Digital approach to the fabrication of a wax prototype for full-mouth rehabilitation of a worn dentition: A clinical report
December 7, 2017 / Categories: Digital Dentistry, Implant Dentistry

Brenes, Christian

Babb, Courtney S.

Bencharit, Sompop
Romero, Mario
Arce, Roger
Abstract
Background
This article describes a technique of the creation of a virtual wax-up and design of a wax prototype used as a pattern for the fabrication of posterior metal–ceramic and anterior pressed lithium disilicate restorations for a patient with a severely worn dentition.
Materials and methods
During the rehabilitation of a patient, computer-aided design (CAD) can be used as a tool to verify marginal adaptation, occlusion and contact points before pressing or fabricating the final restorations. The prototypes work as an esthetic try-in that can be modified easily if necessary.
Results
After proper verification, there were no marginal discrepancies and no occlusal modification was required, nor were contact points adjusted during final delivery. After a 1-year follow-up, the patient reported no complications.
Conclusion
Computer-aided design/computer-aided manufacturing has brought many advantages to restorative dentistry, including producing predictable restorations in less time compared with traditional methods of fabrication. In this comprehensive prosthodontic rehabilitation of a severely worn dentition, the virtual diagnostic wax-up and final restoration CAD took less than 60 min for each procedure. Additionally, the wax prototype is a multipurpose restorative tool, as it serves as both an esthetic and functional try-in device and as a wax pattern for the final restoration.
Keywords
CAD/CAM, wax prototype, smile design, digital design, lithium disilicate, virtual wax-up.
Introduction
Tooth wear is a multifactorial process that can be attributed to the mechanisms of attrition, erosion and abrasion1Johansson A, Johansson AK, Omar R, Carlsson GE. Rehabilitation of the worn dentition.
→ J Oral Rehabil. 2008 Jul;35(7):548–66. and can adversely impact patient satisfaction with appearance, pain levels, oral comfort and chewing capacity.2Al-Omiri MK, Lamey PJ, Clifford T. Impact of tooth wear on daily living.
→ Int J Prosthodont. 2006 Nov–Dec;19(6):601–5. Patients tend to seek help from dental professionals at a more advanced stage of wear, especially when it has esthetically compromised the incisal edges of the anterior teeth.3Vailati F, Carciofo S. CAD/CAM monolithic restorations and full-mouth adhesive rehabilitation to restore a patient with a past history of bulimia: the modified three-step technique.
→ Int J Esthet Dent. 2016 Spring;11(1):36–56. Alteration in clinical crown height may be necessary to improve esthetics, and this is often facilitated by increasing the vertical dimension of occlusion (VDO).4Wassell RW, Steele JG, Welsh G. Considerations when planning occlusal rehabilitation: a review of the literature.
→ Int Dent J. 1998 Dec;48(6):571–81. When changing the incisal position restoratively, trial restorations should be used as a guide for the patient to experience function, comfort, stability and esthetics at the new increased VDO.5Bloom DR, Padayachy JN. Increasing occlusal vertical dimension—why, when and how.
→ Br Dent J. 2006 Mar 11;200(5):251–6. Necessary changes can then be made prior to fabrication of the permanent restorations, instead of having the final restorations created without any verification process, which can potentially lead to minor or major adjustments and possible defects of the ceramic restorations. The wax prototype can easily be modified and used as a template for fabrication.
The advances in computer-aided design/ computer-aided manufacturing (CAD/CAM) technology over the recent years have led to an evolution in restorative dentistry. Digital dentistry can be useful in full-mouth rehabilitation, as it has increased the ability of the dental team to efficiently create, communicate and digitally store smile designs6Ferencz JL. Increasing VDO and the use of CAD/CAM: prosthodontic principles and the full-mouth reconstruction.
→ J Cosmetic Dent. 2013 Summer;29(2):86–96. and wax-ups. The final restorations can be designed and milled based on the digital smile design, or the same smile design can be used to create prototypes of the final restorations for verification purposes. While scanning and milling CAD/CAM restorations have been shown to produce restorations of acceptable marginal fit below 100 μm,7Reich S, Trentzsch L, Gozdowski S, Krey KF. In vitro analysis of laboratory-processed and CAD/CAM-generated occlusal onlay surfaces.
→ Int J Prosthodont. 2009 Nov–Dec;22(6):620–2. recent studies have shown that the combination of a conventional polyvinylsiloxane impression method and the pressed fabrication technique produces the most accurate 3-D and 2-D marginal fit.8Anadioti E, Aquilino SA, Gratton DG, Holloway JA, Denry I, Thomas GW, Qian F. 3D and 2D marginal fit of pressed and CAD/CAM lithium disilicate crowns made from digital and conventional impressions.
→ J Prosthodont. 2014 Dec;23(8):610–7.
The purpose of this article is to describe a technique of the creation of a virtual wax-up and design of a wax prototype used as a pattern for the fabrication of posterior metal–ceramic and anterior pressed lithium disilicate restorations for a patient with a severely worn dentition.
Clinical report
A 66-year-old woman presented to the Department of Prosthodontics at the University of North Carolina at Chapel Hill School of Dentistry, Chapel Hill, N.C., U.S., with the chief complaints of missing teeth and worn dentition (Fig. 1). Clinical examination found multiple teeth with moderate to severe attrition and erosion. The patient stated that she drank lemonade daily and had been without posterior teeth for over 5 years (Figs. 2 & 3). Previous dental history established replacement of missing teeth with a mandibular removable partial denture, which the patient had never tolerated owing to movement and food accumulation. The patient presented with excellent periodontal status and hygiene, and no endodontic lesions or pathologies. After evaluation of the patient records, a digital smile design was created to evaluate the possible esthetic outcome of the treatment to include the midline, occlusal plane and ideal proportions, position, symmetry and shape of the anterior teeth. Incisal edge position was determined first9Chiche GJ, Aoshima H. Functional versus aesthetic articulation of maxillary anterior restorations.
→ Pract Periodontics Aesthet Dent. 1997 Apr;9(3):335–42; quiz 343. by adding composite to the maxillary central incisors and evaluating the lips at rest and during smiling following the Vig and Brundo parameters of lip display.10Vig RG, Brundo GC. The kinetics of anterior tooth display.
→ J Prosthet Dent. 1978 May;39(5):502–4. After the length had been established, a digital smile design protocol was created and width was determined using a proportion close to 80% of the length.11Wolfart S, Thormann H, Freitag S, Kern M. Assessment of dental appearance following changes in incisor proportions.
→ Eur J Oral Sci. 2005 Apr;113(2):159–65. The maxillary lateral incisors, canines and premolars were designed following the curvature of the lower lip and with relative tooth sizes close to the golden percentage (Fig. 4).12Murthy BV, Ramani N. Evaluation of natural smile: Golden proportion, RED or Golden percentage.
→ J Conserv Dent. 2008 Jan;11(1):16–21.
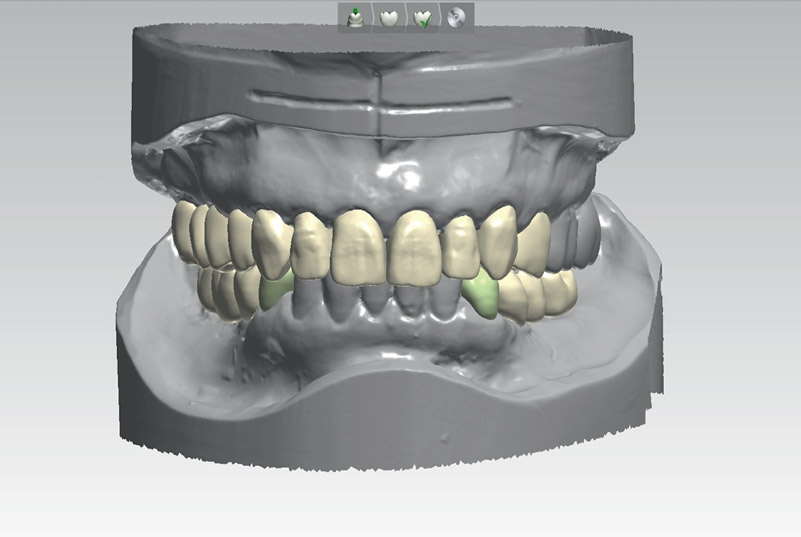
The articulated casts were scanned using a 3-D scanner (3Shape D700, 3Shape, Copenhagen, Denmark). The 3-D image of the smile design was imported into the design software (Smile Composer, 3Shape) to follow the same design during the virtual diagnostic wax-up. The virtual diagnostic wax-up was created at an increased VDO (Fig. 5).
The occlusion was verified in the CAD software, and stereolithographic files were sent to the Microdental laboratory, Raleigh, N.C., U.S., to mill replicas in wax and in polymethyl methacrylate (PMMA) to be used as shell provisionals with a dry milling machine (Zenotec mini, Wieland Dental, Pforzheim, Germany).
Upon completion of the diagnostic wax-up, the dental team developed a treatment plan that included implant-supported fixed partial dentures for the missing mandibular left second premolar through first molar and mandibular right second premolar through second molar, full-coverage crowns for the mandibular left canine and right first premolar, full-coverage crowns for the maxillary anterior teeth, and a fixed partial denture from the maxillary right second molar to second premolar.
-

-
Fig. 1
Preoperative smile view. Note attrition on incisal edges.
-

-
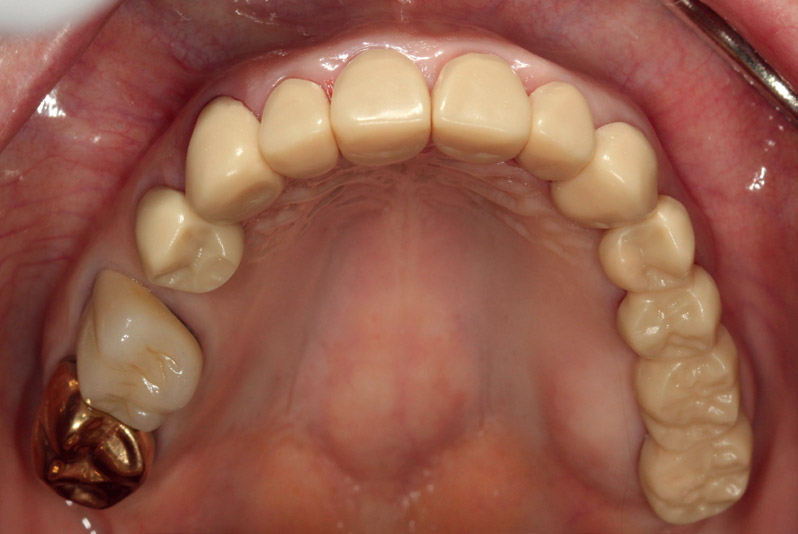
Fig. 2
Preoperative occlusal view of maxillary teeth. Note attrition on incisal edges and erosion on lingual surfaces of anterior teeth.
-

-
Fig. 3
Preoperative occlusal view of mandibular teeth.
-

-
Fig. 4
Digital smile design, establishing maxillary incisal edge position.
-
-
Fig. 5
Completed virtual diagnostic wax-up at increased VDO after digital smile design.
Based on the diagnostic wax-up, a radiographic stent was fabricated and used to perform a cone beam computed tomography scan for implant placement planning. A surgical guide based on the milled wax-up was used to place 2 4.1 × 10.0 mm implants (Tapered Screw-Vent Implants, Zimmer Biomet, Warsaw, Ind., U.S.) in the position of teeth #3.4 and 4.5 and two 4.75 × 10.0 mm Tapered Screw-Vent implants in the positions of teeth #3.6 and 4.7. Three months later, a second-stage surgery was performed to uncover the implants and healing abutments were placed for a period of 2 weeks.
At the preparation appointment, teeth #1.7 through 2.4 and teeth #3.3 and 4.4 were prepared for full-coverage anterior lithium disilicate crowns (IPS e.max Press, Ivoclar Vivadent, Ellwangen, Germany) and posterior metal–ceramic crowns. A double-cord impression technique for prepared teeth and a closed-tray impression technique with the impression abutments in position for the implants were performed to produce final impressions using a silicone impression material (Aquasil Ultra, Dentsply Sirona, York, Pa., U.S.). The milled PMMA provisionals, sectioned into sextants, were relined with self-curing acrylic resin (Jet Acrylic, Lang Dental, Wheeling, Ill., U.S.). Casts made from the final impressions were cross mounted with casts of the provisional restorations. All of the dies and casts were scanned with the 3Shape D700 for custom titanium abutments (Atlantis, Dentsply Sirona, York, Pa., U.S.) to be designed based on a copy of the virtual wax-up.
-

-
Fig. 6
Milled wax prototype try-in, smile view.
-
-
Fig. 7
Milled wax prototype try-in, maxillary occlusal view.
-

-
Fig. 8
Milled wax prototype try-in, mandibular occlusal view.
-

-
Fig. 9
Final restorations cemented.
-

-
Fig. 10
Final restorations, maxillary occlusal view.
-

-
Fig. 11
Final restorations, mandibular occlusal view.
The custom abutments were manufactured, and the CADs of the final restorations were then copy-milled into wax prototypes by the dental laboratory with the purpose of using them as templates for the final restorations. The milled wax prototype was tried in for an occlusal and esthetic evaluation (Figs. 7 & 8). Both arches were evaluated and no occlusal adjustments were necessary in centric relation and during excursive movements. Minimal reduction of the incisal edges was performed to make the esthetics more age-appropriate.13Freedman GA. Contemporary Esthetic Dentistry. 1st ed.
→ St. Louis: Mosby/Elsevier; 2012. 461 p. The case was sent to the dental laboratory for the fabrication of the final restorations. Final characterization was done, followed by glazing and polishing (Table 1).
At delivery, the posterior metal–ceramic restorations and anterior IPS e.max pressed restorations were approved by the patient for esthetics, and the restorations were verified for marginal fit, proximal contacts and occlusion. No adjustments were needed. Implant abutments were torqued to the manufacturer-recommended values, and the posterior restorations were cemented with resin cement (RelyX Unicem, 3M ESPE, Seefeld, Germany). The anterior crowns were bonded using resin cement (Variolink Esthetic, Ivoclar Vivadent; Figs. 9–11). The patient was very satisfied with the treatment outcome and was followed for a period of 6 months, during which time she reported no complications or complaints.
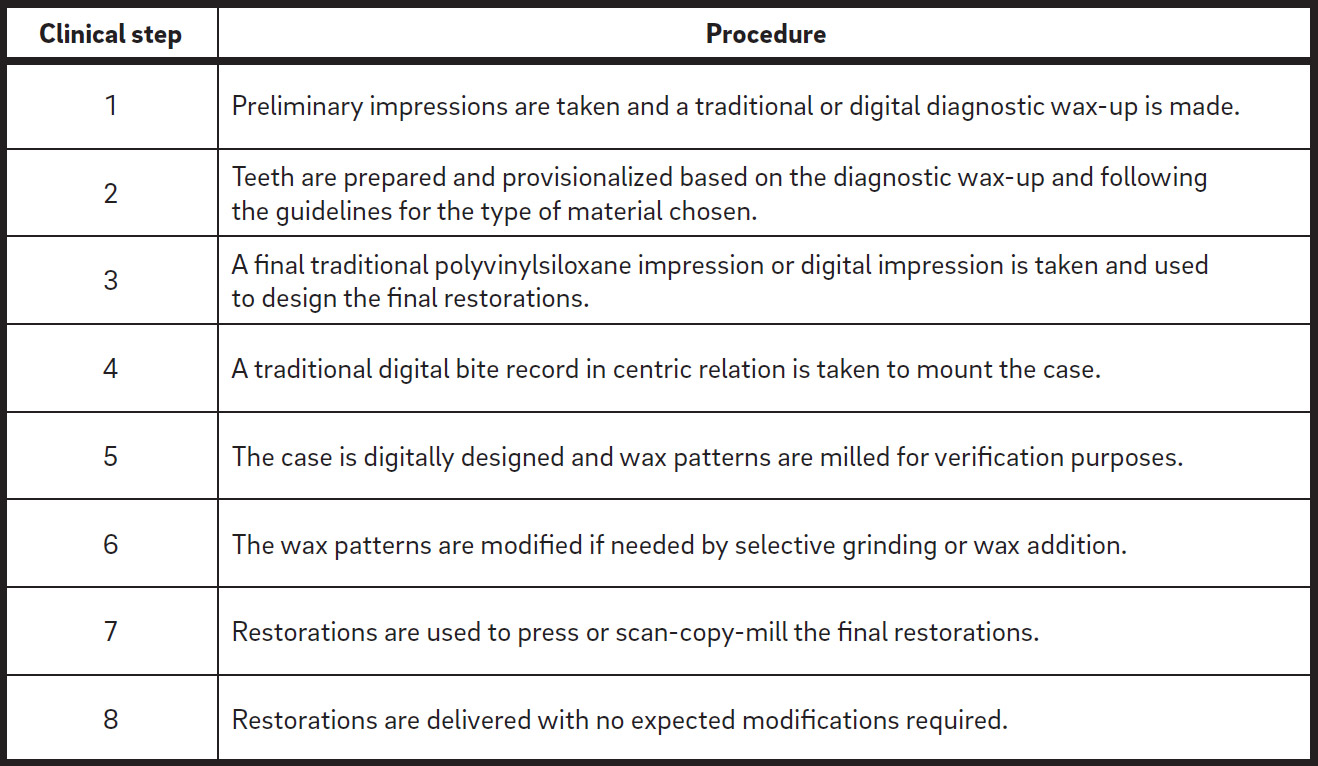
Summary of the steps in the wax prototype technique.
Discussion
This clinical situation illustrated a patient with a severely worn dentition who sought dental treatment after the maxillary anterior incisal edges had become compromised, thereby affecting esthetics. Owing to the loss of clinical crown height of the maxillary incisors subsequent to erosion and attrition, the decision was made to increase the VDO in order to provide adequate space for esthetically pleasing restorations. The patient was amenable to comprehensive fixed prosthodontic rehabilitation because of missing teeth and her inability to tolerate a removable prosthesis. The diagnostic wax-up had revealed very minor issues that the patient was not interested in addressing at the time of the treatment; thus, she did not desire whitening or direct restorations on the mandibular incisors. Traditionally, diagnostic wax-ups done by hand, by the clinician or technician, have been known to be a time-consuming step in the treatment planning process. The advantage of incorporating digital dentistry into the workflow of pressed restorations is that it provides a more consistent result in diagnostic wax-ups obtained through the use of CAD libraries, instead of relying on freehand wax-ups. Additionally, the time needed for the creation of a diagnostic wax-up is significantly reduced; in this situation, the virtual wax-up was created in less than 60 min.
The employment of CAD/CAM to create a milled wax prototype of the final restorations is a revolutionary use of the technology for both dentists and dental technicians. Not only can it be used as an esthetic and functional try-in tool by the clinician to verify marginal adaptation, occlusion and esthetics prior to delivery of the final restorations, but it also can serve as essentially a wax pattern for the fabrication of pressed or metal–ceramic restorations or a scan copy for milled restorations if any modifications are made. The wax used in CAD/CAM milling discs is very different than traditional dental wax. In order to resist the heat produced by the burs during milling, these waxes are developed as a hard hybrid plasticized wax blend, with a melting point between 101.667 and 121.111 °C.14Denry I, Holloway JA. Ceramics for dental applications: a review.
→ Materials (Basel). 2010 Jan;3(1):351–68. During try-in, the shape, marginal fit, occlusion and proximal contacts of the restorations can be verified, because the rigidity of the wax allows for this. If adjustments are needed, the wax can be modified accordingly with heat or rotary instrumentation. One limitation is that the wax prototypes do not have enough retention, a problem with restoration try-ins. Denture adhesive or fit checker (GC America, Tokyo, Japan) can be used to minimize this issue. The wax prototype can then be sent to the laboratory technician, who can then invest it as he or she would a wax pattern created through the traditional waxing process.
This wax prototype technique presents a unique melding of traditional and digital dental processes. CAD/CAM technology is used for designing and milling the wax prototype, which is then used as a traditional wax pattern to create the pressed, metal–ceramic or milled final restorations. Using this method in this clinical situation allowed for all of the restorations to be made in the same method, even though different materials (lithium disilicate for the anterior and metal–ceramic for the posterior) were used, making for a more streamlined production process. When used to create the final restoration, the wax prototype works as a template, to avoid modifying the final restoration during the delivery. In many cases, clinicians need to modify the restoration by grinding and polishing. Depending on the modification process, the final restoration can end up with internals fracture lines developed as a consequence of grinding the ceramic material that are not recognized by the clinician and can jeopardize the treatment plan and the life span of the restoration.
Conclusion
CAD/CAM has brought many advantages to restorative dentistry, including producing predictable restorations in less time compared with traditional methods of fabrication. In this comprehensive prosthodontic rehabilitation of a severely worn dentition, the virtual diagnostic wax-up and final restoration CAD took less than 60 min for each procedure. Additionally, the wax prototype is a multipurpose restorative tool, as it serves as both an esthetic and functional try-in device and as a wax pattern for the final restoration.
Competing interests
The authors declare that they have no conflict of interest regarding the materials used in the present study.
Acknowledgments
The authors thank Dr. William Bracket for his assistance in reviewing this article.
Interview
with Christian Brenes
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Johansson A, Johansson AK, Omar R, Carlsson GE. Rehabilitation of the worn dentition. → J Oral Rehabil. 2008 Jul;35(7):548–66. |
| 2. | ↑ | Al-Omiri MK, Lamey PJ, Clifford T. Impact of tooth wear on daily living. → Int J Prosthodont. 2006 Nov–Dec;19(6):601–5. |
| 3. | ↑ | Vailati F, Carciofo S. CAD/CAM monolithic restorations and full-mouth adhesive rehabilitation to restore a patient with a past history of bulimia: the modified three-step technique. → Int J Esthet Dent. 2016 Spring;11(1):36–56. |
| 4. | ↑ | Wassell RW, Steele JG, Welsh G. Considerations when planning occlusal rehabilitation: a review of the literature. → Int Dent J. 1998 Dec;48(6):571–81. |
| 5. | ↑ | Bloom DR, Padayachy JN. Increasing occlusal vertical dimension—why, when and how. → Br Dent J. 2006 Mar 11;200(5):251–6. |
| 6. | ↑ | Ferencz JL. Increasing VDO and the use of CAD/CAM: prosthodontic principles and the full-mouth reconstruction. → J Cosmetic Dent. 2013 Summer;29(2):86–96. |
| 7. | ↑ | Reich S, Trentzsch L, Gozdowski S, Krey KF. In vitro analysis of laboratory-processed and CAD/CAM-generated occlusal onlay surfaces. → Int J Prosthodont. 2009 Nov–Dec;22(6):620–2. |
| 8. | ↑ | Anadioti E, Aquilino SA, Gratton DG, Holloway JA, Denry I, Thomas GW, Qian F. 3D and 2D marginal fit of pressed and CAD/CAM lithium disilicate crowns made from digital and conventional impressions. → J Prosthodont. 2014 Dec;23(8):610–7. |
| 9. | ↑ | Chiche GJ, Aoshima H. Functional versus aesthetic articulation of maxillary anterior restorations. → Pract Periodontics Aesthet Dent. 1997 Apr;9(3):335–42; quiz 343. |
| 10. | ↑ | Vig RG, Brundo GC. The kinetics of anterior tooth display. → J Prosthet Dent. 1978 May;39(5):502–4. |
| 11. | ↑ | Wolfart S, Thormann H, Freitag S, Kern M. Assessment of dental appearance following changes in incisor proportions. → Eur J Oral Sci. 2005 Apr;113(2):159–65. |
| 12. | ↑ | Murthy BV, Ramani N. Evaluation of natural smile: Golden proportion, RED or Golden percentage. → J Conserv Dent. 2008 Jan;11(1):16–21. |
| 13. | ↑ | Freedman GA. Contemporary Esthetic Dentistry. 1st ed. → St. Louis: Mosby/Elsevier; 2012. 461 p. |
| 14. | ↑ | Denry I, Holloway JA. Ceramics for dental applications: a review. → Materials (Basel). 2010 Jan;3(1):351–68. |





Leave a Reply
Be the First to Comment!