Clinical and histological evaluation of a flapless socket preservation procedure: A prospective single cohort study
April 4, 2016 / Categories: Digital Dentistry, Implant Dentistry

Borgia, Valentina

Alfonsi, Fortunato

Tonelli, Paolo
Bertelli, Lorenzo
Marchionni, Saverio
Iezzi, Giovanna
Covani, Ugo

Barone, Antonio
The objective of this study was to evaluate the dimensional changes to hard and soft tissue after a flapless ridge preservation procedure in the posterior area of the jaw.
Introduction
The treatment of extraction sockets is a daily challenge in clinical practice.
Several changes to the bone dimensions occur after tooth extraction, since the alveolar bone is a tooth-dependent tissue.1Barone A, Aldini NN, Fini M, Giardino R, Calvo Guirado JL, Covani U. Xenograft versus extraction alone for ridge preservation after tooth removal: a clinical and histomorphometric study. → J Periodontol. 2008 Aug 79(8):1370–7. Bone modeling and remodeling are unavoidable during healing of an extraction socket.2Darby I, Chen ST, Buser D. Ridge preservation techniques for implant therapy. → Int J Oral Maxillofac Implants. 2009;24 Suppl:260–71.3Hämmerle CH, Araújo MG, Simion M; Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:80–2.4Barone A, Ricci M, Tonelli P, Santini S, Covani U. Tissue changes of extraction sockets in humans: a comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. → Clin Oral Implants Res. 2013 Nov;24(11):1231–7. A number of studies have pointed out that most of the resorption occurred during the first three months, although dimensional changes have been observed up to one year after a tooth extraction.5Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, Sanz M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:22–38.6Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction: an experimental study in the dog. → J Clin Periodontol. 2005 Feb;32(2):212–8.7Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. → Int J Periodontics Restorative Dent. 2003 Jul-Aug;23(4):313–23.
The changes to the alveolar ridge after tooth extraction showed the greatest amount of bone loss in the horizontal dimension and a concomitant loss of vertical ridge height, which has been reported to be more evident at the buccal level.8Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, Sanz M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:22–38.'9Covani U, Ricci M, Bozzolo G, Mangano F, Zini A, Barone A. Analysis of the pattern of the alveolar ridge remodelling following single tooth extraction. → Clin Oral Implants Res. 2011 Aug;22(8):820–5.'10Fickl S, Zuhr O, Wachtel H, Stappert CF, Stein JM, Hürzeler MB. Dimensional changes of the alveolar ridge contour after different socket preservation techniques. → J Clin Periodontol. 2008 Aug;35(10):906–13. The morphological changes at the extraction sites resulted in narrow and short edentulous alveolar ridges; moreover, the alveolar crest margin tended to shift lingually/palatally according to a specific pattern. Some clinical data has indicated that the alveolar crest tends to move two-thirds lingually/palatally from the original buccal edge; thus, the amount of resorption at the mid-facial point doubled the bone loss at the distal and mesial points.11Covani U, Ricci M, Bozzolo G, Mangano F, Zini A, Barone A. Analysis of the pattern of the alveolar ridge remodelling following single tooth extraction. → Clin Oral Implants Res. 2011 Aug;22(8):820–5.
A recent consensus report assessed that it is important to distinguish between the various procedures used to preserve the alveolar ridge.12Hämmerle CH, Araújo MG, Simion M; Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:80–2. Ridge preservation techniques include all procedures that preserve the ridge volume within the soft- and hard-tissue envelope existing at the time of extraction.13Hämmerle CH, Araújo MG, Simion M; Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:80–2. A ridge preservation procedure is recommended in the following circumstances: when implant placement is not possible at the time of tooth extraction, when the patient is not available for immediate implant placement, when primary stability of the implant cannot be guaranteed, and when treating adolescent patients.14Hämmerle CH, Araújo MG, Simion M; Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:80–2. The use of various techniques and biomaterials has been proposed over time; however, no significant differences have been shown between the various biomaterials, although collagen alone has been proved to be unable to counteract tissue changes after tooth extraction.15Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, Sanz M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:22–38.'16Barone A, Ricci M, Tonelli P, Santini S, Covani U. Tissue changes of extraction sockets in humans: a comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. → Clin Oral Implants Res. 2013 Nov;24(11):1231–7.'17Barone A, Orlando B, Cingano L, Marconcini S, Derchi G, Covani U. A randomized clinical trial to evaluate and compare implants placed in augmented versus non- augmented extraction sockets: 3-year results. → J Periodontol. 2012 Jul;83(7):836–46.
18Oghli AA, Steveling H. Ridge preservation following tooth extraction: a comparison between atraumatic extraction and socket seal surgery. → Quintessence Int. 2010 Jul-Aug;41(7):605–9.19Farina E, Menditti D, De Maria S, Mezzogiorno A, Esposito V, Laino L, Carinci F. A model of human bone regeneration: morphological, cellular and molecular aspects. → J Osseointegration. 2009 Aug;1(2):42–53.
An ideal grafting biomaterial should be resorbable, in order to allow replacement with new bone while balancing the speed of resorption and the volumetric stability. The use of a grafting material with a high resorption rate results in the complete disappearance of the biomaterial after a few months. This has been observed for calcium sulfate after three months and for a poly-lactide-polyglycolide acid sponge after six months.20Serino G, Biancu S, Iezzi G, Piattelli A. Ridge preservation following tooth extraction using a polylactide and polyglycolide sponge as space filler: a clinical and histological study in humans. → Clin Oral Implants Res. 2003 Oct;14(5):651–8. Nevertheless, high resorption of the biomaterial is not always desirable, especially in anatomical sites where vertical and horizontal volumetric shrinkage are expected. The use of collagenated cortico-cancellous porcine bone has shown positive results in socket preservation procedures after three months21Barone A, Borgia V, Covani U, Ricci M, Piattelli A, Iezzi G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. → Clin Oral Implants Res. 2015 Jul;26(7):806–13. Epub 2014 Mar 1.'22Barone A, Toti P, Piattelli A, Iezzi G, Derchi G, Covani U. Extraction socket healing in humans after ridge preservation techniques: comparison between flapless and flapped procedures in a randomized clinical trial. → J Periodontol. 2014 Jan;85(1):14–23. In fact, histological and histomorphometric analyses gave positive results in terms of newly formed bone, absence of inflammatory cells and signs of active resorption of the grafted particles,23Barone A, Borgia V, Covani U, Ricci M, Piattelli A, Iezzi G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. → Clin Oral Implants Res. 2015 Jul;26(7):806–13. Epub 2014 Mar 1. suggesting that collagenated cortico-cancellous porcine bone could be suitable for ridge preservation procedures.
A full-thickness flap elevation during tooth extraction may have accounted for slightly more pronounced bone remodeling compared with a flapless extraction, owing to the interruption of the blood vessels.24Fickl S, Zuhr O, Wachtel H, Stappert CF, Stein JM, Hürzeler MB. Dimensional changes of the alveolar ridge contour after different socket preservation techniques. → J Clin Periodontol. 2008 Aug;35(10):906–13.'25Engler-Hamm D, Cheung WS, Yen A, Stark PC, Griffin T. Ridge preservation using a composite bone graft and a bioabsorbable membrane with and without primary wound closure: a comparative clinical trial. → J Periodontol. 2011 Mar;82(3):377–87.'26Novaes AB Jr, Fernandes PG, Suaid FA, de Moraes Grisi MF, Scombatti de Souza SL, Taba M Jr, Palioto DB, Muglia VA. Ridge preservation with acellular dermal matrix and anorganic bone matrix cell-binding peptide P-15 after tooth extraction in humans. A histologic and morphometric study. → J Osseointegration. 2012 Jun;4(2):23–30. Soft-tissue primary closure was originally considered necessary for proper incorporation of the graft.27Darby I, Chen ST, Buser D. Ridge preservation techniques for implant therapy. → Int J Oral Maxillofac Implants. 2009;24 Suppl:260–71.'28Fickl S, Zuhr O, Wachtel H, Stappert CF, Stein JM, Hürzeler MB. Dimensional changes of the alveolar ridge contour after different socket preservation techniques. → J Clin Periodontol. 2008 Aug;35(10):906–13.'29Lekovic V, Kenney EB, Weinlaender M, Han T, Klokkevold P, Nedic M, Orsini M. Bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of 10 cases. → J Periodontol. 1997 Jun;68(6):563–70.'30Lekovic V, Camargo PM, Klokkevold PR, Weinlaender M, Kenney EB, Dimitrijevic B, Nedic M. Preservation of alveolar bone in extraction sockets using bioabsorbable membranes. → J Periodontol. 1998 Sep;69(9):1044–9. The early exposure of the membrane to the oral cavity was thought to jeopardize the effectiveness of tissue augmentation;31Engler-Hamm D, Cheung WS, Yen A, Stark PC, Griffin T. Ridge preservation using a composite bone graft and a bioabsorbable membrane with and without primary wound closure: a comparative clinical trial. → J Periodontol. 2011 Mar;82(3):377–87.'32Simion M, Maglione M, Iamoni F, Scarano A, Piattelli A, Salvato A. Bacterial penetration through Resolut resorbable membrane in vitro. An histological and scanning electron microscopic study. → Clin Oral Implants Res. 1997 Feb;8(1):23–31. these findings pointed out the importance of achieving full closure and primary healing when the socket is grafted and covered with a membrane.33Darby I, Chen ST, Buser D. Ridge preservation techniques for implant therapy. → Int J Oral Maxillofac Implants. 2009;24 Suppl:260–71.
Experimental models have reported less pronounced bone remodeling when a flapless approach was used for socket preservation,34Fickl S, Zuhr O, Wachtel H, Bolz W, Huerzeler MB. Hard tissue alterations after socket preservation: an experimental study in the beagle dog. → Clin Oral Implants Res. 2008 Nov;19(11):1111–8. but there is still no consensus on the effect of the elevation of a full-thickness flap. However, one study found no significant difference between the flapless and flapped approach.35Araújo MG, Lindhe J. Ridge alteration following tooth extraction with and without flap elevation: an experimental study in the dog. → Clin Oral Implants Res. 2009 Mar;20(6):545–9. A recent study observed the effects of a full-thickness flap elevation on the regenerative process of socket preservation procedures.36Barone A, Borgia V, Covani U, Ricci M, Piattelli A, Iezzi G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. → Clin Oral Implants Res. 2015 Jul;26(7):806–13. Epub 2014 Mar 1. The comparison between the flapped and the flapless procedures showed no significant differences in the histological and histomorphometric analysis, in terms of newly formed bone, residual graft and marrow space rates, suggesting that the exposure of the collagen membrane did not jeopardize the regenerative process.37Barone A, Borgia V, Covani U, Ricci M, Piattelli A, Iezzi G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. → Clin Oral Implants Res. 2015 Jul;26(7):806–13. Epub 2014 Mar 1.
The aim of the current study was to evaluate the clinical outcomes of a ridge preservation technique with a flapless approach in the posterior area of the jaw. Dimensional changes to the hard and soft tissue at fresh extraction sites treated with the use of cortico-cancellous porcine bone and a resorbable collagen membrane were evaluated over the observation period. Bone cores were also harvested at the time of implant placement for histological analysis.
Materials & methods
Study population and design
Patients were recruited from the consultation clinic at the Istituto Stomatologico Toscano, Versilia general hospital, University of Pisa, Lido di Camaiore, Italy, from January 2013 to January 2014. The study was approved by the ethics committee of the Versilia general hospital according to the principles outlined in the Declaration of Helsinki on clinical research involving human subjects. All of the patients received a thorough explanation of the study and completed a written informed consent form prior to being enrolled in the trial.
Forty patients requiring extraction of at least one premolar or one molar and a subsequent implant-supported restoration who were 18 years old or older and able to sign an informed consent form were eligible for inclusion in this trial. One patient showed complete loss of the buccal bone plate immediately after the extraction and two patients did not return for the follow-up examinations. Consequently, these patients were excluded, and 37 patients were included in the study. The patients enrolled in the study had a mean age of 40.5 ± 13.5 and an age range of between 20 and 61.
The exclusion criteria were:
- history of systemic disease that would contraindicate oral surgical treatment
- long-term nonsteroidal anti-inflammatory drug therapy
- intravenous and oral bisphosphonate therapy – lack of the occluding teeth
- absence of adjacent teeth
- complete loss of a bone wall
- surgical sites in the esthetic area
- uncontrolled periodontal disease
- unwillingness to return for the follow-up examination
- smoking of more than ten cigarettes per day — subjects who smoked fewer than ten cigarettes per day were requested to stop smoking before and after surgery; however, their compliance could not be monitored.
Patients who were included in the study were accurately evaluated by examining clinical aspects and periapical and panoramic radiographs. Moreover, data were collected for each patient, including age, sex, smoking habits, and indications for tooth extraction based on both clinical and radiographic examinations, tooth location and the presence or absence of adjacent teeth.
After the consent form had been signed, all of the patients underwent at least one session of scaling and root planing prior to the extraction procedures in order to provide a more favorable oral environment for wound healing. All of the patients underwent the tooth extraction and the ridge preservation procedure at baseline. Four months after tooth extraction, all of the sites were re-entered, bone biopsies were taken and implants were placed.
Surgical treatment
All of the patients received antibiotic therapy (2 g amoxicillin or 600 mg clindamycin, if allergic to penicillin) 1 h before the surgery and continued to take the antibiotic postoperatively (1 g amoxicillin or 300 mg clindamycin) b.i.d. for four days. All of the patients rinsed for 1 min with a 0.2% chlorhexidine mouthwash prior to the surgery (as well as b.i.d. for the following three weeks) and were treated under local anesthesia using lidocaine with 1:50,000 epinephrine. All of the surgical procedures were performed by two surgeons (AB, FA), who received training during a one-week session before beginning the study. The training included calibration for the surgical and follow-up procedures, as well as the handling of any complications. All of the patients were treated with the same surgical technique and periotomes were used around every tooth treated. Moreover, ultrasound bone surgery (PIEZOSURGERY, mectron, Italy) was performed where necessary in order to avoid buccolingual movements of the tooth, thus preventing damage to or a full fracture of the buccal bone wall.
The extraction sockets were thoroughly curetted and irrigated with a sterile saline solution. Cortico-cancellous porcine bone (mp3, Os-teoBiol, Tecnoss Dental, Pianezza, Italy) was lightly condensed inside the socket and a resorbable collagen membrane (Evolution, Osteo-Biol, Tecnoss Dental) was placed over it in order to cover the socket completely. The membrane, which was left exposed to the oral cavity, was stabilized with 4-0 silk sutures, and soft-tissue healing was by secondary intention, since no flap was raised (Figs. 1–8). All of the patients were instructed to continue the antibiotic therapy, and 550 mg naproxen sodium tablets were prescribed as an anti-inflammatory (b.i.d. as necessary). Removable prostheses, if present, were not used for at least three weeks and then adjusted before reuse.
-
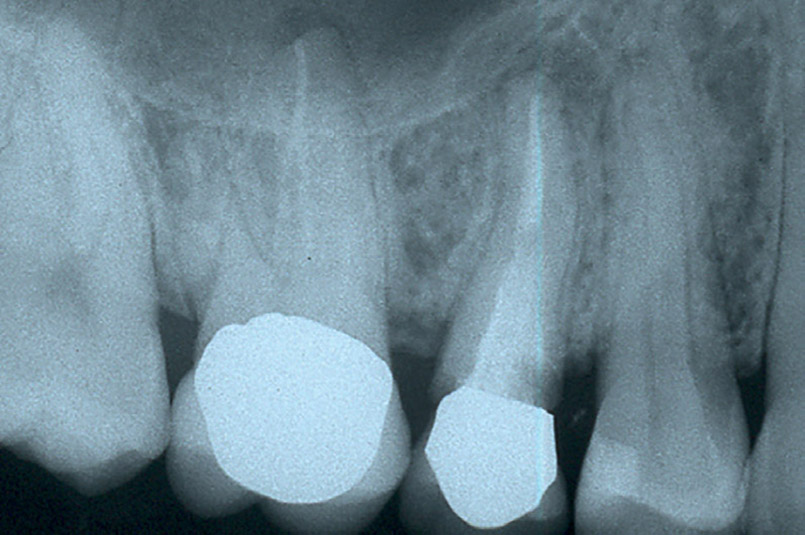
- Preoperative radiograph. Tooth #25 was to be extracted because of nontreatable root decay.
-
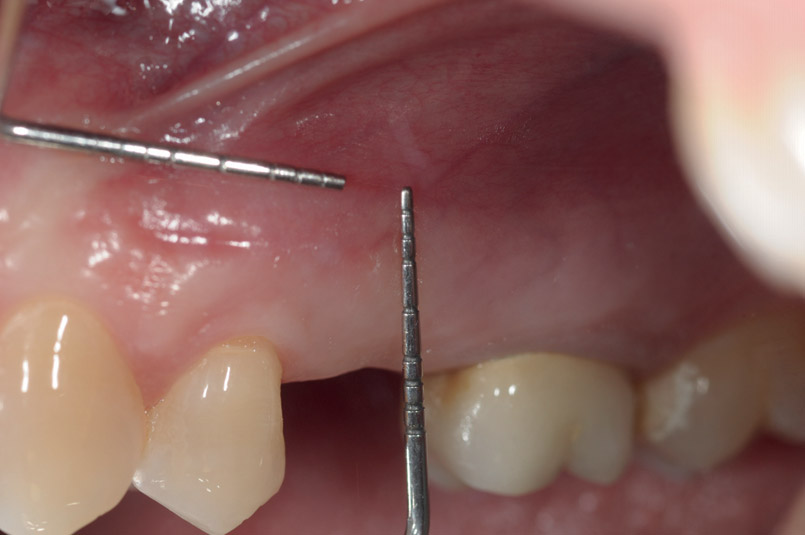
- Example of the probe used for the clinical measurements.
-

- Resin stent positioned on the experimental site in order to standardize the clinical measurements.
-
- Occlusal view of the experimental site showing the preoperative situation.
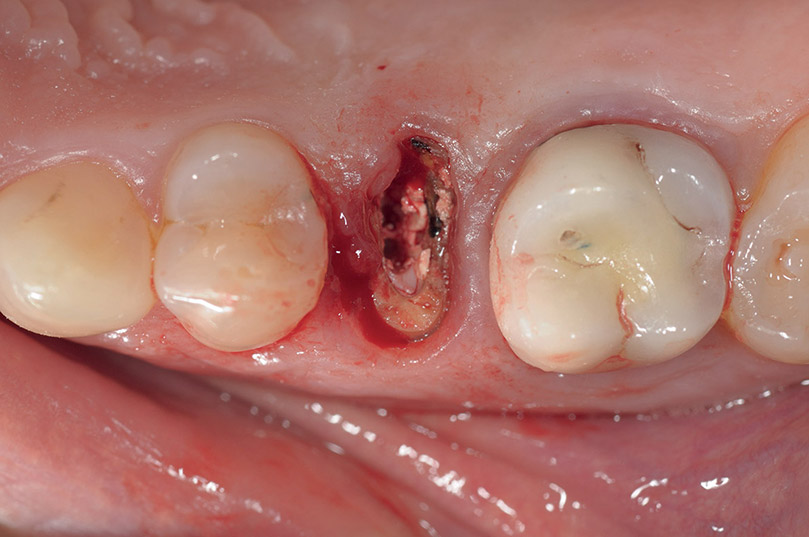
-
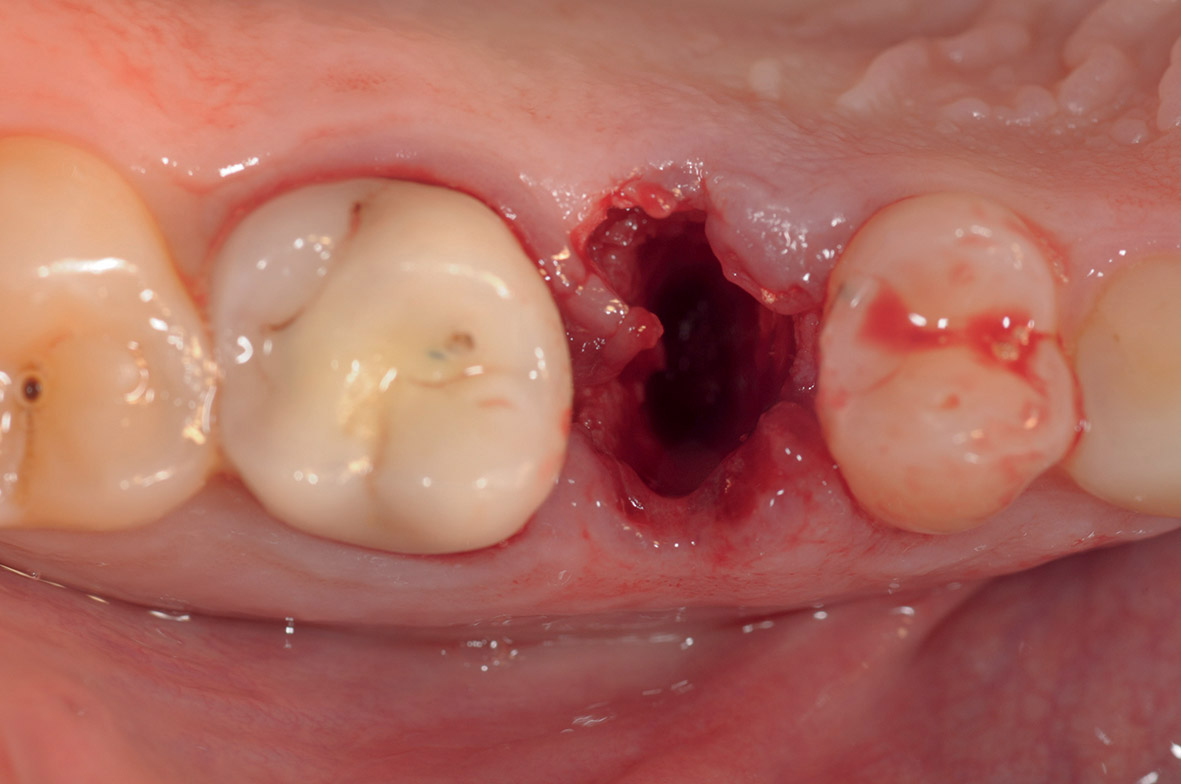
- Post-extraction socket.
-
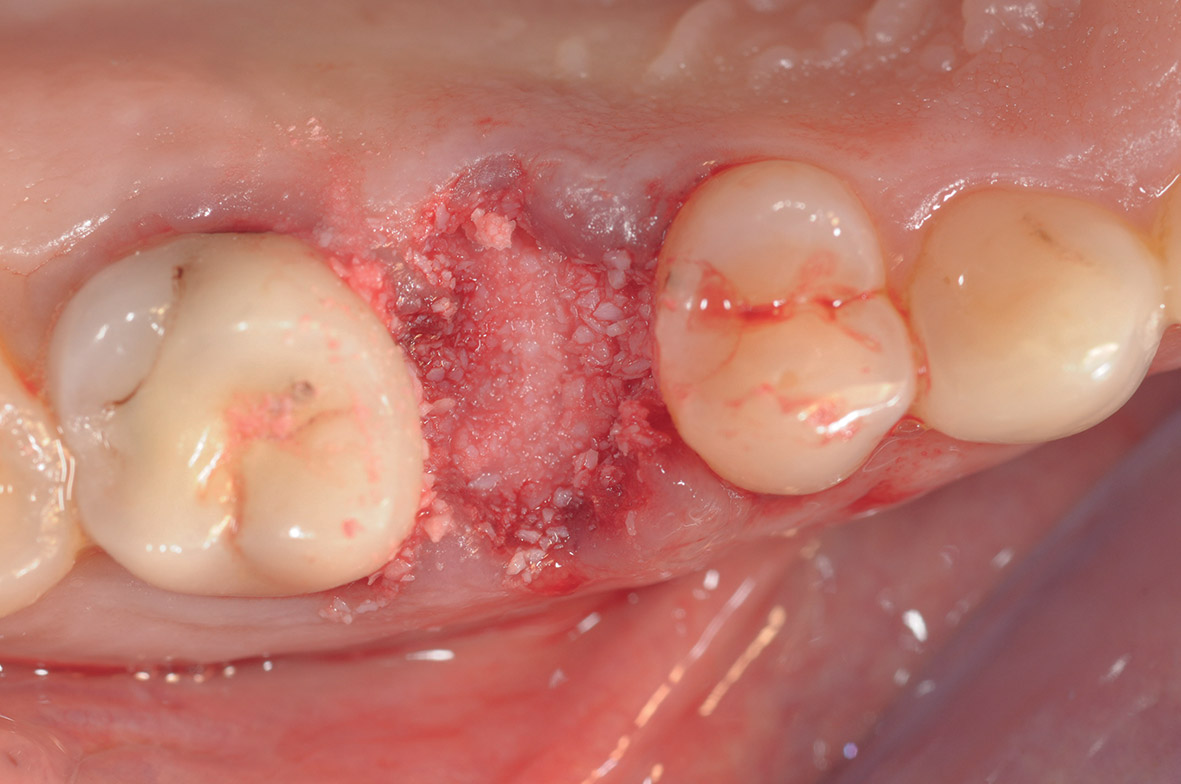
- Cortico-cancellous porcine bone grafted inside the socket.
-
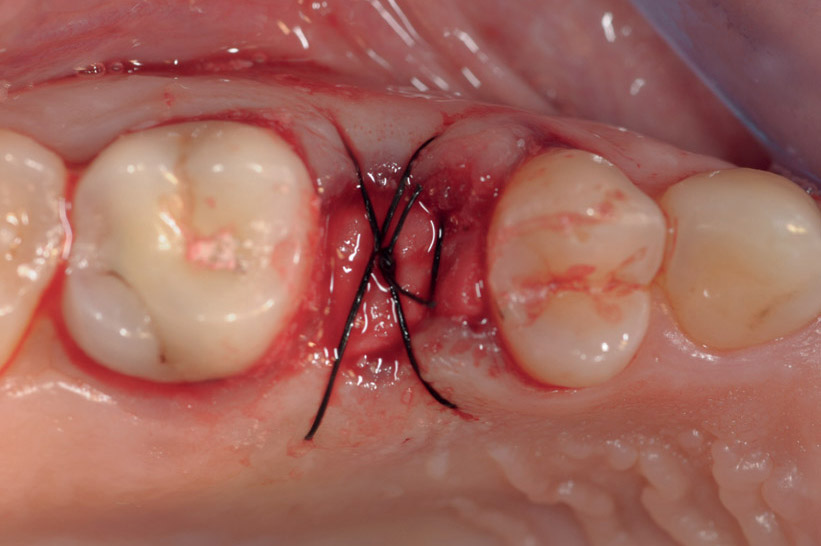
- Sutures used to stabilize the graft and the collagen membrane.
-

- Occlusal view of the experimental site four months after the ridge preservation procedure.
The surgical re-entry was performed four months after the first-stage surgery. Bone biopsies were collected and implants (BL CT, Intra-Lock, Boca Raton, Fla., U.S.) were placed (Fig. 9). Of the implants placed, 61% had a diameter of 5 mm and 39% of 4 mm. Adjunctive augmentation procedures at the time of implant placement were necessary in 7% of the experimental sites. Three months after placement, the implants were uncovered and manually tested for stability (Fig. 10).
-
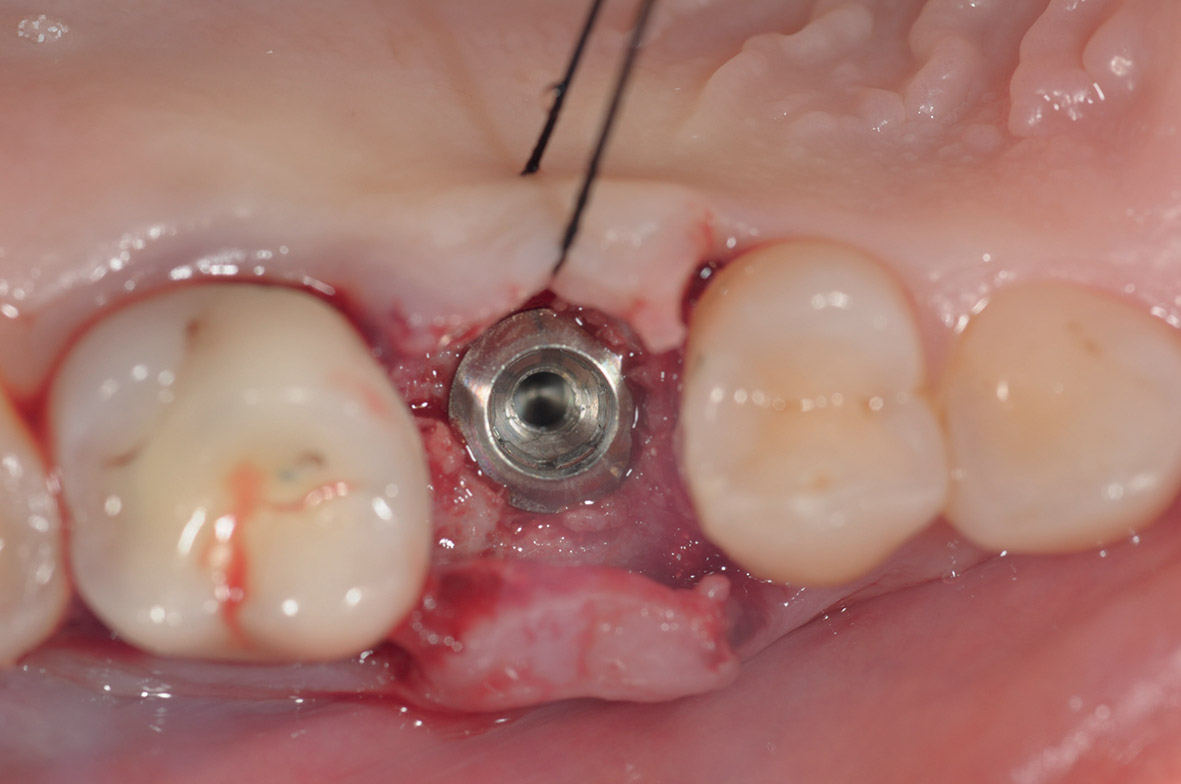
- Implant placement.
-
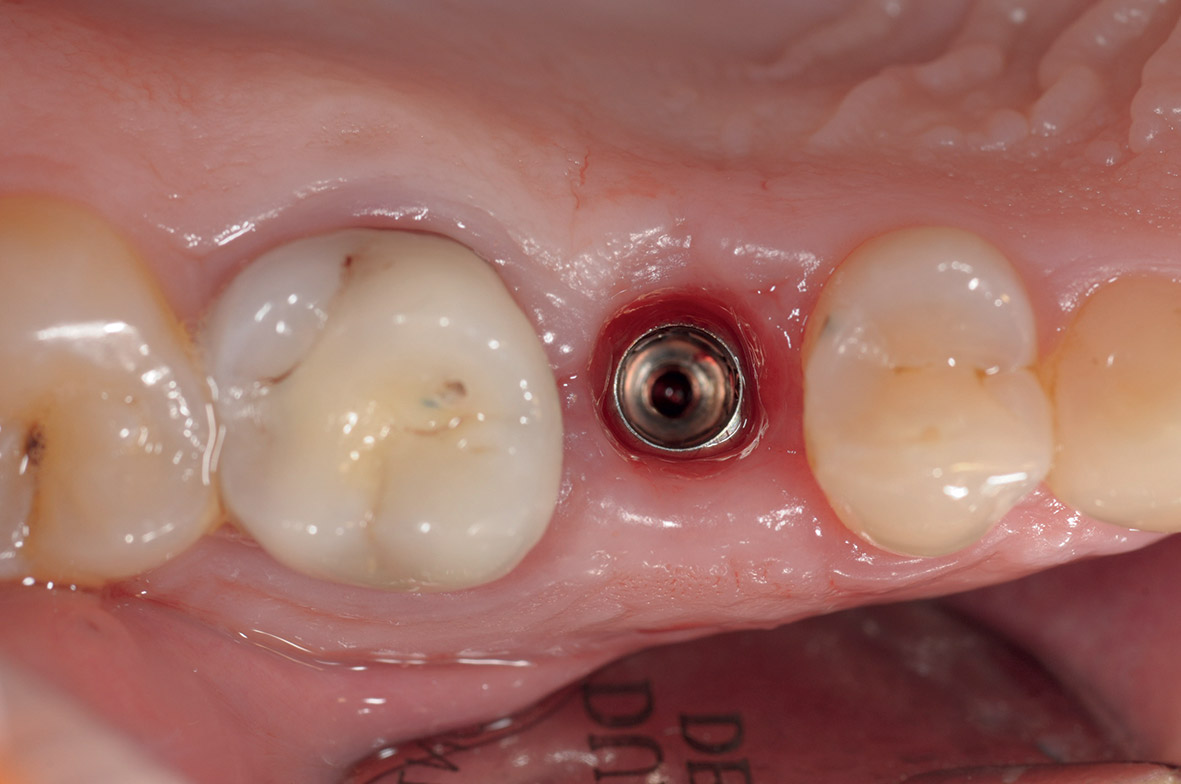
- Implant uncovering.
-

- Radiographs three months after implant placement.
-

- Final prosthesis.
At this time, impressions were taken using a polyvinyl siloxane impression material (Flexitime, Heraeus Kulzer, Hanau, Germany) and customized resin impression trays. Final ceramic restorations were made and seated, and all of the patients were enrolled in an oral hygiene program, with a recall visit every three months(Figs.11&12).
Clinical parameters
Several clinical parameters were measured at each time of examination, including at baseline and four months after the ridge preservation procedure. The clinical parameters taken into consideration in the present study were:
- width of keratinized gingiva, measured at the midfacial point of the buccal aspect using a Williams periodontal probe (at baseline, the measure corresponded to the distance between the mucogingival junction and the gin- gival margin; at the four-month examination, it was the distance between the mucogingival junction and the highest part of the edentulous crest)
- thickness of the buccal bone, measured im-mediately after tooth extraction using a surgical caliper
- vertical bone changes, registered with a surgical stent positioned on the adjacent teeth and measured with a Williams periodontal probe soon after the tooth extraction and at the time of implant placement (four months after the first-stage surgery)
- horizontal bone changes, measured with a Williams periodontal probe soon after the tooth extraction and after four months.
Histological analysis
Bone biopsies were collected during the second-stage surgery. The bone cores were immediately stored in a 10% buffered formalin solution and sent to the Department of Medical and Oral Sciences and Biotechnologies, “Gabriele d’Annunzio” University of Chieti–Pescara, Chieti, Italy. The samples were then processed to obtain thin-ground sections, using the Precise 1 Automated System (Assing, Rome, Italy). The specimens were dehydrated in a graded series of ethanol rinses and embedded in a glycol methacrylate resin (Technovit 7200 VLC, Heraeus Kulzer, Wehrheim, Germany). After polymerization, the specimens were sectioned along the longitudinal axis with a high-precision diamond disc at approximately 150 μm and ground down to approximately 30 μm. Three slides were obtained from each specimen, stained with acid fuchsin and toluidine blue, and examined in transmitted and polarized light using a transmitted light micro-scope (Leitz Laborlux, Leitz, Wetzlar, Germany). One well-trained examiner (GI), who was not involved in the surgical treatment, evaluated the histological results.
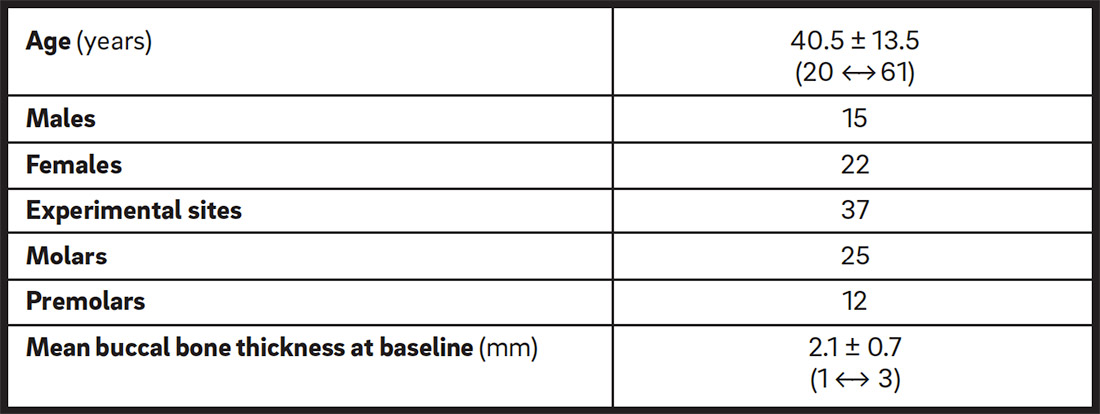
Demographic data.
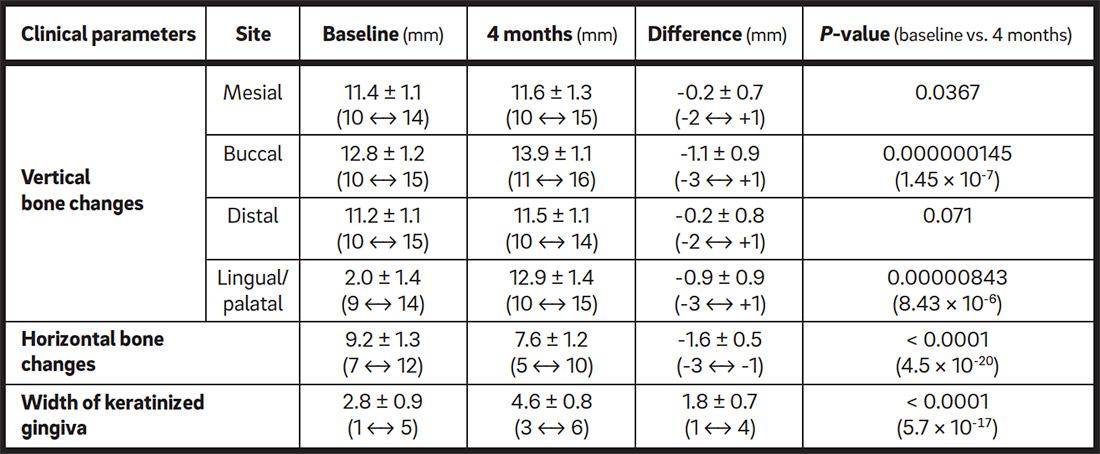
Dimensional changes four months after the ridge preservation procedure.
Statistical analysis
Descriptive statistical analysis was performed on all of the data collected, with SPSS software (Version 6.1.2; SPSS, Chicago, Ill., U.S.). Pearson’s chi-squared test was performed for categorical data. The p-value for significance was set at 0.05. All of the measurements in the text and tables are given as medians and interquartile ranges (the difference between the 75th and 25th percentiles).
Results
A single-tooth extraction with a flapless ridge preservation procedure was performed for each of the 37 patients enrolled in the study, with a total of 25 molars and 12 premolars that needed to be extracted owing to fracture (42%), non-treatable endodontic lesions (14%) and severe root decay (44%). All of the surgical procedures performed in this study were successful and no complications were observed during the healing period (Table 1).
At baseline, the mean width of keratinized gingiva was 2.8 ± 0.9 mm (range of 1.0–5.0 mm). After four months, it was 4.6 ± 0.8 mm, showing an increase of 1.8 ± 0.7 mm, which was statistically significant (p = 0.0001).
The thickness of the buccal bone was measured at baseline and ranged from 1.0 to 3.0 mm, with a mean of 2.1 ± 0.7 mm (Table 1). The mean width of the alveolar crest at baseline was 9.2 ± 1.3 mm, and after four months, it was 7.6 ± 1.2 mm; therefore, the mean width of the alveolar crest showed a decrease of 1.6 ± 0.5 mm (p < 0.0001). The comparison between the thickness of the buccal bone wall and the width of the alveolar crest indicated that the correlation between the two values was statistically significant (Table 2).
Four months after the ridge preservation procedure, the vertical bone loss was 0.2 ± 0.7 mm for mesial sites, 1.1 ± 0.9 mm for buccal sites, 0.2 ± 0.8 mm for distal sites and 0.9 ± 0.9 mm for palatal/lingual sites. The dimensional changes were statistically significant for all of the sites (Table2).
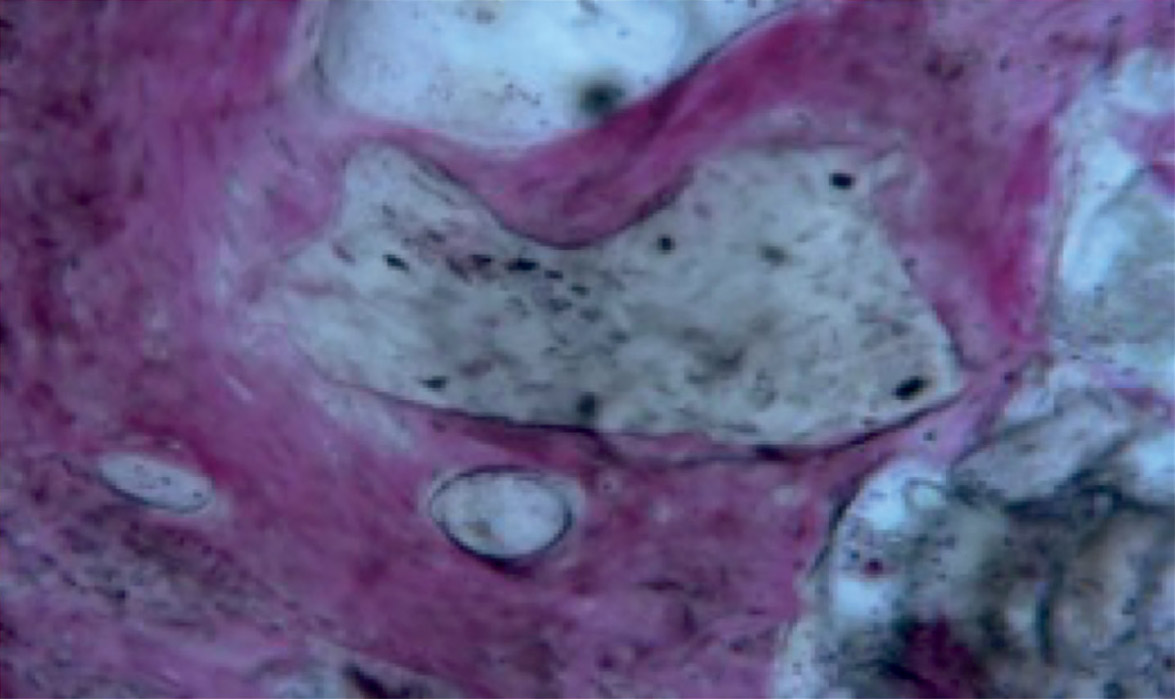 Fig. 13
Fig. 13Newly formed bone around the grafting material. No inflammatory cells or foreign body reaction was observed.
The histological analysis performed on the retrieved bone cores found that the granules of grafted bone were still present, even though new trabecular bone could be observed in all of the specimens. Osteocytic lacunae could be seen on the particles’ surfaces, and newly formed bone was observed inside some of the resorption areas of the biomaterial. Vascular growth close to the newly formed bone was also evident, and no inflammatory cells or foreign body reaction around the biomaterial granules was observed (Fig. 13).
Discussion
Ridge preservation techniques have been proposed in order to reduce the bone volume shrinkage that follows a tooth extraction, since several studies have reported resorption of both vertical and horizontal dimensions.38Barone A, Aldini NN, Fini M, Giardino R, Calvo Guirado JL, Covani U. Xenograft versus extraction alone for ridge preservation after tooth removal: a clinical and histomorphometric study. → J Periodontol. 2008 Aug 79(8):1370–7.'39Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction: an experimental study in the dog. → J Clin Periodontol. 2005 Feb;32(2):212–8.'40Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. → Int J Periodontics Restorative Dent. 2003 Jul-Aug;23(4):313–23.'41Van der Weijden F, Dell’Acqua F, Slot DE. Alveolar bone dimensional changes of post- extraction sockets in humans: a systematic review. → J Clin Periodontol. 2009 Dec;36(12):1048–58. The use of various biomaterials and techniques has been proposed over time, but there is still no evidence to indicate the best choice. In the present study, 37 single-tooth extractions and the subsequent flapless ridge preservation procedures were performed. Cortico-cancellous porcine bone and a resorbable collagen membrane were used in all of the cases, and several clinical parameters were measured at the tooth extraction and after four months, including width of keratinized gingiva, thickness of the buccal bone wall, and changes to the vertical and horizontal dimensions.
A minimally invasive tooth extraction technique, with preservation of the socket walls during the surgery, helps to maintain the architecture of the alveolar crest,42Barone A, Aldini NN, Fini M, Giardino R, Calvo Guirado JL, Covani U. Xenograft versus extraction alone for ridge preservation after tooth removal: a clinical and histomorphometric study. → J Periodontol. 2008 Aug 79(8):1370–7.'43Barone A, Ricci M, Tonelli P, Santini S, Covani U. Tissue changes of extraction sockets in humans: a comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. → Clin Oral Implants Res. 2013 Nov;24(11):1231–7. even if bone remodeling is not completely avoidable.44Fickl S, Zuhr O, Wachtel H, Stappert CF, Stein JM, Hürzeler MB. Dimensional changes of the alveolar ridge contour after different socket preservation techniques. → J Clin Periodontol. 2008 Aug;35(10):906–13. A flapless surgical technique was chosen in our study because, even though some studies have not reported any significant differences between a flapped and a flapless surgical technique,45Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, Sanz M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:22–38.'46Vittorini Orgeas G, Clementini M, De Risi V, de Sanctis M. Surgical techniques for alveolar socket preservation: a systematic review. → Int J Oral Maxillofac Implants. 2013 Jul-Aug;28(4):1049–61. Van der Weijden et al. assert that the elevation of a full-thickness flap is believed to compromise the blood supply, limiting the future regenerative potential.47Van der Weijden F, Dell’Acqua F, Slot DE. Alveolar bone dimensional changes of post- extraction sockets in humans: a systematic review. → J Clin Periodontol. 2009 Dec;36(12):1048–58. Furthermore, the use of a flapless technique has been demonstrated to be less traumatic for both hard tissue—avoiding interruption of the blood flow—and soft tissue—preserving the keratinized gingiva.48Novaes AB Jr, Martins de Barros RR, Papalexiou V, Gonçalves de Almeida AL. Buccal bone loss after immediate implantation can be reduced by the flapless approach. → J Osseointegration. 2011 Oct;3(3):45–55.'49Barone A, Toti P, Piattelli A, Iezzi G, Derchi G, Covani U. Extraction socket healing in humans after ridge preservation techniques: comparison between flapless and flapped procedures in a randomized clinical trial. → J Periodontol. 2014 Jan;85(1):14–23.'50Cardaropoli D, Cardaropoli G. Preservation of the postextraction alveolar ridge: a clinical and histologic study. → Int J Periodontics Restorative Dent. 2008 Sep-Oct;28(5):469–77. The exposure of the collagen membrane and the soft-tissue closure by secondary intention seemed not to jeopardize the bone healing, and 100% of the ridge preservation procedures were successful. The width of the keratinized gingiva gained 1.8 ± 0.7 mm after four months. These results correspond to those of other studies that used a similar surgical protocol.51Barone A, Borgia V, Covani U, Ricci M, Piattelli A, Iezzi G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. → Clin Oral Implants Res. 2015 Jul;26(7):806–13. Epub 2014 Mar 1.
The evaluation of the clinical parameters in this study confirmed the efficacy of this surgical procedure in counteracting the soft- and hard-tissue shrinkage after a tooth extraction: both the vertical and horizontal dimensions showed a minimal decrease. In particular, the vertical dimension lost 0.2 ± 0.7 mm at the mesial sites, 1.1 ± 0.9 mm at the buccal sites, 0.2 ± 0.8 mm at the distal sites and 0.9 ± 0.9 mm at the palatal/lingual sites after four months. These results are in keeping with those reported in a recent systematic review that compared the outcomes after tooth extractions with and without ridge preservation procedures.52Morjaria KR, Wilson R, Palmer RM. Bone healing after tooth extraction with or without an intervention: a systematic review of randomized controlled trials. → Clin Implant Dent Relat Res. 2014 Feb;16(1):1–20. In the case of the ridge preservation procedures, the vertical bone changes ranged from a gain of 1.3 ± 2.0 mm to a loss of 0.62 ± 0.51 mm, with follow-up times ranging from three to nine months.53Morjaria KR, Wilson R, Palmer RM. Bone healing after tooth extraction with or without an intervention: a systematic review of randomized controlled trials. → Clin Implant Dent Relat Res. 2014 Feb;16(1):1–20.
In the current study, the ridge preservation procedures in all of the experimental sites were successful, and implants were placed after four months, with further augmentation procedures being necessary only in 7% of the cases at the time of implant placement. Moreover, bone cores were harvested for the histological analysis at the time of implant placement. Corroborating the findings of other studies,54Iezzi G, Degidi M, Piattelli A, Mangano C, Scarano A, Shibli JA, Perrotti V. Comparative histological results of different biomaterials used in sinus augmentation procedures: a human study at 6 months. → Clin Oral Implants Res. 2012 Dec;23(12):1369–76.’ 55Nannmark U, Sennerby L. The bone tissue responses to prehydrated and collagenated cortico-cancellous porcine bone grafts: a study in rabbit maxillary defects. → Clin Implant Dent Relat Res. 2008 Dec;10(4):264–70. this study found that the cortico-cancellous porcine bone was effective in maintaining the architecture of post-extraction sockets and demonstrated signs of active resorption at the same time. Iezzi et al. examined the use of various biomaterials and performed histological and histomorphometric analyses after six months.56Iezzi G, Degidi M, Piattelli A, Mangano C, Scarano A, Shibli JA, Perrotti V. Comparative histological results of different biomaterials used in sinus augmentation procedures: a human study at 6 months. → Clin Oral Implants Res. 2012 Dec;23(12):1369–76. Among the different grafting materials, cortico-cancellous porcine bone gave rise to a rim of osteoblasts with signs of active bone matrix deposition; in some areas, bone apposition was observed directly on the particles’ surfaces.57Iezzi G, Degidi M, Piattelli A, Mangano C, Scarano A, Shibli JA, Perrotti V. Comparative histological results of different biomaterials used in sinus augmentation procedures: a human study at 6 months. → Clin Oral Implants Res. 2012 Dec;23(12):1369–76. Similarly, the biomaterial used in this study showed a great percentage of newly formed bone. No inflammatory cells or foreign body reaction was observed in the bone samples, but new bone tissue and blood vessel growth. Active resorption signs were evident, since osteocytic lacunae were observed at the surface of the biomaterial granules. As found by another study,58Nannmark U, Sennerby L. The bone tissue responses to prehydrated and collagenated cortico-cancellous porcine bone grafts: a study in rabbit maxillary defects. → Clin Implant Dent Relat Res. 2008 Dec;10(4):264–70. collagenated porcine bone was demonstrated to be resorbable, showing active resorption signs on the surface of the particles.
Another study investigated the effect of the exposure of the resorbable membrane to the oral cavity on bone healing, comparing a flapped and a flapless approach.59Barone A, Borgia V, Covani U, Ricci M, Piattelli A, Iezzi G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. → Clin Oral Implants Res. 2015 Jul;26(7):806–13. Epub 2014 Mar 1. The percentages of newly formed bone, residual graft particles and marrow spaces were similar for the two groups, suggesting that the exposure of the collagen membrane had no detrimental effect on the regenerative process.60Barone A, Borgia V, Covani U, Ricci M, Piattelli A, Iezzi G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. → Clin Oral Implants Res. 2015 Jul;26(7):806–13. Epub 2014 Mar 1. Similarly, in our study, the secondary intention healing seemed not to affect the bone quality, as seen in the bone cores. The findings of this study support the hypothesis that secondary intention healing and exposure of the collagen membrane do not jeopardize bone regeneration, but improve the amount of keratinized gingiva. The ridge preservation technique was demonstrated to be effective in maintaining an adequate bone architecture, allowing the subsequent implant placement without adjunctive augmentation procedures in the majority of the cases.
Further studies are necessary to evaluate the influence of early exposure of the membrane on the formation of new bone and on the integration of the grafting material over time. Furthermore, a longer follow-up period could be useful in order to monitor the success of the biomaterial and the quality of the newly formed bone.
Conclusion
Within the limits of this prospective cohort study, ridge preservation showed adequate regeneration of the bone and stability of the facial soft-tissue level. The flapless ridge preservation procedure maintained the horizontal and vertical bone di- mensions, improving the amount of keratinized tissue. The exposure of the resorbable collagen membrane to the oral cavity seemed not to jeop- ardize the healing process or the quality of the newly formed bone.
Competing Interests
The authors declare that they have no conflict of interests related to this study.
References
| 1, 38, 42. | ↑ | Barone A, Aldini NN, Fini M, Giardino R, Calvo Guirado JL, Covani U. Xenograft versus extraction alone for ridge preservation after tooth removal: a clinical and histomorphometric study. → J Periodontol. 2008 Aug 79(8):1370–7. |
| 2, 27, 33. | ↑ | Darby I, Chen ST, Buser D. Ridge preservation techniques for implant therapy. → Int J Oral Maxillofac Implants. 2009;24 Suppl:260–71. |
| 3, 12, 13, 14. | ↑ | Hämmerle CH, Araújo MG, Simion M; Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:80–2. |
| 4, 16, 43. | ↑ | Barone A, Ricci M, Tonelli P, Santini S, Covani U. Tissue changes of extraction sockets in humans: a comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. → Clin Oral Implants Res. 2013 Nov;24(11):1231–7. |
| 5, 8, 15, 45. | ↑ | Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, Sanz M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:22–38. |
| 6, 39. | ↑ | Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction: an experimental study in the dog. → J Clin Periodontol. 2005 Feb;32(2):212–8. |
| 7, 40. | ↑ | Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. → Int J Periodontics Restorative Dent. 2003 Jul-Aug;23(4):313–23. |
| 9, 11. | ↑ | Covani U, Ricci M, Bozzolo G, Mangano F, Zini A, Barone A. Analysis of the pattern of the alveolar ridge remodelling following single tooth extraction. → Clin Oral Implants Res. 2011 Aug;22(8):820–5. |
| 10, 24, 28, 44. | ↑ | Fickl S, Zuhr O, Wachtel H, Stappert CF, Stein JM, Hürzeler MB. Dimensional changes of the alveolar ridge contour after different socket preservation techniques. → J Clin Periodontol. 2008 Aug;35(10):906–13. |
| 17. | ↑ | Barone A, Orlando B, Cingano L, Marconcini S, Derchi G, Covani U. A randomized clinical trial to evaluate and compare implants placed in augmented versus non- augmented extraction sockets: 3-year results. → J Periodontol. 2012 Jul;83(7):836–46. |
| 18. | ↑ | Oghli AA, Steveling H. Ridge preservation following tooth extraction: a comparison between atraumatic extraction and socket seal surgery. → Quintessence Int. 2010 Jul-Aug;41(7):605–9. |
| 19. | ↑ | Farina E, Menditti D, De Maria S, Mezzogiorno A, Esposito V, Laino L, Carinci F. A model of human bone regeneration: morphological, cellular and molecular aspects. → J Osseointegration. 2009 Aug;1(2):42–53. |
| 20. | ↑ | Serino G, Biancu S, Iezzi G, Piattelli A. Ridge preservation following tooth extraction using a polylactide and polyglycolide sponge as space filler: a clinical and histological study in humans. → Clin Oral Implants Res. 2003 Oct;14(5):651–8. |
| 21, 23, 36, 37, 51, 59, 60. | ↑ | Barone A, Borgia V, Covani U, Ricci M, Piattelli A, Iezzi G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: a histological evaluation in a randomized clinical trial. → Clin Oral Implants Res. 2015 Jul;26(7):806–13. Epub 2014 Mar 1. |
| 22, 49. | ↑ | Barone A, Toti P, Piattelli A, Iezzi G, Derchi G, Covani U. Extraction socket healing in humans after ridge preservation techniques: comparison between flapless and flapped procedures in a randomized clinical trial. → J Periodontol. 2014 Jan;85(1):14–23. |
| 25, 31. | ↑ | Engler-Hamm D, Cheung WS, Yen A, Stark PC, Griffin T. Ridge preservation using a composite bone graft and a bioabsorbable membrane with and without primary wound closure: a comparative clinical trial. → J Periodontol. 2011 Mar;82(3):377–87. |
| 26. | ↑ | Novaes AB Jr, Fernandes PG, Suaid FA, de Moraes Grisi MF, Scombatti de Souza SL, Taba M Jr, Palioto DB, Muglia VA. Ridge preservation with acellular dermal matrix and anorganic bone matrix cell-binding peptide P-15 after tooth extraction in humans. A histologic and morphometric study. → J Osseointegration. 2012 Jun;4(2):23–30. |
| 29. | ↑ | Lekovic V, Kenney EB, Weinlaender M, Han T, Klokkevold P, Nedic M, Orsini M. Bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of 10 cases. → J Periodontol. 1997 Jun;68(6):563–70. |
| 30. | ↑ | Lekovic V, Camargo PM, Klokkevold PR, Weinlaender M, Kenney EB, Dimitrijevic B, Nedic M. Preservation of alveolar bone in extraction sockets using bioabsorbable membranes. → J Periodontol. 1998 Sep;69(9):1044–9. |
| 32. | ↑ | Simion M, Maglione M, Iamoni F, Scarano A, Piattelli A, Salvato A. Bacterial penetration through Resolut resorbable membrane in vitro. An histological and scanning electron microscopic study. → Clin Oral Implants Res. 1997 Feb;8(1):23–31. |
| 34. | ↑ | Fickl S, Zuhr O, Wachtel H, Bolz W, Huerzeler MB. Hard tissue alterations after socket preservation: an experimental study in the beagle dog. → Clin Oral Implants Res. 2008 Nov;19(11):1111–8. |
| 35. | ↑ | Araújo MG, Lindhe J. Ridge alteration following tooth extraction with and without flap elevation: an experimental study in the dog. → Clin Oral Implants Res. 2009 Mar;20(6):545–9. |
| 41, 47. | ↑ | Van der Weijden F, Dell’Acqua F, Slot DE. Alveolar bone dimensional changes of post- extraction sockets in humans: a systematic review. → J Clin Periodontol. 2009 Dec;36(12):1048–58. |
| 46. | ↑ | Vittorini Orgeas G, Clementini M, De Risi V, de Sanctis M. Surgical techniques for alveolar socket preservation: a systematic review. → Int J Oral Maxillofac Implants. 2013 Jul-Aug;28(4):1049–61. |
| 48. | ↑ | Novaes AB Jr, Martins de Barros RR, Papalexiou V, Gonçalves de Almeida AL. Buccal bone loss after immediate implantation can be reduced by the flapless approach. → J Osseointegration. 2011 Oct;3(3):45–55. |
| 50. | ↑ | Cardaropoli D, Cardaropoli G. Preservation of the postextraction alveolar ridge: a clinical and histologic study. → Int J Periodontics Restorative Dent. 2008 Sep-Oct;28(5):469–77. |
| 52, 53. | ↑ | Morjaria KR, Wilson R, Palmer RM. Bone healing after tooth extraction with or without an intervention: a systematic review of randomized controlled trials. → Clin Implant Dent Relat Res. 2014 Feb;16(1):1–20. |
| 54, 56, 57. | ↑ | Iezzi G, Degidi M, Piattelli A, Mangano C, Scarano A, Shibli JA, Perrotti V. Comparative histological results of different biomaterials used in sinus augmentation procedures: a human study at 6 months. → Clin Oral Implants Res. 2012 Dec;23(12):1369–76. |
| 55, 58. | ↑ | Nannmark U, Sennerby L. The bone tissue responses to prehydrated and collagenated cortico-cancellous porcine bone grafts: a study in rabbit maxillary defects. → Clin Implant Dent Relat Res. 2008 Dec;10(4):264–70. |





Leave a Reply
Be the First to Comment!