A minimally invasive technique for transcrestal sinus floor elevation
December 14, 2018 / Categories: Digital Dentistry, Implant Dentistry

Trombelli, Leonardo

Farina, Roberto

Peñarrocha Oltra, David

Franceschetti, Giovanni
Abstract
Background
Transcrestal maxillary sinus floor elevation represents an effective surgical option to vertically enhance the available bone in the edentulous posterior maxilla.
Purpose
The purpose of the present study is to describe a minimally invasive technique for transcrestal sinus floor elevation, the Smart Lift technique, through a paradigmatic clinical case.
Conclusion
The Smart Lift technique is based on specially designed drills and osteotomes used with a stop device that restricts the working action to the residual bone, thus preventing the accidental penetration of instruments into the sinus cavity. Also, the use of a standardized sequence of instruments has been shown to limit the impact of the clinician’s judgement and skill, thus allowing for rapid learning for inexperienced clinicians. The technique is effective to achieve endo-sinusal bone formation with limited post-surgical morbidity.
Introduction
In the posterior maxillary sextants, the insertion of implants of desired length and diameter may be limited by the dimensional alterations of the bone crest that occur after tooth loss,1Pramstraller M, Farina R, Franceschetti G, Pramstraller C, Trombelli L. Ridge dimensions of the edentulous posterior maxilla: a retrospective analysis of a cohort of 127 patients using computerized tomography data. → Clin Oral Implants Res. 2011 Jan;22(1):54–61. Erratum in: Clin Oral Implants Res. 2011 Feb;22(2):235. partly due to the pneumatization of the maxillary sinus.2Farina R, Pramstraller M, Franceschetti G, Pramstraller C, Trombelli L. Alveolar ridge dimensions in maxillary posterior sextants: a retrospective comparative study of dentate and edentulous sites using computerized tomography data. → Clin Oral Implants Res. 2011 Oct;22(10):1138–44. Transcrestal maxillary sinus floor elevation (tSFE) represents an effective surgical option to vertically enhance the available bone in the edentulous posterior maxilla.3Romero-Millán J, Martorell-Calatayud L, Peñarrocha M, García-Mira B. Indirect osteotome maxillary sinus floor elevation: an update. → J Oral Implantol. 2012 Dec;38(6):799–804.,4Pjetursson BE, Lang NP. Sinus floor elevation utilizing the transalveolar approach. → Periodontol 2000. 2014 Oct;66(1):59–71.
Technique description
The Smart Lift technique was developed by the Research Center for the Study of Periodontal and Periimplant Diseases, University of Ferrara, Ferrara, Italy, and the Department of Odontostomatology, Ospedale “Casa Sollievo della Sofferenza,” San Giovanni Rotondo, Italy.5Trombelli L, Minenna P, Franceschetti G, Farina R, Minenna L. Smart-Lift: a new minimally-invasive procedure for sinus floor elevation. → Dental Cadmos. 2008;76:71–83.,6Trombelli L, Minenna P, Franceschetti G, Minenna L, Itro A, Farina R. Minimally invasive technique for transcrestal sinus floor elevation: a case report. → Quintessence Int. 2010 May:41(5):363–9. The technique is characterized by transcrestal access to the sinus cavity by means of specially designed drills and osteotomes. The pristine bone at sites of implant placement is drilled up to the sinus floor with a trephine bur and then used to fracture the sinus floor by hydraulic pressure through osteotomes. In this respect, the procedure represents a modification of the technique proposed by Fugazzotto.7Fugazzotto PA. Immediate implant placement following a modified trephine/ osteotome approach: success rates of 116 implants to 4 years in function. → Int J Oral Maxillofac Implants. 2002 Jan–Feb;17(1):113–20. One of the advantages of the technique lies in the use of all manual and rotating instruments with adjustable stop devices, which are selected in relation to the vertical amount of residual bone at sites where implants have to be placed. These stop devices have a variable length and may be adapted to all manual and rotating instruments. The use of the stop device restricts the working action of burs and osteotomes to the vertical amount of residual bone, thus preventing the accidental penetration of instruments into the sinus cavity. The determination of the working length (i.e., the distance from the bone crest to the sinus floor) where the osteotome and burs have to limit their working action is first diagnosed on 2-D and/or 3-D radiographs, and then verified intra-surgery by means of a specially designed osteotome. The second advantage relates to the standardized sequence of instruments used for the Smart Lift procedure, which has been shown to limit the impact of the clinician’s judgment and skill, thus allowing for rapid learning for inexperienced clinicians.8Franceschetti G, Trombelli L, Minenna L, Franceschetti G, Farina R. Learning curve of a minimally invasive technique for transcrestal sinus floor elevation: a split-group analysis in a prospective case series with multiple clinicians. → Implant Dent. 2015 Oct;24(5):517–26.
The Smart Lift technique shares its clinical indications with the other surgical procedures for tSFE:
- indications for implant-supported prosthetic rehabilitation, based on accurate diagnosis and treatment planning;
- systemic and local conditions that are compatible with implant placement and sinus floor elevation procedures;
- residual bone height (i.e., the distance from the bone crest to the sinus floor) that prevents the insertion of an implant of the desired length and residual bone height of at least 2 mm.
The Smart Lift technique must not be performed whenever systemic and local conditions contraindicate sinus floor elevation.
The Smart Lift technique: Sequence of instruments
According to the prosthetic treatment planning, the locations for implant placement are established, and the residual bone height at such locations is radiographically measured as the distance from the bone crest to the sinus floor (radiographic working length).
All instruments in the surgical set are characterized by laser marks at each millimeter to allow for precise control of the working length. In the conventional sequence (used with a residual bone height of at least 3 mm; Fig. 1), the first drill (locator drill) is used to perforate the cortical bone at the site where the implant is to be placed. A second drill (probe drill), with a diameter of 1.2 mm and cutting only at the top edge, is used to define the position and orientation of the implant. In order to minimize the risk of sinus floor perforation, this bur is used with an adjustable stop device that is set at least 1 mm shorter than the radiographic working length. The probe osteotome (∅: 1.2 mm) is carefully inserted into the site prepared with the probe drill and gently forced in an apical direction through the cancellous bone until the cortical bone resistance of the sinus floor is met. Therefore, the probe osteotome provides the surgical working length, which is the true anatomical distance from the bone crest to the sinus floor in the exact location where the implant should be placed. Thus, the working action of all manual and rotating instruments that will be used in subsequent surgical steps must be set at the surgical working length using the proper adjustable stop device.
A radiographic pin (∅: 1.2 mm) can be used to check direction and depth of the prepared site by means of a periapical radiograph. The radiographic pin handle has a diameter of 4 mm, thus permitting evaluation of the spatial relationship between the prepared site and the buccolingual and mesiodistal dimensions of the alveolar ridge. This will help the clinician to determine the diameter of the implant to be placed.
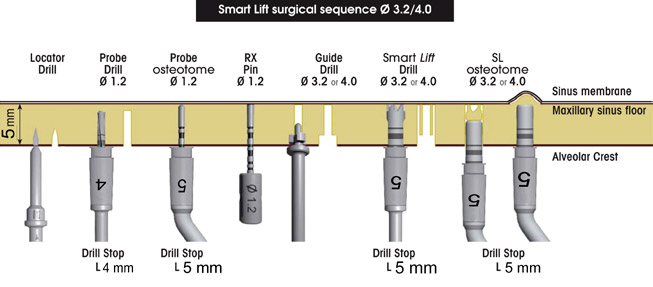
Conventional sequence of the Smart Lift technique (residual bone height ≥ 3 mm)9Trombelli L, Minenna P, Franceschetti G, Farina R, Minenna L. Smart-Lift: a new minimally-invasive procedure for sinus floor elevation. → Dental Cadmos. 2008;76:71–83.,10Trombelli L, Minenna P, Franceschetti G, Minenna L, Itro A, Farina R. Minimally invasive technique for transcrestal sinus floor elevation: a case report. → Quintessence Int. 2010 May:41(5):363–9..
A guide drill with a diameter of 3.2 mm (implant ∅: 3.75 – 4.50 mm) or 4.0 mm (implant ∅: 4.5 mm or larger) is then used. This drill follows the 1.2 mm diameter site preparation and creates a crestal countersink, where the trephine bur (Smart Lift drill) will be inserted. Such a countersink will force the trephine bur to follow the desired direction. The Smart Lift drill (∅: 3.2 or 4.0 mm), set at the surgical working length, produces a bone core up to the sinus floor. The bone core and a variable amount of particulate bone substitute are condensed and malleted to fracture the sinus floor by means of a calibrated osteotome (Smart Lift elevator, ∅: 3.2 or 4.0 mm) that corresponds to the diameter of the trephine preparation. If the alveolar bone core is found to be inside the trephine, the bone core is gently removed from the trephine and replaced in the bone preparation. The osteotome is used under gently malleting forces to implode the trephined bone core over the sinus floor. In relation to the extent of vertical bone augmentation to be achieved, an autogenous cortical bone particulate or a particulate bone substitute can be further grafted and condensed into the sinus with the osteotome. Again, the Smart Lift elevator is used with the proper stop device at the surgical working length, thus preventing any unwanted penetration of the instruments into the sinus cavity. Provided that the residual bone may ensure an adequate primary stability, an implant can be inserted during the same surgical session. Otherwise, a staged approach is recommended. If the residual bone height is 2 mm, a modified sequence must be adopted.11Trombelli L, Franceschetti G, Trisi P, Farina R. Incremental, transcrestal sinus floor elevation with a minimally invasive technique in the rehabilitation of severe maxillary atrophy. Clinical and histological findings from a proof-ofconcept case series. → J Oral Maxillofac Surg. 2015 May;73(5):861–88. The mean duration of the sinus floor elevation procedure (from cortical perforation to the completion of the grafting procedure), as reported in different cohort and randomized controlled trials, ranged between 19 and 32 min.12Trombelli L, Minenna P, Franceschetti G, Minenna L, Itro A, Farina R. Minimally invasive technique for transcrestal sinus floor elevation: a case report. → Quintessence Int. 2010 May:41(5):363–9.,13Franceschetti G, Trombelli L, Minenna L, Franceschetti G, Farina R. Learning curve of a minimally invasive technique for transcrestal sinus floor elevation: a split-group analysis in a prospective case series with multiple clinicians. → Implant Dent. 2015 Oct;24(5):517–26.,14Trombelli L, Minenna P, Franceschetti G, Minenna L, Farina R. Transcrestal sinus floor elevation with a minimally invasive technique. → J Periodontol. 2010 Jan;81(1):158–66.,15Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32.,16Trombelli L, Franceschetti G, Stacchi C, Minenna L, Riccardi O, Di Raimondo R, Rizzi A, Farina R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or -tricalcium phosphate: a multicenter, double-blind, randomized, controlled clinical trial. → J Clin Periodontol. 2014 Mar;41(3):311–9.,17Farina R, Franceschetti G, Travaglini D, Consolo U, Minenna L, Schincaglia GP, Riccardi O, Bandieri A, Maietti E, Trombelli L. Morbidity following transcrestal and lateral sinus floor elevation: a randomized trial. → J Clin Periodontol. 2018 Sep;45(9):1128–39.
In a recent study,18Franceschetti G, Trombelli L, Minenna L, Franceschetti G, Farina R. Learning curve of a minimally invasive technique for transcrestal sinus floor elevation: a split-group analysis in a prospective case series with multiple clinicians. → Implant Dent. 2015 Oct;24(5):517–26. patients treated with the Smart Lift technique by 3 operators with different levels of experience in implant surgery and inexperienced with respect to the Smart Lift technique, showed a substantial extent of sinus elevation in a limited operation time, along with minimal incidence of membrane perforation and post-surgical dosage of anti-inflammatory drugs.19Franceschetti G, Trombelli L, Minenna L, Franceschetti G, Farina R. Learning curve of a minimally invasive technique for transcrestal sinus floor elevation: a split-group analysis in a prospective case series with multiple clinicians. → Implant Dent. 2015 Oct;24(5):517–26.
The clinical application of the Smart Lift technique is illustrated in Figure 2.
The Smart Lift technique: Clinical outcomes
The Smart Lift technique was first reported in 2008.20Trombelli L, Minenna P, Franceschetti G, Farina R, Minenna L. Smart-Lift: a new minimally-invasive procedure for sinus floor elevation. → Dental Cadmos. 2008;76:71–83. During the last 10 years, several studies have been conducted,21Trombelli L, Minenna P, Franceschetti G, Farina R, Minenna L. Smart-Lift: a new minimally-invasive procedure for sinus floor elevation. → Dental Cadmos. 2008;76:71–83.,22Trombelli L, Minenna P, Franceschetti G, Minenna L, Itro A, Farina R. Minimally invasive technique for transcrestal sinus floor elevation: a case report. → Quintessence Int. 2010 May:41(5):363–9.,23Franceschetti G, Trombelli L, Minenna L, Franceschetti G, Farina R. Learning curve of a minimally invasive technique for transcrestal sinus floor elevation: a split-group analysis in a prospective case series with multiple clinicians. → Implant Dent. 2015 Oct;24(5):517–26.,24Trombelli L, Franceschetti G, Trisi P, Farina R. Incremental, transcrestal sinus floor elevation with a minimally invasive technique in the rehabilitation of severe maxillary atrophy. Clinical and histological findings from a proof-ofconcept case series. → J Oral Maxillofac Surg. 2015 May;73(5):861–88.,25Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32.,26Trombelli L, Franceschetti G, Stacchi C, Minenna L, Riccardi O, Di Raimondo R, Rizzi A, Farina R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or -tricalcium phosphate: a multicenter, double-blind, randomized, controlled clinical trial. → J Clin Periodontol. 2014 Mar;41(3):311–9.,27Farina R, Franceschetti G, Travaglini D, Consolo U, Minenna L, Schincaglia GP, Riccardi O, Bandieri A, Maietti E, Trombelli L. Morbidity following transcrestal and lateral sinus floor elevation: a randomized trial. → J Clin Periodontol. 2018 Sep;45(9):1128–39.,28Trombelli L, Franceschetti G, Farina R, Itro A. Smart-lift technique used in association with a hydroxyapatite-based biomaterial. Clinical outcomes and postoperative morbidity. → Eur J Oral Surg. 2010 Sep;2(1):47–55.,29Franceschetti G, Farina R, Stacchi C, Di Lenarda R, Di Raimondo R, Trombelli L. Radiographic outcomes of transcrestal sinus floor elevation performed with a minimally invasive technique in smoker and non-smoker patients. → Clin Oral Implants Res. 2014 Apr;25(4):493–9.,30Franceschetti G, Rizzi A, Minenna L, Pramstraller M, Trombelli L, Farina R. Patient-reported outcomes of implant placement performed concomitantly with transcrestal sinus floor elevation or entirely in native bone. → Clin Oral Implants Res. 2017 Feb;28(2):156–62. reporting data on treatment outcomes and post-surgical morbidity of the procedure (Table 1). Only in 1 case did the Smart Lift technique not allow for the placement of implant concomitant to tSFE31Farina R, Franceschetti G, Travaglini D, Consolo U, Minenna L, Schincaglia GP, Riccardi O, Bandieri A, Maietti E, Trombelli L. Morbidity following transcrestal and lateral sinus floor elevation: a randomized trial. → J Clin Periodontol. 2018 Sep;45(9):1128–39. and implant insertion had to be delayed owing to the lack of primary stability. Implant survival shifted from 100% at 6 months in 8 studies32Trombelli L, Minenna P, Franceschetti G, Farina R, Minenna L. Smart-Lift: a new minimally-invasive procedure for sinus floor elevation. → Dental Cadmos. 2008;76:71–83.,33Trombelli L, Minenna P, Franceschetti G, Minenna L, Itro A, Farina R. Minimally invasive technique for transcrestal sinus floor elevation: a case report. → Quintessence Int. 2010 May:41(5):363–9.,34Franceschetti G, Trombelli L, Minenna L, Franceschetti G, Farina R. Learning curve of a minimally invasive technique for transcrestal sinus floor elevation: a split-group analysis in a prospective case series with multiple clinicians. → Implant Dent. 2015 Oct;24(5):517–26.,35Trombelli L, Minenna P, Franceschetti G, Minenna L, Farina R. Transcrestal sinus floor elevation with a minimally invasive technique. → J Periodontol. 2010 Jan;81(1):158–66.,36Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32.,37Trombelli L, Franceschetti G, Stacchi C, Minenna L, Riccardi O, Di Raimondo R, Rizzi A, Farina R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or -tricalcium phosphate: a multicenter, double-blind, randomized, controlled clinical trial. → J Clin Periodontol. 2014 Mar;41(3):311–9.,38Franceschetti G, Farina R, Stacchi C, Di Lenarda R, Di Raimondo R, Trombelli L. Radiographic outcomes of transcrestal sinus floor elevation performed with a minimally invasive technique in smoker and non-smoker patients. → Clin Oral Implants Res. 2014 Apr;25(4):493–9.,39Franceschetti G, Rizzi A, Minenna L, Pramstraller M, Trombelli L, Farina R. Patient-reported outcomes of implant placement performed concomitantly with transcrestal sinus floor elevation or entirely in native bone. → Clin Oral Implants Res. 2017 Feb;28(2):156–62. to 94% at 12 months in 1 study.40Farina R, Franceschetti G, Travaglini D, Consolo U, Minenna L, Schincaglia GP, Riccardi O, Bandieri A, Maietti E, Trombelli L. Morbidity following transcrestal and lateral sinus floor elevation: a randomized trial. → J Clin Periodontol. 2018 Sep;45(9):1128–39. The length of the inserted implants varied between 9.06 and 10.3 mm,41Trombelli L, Minenna P, Franceschetti G, Minenna L, Farina R. Transcrestal sinus floor elevation with a minimally invasive technique. → J Periodontol. 2010 Jan;81(1):158–66. and the height of the residual bone ranged from 4.513 to 6.6 mm.42Trombelli L, Minenna P, Franceschetti G, Farina R, Minenna L. Smart-Lift: a new minimally-invasive procedure for sinus floor elevation. → Dental Cadmos. 2008;76:71–83. The extent of sinus lift ranged from 5.38 to 7.7 mm.43Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32.
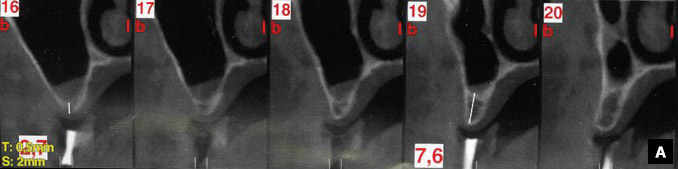
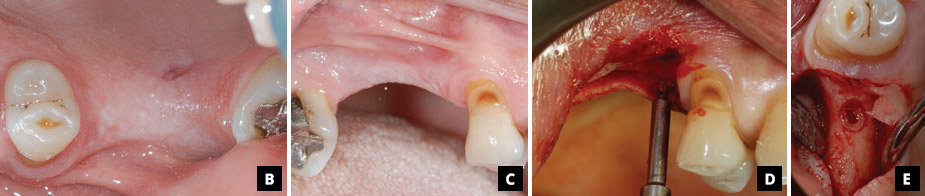
A 52-year-old male patient presented with an eden tulous area in the maxillary right quadrant. Neither systemic nor local conditions contraindicating implant surgery or sinus lift procedures were identified at the screening visit. The prosthetic rehabilitation plan included the placement of 2 implant- supported crowns in the region of the maxillary right second premolar and first molar, which had been extracted 3 years prior to the visit.(A) Computed tomography scans showed a radiographic working length of 2.7 mm at the first molar site and 7.6 mm at the second premolar site. (B) Lateral clinical photograph. (C) Occlusal clinical photograph. (D) The surgical working length assessed at the position of the second premolar was 6 mm as diagnosed with the probe osteotome. Therefore, a tSFE procedure was performed also at this site. (E) A countersink was prepared with the guide drill.
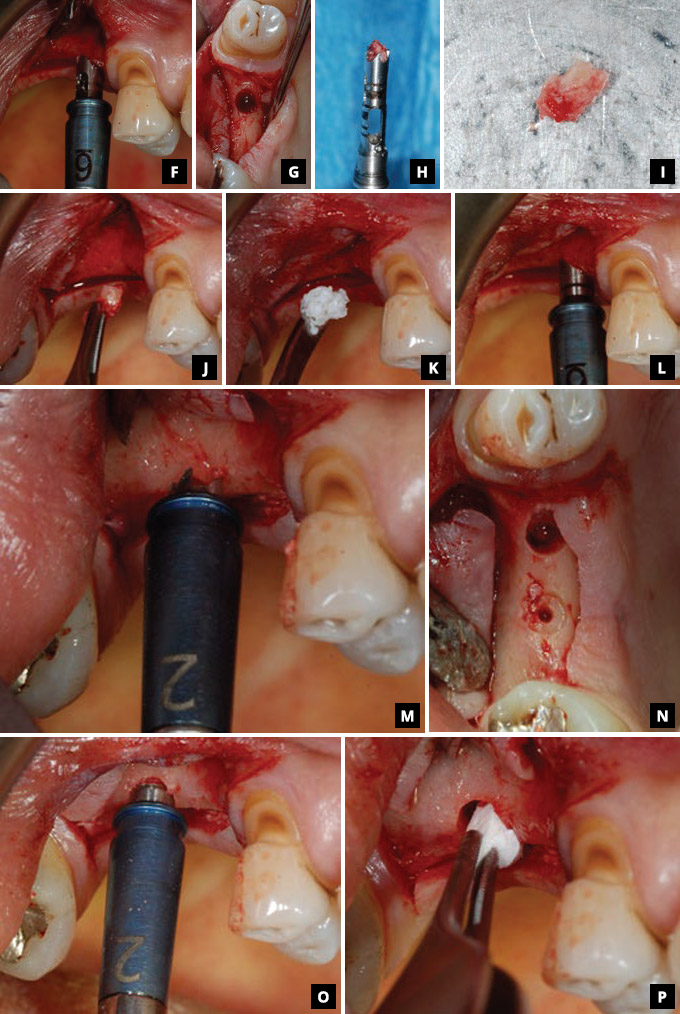
(F–I) A trephined bone core was created with the Smart Lift drill with a diameter of 3.2 mm.
(J–L) The bone core, along with a bone substitute (Bio-Oss spongiosa granules, particle size of 0.25–1.00 mm, 500 mg package; Geistlich Pharma), was gently malleted using the 3.2 mm diameter Smart Lift elevator with the 6 mm stop device until the sinus floor was fractured.
(M) At the distal implant site, the surgical working length was 2 mm as assessed using the probe osteotome.
(N) A countersink created with the guide drill superficially marked the area for the Smart Lift elevator.
(O) The residual bone was gently malleted into the sinus with the Smart Lift elevator.
(P) A 3-D collagen matrix (Mucograft Seal) was trimmed and inserted into the crestal access.
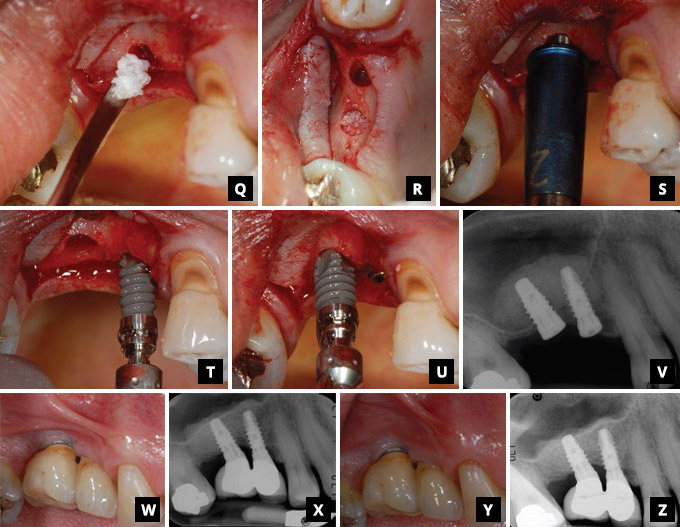
(Q–S)The grafting procedure was performed by repeated insertion of the bone substitute by means of the Smart Lift elevator.
(T–V) Two implants (9.5 × 3.5 mm and 8.0 × 4.0 mm; SPI Element Inicell, Thommen Medical) were inserted at the second premolar and first molar sites, respectively. The distal implant was slightly angulated in order to enhance primary stability.
(W–Z) Clinical and radiographic aspects of the rehabilitated sites at 1 and 3 years post-surgery.
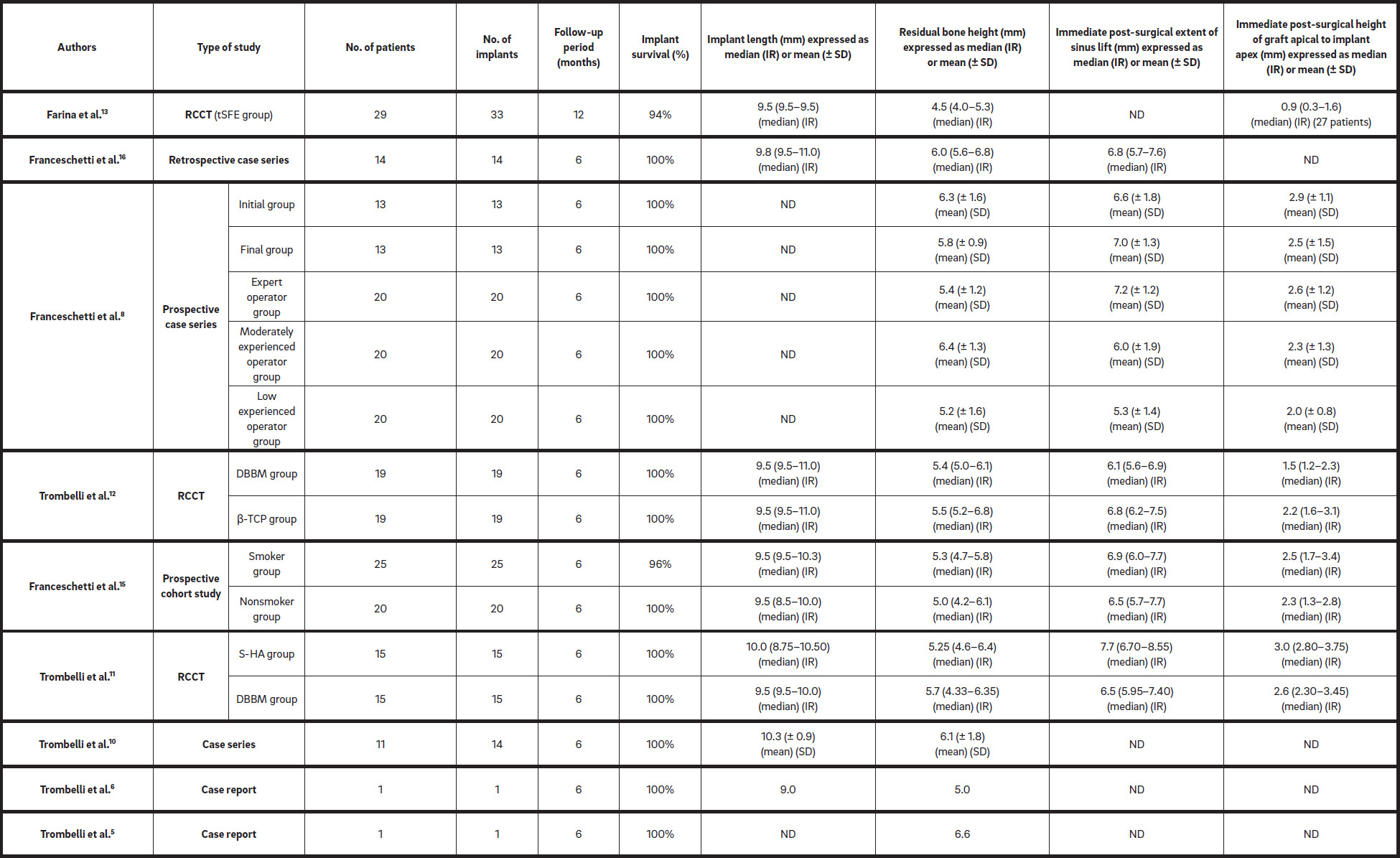
TCP = tricalcium phosphate; ND = no data; IR = interquartile range; S-HA = synthetic hydroxyapatite.Table 1
Studies reporting data on treatment outcomes of the Smart Lift technique.
The Smart Lift technique : Post – surgical morbidity
The mean scores for post-surgical pain and discomfort, as reported on a 100 mm visual analog scale,44McCormack HM, Horne DJ, Sheather S. Clinical applications of visual analogue scales: a critical review. → Psychol Med. 1988 Nov;18(4):1007–19. ranged from 0 to 62 mm and from 0 to 17 mm, respectively.45Franceschetti G, Trombelli L, Minenna L, Franceschetti G, Farina R. Learning curve of a minimally invasive technique for transcrestal sinus floor elevation: a split-group analysis in a prospective case series with multiple clinicians. → Implant Dent. 2015 Oct;24(5):517–26.,46Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32. The level of pain significantly decreases, starting from the first day post- surgery,47Farina R, Franceschetti G, Travaglini D, Consolo U, Minenna L, Schincaglia GP, Riccardi O, Bandieri A, Maietti E, Trombelli L. Morbidity following transcrestal and lateral sinus floor elevation: a randomized trial. → J Clin Periodontol. 2018 Sep;45(9):1128–39. and reaches very low levels (ranging from 1.0 to 2.1 mm) at the seventh day.48Trombelli L, Minenna P, Franceschetti G, Minenna L, Itro A, Farina R. Minimally invasive technique for transcrestal sinus floor elevation: a case report. → Quintessence Int. 2010 May:41(5):363–9.,49Franceschetti G, Trombelli L, Minenna L, Franceschetti G, Farina R. Learning curve of a minimally invasive technique for transcrestal sinus floor elevation: a split-group analysis in a prospective case series with multiple clinicians. → Implant Dent. 2015 Oct;24(5):517–26.,50Trombelli L, Minenna P, Franceschetti G, Minenna L, Farina R. Transcrestal sinus floor elevation with a minimally invasive technique. → J Periodontol. 2010 Jan;81(1):158–66.,51Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32.,52Trombelli L, Franceschetti G, Stacchi C, Minenna L, Riccardi O, Di Raimondo R, Rizzi A, Farina R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or -tricalcium phosphate: a multicenter, double-blind, randomized, controlled clinical trial. → J Clin Periodontol. 2014 Mar;41(3):311–9.,53Farina R, Franceschetti G, Travaglini D, Consolo U, Minenna L, Schincaglia GP, Riccardi O, Bandieri A, Maietti E, Trombelli L. Morbidity following transcrestal and lateral sinus floor elevation: a randomized trial. → J Clin Periodontol. 2018 Sep;45(9):1128–39.
Six studies have reported data on intra- and post-surgical complications.10–13 Membrane perforation was the most frequent complication, with the incidence ranging from 054Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32. to 13%.55Trombelli L, Franceschetti G, Stacchi C, Minenna L, Riccardi O, Di Raimondo R, Rizzi A, Farina R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or -tricalcium phosphate: a multicenter, double-blind, randomized, controlled clinical trial. → J Clin Periodontol. 2014 Mar;41(3):311–9. In all cases, the perforation was managed with the insertion of a surgical hemostatic dressing (Gingistat, GABA Vebas) or a collagen matrix (Mucograft Seal, Geistlich Pharma). In all cases, the grafting procedure was completed and the implant was inserted. Rarely, other types of complications, such as transitory paresthesia in the suborbital area (1 case),56Franceschetti G, Farina R, Stacchi C, Di Lenarda R, Di Raimondo R, Trombelli L. Radiographic outcomes of transcrestal sinus floor elevation performed with a minimally invasive technique in smoker and non-smoker patients. → Clin Oral Implants Res. 2014 Apr;25(4):493–9. tinnitus (1 case)57Franceschetti G, Farina R, Stacchi C, Di Lenarda R, Di Raimondo R, Trombelli L. Radiographic outcomes of transcrestal sinus floor elevation performed with a minimally invasive technique in smoker and non-smoker patients. → Clin Oral Implants Res. 2014 Apr;25(4):493–9. and benign paroxysmal positional vertigo (1 case)58Trombelli L, Franceschetti G, Stacchi C, Minenna L, Riccardi O, Di Raimondo R, Rizzi A, Farina R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or -tricalcium phosphate: a multicenter, double-blind, randomized, controlled clinical trial. → J Clin Periodontol. 2014 Mar;41(3):311–9. occurred. All these complications spontaneously subsided within the first week post-surgery.
Conclusion
In the edentulous maxillary posterior sextants, the vertical dimension of the residual bone crest may frequently call for bone augmentation procedures to allow for the placement of implants of adequate length and width. Among the techniques for tSFE that have been proposed in the literature, the Smart Lift technique represents a simplified, user-friendly, standardized procedure that allows for a substantial extent of sinus lift with limited post-surgical morbidity.
Competing interests
The authors declare that they have no competing interests.

Interview
with Leonardo Trombelli
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry? And what is the relevance of your study’s findings to the daily practice of a dentist?
Dr. Farina: We are convinced that findings from our studies on the Smart Lift technique are of clinical relevance to the profession, irrespective of the level of experience of the surgeon. In this respect, the Smart Lift technique is substantially effective, even when applied by practitioners with limited experience in implant surgery in general and sinus floor elevation procedures in particular. However, the Smart Lift technique now represents a valid alternative to traditional sinus floor elevation with a lateral approach for the experienced dentist: The Smart Lift technique was recently shown to be characterized by 80% less graft material, 50% shorter operative times and lower postoperative morbidity when compared with the lateral approach.
In several studies, we have tested the Smart Lift technique with different graft materials, demonstrating that the technique can be successfully used in combination with slowly resorbed graft materials (e.g., bovine-derived xenograft and synthetic hydroxyapatite), as well as materials that resorb more rapidly, such as beta-tricalcium phosphate. This seems to indicate that the practitioner who decides to apply the Smart Lift technique in his or her practice may effectively combine the technique with a wide selection of grafts commonly used in bone reconstructive surgery.
Finally, we have tested the Smart Lift technique in unfavorable patient conditions, with encouraging findings. More specifically, we showed that the Smart Lift technique may be effectively used in smoker patients (well known for representing a patient category at high risk for complications and impaired outcomes after oral reconstructive surgery). Interestingly, clinical outcomes of the Smart Lift technique in smokers were shown to be comparable to those observed in nonsmokers. In addition, we demonstrated that the Smart Lift technique can be used effectively according to a modified sequence of its instruments to augment the vertical dimension of the residual bone crest at sites showing extreme bone atrophy (i.e., residual bone height of 2–3 mm). Therefore, it seems to represent an option for oral rehabilitation even in some of the most challenging clinical situations.
What are your recommendations for further investigation of the topic of your article?
Prof. Trombelli: There are some aspects that undoubtedly deserve further investigation regarding this topic. First, we are interested in evaluating the long-term clinical and radiographic outcomes of the procedure. To accomplish this purpose, we are finalizing a long-term observational cohort study that will soon be submitted for publication. I can anticipate that, despite a long-term dimensional reduction of the grafted space (as described for other techniques), the results remain excellent even at long time intervals (5–7 years).
Second, but not less important, we are interested in evaluating histologically the early and latest phases of maturation of the grafted area in the endo-sinusal space. Obviously, this interest is complicated by the fact that the implant is placed concomitant with the procedure in the great majority of cases, thus making it impossible to justify a surgical re-entry to collect a tissue sample.
References
| 1. | ↑ | Pramstraller M, Farina R, Franceschetti G, Pramstraller C, Trombelli L. Ridge dimensions of the edentulous posterior maxilla: a retrospective analysis of a cohort of 127 patients using computerized tomography data. → Clin Oral Implants Res. 2011 Jan;22(1):54–61. Erratum in: Clin Oral Implants Res. 2011 Feb;22(2):235. |
| 2. | ↑ | Farina R, Pramstraller M, Franceschetti G, Pramstraller C, Trombelli L. Alveolar ridge dimensions in maxillary posterior sextants: a retrospective comparative study of dentate and edentulous sites using computerized tomography data. → Clin Oral Implants Res. 2011 Oct;22(10):1138–44. |
| 3. | ↑ | Romero-Millán J, Martorell-Calatayud L, Peñarrocha M, García-Mira B. Indirect osteotome maxillary sinus floor elevation: an update. → J Oral Implantol. 2012 Dec;38(6):799–804. |
| 4. | ↑ | Pjetursson BE, Lang NP. Sinus floor elevation utilizing the transalveolar approach. → Periodontol 2000. 2014 Oct;66(1):59–71. |
| 5, 9, 20, 21, 32, 42. | ↑ | Trombelli L, Minenna P, Franceschetti G, Farina R, Minenna L. Smart-Lift: a new minimally-invasive procedure for sinus floor elevation. → Dental Cadmos. 2008;76:71–83. |
| 6, 10, 12, 22, 33, 48. | ↑ | Trombelli L, Minenna P, Franceschetti G, Minenna L, Itro A, Farina R. Minimally invasive technique for transcrestal sinus floor elevation: a case report. → Quintessence Int. 2010 May:41(5):363–9. |
| 7. | ↑ | Fugazzotto PA. Immediate implant placement following a modified trephine/ osteotome approach: success rates of 116 implants to 4 years in function. → Int J Oral Maxillofac Implants. 2002 Jan–Feb;17(1):113–20. |
| 8, 13, 18, 19, 23, 34, 45, 49. | ↑ | Franceschetti G, Trombelli L, Minenna L, Franceschetti G, Farina R. Learning curve of a minimally invasive technique for transcrestal sinus floor elevation: a split-group analysis in a prospective case series with multiple clinicians. → Implant Dent. 2015 Oct;24(5):517–26. |
| 11, 24. | ↑ | Trombelli L, Franceschetti G, Trisi P, Farina R. Incremental, transcrestal sinus floor elevation with a minimally invasive technique in the rehabilitation of severe maxillary atrophy. Clinical and histological findings from a proof-ofconcept case series. → J Oral Maxillofac Surg. 2015 May;73(5):861–88. |
| 14, 35, 41, 50. | ↑ | Trombelli L, Minenna P, Franceschetti G, Minenna L, Farina R. Transcrestal sinus floor elevation with a minimally invasive technique. → J Periodontol. 2010 Jan;81(1):158–66. |
| 15, 25, 36, 43, 46, 51, 54. | ↑ | Trombelli L, Franceschetti G, Rizzi A, Minenna P, Minenna L, Farina R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomized clinical trial. → Clin Oral Implants Res. 2012 Apr;23(4):424–32. |
| 16, 26, 37, 52, 55, 58. | ↑ | Trombelli L, Franceschetti G, Stacchi C, Minenna L, Riccardi O, Di Raimondo R, Rizzi A, Farina R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or -tricalcium phosphate: a multicenter, double-blind, randomized, controlled clinical trial. → J Clin Periodontol. 2014 Mar;41(3):311–9. |
| 17, 27, 31, 40, 47, 53. | ↑ | Farina R, Franceschetti G, Travaglini D, Consolo U, Minenna L, Schincaglia GP, Riccardi O, Bandieri A, Maietti E, Trombelli L. Morbidity following transcrestal and lateral sinus floor elevation: a randomized trial. → J Clin Periodontol. 2018 Sep;45(9):1128–39. |
| 28. | ↑ | Trombelli L, Franceschetti G, Farina R, Itro A. Smart-lift technique used in association with a hydroxyapatite-based biomaterial. Clinical outcomes and postoperative morbidity. → Eur J Oral Surg. 2010 Sep;2(1):47–55. |
| 29, 38, 56, 57. | ↑ | Franceschetti G, Farina R, Stacchi C, Di Lenarda R, Di Raimondo R, Trombelli L. Radiographic outcomes of transcrestal sinus floor elevation performed with a minimally invasive technique in smoker and non-smoker patients. → Clin Oral Implants Res. 2014 Apr;25(4):493–9. |
| 30, 39. | ↑ | Franceschetti G, Rizzi A, Minenna L, Pramstraller M, Trombelli L, Farina R. Patient-reported outcomes of implant placement performed concomitantly with transcrestal sinus floor elevation or entirely in native bone. → Clin Oral Implants Res. 2017 Feb;28(2):156–62. |
| 44. | ↑ | McCormack HM, Horne DJ, Sheather S. Clinical applications of visual analogue scales: a critical review. → Psychol Med. 1988 Nov;18(4):1007–19. |





Leave a Reply
Be the First to Comment!