Accuracy of computer-assisted templatebased implant placement using a conventional impression and scan model or digital impression: A preliminary report from a randomized controlled trial
September 18, 2017 / Categories: Digital Dentistry, Implant Dentistry

Tallarico, Marco

Xhanari, Erta

Schipani, Franco

Canullo, Luigi

Cocchi, Fabio

Meloni, Silvio Mario
Abstract
Objective
The objective of the present study was to evaluate bone–implant contact (BIC) in a new implant design after immediate and delayed placement at different levels in relation to crestal bone in American Foxhound dogs.
Materials and methods
The second, third and fourth mandibular premolars and first molars of 6 American Foxhound dogs were extracted bilaterally. At random, 4 immediate implants were placed in the hemimandibles of each dog in the crestal (control group) and subcrestal position (test group). Three dogs were allowed a healing period of 8 weeks; the other 3 had a healing period of 12 weeks. After the healing periods, histomorphometric analysis of the specimens was performed to measure BIC values and bone remodeling in crestal and subcrestal implants. Results All of the implants healed without incident and were available for histological analysis. Lower bone resorption was observed in the group of implants placed subcrestally in healed bone and immediately postextraction.
Conclusion
Our findings suggest that less resorption can be expected when implants are inserted 2 mm subcrestally overall for both immediate and deferred implants compared with placement at the crestal level. In addition, higher BIC values were found at 12 weeks of follow-up in the group of implants placed subcrestally in healed bone compared with those placed subcrestally immediately. Keywords Top DM, tapered implants, healed bone.
Introduction
Proper implant position has a significant impact on the esthetic and functional outcomes of implant-supported restorations.1Canullo L, Tallarico M, Radovanovic S, Delibasic B, Covani U, Rakic M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered peri-implantitis.
→ Clin Oral Implants Res. 2016 Oct;27(10):1243–50. Epub 2015 Nov 20.2Furhauser R, Mailath-Pokorny G, Haas R, Busenlechner D, Watzek G, Pommer B. Esthetics of flapless single-tooth implants in the anterior maxilla using guided surgery: association of three-dimensional accuracy and pink esthetic score.
→ Clin Implant Dent Relat Res. 2015 Oct;17 Suppl 2:e427–33. Epub 2014 Oct 27.
Therefore, the implant must be placed accurately according to the treatment plan. Computer-assisted template-based implant placement (guided surgery) has become increasingly popular owing to improved planning and the higher transfer accuracy of the virtual plan to the surgical site compared with freehand insertion or freehand final drilling.3Vermeulen J. The accuracy of implant placement by experienced surgeons: guided vs freehand approach in a simulated plastic model.
→ Int J Oral Maxillofac Implants. 2017 Mar/Apr;32(3):617–624. Epub 2016 Oct 14. Hence, it has undoubtedly been a major achievement to provide optimal 3-D implant positioning with respect to both anatomical and prosthetic parameters, as well as higher patient satisfaction.4Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial.
→ Eur J Oral Implantol. 2014 Autumn;7(3):229–42.
A recently published meta-analysis of in vitro and in vivo studies found a total mean error of 1.12 mm at the entry point and 1.39 mm at the apex.5Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: a systematic review.
→ Int J Oral Maxillofac Implants. 2014;29 Suppl:25–42. The accuracy of computer-assisted template-based implant placement depends on several factors, from data set acquisition to the surgical procedure. Originally, guided surgery protocols advocated a dual-scan protocol.6Van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, Wendelhag I. Computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicenter study.
→ Clin Implant Dent Relat Res. 2005;7 Suppl 1:111–20. In recent years, new technologies combining data from computed tomography (CT) or cone beam computed tomography (CBCT) images with information on the soft tissue and crown morphology have been developed. Dedicated software allows for accurate virtual implant planning, always based on the prosthetic volume of the teeth to be rehabilitated and making immediate loading easier.7Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial.
→ Eur J Oral Implantol. 2014 Autumn;7(3):229–42.8Polizzi G, Cantoni T, Pasini E, Tallarico M. Immediate loading of variable-thread expanding tapered-body implants placed into maxillary post-extraction or healed sites using a guided surgery approach: an up-to-five-year retrospective analysis.
→ J Oral Science Rehabilitation. 2016 Sep;2(3):50–60.9Meloni SM, Tallarico M, Pisano M, Xhanari E, Canullo L. Immediate loading of fixed complete denture prosthesis supported by 4-8 implants placed using guided surgery: a 5-year prospective study on 66 patients with 356 implants.
→ Clin Implant Dent Relat Res. 2017 Feb;19(1):195–206. Epub 2016 Sep 15.10Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. Five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery.
→ Clin Implant Dent Relat Res. 2016 Oct;18(5):965–72. Epub 2015 Oct 7. Surgical guides may be produced by computer-aided design/ computer-aided manufacture technology, such as stereolithography, manually in a dental laboratory or by high-resolution 3-D printer. Finally, irrespective of the method of manufacture, the optimal fit of the surgical template and its stabilization are essential to accurately transfer the virtual implant position to the patient’s mouth.
Digital impressions replace the need for conventional materials that can be inconvenient and messy for patients. Today, there is no doubt about the potential of recent intraoral optical impression systems available on the market as regards diagnosis and the treatment plan. Particularly noteworthy is the complete integration with other digital technologies to provide for accurate and faster patient-centered health solutions.11Chochlidakis KM, Papaspyridakos P, Geminiani A, Chen CJ, Feng IJ, Ercoli C. Digital versus conventional impressions for fixed prosthodontics: a systematic review and meta-analysis.
→ J Prosthet Dent. 2016 Aug;116(2):184–190.e12. Epub 2016 Mar 2.12Ahlholm P, Sipila K, Vallittu P, Jakonen M, Kotiranta U. Digital versus conventional impressions in fixed prosthodontics: a review.
→ J Prosthodont. 2016 Aug 2. doi:10.1111/jopr.12527. [Epub ahead of print] Nevertheless, to the best of our knowledge, at the time of writing this article, there were no other published randomized clinical trials evaluating a fully digital approach to computer-assisted template-based implant placement.
The aim of the present study was to compare implant survival rate, template-related complications and virtual planning accuracy of computer-assisted template-based implant placement using a conventional impression and scan model or digital impression. The null hypothesis was that there would be no difference between these interventions. This trial is reported in accordance with the CONSORT Statement for improving the quality of reporting of parallel-group randomized trials.13Tallarico M, Meloni SM. Open-cohort prospective study on early implant failure and physiological marginal remodeling expected using sandblasted and acid-etched bone level implants featuring an 11° Morse taper connection within one year after loading.
→ J Oral Science Rehabilitation. 2017 Mar;3(1):68–79.
Materials and methods
This study was designed as a randomized controlled trial of parallel-group design conducted at a private center in Rome, between May 2016 and March 2017. Surgical and prosthetic procedures were performed by one expert clinician (MT). To the best of our knowledge, at the time of writing this article, there were no other similar studies, not allowing for a true sample size calculation. Hence, it was decided to publish preliminary results with 12 patients.
Partially edentulous patient aged 18 years or older, able to sign an informed consent form and in need of an implant-supported fixed restoration was considered eligible for this study. Any potential implant locations based on individual patient requirements were considered eligible in the present trial. No set location or group of locations was excluded.
Patients were not admitted to the study if any of the following exclusion criteria were present: general medical contraindication to oral surgery (American Society of Anesthesiologists (ASA) Physical Status Class III or IV), irradiation of the head and neck area less than 1 year before implantation, psychiatric problems, alcohol or drug abuse, pregnant or nursing, untreated periodontitis, severe bruxism or clenching, uncontrolled diabetes, poor oral hygiene and motivation, and inability to complete the follow-up. The investigation was conducted according to the principles embodied in the Declaration of Helsinki of 1975 for biomedical research involving human subjects, as revised in 2008. All of the patients were informed about the nature of the treatment and their written consent was obtained. Data collection was designed to preserve patient anonymity.
All of the patients received preoperative photographs, periapical radiographs or panoramic radiographs for initial screening and evaluation. The prosthetic-driven planning workflow started with taking a CBCT scan (CRANEX 3Dx, SOREDEX, Tuusula, Finland) of the enrolled patient, using a wax bite to separate the dental arches. The next step was to create a digital model, accomplished in two ways: the clinician used an intraoral scanner to create a digital impression (Fig. 1), or the clinician took a conventional impression and then scanned the impression using an extraoral scanner (Fig. 2). Patients were randomly assigned to undergo intraoral digital impressions (fully digital group) or conventional impressions (control group). In the fully digital group, a digital impression was taken using a CS 3600 intraoral scanner (Carestream Dental, Atlanta, Ga., U.S.). The digital data (STL interface format) were imported into 3-D design software (exocad DentalCAD, exocad, Darmstadt, Germany) to realize a virtual wax-up according to the functional and esthetic requirements. In the control group, a polyether impression (Impregum, 3M ESPE, Seefeld, Germany) was taken with a customized tray (Diatray Top, Dental Kontor, Stockelsdorf, Germany). The impressions were poured with Type IV Gypsum (T6, Techim Group, Arese, Italy) and then the models were mounted in a fully adjustable articulator (PROTARevo 7, KaVo Dental, Biberach, Germany). Afterward, a dental wax-up was produced according to the functional and esthetic requirements. Finally, the master cast and wax-up were digitalized using a laboratory scanner (Sinergia-Scan, Version 2016 Plus, Nobil-Metal, Villafranca d’Asti, Italy).
-

- Fig. 1
-
- Fig. 2
Fig. 1
Intraoral digital impressionin the fully digital group.
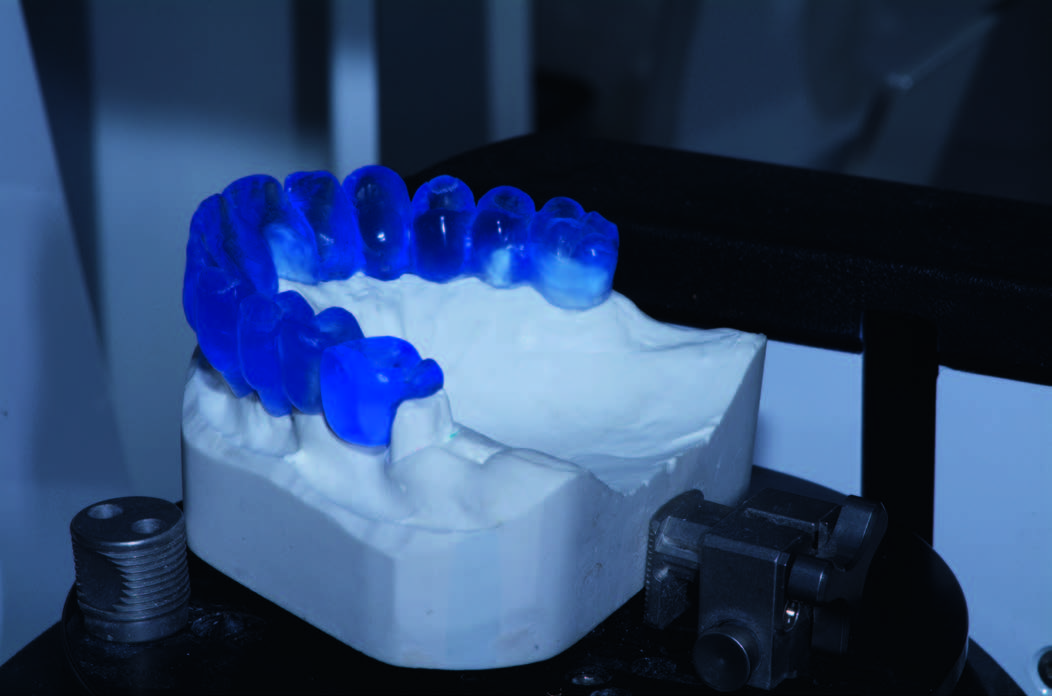
Fig. 2
Conventional impression, wax-up and scan model in the control group.
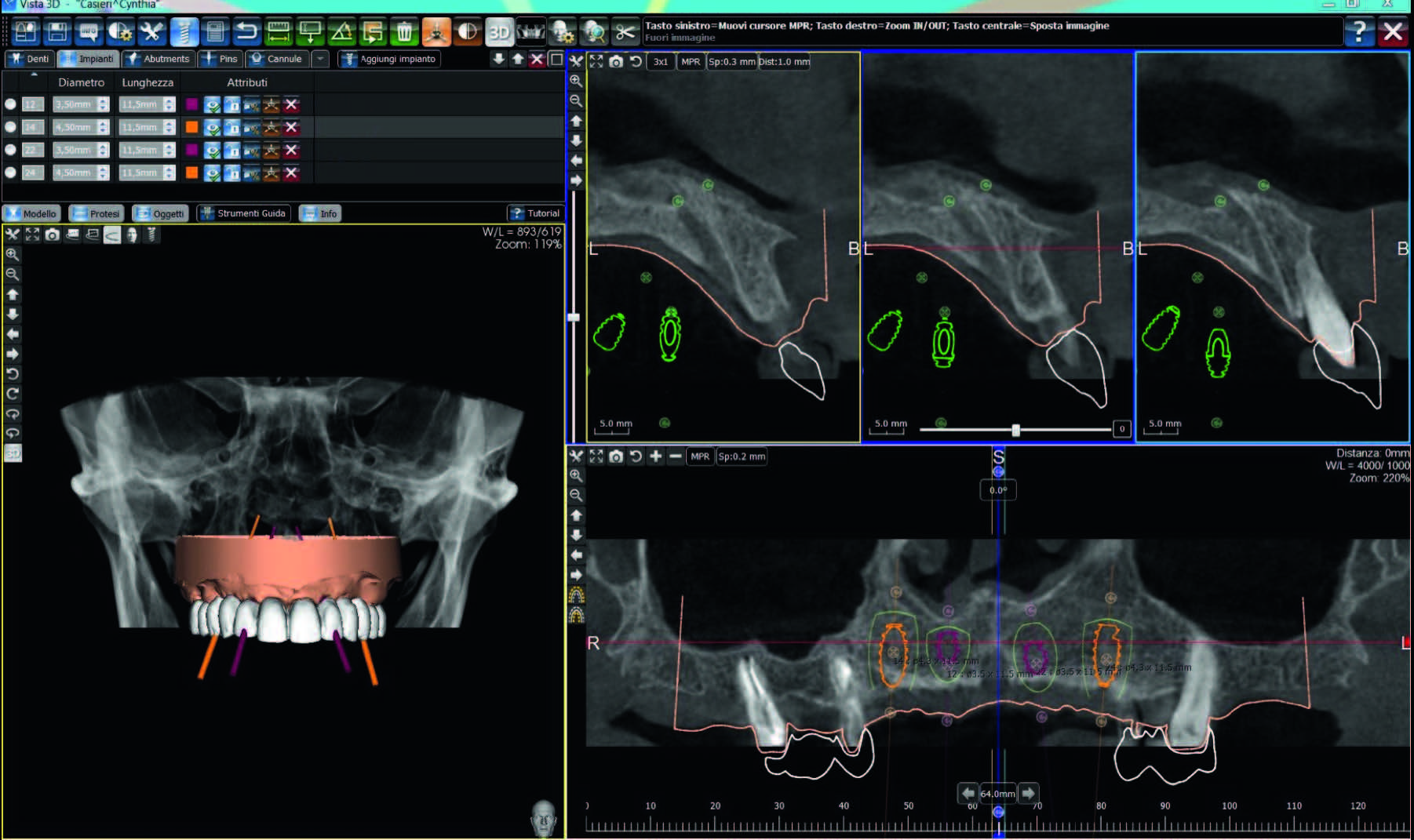
Fig. 3
Merging of CBCT, DICOM and STL files. Frontal and cross-sectional views of virtual implant planning used to create the surgical templates.
In both groups, the STL and DICOM data were imported into a 3-D software planning program (3Diagnosys, Version 4.2, 3DIEMME, Cantù, Italy). Then, the reprocessed surface extrapolated from the DICOM data (using a Hounsfield scale filter) and the surface generated by the master cast scanning process or by the intraoral scanning process were merged using the software’s best-fitting repositioning tools. At this point, the size and location of prosthetic- driven implants/abutments were planned, taking into account the bone quality/ quantity, soft-tissue thickness, anatomical landmarks, and the type, volume and shape of the final restoration (Fig. 3). After careful functional and esthetic evaluation and final verification, the prosthetic-driven plan was approved, and a stereolithographic surgical template was fabricated with a newer rapid prototyping technology (New Ancorvis, Bologna, Italy).
-
- Fig. 3
One hour before implant placement, all of the patients underwent professional oral hygiene, used a prophylactic antiseptic containing 0.2% chlorhexidine (CURASEPT, Curaden Healthcare, Saronno, Italy) for 1 min and received prophylactic antibiotic therapy (2 g of amoxicillin or 600 mg of clindamycin if allergic to penicillin). In the control group, the accurate fit of the surgical templates was tried on the master model and tested in the patient’s mouth, while in the fully guided group, the fit of the surgical template was tried directly in the patient’s mouth to fit (Fit Checker, GC, Tokyo, Japan). All of the patients were treated under local anesthesia using articaine with 1:100,000 epinephrine, administered 20 min before surgery. The surgical template was stabilized in relation to the opposing arch using a silicone surgical index, derived from the mounted casts (control group) or from the virtual plane (fully guided group), and two to four preplanned anchor pins.
Hopeless teeth were extracted after implant placement in order to improve the stability of the surgical template and to align the pre- and post-surgical scans. In the case of immediate post-extractive implants, residual teeth were extracted as atraumatically as possible immediately before surgery. Residual gaps were filled using a synthetic hydroxyapatite enriched with magnesium (SINTlife, Finceramica, Faenza, Italy) or with beta-tricalcium phosphate (Q-Oss+, Osstem, Seoul, South Korea). Sinus lift procedures were performed using minimally invasive transcrestal sinus floor elevation (Crestal Approach Sinus KIT, CAS-KIT, Osstem).14Tallarico M, Meloni SM. Open-cohort prospective study on early implant failure and physiological marginal remodeling expected using sandblasted and acid-etched bone level implants featuring an 11° Morse taper connection within one year after loading.
→ J Oral Science Rehabilitation. 2017 Mar;3(1):68–79. The bone graft material was based on autogenous bone collected at the implant site, combined with a synthetic hydroxyapatite enriched with magnesium (SINTlife) or with beta-tricalcium phosphate (Q-Oss+).
Planned implants (Osstem TSIII, Osstem) were placed flapless or with a minimally invasive flap using dedicate drills (OsstemGuide Kit [Taper], Osstem), according to a fully guided protocol. Implant sites were prepared based on the bone density evaluated by the surgeon at the first drilling. In the case of poor bone density, the implant site was underprepared.15Tallarico M, Meloni SM. Open-cohort prospective study on early implant failure and physiological marginal remodeling expected using sandblasted and acid-etched bone level implants featuring an 11° Morse taper connection within one year after loading.
→ J Oral Science Rehabilitation. 2017 Mar;3(1):68–79. All of the implants were inserted with a minimum insertion torque of 35 Ncm and were immediately loaded at implant or abutment level. Any flaps were then sutured with Vicryl 4-0 sutures (Ethicon J&J International, Sint-Stevens- Woluwe, Belgium). The prefabricated temporary acrylic restorations were trimmed and polished chairside. Single restorations received a nonoccluding occlusal scheme. Multiple-unit implant-supported temporary restorations were splinted together and reinforced using a metal framework.
Immediately after implant placement, patients of both groups received a digital impression (CS 3600), taken at implant level using dedicate abutments (Type AQ scan body, New Ancorvis), to check the position of the placed implants. Afterwards, all of the patients received oral and written recommendations about medication, oral hygiene maintenance and diet. Any sutures were removed 10–14 days later, after local cleaning using an antiseptic agent (0.2% chlorhexidine, CURASEPT). Patients were followed monthly for up to one year after implant placement (Figs. 4 & 5).
-

- Fig. 4
-

- Fig. 5
Fig. 4
Dental panoramic tomogram taken 1 year after loading.
Fig. 5
Frontal photograph taken 1 year after loading.
Outcome measurements
- Early implant failure: An implant was considered to be a failure if it was lost owing to mobility, implant fracture and/or any infection requiring implant removal. The stability of each implant was measured manually with a torque of 25 N cm at delivery of the final restoration and later with the prosthesis removed, if needed (infection, extensive periapical bone loss, mucosal inflammation).
- Template-related complications: limited access in posterior areas; buccal bony dehiscence (due to a mismatch of the surgical template), evaluated by sounding the implant site with a periodontal probe (PCPUNC156, Hu-Friedy Italy, Milan, Italy) before implant placement; insertion of a different implant than planned and fracture of the surgical template. All of the complications were recorded during follow-up by the same clinician (MT), who performed all of the surgical procedures.
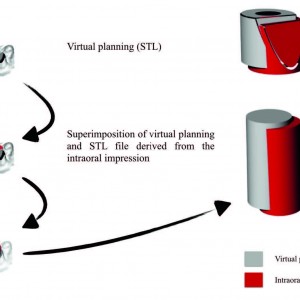
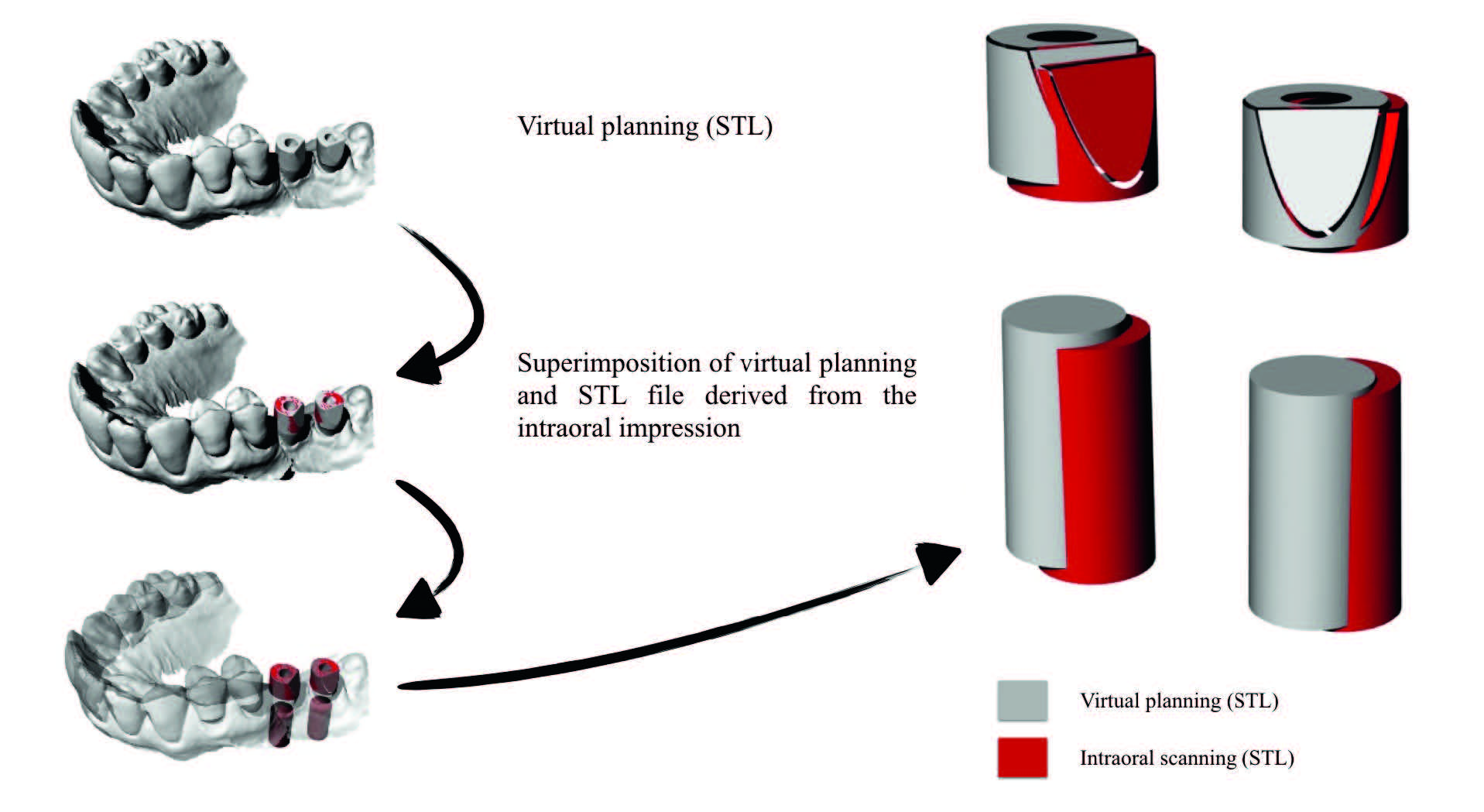
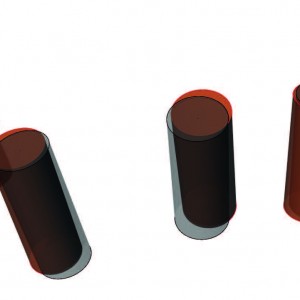
- Accuracy: Three deviation parameters (horizontal, vertical and angular) were defined and calculated between the planned and placed implant positions (Fig. 6). The postoperative STL file, derived from the intraoral scan (Fig. 7), was geometrically aligned with the files exported from the planning, by automated image registration using maximization of mutual information (Dental SCAN, Version 6, Open Technologies, Brescia, Italy; Figs. 8 & 9). The horizontal (lateral), vertical (depth) and angular deviations between virtual and placed implants was calculated along the long axis of each implant. An expert engineer (FC) performed all of the measurements.
-
- Fig. 6

-
- Fig. 7

-
- Fig. 8
-
- Fig. 9
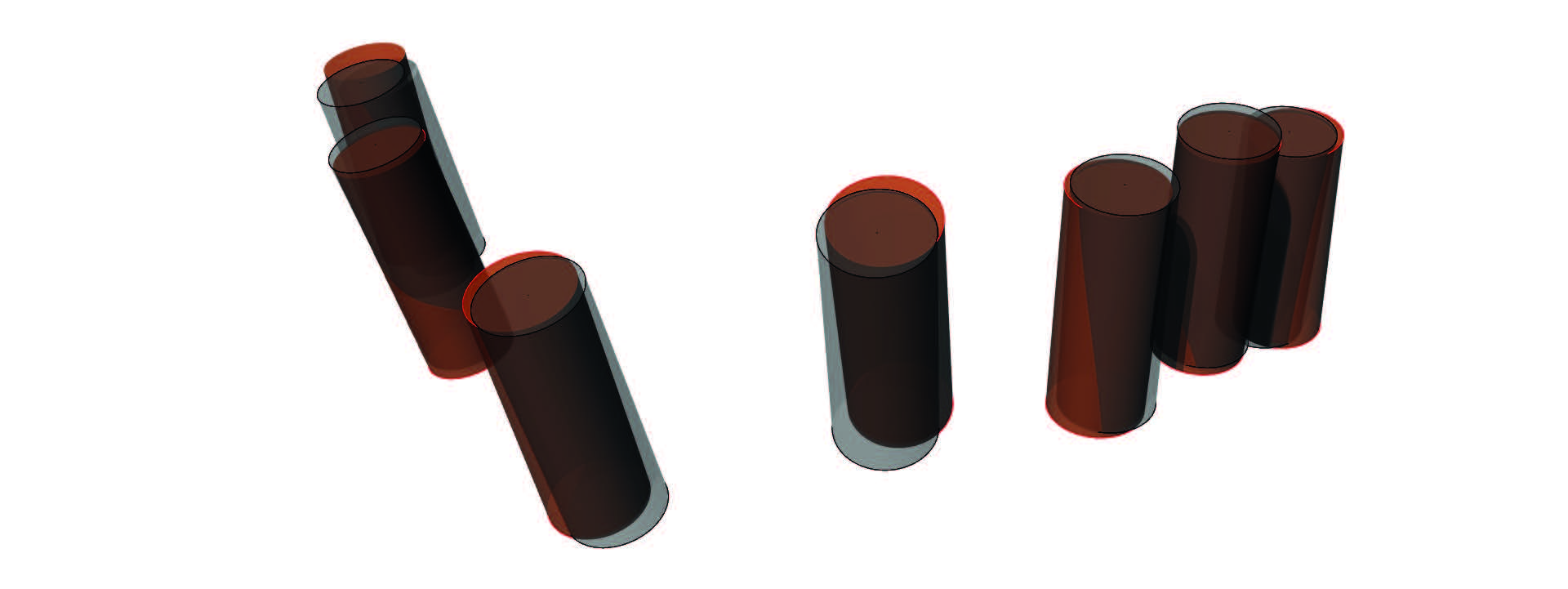
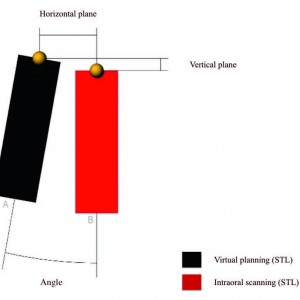
Fig. 6
Schematic diagram of the measurement of deviations between planned and placed implants.
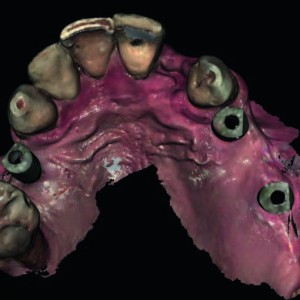
Fig. 7
Postoperative intraoral digital impression.
Fig. 8
Schematic diagram of the superimposition of virtual planning (gray) and the STL file derived from the intraoral impression (red).
Fig. 9
Three-dimensional superimposition of planned and placed implants.
Randomization
One computer-generated restricted randomization list was created. Only one of the investigators, not involved in the selection and treatment of the patients, was aware of the randomization sequence and had access to the randomization lists stored in a password-protected portable computer. The random codes were enclosed in sequentially numbered, identical, opaque sealed envelopes. Envelopes were opened sequentially after eligible patients signed the informed consent forms; therefore, treatment allocation was concealed from the investigators in charge of enrolling and treating the patients.
Statistical analysis
Patient data were collected in a Numbers spreadsheet (Version 3.6.1 for Mac OS X 10.11.4). A biostatistician with expertise in dentistry analyzed the data using SPSS software (IBM SPSS Statistics for Macintosh, Version 22.0, IBM, Armonk, N.Y., U.S.) for statistical analysis. Descriptive analysis was performed for numeric parameters using mean ± standard deviation and median with a 95% confidence interval. Template-related complications between the two groups were compared using the Fisher exact probability test. The mean differences in the overall deviation in the clinical outcomes compared with the virtual plan were compared between groups using a mixed-design repeated-measures analysis of variance model. All statistical comparisons were conducted with a P value set at 0.05.
Results
Preliminary data from the 12 patients were included in the present study. Patients were randomized to the fully digital group (6 patients with 17 implants) and control group (6 patients with 20 implants). All of the implants were inserted according to the manufacturer’s instructions, with an insertion torque ranging between 35 and 45 N cm. Overall, the analysis of the final accuracy found a total mean error of 2.34 ± 1.44° (range: 0.3–5.8°) in angle, 0.49 ± 0.29 mm (range: 0.1–1.1 mm) in the horizontal plane (mesiodistal) and 0.53 ± 0.42 mm (range: 0.0–1.6 mm) in the vertical plane (apico-coronal). All the measurements were within the safety margins of the software. In all the three measures, there were no statistically significant differences between fully digital and conventional impressions. The mean error in angle was 2.56 ± 1.52° (range: 0.3–5.0°) in the fully digital group and 2.18 ± 1.41° (range: 0.3– 5.8°) in the control group (P = 0.519). In the horizontal plane (mesiodistal), the mean error was 0.57 ± 0.32 mm (range: 0.1–1.1 mm) in the fully digital group and 0.43 ± 0.26 mm (range: 0.1– 0.9 mm) in the control group (P = 0.249). In the vertical plane (apico-coronal), the mean error was 0.67 ± 0.51 mm (range: 0.0–1.6 mm) in the fully digital group and 0.43 ± 0.32 mm (range: 0.0–1.2 mm) in the control group (P = 0.180).
Discussion
This randomized controlled trial was conducted with the aim of understanding which procedure is preferable, a conventional impression and a scan model or a digital impression, to rehabilitate partially edentulous patients using computer-assisted template-based implant placement. Implants were placed flapless or with a minimally invasive flap and when possible loaded immediately. Both techniques achieved successful results, and no statistically significant differences were observed regarding early implant failure, template-related complications or virtual planning accuracy.
To the best of our knowledge, at the time of writing this article, there were no other published randomized clinical trials comparing conventional impressions and scan models to digital impressions to plan and rehabilitate partially edentulous patients using computer-assisted template-based implant placement. This made it difficult to evaluate the results of the present study against comparable studies.
The scientific evidence available concluded that, regarding implant survival rate, guided surgery has no obvious differences compared with the conventional protocols.16Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial.
→ Eur J Oral Implantol. 2014 Autumn;7(3):229–42. However, according to D’haese et al., the most frequent surgical and mechanical complications are recognized to be specifically associated with computer-guided template-assisted surgery, including misfit of the surgical guide, fracture of the complete acrylic denture and misfit of the suprastructure.17D’haese J, Van De Velde T, Komiyama A, Hultin M, De Bruyn H. Accuracy and complications using computer-designed stereolithographic surgical guides for oral rehabilitation by means of dental implants: a review of the literature.
→ Clin Implant Dent Relat Res. 2012 Jun;14(3):321–35. Epub 2010 May In the present study, no implant failed early and no templated-related complications were observed in either group.
Several independent uncontrolled prospective studies reported substantial deviations in 3-D directions between virtual planning and final implant position, as well as postsurgical complications. 18Komiyama A, Klinge B, Hultin M. Treatment outcome of immediately loaded implants installed in edentulous jaws following computer-assisted virtual treatment planning and flapless surgery.
→ Clin Oral Implants Res. 2008 Jul;19(7):677–85.19Merli M, Bernardelli F, Esposito M. Computer-guided flapless placement of immediately loaded dental implants in the edentulous maxilla: a pilot prospective case series.
→ Eur J Oral Implantol. 2008 Spring;1(1):61–9.20Johansson B, Friberg B, Nilson H. Digitally planned, immediately loaded dental implants with prefabricated prostheses in the reconstruction of edentulous maxillae: a 1-year prospective, multicenter study.
→ Clin Implant Dent Relat Res. 2009 Sep;11(3):194–200. Epub 2008 Sep 9. However, excellent clinical results have also been reported using this technique.21Meloni SM, Tallarico M, Pisano M, Xhanari E, Canullo G. Immediate loading of fixed complete denture prosthesis supported by 4-8 implants placed using guided surgery: a 5-year prospective study on 66 patients with 356 implants.
→ Clin Implant Dent Relat Res. 2017 Feb;19(1):195–206. Epub 2016 Sep22D’haese J, Van De Velde T, Komiyama A, Hultin M, De Bruyn H. Accuracy and complications using computer-designed stereolithographic surgical guides for oral rehabilitation by means of dental implants: a review of the literature.
→ Clin Implant Dent Relat Res. 2012 Jun;14(3):321–35. Epub 2010 May23Polizzi G, Cantoni T, Pasini E, Tallarico M. Immediate loading of variable-thread expanding tapered-body implants placed into maxillary post-extraction or healed sites using a guided surgery approach: an up-to-5-year retrospective analysis.
→ J Oral Science Rehabilitation. 2016 Sep;2(3):50–60.24Tallarico M, Canullo L, Pisano M, Penarrocha-Oltra D, Penarrocha-Oltra M, Meloni, SM. An up to 7-year retrospective analysis of biologic and technical complication with the All-on-4 concept.
→ J Oral Implantol. 2016 Jun;42(3):265–71. Epub 2015 Dec 11. Vasak et al. found a mean deviation of 0.43 mm (buccolingual), 0.46 mm (mesiodistal) and 0.53 mm (depth) at the level of the implant shoulder and of 0.70 mm (buccolingual), 0.63 mm (mesiodistal) and 0.52 mm (depth) at the apex level, respectively.25Vasak C, Watzak G, Gahleitner A, Strbac G, Schemper M, Zechner W. Computed tomography-based evaluation of template (NobelGuide™)-guided implant positions: a prospective radiological study.
→ Clin Oral Implants Res. 2011 Oct;22(10):1157–63. Epub 2011 Jan 18. A maximum deviation of 2.02 mm was found in the apico-coronal direction; nevertheless, significantly lower deviations in the mesiodistal direction were observed for implants in the anterior region and mandibular implants than for implants in the posterior region and maxillary implants. In a historical systematic review and meta-analysis by Jung et al., a mean error in angulation of 4.0°, with a maximum of 20.4°, was found.26Jung RE, Schneider D, Ganeles J, Wismeijer D, Zwahlen M, Hämmerle CH, Tahmaseb A. Computer technology applications in surgical implant dentistry: a systematic review.
→ Int J Oral Maxillofac Implants. 2009;24 Suppl:92–109. In the present study, a total mean error of 2.34 ± 1.44° (range: 0.3–5.8°) in angle, 0.49 ± 0.29 mm (range: 0.1–1.1 mm) in the horizontal plane (mesiodistal) and 0.53 ± 0.42 mm (range: 0.0–1.6 mm) in the vertical plane (apico-coronal) was found. In all of the cases, the maximum values (5.8° in angle, 1.1 mm in the horizontal plane and 1.6 mm in the vertical plane) did not exceed the safe offset of the software (1.5 mm in the horizontal plane and 2.0 mm in the vertical plane). Although no statistically significant differences were observed between conventional impressions and scan models and digital impressions, a trend of higher discrepancy between virtual and placed implants was observed in the fully digital group (mean error of 2.56 ± 1.52° in angle, 0.57 ± 0.32 mm in the horizontal plane and 0.67 ± 0.51 mm in the vertical plane). Major deviations were found for edentulous areas of three or more teeth (1.1 mm in the horizontal plane in the mandible and 1.6 mm in the vertical plane in the maxilla).
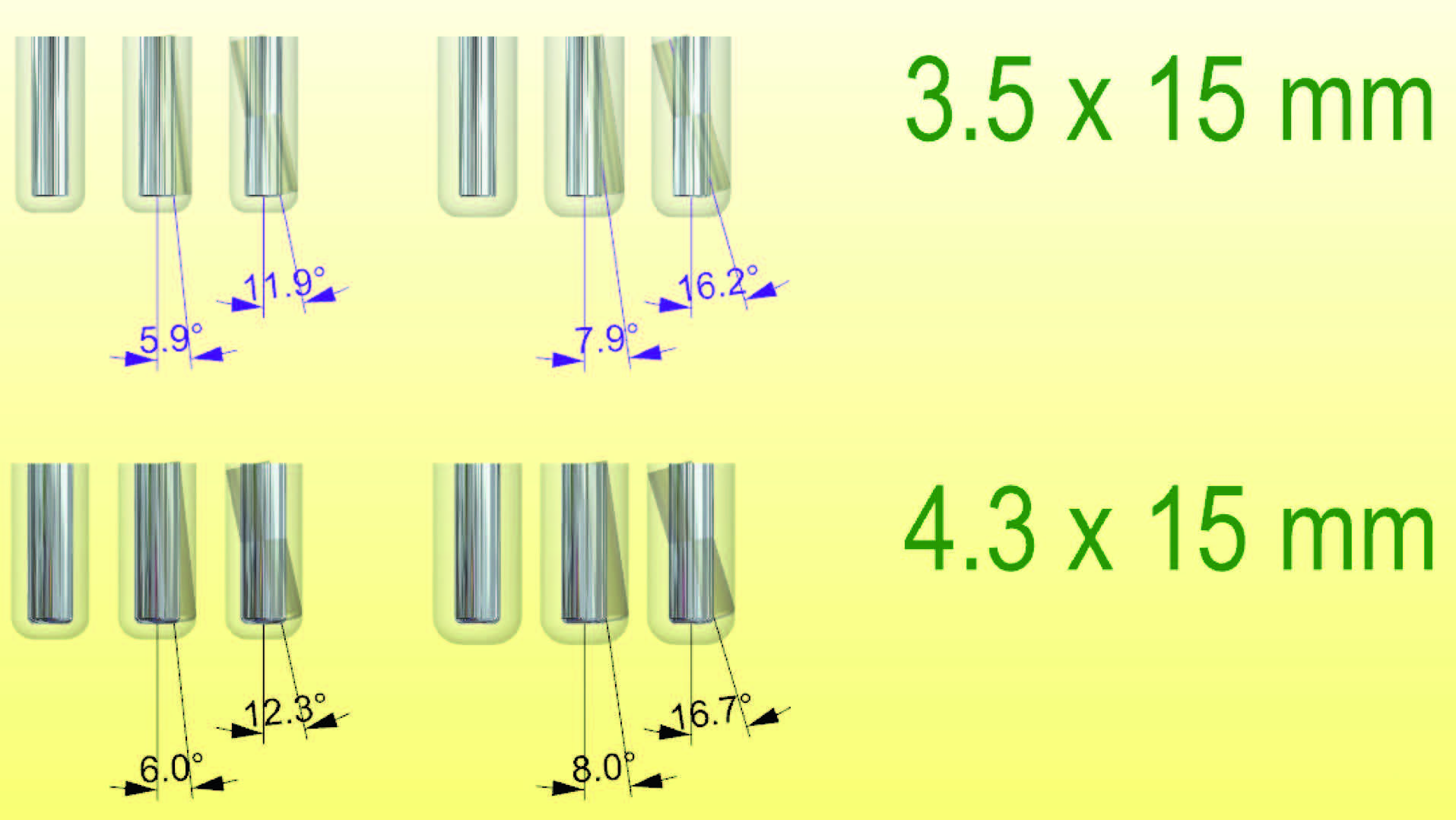
No data were reported in the scientific literature about the acceptable angle deviation. In the present study, based on a worse projection using implants of 3.5 and 4.0 mm in width and 15.0 mm in length and with standard offset, the maximum acceptable value ranged from 5.9 to 12.3° (Fig. 10). In the present study, a higher angular deviation was found in partially edentulous patients treated in the control group (5.8°). In contrast, minimum values of 0.1 mm in the horizontal plane and 0.0 mm in the vertical plane were observed in both groups, while a minimum angular deviation of 0.3° was observed in the fully guided group.
-
- Fig. 10
Fig. 10
Maximum angular deviation calculated according to the implant diameter and length.
The main purpose of computer-guided template-assisted surgery is to pre-visualize the approved prosthetic design of the tooth or teeth to be replaced and to relate it to the patient’s available soft and hard tissue. According to a recent study by Vermeulen, in cases of one or more missing teeth in the anterior maxilla, guided surgery yields significantly higher predictability and accuracy than freehand surgery in transferring the virtual implant position to a model situation.27Vermeulen J. The accuracy of implant placement by experienced surgeons: guided vs freehand approach in a simulated plastic model.
→ Int J Oral Maxillofac Implants. 2017 Mar/Apr;32(3):617–624. Epub 2016 Oct 14. Therefore, implant position can be optimized according to the esthetic and functional needs and an interim prosthesis can be manufactured prior to the surgical procedure, allowing immediate function.
Conclusion
Within the limitations of the present randomized controlled trial, it was found that intraoral digital impressions may be a viable alternative to conventional impressions and scan models for the rehabilitation of partially edentulous patients using computer-guided template-assisted implant placement. In both groups, the maximum 3-D deviations did not exceed the safe offset of the software.
Competing interests
The authors declare that they have no competing interests.
Interview
with Xhanari Erta
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Canullo L, Tallarico M, Radovanovic S, Delibasic B, Covani U, Rakic M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered peri-implantitis. → Clin Oral Implants Res. 2016 Oct;27(10):1243–50. Epub 2015 Nov 20. |
| 2. | ↑ | Furhauser R, Mailath-Pokorny G, Haas R, Busenlechner D, Watzek G, Pommer B. Esthetics of flapless single-tooth implants in the anterior maxilla using guided surgery: association of three-dimensional accuracy and pink esthetic score. → Clin Implant Dent Relat Res. 2015 Oct;17 Suppl 2:e427–33. Epub 2014 Oct 27. |
| 3, 27. | ↑ | Vermeulen J. The accuracy of implant placement by experienced surgeons: guided vs freehand approach in a simulated plastic model. → Int J Oral Maxillofac Implants. 2017 Mar/Apr;32(3):617–624. Epub 2016 Oct 14. |
| 4, 7, 16. | ↑ | Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial. → Eur J Oral Implantol. 2014 Autumn;7(3):229–42. |
| 5. | ↑ | Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:25–42. |
| 6. | ↑ | Van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, Wendelhag I. Computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicenter study. → Clin Implant Dent Relat Res. 2005;7 Suppl 1:111–20. |
| 8. | ↑ | Polizzi G, Cantoni T, Pasini E, Tallarico M. Immediate loading of variable-thread expanding tapered-body implants placed into maxillary post-extraction or healed sites using a guided surgery approach: an up-to-five-year retrospective analysis. → J Oral Science Rehabilitation. 2016 Sep;2(3):50–60. |
| 9. | ↑ | Meloni SM, Tallarico M, Pisano M, Xhanari E, Canullo L. Immediate loading of fixed complete denture prosthesis supported by 4-8 implants placed using guided surgery: a 5-year prospective study on 66 patients with 356 implants. → Clin Implant Dent Relat Res. 2017 Feb;19(1):195–206. Epub 2016 Sep 15. |
| 10. | ↑ | Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. Five-year results of a randomized controlled trial comparing patients rehabilitated with immediately loaded maxillary cross-arch fixed dental prosthesis supported by four or six implants placed using guided surgery. → Clin Implant Dent Relat Res. 2016 Oct;18(5):965–72. Epub 2015 Oct 7. |
| 11. | ↑ | Chochlidakis KM, Papaspyridakos P, Geminiani A, Chen CJ, Feng IJ, Ercoli C. Digital versus conventional impressions for fixed prosthodontics: a systematic review and meta-analysis. → J Prosthet Dent. 2016 Aug;116(2):184–190.e12. Epub 2016 Mar 2. |
| 12. | ↑ | Ahlholm P, Sipila K, Vallittu P, Jakonen M, Kotiranta U. Digital versus conventional impressions in fixed prosthodontics: a review. → J Prosthodont. 2016 Aug 2. doi:10.1111/jopr.12527. [Epub ahead of print] |
| 13, 14, 15. | ↑ | Tallarico M, Meloni SM. Open-cohort prospective study on early implant failure and physiological marginal remodeling expected using sandblasted and acid-etched bone level implants featuring an 11° Morse taper connection within one year after loading. → J Oral Science Rehabilitation. 2017 Mar;3(1):68–79. |
| 17, 22. | ↑ | D’haese J, Van De Velde T, Komiyama A, Hultin M, De Bruyn H. Accuracy and complications using computer-designed stereolithographic surgical guides for oral rehabilitation by means of dental implants: a review of the literature. → Clin Implant Dent Relat Res. 2012 Jun;14(3):321–35. Epub 2010 May |
| 18. | ↑ | Komiyama A, Klinge B, Hultin M. Treatment outcome of immediately loaded implants installed in edentulous jaws following computer-assisted virtual treatment planning and flapless surgery. → Clin Oral Implants Res. 2008 Jul;19(7):677–85. |
| 19. | ↑ | Merli M, Bernardelli F, Esposito M. Computer-guided flapless placement of immediately loaded dental implants in the edentulous maxilla: a pilot prospective case series. → Eur J Oral Implantol. 2008 Spring;1(1):61–9. |
| 20. | ↑ | Johansson B, Friberg B, Nilson H. Digitally planned, immediately loaded dental implants with prefabricated prostheses in the reconstruction of edentulous maxillae: a 1-year prospective, multicenter study. → Clin Implant Dent Relat Res. 2009 Sep;11(3):194–200. Epub 2008 Sep 9. |
| 21. | ↑ | Meloni SM, Tallarico M, Pisano M, Xhanari E, Canullo G. Immediate loading of fixed complete denture prosthesis supported by 4-8 implants placed using guided surgery: a 5-year prospective study on 66 patients with 356 implants. → Clin Implant Dent Relat Res. 2017 Feb;19(1):195–206. Epub 2016 Sep |
| 23. | ↑ | Polizzi G, Cantoni T, Pasini E, Tallarico M. Immediate loading of variable-thread expanding tapered-body implants placed into maxillary post-extraction or healed sites using a guided surgery approach: an up-to-5-year retrospective analysis. → J Oral Science Rehabilitation. 2016 Sep;2(3):50–60. |
| 24. | ↑ | Tallarico M, Canullo L, Pisano M, Penarrocha-Oltra D, Penarrocha-Oltra M, Meloni, SM. An up to 7-year retrospective analysis of biologic and technical complication with the All-on-4 concept. → J Oral Implantol. 2016 Jun;42(3):265–71. Epub 2015 Dec 11. |
| 25. | ↑ | Vasak C, Watzak G, Gahleitner A, Strbac G, Schemper M, Zechner W. Computed tomography-based evaluation of template (NobelGuide™)-guided implant positions: a prospective radiological study. → Clin Oral Implants Res. 2011 Oct;22(10):1157–63. Epub 2011 Jan 18. |
| 26. | ↑ | Jung RE, Schneider D, Ganeles J, Wismeijer D, Zwahlen M, Hämmerle CH, Tahmaseb A. Computer technology applications in surgical implant dentistry: a systematic review. → Int J Oral Maxillofac Implants. 2009;24 Suppl:92–109. |





Leave a Reply
Be the First to Comment!