Zero apicectomy in endodontic microsurgery
September 18, 2017 / Categories: Digital Dentistry, Implant Dentistry

Harik, Randa

Issa, Grace

Sleiman, Philippe
Abstract
Background
Surgical endodontic treatment is an option for teeth with periapical periodontitis and may be indicated for teeth previously submitted to unsuccessful endodontic treatment and teeth with a strong possibility of failure by the nonsurgical approach. This procedure includes root sectioning and preparation of a cavity in the root canal followed by retrograde obturation.
Furthermore, the presence of apical true cysts requires surgical treatment as well, as these cysts are less likely to heal by nonsurgical root canal therapy because they are self-sustaining and no longer dependent on the presence or absence of root canal infection. Accordingly, surgical intervention of apical true cysts is necessary.
The limitations of periapical radiography have led to significant interest in cone beam computed tomography (CBCT) in endodontic applications. The number of CBCT scans taken every year is increasing as awareness increases, resolution increases and costs decrease.
Case presentation
In this article, we describe a new approach in surgical endodontics that focuses on preserving the integrity of the apical part of the root. This approach entails conducting root canal treatment and surgical cyst removal in one session. We illustrate this approach with a series of cases showing the preoperative condition and postoperative healing, with a recall period of 6 months, 1 year, 2 years, and yearly up to 5 years.
Conclusion
Zero apicectomy in endodontic surgery is a novel technique that combines high-resolution CBCT visualization of the apical situation, root canal treatment with the use of efficient irrigation with EndoVac, and root surface conditioning in order to allow the preservation of the apical part of the root ad integrum. Zero apicectomy clears the infection from inside the bone and treats the root canal in the same session, giving the body a greater opportunity to heal in a healthy, clean environment. Current literature has not described this technique; however, clinical cases have proven its success.
Keywords
Apicectomy, EndoVac, CBCT, surgical endodontic treatment.
Introduction
Surgical endodontic treatment is an option for teeth with apical periodontitis and may be indicated for teeth previously submitted to unsuccessful endodontic treatment and teeth with a strong possibility of failure by the nonsurgical approach.1Bernarde RA, De Moraes IG, Garcia RB, Bernardineli N, Baldi JV, Victorino FR, Vasconcelos BC, Duarte MA, Bramante CM. Evaluation of apical cavity preparation with a new type of ultrasonic diamond tip.
→ J Endod. 2007 Apr;33(4):484–7.2Gutmann JL, Harrison JW, editors. Surgical endodontics: past, present, and future. In: Surgical endodontics.
→ Cambridge: Blackwell Scientific; 1991. p. 216–30.3Tsesis I, Rosen E, Schwartz-Arad D, Fuss Z. Retrospective evaluation of surgical endodontic treatment: traditional versus modern technique.
→ J Endod. 2006 May;32(5):412–6. This procedure usually consists of several steps, including retrograde obturation, which is performed after root sectioning and preparation of a cavity in the root canal.4Bernarde RA, De Moraes IG, Garcia RB, Bernardineli N, Baldi JV, Victorino FR, Vasconcelos BC, Duarte MA, Bramante CM. Evaluation of apical cavity preparation with a new type of ultrasonic diamond tip.
→ J Endod. 2007 Apr;33(4):484–7.
Furthermore, the presence of apical true cysts requires surgical treatment as well, as these cysts are less likely to heal by conventional root canal therapy because they are selfsustaining and no longer dependent on the presence or absence of root canal infection.5Cohn S, Hagreaves K. Pathways of the pulp. 9th ed.
→ St Louis: Mosby; 2006. 662. p.6Orstavik D, Pitt Ford TR. Essential endodontology. 2nd ed.
→ Oxford: Blackwell Science; 2008. 162-3 p.7Nair PN, Sjogren U, Schumacher E, Sundqvist G. Radicular cyst affecting a root-filled human tooth: a long-term post-treatment follow-up.
→ Int Endod J. 1993 Jul;26(4):225–33. Accordingly, surgical intervention of apical true cysts is necessary.8Ingle J, Bakland L, Baugartner C. Ingle’s endodontics. 6th ed.
→ St Louis: Saunders; 2009. 221-308 p.9Lin LM, Ricucci D, Lin J, Rosenberg PA. Nonsurgical root canal therapy of large cyst-like inflammatory periapical lesions and inflammatory apical cysts.
→ J Endod. 2009 May;35(5):607–15.10Nair PN. New perspectives on radicular cysts: do they heal?
→ Int Endod J. 1998 May;31(3):155–60.11Natkin E, Oswald RJ, Carnes LI. The relationship of lesion size to diagnosis, incidence, and treatment of periapical cysts and granulomas.
→ Oral Surg Oral Med Oral Pathol. 1984 Jan;57(1):82–94. This technique can be performed when conducting a root canal treatment or a retreatment of the root canal system, combined with a surgical approach for the removal of the cyst. If access to the root canal system is not possible, a conventional apicectomy can be performed.
The limitations of periapical radiography have led to significant interest in cone beam computed tomography (CBCT) in endodontic applications. It seems that number of CBCT scans taken every year is increasing as awareness increases, resolution increases and costs decrease.12Pope O, Sathorn C, Parashos PA. Comparative investigation of cone-beam computed tomography and periapical radiography in the diagnosis of a healthy periapex.
→ J Endod. 2014 Mar;40(3):360–5. With the use of CBCT, cystic lesions are easily identified.
In this article, we will describe a new approach in surgical endodontics that focuses on preserving the integrity of the apical part of the root. We will illustrate this approach with a series of cases showing the preoperative condition and postoperative healing.
Materials and methods
Once there is a positive diagnosis of an apical cyst with CBCT, the patient is informed of the situation and the different steps of the treatment. The procedure is performed under local anesthesia with the use of articaine with 1:100,000 epinephrine infiltrated under the periosteum. We then proceed by isolating the tooth or teeth with a rubber dam and then shaping and cleaning the root canal system. The irrigation is conducted with the EndoVac negative-pressure device ( Sybron Endo, Orange, Ca., U.S.).13Miller TA, Baumgartner JC. Comparison of the antimicrobial efficacy of irrigation using the EndoVac to endodontic needle delivery.
→ J Endod. 2010 Mar;36(3):509–11. Once the working length has been determined electronically the irrigation cannula can be placed at the working length.14Miller TA, Baumgartner JC. Comparison of the antimicrobial efficacy of irrigation using the EndoVac to endodontic needle delivery.
→ J Endod. 2010 Mar;36(3):509–11. After the irrigation is completed, a temporary filling is placed in the access cavity and the rubber dam removed. The obturation of the canal is deferred, as the canal cannot be properly dried at this stage.
The following step is performing the surgical part, first by raising a flap and identifying the cyst. The cystic area is carefully spooned out while preserving the cementum and ligaments that are attached to the root surface. The exposed part of the root is rinsed with normal saline followed by the application of citric acid at a neutral pH with a microbrush on the root surface. After the latter step, the area is rinsed abundantly again with sterile water or normal saline. As the flap is temporarily put back in place, the tooth or teeth are isolated again with a rubber dam, the temporary filling is removed and a full sequence of irrigation with the use of EndoVac is conducted again. The master cone is adjusted, and full obturation of the root canal system is performed using warm vertical obturation. A temporary filling material is then placed in the access cavity and the isolating dam removed. The final step consists of raising the flap again and checking whether any large extrusion of the obturation material occurred that would need to be removed. The sutures are placed, and postoperative medication is prescribed.
Discussion
Apical periodontitis (AP) is an inflammatory or immune response in the apical periodontium that often results from intracanal microorganisms. The resulting apical bone resorption is a defense mechanism that prevents the spread of infection and appears radiolucent on radiographs. 15Nair PN. New perspectives on radicular cysts: do they heal?
→ Int Endod J. 1998 May;31(3):155–60.16Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats.
→ Oral Surg Oral Med Oral Pathol. 1965 Sep;20:340–9. Because AP is usually asymptomatic, it is frequently only detected during routine radiographic examination.17Bender IB. Factors influencing the radiographic appearance of bony lesions.
→ J Endod. 1982 Apr;8(4):161–70. In this sense, radiography is essential for the successful and timely diagnosis of AP and historically has been limited to periapical and panoramic radiographs.18American Association of Endodontists and American Academy of Oral and Maxillofacial Radiology. Use of cone-beam computed tomography in endodontics. Joint position statement of the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology.
→ Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Feb;111(2):234–7. Furthermore, radiographic imaging is essential in all stages of endodontics, from diagnosis through long-term assessment of healing outcomes. In conjunction with symptoms, outcome is assessed by comparison of preoperative and immediate postoperative radiographs, with subsequent radiographs taken at recall appointments. 19Gelfand M, Sunderman EJ, Goldman M. Reliability of radiographical interpretations.
→ J Endod. 1983 Feb;9(2):71–5.20Lambrianidis T. Observer variations in radiographic evaluation of endodontic therapy.
→ Endod Dent Traumatol. 1985 Dec;1(6):235–41.
The diagnostic value of pretreatment radiographs depends on how well they reflect the histology of AP. Studies that have investigated the correlation between histological appearance and radiographic manifestations have found that the absence of radiographic signs does not preclude apical inflammation, and the radiographic appearance is always smaller than the histological extent of the lesion.21Lin LM, Ricucci D, Lin J, Rosenberg PA. Nonsurgical root canal therapy of large cyst-like inflammatory periapical lesions and inflammatory apical cysts.
→ J Endod. 2009 May;35(5):607–15.22Miller TA, Baumgartner JC. Comparison of the antimicrobial efficacy of irrigation using the EndoVac to endodontic needle delivery.
→ J Endod. 2010 Mar;36(3):509–11.23Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review.
→ J Endod. 2007 Jan;33(1):1–6.24Nair PN. New perspectives on radicular cysts: do they heal?
→ Int Endod J. 1998 May;31(3):155–60. Radiographic signs pathognomonic of AP include radiolucent changes in periradicular trabecular pattern and altered shape and width of the periodontal ligament (PDL) space.25Barthel CR, Zimmer S, Trope M. Relationship of radiologic and histologic signs of inflammation in human root-filled teeth.
→ J Endod. 2004 Feb;30(2):75–9.26Brynolf, I. A histological and roentgenological study of the periapical region of human upper incisors. Odontologisk Revy. 1967. Almquist & Wiksell;18: 1-176.27Fouad AF, Walton RE, Rittman BR. Induced periapical lesions in ferret canines: histologic and radiographic evaluation.
→ Endod Dent Traumatol. 1992 Apr;8(2):56–62.28Green TL, Walton RE, Taylor JK, Merrell P. Radiographic and histologic periapical findings of root canal treated teeth in cadaver.
→ Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997 Jun;83(6):707–11. However, periapical radiographs and panoramic imaging have inherent limitations, such as superimposition and distortion of important structures that commonly mask lesions.29Katebzadeh N, Hupp J, Trope M. Histological periapical repair after obturation of infected root canals in dogs.
→ J Endod. 1999 May;25(5):364–8.30LeQuire AK, Cunningham CJ, Pelleu GB Jr. Radiographic interpretation of experimentally produced osseous lesions of the human mandible.
→ J Endod. 1977 Jul;3(7):274–6. In addition, lesions in cancellous bone cannot be consistently detected with these radiographic techniques.31Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: II.
→ J Am Dent Assoc. 1961 Jun;62(6):708–16. Therefore, in some cases, extensive bone resorption may be present even when there is no radiographic evidence of it.32Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: II.
→ J Am Dent Assoc. 1961 Jun;62(6):708–16. The appearance of the periapical tissue on a radiograph is influenced by the superimposition of anatomical structures and the variable nature of the overlying bone density and texture.33Gelfand M, Sunderman EJ, Goldman M. Reliability of radiographical interpretations.
→ J Endod. 1983 Feb;9(2):71–5.34Lambrianidis T. Observer variations in radiographic evaluation of endodontic therapy.
→ Endod Dent Traumatol. 1985 Dec;1(6):235–41. The limitations of periapical radiography have led to significant interest in CBCT.
Currently, the use of CBCT imaging has made it possible to visualize the related anatomical structures in 3-D with higher resolution. This has improved the overall diagnostic efficacy and made early diagnosis possible for some specific clinical situations.35Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review.
→ J Endod. 2007 Jan;33(1):1–6.36Patel S, Durack C, Abella F, Shemesh H, Roig M, Lemberg K. Cone beam computed tomography in endodontics—a review.
→ Int Endod J. 2015 Jan;48(1):3–15. In endodontic practice, CBCT imaging with limited fields of view has been suggested for diagnosis in patients with contradictory or nonspecific clinical signs and symptoms.37Patel S, Durack C, Abella F, Shemesh H, Roig M, Lemberg K. Cone beam computed tomography in endodontics—a review.
→ Int Endod J. 2015 Jan;48(1):3–15.
Postsurgical excisional wound healing after periradicular surgery entails dentoalveolar healing (i.e., reestablishment of an apical attachment apparatus) and alveolar healing (i.e., osseous repair of trabecular and cortical bone).38Andreasen JO. Cementum repair after apicoectomy in humans.
→ Acta Odontol Scand. 1973 Oct;31(4):211–21. Cementum deposition on the root end is considered the critical step in dentoalveolar wound healing.39Andreasen JO. Cementum repair after apicoectomy in humans.
→ Acta Odontol Scand. 1973 Oct;31(4):211–21. Consequently, creating an environment conducive to cementogenesis should enhance the healing process after surgical endodontic treatment.
In periodontal surgery, dentin demineralization leads to enhanced connective tissue attachment through splicing of exposed dentinal collagen with new collagen fibers produced during wound healing and early deposition of cementum on the dentinal surfaces.40Craig KR, Harrison JW. Wound healing following demineralization of resected root ends in periradicular surgery.
→ J Endod. 1993 Jul;19(7):339–47.
Demineralizing the root surface with citric acid has been shown to increase cementogenesis and promote periradicular wound healing by exposing the collagen matrix, which stimulates fibroblast attachment and growth.41Craig KR, Harrison JW. Wound healing following demineralization of resected root ends in periradicular surgery.
→ J Endod. 1993 Jul;19(7):339–47. The lower pH of citric acid may induce initially a more intense inflammatory response compared with saline. This may inhibit the healing process as measured by new bone formation. As healing progresses, the potential benefits of the anticollagenase activity may allow for more rapid collagen formation and ultimately allow more rapid new bone formation.42Davis JL, Jeansonne BG, Davenport WD, Gardiner D. The effect of irrigation with doxycycline or citric acid on leakage and osseous wound healing.
→ J Endod. 2003 Jan;29(1):31–5.
The irrigation is conducted with EndoVac, as the EndoVac System safely delivers irrigants to the apical terminus of root canals.43Miller TA, Baumgartner JC. Comparison of the antimicrobial efficacy of irrigation using the EndoVac to endodontic needle delivery.
→ J Endod. 2010 Mar;36(3):509–11. The device consists of a delivery/evacuation tip attached to a syringe of irrigant and the high-volume suction of the dental chair. Using a combination of a macro- or microcannula attached to the suction device, the irrigant introduced into the pulp chamber is pulled by negative pressure down the canal into the tip of the cannula and removed through the suction hose, thus avoiding any extrusion of the irrigant outside the root canal area, since the PDL barrier is lost then and the use of conventional irrigating methods could result in pushing the chemicals into the exposed surgical site.44Miller TA, Baumgartner JC. Comparison of the antimicrobial efficacy of irrigation using the EndoVac to endodontic needle delivery.
→ J Endod. 2010 Mar;36(3):509–11.
Case descriptions
Case 1
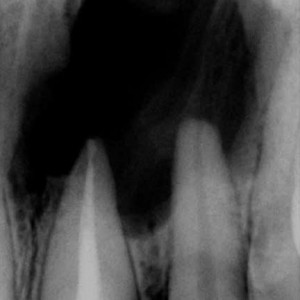
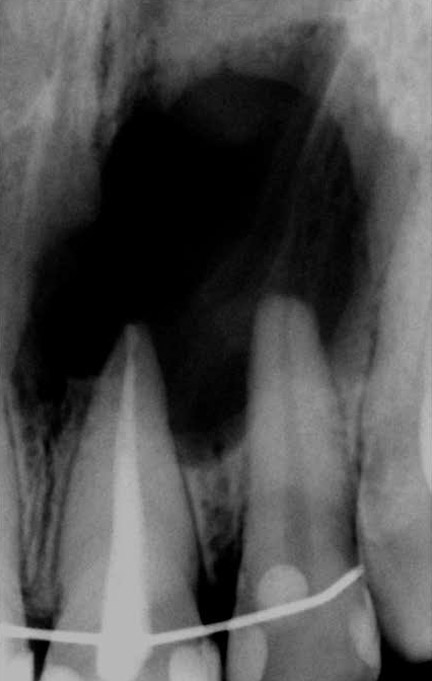
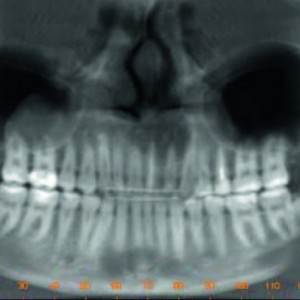
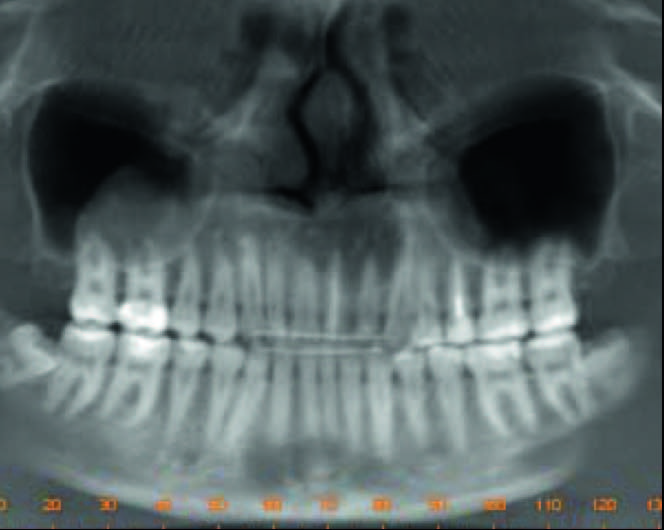
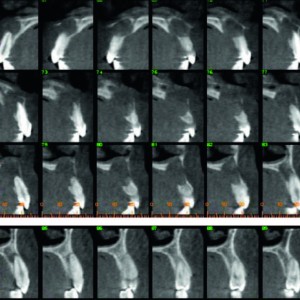
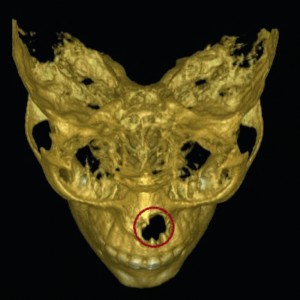
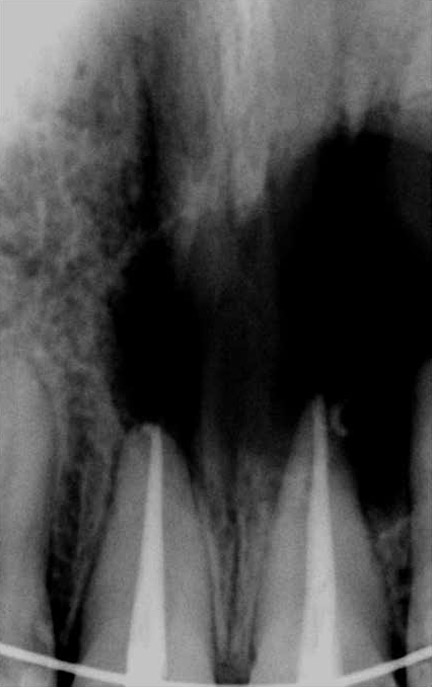
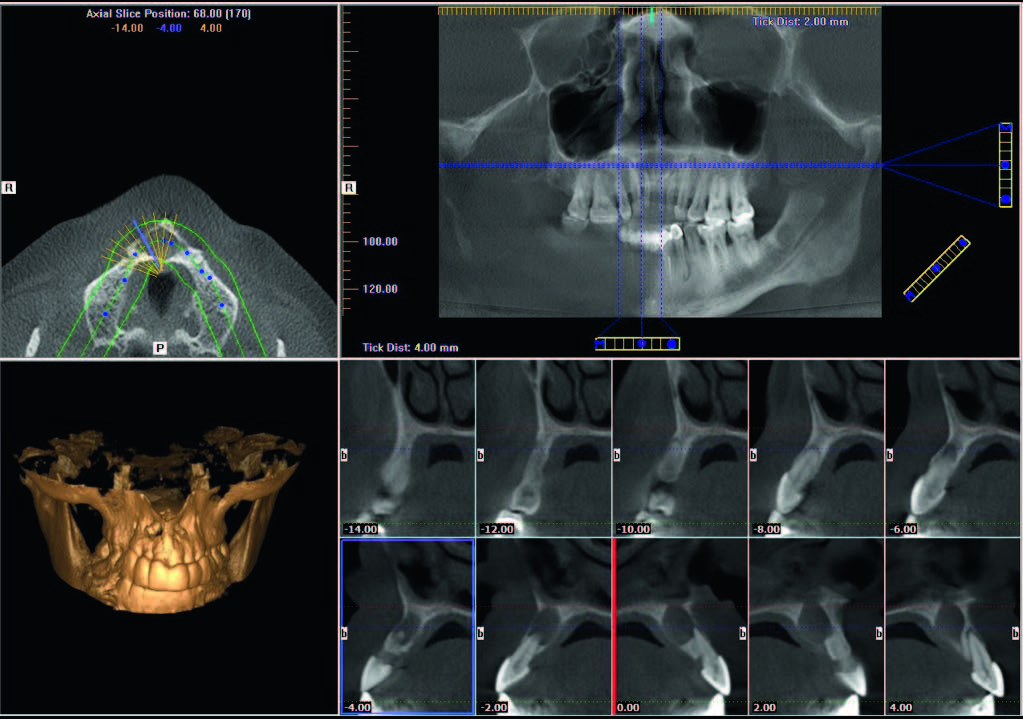
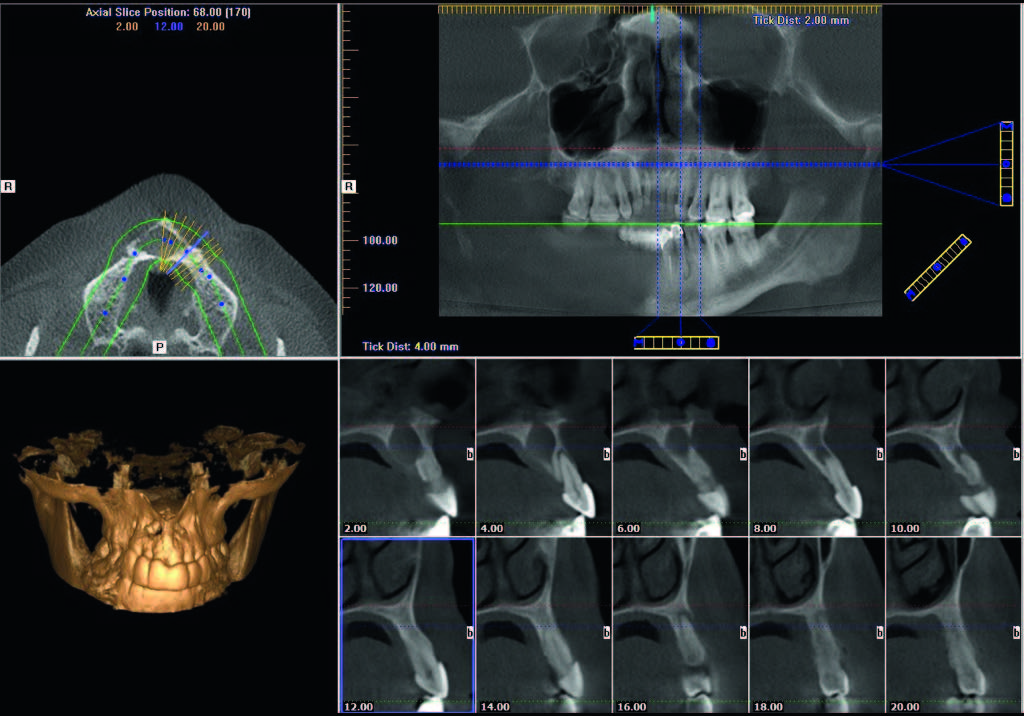
The patient was referred to the clinic with a swelling in the palatal area of the maxillary lateral incisor (Figs. 1a & b). Axial slices of CBCT cans showed substantial bone loss at the apical level of the maxillary lateral incisor (Fig. 1c) and at the level of the two maxillary central incisors (Fig. 1d).
-
- Fig. 1a
-
- Fig. 1b
-
- Fig. 1c

-
- Fig. 1d
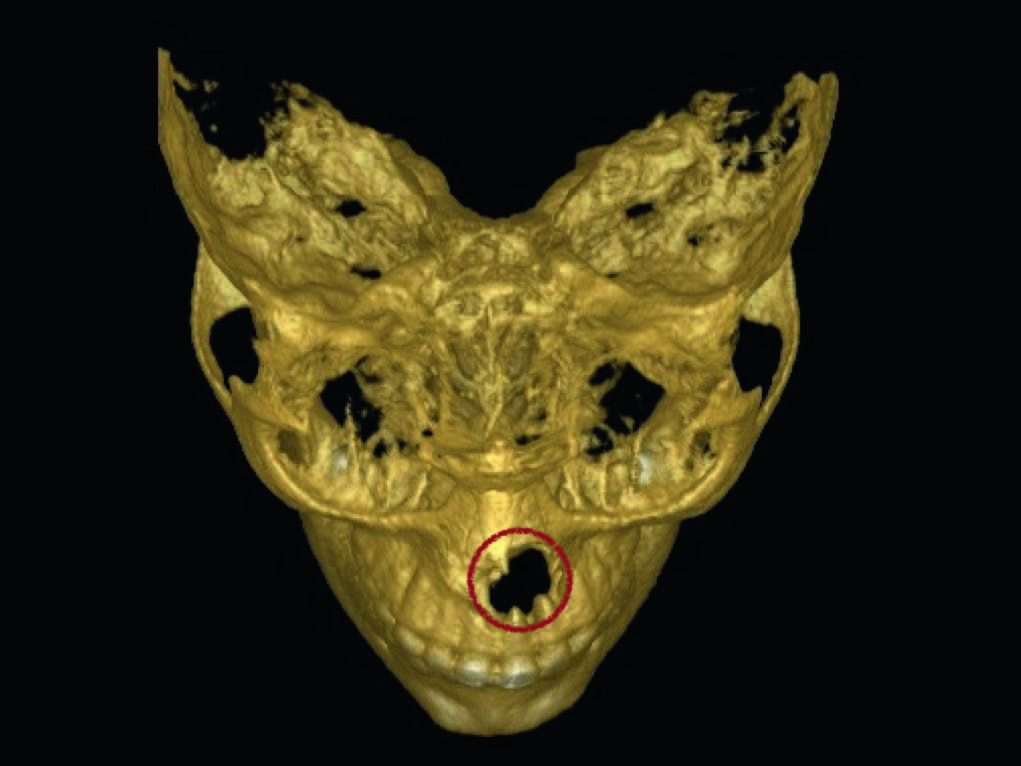
Fig. 1a & b
Preoperative periapical and panoramic radiographs.
Fig. 1c
CBCT axial slices.
Fig. 1d
CBCT 3-D reconstruction demonstrating the extent of the lesion(s).
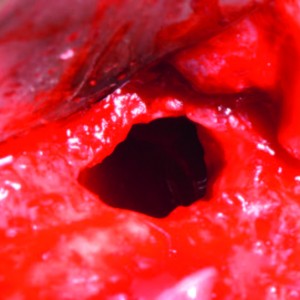
After administration of the anesthesia, a syringe was inserted into the palatal mucosa and a large amount of pus was aspirated. After following the procedural steps previously described and the removal of the cystic reaction, a long section of the root canals was exposed, especially that of the lateral and central incisors.
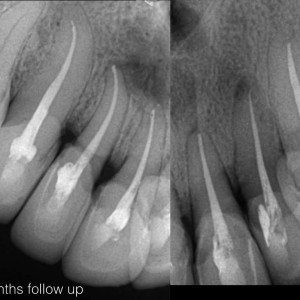
Immediate postoperative radiographs were taken (Figs. 1e & f), and then 1-year follow-up radiographs (Figs. 1g & h). The 1-year follow-up images showed the formation of new bone around the teeth and of a new PDL. The 5-year follow-up radiograph (Fig. 1i) indicated an intact PDL, a smaller fibrous area and no signs of external or internal resorption.
-

- Fig. 1e
-
- Fig. 1f
-

- Fig. 1g
-

- Fig. 1h
-

- Fig. 1i
Fig. 1e & f
Immediate postoperative radiographs of the lateral incisor (left) and central incisor (right).
Fig. 1g & h
One-year follow-up radiographs.
Fig. 1i
Five-year follow-up radiograph.
Case 2
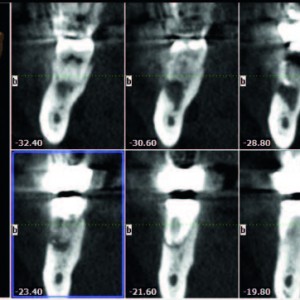
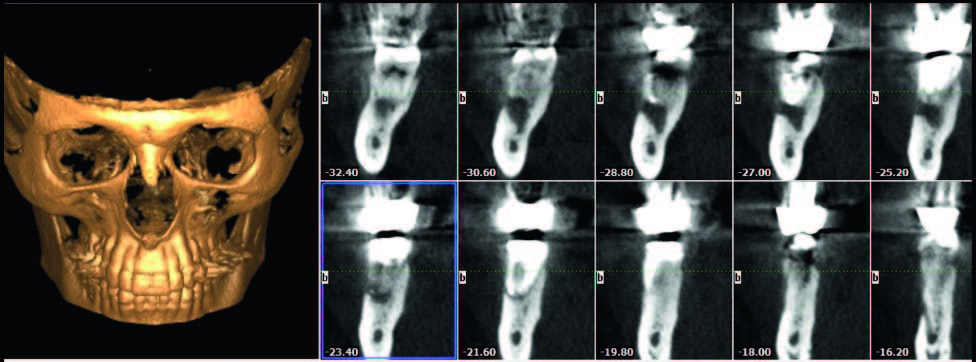
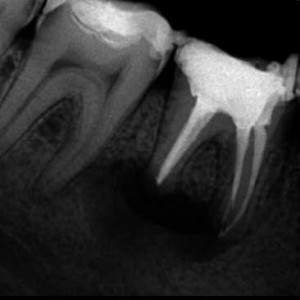
The patient was referred to have a mandibular molar checked. He was trying by all means to retain the molar, even though he had been advised to have it extracted and replaced with an implant. The preoperative radiograph (Fig. 2a) showed a substantial periapical lesion, although the previous dentist had placed calcium hydroxide paste in the canals. Furthermore, the patient was complaining of tingling in his lower lip. The i-CAT KaVo Dental, Biberach; Germany, showed that the cystic reaction extended far, almost reaching the mandibular canal (Fig. 2b).
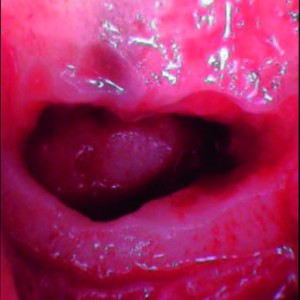
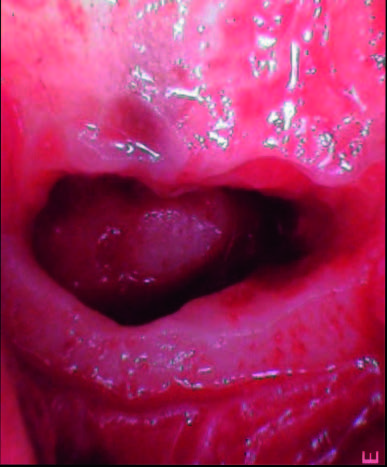
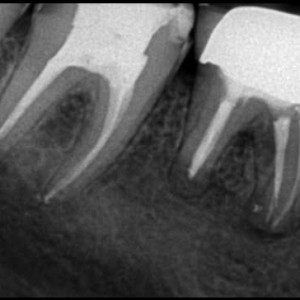
The same approach as described previously was performed in an attempt to treat and save the molar. Once the flap had been elevated, it appeared that the cystic reaction was also manifesting under the periosteum above the cortical bone and there was another cystic reaction close to the mandibular nerve (Fig. 2c). Postoperative radiographs were taken (Fig. 2d) and complete healing was seen with full reconstruction of the bone (Fig. 2e).
-

- Fig. 2a

-
- Fig. 2b
-
- Fig. 2c
-
- Fig. 2d

-

- Fig. 2e

-
- Fig. 2f
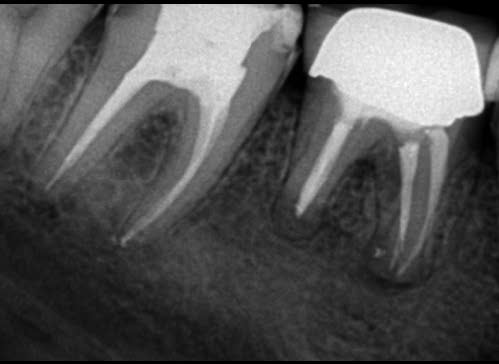
Fig. 2a
Preoperative periapical radiograph.
Fig. 2b
CBCT images of the patient.
Fig. 2c
The cystic reaction in the vicinity of the mandibular canal.
Fig. 2d
Immediate postoperative radiograph (left).
Fig. 2e
One-year follow-up radiograph.
Fig. 2f
Two-year follow-up radiograph.
Case 3
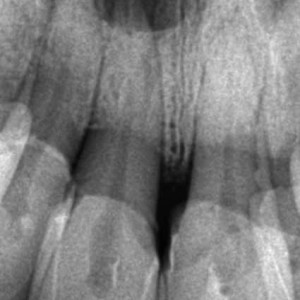
The patient was referred to the clinic to have the maxillary anterior teeth checked. The patient had had crowns placed several years before and apparently the pulps of those teeth had become necrotic and resulted in periapical infections. On the preoperative radiographs (Figs. 3a–c) and on the Icat (Figs. 3d & e), the periapical cysts could be easily identified and massive bone loss was evident.
-

- Fig. 3a

-

- Fig. 3b

-
- Fig. 3c

-
- Fig. 3d
-
- Fig. 3e
The same approach as described previously was used to treat all of the anterior teeth to remove the multiple cysts while preserving the bone as far as possible and only using the bone defect that was created by the infection to scoop out the cystic reaction (Figs. 3f & g). Postoperative radiographs were taken (Fig. 3h), as well as radiographs at the 18-month follow-up (Fig. 3i). Further follow-up was not done, as the patient was unavailable.
-

- Fig. 3f

-
- Fig. 3g

-

- Fig. 3h

-
- Fig. 3i

Fig. 3a–c
Preoperative radiographs: maxillary anterior teeth.
Fig. 3d & e
CBCT images.
Fig. 3f & g
Intraoperative photographs showing the defects resulting from the cystic reactions.
Fig. 3h
Immediate postoperative radiographs.
Fig. 3i
Eighteen-month follow-up radiographs.
Conclusion
Zero apicectomy in endodontic surgery is a novel technique that combines high-resolution CBCT visualization of the apical situation with the use of efficient irrigation with EndoVac, root canal treatment and root surface conditioning in order to allow the preservation of the apical part of the root ad integrum. Preserving the total length of the root has many benefits, including, most importantly, the stability and longevity of the tooth, as cutting the root exposes dentinal tubules. Since we perform retrograde obturation of the main canal, we cannot guarantee that the exposed dentin is bacteria-free. Comparing this with other techniques, in which we drain the cyst for a certain period without having the ability to know in advance if surgery will be needed later, zero apicectomy clears the infection from inside the bone and treats the root canal in the same session, giving the body a greater opportunity to heal in a healthy, clean environment. Current literature has not described this technique; however, clinical cases have proven its success.
Competing interests
The authors declare that they have no competing interests.

Interview
with Philippe Sleiman
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 4. | ↑ | Bernarde RA, De Moraes IG, Garcia RB, Bernardineli N, Baldi JV, Victorino FR, Vasconcelos BC, Duarte MA, Bramante CM. Evaluation of apical cavity preparation with a new type of ultrasonic diamond tip. → J Endod. 2007 Apr;33(4):484–7. |
| 2. | ↑ | Gutmann JL, Harrison JW, editors. Surgical endodontics: past, present, and future. In: Surgical endodontics. → Cambridge: Blackwell Scientific; 1991. p. 216–30. |
| 3. | ↑ | Tsesis I, Rosen E, Schwartz-Arad D, Fuss Z. Retrospective evaluation of surgical endodontic treatment: traditional versus modern technique. → J Endod. 2006 May;32(5):412–6. |
| 5. | ↑ | Cohn S, Hagreaves K. Pathways of the pulp. 9th ed. → St Louis: Mosby; 2006. 662. p. |
| 6. | ↑ | Orstavik D, Pitt Ford TR. Essential endodontology. 2nd ed. → Oxford: Blackwell Science; 2008. 162-3 p. |
| 7. | ↑ | Nair PN, Sjogren U, Schumacher E, Sundqvist G. Radicular cyst affecting a root-filled human tooth: a long-term post-treatment follow-up. → Int Endod J. 1993 Jul;26(4):225–33. |
| 8. | ↑ | Ingle J, Bakland L, Baugartner C. Ingle’s endodontics. 6th ed. → St Louis: Saunders; 2009. 221-308 p. |
| 9, 21. | ↑ | Lin LM, Ricucci D, Lin J, Rosenberg PA. Nonsurgical root canal therapy of large cyst-like inflammatory periapical lesions and inflammatory apical cysts. → J Endod. 2009 May;35(5):607–15. |
| 10, 15, 24. | ↑ | Nair PN. New perspectives on radicular cysts: do they heal? → Int Endod J. 1998 May;31(3):155–60. |
| 11. | ↑ | Natkin E, Oswald RJ, Carnes LI. The relationship of lesion size to diagnosis, incidence, and treatment of periapical cysts and granulomas. → Oral Surg Oral Med Oral Pathol. 1984 Jan;57(1):82–94. |
| 12. | ↑ | Pope O, Sathorn C, Parashos PA. Comparative investigation of cone-beam computed tomography and periapical radiography in the diagnosis of a healthy periapex. → J Endod. 2014 Mar;40(3):360–5. |
| 13, 14, 22, 43, 44. | ↑ | Miller TA, Baumgartner JC. Comparison of the antimicrobial efficacy of irrigation using the EndoVac to endodontic needle delivery. → J Endod. 2010 Mar;36(3):509–11. |
| 16. | ↑ | Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. → Oral Surg Oral Med Oral Pathol. 1965 Sep;20:340–9. |
| 17. | ↑ | Bender IB. Factors influencing the radiographic appearance of bony lesions. → J Endod. 1982 Apr;8(4):161–70. |
| 18. | ↑ | American Association of Endodontists and American Academy of Oral and Maxillofacial Radiology. Use of cone-beam computed tomography in endodontics. Joint position statement of the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Feb;111(2):234–7. |
| 19, 33. | ↑ | Gelfand M, Sunderman EJ, Goldman M. Reliability of radiographical interpretations. → J Endod. 1983 Feb;9(2):71–5. |
| 20, 34. | ↑ | Lambrianidis T. Observer variations in radiographic evaluation of endodontic therapy. → Endod Dent Traumatol. 1985 Dec;1(6):235–41. |
| 23, 35. | ↑ | Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. → J Endod. 2007 Jan;33(1):1–6. |
| 25. | ↑ | Barthel CR, Zimmer S, Trope M. Relationship of radiologic and histologic signs of inflammation in human root-filled teeth. → J Endod. 2004 Feb;30(2):75–9. |
| 26. | ↑ | Brynolf, I. A histological and roentgenological study of the periapical region of human upper incisors. Odontologisk Revy. 1967. Almquist & Wiksell;18: 1-176. |
| 27. | ↑ | Fouad AF, Walton RE, Rittman BR. Induced periapical lesions in ferret canines: histologic and radiographic evaluation. → Endod Dent Traumatol. 1992 Apr;8(2):56–62. |
| 28. | ↑ | Green TL, Walton RE, Taylor JK, Merrell P. Radiographic and histologic periapical findings of root canal treated teeth in cadaver. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997 Jun;83(6):707–11. |
| 29. | ↑ | Katebzadeh N, Hupp J, Trope M. Histological periapical repair after obturation of infected root canals in dogs. → J Endod. 1999 May;25(5):364–8. |
| 30. | ↑ | LeQuire AK, Cunningham CJ, Pelleu GB Jr. Radiographic interpretation of experimentally produced osseous lesions of the human mandible. → J Endod. 1977 Jul;3(7):274–6. |
| 31, 32. | ↑ | Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: II. → J Am Dent Assoc. 1961 Jun;62(6):708–16. |
| 36, 37. | ↑ | Patel S, Durack C, Abella F, Shemesh H, Roig M, Lemberg K. Cone beam computed tomography in endodontics—a review. → Int Endod J. 2015 Jan;48(1):3–15. |
| 38, 39. | ↑ | Andreasen JO. Cementum repair after apicoectomy in humans. → Acta Odontol Scand. 1973 Oct;31(4):211–21. |
| 40, 41. | ↑ | Craig KR, Harrison JW. Wound healing following demineralization of resected root ends in periradicular surgery. → J Endod. 1993 Jul;19(7):339–47. |
| 42. | ↑ | Davis JL, Jeansonne BG, Davenport WD, Gardiner D. The effect of irrigation with doxycycline or citric acid on leakage and osseous wound healing. → J Endod. 2003 Jan;29(1):31–5. |





Leave a Reply
Be the First to Comment!