A surgical approach to the management of periapical implant lesions: A report of 3 clinical cases with up to 6 years of follow-up
September 26, 2018 / Categories: Digital Dentistry, Implant Dentistry

Blaya Tárraga, Juan Antonio

Peñarrocha Oltra, David
Menéndez Nieto, Isabel

Peñarrocha Diago, Maria
Abstract
Background
Periapical implant lesions may be a cause of early failure of implants. The purpose of this article is to describe the surgical treatment of the periapical implant lesion and its intraoperative approach.
Case presentations
Three patients with periapical implant lesions (2 in the maxilla and 1 in the mandible) after implant placement are described. All 3 patients reported inflammation and pain. Periapical and panoramic radiographic examination showed periapical radiolucency around the 3 implants. The diagnosis was acute suppurative stage in all 3 cases. After surgical treatment, all of the implants survived. Clinical and radiographic controls showed signs of health with a follow-up of 3, 6 and 4 years, respectively.
Conclusion
In the patients studied, pain in the area after implant placement suggested a periapical implant lesion. The surgical approach used to remove the granulation tissue showed good results. Up to 6-year clinical and radiographic controls, all 3 cases showed complete healing of soft and hard tissue. Diagnosis and early treatment are crucial to ensure a correct osseointegration process and avoid implant failure.
Keywords
Surgical procedures; operative; periapical implant lesion; implant lesion; early apical periimplantitis; early failure.
Background
A periapical implant lesion may be a cause of implant failure. This lesion, also referred to as apical periimplantitis or retrograde periimplantitis, was described by McAllister in 1992 as injuries in the apical portion of implants.1McAllister BS, Masters D, Meffert RM. Treatment of implants demonstrating periapical radiolucencies. → Pract Periodontics Aesthet Dent. 1992 Nov–Dec;4(9):37–41. A year later, Sussman and Moss defined the lesion as an infectious-inflammatory process of the tissue surrounding the implant apex.2Sussman HI, Moss SS. Localized osteomyelitis secondary to endodontic- implant pathosis. A case report. → J Periodontol. 1993 Apr;64(4):306–10. In a recent consensus,3Peñarrocha-Diago M, Peñarrocha-Diago M, Blaya-Tárraga JA. State of the art and clinical recommendations in periapical implant lesions. 9th Mozo-Grau Ticare Conference in Quintanilla, Spain. → J Clin Exp Dent. 2017 Mar 1;9(3):e471–3. doi: 10.4317/ jced.53600. it was agreed to define it as a lesion of inflammatory and infectious nature, developing in the axial axis of the implant during osseointegration, with the maintenance of normal coronal bone in early stages.
The frequency described in the literature of this lesion is low, between 0.26% and 2.70%.4Quirynen M, Vogels R, Alsaadi G, Naert I, Jacobs R, van Steenberghe D. Predisposing conditions for retrograde peri-implantitis, and treatment suggestions. → Clin Oral Implants Res. 2005 Oct;16(5):599–608.,5Reiser GM, Nevins M. The implant periapical lesion: etiology, prevention, and treatment. → Compend Contin Educ Dent. 1995 Aug;16(8):768, 770, 772 passim.,6Peñarrocha-Diago M, Boronat-Lopez A, García-Mira B. Inflammatory implant periapical lesion: etiology, diagnosis, and treatment—presentation of 7 cases. → J Oral Maxillofac Surg. 2009 Jan;67(1):168–73. Zhou et al. found an increase of up to 7.8% in frequency with the presence of an endodontically treated adjacent tooth.7Zhou W, Han C, Li D, Li Y, Song Y, Zhao Y. Endodontic treatment of teeth induces retrograde peri-implantitis. → Clin Oral Implants Res. 2009 Dec;20(12):1326–32. Several factors have been proposed that could be related to the onset of this lesion: endodontic pathology of the tooth replaced by the implant or of the adjacent tooth;8Reiser GM, Nevins M. The implant periapical lesion: etiology, prevention, and treatment. → Compend Contin Educ Dent. 1995 Aug;16(8):768, 770, 772 passim.,9Peñarrocha-Diago M, Boronat-Lopez A, García-Mira B. Inflammatory implant periapical lesion: etiology, diagnosis, and treatment—presentation of 7 cases. → J Oral Maxillofac Surg. 2009 Jan;67(1):168–73.,10Zhou W, Han C, Li D, Li Y, Song Y, Zhao Y. Endodontic treatment of teeth induces retrograde peri-implantitis. → Clin Oral Implants Res. 2009 Dec;20(12):1326–32.,11Brisman DL, Brisman AS, Moses MS. Implant failures associated with asymptomatic endodontically treated teeth. → J Am Dent Assoc. 2001 Feb;132(2):191–5.,12Temmerman A, Lefever D, Teughels W, Balshi TJ, Balshi SF, Quirynen M. Etiology and treatment of periapical lesions around dental implants. → Periodontol 2000. 2014 Oct;66(1):247–54.,13Lefever D, Van Assche N, Temmerman A, Teughels W, Quirynen M. Aetiology, microbiology and therapy of periapical lesions around oral implants: a retrospective analysis. → J Clin Periodontol. 2013 Mar;40(3):296–302. pre-existing bone disease or the presence of root fragments or foreign bodies;14McAllister BS, Masters D, Meffert RM. Treatment of implants demonstrating periapical radiolucencies. → Pract Periodontics Aesthet Dent. 1992 Nov–Dec;4(9):37–41.,15Quirynen M, Vogels R, Alsaadi G, Naert I, Jacobs R, van Steenberghe D. Predisposing conditions for retrograde peri-implantitis, and treatment suggestions. → Clin Oral Implants Res. 2005 Oct;16(5):599–608.,16Reiser GM, Nevins M. The implant periapical lesion: etiology, prevention, and treatment. → Compend Contin Educ Dent. 1995 Aug;16(8):768, 770, 772 passim.,17Peñarrocha-Diago M, Boronat-Lopez A, García-Mira B. Inflammatory implant periapical lesion: etiology, diagnosis, and treatment—presentation of 7 cases. → J Oral Maxillofac Surg. 2009 Jan;67(1):168–73.,18Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. → Eur J Oral Sci. 1998 Feb;106(1):527–51.,19Chaffee NR, Lowden K, Tiffee JC, Cooper LF. Periapical abscess formation and resolution adjacent to dental implants: a clinical report. → J Prosthet Dent. 2001 Feb;85(2):109–12.,20Oh TJ, Yoon J, Wang HL. Management of the implant periapical lesion: a case report. → Implant Dent. 2003 Mar;12(1):41–6. ,21Scarano A, Di Domizio P, Petrone G, Iezzi G, Piattelli A. Implant periapical lesion: a clinical and histologic case report. → J Oral Implantol. 2000 Apr;26(2):109–13. contamination of the implant surface, and bone overheating during milling or overmilling.22Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. → Eur J Oral Sci. 1998 Feb;106(1):527–51.,23Ayangco L, Sheridan PJ. Development and treatment of retrograde peri-implantitis involving a site with a history of failed endodontic and apicoectomy procedures: a series of reports. → Int J Oral Maxillofac Implants. 2001 May–Jun;16(3):412–7.,24Esposito M, Hirsch J, Lekholm U, Thomsen P. Differential diagnosis and treatment strategies for biologic complications and failing oral implants: a review of the literature. → Int J Oral Maxillofac Implants. 1999 Jul–Aug;14(4):473–90.
Diagnosis of the periapical implant lesion involves clinical and radiographic evaluations, and the treatment will vary according to the findings:
- If the implant has a radiolucent area (not present after surgery owing to overdrilling and manifesting over time) without pain, monitoring of the lesion is recommended, without medical treatment.
- If the radiolucency has increased in size or if the patient develops pain, medical and surgical treatment is indicated.25Peñarrocha-Diago M, Maestre-Ferrín L, Peñarrocha-Oltra D, Canullo L, Piattelli A, Peñarrocha-Diago M. Inflammatory implant periapical lesion prior to osseointegration: a case series study. → Int J Oral Maxillofac Implants. 2013 Jan–Feb;28(1):158–62.,26Peñarrocha-Diago M, Maestre-Ferrín L, Cervera-Ballester J, Peñarrocha-Oltra D. Implant periapical lesion: diagnosis and treatment. → Med Oral Patol Oral Cir Bucal. 2012 Nov 1;17(6):e1023–7. doi: 10.4317/ medoral.17996.
Antibiotics (amoxicillin, amoxicillin/clavulanate, metronidazole and clindamycin) have been used in medical treatment,27Blaya-Tárraga JA, Cervera-Ballester J, Peñarrocha-Oltra D, Peñarrocha-Diago M. Periapical implant lesion: a systematic review. → Med Oral Patol Oral Cir Bucal. 2017 Nov 1;22(6):e737–49. doi: 10.4317/ medoral.21698. although it has been described that initial treatment with antibiotics is not effective in controlling symptomatic or active lesions, and requires surgical access.28Romanos GE, Froum S, Costa-Martins S, Meitner S, Tarnow DP. Implant periapical lesions: etiology and treatment options. → J Oral Implantol. 2011 Feb;37(1):53–63. There is no established gold standard treatment, so the goal is to eliminate the area of infection. Surgical treatment consists of infiltrative anesthesia, incision, full-thickness flap, ostectomy, apical curettage of granulation tissue and profuse irrigation.29Blaya-Tárraga JA, Cervera-Ballester J, Peñarrocha-Oltra D, Peñarrocha-Diago M. Periapical implant lesion: a systematic review. → Med Oral Patol Oral Cir Bucal. 2017 Nov 1;22(6):e737–49. doi: 10.4317/ medoral.21698. This paper describes the surgical approach in 3 clinical cases of periapical implant lesions.
Case presentations
All of the cases were diagnosed and treated in the Oral Surgery Department, Faculty of Medicine and Dentistry, University of Valencia, Valencia, Spain. All of the patients were informed about the study design and procedures. Prior to participating, they were requested to sign an informed consent document.
The classification proposed by Peñarrocha-Diago et al. was used to diagnose the stage of early periimplantitis as nonsuppurative phase, suppurative phase or subacute phase.30Peñarrocha-Diago M, Maestre-Ferrín L, Cervera-Ballester J, Peñarrocha-Oltra D. Implant periapical lesion: diagnosis and treatment. → Med Oral Patol Oral Cir Bucal. 2012 Nov 1;17(6):e1023–7. doi: 10.4317/ medoral.17996.
Surgical procedures
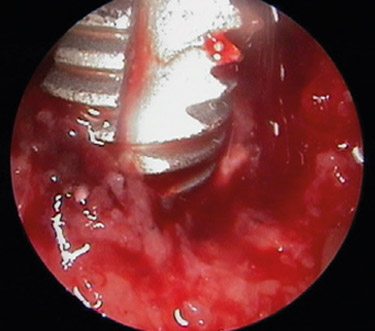
The same surgical procedure was carried out in the 3 cases presented. After infiltrative loco-regional anesthesia and submarginal incision, a full-thickness flap was elevated, and ostectomy was carried out using a round 0.27 mm tungsten carbide bur (JOTA) mounted in a handpiece under abundant irrigation. Surgical curettage of the cavity and the implant surface was performed with an ultrasonic device (Piezon Master 700, E.M.S. Electro Medical Systems) and curettes (Double Gracey Mini Anterior/Posterior, American Eagle Instruments), under profuse irrigation with a sterile saline solution to remove any remaining contaminated tissue. The apical portion of the implant and the surrounding bone were inspected using a rigid endoscope (MÖLLER-WEDEL).
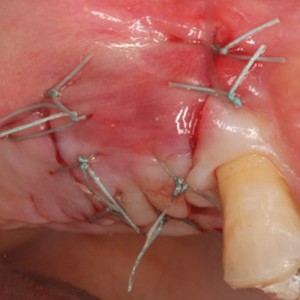
When the adjacent tooth showed an apical lesion, root canal therapy or periapical surgery, if the tooth had been endodontically treated, was performed. Before closure, if the marginal defect was wide, a collagen membrane was placed in order to avoid soft-tissue infiltration in the apex of the implant and improve new bone formation in the cavity.31Peñarrocha-Diago M, Peñarrocha-Diago M, Blaya-Tárraga JA. State of the art and clinical recommendations in periapical implant lesions. 9th Mozo-Grau Ticare Conference in Quintanilla, Spain. → J Clin Exp Dent. 2017 Mar 1;9(3):e471–3. doi: 10.4317/ jced.53600. Tension-free soft-tissue flap closure was performed with a 6-0 polyamide suture (SERALON, SERAG-WIESSNER). Sutures were removed after 1 week.
In all cases, the following medications was prescribed: 2 g amoxicillin and a 0.12% chlorhexidine and 0.05% cetylpyridinium chloride rinse (CPC; Perio·Aid, Dentaid) for 1 min before anesthetizing the patient. Postoperatively, all 3 patients were prescribed 500 mg of amoxicillin and 250 mg of metronidazole every 8 h for 7 days, 25 mg dexketoprofen as required, and a 0.12% chlorhexidine and 0.05% CPC rinse twice daily for 10 days.
-

- Fig. 1A
-

- Fig. 1B
-

- Fig. 1C
(A) Radiograph of the apical lesions involving teeth #44 and 45. (B) Clinical photograph before extractions. (C) Radiograph after extractions, curettage of the apical granulation tissue and alveolar preservation.
-

- Fig. 2A
-

- Fig. 2B
-
- Fig. 3A
-

- Fig. 3B
-
- Fig. 3C
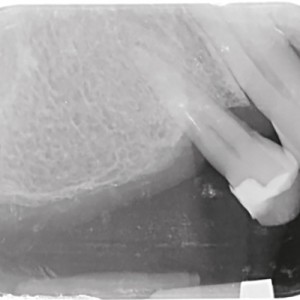
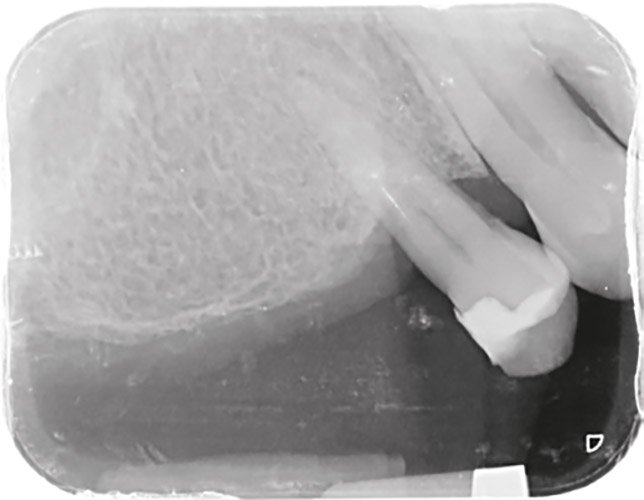
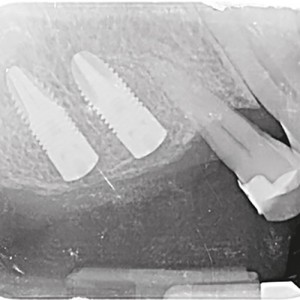
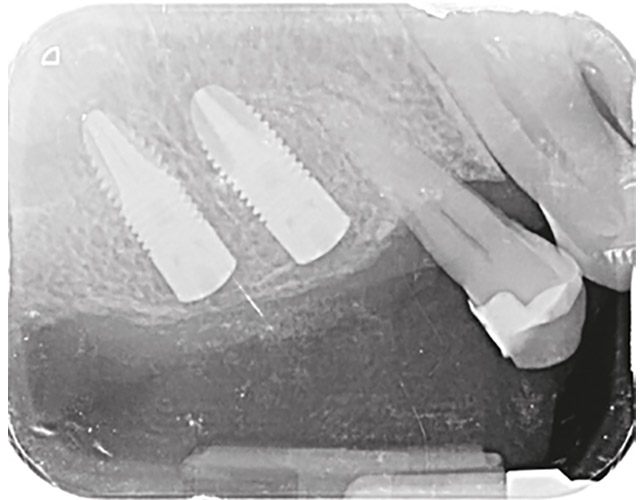
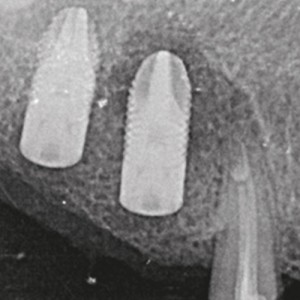
(A) After 3 months, implants were placed. (B) Radiograph after implant placement.
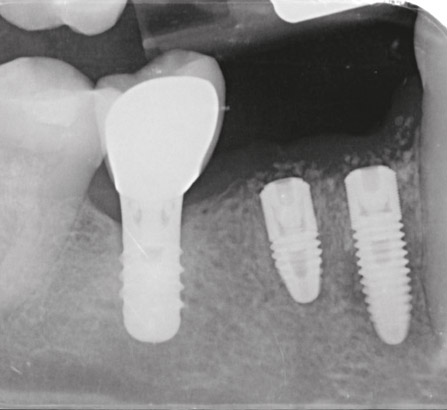
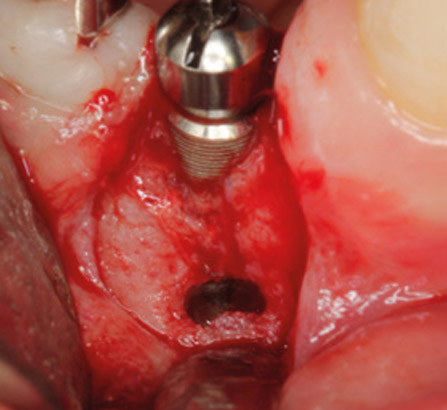
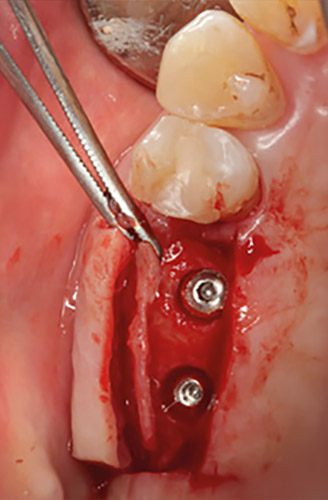
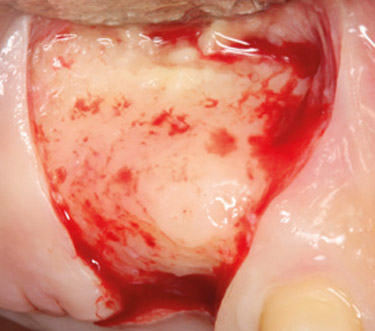
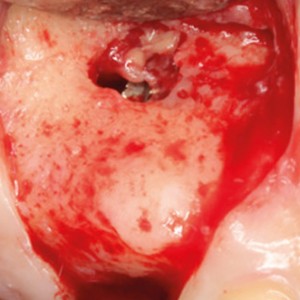
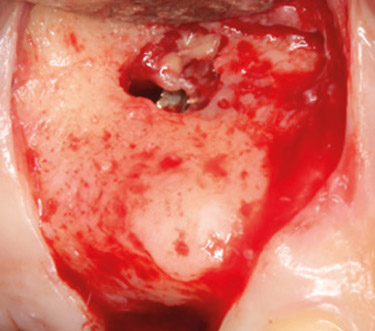
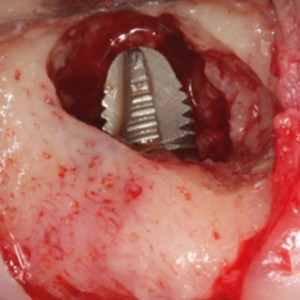
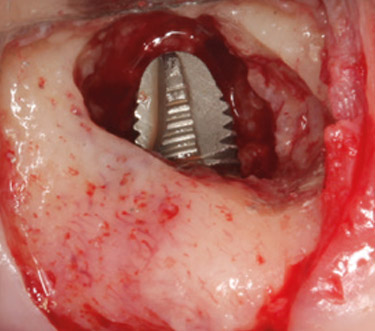
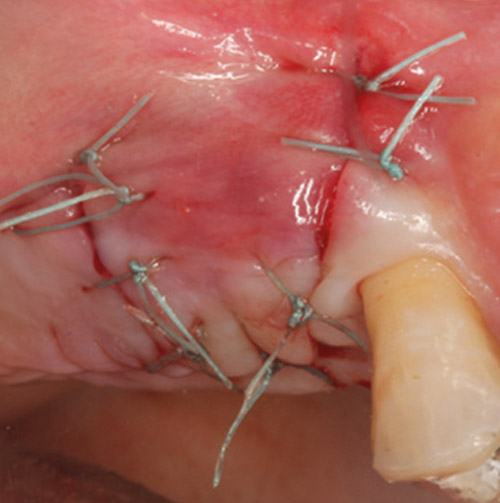
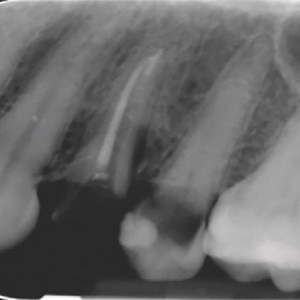
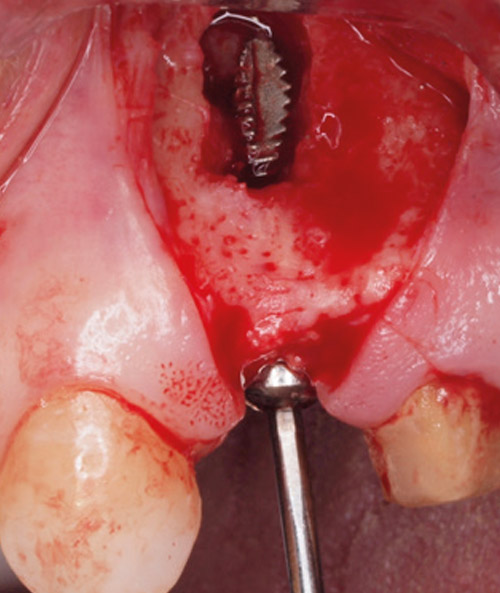
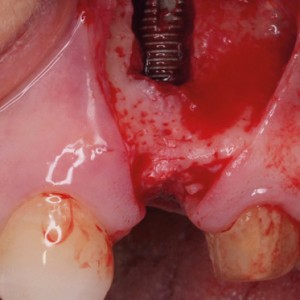
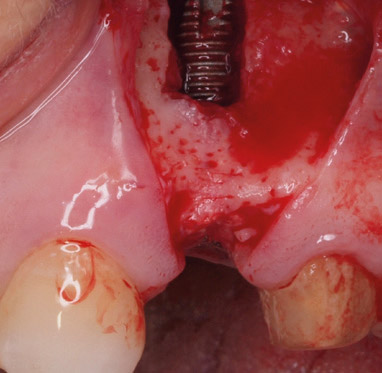
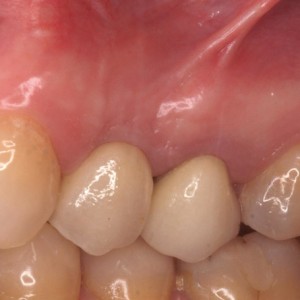
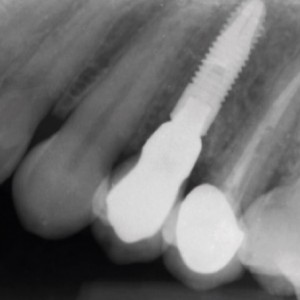
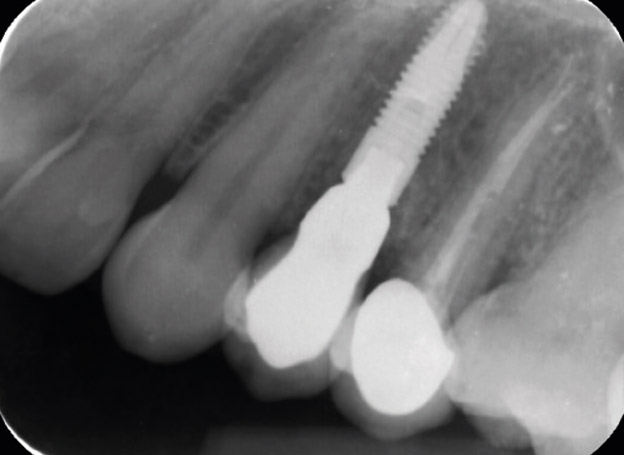
(A) Periapical radiograph showing apical radiolucency localized at implant #44. (B) Swelling of surrounding tissue. (C) Periapical implant surgery.
-

- Fig. 4A

-

- Fig. 4B

-

- Fig. 4C

-
- Fig. 5
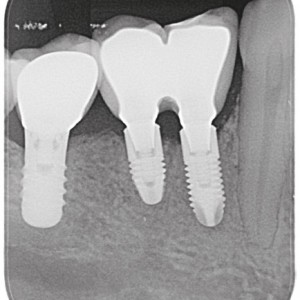
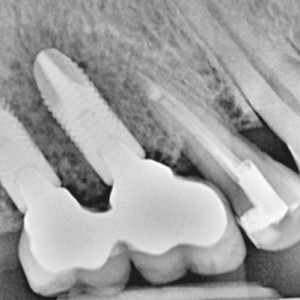
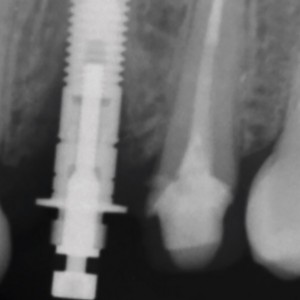
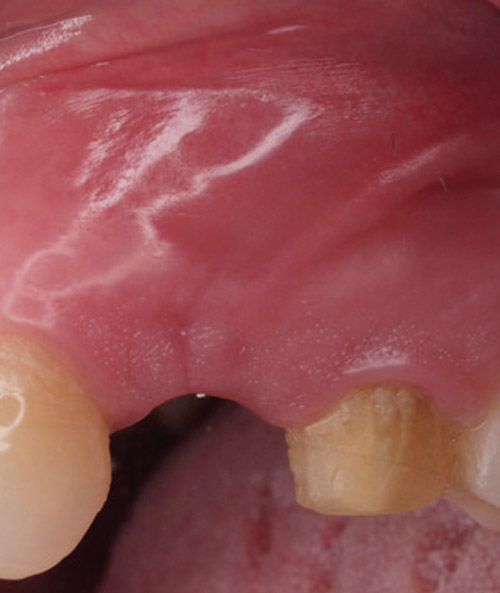
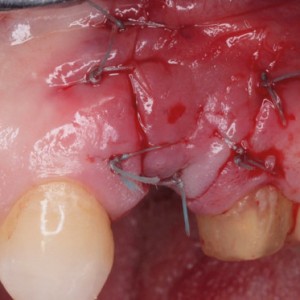
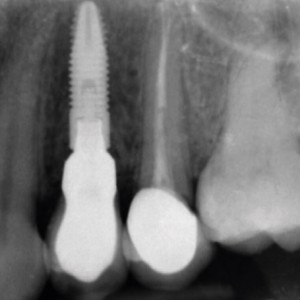
(A) Occlusal view at the 1-year follow-up. (B) Lateral view at the 1-year follow-up. (C) Periapical radiograph at the 1-year follow-up.
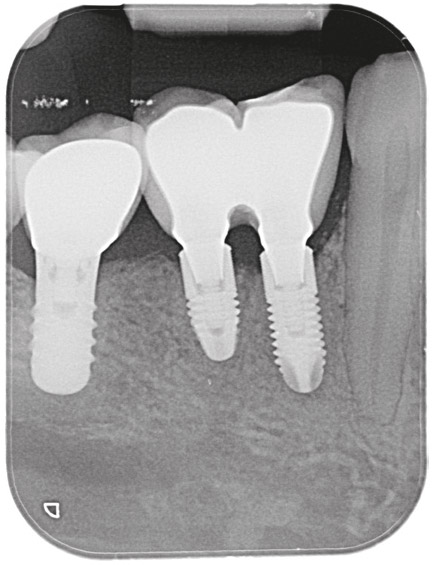
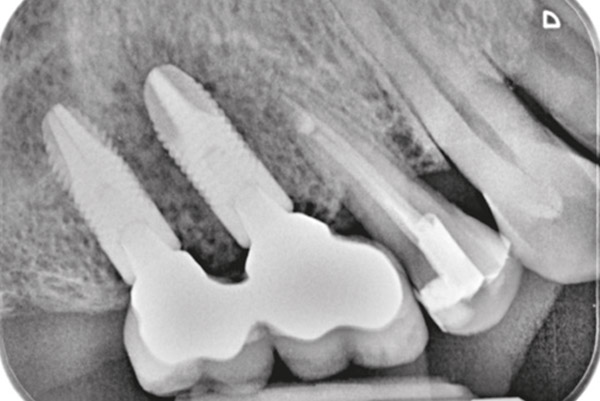
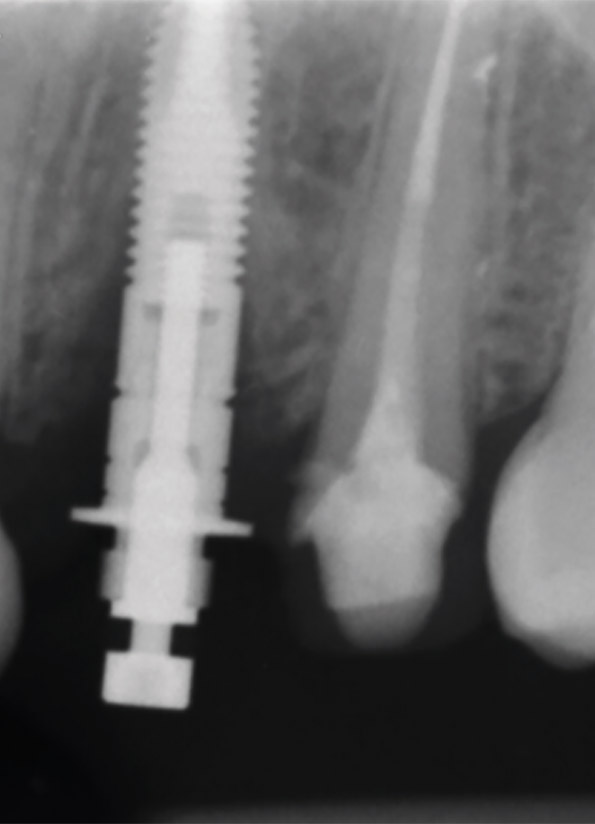
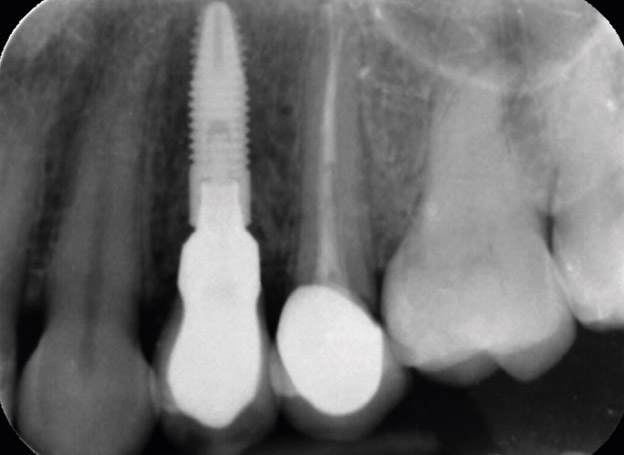
Periapical radiograph at the 3-year follow-up.
Case 1
The 48-year-old female patient, who was allergic to acetylsalicylic acid, reported discomfort in the area of teeth #44 and 45. After periapical radiographic and periodontal probing, it was decided to perform extractions, curettage of the apical granulation tissue and alveolar preservation of teeth #44 and 45 (Fig. 1).
After 3 months, 2 Ticare implants (Mozo Grau; 4.2 × 8.0 mm and 4.2 × 11.5 mm) were placed (Fig. 2). After 15 days, the patient returned for a check and reported discomfort and swelling in the vestibular area of the implant placed in position #44; a radiolucency was observed radiographically at the apex of the implant. The lesion was diagnosed as in the acute suppurative stage. A surgical approach was performed to access the lesion, curette the granulation tissue and irrigate with sterile saline (Fig. 3). After the osseointegration period, the implant and tissue healing were monitored. At 1- and 3-year follow-up, the treated implant remained functional for prosthetic support, maintaining bone integration (Figs. 4 & 5).
Case 2
The 53-year-old female patient had no relevant medical history. Rehabilitation of the edentulous area of the right maxilla was evaluated. Two Ticare implants of 4.2 × 11.5 mm were placed in positions #15 and 16 (Fig. 6).
After 16 days of surgery, the patient reported pain. A radiolucency was observed at the apex of implant #15 and tooth #14 on a periapical radiograph (Fig. 7). Endodontic treatment of tooth #14 was performed owing to a negative vitality test. It was diagnosed as an acute suppurative stage lesion. The surgical approach entailed raising a flap to full thickness, with 2 objectives: accessing the apex of the implant to remove granulation tissue and pus, and performing periapical surgery on the adjacent tooth. The retrograde cavity was performed for its subsequent sealing with mineral trioxide aggregate (Dentsply Tulsa Dental), and it was evaluated with the endoscope. After irrigation with sterile saline, it was checked again with the endoscope that the bony crypt was clean. Owing to the ostectomy for surgical access, the marginal bone defect was extensive and a collagen sponge was placed to avoid the collapse of the soft tissue during the healing period. After suturing, a postoperative periapical radiograph was performed (Fig. 7).
After 3 months, the healing abutments were placed in the second surgical phase to rehabilitate them prosthetically (Fig. 8). After 6 years, the implant and the treated tooth presented stable clinical parameters (Fig. 9).
-
- Fig. 6A
-

- Fig. 6B

-

- Fig. 6C
-
- Fig. 6D
(A) Radiograph of the edentulous area of positions #15 and 16. (B) Occlusal view of the edentulous area. (C) Implant placement into positions #15 and 16. (D) Periapical radiograph after implant placement.
-

- Fig. 7A

-

- Fig. 7B
-
- Fig. 7C
-
- Fig. 7D
-

- Fig. 7E
-

- Fig. 7F

-

- Fig. 7G

-
- Fig. 7H
-
- Fig. 7I

(A) Radiolucent lesion around implant #15 and tooth #14. (B) A flap was raised through trapezoidal incision. Appreciation of pus in the apical area. (C) Visible bone defect after pus drainage. (D) An ostectomy was performed to access the apical portion of the implant and the tooth. (E) An endoscope was used to confirm the correct removal of the granulation tissue. (F) Evaluation of the apical seal after periapical surgery of tooth #14. (G) A collagen sponge was used to avoid soft-tissue collapse. (H) Closure of the flap with interrupted sutures. (I) ostoperative periapical radiograph.
-

- Fig. 8A

-

- Fig. 8B

-
- Fig. 8C
(A) Lateral view of the prosthetic restoration. (B) Occlusal view of the prosthetic restoration. (C) Periapical radiograph after prosthetic restoration.
Case 3
The 43-year-old female patient smoked 2 cigarettes per day. She had a coronal fracture of tooth #24 that had previously been endodontically treated. Tooth #25 was assessed and referred for root canal therapy prior to surgery. After careful extraction of the root, an implant (Ticare, 4.2 × 11.5 mm) was immediately placed in position #24 (Fig. 10).
Twenty days after implant placement, the patient came to the clinic owing to discomfort in the area. The radiograph showed a radiolucency apical and lateral to the implant. It was diagnosed as an acute suppurative periapical implant lesion. After raising the mucoperiosteal flap, it was found that the lesion had perforated the buccal bone. An ostectomy was performed and the granulation tissue was removed. Once the bony crypt had been cleaned, the stability of the implant was assessed, and owing to its mobility, it was placed more apically to stabilize it. After suturing, a postoperative control radiograph was performed (Fig. 11).
During the first year, healing of the soft and hard tissue was monitored (Fig. 12). At 4 years, the implant was still functional (Fig. 13).
Discussion
The literature describes the diagnosis of periapical implant lesions as occurring between 7 and 16 days after implant placement.32Zhou W, Han C, Li D, Li Y, Song Y, Zhao Y. Endodontic treatment of teeth induces retrograde peri-implantitis. → Clin Oral Implants Res. 2009 Dec;20(12):1326–32.,33Peñarrocha-Diago M, Maestre-Ferrín L, Peñarrocha-Oltra D, Canullo L, Piattelli A, Peñarrocha-Diago M. Inflammatory implant periapical lesion prior to osseointegration: a case series study. → Int J Oral Maxillofac Implants. 2013 Jan–Feb;28(1):158–62.,34Ataullah K, Chee LF, Peng LL, Lung HH. Management of retrograde peri-implantitis: a clinical case report. → J Oral Implantol. 2006 Dec;32(6):308–12. Two of the treated cases were diagnosed within this period, and 1 after 20 days. The early diagnosis of periapical implant lesions during the osseointegration phase and early surgical treatment will lead to a higher survival rate of implants treated, hence preventing the need for implant extraction.35Peñarrocha-Diago M, Peñarrocha-Diago M, Blaya-Tárraga JA. State of the art and clinical recommendations in periapical implant lesions. 9th Mozo-Grau Ticare Conference in Quintanilla, Spain. → J Clin Exp Dent. 2017 Mar 1;9(3):e471–3. doi: 10.4317/ jced.53600.
-

- Fig. 9

-
- Fig. 10A

-

- Fig. 10B

-

- Fig. 10C

-
- Fig. 10D
Periapical radiograph at the 6-year follow-up.
(A) Periapical radiograph showing coronal fracture of tooth #24. (B) Occlusal view of tooth #24. (C) Occlusal view after extraction and immediate implant placement. (D) Periapical radiograph after implant placement.
-

- Fig. 11A

-

- Fig. 11B
-

- Fig. 11C

-

- Fig. 11D
-
- Fig. 11E
-
- Fig. 11F

-

- Fig. 11G

(A) Radiolucency apical and lateral to implant #24. (B) Clinical view of swollen tissue. (C) Raising of the mucoperiosteal flap. (D) Assessment of the stability of the implant. (E) Apical repositioning of the implant to stabilize it. (F) Interrupted sutures were used to close the flap. (G) Postoperative periapical radiograph.
The etiologies of the cases were diverse. In the first case presented, the tooth to be replaced had an endodontic apical lesion. After its extraction and despite the curettage of the alveolus and delayed placement of the implant, the surrounding tissue remained contaminated, favoring the development of a periapical implant lesion. Several authors have described similar conditions after implant placement in locations where the tooth being replaced had a periapical lesion.36Reiser GM, Nevins M. The implant periapical lesion: etiology, prevention, and treatment. → Compend Contin Educ Dent. 1995 Aug;16(8):768, 770, 772 passim.,37Chaffee NR, Lowden K, Tiffee JC, Cooper LF. Periapical abscess formation and resolution adjacent to dental implants: a clinical report. → J Prosthet Dent. 2001 Feb;85(2):109–12.,38Oh TJ, Yoon J, Wang HL. Management of the implant periapical lesion: a case report. → Implant Dent. 2003 Mar;12(1):41–6.
In the second case, the implant was placed in mature bone. The source of contamination came from the adjacent tooth that previously did not present symptoms. The infectious process involved tooth and implant, and after the removal of the granulation tissue, its relation to the bony crypt was observed with the endoscope. Similar cases have been reported,39Zhou W, Han C, Li D, Li Y, Song Y, Zhao Y. Endodontic treatment of teeth induces retrograde peri-implantitis. → Clin Oral Implants Res. 2009 Dec;20(12):1326–32.,40Brisman DL, Brisman AS, Moses MS. Implant failures associated with asymptomatic endodontically treated teeth. → J Am Dent Assoc. 2001 Feb;132(2):191–5.,41Temmerman A, Lefever D, Teughels W, Balshi TJ, Balshi SF, Quirynen M. Etiology and treatment of periapical lesions around dental implants. → Periodontol 2000. 2014 Oct;66(1):247–54. although these were cases with the adjacent tooth endodontically treated; in this case, the adjacent tooth was vital before implant placement.
In the last case presented, the implant was placed immediately after the extraction of an endodontically treated tooth. Despite the curettage and abundant irrigation after the extraction, it is possible that there were epithelial remains that favored the development of a periapical implant lesion. Zhao et al. in a meta-analysis suggested that immediate placing of a dental implant into an infected site may increase the risk of implant failure.42Zhao D, Wu Y, Xu C, Zhang F. Immediate dental implant placement into infected vs. non-infected sockets: a meta-analysis. → Clin Oral Implants Res. 2016 Oct;27(10):1290–6.
Various therapeutic alternatives have been proposed to restore the osseointegration process in implants affected by periapical implant lesions. Curettage,43Peñarrocha-Diago M, Boronat-Lopez A, García-Mira B. Inflammatory implant periapical lesion: etiology, diagnosis, and treatment—presentation of 7 cases. → J Oral Maxillofac Surg. 2009 Jan;67(1):168–73.,44Ayangco L, Sheridan PJ. Development and treatment of retrograde peri-implantitis involving a site with a history of failed endodontic and apicoectomy procedures: a series of reports. → Int J Oral Maxillofac Implants. 2001 May–Jun;16(3):412–7.,45Dahlin C, Nikfarid H, Alsén B, Kashani H. Apical peri-implantitis: possible predisposing factors, case reports, and surgical treatment suggestions. → Clin Implant Dent Relat Res. 2009 Sep;11(3):222–7. irrigation with sterile saline46McAllister BS, Masters D, Meffert RM. Treatment of implants demonstrating periapical radiolucencies. → Pract Periodontics Aesthet Dent. 1992 Nov–Dec;4(9):37–41.,47Peñarrocha-Diago M, Boronat-Lopez A, García-Mira B. Inflammatory implant periapical lesion: etiology, diagnosis, and treatment—presentation of 7 cases. → J Oral Maxillofac Surg. 2009 Jan;67(1):168–73.,48Piattelli A, Scarano A, Balleri P, Favero GA. Clinical and histologic evaluation of an active “implant periapical lesion”: a case report. → Int J Oral Maxillofac Implants. 1998 Sep–Oct;13(5):713–6. or chlorhexidine,7 topical decontamination of the implant surface with calcium hydroxide paste49Flanagan D. Calcium hydroxide paste as a surface detoxifying agent for infected dental implants: two case reports. → J Oral Implantol. 2009 Aug;35(4):204–9. or tetracycline paste,50Zhou W, Han C, Li D, Li Y, Song Y, Zhao Y. Endodontic treatment of teeth induces retrograde peri-implantitis. → Clin Oral Implants Res. 2009 Dec;20(12):1326–32.,51Ayangco L, Sheridan PJ. Development and treatment of retrograde peri-implantitis involving a site with a history of failed endodontic and apicoectomy procedures: a series of reports. → Int J Oral Maxillofac Implants. 2001 May–Jun;16(3):412–7.,52Piattelli A, Scarano A, Balleri P, Favero GA. Clinical and histologic evaluation of an active “implant periapical lesion”: a case report. → Int J Oral Maxillofac Implants. 1998 Sep–Oct;13(5):713–6. and guided bone regeneration53Quirynen M, Vogels R, Alsaadi G, Naert I, Jacobs R, van Steenberghe D. Predisposing conditions for retrograde peri-implantitis, and treatment suggestions. → Clin Oral Implants Res. 2005 Oct;16(5):599–608.,54Tözüm TF, Sençimen M, Ortakoğlu K, Ozdemir A, Aydin OC, Keleş M. Diagnosis and treatment of a large periapical implant lesion associated with adjacent natural tooth: a case report. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Jun;101(6):e132–8. doi: 10.1016/j.tripleo.2005.11.029. have been described, but there is no evidence of the efficacy of any of them. Further studies with larger patient samples are needed to expand knowledge about this lesion.
Conclusion
Up to 6 years of clinical and radiographic controls, all 3 cases showed complete healing of soft and hard tissue. Diagnosis and early treatment are crucial to ensure a correct osseointegration process and avoid implant failure.
Competing interests
The authors have no conflicts of interest related to this study.
-

- Fig. 12A

-
- Fig. 12B

-
- Fig. 12C
-
- Fig. 13
(A) Frontal view at the 1-year follow-up. (B) Lateral view at the 1-year follow-up. (C) Periapical radiograph at the 1-year follow-up.
Periapical radiograph at the 4-year follow-up.
Interview
Juan Antonio Blaya Tárraga
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 14, 46. | ↑ | McAllister BS, Masters D, Meffert RM. Treatment of implants demonstrating periapical radiolucencies. → Pract Periodontics Aesthet Dent. 1992 Nov–Dec;4(9):37–41. |
| 2. | ↑ | Sussman HI, Moss SS. Localized osteomyelitis secondary to endodontic- implant pathosis. A case report. → J Periodontol. 1993 Apr;64(4):306–10. |
| 3, 31, 35. | ↑ | Peñarrocha-Diago M, Peñarrocha-Diago M, Blaya-Tárraga JA. State of the art and clinical recommendations in periapical implant lesions. 9th Mozo-Grau Ticare Conference in Quintanilla, Spain. → J Clin Exp Dent. 2017 Mar 1;9(3):e471–3. doi: 10.4317/ jced.53600. |
| 4, 15, 53. | ↑ | Quirynen M, Vogels R, Alsaadi G, Naert I, Jacobs R, van Steenberghe D. Predisposing conditions for retrograde peri-implantitis, and treatment suggestions. → Clin Oral Implants Res. 2005 Oct;16(5):599–608. |
| 5, 8, 16, 36. | ↑ | Reiser GM, Nevins M. The implant periapical lesion: etiology, prevention, and treatment. → Compend Contin Educ Dent. 1995 Aug;16(8):768, 770, 772 passim. |
| 6, 9, 17, 43, 47. | ↑ | Peñarrocha-Diago M, Boronat-Lopez A, García-Mira B. Inflammatory implant periapical lesion: etiology, diagnosis, and treatment—presentation of 7 cases. → J Oral Maxillofac Surg. 2009 Jan;67(1):168–73. |
| 7, 10, 32, 39, 50. | ↑ | Zhou W, Han C, Li D, Li Y, Song Y, Zhao Y. Endodontic treatment of teeth induces retrograde peri-implantitis. → Clin Oral Implants Res. 2009 Dec;20(12):1326–32. |
| 11, 40. | ↑ | Brisman DL, Brisman AS, Moses MS. Implant failures associated with asymptomatic endodontically treated teeth. → J Am Dent Assoc. 2001 Feb;132(2):191–5. |
| 12, 41. | ↑ | Temmerman A, Lefever D, Teughels W, Balshi TJ, Balshi SF, Quirynen M. Etiology and treatment of periapical lesions around dental implants. → Periodontol 2000. 2014 Oct;66(1):247–54. |
| 13. | ↑ | Lefever D, Van Assche N, Temmerman A, Teughels W, Quirynen M. Aetiology, microbiology and therapy of periapical lesions around oral implants: a retrospective analysis. → J Clin Periodontol. 2013 Mar;40(3):296–302. |
| 18, 22. | ↑ | Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. → Eur J Oral Sci. 1998 Feb;106(1):527–51. |
| 19, 37. | ↑ | Chaffee NR, Lowden K, Tiffee JC, Cooper LF. Periapical abscess formation and resolution adjacent to dental implants: a clinical report. → J Prosthet Dent. 2001 Feb;85(2):109–12. |
| 20, 38. | ↑ | Oh TJ, Yoon J, Wang HL. Management of the implant periapical lesion: a case report. → Implant Dent. 2003 Mar;12(1):41–6. |
| 21. | ↑ | Scarano A, Di Domizio P, Petrone G, Iezzi G, Piattelli A. Implant periapical lesion: a clinical and histologic case report. → J Oral Implantol. 2000 Apr;26(2):109–13. |
| 23, 44, 51. | ↑ | Ayangco L, Sheridan PJ. Development and treatment of retrograde peri-implantitis involving a site with a history of failed endodontic and apicoectomy procedures: a series of reports. → Int J Oral Maxillofac Implants. 2001 May–Jun;16(3):412–7. |
| 24. | ↑ | Esposito M, Hirsch J, Lekholm U, Thomsen P. Differential diagnosis and treatment strategies for biologic complications and failing oral implants: a review of the literature. → Int J Oral Maxillofac Implants. 1999 Jul–Aug;14(4):473–90. |
| 25, 33. | ↑ | Peñarrocha-Diago M, Maestre-Ferrín L, Peñarrocha-Oltra D, Canullo L, Piattelli A, Peñarrocha-Diago M. Inflammatory implant periapical lesion prior to osseointegration: a case series study. → Int J Oral Maxillofac Implants. 2013 Jan–Feb;28(1):158–62. |
| 26, 30. | ↑ | Peñarrocha-Diago M, Maestre-Ferrín L, Cervera-Ballester J, Peñarrocha-Oltra D. Implant periapical lesion: diagnosis and treatment. → Med Oral Patol Oral Cir Bucal. 2012 Nov 1;17(6):e1023–7. doi: 10.4317/ medoral.17996. |
| 27, 29. | ↑ | Blaya-Tárraga JA, Cervera-Ballester J, Peñarrocha-Oltra D, Peñarrocha-Diago M. Periapical implant lesion: a systematic review. → Med Oral Patol Oral Cir Bucal. 2017 Nov 1;22(6):e737–49. doi: 10.4317/ medoral.21698. |
| 28. | ↑ | Romanos GE, Froum S, Costa-Martins S, Meitner S, Tarnow DP. Implant periapical lesions: etiology and treatment options. → J Oral Implantol. 2011 Feb;37(1):53–63. |
| 34. | ↑ | Ataullah K, Chee LF, Peng LL, Lung HH. Management of retrograde peri-implantitis: a clinical case report. → J Oral Implantol. 2006 Dec;32(6):308–12. |
| 42. | ↑ | Zhao D, Wu Y, Xu C, Zhang F. Immediate dental implant placement into infected vs. non-infected sockets: a meta-analysis. → Clin Oral Implants Res. 2016 Oct;27(10):1290–6. |
| 45. | ↑ | Dahlin C, Nikfarid H, Alsén B, Kashani H. Apical peri-implantitis: possible predisposing factors, case reports, and surgical treatment suggestions. → Clin Implant Dent Relat Res. 2009 Sep;11(3):222–7. |
| 48, 52. | ↑ | Piattelli A, Scarano A, Balleri P, Favero GA. Clinical and histologic evaluation of an active “implant periapical lesion”: a case report. → Int J Oral Maxillofac Implants. 1998 Sep–Oct;13(5):713–6. |
| 49. | ↑ | Flanagan D. Calcium hydroxide paste as a surface detoxifying agent for infected dental implants: two case reports. → J Oral Implantol. 2009 Aug;35(4):204–9. |
| 54. | ↑ | Tözüm TF, Sençimen M, Ortakoğlu K, Ozdemir A, Aydin OC, Keleş M. Diagnosis and treatment of a large periapical implant lesion associated with adjacent natural tooth: a case report. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Jun;101(6):e132–8. doi: 10.1016/j.tripleo.2005.11.029. |





Leave a Reply
Be the First to Comment!