All-on-4 with tapered neck implants and a hybrid prosthesis with a fiberglassreinforced structure
November 26, 2019 / Categories: Digital Dentistry, Implant Dentistry
Cabanes Gumbau, Guillermo

Canet López, Álvaro

Peñarrocha Diago, Miguel

Peñarrocha Diago, Maria
Abstract
Introduction
The All-on-4 treatment concept (Nobel Biocare) was developed to optimize remaining bone in completely edentulous patients, allowing immediate rehabilitation and avoiding the need for other regenerative procedures, which increase morbidity and costs. The present article describes a patient followed up on for 2 years after the placement of 4 transmucosal tapered neck implants restored with a hybrid prosthesis with a novel fiberglass- and resin-reinforced structure (TriLor Arch, Harvest Dental Products).
Clinical case
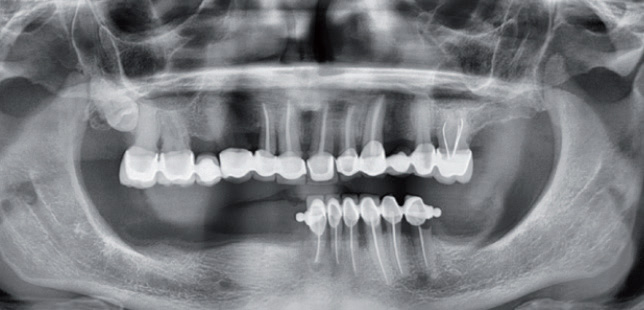
A 68-year-old woman presented with teeth in the anterior mandibular segment, numerous caries-affected teeth, missing teeth in the posterior segment, and mandibular bone atrophy. An All-on-4 procedure for immediate occlusal loading on 4 implants with a resin provisional fixed prosthesis was planned. Restoration with the definitive fixed prosthesis took place 6 months after surgery.
Conclusion
In atrophic mandibles, the use of tapered neck implants in conjunction with a novel nonmetallic fiberglass- and resin-reinforced structure (Trilor Arch) through an All on 4 technique, provides adequate functional and esthetic results after 2 years of follow-up.
Keywords
All-on-4; tilted implants; dental prostheses; immediate occlusal loading; fiberglass-reinforced composite structure.
Introduction
The All-on-4 treatment concept (Nobel Biocare) was developed to optimize the use of remaining bone in atrophic mandibles, allowing immediate rehabilitation and avoiding the need for other regenerative procedures that increase morbidity and cost.1Maló P, Rangert B, Dvärsäter L. Immediate function of Brånemark implants in the esthetic zone: a retrospective clinical study with 6 months to 4 years of follow-up. → Clin Implant Dent Relat Res. 2000 Jul;2(3):138–46. The treatment protocol involves the placement of 4 implants in the anterior maxillary segment or in the space between the mental foramina of the mandible. The 2 most anterior implants are positioned axially, while the 2 posterior implants are distalized and tilted in order to minimize the cantilever length and thus allow extension of the prosthesis to the area of the first molar, thereby improving masticatory efficiency.2Maló P, Rangert B, Nobre M. “All-on-four” immediatefunction concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:2–9.,3Maló P, Friberg B, Polizzi G, Gualini F, Vighagen T, Rangert B. Immediate and early function of Brånemark System implants placed in the esthetic zone: a 1-year prospective clinical multicenter study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:37–46. This treatment strategy affords promising results over the short and middle term and is highly successful in terms of implant survival rate, as described in the literature,4Soto-Penaloza D, Zaragozí-Alonso R, Penarrocha- Diago M, Penarrocha-Diago M. The all-on-four treatment concept: systematic review. → J Clin Exp Dent. 2017 Mar 1;9(3):e474–88. doi: 10.4317/jced.53613. provided adequate surgical and prosthetic protocols are used.5Penarrocha-Diago M, Penarrocha-Diago M, Zaragozí- Alonso R, Soto-Penaloza D, on behalf of the Ticare Consensus M. Consensus statements and clinical recommendations on treatment indications, surgical procedures, prosthetic protocols and complications following All-on-4 standard treatment. 9th Mozo-Grau Ticare Conference in Quintanilla, Spain. → J Clin Exp Dent. 2017 May;9(5):e712–5. doi: 10.4317/jced.53759.
-
- Fig. 1
Primary implant stability is an essential pre-requisite for immediate loading, it can be improved by adapting drilling protocols to enhance lateral compression of the bone and by using tapered implant designs.6De Bruyn, H. , Raes, S. , Östman, P. and Cosyn, J. (2014), Immediate loading in partially and completely edentulous jaws: a review of the literature with clinical guidelines. → Periodontol. 2000;66:153-87. The prosthetic restoration should provide rigidity and not be flexible in order to avoid micro-movements, and should be strong enough to not fracture.7Penarrocha-Diago M, Penarrocha-Diago M, Zaragozí- Alonso R, Soto-Penaloza D, on behalf of the Ticare Consensus M. Consensus statements and clinical recommendations on treatment indications, surgical procedures, prosthetic protocols and complications following All-on-4 standard treatment. 9th Mozo-Grau Ticare Conference in Quintanilla, Spain. → J Clin Exp Dent. 2017 May;9(5):e712–5. doi: 10.4317/jced.53759.
The original Brånemark surgical and prosthetic protocol advocated the placement of 4 implants for the restoration of a resorbed mandible and 6 implants in the case of mandibles with minimal or moderate resorption.8De Bruyn, H. , Raes, S. , Östman, P. and Cosyn, J. (2014), Immediate loading in partially and completely edentulous jaws: a review of the literature with clinical guidelines. → Periodontol. 2000;66:153-87. Other guidelines were subsequently also developed.9Maló P, Rangert B, Nobre M. “All-on-four” immediatefunction concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:2–9. The present clinical case describes the results after 2 years of follow-up in a patient subjected to All-on-4 rehabilitation involving 2 novel elements that appear to offer interesting advantages over the conventional technique. From the surgical perspective, the dental implants used present a new tapered neck design, while from the prosthodontic perspective, the definitive prosthesis is manufactured with a novel nonmetallic fiberglass- and resin-reinforced structure (TriLor Arch, Harvest Dental Products).
Clinical case
A 68-year-old woman presented with teeth in the anterior mandibular segment, numerous caries-affected teeth, missing teeth in the posterior segment, and mandibular bone atrophy (Fig. 1). After extractions and preoperative examination, it was observed that the posterior segment was located close to the inferior alveolar nerve. An All-on-4 procedure was planned involving 4 Prama implants (Sweden & Martina, Padua, Italy), with immediate occlusal loading of the resin provisional fixed prosthesis. Restoration with the definitive fixed prosthesis with TriLor Arch internal reinforcement would take place 6 months after surgery.
Surgical technique
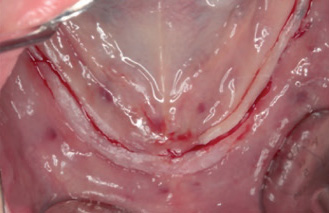
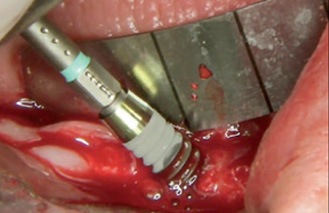
A full-thickness mucoperiosteal flap was raised with central and distal releasing incisions, allowing us to visualize emergence of the mental nerves and access the anterior bone. A 2 × 10 mm central bone perforation was performed, the axis coinciding with the facial midline, in order to insert the stem of a standard metal surgical guide with vertical marks to help orientate dental implant placement tilted at 30°, while also keeping the tongue away from the surgical field.
-
- Fig. 2a
-
- Fig. 2b
-

- Fig. 2c
-
- Fig. 2d
-

- Fig. 2e
-

- Fig. 2f
-
- Fig. 3a
-

- Fig. 3b
-

- Fig. 3c
-

- Fig. 3d
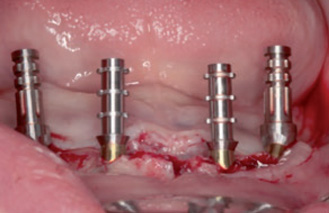
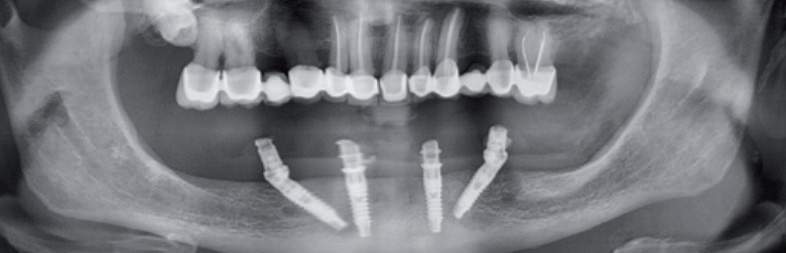
Two tilted distal implants (3.8 × 13.0 mm) were placed with a minimum insertion torque of 35–40 N cm. Transmucosal abutments were placed on the 2 distal implants to correct tilting in the screw-retained prosthesis, applying a torque of 25 N cm, and 2 provisional straight titanium abutments were fitted over them. Then, the beds of the 2 mesial implants were prepared, seeking to maintain equidistance and parallelism between them and the 2 distal abutments. Two cylindrical implants (3.8 × 11.5 mm) were placed in these positions with undersized drilling using conical burs and a minimum insertion torque of 35–45 N cm. Two provisional straight titanium abutments (Sweden & Martina, Padua, Italy) without a hexagonal base were screwed over these 2 central implants, with no need for an intermediate abutment thanks to the large transmucosal portion specific to implants of this kind. Panoramic radiographs were obtained, thereby completing the surgical phase of the All-on-4 procedure (Fig. 2).
-

- Fig. 4a

-

- Fig. 4b

-
- Fig. 4c
Immediate occlusal loading prosthodontic technique
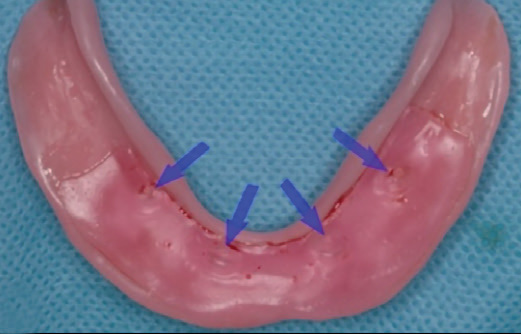
A thin layer of soft warm wax on the tissue aspect of the provisional prosthesis allowed pressure marking of the healing abutments as a simple way to indicate the location of the implants for making 4 perforations in the prosthesis where photopolymerizing fluid composite was used to splint the provisional titanium abutments directly in the mouth (Fig. 3). These abutments were then definitively incorporated into the prosthesis in the laboratory, the lateral posterior wings of the prosthesis were trimmed, and 3 h after surgery, we were able to position the prosthesis in the mouth with correct passive and occlusal fit (Fig. 4).
Prosthodontic technique for the definitive prosthesis
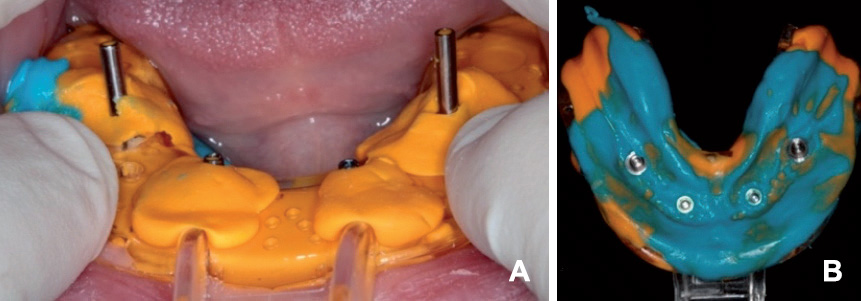
A screw-retained hybrid prosthesis containing a fiberglass- and resin-reinforced structure (TriLor Arch) was manufactured. The definitive prosthetic phase started by unscrewing the provisional prosthesis, performing hygiene and fitting 4 transfer copings for impression taking using the open-tray technique with silicone of 2 consistencies. The impression thus obtained recorded the positioning of the implants and of the soft tissue (Fig. 5).
A mandibular baseplate was prepared in the laboratory for a maxillomandibular relationship record to determine the vertical dimension. The provisional prosthesis also served as reference, thanks to correct adaptation and patient comfort. The passive fit of the resin-splinted definitive abutments was checked, and the assembly was sent to the laboratory again (Fig. 6).
Separate testing was done of the teeth and TriLor Arch bar, which bore the orifices for fitting of the definitive abutments, and these were later cemented in the laboratory (fixed with dual-polymerizing composite cement [URC Bioloren]). The occlusion was checked, and the assembly was sent to the laboratory for integration of the TriLor Arch structure to the tooth (Fig. 7). The definitive prosthesis therefore contained the reinforcing structure integrated into the resin, which had convex compressive fit on its tissue aspect, in the inter-implant zones, to facilitate hygiene and ensure less plaque retention (Fig. 8).
-
- Fig. 5
-
- Fig. 6
-

- Fig. 7
-

- Fig. 8
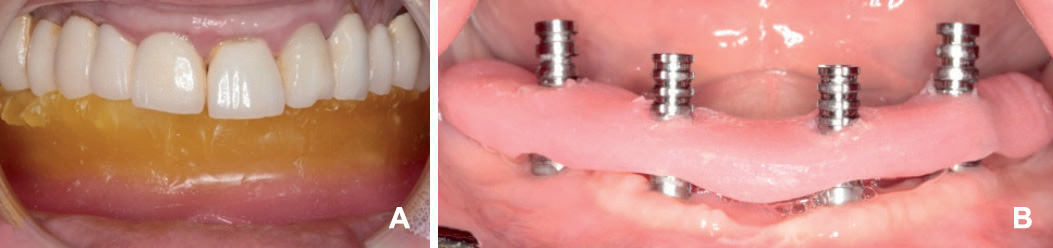
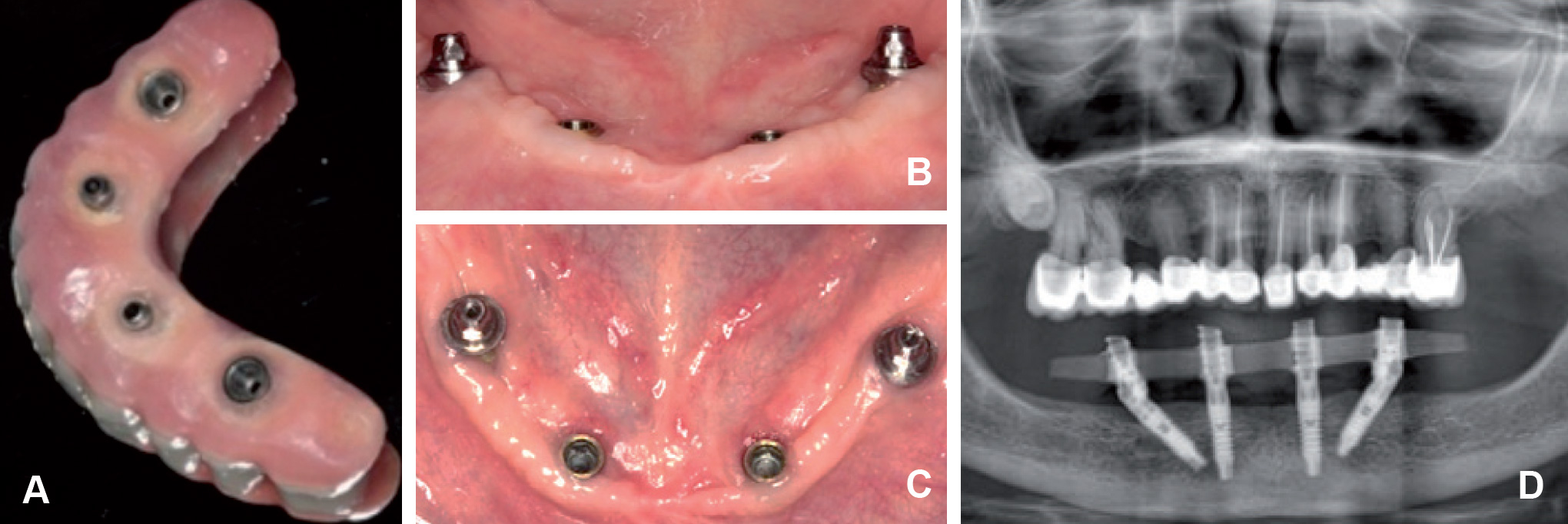
After 2 years of follow-up, correct periimplant soft tissue conditions were confirmed, as was integrity of the structure and good bone stability (Fig. 9). The mean marginal bone loss after 24 months was 0.5 ± 0.09 for tilted straight implants. A similar bone loss pattern between tilted and straight implants is observed. The bleeding on probing (BOP) according to Mombelli index was 0 in all implants.10Hashim D, Cionca N, Combescure C, Mombelli A. The diagnosis of peri-implantitis: A systematic review on the predictive value of bleeding on probing. → Clin Oral Implants Res. 2018 Oct;29 Suppl 16:276-93. Hygiene was performed every 6 months, and the patient received instructions on how to maintain good implant conditions and health.
-
- Fig. 9
-
- Fig. 10a
-
- Fig. 10b
Discussion
The present 2-year follow-up study has provided a detailed description of the All-on-4 technique and shown it to be a reliable, immediate, simple, safe and costeffective solution for the implant-based rehabilitation of patients involving immediate occlusal loading with a screw-retained prosthesis followed by the fitting of a hybrid prosthesis with a novel fiberglass- and resinreinforced structure (TriLor Arch). Moreover, the use of tissue level implants with a tapered design at the transmucosal portion appears to offer a number of additional advantages thanks to the large transepithelial machined portion specific to implants of this kind.
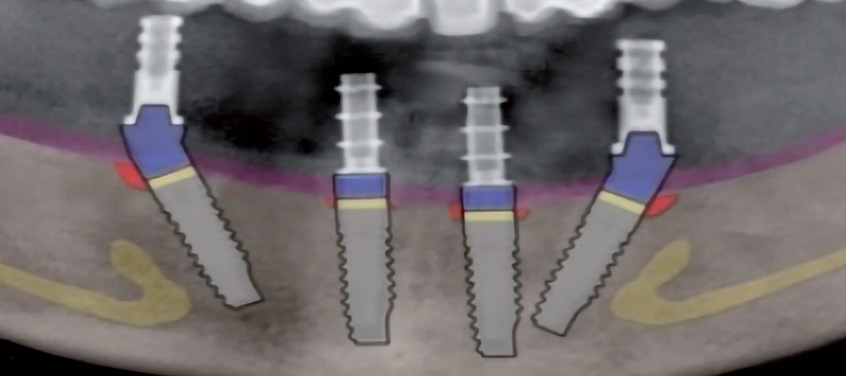
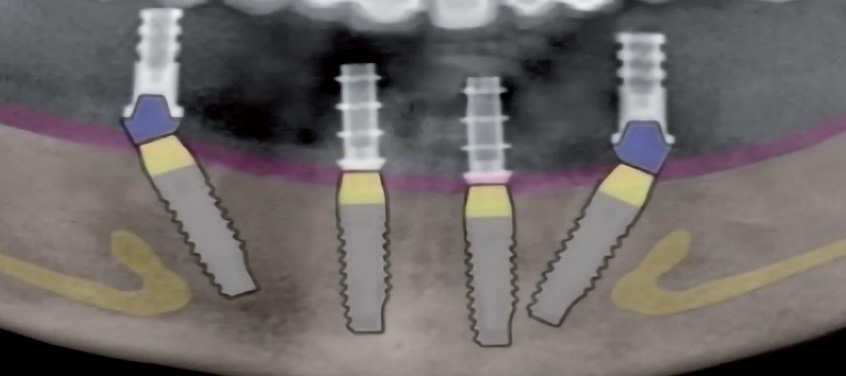
Implants of this kind eliminate the need observed with other types of implants to perform aggressive drilling of the bone crest to accommodate the tilted implant in order to submerge its distal occlusal table in the bone and avoid mesial thread exposure. This type of treatment avoids the appearance of cratering effects arising from the location of the implant–transepithelial junction gap at infrabony level (Fig. 10).
There is no need to use transmucosal abutments on the 2 mesial straight implants on which the provisional titanium prosthesis is directly screwed. The resulting intraoral clinical work is more convenient as a result, and fewer screws and accessories are used. Furthermore, the chosen titanium abutment design, with anatomical emergence, facilitates smooth and hygienic fitting of the resin of the prosthesis on its tissue aspect facing the implant.
Frequent exposure of the polished neck of the implant secondary to physiological gingival retraction in the context of the postoperative tissue remodeling process is no problem for the definitive prosthesis, since the tapered coronal part of the implant has no limiting chamfer or shoulder, and the prosthesis can be freely adjusted over any level of its coronal hyperbolic portion.11Brånemark PI, Engstrand P, Ohrnell LO, Gröndahl K, Nilsson P, Hagberg K. Brånemark Novum®: a new treatment concept for rehabilitation of the edentulous mandible. Preliminary results from a prospective clinical follow- up study. → Clin Implant Dent Relat Res. 1999;1:2–16.,12Loi I, Scutellà F, Galli F. Tecnica di preparazione orientata biologicamente (BOPT). Un nuovo approccio nella preparazione protesica in odontostomatologia (The biologically oriented preparation technique [BOPT]. A new approach to prosthetic preparation in oral surgery). → Quintessenza Int. 2008 Sep–Oct;24(5):69–75.,13Loi I. Protesi su denti naturali nei settori di rilevanza estetica con tecnica BOPT: Case series report (Prosthesis on natural teeth in areas of aesthetic relevance with BOPT technique: Case series report). → Dent Cadmos. 2008;76:51–9.,14Loi I, Galli F, Scutellà F, Felice A. Il contorno coronale protesico con tecnica di preparazione BOPT (biologically oriented preparation technique): considerazioni tecniche. → Quintessenza Int. 2009 Jul–Aug;25(4):4–19.,15Loi I, Di Felice A. Biologically oriented preparation technique (BOPT): a new approach for prosthetic restoration of periodontically healthy teeth. → Eur J Esthet Dent. 2013 Spring;8(1):10–23.
This All-on-4 immediate occlusal loading protocol for completely edentulous mandibles has yielded longterm success rates of over 95% at 7 years for implants and 99% for prostheses and a mean crestal bone loss of 1.81 mm at 5 years.16Cabanes G. Experiencia en clínica de la técnica BOPT sobre implantes: preparación vertical de pilares y conformación de la emergencia coronaria. In: Agustin- Panadero R, Chust López C, editors. Protocolo clinicoprotésico de la técnica BOPT. → Barcelona: Ediciones Especializadas Europeas; 2016. p. 207–13.
Biomechanical properties are an essential element in this rehabilitation protocol. The tilted implants afford an optimum distance between implants, allowing support of the free ends of the prosthesis.17Maló P, de Araújo Nobre M, Lopes A, Ferro A, Gravito I. All-on-4® treatment concept for the rehabilitation of the completely edentulous mandible: a 7-year clinical and 5-year radiographic retrospective case series with risk assessment for implant failure and marginal bone level. → Clin Implant Dent Relat Res. 2015 Oct;17 Suppl 2:e531–41. doi: 10.1111/cid.12282. In a systematic review and meta-analysis no effect of implant inclination on implant survival or periimplant bone loss were found as in our case.18Apaza Alccayhuaman, KA, Soto-Peñaloza, D, Nakajima, Y, Papageorgiou, SN, Botticelli, D, Lang, NP. Biological and technical complications of tilted implants in comparison with straight implants supporting fixed dental prostheses. A systematic review and metaanalysis. → Clin Oral Impl Res. 2018; 29(Suppl. 18): 295– 308. With regard to the restoration phase in our patient, the novel fiberglass- and resin-reinforced internal structure appears to offer a number of interesting advantages. It consists of a newgeneration polymer composed of thermally hardened resin with multidirectional fiberglass reinforcement. Such fiber-reinforced composites (FRCs) are used in aeronautical engineering and in many other fields where high resistance and low weight are key requirements. The multidirectional braided-fiber structure of the reinforcement offers good performance in terms of load and tension distribution in response to forces applied from different incident angles.
The technique simplifies the manufacture of reinforcing superstructures with passive fit by only requiring manual processing in the laboratory, with no need for CAD/CAM procedures. The preformed presentation in the form of a flat arc makes it possible to establish connecting structures between the implant abutments or reinforcing elements for removable prostheses. These structures and elements can easily be incorporated within the fiberglass- and resin-reinforced internal structure of the prosthesis, establishing true chemical bonding, in contrast to what is seen with metal reinforcement structures.
Conclusion
In the case reported, tapered neck implants with immediate occlusal loading based on the All-on-4 technique, with the use of a nonmetallic reinforcing structure in the hybrid prosthesis, afforded optimum biomechanical performance and hygiene after 2 years of follow-up. Further studies are needed to assess the mid- and long-term outcomes of the procedure.
Competing interests
The authors declare that they have no competing interests.
Figure legends
Fig. 1 – Initial panoramic radiographic view.
Fig. 2 – (A) Full-thickness mucoperiosteal flap. (B) Placement of the tilted distal implant with the surgical guide. (C) Implants placed with 2 transmucosal abutments to correct tilting of the distal implants. (D) Provisional straight titanium abutments. (E) Wound suture. (F) Final panoramic radiographic view after placement of the 4 Prama implants.
Fig. 3 – (A) Tissue aspect of the prosthesis coated with soft wax. (B) Perforations in the provisional complete prosthesis. (C) & (D) Fitting and splinting of the titanium abutments in the provisional prosthesis.
Fig. 4 – (A) Tissue aspect of the provisional prosthesis with the wings trimmed. (B) Provisional prosthesis placed 3 h after surgery. (C) Control radiograph after placing of the prosthesis.
Fig. 5 – (A) & (B) Impression using silicone of 2 consistencies, registering the soft tissue and implant positioning.
Fig. 6 – Mandibular baseplate for determining vertical dimension (A) and checking of passive fit of the resin-splinted abutments (B).
Fig. 7 – TriLor Arch structure with the orifices for fitting of the definitive titanium abutments with composite cement and wax tooth testing.
Fig. 8 – Completed definitive implant-supported hybrid prosthesis with TriLor Arch reinforcement.
Fig. 9 – (A) Tissue aspect of the prosthesis after 2 years. (B) & (C) Periimplant soft tissue condition after 2 years. (D) Panoramic radiographic view after 2 years of followup.
Fig. 10 – Advantages of tapered neck transmucosal implants (A) over conventional implants (B).
Interview
with Dr. Álvaro Canet López
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Maló P, Rangert B, Dvärsäter L. Immediate function of Brånemark implants in the esthetic zone: a retrospective clinical study with 6 months to 4 years of follow-up. → Clin Implant Dent Relat Res. 2000 Jul;2(3):138–46. |
| 2, 9. | ↑ | Maló P, Rangert B, Nobre M. “All-on-four” immediatefunction concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:2–9. |
| 3. | ↑ | Maló P, Friberg B, Polizzi G, Gualini F, Vighagen T, Rangert B. Immediate and early function of Brånemark System implants placed in the esthetic zone: a 1-year prospective clinical multicenter study. → Clin Implant Dent Relat Res. 2003 Mar;5 Suppl 1:37–46. |
| 4. | ↑ | Soto-Penaloza D, Zaragozí-Alonso R, Penarrocha- Diago M, Penarrocha-Diago M. The all-on-four treatment concept: systematic review. → J Clin Exp Dent. 2017 Mar 1;9(3):e474–88. doi: 10.4317/jced.53613. |
| 5, 7. | ↑ | Penarrocha-Diago M, Penarrocha-Diago M, Zaragozí- Alonso R, Soto-Penaloza D, on behalf of the Ticare Consensus M. Consensus statements and clinical recommendations on treatment indications, surgical procedures, prosthetic protocols and complications following All-on-4 standard treatment. 9th Mozo-Grau Ticare Conference in Quintanilla, Spain. → J Clin Exp Dent. 2017 May;9(5):e712–5. doi: 10.4317/jced.53759. |
| 6, 8. | ↑ | De Bruyn, H. , Raes, S. , Östman, P. and Cosyn, J. (2014), Immediate loading in partially and completely edentulous jaws: a review of the literature with clinical guidelines. → Periodontol. 2000;66:153-87. |
| 10. | ↑ | Hashim D, Cionca N, Combescure C, Mombelli A. The diagnosis of peri-implantitis: A systematic review on the predictive value of bleeding on probing. → Clin Oral Implants Res. 2018 Oct;29 Suppl 16:276-93. |
| 11. | ↑ | Brånemark PI, Engstrand P, Ohrnell LO, Gröndahl K, Nilsson P, Hagberg K. Brånemark Novum®: a new treatment concept for rehabilitation of the edentulous mandible. Preliminary results from a prospective clinical follow- up study. → Clin Implant Dent Relat Res. 1999;1:2–16. |
| 12. | ↑ | Loi I, Scutellà F, Galli F. Tecnica di preparazione orientata biologicamente (BOPT). Un nuovo approccio nella preparazione protesica in odontostomatologia (The biologically oriented preparation technique [BOPT]. A new approach to prosthetic preparation in oral surgery). → Quintessenza Int. 2008 Sep–Oct;24(5):69–75. |
| 13. | ↑ | Loi I. Protesi su denti naturali nei settori di rilevanza estetica con tecnica BOPT: Case series report (Prosthesis on natural teeth in areas of aesthetic relevance with BOPT technique: Case series report). → Dent Cadmos. 2008;76:51–9. |
| 14. | ↑ | Loi I, Galli F, Scutellà F, Felice A. Il contorno coronale protesico con tecnica di preparazione BOPT (biologically oriented preparation technique): considerazioni tecniche. → Quintessenza Int. 2009 Jul–Aug;25(4):4–19. |
| 15. | ↑ | Loi I, Di Felice A. Biologically oriented preparation technique (BOPT): a new approach for prosthetic restoration of periodontically healthy teeth. → Eur J Esthet Dent. 2013 Spring;8(1):10–23. |
| 16. | ↑ | Cabanes G. Experiencia en clínica de la técnica BOPT sobre implantes: preparación vertical de pilares y conformación de la emergencia coronaria. In: Agustin- Panadero R, Chust López C, editors. Protocolo clinicoprotésico de la técnica BOPT. → Barcelona: Ediciones Especializadas Europeas; 2016. p. 207–13. |
| 17. | ↑ | Maló P, de Araújo Nobre M, Lopes A, Ferro A, Gravito I. All-on-4® treatment concept for the rehabilitation of the completely edentulous mandible: a 7-year clinical and 5-year radiographic retrospective case series with risk assessment for implant failure and marginal bone level. → Clin Implant Dent Relat Res. 2015 Oct;17 Suppl 2:e531–41. doi: 10.1111/cid.12282. |
| 18. | ↑ | Apaza Alccayhuaman, KA, Soto-Peñaloza, D, Nakajima, Y, Papageorgiou, SN, Botticelli, D, Lang, NP. Biological and technical complications of tilted implants in comparison with straight implants supporting fixed dental prostheses. A systematic review and metaanalysis. → Clin Oral Impl Res. 2018; 29(Suppl. 18): 295– 308. |





Leave a Reply
Be the First to Comment!