Antimicrobial efficacy of mouthwashes containing zinc-substituted nanohydroxyapatite and zinc L-pyrrolidone carboxylate on suture threads after surgical procedures
December 7, 2017 / Categories: Digital Dentistry, Implant Dentistry

Cosola, Saverio

Marconcini, Simone

Giammarinaro, Enrica
Marchisio, Olivia
Lelli, Marco
Roveri, Norberto
Genovesi, Anna Maria
Abstract
Objective
Suture threads used after oral surgery may be colonized by pathogenic microorganisms which could infect the surrounding tissue and impair the wound-healing process. Therefore, the postoperative use of antimicrobial mouthwashes is highly recommended. In this study, a mouthwash containing zinc-substituted nanohydroxyapatite (Zn-nHAp) and zinc L-pyrrolidone carboxylate (Zn-PCA) was compared with a product containing chlorhexidine for its efficacy in reducing microbial adherence to suture threads.
Materials and methods
Twenty-six patients subjected to minimal surgical interventions were randomized into a chlorhexidine group (C-group; n = 13) and a hydroxyapatite group (H-group; n = 13). All of the subjects followed a postoperative home treatment with a mouthwash containing chlorhexidine and a mouthwash containing Zn-nHAp/Zn-PCA, respectively. After their removal, suture threads were cut into segments and bacteria present on them were allowed to grow in different media and under different conditions. Colony-forming units were then enumerated.
Results
Quantification of mesophilic bacteria, Lactobacillus spp and total bacterial load and the search for specific anaerobic strains resulted in no statistically significant differences between the C-group and H-group. Hydroxyapatite, zinc ions and Zn-PCA are all endowed with antimicrobial properties. All of them presumably contribute to the overall high antimicrobial efficacy shown by oral care products containing a combination of these components.
Conclusion
The mouthwash containing Zn-nHAp and Zn-PCA was found to possess at least the same antibacterial efficacy as the mouthwash containing chlorhexidine, but without exerting the typical side effects of chlorhexidine itself.
Keywords
Zinc-substituted nanohydroxyapatite, zinc L-pyrrolidone carboxylate, bacterial load, mouthwash, suture thread.
Introduction
Oral surgery interventions usually require sutures in order to facilitate wound healing and to prevent dehiscence. However, suture threads are inevitably colonized by microorganisms that could infect surrounding tissue and impair the wound-healing process.1Otten JE, Wiedmann-Al-Ahmad M, Jahnke H, Pelz K. Bacterial colonization on different suture materials—a potential risk for intraoral dentoalveolar surgery.
→ J Biomed Mater Res B Appl Biomater. 2005 Jul;74(1):627–35.2Katz S, Izhar M, Mirelman D. Bacterial adherence to surgical sutures. A possible factor in suture induced infection.
→ Ann Surg. 1981 Jul;194(1):35–41.3Banche G, Roana J, Mandras N, Amasio M, Gallesio C, Allizond V, Angeretti A, Tullio V, Cuffini AM. Microbial adherence on various intraoral suture materials in patients undergoing dental surgery.
→ J Oral Maxillofac Surg. 2007 Aug;65(8):1503–7.4Pons-Vicente O, López-Jiménez L, Sánchez-Garcés MA, Sala-Pérez S, Gay-Escoda C. A comparative study between two different suture materials in oral implantology.
→ Clin Oral Implants Res. 2011 Mar;22(3):282–8.
Many different kinds of surgical sutures (natural and synthetic) with different properties have been proposed over the years to overcome plaque stratification over threads. It is already known that bacterial adherence to suture threads may delay and affect the wound-healing process. For this purpose, several antimicrobial agents have been tested to be incorporated in or to coat suture threads.5Harnet JC, Le Guen E, Ball V, Tenenbaum H, Ogier J, Haikel Y, Vodouhe C. Antibacterial protection of suture material by chlorhexidine-functionalized polyelectrolyte multilayer films.
→ J Mater Sci Mater Med. 2009 Jan;20(1):185–93. Mouthwashes are highly recommended for home care maintenance as an adjunctive measure to reduce bacterial colonization of sutures and postoperative inflammation.6Brown AR, Papasian CJ, Shultz P, Theisen FC, Shultz RE. Bacteremia and intraoral suture removal: can an antimicrobial rinse help?
→ J Am Dent Assoc. 1998 Oct;129(10):1455–61. Nowadays, chlorhexidine is the gold standard in terms of antimicrobial activity because of its wide spectrum of actions. Chlorhexidine has been commercially proposed in many different formulas.7Jones CG. Chlorhexidine: is it still the gold standard?
→ Periodontol 2000. 1997 Oct;15:55–62. Even though its several advantages have been profusely demonstrated, some adverse effects, such as tooth staining,8Addy M, Sharif N, Moran J. A nonstaining chlorhexidine mouthwash? Probably not: a study in vitro.
→ Int J Dent Hyg. 2005 May;3(2):59–63.9Bagis B, Baltacioglu E, Özcan M, Ustaomer S. Evaluation of chlorhexidine gluconate mouthrinse-induced staining using a digital colorimeter: an in vivo study.
→ Quintessence Int. 2011 Mar;42(3):213–23. tongue discoloration, and desquamation and soreness of the oral mucosa, should be considered.10Banche G, Roana J, Mandras N, Amasio M, Gallesio C, Allizond V, Angeretti A, Tullio V, Cuffini AM. Microbial adherence on various intraoral suture materials in patients undergoing dental surgery.
→ J Oral Maxillofac Surg. 2007 Aug;65(8):1503–7.11Helms JA, Della-Fera MA, Mott AE, Frank ME. Effects of chlorhexidine on human taste perception.
→ Arch Oral Biol. 1995 Oct;40(10):913–20.12Frank ME, Gent JF, Hettinger TP. Effects of chlorhexidine on human taste perception.
→ Physiol Behav. 2001 Sep 1–15;74(1–2):85–99.13. Marinone MG, Savoldi E. Chlorhexidine and taste. Influence of mouthwashes concentration and of rinsing time.
→ Minerva Stomatol. 2000 May;49(5):221–6. Because of its nature, clinicians must look at chlorhexidine as an antimicrobial agent to which bacteria could develop resistance, especially in the case of long-term use.14Russell AD. Biocide use and antibiotic resistance: the relevance of laboratory findings to clinical and environmental situations.
→ Lancet Infect Dis. 2003 Dec;3(12):794–803. Given those issues, researchers have been seeking alternatives to chlorhexidine in terms of antiseptic designs. In the present study, the authors tested a mouthwash containing zinc-substituted nanohydroxyapatite (Zn-nHAp) and zinc L-pyrrolidone carboxylate (Zn-PCA) in terms of microbial adherence to suture threads compared with a mouthwash containing chlorhexidine.
Materials and methods
Study protocol
The present clinical case–control study was a multicenter study including the Tuscan Stomatologic Institute, Versilia General Hospital, Lido di Camaiore, Italy, and the University of Bologna, Bologna, Italy. All of the participants were screened according to the following inclusion and exclusion criteria.
Inclusion criteria:
- aged 30 years and older;
- received minimal surgical interventions (extraction, implant surgery, periodontal surgery) with sutures; and
- compliance with the study protocol and willingness to adhere to the hygiene instructions.
Exclusion criteria:
- pregnancy;
- antibiotics, nonsteroidal anti-inflammatory drugs, or steroids in the previous 3 months;
- severe systemic disease that could compromise the conduct of the study;
- untreated diabetes;
- chronic or aggressive periodontitis or other severe oral pathologies;
- smoking more than 5 cigarettes a day; and
- alcohol or other drug abuse.
At the end of the screening procedure, 26 patients were enrolled in the study and randomized into 2 maintenance groups according to the mouthwash used: (a) a control group (the chlorhexidine group, or C-group, n = 13), in which the patients followed a postoperative home treatment for at least 7 days with a mouthwash containing 0.2% chlorhexidine (Dentosan, Johnson & Johnson, Rome, Italy); and a treatment group (the hydroxyapatite group, or H-group, n = 13), in which the patients followed a postoperative home treatment for at least 7 days with a mouthwash containing Zn-nHAp/Zn-PCA (Biorepair, Coswell, Funo, Italy), with a 2.0% w/v concentration of Zn-nHAp and an overall concentration of Zn of 11.0% w/v. Nonabsorbable silk sutures (Sweden & Martina, Due Carrare, Italy) were removed after 10 days from the surgical sites of all of the patients.
All sutures were placed and removed by the same skilled operator to eliminate interexaminer variability. The collected samples were immediately transported to the laboratory and stored at -20 °C until microbiological analysis. All subject randomization was performed by means of a computer program generating random numbers. Oral and written information was given to each enrolled subject. All of the patients enrolled were informed about the study protocol and were asked to sign an informed written consent for participation. This study was carried out according to the ethical principles of the Declaration of Helsinki of 1975, as revised in 2013, for medical research involving human subjects. Figure 1 provides a flowchart summarizing the study protocol.
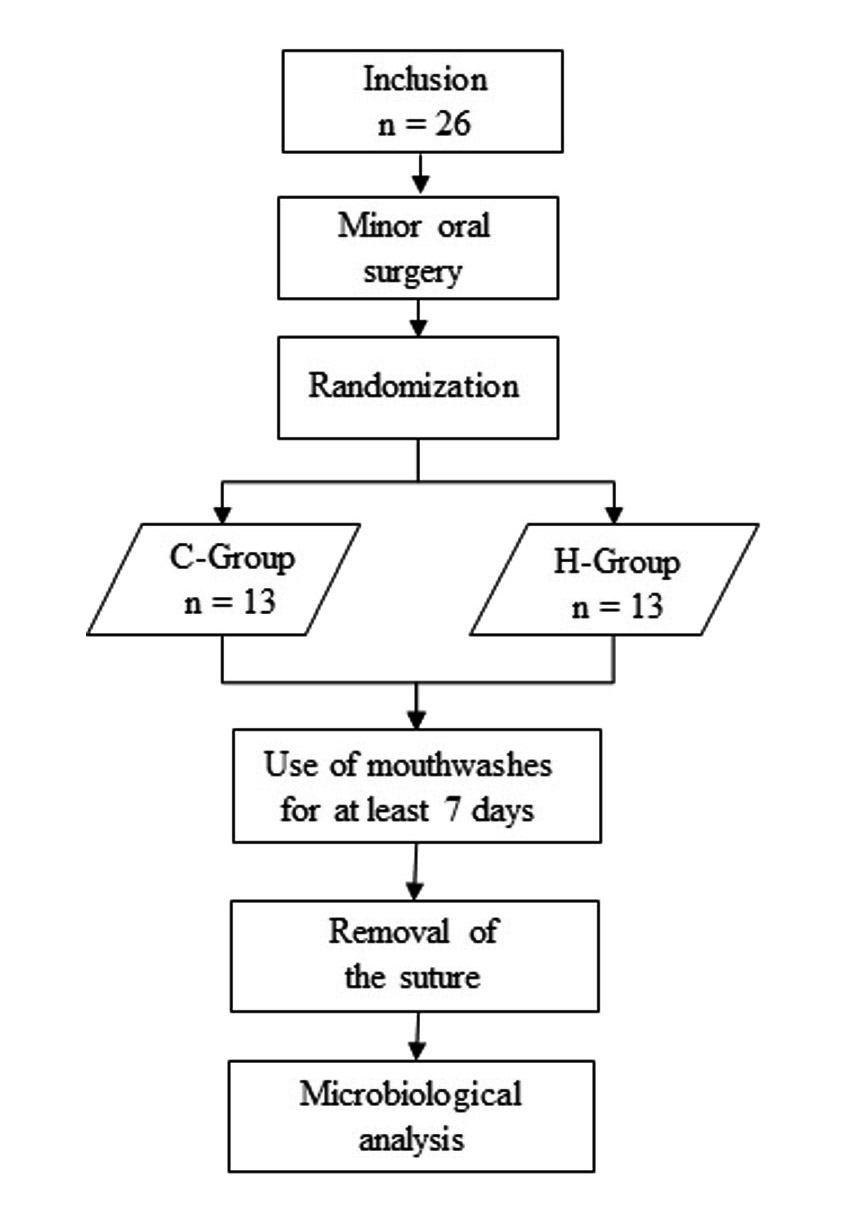
Fig. 1
Flowchart illustrating the study protocol.
Culture media and conditions
Bacteria were cultured in Petri dishes containing tryptone soy agar (TSA) as growth medium at an incubation temperature of 36 ± 1 °C. In this way, it was possible to obtain the growth of mesophilic bacteria. De Man, Rogosa and Sharpe (MRS) agar at 36 ± 1 °C allowed the growth of Lactobacillus spp. Bacteroides bile esculin (BBE) agar and brucella blood agar (BRU) with vitamin K and hemin, incubated at 36 ± 1 °C under anaerobic conditions allowed the qualitative analysis of specific anaerobic strains.
Test procedureand bacterial scoring
Microbial load was assessed after suture removal using in vitro bacterial cultures. Suture thread samples were stored at -20 °C until microbiological analysis. Before testing, samples were thawed at room temperature. Each sample was cut into 3 segments of similar length, then each thread sample was subjected to analysis as follows. The control sample was represented by segments of a sterile, unused suture thread.
Assessment of the absence/presence of bacterial load: Two segments of the thread were scraped on 2 culture plates containing agarbased broth media (TSA and MRS) and incubated for 48 h at 36 ± 1 °C in order to determine whether microbial load was present on the thread surface. The plates were visually inspected and bacterial load accordingly classified as absent or present.
Enumeration of bacterial colonies: One segment was placed in a tube containing a diluent solution (buffered peptone water; BPW) for 1 h, then, further serial decimal dilutions were carried out.
Each dilution, the first included, was seeded in plates with the same agar-based broth media and incubated for 48 h at 36 ± 1 °C in order to quantify the microbial load. Bacterial colonies were then counted and expressed as colony-forming units per mL (cfu/mL). Concerning the enumeration of bacterial colonies, a bacterial score (BS) was obtained by classifying the enumerated bacterial colonies according to the following scheme:
- Class 0: BS ≤ 103 cfu/mL
- Class 1: ≤ 103 cfu/mL BS ≤ 105 cfu/mL
- Class 2: ≤ 105 cfu/mL BS ≤1 07 cfu/mL
- Class 3: BS > 107 cfu/mL
Search for specific anaerobic bacteria : Each sample was seeded on 2 different plates (BBE and brucella blood agar) to determine the eventual presence of anaerobic microbial strains. Seeded plates were placed in the oxygen-free vessels and incubated at 36 ± 1 °C for 7 days. After this period, the plates were analyzed to evaluate the presence of bacterial colonies. In positive cases, individual colonies were reseeded to achieve a pure bacterial culture suitable for biochemical recognition. For evaluation of the growth of specific anaerobic bacteria, the classes of “growth” and “no growth” were established, depending on whether bacterial growth was observed.
Statistical analysis
Data were expressed as mean ± standard deviation (SD) of BS values, where available. The Mann–Whitney U test for independent samples was used to evaluate the difference between the C-group and H-group. In the case of categorical data, that is growth/no growth classes and absence/presence classes, data were organized in contingency tables and analyzed by the Fisher exact test. A value of P ≤ 0.05 was taken as statistically significant. Statistical analysis was performed using OpenStat version 26.03.2012 (www.statprograms4u.com).
Results
The results of the microbiological analysis are summarized in Tables 1–4. Table 1 reports mean ± SD values for BSs calculated from the cfus developed under different conditions. The mean ± SD score of bacteria seeding calculated on TSA was 2.000 ± 1.080 and 1.462 ± 1.198 in the H-group and C-group, respectively. The mean ± SD score of bacteria-seeding calculated on MRS was 1.462 ± 1.050 and 1.077 ± 1.320 in the H-group and C-group, respectively. In all cases, the P values were not statistically significant, meaning that no statistically significant differences were observed between the H-group and the C-group. In more detail, the total bacterial load developed after seeding BPW solutions that had been in contact with suture thread segments on TSA plates and the Lactobacillus spp. developed after seeding BPW solutions that had been in contact with suture thread segments were comparable between groups. Table 2 is the contingency table summarizing data resulting from inoculation on BRU plates. In this case too, no statistically significant differences between the H-group and C-group were observed (P = 0.411). Tables 3 and 4 are contingency tables summarizing data resulting from scraping suture thread segments on TSA plates and MRS plates, respectively. Again, no statistically significant differences between the H-group and C-group were observed. Inoculation in BBE under anaerobic conditions produced negative results (no growth) for all samples and the control. Figure 2 illustrates Petri dishes after the optional development of bacterial colonies.
Discussion
The present study aimed to evaluate the bacterial load on suture threads after their removal in 2 different situations. Patients were assigned either to a chlorhexidine mouthwash or to a zinc one. Among the suture thread samples taken from the 13 patients who used the mouthwash containing chlorhexidine (C-group), 7 showed a high bacterial load (BS = 2 or 3) with the presence of Lactobacillus spp, in 5 cases; 2 of them presented a poor bacterial load (BS = 1); and 4 of them did not present any appreciable microbial colonization (BS = 0). The search for specific anaerobic strains, when positive (3 samples), resulted in establishing the presence of Fusobacterium varium (1 occurrence), Actinomyces meyeri (1 occurrence) and Streptococcus intermedius (1 occurrence). Of the 13 suture thread samples taken from patients who used a mouthwash containing Zn-nHAp/Zn-PCA, 10 showed a high bacterial load (BS = 2 or 3) associated with the presence of Lactobacillus spp., 1 had a moderate bacterial load (BS = 1), and 2 did not show any appreciable microbial colonization. The search for specific anaerobic strains, when positive (6 samples), resulted in establishing the presence of Actinomyces meyeri (3 occurrences), Bifidobacterium spp. (1 occurrence), Staphylococcus saccharolyticus (1 occurrence) and Actinomyces viscosus (1 occurrence).



† The total number of suture threads in the H-group was 12 instead of 13 because 1 thread was too short to be cut into segments for scraping on TSA plates.

† The total number of suture threads in the H-group was 12 instead of 13 because 1 thread was too short to be cut into segments for scraping on MRS plates.
Mean ± SD values for BSs calculated from the cfus developed under different conditions. From left to right, the columns report data concerning the quantification of total bacterial load and Lactobacillus spp., respectively, after seeding the BPW solutions that had been in contact with suture thread segments. Growth media were TSA and MRS agar, respectively.
Table 2
Contingency table summarizing data resulting from inoculation on BRU.
Table 3
summarizing data resulting from scraping on TSA.
Table 4
Contingency table summarizing data resulting from scraping on MRS.
In vitro studies have already demonstrated that hydroxyapatite shows antimicrobial activity; for example, Tin-Oo et al. reported the efficacy of HAp against Streptococcus mutans.15Yang Z, Suomalainen T, Mäyrä-Mäkinen A, Huttunen E. Antimicrobial activity of 2-pyrrolidone-5-carboxylic acid produced by lactic acid bacteria.
→ J Food Protect. 1997 Jul;60(7):786–90. The antimicrobial activity of nHAp was also investigated when intercalated by several metal ions, including zinc ions,16Swetha M, Sahithi K, Moorthi A, Saranya N, Saravanan S, Ramasamy K, Srinivasan N, Selvamurugan N. Synthesis, characterization, and antimicrobial activity of nano-hydroxyapatite-zinc for bone tissue engineering applications.
→ J Nanosci Nanotechnol. 2012 Jan;12(1):167–72.17Kim TN, Feng QL, Kim JO, Wu J, Wang H, Chen GC, Cui FZ. Antimicrobial effects of metal ions (Ag+, Cu2+, Zn2+) in hydroxyapatite.
→ J Mater Sci Mater Med. 1998 Mar;9(3):129–34. and shown to be higher than that of nHAp alone. Furthermore, zinc ions are known to possess antimicrobial properties, and the activity of zinc in the oral cavity has been well documented.18Lynch RJ. Zinc in the mouth, its interactions with dental enamel and possible effects on caries; a review of the literature.
→ Int Dental J. 2011 Aug;61 Suppl 3:46–54.19Hannig C, Basche S, Burghardt T, Al-Ahmad A, Hannig M. Influence of a mouthwash containing hydroxyapatite microclusters on bacterial adherence in situ.
→ Clin Oral Investig. 2013 Apr;17(3):805–14. PCA possesses a certain antimicrobial activity as well, as demonstrated by Yang et al., who tested it in in vivo studies against several microorganisms.20Yang Z, Suomalainen T, Mäyrä-Mäkinen A, Huttunen E. Antimicrobial activity of 2-pyrrolidone-5-carboxylic acid produced by lactic acid bacteria.
→ J Food Protect. 1997 Jul;60(7):786–90. Moreover, PCA increases the solubility rate of zinc ions in the saliva such that its antibacterial action is readily exerted.
Oral care products based on the association of Zn-nHAp and Zn-PCA could create a combination of 3 active ingredients that are very well tolerated and maintain the same efficacy of chlorhexidine against bacteria. Indeed, the present study demonstrated that mouthwashes containing Zn-nHAp and Zn-PCA represent a valid alternative to mouthwashes containing chlorhexidine. They do not exert the typical side effects of chlorhexidine, such as alteration of taste perception, tooth staining, tongue discoloration, and desquamation and soreness of the oral mucosa, while maintaining at least its same antibacterial efficacy.21Flötra L, Gjermo P, Rölla G, Waerhaug J. Side effects of chlorhexidine mouth washes.
→ Scand J Dent Res. 1971;79(2):119–25. Also, Marchetti et al., in a clinical comparative trial, found a similar effect of inhibiting plaque regrowth between zinc and chlorhexidine mouthwashes.22Marchetti E, Casalena F, Capestro A, Tecco S, Mattei A, Marzo G. Efficacy of two mouthwashes on 3-day supragingival plaque regrowth: a randomized crossover clinical trial.
→ Int J Dent Hyg. 2017 Feb;15(1):73–80. Further studies are needed to better understand whether this new antimicrobial mouthwash could substitute chlorhexidine as the gold standard in promoting wound healing after surgery owing to its antimicrobial effect and no side effects.
Conclusion
Within the limitations of this study, the mouthwash containing Zn-nHAp and Zn-PCA was found to have similar antibacterial efficacy to the mouthwash containing chlorhexidine, but without exerting the typical side effects of chlorhexidine itself. These results should be interpreted with caution owing to the small sample of the study and the few kinds of bacteria analyzed.
-
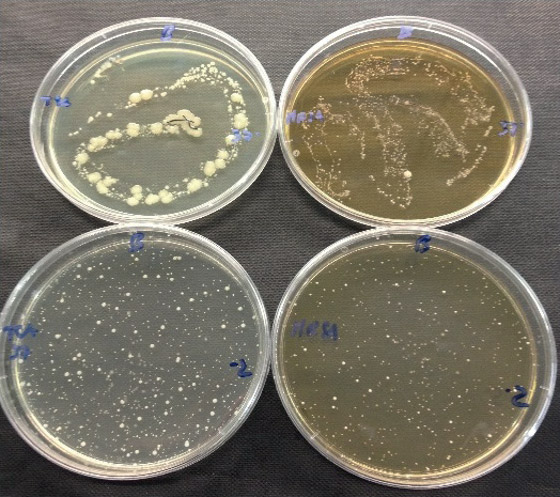
- A. Chlorhexidine
-
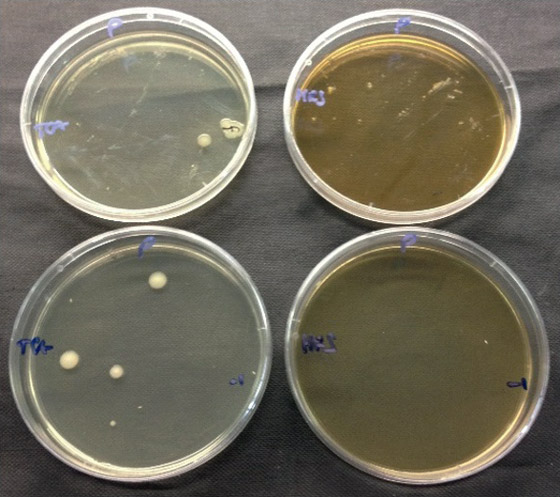
- B. Chlorhexidine
-
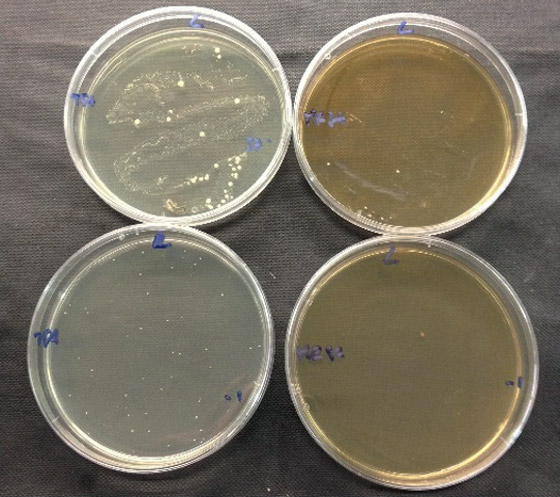
- C. Hydroxyapatite
-
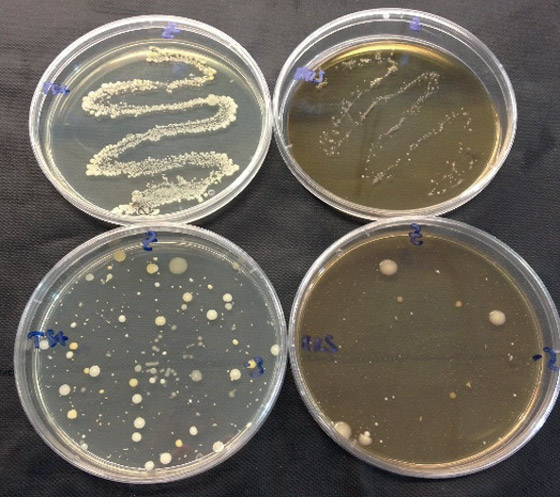
- D. Hydroxyapatite
-
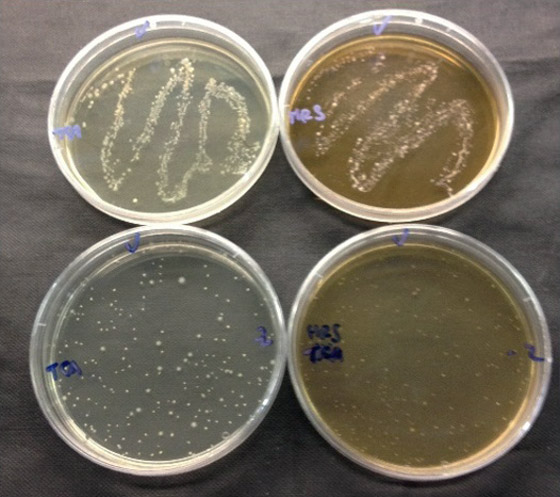
- E. Hydroxyapatite
-
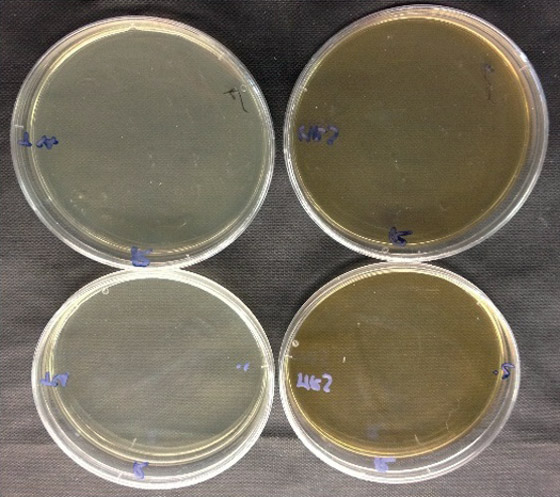
- F. Control
Petri dishes after the optional development of bacterial colonies. A and B come from patients who used a mouthwash containing chlorhexidine for 7 days after surgery. C, D and E come from patients who used a mouthwash containing Zn-nHAp and Zn-PCA for 7 days after surgery. F represents control plates. Within each photograph, the upper left and right plates correspond to suture thread segments scraped on TSA for the growth of mesophilic bacteria and MRS agar for the growth of Lactobacillus spp., respectively. The bottom left and right plates correspond to the quantitative analysis of mesophilic bacteria on TSA and Lactobacillus spp. on MRS agar, respectively.
Competing interests
The authors declare that they have no conflict of interest regarding the present research.
Acknowledgments
The authors are grateful to the Chemical Center, Bologna, Italy, for technical support and to Drs. Alice Borghini and Daniele Pietra for statistical analysis and manuscript drafting.
For their important contribution to this investigation, the authors are also very grateful to
- Prof. Ugo Covani, Department of Surgical, Medical, Molecular and Critical Area Pathology, University of Pisa, Pisa, Italy; and Tuscan Stomatologic Institute, Foundation for Dental Clinic, Research and Continuing Education, Versilia General Hospital, Lido di Camaiore, Italy;
- Dr. Andrea Butera, Department of Surgical Sciences, Dental and Maxillofacial Department, University of Pavia, Pavia, Italy; and
- Drs. Dario Bertossi, Antonio Iurlaro and Federico Gelpi, Department of Surgical Sciences and Dental and Maxillofacial Department, University of Verona, Verona, Italy.
Interview
with Saverio Cosola
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Otten JE, Wiedmann-Al-Ahmad M, Jahnke H, Pelz K. Bacterial colonization on different suture materials—a potential risk for intraoral dentoalveolar surgery. → J Biomed Mater Res B Appl Biomater. 2005 Jul;74(1):627–35. |
| 2. | ↑ | Katz S, Izhar M, Mirelman D. Bacterial adherence to surgical sutures. A possible factor in suture induced infection. → Ann Surg. 1981 Jul;194(1):35–41. |
| 3, 10. | ↑ | Banche G, Roana J, Mandras N, Amasio M, Gallesio C, Allizond V, Angeretti A, Tullio V, Cuffini AM. Microbial adherence on various intraoral suture materials in patients undergoing dental surgery. → J Oral Maxillofac Surg. 2007 Aug;65(8):1503–7. |
| 4. | ↑ | Pons-Vicente O, López-Jiménez L, Sánchez-Garcés MA, Sala-Pérez S, Gay-Escoda C. A comparative study between two different suture materials in oral implantology. → Clin Oral Implants Res. 2011 Mar;22(3):282–8. |
| 5. | ↑ | Harnet JC, Le Guen E, Ball V, Tenenbaum H, Ogier J, Haikel Y, Vodouhe C. Antibacterial protection of suture material by chlorhexidine-functionalized polyelectrolyte multilayer films. → J Mater Sci Mater Med. 2009 Jan;20(1):185–93. |
| 6. | ↑ | Brown AR, Papasian CJ, Shultz P, Theisen FC, Shultz RE. Bacteremia and intraoral suture removal: can an antimicrobial rinse help? → J Am Dent Assoc. 1998 Oct;129(10):1455–61. |
| 7. | ↑ | Jones CG. Chlorhexidine: is it still the gold standard? → Periodontol 2000. 1997 Oct;15:55–62. |
| 8. | ↑ | Addy M, Sharif N, Moran J. A nonstaining chlorhexidine mouthwash? Probably not: a study in vitro. → Int J Dent Hyg. 2005 May;3(2):59–63. |
| 9. | ↑ | Bagis B, Baltacioglu E, Özcan M, Ustaomer S. Evaluation of chlorhexidine gluconate mouthrinse-induced staining using a digital colorimeter: an in vivo study. → Quintessence Int. 2011 Mar;42(3):213–23. |
| 11. | ↑ | Helms JA, Della-Fera MA, Mott AE, Frank ME. Effects of chlorhexidine on human taste perception. → Arch Oral Biol. 1995 Oct;40(10):913–20. |
| 12. | ↑ | Frank ME, Gent JF, Hettinger TP. Effects of chlorhexidine on human taste perception. → Physiol Behav. 2001 Sep 1–15;74(1–2):85–99. |
| 13. | ↑ | . Marinone MG, Savoldi E. Chlorhexidine and taste. Influence of mouthwashes concentration and of rinsing time. → Minerva Stomatol. 2000 May;49(5):221–6. |
| 14. | ↑ | Russell AD. Biocide use and antibiotic resistance: the relevance of laboratory findings to clinical and environmental situations. → Lancet Infect Dis. 2003 Dec;3(12):794–803. |
| 15, 20. | ↑ | Yang Z, Suomalainen T, Mäyrä-Mäkinen A, Huttunen E. Antimicrobial activity of 2-pyrrolidone-5-carboxylic acid produced by lactic acid bacteria. → J Food Protect. 1997 Jul;60(7):786–90. |
| 16. | ↑ | Swetha M, Sahithi K, Moorthi A, Saranya N, Saravanan S, Ramasamy K, Srinivasan N, Selvamurugan N. Synthesis, characterization, and antimicrobial activity of nano-hydroxyapatite-zinc for bone tissue engineering applications. → J Nanosci Nanotechnol. 2012 Jan;12(1):167–72. |
| 17. | ↑ | Kim TN, Feng QL, Kim JO, Wu J, Wang H, Chen GC, Cui FZ. Antimicrobial effects of metal ions (Ag+, Cu2+, Zn2+) in hydroxyapatite. → J Mater Sci Mater Med. 1998 Mar;9(3):129–34. |
| 18. | ↑ | Lynch RJ. Zinc in the mouth, its interactions with dental enamel and possible effects on caries; a review of the literature. → Int Dental J. 2011 Aug;61 Suppl 3:46–54. |
| 19. | ↑ | Hannig C, Basche S, Burghardt T, Al-Ahmad A, Hannig M. Influence of a mouthwash containing hydroxyapatite microclusters on bacterial adherence in situ. → Clin Oral Investig. 2013 Apr;17(3):805–14. |
| 21. | ↑ | Flötra L, Gjermo P, Rölla G, Waerhaug J. Side effects of chlorhexidine mouth washes. → Scand J Dent Res. 1971;79(2):119–25. |
| 22. | ↑ | Marchetti E, Casalena F, Capestro A, Tecco S, Mattei A, Marzo G. Efficacy of two mouthwashes on 3-day supragingival plaque regrowth: a randomized crossover clinical trial. → Int J Dent Hyg. 2017 Feb;15(1):73–80. |





Leave a Reply
Be the First to Comment!