, Del Fabbro M. Maxillary sinus vascular anatomy and its relation to sinus lift surgery. → Clin Oral Implants Res. 2011 Jul;22(7):711–5.50Jensen SS, Eriksen J, Schiodt M. Severe bleeding after sinus floor elevation using the transcrestal technique: a case report. → Eur J Oral Implantol. 2012 Autumn;5(3):287–91. One of the most important advantages of the present technique is, however, the presence of intact bone walls, whereas in the lateral access technique, the lateral wall is removed to a large extent, compromising bone formation. In fact, it has been shown that bone is formed from parent bone, while the sinus mucosa does not contribute to such formation, at least during the earliest periods of healing.51Scala A, Botticelli D, Rangel IG Jr, de Oliveira JA, Okamoto R, Lang NP. Early healing after elevation of the maxillary sinus floor applying a lateral access: a histological study in monkeys. → Clin Oral Implants Res. 2010 Dec;21(12):1320–6.’ 52Scala A, Botticelli D, Faeda RS, Rangel IG Jr, de Oliveira JA, Lang NP. Lack of influence of the Schneiderian membrane in forming new bone apical to implants simultaneously installed with sinus floor elevation: an experimental study in monkeys. → Clin Oral Implants Res. 2012 Feb;23(2):175–81. Finally, in the case of thin alveolar ridges, a split-crest procedure may be applied concomitantly, so that the width of the ridge may also be augmented.
The crestal approach described in the present article also has some disadvantages, such as the low visibility within the elevated zone and the complex learning curve. The chisels and mallet have to be used carefully to avoid damage to the sinus membrane and discomfort for the patient. Moreover, the technique illustrated in the present article requires the sinus elevation to be performed twice, the implant being placed during the second surgery.
The sonic handpiece instrument and the micro-saw inserts used allow the operator to perform sharp and thin incisions with a clear view of the area, cleaned of bone smear and blood by irrigation. Moreover, incision with vibrating tools weakens the bone along the lines of the osteotomy, minimizing the use of the mallet and consequently resulting in less discomfort for the patient. Sonic instruments have been shown to produce a very low increase in temperature compared with ultrasonic instruments53Heinemann F, Hasan I, Kunert-Keil C, Götz W, Gedrange T, Spassov A, Schweppe J, Gredes T. Experimental and histological investigations of the bone using two different oscillating osteotomy techniques compared with conventional rotary osteotomy. → Ann Anat. 2012 Mar;194(2):165–70. and very limited soft-tissue damage.54Geminiani A, Papadimitriou DE, Ercoli C. Maxillary sinus augmentation with a sonic handpiece for the osteotomy of the lateral window: a clinical report. → J Prosthet Dent. 2011 Nov;106(5):279–83.55Geminiani A, Weitz DS, Ercoli C, Feng C, Caton JG, Papadimitriou DE. A comparative study of the incidence of Schneiderian membrane perforations during maxillary sinus augmentation with a sonic oscillating handpiece versus a conventional turbine handpiece. → Clin Implant Dent Relat Res. 2015 Apr;17(2):327–34. Epub 2013 Jul 9.56Weitz DS, Geminiani A, Papadimitriou DE, Ercoli C, Caton JG. The incidence of membrane perforation during sinus floor elevation using sonic instruments: a series of 40 cases. → Int J Periodontics Restorative Dent. 2014 Jan-Feb;34(1):105–12. The use of sonic instruments has been proposed for the extraction of impacted canines57Agabiti I, Bernardello F, Nevins M, Wang HL. Impacted canine extraction by ridge expansion using air scaler surgical instruments: a case report. → Int J Periodontics Restorative Dent.2014 Sep-Oct;34(5):681–7. and successfully tested for implant placement in an animal experiment.58Viganò P, Botticelli D, Salata LA, Schweikert MT, Urbizo Velez J, Lang NP. Healing at implant sites prepared conventionally or by means of Sonosurgery. An experimental study in dogs. → Clin Oral Implants Res. 2015 Apr;26(4):377–82.
Conclusion
The technique illustrated in the present article allowed the placement of implants of proper length in a widely pneumatized sinus where the bone height of the floor was insufficient for immediate stabilization. After three years of function, neither marginal bone loss nor clinical signs of inflammation were observed.
Competing interests
IA developed the Sonosurgery device and microsaw inserts used in the treatment of this case, and hence declares a competing interest. DB declares that he has no competing interests in relation to this study. The study was self-funded by the authors.
References
| 1. | ↑ | Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. → Int J Periodontics Restorative Dent. 2003 Jul-Aug;23(4):313–24. |
| 2. | ↑ | Sharan A, Madjar D. Maxillary sinus pneumatization following extractions: a radiographic study. → Int J Oral Maxillofac Implants. 2008 Jan-Feb;23(1):48–56. |
| 3. | ↑ | Brånemark PI, Adell R, Albrektsson T, Lekholm U, Lindström J, Rockler B. An experimental and clinical study of osseointegrated implants penetrating the nasal cavity and maxillary sinus. → J Oral Maxillofac Surg. 1984 Aug;42(8):497–505. |
| 4, 7. | ↑ | Ellegaard B, Kølsen-Petersen J, Baelum V. Implant therapy involving maxillary sinus lift in periodontally compromised patients. → Clin Oral Implants Res. 1997 Aug;8(4):305–15. |
| 5, 8. | ↑ | Ellegaard B, Baelum V, Kølsen-Petersen J. Non-grafted sinus implants in periodontally compromised patients: a time-to-event analysis. → Clin Oral Implants Res. 2006 Apr;17(2):156–64. |
| 6, 9. | ↑ | Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. → J Oral Surg. 1980 Aug;38(8):613–6. |
| 10. | ↑ | Lundgren S, Anderson S, Gualini F, Sennerby L. Bone reformation with sinus membrane elevation: a new surgical technique for maxillary sinus floor augmentation. → Clin Implant Dent Relat Res. 2004 Sep;6(3):165–73. |
| 11. | ↑ | Barone A, Santini S, Sbordone L, Crespi R, Covani U. A clinical study of the outcomes and complications associated with maxillary sinus augmentation. → Int J Oral Maxillofac Implants. 2006 Jan-Feb;21(1):81–5. |
| 12. | ↑ | Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. → J Clin Periodontol. 2008 Sep;35(8 Suppl):216–40. |
| 13, 34. | ↑ | Summers RB. A new concept in maxillary implant surgery: the osteotome technique. → Compendium. 1994 Feb;15(2):152, 154–6, 158 passim; quiz 162. |
| 14. | ↑ | Toffler M. Osteotome-mediated sinus floor elevation: a clinical report. → Int J Oral Maxillofac Implants. 2004 Mar-Apr;19(2):266–73. |
| 15. | ↑ | Schwartz-Arad D, Herzberg R, Dolev E. The prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. → J Periodontol. 2004 Apr;75(4):511–6. |
| 16. | ↑ | Pjetursson BE, Rast C, Brägger U, Schmidlin K, Zwahlen M, Lang NP. Maxillary sinus floor elevation using the (transalveolar) osteotome technique with or without grafting material. Part I: implant survival and patients’ perception. → Clin Oral Implants Res. 2009 Jul;20(7):667–76. |
| 17. | ↑ | Pjetursson BE, Ignjatovic D, Matuliene G, Brägger U, Schmidlin K, Lang NP. Transalveolar maxillary sinus floor elevation using osteotomes with or without grafting material. Part II: radiographic tissue remodeling. → Clin Oral Implants Res. 2009 Jul;20(7):677–83. |
| 18. | ↑ | Cosci F, Luccioli M. A new sinus lift technique in conjunction with placement of 265 implants: a 6-year retrospective study. → Implant Dent. 2000 Winter;9(4):363–8. |
| 19. | ↑ | Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32. |
| 20. | ↑ | Trombelli L, Franceschetti G, Stacchi C, Minenna L, Riccardi O, Di Raimondo R, Rizzi A, Farina R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or β-tricalcium phosphate: a multicenter, double-blind, randomized, controlled clinical trial. → J Clin Periodontol. 2014 Mar;41(3):311–9. Epub 2014 Jan 2. |
| 21. | ↑ | Baldi D, Menini M, Pera F, Ravera G, Pera P. Sinus floor elevation using osteotomes or piezoelectric surgery. → Int J Oral Maxillofac Surg. 2011 May;40(5):497–503. |
| 22. | ↑ | Vercellotti T, De Paoli S, Nevins M. The piezoelectric bony window osteotomy and sinus membrane elevation: introduction of a new technique for simplification of the sinus augmentation procedure. → Int J Periodontics Restorative Dent. 2001 Dec;21(6):561–7. |
| 23. | ↑ | Diserens V, Mericske E, Mericske-Stern R. Radiographic analysis of the transcrestal sinus floor elevation: short-term observations. → Clin Implant Dent Relat Res. 2005 Apr;7(2):70–8. |
| 24, 45. | ↑ | Bruschi GB, Scipioni A, Calesini G, Bruschi E. Localized management of sinus floor with simultaneous implant placement:a clinical report. → Int J Oral Maxillofac Implants. 1998 Mar-Apr;13(2):219–26. |
| 25. | ↑ | Winter AA, Pollack AS, Odrich RB. Placement of implants in the severely atrophic posterior maxilla using localized management of the sinus floor: a preliminary study. → Int J Oral Maxillofac Implants. 2002 Sep-Oct;17(5):687–95. |
| 26. | ↑ | Winter AA, Pollack AS, Odrich RB. Sinus/alveolar crest tenting (SACT): a new technique for implant placement in atrophic maxillary ridges without bone grafts or membranes. → Int J Periodontics Restorative Dent. 2003 Nov-Dec;23(6):557–65. |
| 27. | ↑ | Scipioni A, Bruschi GB, Calesini G. The edentulous ridge expansion technique: a five-year study. → Int J Periodontics Restorative Dent. 1994 Oct;14(5):451–60. |
| 28, 51. | ↑ | Scala A, Botticelli D, Rangel IG Jr, de Oliveira JA, Okamoto R, Lang NP. Early healing after elevation of the maxillary sinus floor applying a lateral access: a histological study in monkeys. → Clin Oral Implants Res. 2010 Dec;21(12):1320–6. |
| 29, 52. | ↑ | Scala A, Botticelli D, Faeda RS, Rangel IG Jr, de Oliveira JA, Lang NP. Lack of influence of the Schneiderian membrane in forming new bone apical to implants simultaneously installed with sinus floor elevation: an experimental study in monkeys. → Clin Oral Implants Res. 2012 Feb;23(2):175–81. |
| 30. | ↑ | Gruber R, Kandler B, Fuerst G, Fisher MB, Watzek G. Porcine sinus mucosa holds cells that respond to bone morphogenetic protein (BMP)-6 and BMP-7 with increased osteogenic differentiation in vitro. → Clin Oral Implants Res. 2004 Oct;15(5):575–80. |
| 31. | ↑ | Srouji S, Kizhner T, Ben David D, Riminucci M, Bianco P, Livne E. The Schneiderian membrane contains osteoprogenitor cells: in vivo and in vitro study. → Calcif Tissue Int. 2009 Feb;84(2):138–45. |
| 32. | ↑ | Srouji S, Ben-David D, Lotan R, Riminucci M, Livne E, Bianco P. The innate osteogenic potential of the maxillary sinus (Schneiderian) membrane: an ectopic tissue transplant model simulating sinus lifting. → Int J Oral Maxillofac Surg. 2010 Aug;39(8):793–801. |
| 33. | ↑ | Srouji S, Ben-David D, Funari A, Riminucci M, Bianco P. Evaluation of the osteoconductive potential of bone substitutes embedded with Schneiderian membrane- or maxillary bone marrow- derived osteoprogenitor cells. → Clin Oral Implants Res. 2013 Dec;24(12):1288–94. |
| 35, 40. | ↑ | Zitzmann NU, Schärer P. Sinus elevation procedures in the resorbed posterior maxilla: comparison of the crestal and lateral approaches. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Jan;85(1):8–17. |
| 36, 41. | ↑ | Chao YL, Chen HH, Mei CC, Tu YK, Lu HK. Meta-regression analysis of the initial bone height for predicting implant survival rates of two sinus elevation procedures. → J Clin Periodontol. 2010 May;37(5):456–65. |
| 37, 42. | ↑ | Bernardello F, Righi D, Cosci F, Bozzoli P, Soardi CM, Spinato S. Crestal sinus lift with sequential drills and simultaneous implant placement in sites with <5 mm of native bone: a multicenter retrospective study. → Implant Dent. 2011 Dec;20(6):439–44. |
| 38, 43. | ↑ | He L, Chang X, Liu Y. Sinus floor elevation using osteotome technique without grafting materials: a 2-year retrospective study. → Clin Oral Implants Res. 2013 Aug;24 Suppl A100:63–7. |
| 39, 44. | ↑ | Kang T. Sinus elevation using a staged osteotome technique for site development prior to implant placement in sites with less than 5 mm of native bone: a case report. → Int J Periodontics Restorative Dent. 2008 Jan-Feb;28(1):73–81. |
| 46. | ↑ | Listl S, Faggion CM Jr. An economic evaluation of different sinus lift techniques. → J Clin Periodontol. 2010 Aug;37(8):777–87. |
| 47. | ↑ | Solar P, Geyerhofer U, Traxler H, Windisch A, Ulm C, Watzek G. Blood supply to the maxillary sinus relevant to sinus floor elevation procedures. → Clin Oral Implants Res. 1999 Feb;10(1):34–44. |
| 48. | ↑ | Elian N, Wallace S, Cho SC, Jalbout ZN, Froum S. Distribution of the maxillary artery as it relates to sinus floor augmentation. → Int J Oral Maxillofac Implants. 2005 Sep-Oct;20(5):784–7. |
| 49. | ↑ | Rosano G, Taschieri S, Gaudy JF, Weinstein T, Del Fabbro M. Maxillary sinus vascular anatomy and its relation to sinus lift surgery. → Clin Oral Implants Res. 2011 Jul;22(7):711–5. |
| 50. | ↑ | Jensen SS, Eriksen J, Schiodt M. Severe bleeding after sinus floor elevation using the transcrestal technique: a case report. → Eur J Oral Implantol. 2012 Autumn;5(3):287–91. |
| 53. | ↑ | Heinemann F, Hasan I, Kunert-Keil C, Götz W, Gedrange T, Spassov A, Schweppe J, Gredes T. Experimental and histological investigations of the bone using two different oscillating osteotomy techniques compared with conventional rotary osteotomy. → Ann Anat. 2012 Mar;194(2):165–70. |
| 54. | ↑ | Geminiani A, Papadimitriou DE, Ercoli C. Maxillary sinus augmentation with a sonic handpiece for the osteotomy of the lateral window: a clinical report. → J Prosthet Dent. 2011 Nov;106(5):279–83. |
| 55. | ↑ | Geminiani A, Weitz DS, Ercoli C, Feng C, Caton JG, Papadimitriou DE. A comparative study of the incidence of Schneiderian membrane perforations during maxillary sinus augmentation with a sonic oscillating handpiece versus a conventional turbine handpiece. → Clin Implant Dent Relat Res. 2015 Apr;17(2):327–34. Epub 2013 Jul 9. |
| 56. | ↑ | Weitz DS, Geminiani A, Papadimitriou DE, Ercoli C, Caton JG. The incidence of membrane perforation during sinus floor elevation using sonic instruments: a series of 40 cases. → Int J Periodontics Restorative Dent. 2014 Jan-Feb;34(1):105–12. |
| 57. | ↑ | Agabiti I, Bernardello F, Nevins M, Wang HL. Impacted canine extraction by ridge expansion using air scaler surgical instruments: a case report. → Int J Periodontics Restorative Dent.2014 Sep-Oct;34(5):681–7. |
| 58. | ↑ | Viganò P, Botticelli D, Salata LA, Schweikert MT, Urbizo Velez J, Lang NP. Healing at implant sites prepared conventionally or by means of Sonosurgery. An experimental study in dogs. → Clin Oral Implants Res. 2015 Apr;26(4):377–82. |





Leave a Reply
Be the First to Comment!