Buccal plate reconstruction with an intentionally exposed nonresorbable membrane: 1 year after loading results of a prospective study
December 7, 2017 / Categories: Digital Dentistry, Implant Dentistry

Tallarico, Marco

Luongo, Roberto

Bianco, Giuseppe

Bugea, Calogero
Abstract
Objective
The aim of this study was to investigate the barrier effect of a high-density polytetrafluoroethylene (d-PTFE) membrane left intentionally exposed in post-extraction sockets grafted with an allograft biomaterial and removed after 5 weeks.
Materials and methods
Forty-seven hopeless teeth were extracted. Residual sockets were grafted with an allograft biomaterial and covered with a d-PTFE membrane. Six months later, 47 submerged implants were installed. Four months later, implants were uncovered and a temporary restoration was delivered. Outcomes were implant and prosthetic survival rate, complications, alveolar ridge width measurement, marginal bone loss (MBL) and gingival recession. Follow-up ranged from 1 to 3 years. The buccal plate was measured after tooth extraction (BPS), at implant placement (BPW) and at implant uncovering/loading (BBT).
Results
No deviation from the original protocol occurred. All of the implants were osseointegrated. None of the prostheses failed and no complications occurred during the follow-up. The mean BPS at the midpoint was 6.5 ± 1.5 mm (at the time of extraction; T0). At time of implant placement
(T1), the mean BPW was 6.30 ± 1.30 mm, with a crestal reduction of 0.19 ± 0.34 mm (P = 0.0006). At implant uncovering/loading, the mean BBT was 1.7 ± 0.5 mm. One year after loading (T3), periapical radiographs revealed a mean MBL of 0.62 ± 0.16 mm, compared with T1. One year after initial loading there was no buccal gingival recession compared with T0, with a mean soft-tissue creeping of 0.8 ± 0.2 mm.
Conclusion
Buccal plate reconstruction with an intentionally exposed nonresorbable membrane is an effective and easy procedure for regeneration of a resorbed buccal bone plate.
Keywords
Dental implants, biomaterials, guided bone regeneration, dense PTFE.
Introduction
A significant 3-D remodeling of the bone crest, especially horizontally, always occurs after the extraction of a tooth.1Tallarico M, Xhanari E, Pisano M, De Riu G, Tullio A, Meloni SM. Single post-extractive ultra-wide 7 mm-diameter implants versus implants placed in molar healed sites after socket preservation for molar replacement: 6-month post-loading results from a randomised controlled trial.
→ Eur J Oral Implantol. 2016 Oct;9(3):263–75. This makes it difficult to insert an implant, especially in the frontal areas, where residual bone thickness is fundamental for optimal esthetic results. In order to reduce this contraction, a socket preservation technique entailing the insertion of a bone graft and of a resorbable membrane inside the socket, followed after 4–6 months by the positioning of a delayed implant, has usually been proposed.2Canullo L, Wiel Marin G, Tallarico M, Canciani E, Musto F, Dellavia C. Histological and histomorphometrical evaluation of postextractive sites grafted with mg-enriched nano-hydroxyapatite: a randomized controlled trial comparing 4 versus 12 months of healing.
→ Clin Implant Dent Relat Res. 2016 Oct;18(5):973–83.3Tallarico M, Xhanari E, Pisano M, Gatti F, Meloni SM. Molar replacement with 7 mm wide diamieter implants: to place the implant immediately or to wait 4 months after socket preservation? 1 year loading results from a randomized controlled trial.
→ Eur J Oral Implantol. 2017 Sep;10(2):169–78. However, such a technique does not always have predictable results, especially when the buccal plate of the alveolar socket is missing after tooth extraction.
Guided bone regeneration (GBR) has been proposed as a possible alternative for patients with severe horizontal bone atrophy, to overcome the drawback of bone block techniques.4Buser D, Ingimarsson S, Dula K, Lussi A, Hirt HP, Belser UC. Long-term stability of osseointegrated implants in augmented bone: a 5-year prospective study in partially edentulous patients.
→ Int J Periodontics Restorative Dent. 2002 Apr;22(2):109–17.5Urban IA, Jovanovic S, Lozada JL. Vertical ridge augmentation using guided bone regeneration (GBR) in three clinical scenarios prior to implant placement: a retrospective study of 35 patients 12 to 72 months after loading.
→ Int J Oral Maxillofac Implants. 2009 May-Jun;24(3):502–10. In order to protect the clot and prevent the invasion of the clot by nonosteogenic cells, maintaining an adequate biological space for the regeneration of bone tissue, the use of either nonresorbable or resorbable membranes has been proposed.6Urban IA, Caplanis N, Lozada JL. Simultaneous vertical guided bone regeneration and guided tissue regeneration in the posterior maxilla using recombinant human plateletderived growth factor: a case report.
→ J Oral Implantol. 2009 Oct;35(5):251–6. Expanded polytetrafluoroethylene (e-PTFE) membranes and resorbable membranes classically require soft-tissue coverage or primary closure to prevent soft-tissue ingrowth, bacterial contamination, infection, membrane migration, early membrane degradation, and graft exposure. The major feature of the e-PTFE membrane is macroporosity, which is believed to enhance regeneration by improving wound stability.7Carbonell JM, Martin IS, Santos A, Pujol A, Sanz-Moliner JD, Nart J. High-density polytetrafluoroethylene membranes in guided bone and tissue regeneration procedures: a literature review.
→ Int J Oral Maxillofac Surg. 2014 Jan;43(1):75–84. Nevertheless, its main drawback is that an early bacterial infection can occur, affecting the outcome of the regeneration.
High-density polytetrafluoroethylene (d-PTFE) membranes offer an alternative to e-PTFE or resorbable membranes.8Waasdorp J, Feldman S. Bone regeneration around immediate implants utilizing a dense polytetrafluoroethylene membrane without primary closure: a report of 3 cases.
→ J Oral Implantol. 2013 Jun;39(3):355–61. Epub 2011 Sep 9.9Hoffmann O, Bartee BK, Beaumont C, Kasaj A, Deli G, Zafiropoulos GG. Alveolar bone preservation in extraction sockets using non-resorbable dPTFE membranes: a retrospective non-randomized study.
→ J Periodontol. 2008 Aug;79(8):1355–69.10Barber HD, Lignelli J, Smith BM, Bartee BK. Using a dense PTFE membrane without primary closure to achieve bone and tissue regeneration.
→ J Oral Maxillofac Surg. 2007 Apr;65(4):748–52.11Monteiro AS, Macedo LG, Macedo NL, Balducci I. Polyurethane and PTFE membranes for guided bone regeneration: histopathological and ultrastructural evaluation.
→ Med Oral Patol Oral Cir Bucal. 2010 Mar;15(2):e401–6. A d-PTFE membrane is made of 100% pure medical-grade bio-inert PTFE, which is nonporous, dense, nonexpanded and nonpermeable.12Tallarico M, Xhanari E, Pisano M, Gatti F, Meloni SM. Molar replacement with 7 mm wide diamieter implants: to place the implant immediately or to wait 4 months after socket preservation? 1 year loading results from a randomized controlled trial.
→ Eur J Oral Implantol. 2017 Sep;10(2):169–78.13Urban IA, Jovanovic S, Lozada JL. Vertical ridge augmentation using guided bone regeneration (GBR) in three clinical scenarios prior to implant placement: a retrospective study of 35 patients 12 to 72 months after loading.
→ Int J Oral Maxillofac Implants. 2009 May-Jun;24(3):502–10. The thickness of the various commercially available membranes ranges from 0.13 to 0.25 mm and their low porosity ranges from 0.2 to 0.3 mm; e-PTFE membranes have a similar thickness, but a higher porosity (5–30 nm).14Laurito D, Cugnetto R, Lollobrigida M, Guerra F, Vestri A, Gianno F, Bosco S, Lamazza L, De Biase A. Socket preservation with d-PTFE membrane: histologic analysis of the newly formed matrix at membrane removal.
→ Int J Periodontics Restorative Dent. 2016 Nov/Dec;36(6):877–83. The indications for d-PTFE membranes are similar to those for e-PTFE, but the different porosity of the first avoids any inflammation of the surrounding soft tissue in case of accidental exposure.15Bartee BK. Evaluation of a new polytetrafluoroethylene guided tissue regeneration membrane in healing extraction sites.
→ Compend Contin Educ Dent. 1998 Dec;19(12):1256–8, 1260, 1262–4. There is limited clinical and histological evidence for the use of d-PTFE membranes at present, with some indications for guided tissue regeneration and GBR, especially in immediate implants and fresh extraction sockets.16Carbonell JM, Martin IS, Santos A, Pujol A, Sanz-Moliner JD, Nart J. High-density polytetrafluoroethylene membranes in guided bone and tissue regeneration procedures: a literature review.
→ Int J Oral Maxillofac Surg. 2014 Jan;43(1):75–84.
The aim of the present prospective study was to investigate the barrier effect of a d-PTFE membrane left intentionally exposed in post-extraction sockets grafted with an allograft biomaterial and removed after 5 weeks. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement for improving the quality of observational studies.17Elm von E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies.
→ BMJ. 2007 Oct 20;335(7624):806–8.
Materials and methods
This prospective study was conducted in a private dental practice from February 2012 to March 2016. Forty-three patients of both sexes requiring 47 implant-supported single-crown restorations to rehabilitate an esthetic area with a hopeless tooth with an Elian type II socket (facial soft tissue was present, but the buccal plate was partially missing after extraction of the tooth),18Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classification and repair technique.
→ Pract Proced Aesthet Dent. 2007 Mar;19(2):99–104; quiz 106. aged 18 years or older and able to sign an informed consent form, were enrolled and treated consecutively. This was provided that they fulfilled the inclusion criteria and gave their written consent to take part in the study. The buccal plate was defined as partially missing when the distance from the gingival margin to the most coronal part of the buccal plate was greater than 4 mm, even in only 1 of the 3 reference points (mesial, distal and midpoint), while both the mesial, distal and the palatal bony walls were present at a distance of less than 4 mm from the palatal gingival margin.
The exclusion criteria were positive medical findings (such as stroke, recent myocardial infarction, severe bleeding disorder, uncontrolled diabetes, or cancer), psychiatric therapy, pregnancy or nursing, smoking more than 10 cigarettes per day, untreated periodontitis, acute or chronic infections of the adjacent tissue or natural dentition, previous radiotherapy of the oral and maxillofacial region within the last 5 years, absence of teeth in the opposing jaw, severe clenching or bruxism, severe maxillomandibular skeletal discrepancy, and poor oral hygiene (full-mouth bleeding and a full-mouth plaque index of higher than or equal to 25%). Patients were informed about the clinical procedures, the materials to be used, the benefits, potential risks and complications, as well as any follow-up evaluations required for the clinical study. The medical history of the enrolled patients was collected and study models were produced. Preoperative radiographs, including periapical and panoramic radiographs, and computed tomography or cone beam computed tomography scans, were obtained for initial screening and evaluation.
All procedures were conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2013, for biomedical research involving human subjects. One clinician (RL) performed all of the surgical and prosthetic procedures, and one dental laboratory manufactured all of the restorations.
Surgical and prosthetic protocols
The teeth were atraumatically extracted with the aid of a periotome and atraumatic elevators (PT1 and EPTSMS, Hu-Friedy Italy, Milan, Italy) to reduce trauma to the bony walls (Fig. 1). After accurate debridement of the socket with a curette (CL866, Hu-Friedy), the distance from the gingival margin to the residual buccal or palatal bone plate was measured with the aid of a periodontal probe (PCPUNC15, Hu-Friedy, Chicago, Ill., U.S.) in order to verify the degree of bone crest resorption.
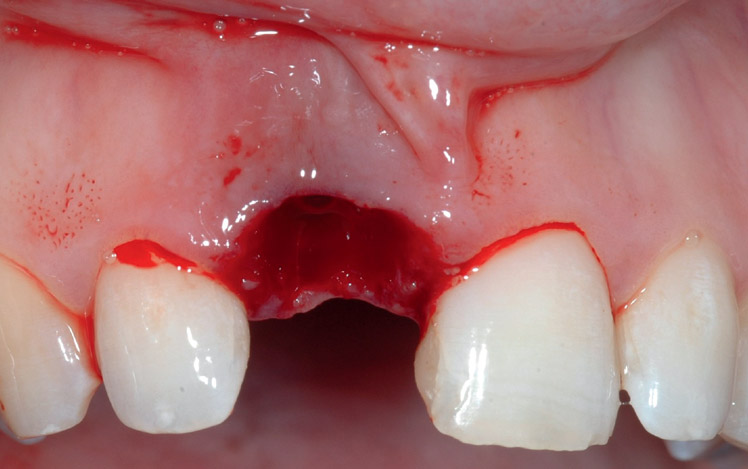


Clinical view of the central incisor before (a,b) and after extraction (c).
If the distance was more than 5 mm, a nonresorbable d-PTFE membrane (Cytoplast TXT-200, De Ore, Negrar, Italy), adequately cut into an ice-cream cone shape,19Tan-Chu JH, Tuminelli FJ, Kurtz KS, Tarnow DP. Analysis of buccolingual dimensional changes of the extraction socket using the “ice cream cone” flapless grafting technique.
→ Int J Periodontics Restorative Dent. 2014 May-Jun;34(3):399–403. was introduced into the socket corresponding to the area of the missing buccal plate, in order to prevent soft-tissue proliferation. Subsequently, the d-PTFE membrane was inserted into the socket with the narrower part facing the buccal soft tissue and stabilized with a corticocancellous particulate allograft biomaterial (Puros, Zimmer Dental, Carlsbad, Calif., U.S.), placed inside the socket using a curved stainless- steel graft delivery syringe with a 4.5 mm funnel opening (ACE Surgical Supply, Brockton, Mass., U.S.; Fig. 2a). Then the wider part of the membrane was overturned above the bone graft and sutured with a 5-0 PTFE mattress suture (Cytoplast, De Ore) to the palatal and buccal mucosa, leaving it intentionally exposed (Fig. 2b). The patient was placed on an antibiotic regimen of 1 g of amoxicillin and clavulanic acid (Augmentin, GlaxoSmithKline, Verona, Italy) twice a day, starting the day before the surgery and continuing 7 days after, and an analgesic (ibuprofen, 600 mg) was prescribed if needed. All of the patients were instructed to rinse with 0.12% chlorhexidine 3 times a day for 1 min after brushing their teeth. No special indications were recommended for the area of the graft.


Allograft inserted into the socket after d-PTFE membrane placement (a) and suturing (b) at T0.
After 5 weeks, the membrane was removed without the need for anesthetic, leaving the exposed site to heal by secondary intention (Fig. 3).
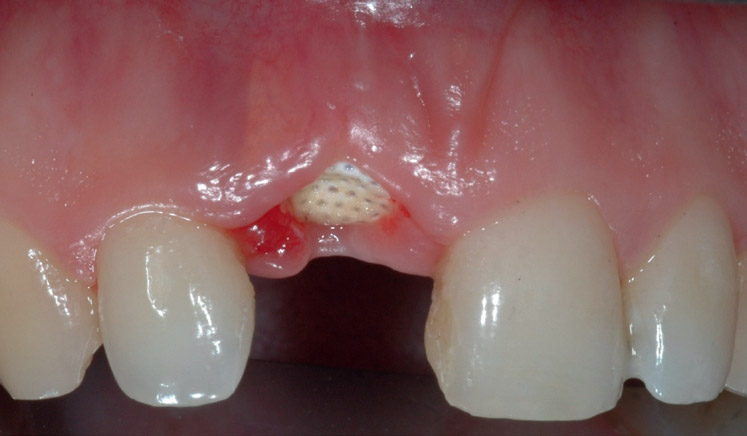

Membrane after 5 weeks (a). Well-vascularized osteoid tissue was evident after removal (b).
After 6 months, a crestal incision was performed, then a full-thickness flap was elevated, and an implant of 4.0 mm in width and 11.5 mm in length was placed according to the manufacturer’s instruction (Full OSSEOTITE Tapered Natural, Implant Innovations, Palm Beach Gardens, Fla., U.S.; Fig. 4).

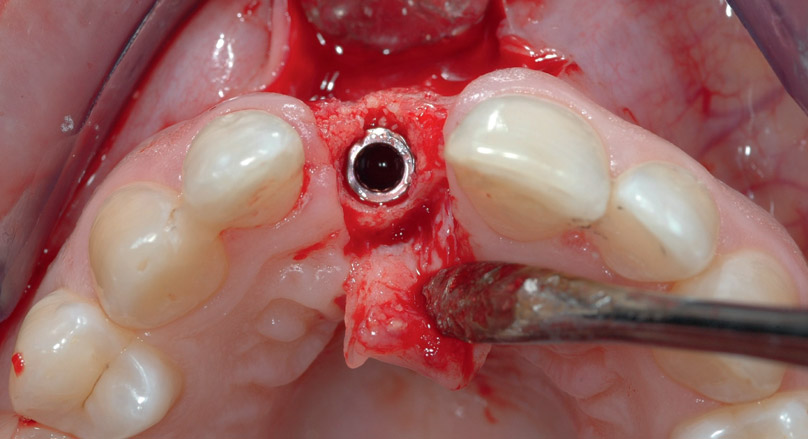
Implant placement at T1: The ridge appeared well formed (a), and the implant could be placed in an ideal position (b).
The implant was submerged and the flap was sutured using a resorbable suture (4-0; Vicryl, Ethicon, Ohio, U.S.), obtaining a primary closure healing. After 4 months of healing, the implant was uncovered and the provisional prosthesis was immediately delivered. Four months later, the definitive metal-free crown was delivered and the occlusion was adjusted (Fig. 5). The patients were enrolled in a strict hygiene program and were followed up to 3 years after initial loading.
The primary outcome measures were the success rates of the implants and prostheses and any surgical and prosthetic complications that occurred during the entire follow-up. An independent blinded assessor recorded all of the measurements and collected the related data according to the following criteria:
- An implant was considered a failure if it presented with any mobility, tested by tapping or rocking the implant head with a hand instrument and/or any signs of radiolucency and/or fracture on an intraoral radiograph taken with the paralleling technique strictly perpendicular to the implant–bone interface. The implant stability was assessed at initial loading and at each follow-up.
- A prosthesis was considered a failure if it needed to be replaced with a different type of prosthesis.
- Complications: Any biological (pain, swelling, suppuration, etc.) and/or mechanical (fracture of the framework and/or the veneering material, screw loosening, etc.) complication was considered.

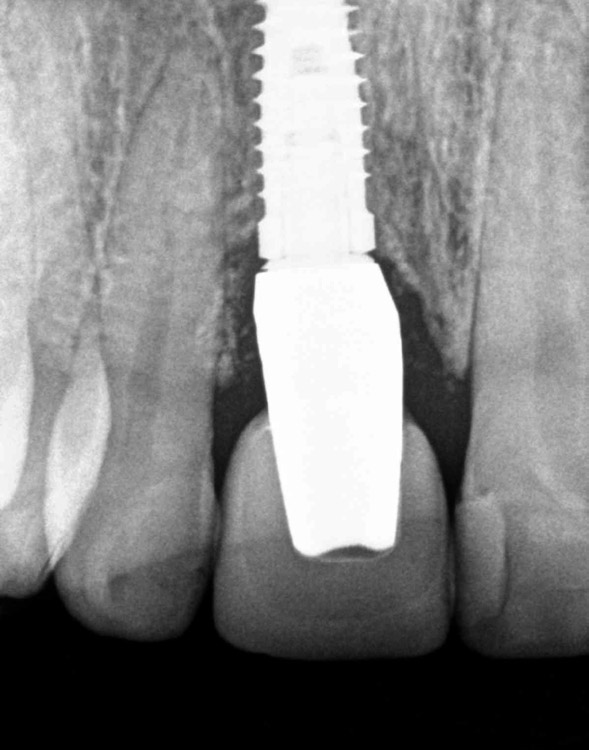
The final restoration delivery at T2 showed a good esthetic result (a) and marginal periimplant bone preserved at T3 (b).
The secondary outcome measures were dimensional changes in the alveolar ridge width, marginal bone level changes and gingival recession.
– The alveolar ridge width was measured to the nearest millimeter using a periodontal probe (PCPUNC156, Hu-Friedy) at the time of tooth extraction (T0), at implant placement (6 months later; T1), and at the time of implant uncovering/loading (4 months later; T2). The same clinicians who performed the tooth extractions and implant placement performed all of the measurements as follows: After tooth extraction (T0), the buccolingual dimension of the alveolar crest was measured from the inner part of the buccal gingival margin to the inner part of the palatal soft tissue at the mesiodistal midpoint of the socket (BPS), 3 mm subgingivally, using a periodontal probe (PCPUNC 15; Fig. 6). Six months later, at (T1), a crestal incision was done and a full-thickness flap was elevated in order to expose the edentulous ridge. Then the alveolar ridge thickness was measured from the buccal to the palatal side at the mesiodistal midpoint (BPW), as previously described (Fig. 7). Four months later, at (T2), the horizontal width of the ridge was measured buccally, starting from the outer part of the implant platform (BBT; Fig. 8).
-

-
Fig. 6
BPS: the distance from the inner part of the buccal gingival margin to the inner part of the palatal soft tissue at the mesiodistal midpoint of the socket 3 mm subgingivally at T0.
-
-
Fig. 7
BPW: the alveolar ridge thickness from the buccal to the palatal side at the mesiodistal midpoint at T1.
-
-
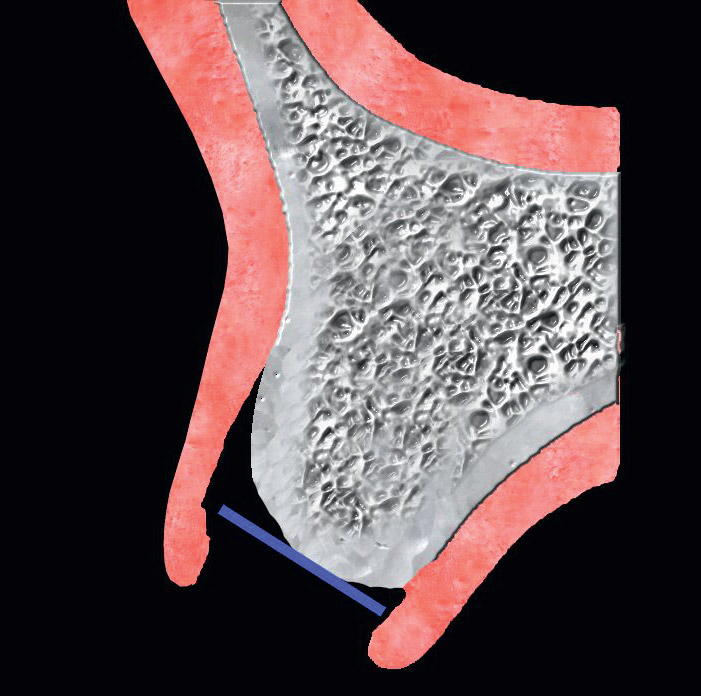
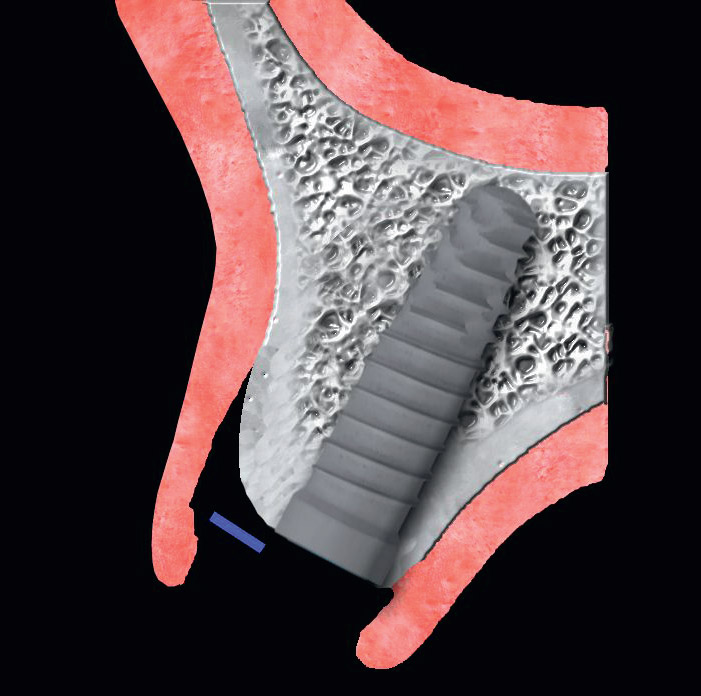
Fig. 8
BBT: the horizontal width of the ridge measured from the outer part of the implant platform to the buccal bone at T2.
– Marginal bone level changes were assessed using intraoral digital periapical radiographs taken with the paralleling technique at (T1) and 1 year after loading (T3), using a customized holder. The radiographs were accepted or rejected for evaluation based on the clarity of the implant threads. All readable radiographs were viewed in an image analysis program (Kodak Digital Imaging Software, Version 6.11.7.0, Eastman Kodak, Rochester, N.Y., U.S.) on a 24-in LCD screen (iMac, Apple, Cupertino, Calif., U.S.) and evaluated under standardized conditions (ISO 12646:2004). The software was calibrated for every image using the known implant diameter or length. The distance from the most coronal margin of the implant collar and the top of the bone crest was taken as marginal bone level. The average radiographic values of the mesial and distal measurements were taken for each implant at the time of implant placement and 6 months later. The difference between the marginal bone levels at various time points was taken as marginal bone loss (MBL). An independent radiologist performed all of the bone measurements.
– Gingival recession was evaluated using a reference line connecting the midfacial gingival level of the 2 adjacent teeth. The changes in the gingival margin of the implant restoration were evaluated before extraction (T0) and at T3. All data analysis was carried out according to a pre-established analysis plan using software (IBM SPSS Statistics for Macintosh, Version 22.0, IBM, Armonk, N.Y., U.S.). Descriptive analysis was performed using mean and standard deviation. Comparison of the means was performed by paired tests. A biostatistician with expertise in dentistry analyzed the data.
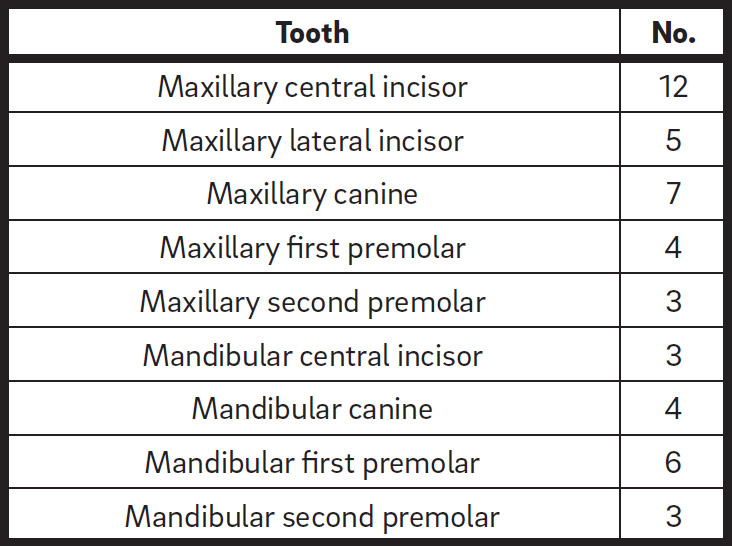
Table 1
Extracted teeth.
Results
In total, 47 teeth were extracted in 43 patients, 26 women and 17 men, with a mean age of 54 years (Table 1). At the last follow-up, no dropout and no deviation from the original protocol occurred. All 47 implants were osseointegrated and none of the prostheses failed. The follow-up ranged from a minimum of 1 year to a maximum of 3 years after loading.
In all of the treated cases, there was no dehiscence of the buccal or palatal portion of the implant at the moment of its exposure. There was no site infection either before or after the removal of the nonresorbable membrane, and no patient presented with edema or ecchymosis post-implant surgery.
The mean BPS at the midpoint was 6.5 ± 1.5 mm at T0. At T1, the mean BPW was 6.30 ± 1.30 mm, with a crestal reduction of 0.19 ± 0.34 mm (P = 0.0006), while at T2, the mean BBT was 1.7 ± 0.5 mm. At T3, periapical radiographs revealed a marginal bone loss of 0.62 ± 0.16 mm in the area surrounding the implant, compared with T0. At T3, a mean soft-tissue gain of 0.8 ± 0.2 mm was recorded, with no buccal gingival recession compared with T0.
Discussion
This study has presented the results of a new technique for the spontaneous regeneration of the missing buccal plate of a dental socket that avoids the ingrowth of soft tissue inside it and regenerates the previously resorbed buccal cortical bone. This technique may avoid invasive further regenerative techniques, thus notably reducing treatment time without impairing the esthetic results, the predictability of the implant treatment or patient satisfaction.
A limiting situation for post-extraction implants, especially in areas of high esthetic concern, is the resorption of the buccal bone plate, which is fundamental for soft-tissue stability in the area surrounding the fixture and therefore for long-term esthetic results. The reconstruction of such a bone wall almost always requires an additional regenerative surgery, usually invasive for the patient, and precedes the prosthetically guided insertion of an implant. The use of a nonresorbable membrane intentionally left exposed inside the socket and removed after 4–6 weeks seems to work as a barrier in the separation of the soft tissue from the bone graft.20.Bartee BK. A simplified technique for ridge preservation after tooth extraction.
→ Dent Today. 1995 Oct;14(10):62–7. The removal of the membrane after 4–6 weeks seems to give sufficient time to seclude fibroblasts from the gingival flap and to allow inside the socket the differentiation of mesenchymal cells into osteoblasts, leading then to bone. In a histological human study, a biopsy, taken at the moment of removal of a d-PTFE membrane left intentionally exposed for 28 days before, demonstrated the absence of epithelial tissue over a dense connective tissue matrix.21Laurito D, Cugnetto R, Lollobrigida M, Guerra F, Vestri A, Gianno F, Bosco S, Lamazza L, De Biase A. Socket preservation with d-PTFE membrane: histologic analysis of the newly formed matrix at membrane removal.
→ Int J Periodontics Restorative Dent. 2016 Nov/Dec;36(6):877–83. This finding indicates that this connective tissue seems to be a well-vascularized osteoid matrix that needs some more maturation time to become a mineralized tissue and allow placement of an implant.22Beck TM, Mealey BL. Histologic analysis of healing after tooth extraction with ridge preservation using mineralized human bone allograft.
→ J Periodontol. 2010 Dec;81(12):1765–72. This period can last from 3 to 6 months, depending on the size of the defect and the biomaterial used as a graft.
In another histological study, a combination of 70% mineralized and 30% demineralized cortical allograft material placed in a post-extraction socket together with a d-PTFE membrane intentionally left exposed was compared with a group for which only a mineralized allograft material was used. The biopsy showed increased vital bone formation (36.16%) and a reduced residual graft (18.24%) compared with the 100% mineralized bone allograft group (24.69% and 27.04%, respectively).23Borg TD, Mealey BL. Histologic healing following tooth extraction with ridge preservation using mineralized versus combined mineralized-demineralized freeze-dried bone allograft: a randomized controlled clinical trial.
→ J Periodontol. 2015 Mar;86(3):348–55.
In the present study, no infection of either the surrounding soft tissue or of the underlying graft was experienced owing to the low porosity of the d-PTFE membrane, which does not allow bacterial contamination. The nanoporosity of the d-PTFE membrane is about 0.2–0.3 μ, too small for the penetration of a bacterium, the size of which is about 5 μ. This was confirmed by a histological study in which a membrane, removed after 21 days, did not show any bacterial cell on the inferior border or surface.24Krauser JT. High-density PTFE membranes: uses with root-form implants.
→ Dent Implantol Update. 1996 Sep;7(9):65–9.
Another important result of this study is the regeneration of the most coronal part of the buccal plate with the combination of the icecream cone membrane technique and a nonresorbable membrane intentionally left exposed. The results of this study have shown that minimal crestal resorption occurs even if part of the buccal plate is missing. The minimal crestal resorption allows ideal implant placement with the presence of about 2 mm of residual buccal bone, fundamental to support the soft-tissue margins, avoiding in this way gingival recession. These results seem to be stable even 6 months after crown placement with creeping of the soft tissue on the buccal side compared with the initial situation. However, further histological studies are needed to validate these promising clinical results.
Conclusion
Buccal plate reconstruction with an intentionally exposed nonresorbable membrane is an effective and easy procedure for regeneration of a resorbed buccal bone plate, especially after tooth extraction in the esthetic zone, where the stability of the periimplant tissue is fundamental.
Competing interests
The authors declare that they have no conflict of interest regarding the materials used in the present study.
Interview
with Marco Tallarico
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Tallarico M, Xhanari E, Pisano M, De Riu G, Tullio A, Meloni SM. Single post-extractive ultra-wide 7 mm-diameter implants versus implants placed in molar healed sites after socket preservation for molar replacement: 6-month post-loading results from a randomised controlled trial. → Eur J Oral Implantol. 2016 Oct;9(3):263–75. |
| 2. | ↑ | Canullo L, Wiel Marin G, Tallarico M, Canciani E, Musto F, Dellavia C. Histological and histomorphometrical evaluation of postextractive sites grafted with mg-enriched nano-hydroxyapatite: a randomized controlled trial comparing 4 versus 12 months of healing. → Clin Implant Dent Relat Res. 2016 Oct;18(5):973–83. |
| 3, 12. | ↑ | Tallarico M, Xhanari E, Pisano M, Gatti F, Meloni SM. Molar replacement with 7 mm wide diamieter implants: to place the implant immediately or to wait 4 months after socket preservation? 1 year loading results from a randomized controlled trial. → Eur J Oral Implantol. 2017 Sep;10(2):169–78. |
| 4. | ↑ | Buser D, Ingimarsson S, Dula K, Lussi A, Hirt HP, Belser UC. Long-term stability of osseointegrated implants in augmented bone: a 5-year prospective study in partially edentulous patients. → Int J Periodontics Restorative Dent. 2002 Apr;22(2):109–17. |
| 5, 13. | ↑ | Urban IA, Jovanovic S, Lozada JL. Vertical ridge augmentation using guided bone regeneration (GBR) in three clinical scenarios prior to implant placement: a retrospective study of 35 patients 12 to 72 months after loading. → Int J Oral Maxillofac Implants. 2009 May-Jun;24(3):502–10. |
| 6. | ↑ | Urban IA, Caplanis N, Lozada JL. Simultaneous vertical guided bone regeneration and guided tissue regeneration in the posterior maxilla using recombinant human plateletderived growth factor: a case report. → J Oral Implantol. 2009 Oct;35(5):251–6. |
| 7, 16. | ↑ | Carbonell JM, Martin IS, Santos A, Pujol A, Sanz-Moliner JD, Nart J. High-density polytetrafluoroethylene membranes in guided bone and tissue regeneration procedures: a literature review. → Int J Oral Maxillofac Surg. 2014 Jan;43(1):75–84. |
| 8. | ↑ | Waasdorp J, Feldman S. Bone regeneration around immediate implants utilizing a dense polytetrafluoroethylene membrane without primary closure: a report of 3 cases. → J Oral Implantol. 2013 Jun;39(3):355–61. Epub 2011 Sep 9. |
| 9. | ↑ | Hoffmann O, Bartee BK, Beaumont C, Kasaj A, Deli G, Zafiropoulos GG. Alveolar bone preservation in extraction sockets using non-resorbable dPTFE membranes: a retrospective non-randomized study. → J Periodontol. 2008 Aug;79(8):1355–69. |
| 10. | ↑ | Barber HD, Lignelli J, Smith BM, Bartee BK. Using a dense PTFE membrane without primary closure to achieve bone and tissue regeneration. → J Oral Maxillofac Surg. 2007 Apr;65(4):748–52. |
| 11. | ↑ | Monteiro AS, Macedo LG, Macedo NL, Balducci I. Polyurethane and PTFE membranes for guided bone regeneration: histopathological and ultrastructural evaluation. → Med Oral Patol Oral Cir Bucal. 2010 Mar;15(2):e401–6. |
| 14, 21. | ↑ | Laurito D, Cugnetto R, Lollobrigida M, Guerra F, Vestri A, Gianno F, Bosco S, Lamazza L, De Biase A. Socket preservation with d-PTFE membrane: histologic analysis of the newly formed matrix at membrane removal. → Int J Periodontics Restorative Dent. 2016 Nov/Dec;36(6):877–83. |
| 15. | ↑ | Bartee BK. Evaluation of a new polytetrafluoroethylene guided tissue regeneration membrane in healing extraction sites. → Compend Contin Educ Dent. 1998 Dec;19(12):1256–8, 1260, 1262–4. |
| 17. | ↑ | Elm von E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. → BMJ. 2007 Oct 20;335(7624):806–8. |
| 18. | ↑ | Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classification and repair technique. → Pract Proced Aesthet Dent. 2007 Mar;19(2):99–104; quiz 106. |
| 19. | ↑ | Tan-Chu JH, Tuminelli FJ, Kurtz KS, Tarnow DP. Analysis of buccolingual dimensional changes of the extraction socket using the “ice cream cone” flapless grafting technique. → Int J Periodontics Restorative Dent. 2014 May-Jun;34(3):399–403. |
| 20. | ↑ | .Bartee BK. A simplified technique for ridge preservation after tooth extraction. → Dent Today. 1995 Oct;14(10):62–7. |
| 22. | ↑ | Beck TM, Mealey BL. Histologic analysis of healing after tooth extraction with ridge preservation using mineralized human bone allograft. → J Periodontol. 2010 Dec;81(12):1765–72. |
| 23. | ↑ | Borg TD, Mealey BL. Histologic healing following tooth extraction with ridge preservation using mineralized versus combined mineralized-demineralized freeze-dried bone allograft: a randomized controlled clinical trial. → J Periodontol. 2015 Mar;86(3):348–55. |
| 24. | ↑ | Krauser JT. High-density PTFE membranes: uses with root-form implants. → Dent Implantol Update. 1996 Sep;7(9):65–9. |





Leave a Reply
Be the First to Comment!