How can the tapered implant design influence bundle bone preservation: An experimental study in American Foxhound dogs
September 18, 2017 / Categories: Digital Dentistry, Implant Dentistry

Calvo Guirado, José Luis

Maté Sánchez de Val, José Eduardo

Ramírez Fernández, Maria Piedad

Pérez Albacete Martínez, Carlos
Delgado Ruiz, Rafael Arcesio

Gehrke, Sérgio Alexandre

Benítez García, José Antonio

Domínguez, Manuel Fernández
Abstract
Objective
The objective of the present study was to evaluate bone–implant contact (BIC) in a new implant design after immediate and delayed placement at different levels in relation to crestal bone in American Foxhound dogs.
Materials and methods
The second, third and fourth mandibular premolars and first molars of 6 American Foxhound dogs were extracted bilaterally. At random, 4 immediate implants were placed in the hemimandibles of each dog in the crestal (control group) and subcrestal position (test group). Three dogs were allowed a healing period of 8 weeks; the other 3 had a healing period of 12 weeks. After the healing periods, histomorphometric analysis of the specimens was performed to measure BIC values and bone remodeling in crestal and subcrestal implants.
Results
All of the implants healed without incident and were available for histological analysis. Lower bone resorption was observed in the group of implants placed subcrestally in healed bone and immediately postextraction.
Conclusion
Our findings suggest that less resorption can be expected when implants are inserted 2 mm subcrestally overall for both immediate and deferred implants compared with placement at the crestal level. In addition, higher BIC values were found at 12 weeks of follow-up in the group of implants placed subcrestally in healed bone compared with those placed subcrestally immediately.
Keywords
Top DM, tapered implants, healed bone.
Introduction
After loss of a tooth, there is progressive involution of the alveolar bone in both the horizontal and vertical dimensions.1Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog.
→ J Clin Periodontol. 2005 Feb;32(2):212–8. 2Araújo MG, Sukekava F, Wensström JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog.
→ J Clin Periodontol. 2005 Jun;32(6):645–52. 3Botticelli D, Berglundh T, Lindhe J. The influence of a biomaterial on the closure of a marginal hard tissue defect adjacent to implants. An experimental study in the dog.
→ Clin Oral Implants Res. 2004 Jun;15(3):285–92.4Botticelli D, Berglundh T, Lindhe J. Resolution of bone defects of varying dimension and configuration in the marginal portion of the peri-implant bone. An experimental study in the dog.
→ J Clin Periodontol. 2004 Apr;31(4):309–17. In addition, the most rapid reduction of alveolar bone after dental extraction occurs during the first months.5Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog.
→ J Clin Periodontol. 2005 Feb;32(2):212–8. 6Araújo MG, Sukekava F, Wensström JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog.
→ J Clin Periodontol. 2005 Jun;32(6):645–52.
For more than a decade, different clinical studies have demonstrated that immediate implant placement in fresh extraction sites may be an effective therapy not only because it reduces the number of surgical procedures,7Nemcovsky CE, Artzi Z, Moses O, Gelernter I. Healing of marginal defects at implants placed in fresh extraction sockets or after 4-6 weeks of healing. A comparative study.
→ Clin Oral Implants Res. 2002 Aug;13(4):410–9. 8Paolantonio M, Dolci M, Scarano A, d’Archivio D, di Placido G, Tumini V, Piattelli A. Immediate implantation in fresh extraction sockets. A controlled clinical and histological study in man.
→ J Periodontol. 2001 Nov;72(11):1560–71. but also because it favors the preservation of the ridges’ morphological contours and simplifies clinical techniques. 9Becker BE, Becker W, Ricci A, Geurs N. A prospective clinical trial of endosseous screw-shaped implants placed at the time of tooth extraction without augmentation.
→ J Periodontol. 1998 Aug;69(8):920–6. 10Grunder U, Polizzi G, Goene R, Hatano N, Henry P, Jackson WJ, Kawamura K, Köhler S, Renouard F, Rosenberg R, Triplett G, Werbitt M, Lithner B. A 3-year prospective multicenter follow-up report on the immediate and delayed-immediate placement of implants.
→ Int J Oral Maxillofac Implants. 1999 Mar-Apr;14(2):210–6.11Lazzara RJ. Immediate implant placement into extraction sites: surgical and restorative advantages.
→ Int J Periodontics Restorative Dent. 1989;9(5):332–43.12Schwartz-Arad D, Chaushu G. Placement of implants into fresh extraction sites: 4 to 7 years retrospective evaluation of 95 immediate implants.
→ J Periodontol. 1997 Nov;68(11):1110–6. 13Schwartz-Arad D, Chaushu G. The ways and wherefores of immediate placement of implants into fresh extraction sites: a literature review.
→ J Periodontol. 1997 Oct;68(10):915–23. Bone remodeling begins directly after the preparation of the implant bed, as well as the healing process of the bone. Osteoblast adhesion to the implant surface and the osseointegration process begins approximately 3 weeks after surgery.14Terheyden H, Stadlinger B, Sanz M, Garbe AI, Meyle J. Inflammatory reaction – communication of cells.
→ Clin Oral Implants Res. 2014 Apr;25(4):399–407. During this healing process, bone remodeling occurs.15Iezzi G, Degidi M, Shibli JA, Vantaggiato G, Piattelli A, Perrotti V. Bone response to dental implants after a 3- to 10-year loading period: a histologic and histomorphometric report of four cases.
→ Int J Periodontics Restorative Dent. 2013 Nov-Dec;33(6):755–61. 16Schwarz F, Alcoforado G, Nelson K, Schaer A, Taylor T, Beuer F, Strietzel, FP. Impact of implant-abutment connection, positioning of the machined collar/microgap, and platform switching on crestal bone level changes. Camlog Foundation consensus report.
→ Clin Oral Implants Res. 2014 Nov;25(11):1301–3. This often results in crestal bone loss.17Hermann JS, Buser D, Schenk RK, Higginbottom FL, Cochran DL. Biologic width around titanium implants. A physiologically formed and stable dimension over time.
→ Clin Oral Implants Res. 2000 Feb;11(1):1–11. 18Hermann JS, Buser D, Schenk RK, Schoolfield JD, Cochran DL. Biologic width around one- and two-piece titanium implants.
→ Clin Oral Implants Res. 2001 Dec;12(6):559–71. However, findings from experiments in humans and dogs have demonstrated that marked reduction in the height of the alveolar ridge occurred consistently after tooth extraction4 and that implant placement in fresh extraction sockets had no effect on the process of bone modeling. 19Araújo MG, Sukekava F, Wensström JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog.
→ J Clin Periodontol. 2005 Jun;32(6):645–52. 20Barros RR, Novaes AB Jr, Papapelxiou V. Buccal bone remodeling after immediate implantation with a flap or flapless approach. A pilot study in dogs.
→ Titanium. 2009;1:45–51. 21Botticelli D, Berglundh T, Lindhe J. The influence of a biomaterial on the closure of a marginal hard tissue defect adjacent to implants. An experimental study in the dog.
→ Clin Oral Implants Res. 2004 Jun;15(3):285–92. 22Botticelli D, Berglundh T, Lindhe J. Resolution of bone defects of varying dimension and configuration in the marginal portion of the peri-implant bone. An experimental study in the dog.
→ J Clin Periodontol. 2004 Apr;31(4):309–17.
Several authors have studied the clinical and radiographic changes that occur around dental implants inserted at different levels in relation to the crestal bone. Clinically, implants are often placed subcrestally in esthetic areas to avoid exposure to metals and to create sufficient space to develop a suitable emergence profile.23Buser D, Martin WC, Belser UC. Surgical considerations for single-tooth replacements in the esthetic zone: standard procedures in sites without bone deficiencies.
→ In: Belser UC, Martin W, Jung R, Hammerle CH, Schmid B, Morton D, Buser D, editors. ITI treatment guide. Vol. 1, Implant therapy in the esthetic zone. Single-tooth replacements. Berlin: Quintessence. 2007. p. 26–37. Subcrestal placement of implants may have an additional benefit, as it improves bone–implant contact (BIC) in the neck region of the implant.24Hämmerle CH, Brägger U, Bürgin W, Lang NP. The effect of subcrestal placement of the polished surface of ITI implants on marginal soft and hard tissues.
→ Clin Oral Implants Res. 1996 Jun;7(2):111–9. 25Welander M, Abrahamsson I, Berglundh T. Placement of two-part implants in sites with different buccal and lingual bone heights.
→ J Periodontol. 2009 Feb;80(2):324–9.
Positioning the implant–abutment junction more apically contributes to the maintenance of mucosal texture and tonality and favors the re-establishment of marginal tissue architecture. 26Fickl S, Zuhr O, Stein JM, Hürzeler MB. Peri-implant bone level around implants with platform-switched abutments.
→ Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):577–81. Thus, different microgap designs result in different shapes and sizes of the periimplant (dis-shaped) bone defect in submerged implants in either equicrestal or subcrestal positions.58 A previous animal study evaluated bone remodeling and BIC after immediate placement at different levels in relation to the crestal bone of beagle dogs. Cylindrical and tapered implants were inserted crestally and 2 mm subcrestally. These studies suggested that apical positioning of the top of the implant does not jeopardize bone crest and periimplant tissue remodeling.
However, less resorption was observed when implants were placed 2 mm subcrestally. Moreover, higher BIC values were found in implants placed subcrestally.27Negri B, Calvo-Guirado JL, Ramírez-Fernández MP, Maté Sánchezde Val J, Guardia J, Muñoz-Guzón F. Peri-implant bone reactions to immediate implants placed at different levels in relation to crestal bone. Part II: a pilot study in dogs.
→ Clin Oral Implants Res. 2012 Feb;23(2):236–44. 28Negri B, Calvo-Guirado JL, Pardo-Zamora G, Ramírez-Fernández MP, Delgado-Ruíz RA, Muñoz-Guzón F. Peri-implant bone reactions to immediate implants placed at different levels in relation to crestal bone. Part I: a pilot study in dogs.
→ Clin Oral Implants Res. 2012 Feb;23(2):228–35.
Bone–implant contact is among the most important factors contributing to implant stability. Thus, many authors have specified the factors that influence BIC levels, implant position and bone density.29Calvo-Guirado JL, Ortiz-Ruiz AJ, Negri B, López-Marí L, Rodríguez-Barba C, Schlottig F. Histological and histomorphometric evaluation of immediate implant placement on a dog model with a new implant surface treatment.
→ Clin Oral Implants Res. 2010 Mar;21(3):308–15. 30Caneva M, Salata LA, de Souza SS, Bressan E, Botticelli D, Lang NP. Hard tissue formation adjacent to implants of various size and configuration immediately placed into extraction sockets: an experimental study in dogs.
→ Clin Oral Implants Res. 2010 Sep;21(9):885–90. 31Cho GC. Evidence-based approach for treatment planning options for the extensively damaged dentition.
→ J Calif Dent Assoc. 2004 Dec;32(12):983–90. 32Sanz M, Cecchinato D, Ferrus J, Pjetursson EB, Lang NP, Lindhe J. A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla.
→ Clin Oral Implants Res. 2010 Jan;21(1):13–21. 33Trisi P, Lazzara R, Rao W, Rebaudi A. Bone-implant contact and bone quality: evaluation of expected and actual bone contact on machined and osseotite implant surfaces.
→ Int J Periodontics Restorative Dent. 2002 Dec;22(6):535–45. 34Trisi P, Marcato C, Todisco M. Bone-to-implant apposition with machined and MTX microtextured implant surfaces in human sinus grafts.
→ Int J Periodontics Restorative Dent. 2003 Oct;23(5):427–37. Experimental and clinical studies have demonstrated that implants designed with a shorter, smooth coronal collar caused no additional bone loss and might help reduce the risk of an exposed metal implant margin in areas of esthetic concern.35Alomrani AN, Hermann JS, Jones AA, Buser D, Schoolfield J, Cochran DL. The effect of a machined collar on coronal hard tissue around titanium implants: a radiographic study in the canine mandible.
→ Int J Oral Maxillofac Implants. 2005 Sep-Oct;20(5):677–86. 36Hänggi MP, Hänggi DC, Schoolfield JD, Meyer J, Cochran DL, Hermann, JS. Crestal bone changes around titanium implants. Part I: a retrospective radiographic evaluation in humans comparing two non-submerged implant designs with different machined collar lengths.
→ J Periodontol. 2005 May;76(5):791–802.
The anatomy and surface treatment of the neck of the implant, together with the type of connection between the implant and the prosthetic components, have been considered as with regard to reducing crestal bone loss.37Fickl S, Zuhr O, Stein JM, Hürzeler MB. Peri-implant bone level around implants with platform-switched abutments.
→ Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):577–81. Based on the data revised, it is hypothesized that the vertical positioning of the implant platform in relation to the crestal bone may influence the location of the first BIC. As a consequence, the biological width may be established in a more coronal position. Therefore, the objective of this study was to compare the BIC of implants with smooth necks and no microthreads, which represent a rough surface, placed at crestal and subcrestal levels in healed bone and immediately post-extraction in dogs.
Materials and methods
Six American Foxhound dogs of approximately 1 year of age were used in this study. The Ethics Committee for Animal Research at the University of Murcia, Murcia, Spain, approved the study protocol, which followed guidelines established by the European Union Council Directive of February 2013 (R.D.53/2013). Clinical examination determined that all of the animals were in good general health; moreover, all of the animals presented with intact maxillae, without any general occlusal trauma or oral viral or fungal lesions.
The choice of this kind of dog was due to these being the animals that we have in our animal facilities approved for research. The animals were quarantined for the application of rabies vaccines and vitamins. The dogs were kept in kennel cages before and after surgery, received appropriate veterinary care, and were allowed free access to water and standard laboratory nutritional support throughout the trial period. After surgery, the animals received antibiotics (enrofloxacin, 5 mg/kg, bid) and analgesics (meloxicam, 0.2 mg/kg, tid) via the systemic route.
Surgical procedure
The animals were pre-anesthetized with acepromazine (0.12%, 0.25 mg/kg), buprenorphine (0.01 mg/kg) and medetomidine (35 μg/kg). The mixture was injected intramuscularly into the femoral quadriceps. The animals were then taken to the operating theater, where, at the earliest opportunity, an intravenous catheter was inserted (diameter of 22 or 20 G) into the cephalic vein, and propofol was infused at a slow, constant infusion rate of 0.4 mg/kg/min. Conventional dental infiltration anesthesia (articaine, 40 mg; 1% epinephrine) was administered at the surgical sites. These procedures were carried out under the supervision of a veterinary surgeon. Mandibular premolar and molar extractions (P2, P3, P4 and M1) were performed bilaterally. The teeth were sectioned in the buccolingual direction at the bifurcation using a tungsten carbide bur so that the roots could be extracted individually without damaging the remaining bony walls with a contra-angle handpiece (W&H, Bürmoos, Austria). The surgical device used for odontosection was the Implantmed (W&H).
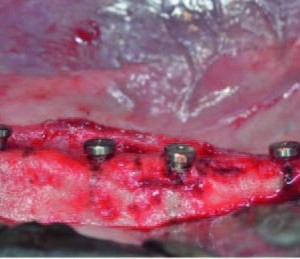
Crestal incisions were performed bilaterally in the premolar–molar region of the mandible. Full-thickness mucoperiosteal flaps were elevated, and recipient sites in the molar regions on both sides of the mandible were prepared for the present experiment, while the other regions were used for different experimental purposes, the results of which are reported elsewhere. The healed bone was prepared to place cylindrical, self-tapping implants with BIONER’s Top DM expansive core (BIONER Sistemas Implantológicos, Sant Just Desvern, Spain; 8.0 mm in length, 3.5 mm in diameter). A total of 48 implants were installed, 8 in each dog in healed and post-extraction bone (Figs. 1a–d). The implants had a bioetch surface characterized by a moderate, acid-etched without sandblasting, roughnessalong the implant body.
-
- Fig. 1a

-

- Fig. 1b
-
- Fig. 1c

-
- Fig. 1d
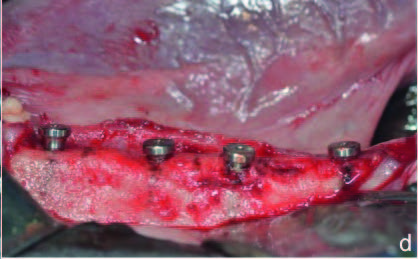
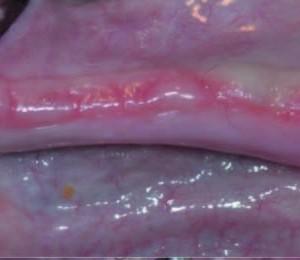
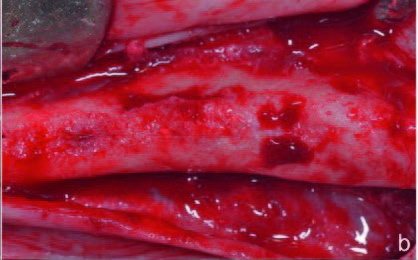
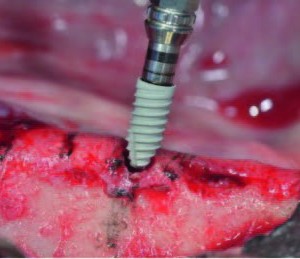
Figs. 1a–d
(a) Healed bone.
(b) Separate flap where bone repair was observed after 8 weeks of healing.
(c) Top DM implant.
(d) Implants with healing screws placed at crestal and subcrestal levels.
The crestal or subcrestal positioning of the implants and the type of placement (healed bone or immediately post-extraction) were determined randomly by the randomization plan generator at www.randomization.com. The subcrestal position was 2 mm below the buccal and lingual bone crests. After insertion of the implants, the healing abutments were connected to evaluate the periimplant soft tissue. The flaps were sutured with 4-0 silk (Lorca Marín, Lorca, Spain).
After the surgical procedures, the animals received antibiotic treatment (amoxicillin, 500 mg, bid) and analgesics (ibuprofen, 600 mg, tid) systemically. In addition, the dogs were fed a soft diet for 7 days and plaque control was maintained through the application of Sea4 (Blue Sea Laboratories, Alicante, Spain). The wounds were inspected daily for postoperative clinical complications. Two weeks after surgery, the sutures were removed.
Histological and histomorphometric analysis
Three animals were sacrificed at 8 weeks and the other 3 animals were sacrificed at 12 weeks through an overdose of Pentothal Natrium (Laboratorios Abbot, Madrid, Spain) and perfused through the carotid arteries with a fixative containing 5% glutaraldehyde and 5% formaldehyde. The specimens were washed in saline and fixed in 10% buffered formalin. The specimens were processed to obtain thin sections of soil with the Precise 1 automated system (Assing, Rome, Italy). The specimens were dehydrated in ascending series with alcohol and embedded in a glycol methacrylate resin (Technovit 7200 VLC, Kulzer, Wehrheim, Germany). After polymerization, the specimens were sectioned along their longitudinal axes with a high-precision diamond disk, at about 150–30 μm. A total of 2 slides were obtained for each implant. The slides were stained with toluidine blue and observed under a normal transmitted light microscope and a polarized light microscope (Leitz, Wetzlar, Germany).
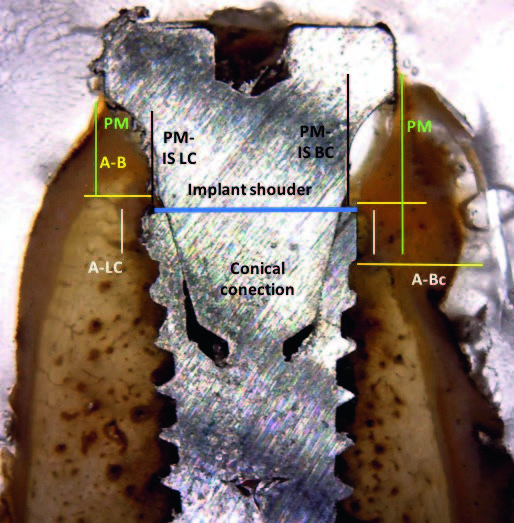
The histological preparation evaluated the distance from the top of the implant collar to the first contact with buccal and lingual bone (A-Bc and A-Lc), as well as the heights of the buccal and lingual bone ridges with respect to the neck of the implant (Fig. 2). Resorption of the buccal bone wall compared with resorption of the lingual bone wall was expressed as a linear measure. The buccal and lingual bone plates were measured from the implant shoulder to the first BIC and to the top of the bony crest. The percentage of BIC of native bone was also measured along the perimeter of the implant between the coronal end of osseointegration at the buccal and lingual aspects. The apical portion of each implant was excluded from the measurement because some implants were inserted into the dental nerve. The total amount of bone in contact with the implant was calculated as the sum of native bone and newly formed bone (BIC%). Histomorphometry of BIC percentages was performed using a light microscope (Laborlux S, Leitz) connected to a high-resolution video camera (3CCD, JVC KY-F55B, Yokohama, Japan) and connected to a monitor and PC (Intel Pentium III 1200 MMX, Intel, Santa Clara, Calif., U.S.). This optical system was associated with a scanning pad (Matrix Vision, Oppenweiler, Germany) and a software package for histometry with image capture capabilities (Image-Pro Plus 4.5, Media Cybernetics, Immagini & Computer, Milan, Italy). The total amount of bone in contact with the implants was calculated as the sum of native bone and newly formed bone.”
-
- Fig. 2
Fig. 2
The histological preparation evaluated the distance from the top of the implant collar to the first contact with buccal and lingual bone (A-Bc and A-Lc), as well as the heights of the buccal and lingual bone ridges with respect to the neck of the implant.
Statistical analysis
Mean values and standard deviations were calculated using a BIC descriptive test and bone resorption measurements. The Wilcoxon test was applied to the comparison of mean averages and to quantify relationships between differences. Brunner and Langer nonparametric tests were applied to the mean values for crestal and subcrestal implants and for periimplant mucosa measurement. All histomorphometric parameters were analyzed using descriptive methods (IBM SPSS Statistics for Windows version 19.0, IBM Corp., Armonk, N.Y., U.S.). For all of the tests performed, the significance level chosen was 5% (p < 0.05).
Results
When buccal, lingual, mesial and distal dimensions of the entrance to the fresh extraction sockets were measured before implant placement, mean alveolar ridge measurements of the extraction sockets were 5.3 ± 0.6 mm (2P2), 5.7 ± 0.2 mm (3P3), 5.9 ± 0.2 mm (4P4) and 8.9 ± 0.5 mm (1M1).
Histological evaluation
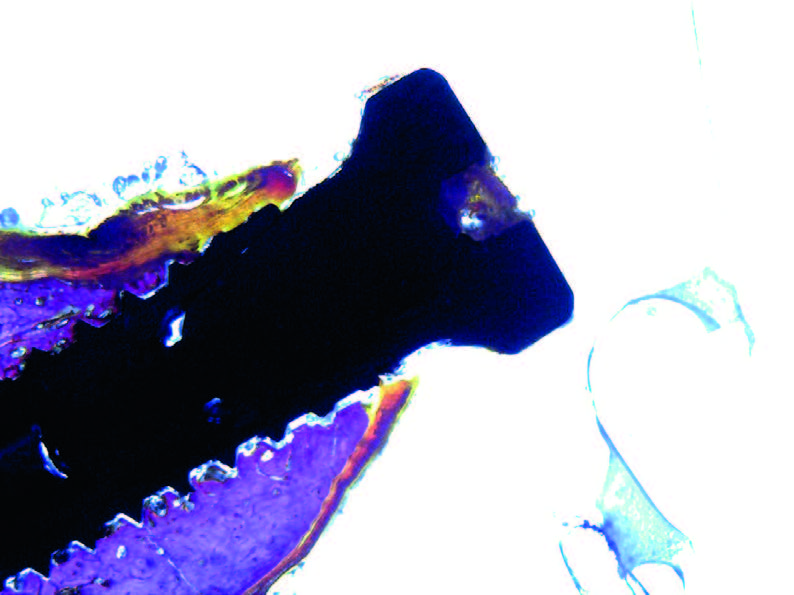
Healing was uneventful for all of the animals and no implants were lost. Operative surgical sites healed without incident. All of the implants were available for histological analysis. The gaps between all of the implants and the bony walls disappeared as a result of bone filling and resorption of the alveolar crest in both groups (control and test). Direct contact between the living bone with slight vestibular resorption was observed, with stable soft tissue at 8 weeks for the crestal position and with a thicker gingiva in implants placed at the subcrestal level. Bone remodeling in the region of the marginal defect was accompanied by marked decreases in the dimensions of the buccal and lingual bone walls at 12 weeks at crestal and subcrestal levels (Figs. 3 & 4). For all of the implants, the keratinized oral epithelium was continuous with the junctional epithelium along the implants and the healing screws. Underlying connective tissue was observed with a dense network of collagen fibers around the implants placed in subcrestal healed bone, improving the quality of the periimplant gingiva (Fig. 5) compared with crestally placed implants.
After evaluation of all of the measurements, the distance from the top of the implant neck to the first BICat the buccal aspect (A-Bc) showed statistically significant differences at 12 weeks in the test group compared with the control group (Figs. 6 & 7). In addition, the distance from the top of the implant collar to the lingual bone crest (A-Lc) showed significant differences between the crestal group and the subcrestal group after the healing period of 8 weeks. The A-Lc measure (distance between the implant collar top and the first BIC in the lingual aspect) was statistically significant after the healing period of 12 weeks in the subcrestal group.
Total BIC values were higher for implants of the test group at 8 weeks with subcrestal placement and even higher in this group of implants after 12 weeks of healing compared with the crestal placement group (Table 1). The values of the BIC lingual aspect are described in Table 2. These were higher for the subcrestal group, and values increased from 8 to 12 weeks. The direct contact surface between the implant and the bone was larger for the test implants, with no statistically significant differences. Subcrestal placement always showed higher BIC values at 8 and 12 weeks (Figs. 5 & 8).
Table 3 shows that the analysis of the periimplant mucosa and buccal implant shoulder (PM-IS BC) presented higher values for the implants placed crestally at 8 and 12 weeks compared with subcrestal placement, with statistically significantly different values at 12 weeks.
-
- Fig. 3
-

- Fig. 4
-
- Fig. 5
-

- Fig. 6
-

- Fig. 7
-

- Fig. 8
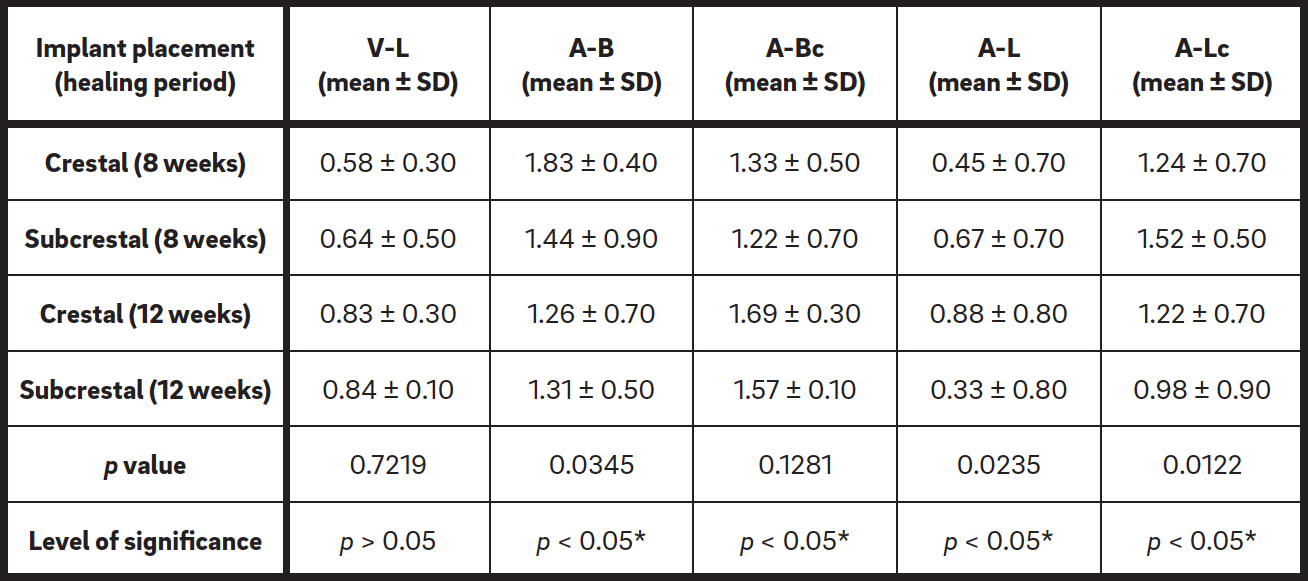
V-L = difference between the buccal bone crest and the lingual bone crest;
SD = standard deviation;
A-B = distance from the top of the implant neck to the buccal bone crest;
A-Bc = distance from the top of the implant collar to the first BIC at the buccal aspect;
A-L = distance between the top of the implant collar and the lingual bone crest;
A-Lc = distance from the top of the implant collar to the first BIC at the lingual aspect;
* indicates statistical significance.

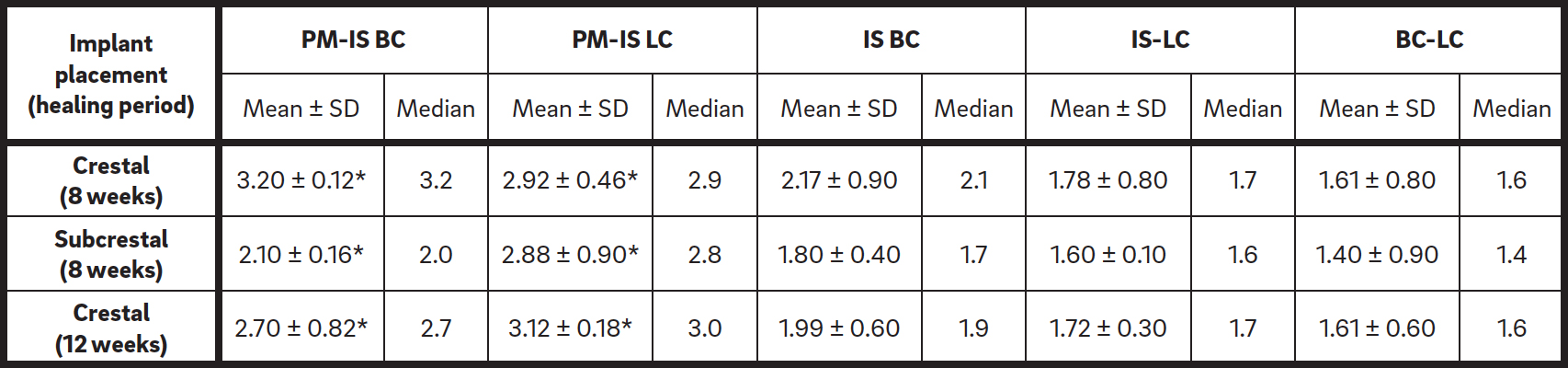
PM-IS BC = distance from the periimplant mucosa to the buccal bone crest;
PM-IS LC = distance from the periimplant mucosa to the lingual bone crest;
IS-BC = distance from the top of the implant shoulder to the first BIC at the buccal aspect;
IS-LC = distance from the top of the implant shoulder to the lingual bone crest;
BL-LC = difference between buccal bone crest and lingual bone crest;
SD = standard deviation; * indicates statistical significance.
Fig. 3
Biopsy at 8 weeks of an implant placed at the crestal level. Slight resorption of the vestibular wall was observed, with stable and thick soft tissue.
Fig. 4
Biopsy at 8 weeks of an implant placed at the subcrestal level. Slight resorption of the vestibular wall with neoformed bone was observed around the implant neck, with stable and thick soft tissue.
Fig. 5
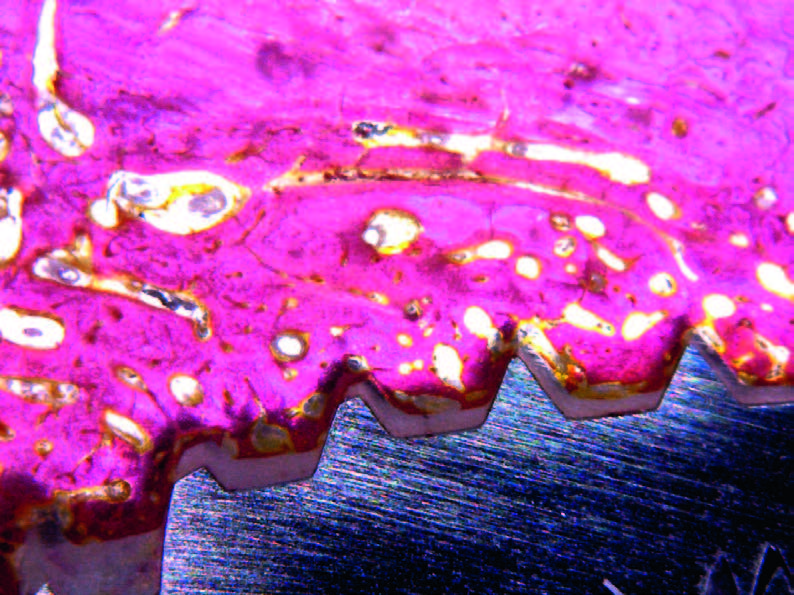
Bone–implant contact at 12 weeks in unloaded bone. The bone was in intimate contact with the BIOETCH surface.
Fig. 6
Biopsy at 12 weeks of an implant placed at the crestal level. Remodeling of the buccal and lingual walls with neoformed bone around the implant neck was observed.
Fig. 7
Biopsy at 12 weeks of an implant placed at the subcrestal level. Remodeling of the vestibular and lingual walls with a large amount of neoformed bone protecting the implant neck was observed.
Fig. 8
Bone–implant contact at 8 weeks in healed bone. The bone was in intimate contact with the BIOETCH surface.
Table. 1
Mean values (mm) ± standard deviation mm for the Brunner and Langer test (nonparametric analysis of repeated measures). Description of the data in healed bone.
Table. 2
Mean values of BIC % ± standard deviation at the different time periods. Description of the data in healed bone.
Table. 3
Brunner and Langer test (nonparametric repeated measures analysis of variance) applied to mean values ± standard deviation and median values (mm) related to implants placed subcrestally. The level of significance was set at p < 0.05.
Discussion
The removal of single teeth followed by immediate placement of an implant results in marked alterations to buccal ridge dimensions (30–43%) and the horizontal (63–80%) and vertical (65–69%) gaps between the implant and bone walls.38Sanz M, Cecchinato D, Ferrus J, Pjetursson EB, Lang NP, Lindhe J. A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla.
→ Clin Oral Implants Res. 2010 Jan;21(1):13–21. The present investigation showed marked alterations after a healing period of 8 weeks that affected both the buccal and lingual bone walls. A-Bc and A-Lc values were lower for implants placed in healed bone at the subcrestal level than for those placed at the crestal level In addition, resorption was more pronounced, which is in agreement with studies previously published by our group.39Calvo-Guirado JL, Ortiz-Ruiz AJ, Negri B, López-Marí L, Rodríguez-Barba C, Schlottig F. Histological and histomorphometric evaluation of immediate implant placement on a dog model with a new implant surface treatment.
→ Clin Oral Implants Res. 2010 Mar;21(3):308–15. The present study revealed a greater depth of crestal bone resorption in the buccal bone than in the lingual crest. This bone dehiscence after implant placement corroborates the previously reported findings.40Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog.
→ J Clin Periodontol. 2005 Feb;32(2):212–8. 41Araújo MG, Sukekava F, Wensström JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog.
→ J Clin Periodontol. 2005 Jun;32(6):645–52. 42Calvo-Guirado JL, Ortiz-Ruiz AJ, Negri B, López-Marí L, Rodríguez-Barba C, Schlottig F. Histological and histomorphometric evaluation of immediate implant placement on a dog model with a new implant surface treatment.
→ Clin Oral Implants Res. 2010 Mar;21(3):308–15. 43Cardaropoli G, Lekholm U, Wennström JL. Tissue alterations at implant-supported single-tooth replacements: a 1-year prospective clinical study.
→ Clin Oral Implants Res. 2006 Apr;17(2):165–71. 44Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering.
→ Ann Periodontol. 2000 Dec;5(1):119–28.
Moreover, the delicate marginal portion of the buccal bone wall frequently contains proportionally larger amounts of bundle bone than the lingual wall does.45Becker BE, Becker W, Ricci A, Geurs N. A prospective clinical trial of endosseous screw-shaped implants placed at the time of tooth extraction without augmentation.
→ J Periodontol. 1998 Aug;69(8):920–6. Bundle bone is a tooth-related tissue that, after tooth loss, will model and eventually disappear.46Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog.
→ J Clin Periodontol. 2005 Feb;32(2):212–8. 47Araújo MG, Sukekava F, Wensström JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog.
→ J Clin Periodontol. 2005 Jun;32(6):645–52.
In the present study, BIC values decreased in the subcrestal group from the healing period of 8 weeks to the 12-week healing period in implants placed in healed bone. This finding corroborates that of Araújo et al.48Araújo MG, Wennström JL, Lindhe J. Modeling of the buccal and lingual bone walls of fresh extraction sites following implant installation.
→ Clin Oral Implants Res. 2006 Dec;17(6):606–14. 49Araújo MG, Sukekava F, Wennström JL, Lindhe J. Tissue modeling following implant placement in fresh extraction sockets.
→ Clin Oral Implants Res. 2006 Dec;17(6):615–24. The authors concluded that the BIC established during the early healing phase after implant insertion was partially lost when the buccal bone wall was resorbed. The gaps between the implant and the walls of the alveoli for immediate post-extraction implants were filled with bone tissue after the 8-week healing period. In the present study, a more coronal BIC was obtained in the test group (subcrestal). The total BIC revealed higher values in the subcrestal group. The higher BIC values of the test group after 8 and 12 weeks of healing suggest that bone regeneration may be more favorable for implants placed subcrestally, which is in agreement with results reported by other authors.50Tran BH, Chen ST, Caiafa A, Davies HMS, Darby IB. Transmucosal healing around peri-implant defects: crestal and subcrestal implant placement in dogs.
→ Clin Oral Implants Res. 2010 Aug;21(8):794–803. Therefore, subcrestal insertion of dental implants may facilitate anterior BIC at the implant neck. It was also observed that a comparatively larger portion of the implant surface was in direct contact with the bone within the defect area after a period of 12-week wound healing for the control and test implants compared with the 8-week healing period This is in accordance with previous articles published by other authors.51Tran BH, Chen ST, Caiafa A, Davies HMS, Darby IB. Transmucosal healing around peri-implant defects: crestal and subcrestal implant placement in dogs.
→ Clin Oral Implants Res. 2010 Aug;21(8):794–803. They concluded that higher BIC values were found after 3 months of healing, compared with results after 1 month of healing.
The present study demonstrated that, regardless of the vertical positioning, subcrestal placement (test group) and crestal placement (control group) showed similar outcomes and bone resorption patterns, with minor differences between them.
The buccal and lingual BIC values were always higher for the subcrestal implants. Therefore, for these measurements, more favorable results should be obtained with subcrestal placement of implants. Clinically, implants are often inserted at crestal bone level.52Bornstein MM, Lussi A, Schmid B, Belser UC, Buser D. Early loading of nonsubmerged titanium implants with a sandblasted and acid-etched (SLA) surface: 3-year results of a prospective study in partially edentulous patients.
→ Int J Oral Maxillofac Implants. 2003 Sep-Oct;18(5):659–66. 53Bornstein MM, Schmid B, Belser UC, Lussi A, Buser D. Early loading of non-submerged titanium implants with a sandblasted and acid-etched surface. 5-year results of a prospective study in partially edentulous patients.
→ Clin Oral Implants Res. 2005 Dec;16(6):631–8. However, implants can be inserted subcrestally in esthetic areas to minimize the risk of exposure to metals and to allow sufficient space in the vertical dimension to develop an adequate emergence profile.54Caneva M, Salata LA, de Souza SS, Bressan E, Botticelli D, Lang NP. Hard tissue formation adjacent to implants of various size and configuration immediately placed into extraction sockets: an experimental study in dogs.
→ Clin Oral Implants Res. 2010 Sep;21(9):885–90. 55Negri B, Calvo-Guirado JL, Ramírez-Fernández MP, Maté Sánchezde Val J, Guardia J, Muñoz-Guzón F. Peri-implant bone reactions to immediate implants placed at different levels in relation to crestal bone. Part II: a pilot study in dogs.
→ Clin Oral Implants Res. 2012 Feb;23(2):236–44. 56Negri B, Calvo-Guirado JL, Pardo-Zamora G, Ramírez-Fernández MP, Delgado-Ruíz RA, Muñoz-Guzón F. Peri-implant bone reactions to immediate implants placed at different levels in relation to crestal bone. Part I: a pilot study in dogs.
→ Clin Oral Implants Res. 2012 Feb;23(2):228–35. The modeling in the marginal defect region was accompanied by marked attenuation of the dimensions of both the delicate buccal and the wider lingual bone walls. At the buccal aspect, this resulted in some marginal loss of osseointegration. 57Araújo MG, Wennström JL, Lindhe J. Modeling of the buccal and lingual bone walls of fresh extraction sites following implant installation.
→ Clin Oral Implants Res. 2006 Dec;17(6):606–14. 58Araújo MG, Sukekava F, Wennström JL, Lindhe J. Tissue modeling following implant placement in fresh extraction sockets.
→ Clin Oral Implants Res. 2006 Dec;17(6):615–24. In this regard, Caneva et al. suggested that implants should be placed 1 mm subcrestally to reduce or eliminate exposure of the rough portion of the implant above the alveolar ridge.59Caneva M, Salata LA, de Souza SS, Bressan E, Botticelli D, Lang NP. Hard tissue formation adjacent to implants of various size and configuration immediately placed into extraction sockets: an experimental study in dogs.
→ Clin Oral Implants Res. 2010 Sep;21(9):885–90. In addition, subcrestal placement of an implant may facilitate BIC earlier at the implant neck.
Conclusion
Our findings suggest that less resorption can be expected when implants are inserted 2 mm subcrestally for both immediate and deferred implants compared with placement at the crestal level. In addition, higher BIC values were found at 12 weeks of follow-up in the group of implants placed subcrestally in healed bone compared with those placed subcrestally immediately. The design of an implant with a smooth neck without microthreads and with a surface highly receptive to osteoblasts improves osseointegration in the initial stages, which a posteriori increases.
Competing interests
The authors declare that they have no competing interests.
Interview
with José Luis Calvo Guirado
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
surfaces. Large threads in the middle of the implant body could protect the alveolar bone.
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 5, 40, 46. | ↑ | Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. → J Clin Periodontol. 2005 Feb;32(2):212–8. |
| 2, 6, 19, 41, 47. | ↑ | Araújo MG, Sukekava F, Wensström JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. → J Clin Periodontol. 2005 Jun;32(6):645–52. |
| 3. | ↑ | Botticelli D, Berglundh T, Lindhe J. The influence of a biomaterial on the closure of a marginal hard tissue defect adjacent to implants. An experimental study in the dog. → Clin Oral Implants Res. 2004 Jun;15(3):285–92. |
| 4, 22. | ↑ | Botticelli D, Berglundh T, Lindhe J. Resolution of bone defects of varying dimension and configuration in the marginal portion of the peri-implant bone. An experimental study in the dog. → J Clin Periodontol. 2004 Apr;31(4):309–17. |
| 7. | ↑ | Nemcovsky CE, Artzi Z, Moses O, Gelernter I. Healing of marginal defects at implants placed in fresh extraction sockets or after 4-6 weeks of healing. A comparative study. → Clin Oral Implants Res. 2002 Aug;13(4):410–9. |
| 8. | ↑ | Paolantonio M, Dolci M, Scarano A, d’Archivio D, di Placido G, Tumini V, Piattelli A. Immediate implantation in fresh extraction sockets. A controlled clinical and histological study in man. → J Periodontol. 2001 Nov;72(11):1560–71. |
| 9, 45. | ↑ | Becker BE, Becker W, Ricci A, Geurs N. A prospective clinical trial of endosseous screw-shaped implants placed at the time of tooth extraction without augmentation. → J Periodontol. 1998 Aug;69(8):920–6. |
| 10. | ↑ | Grunder U, Polizzi G, Goene R, Hatano N, Henry P, Jackson WJ, Kawamura K, Köhler S, Renouard F, Rosenberg R, Triplett G, Werbitt M, Lithner B. A 3-year prospective multicenter follow-up report on the immediate and delayed-immediate placement of implants. → Int J Oral Maxillofac Implants. 1999 Mar-Apr;14(2):210–6. |
| 11. | ↑ | Lazzara RJ. Immediate implant placement into extraction sites: surgical and restorative advantages. → Int J Periodontics Restorative Dent. 1989;9(5):332–43. |
| 12. | ↑ | Schwartz-Arad D, Chaushu G. Placement of implants into fresh extraction sites: 4 to 7 years retrospective evaluation of 95 immediate implants. → J Periodontol. 1997 Nov;68(11):1110–6. |
| 13. | ↑ | Schwartz-Arad D, Chaushu G. The ways and wherefores of immediate placement of implants into fresh extraction sites: a literature review. → J Periodontol. 1997 Oct;68(10):915–23. |
| 14. | ↑ | Terheyden H, Stadlinger B, Sanz M, Garbe AI, Meyle J. Inflammatory reaction – communication of cells. → Clin Oral Implants Res. 2014 Apr;25(4):399–407. |
| 15. | ↑ | Iezzi G, Degidi M, Shibli JA, Vantaggiato G, Piattelli A, Perrotti V. Bone response to dental implants after a 3- to 10-year loading period: a histologic and histomorphometric report of four cases. → Int J Periodontics Restorative Dent. 2013 Nov-Dec;33(6):755–61. |
| 16. | ↑ | Schwarz F, Alcoforado G, Nelson K, Schaer A, Taylor T, Beuer F, Strietzel, FP. Impact of implant-abutment connection, positioning of the machined collar/microgap, and platform switching on crestal bone level changes. Camlog Foundation consensus report. → Clin Oral Implants Res. 2014 Nov;25(11):1301–3. |
| 17. | ↑ | Hermann JS, Buser D, Schenk RK, Higginbottom FL, Cochran DL. Biologic width around titanium implants. A physiologically formed and stable dimension over time. → Clin Oral Implants Res. 2000 Feb;11(1):1–11. |
| 18. | ↑ | Hermann JS, Buser D, Schenk RK, Schoolfield JD, Cochran DL. Biologic width around one- and two-piece titanium implants. → Clin Oral Implants Res. 2001 Dec;12(6):559–71. |
| 20. | ↑ | Barros RR, Novaes AB Jr, Papapelxiou V. Buccal bone remodeling after immediate implantation with a flap or flapless approach. A pilot study in dogs. → Titanium. 2009;1:45–51. |
| 21. | ↑ | Botticelli D, Berglundh T, Lindhe J. The influence of a biomaterial on the closure of a marginal hard tissue defect adjacent to implants. An experimental study in the dog. → Clin Oral Implants Res. 2004 Jun;15(3):285–92. |
| 23. | ↑ | Buser D, Martin WC, Belser UC. Surgical considerations for single-tooth replacements in the esthetic zone: standard procedures in sites without bone deficiencies. → In: Belser UC, Martin W, Jung R, Hammerle CH, Schmid B, Morton D, Buser D, editors. ITI treatment guide. Vol. 1, Implant therapy in the esthetic zone. Single-tooth replacements. Berlin: Quintessence. 2007. p. 26–37. |
| 24. | ↑ | Hämmerle CH, Brägger U, Bürgin W, Lang NP. The effect of subcrestal placement of the polished surface of ITI implants on marginal soft and hard tissues. → Clin Oral Implants Res. 1996 Jun;7(2):111–9. |
| 25. | ↑ | Welander M, Abrahamsson I, Berglundh T. Placement of two-part implants in sites with different buccal and lingual bone heights. → J Periodontol. 2009 Feb;80(2):324–9. |
| 26, 37. | ↑ | Fickl S, Zuhr O, Stein JM, Hürzeler MB. Peri-implant bone level around implants with platform-switched abutments. → Int J Oral Maxillofac Implants. 2010 May-Jun;25(3):577–81. |
| 27, 55. | ↑ | Negri B, Calvo-Guirado JL, Ramírez-Fernández MP, Maté Sánchezde Val J, Guardia J, Muñoz-Guzón F. Peri-implant bone reactions to immediate implants placed at different levels in relation to crestal bone. Part II: a pilot study in dogs. → Clin Oral Implants Res. 2012 Feb;23(2):236–44. |
| 28, 56. | ↑ | Negri B, Calvo-Guirado JL, Pardo-Zamora G, Ramírez-Fernández MP, Delgado-Ruíz RA, Muñoz-Guzón F. Peri-implant bone reactions to immediate implants placed at different levels in relation to crestal bone. Part I: a pilot study in dogs. → Clin Oral Implants Res. 2012 Feb;23(2):228–35. |
| 29, 39, 42. | ↑ | Calvo-Guirado JL, Ortiz-Ruiz AJ, Negri B, López-Marí L, Rodríguez-Barba C, Schlottig F. Histological and histomorphometric evaluation of immediate implant placement on a dog model with a new implant surface treatment. → Clin Oral Implants Res. 2010 Mar;21(3):308–15. |
| 30, 54, 59. | ↑ | Caneva M, Salata LA, de Souza SS, Bressan E, Botticelli D, Lang NP. Hard tissue formation adjacent to implants of various size and configuration immediately placed into extraction sockets: an experimental study in dogs. → Clin Oral Implants Res. 2010 Sep;21(9):885–90. |
| 31. | ↑ | Cho GC. Evidence-based approach for treatment planning options for the extensively damaged dentition. → J Calif Dent Assoc. 2004 Dec;32(12):983–90. |
| 32, 38. | ↑ | Sanz M, Cecchinato D, Ferrus J, Pjetursson EB, Lang NP, Lindhe J. A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla. → Clin Oral Implants Res. 2010 Jan;21(1):13–21. |
| 33. | ↑ | Trisi P, Lazzara R, Rao W, Rebaudi A. Bone-implant contact and bone quality: evaluation of expected and actual bone contact on machined and osseotite implant surfaces. → Int J Periodontics Restorative Dent. 2002 Dec;22(6):535–45. |
| 34. | ↑ | Trisi P, Marcato C, Todisco M. Bone-to-implant apposition with machined and MTX microtextured implant surfaces in human sinus grafts. → Int J Periodontics Restorative Dent. 2003 Oct;23(5):427–37. |
| 35. | ↑ | Alomrani AN, Hermann JS, Jones AA, Buser D, Schoolfield J, Cochran DL. The effect of a machined collar on coronal hard tissue around titanium implants: a radiographic study in the canine mandible. → Int J Oral Maxillofac Implants. 2005 Sep-Oct;20(5):677–86. |
| 36. | ↑ | Hänggi MP, Hänggi DC, Schoolfield JD, Meyer J, Cochran DL, Hermann, JS. Crestal bone changes around titanium implants. Part I: a retrospective radiographic evaluation in humans comparing two non-submerged implant designs with different machined collar lengths. → J Periodontol. 2005 May;76(5):791–802. |
| 43. | ↑ | Cardaropoli G, Lekholm U, Wennström JL. Tissue alterations at implant-supported single-tooth replacements: a 1-year prospective clinical study. → Clin Oral Implants Res. 2006 Apr;17(2):165–71. |
| 44. | ↑ | Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. → Ann Periodontol. 2000 Dec;5(1):119–28. |
| 48, 57. | ↑ | Araújo MG, Wennström JL, Lindhe J. Modeling of the buccal and lingual bone walls of fresh extraction sites following implant installation. → Clin Oral Implants Res. 2006 Dec;17(6):606–14. |
| 49. | ↑ | Araújo MG, Sukekava F, Wennström JL, Lindhe J. Tissue modeling following implant placement in fresh extraction sockets. → Clin Oral Implants Res. 2006 Dec;17(6):615–24. |
| 50, 51. | ↑ | Tran BH, Chen ST, Caiafa A, Davies HMS, Darby IB. Transmucosal healing around peri-implant defects: crestal and subcrestal implant placement in dogs. → Clin Oral Implants Res. 2010 Aug;21(8):794–803. |
| 52. | ↑ | Bornstein MM, Lussi A, Schmid B, Belser UC, Buser D. Early loading of nonsubmerged titanium implants with a sandblasted and acid-etched (SLA) surface: 3-year results of a prospective study in partially edentulous patients. → Int J Oral Maxillofac Implants. 2003 Sep-Oct;18(5):659–66. |
| 53. | ↑ | Bornstein MM, Schmid B, Belser UC, Lussi A, Buser D. Early loading of non-submerged titanium implants with a sandblasted and acid-etched surface. 5-year results of a prospective study in partially edentulous patients. → Clin Oral Implants Res. 2005 Dec;16(6):631–8. |
| 58. | ↑ | Araújo MG, Sukekava F, Wennström JL, Lindhe J. Tissue modeling following implant placement in fresh extraction sockets. → Clin Oral Implants Res. 2006 Dec;17(6):615–24. |





Leave a Reply
Be the First to Comment!