Periimplant soft-tissue management in patients with a fibula free flap reconstruction: Case series and description of a new technique
January 6, 2017 / Categories: Digital Dentistry, Implant Dentistry

Meloni, Silvio Mario

Tallarico, Mario

Canullo, Luigi
De Riu, Giacomo

Massarelli, Olindo
The aim of the present pilot case series study was to present a new technique for managing the periimplant soft tissue before implant placement, the soft-tissue template technique.
Introduction
Bone continuity defects after oncological jaw resection or for other reasons may result in a series of problems, such as facial contour disfigurement, large oronasal and oroantral communications, saliva retention, and impaired speech, swallowing and mastication.
Fibula and iliac crest free flaps have demonstrated high reliability for reconstruction of mandibular and maxillary large bone defects. They are used as both osseomuscular and osseomyocutaneous flaps and allow the simultaneous reconstruction of bone continuity and both intraoral (cheek mucosa, palate, floor of the mouth, etc.) and cutaneous (chin, cheek, etc.) soft-tissue deficiencies. 1Hidalgo DA. Titanium miniplate fixation in free flap mandible reconstruction.
→ Ann Plast Surg. 1989 Dec;23(6):498–507.
2Riaz N, Warraich R. Reconstruction of mandible by free fibular flap.
→ J Coll Physicians Surg Pak. 2010 Nov;20(11):723–7. Additionally, patients with oral cavity defects often present with loss of teeth and alveolar and basal jawbone, which can lead to significant impairment of mastication. With this microvascular reconstructive option, dental prosthetic rehabilitation is possible even if the prosthesis-based rehabilitation remains a challenge.3Hayter JP, Cawood JI. Oral rehabilitationwith endosteal implants and free flaps.
→ Int J Oral Maxillofac Surg. 1996 Feb;25(1):3–12.
4Chiapasco M, Biglioli F, Autelitano L, Romeo E, Brusati R. Clinical outcome of dental implants placed in fibula-free flaps used for the reconstruction of maxillo-mandibular defects following ablation for tumors or osteoradionecrosis.
→ Clin Oral Implants Res. 2006 Apr;17(2):220–8.
Implant-based dental restorations in patients reconstructed with fibula flaps have been shown to offer many benefits, such as sufficient stabilization of the prosthesis, even in patients with marked irregularities of the hard and soft-tissue anatomy, and they can compensate for small local soft-tissue deficiencies, contributing to an improved aesthetic result (i.e., by supporting the lip profile). A recurring problem during implantprosthesis rehabilitation after reconstruction with vascularized free flaps is the hyperplastic granulomatous reactive tissue that can grow around the implant abutments of the prosthesis.
The reconstructed soft tissue lacks the physiological properties and function of native mucosa.
Normal attached gingiva and alveolar mucosa differ from soft tissue reconstructed with skin and muscle.
After implant-prosthesis restoration, excessive soft-tissue bulk, movement, chronic inflammation and hypertrophy are readily observed around implants and risk compromising the long-term implant success. This phenomenon, which has been described by others,5Jaquiéry C, Rohner D, Kunz C, Bucher P, Peters F, Schenk RK, Hammer B. Reconstruction of maxillary and mandibular defects using prefabricated microvascular fibular grafts and osseointegrated dental implants—a prospective study.
→ Clin Oral Implants Res. 2004 Oct;15(5):598–606. is an unresolved problem. Various clinical reports suggest different approaches, with contradictory results.6 Lizio G, Corinaldesi G, Pieri F, Marchetti C. Problems with dental implants that were placed on vertically distracted fibular free flaps after resection: a report of six cases.
→ Br J Oral Maxillofac Surg. 2009 Sep;47(6):455–60.
Some have harvested keratinized mucosa from the hard palate and grafted it around the implants after removing the skin.7Meloni SM, De Riu G, Pisano M, Massarelli O, Tullio A. Computer assisted dental rehabilitation in free flaps reconstructed jaws: one year follow-up of a prospective clinical study.
→ Br J Oral Maxillofac Surg. 2012 Dec;50(8):726–31. Others prefer skin grafts associated with remodeling and deepening of the fornix. Both procedures are often associated with soft-tissue remodeling as a result of the prosthesis.8Meloni SM, De Riu G, Pisano M, Massarelli O, Tullio A. Computer assisted dental rehabilitation in free flaps reconstructed jaws: one year follow-up of a prospective clinical study.
→ Br J Oral Maxillofac Surg. 2012 Dec;50(8):726–31.
9De Riu G, Meloni SM, Pisano M, Massarelli O, Tullio A. Computed tomography-guided implant surgery for dental rehabilitation in mandible reconstructed with a fibular free flap: description of the technique.
→ Br J Oral Maxillofac Surg. 2012 Jan;50(1):30–5.
10Meloni SM, Tallarico M, De Riu G, Pisano M, Deledda A, Lolli FM, Massarelli O, Tullio A. Guided implant surgery after free-flap reconstruction: four-year results from a prospective clinical trial.
→ J Craniomaxillofac Surg. 2015 Oct;43(8):1348–55.
The aim of the present pilot case series study was to present a new technique for managing the periimplant soft tissue before implant placement, the soft-tissue template technique.
Materials and methods
This study was designed as a pilot case series study aimed at evaluating a new technique for periimplant soft-tissue management (soft-tissue template technique) in patients reconstructed with fibula free flaps after mandibular or maxillary resection for oncological reasons. Patients were selected and consecutively treated at the Maxillofacial Surgery Unit, University Hospital of Sassari, Sassari, Italy. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki of 1964 for biomedical research involving human subjects, as amended in 2008. The patients were duly informed about the nature of the study. Written informed consent to surgical treatment was obtained from each patient.
Patients were not admitted to the study if any of the following exclusion criteria were present: general contraindications to implant surgery; subjected to irradiation in the head and neck area less than one year before implantation; untreated periodontitis; signs or symptoms of cancer recurrence; poor oral hygiene and motivation; uncontrolled diabetes; alcohol abuse; psychiatric problems or unrealistic expectations; active infection or severe inflammation in the area intended for implant placement; and inability to attend the follow-up visits.
Clinical procedures and description of the technique
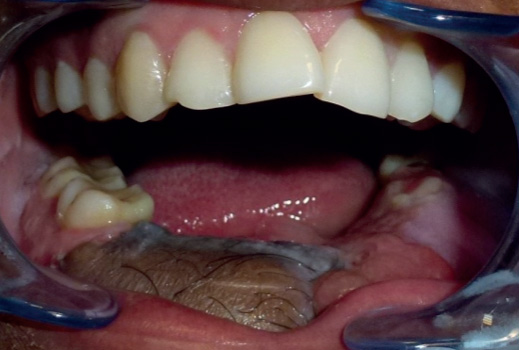
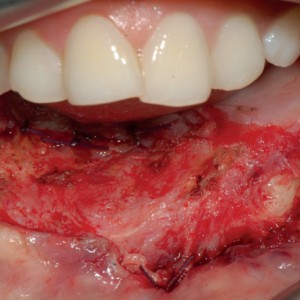
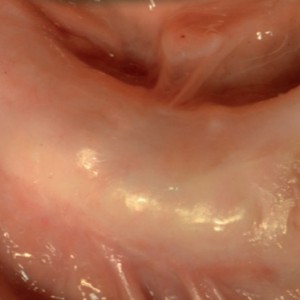
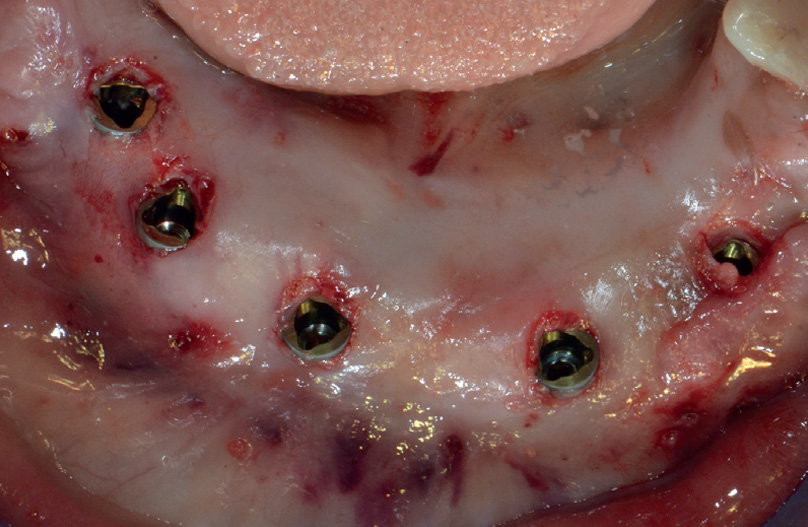
At least six months after reconstruction with a fibula free flap (Fig. 1), all crestal soft tissue, including skin and muscle, was removed, leaving only periosteum attached to the reconstructed alveolar crest (Fig. 2). Immediately after removing the soft tissue, an impression was taken of the crest and residual teeth using a silicone material to customize an acrylic soft-tissue template. The template was shaped to cover the entire crest and have a large vestibular flange used to deepen the fornix. A small space was left between the crest and acrylic template. The soft-tissue template was delivered 24 h after surgical soft-tissue removal and the patient was asked to apply corticosteroid cream under the template b.i.d. for one month (Fig. 3). Subsequently, the new tissue appeared more similar to the gingiva, with reduced thickness and greater attachment to the underlying bone (Figs. 4–6). One month later, implants were inserted with a flapless technique using a computer-guided implant template. Three to six months later, a definitive screw-retained implant supported bridge was delivered.
-

- Fig. 1
-
- Fig. 2

-

- Fig. 3

-
- Fig. 4

-

- Fig. 5
-

- Fig. 6

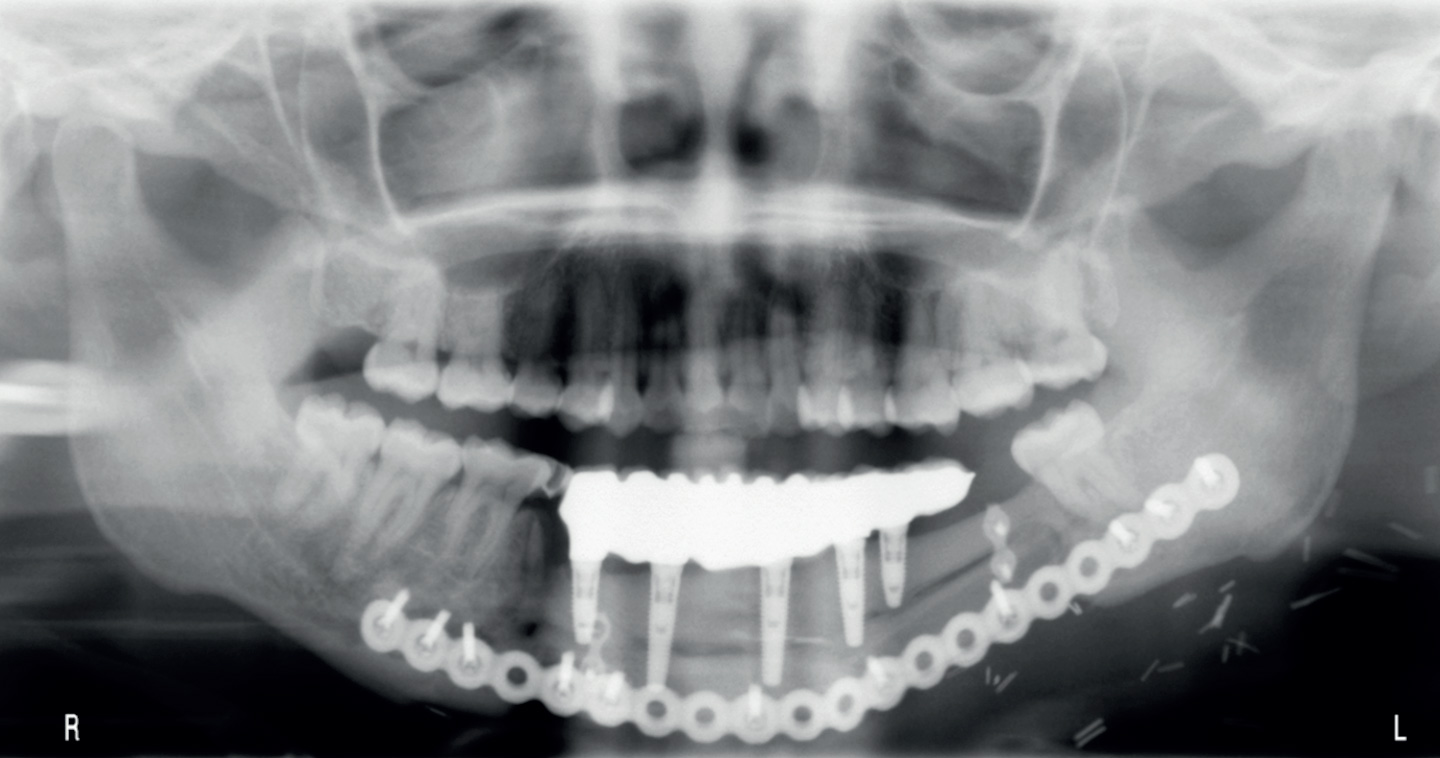
Fig. 1
Reconstructed soft tissue six months after surgery.
Fig. 2
Clinical view fibula free flap after soft-tissue removal.
Fig. 3
A patient wearing the soft-tissue template.
Fig. 4
Reconstructed soft tissue one month after treatment.
Fig. 5
Occlusal view after implant placement.
Fig. 6
Final prosthesis five years after loading.
Fig.7
Panoramic radiograph five years after loading.
Outcome measures were:
Implant failure: Implants that had to be removed at implant insertion owing to lack of stability, implant mobility, removal of stable implants dictated by prozgressive marginal bone loss or infection, and any technical complications (e.g., implant fracture), rendering the implant unusable.The stability of individual implants was assessed at delivery of the definitive prosthesis by tightening the abutment screw at a torque of 20 N cm and 12 months after definitive prosthesis delivery.
Complications: Any biological (pain, swelling, suppuration, etc.) and/or technical complication (fracture of the framework and/or the veneering material, screw loosening, etc.) was considered.
Periimplant mucosal response: Probing pocket depth (PPD) and bleeding on probing (BOP) were measured by a blinded operator with a periodontal probe (PCP-UNC 15, Hu-Friedy, Chicago, Ill., U.S.) 12 months after definitive prosthesis delivery. Three vestibular and three lingual values were collected for each implant and averaged at patient level.An independent hygienist performed all of the periodontal measurements.
Results
Six patients (four males and two females) with a mean age of 48.4 years were considered eligible and treated. A total of 32 implants (NobelReplace Tapered Groovy, Nobel Biocare, Göteborg, Sweden), ranging from 8.0 mm to 16.0 mm in length and from 3.5 mm to 5.0 mm in width, were placed. No dropout occurred during the entire follow-up period. No implant failed and the overall implant survival rate was 100% one year after definitive prosthesis delivery. All of the patients presented with healthy soft tissue, stable PPD and good BOP values at the one-year follow-up.
The mean PPD and BOP values were 3.6 ± 0.6 mm and 9 ± 4.8%, respectively.
Discussion
Fibula and iliac crest osseomyocutaneous free flaps have been demonstrated to be very reliable for the reconstruction of large composite facial defects after resection of tumors, osteoradionecrosis or gunshot trauma. Moreover, implantsupported prosthetic rehabilitation is reliable with this microvascular reconstructive option because of sufficient volume and good bone quality.11Chiapasco M, Biglioli F, Autelitano L, Romeo E, Brusati R. Clinical outcome of dental implants placed in fibula-free flaps used for the reconstruction of maxillo-mandibular defects following ablation for tumors or osteoradionecrosis.
→ Clin Oral Implants Res. 2006 Apr;17(2):220–8. 12Meloni SM, Tallarico M, De Riu G, Pisano M, Deledda A, Lolli FM, Massarelli O, Tullio A. Guided implant surgery after free-flap reconstruction: four-year results from a prospective clinical trial.
→ J Craniomaxillofac Surg. 2015 Oct;43(8):1348–55. Nevertheless, prosthesis-based implant treatment still represents a major challenge in these difficult cases. The surgical procedure for implant placement can be more difficult owing to limited opening of the scar-contracted oral cavity or the presence of large volumes of soft tissue with little information on the profile of the underlying bone, which is necessary for a valid surgical guide. Moreover, the need to limit the exposure of frequently irradiated bone or scarred fields reduces surgical precision. Furthermore, scars and the thickness of the soft tissue can interfere with the prosthetic procedures, such as taking fixture impressions, and may lead to imprecise results.
A detailed soft-tissue analysis of these patients is essential. It is clear that normal attached gingiva and alveolar mucosa differ from soft tissue reconstructed with skin and muscle. A frequent complication arising from the reconstruction of intraoral soft tissue with skin is the hyperplastic/inflammatory response of the skin and subcutaneous tissue around implant abutments and the formation of a granulomatous tissue, which may cause pain and bleeding during brushing. This phenomenon, Although no specific data are available concerning this phenomenon, which has already been described by others,13Jaquiéry C, Rohner D, Kunz C, Bucher P, Peters F, Schenk RK, Hammer B. Reconstruction of maxillary and mandibular defects using prefabricated microvascular fibular grafts and osseointegrated dental implants—a prospective study.
→ Clin Oral Implants Res. 2004 Oct;15(5):598–606. it is possible to speculate that the reconstructed skin is not a suitable tissue around implants and may react negatively in the oral environment. In our opinion, many of the techniques described for managing the transplanted tissue, such palatal epithelial connective tissue grafts or free skin grafts, present some limitations owing to the difficulty in obtaining a real engraftement. A unique solution to this problem does not exist and therefore it requires an individualized approach. The approach described in this article appears to be useful especially because it does not require grafting and it appears to radically reduce the thickness of transplanted soft tissue. However, long-term prospective clinical trials eventually supported by histological data are needed to confirm these clinical findings.
Conclusion
Within the limitations of the study, this technique appears to minimize the donor site morbidity that results from harvesting tissue (skin or gingiva) from elsewhere. In addition, after implant placement and prosthesis loading, the reconstructed tissue appeared stable, fixed around the abutment and implant neck, and clinically healthy. Further clinical trials are needed to validate this approach.
Competing interests
The authors declare that they have no competing interests.
Interview
with Silvio Mario Meloni
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Hidalgo DA. Titanium miniplate fixation in free flap mandible reconstruction. → Ann Plast Surg. 1989 Dec;23(6):498–507. |
| 2. | ↑ | Riaz N, Warraich R. Reconstruction of mandible by free fibular flap. → J Coll Physicians Surg Pak. 2010 Nov;20(11):723–7. |
| 3. | ↑ | Hayter JP, Cawood JI. Oral rehabilitationwith endosteal implants and free flaps. → Int J Oral Maxillofac Surg. 1996 Feb;25(1):3–12. |
| 4, 11. | ↑ | Chiapasco M, Biglioli F, Autelitano L, Romeo E, Brusati R. Clinical outcome of dental implants placed in fibula-free flaps used for the reconstruction of maxillo-mandibular defects following ablation for tumors or osteoradionecrosis. → Clin Oral Implants Res. 2006 Apr;17(2):220–8. |
| 5, 13. | ↑ | Jaquiéry C, Rohner D, Kunz C, Bucher P, Peters F, Schenk RK, Hammer B. Reconstruction of maxillary and mandibular defects using prefabricated microvascular fibular grafts and osseointegrated dental implants—a prospective study. → Clin Oral Implants Res. 2004 Oct;15(5):598–606. |
| 6. | ↑ | Lizio G, Corinaldesi G, Pieri F, Marchetti C. Problems with dental implants that were placed on vertically distracted fibular free flaps after resection: a report of six cases. → Br J Oral Maxillofac Surg. 2009 Sep;47(6):455–60. |
| 7. | ↑ | Meloni SM, De Riu G, Pisano M, Massarelli O, Tullio A. Computer assisted dental rehabilitation in free flaps reconstructed jaws: one year follow-up of a prospective clinical study. → Br J Oral Maxillofac Surg. 2012 Dec;50(8):726–31. |
| 8. | ↑ | Meloni SM, De Riu G, Pisano M, Massarelli O, Tullio A. Computer assisted dental rehabilitation in free flaps reconstructed jaws: one year follow-up of a prospective clinical study. → Br J Oral Maxillofac Surg. 2012 Dec;50(8):726–31. |
| 9. | ↑ | De Riu G, Meloni SM, Pisano M, Massarelli O, Tullio A. Computed tomography-guided implant surgery for dental rehabilitation in mandible reconstructed with a fibular free flap: description of the technique. → Br J Oral Maxillofac Surg. 2012 Jan;50(1):30–5. |
| 10. | ↑ | Meloni SM, Tallarico M, De Riu G, Pisano M, Deledda A, Lolli FM, Massarelli O, Tullio A. Guided implant surgery after free-flap reconstruction: four-year results from a prospective clinical trial. → J Craniomaxillofac Surg. 2015 Oct;43(8):1348–55. |
| 12. | ↑ | Meloni SM, Tallarico M, De Riu G, Pisano M, Deledda A, Lolli FM, Massarelli O, Tullio A. Guided implant surgery after free-flap reconstruction: four-year results from a prospective clinical trial. → J Craniomaxillofac Surg. 2015 Oct;43(8):1348–55. |





Leave a Reply
Be the First to Comment!