Evaluation of primary stability and early healing of 2 implant macrodesigns placed in the posterior maxilla: A split-mouth prospective randomized controlled clinical study
November 26, 2019 / Categories: Digital Dentistry, Implant Dentistry

Sánchez-Siles, Marino
Baptista Ilha, Joao
Fernández Ruiz, Juan Alberto
Camacho Alonso, Fabio
Abstract
Objective
The aim of this study was to evaluate the clinical behavior of 2 implants of different macrodesigns placed in low-density bone at the moment of insertion and during bone healing.
Materials and methods
In this split-mouth prospective randomized controlled clinical study, 60 Avinent dental implants (Avinent Implant System) were placed in the posterior maxillae of 30 patients. Each patient received 1 tapered implant with a wide thread (OCEAN) and 1 cylindrical implant with a narrow thread (CORAL). Primary stability was evaluated at baseline by measuring the insertion torque applied and registering the implant stability quotient (ISQ). Periimplant crestal bone loss was evaluated from intraoral radiographs taken at 1 and 4 months after implant placement. Lastly, ISQ was registered after 4 months.
Results
At baseline, both insertion torque and ISQ values were significantly higher for tapered implants (P = 0.008). There was less periimplant crestal bone loss at 1 and 4 months with tapered implants with a wide thread (0.43 ± 0.27 mm and 0.59 ± 0.31 mm, respectively) than with cylindrical implants with a narrow thread (0.73 ± 0.28 mm and 0.95 ± 0.43 mm, respectively), and the differences at both evaluation times were significant (P < 0.001 and P = 0.001, respectively). The ISQ values at 4 months were higher for tapered implants with a wide thread, and the difference was significant (P = 0.014).
Conclusion
Although both implant macrodesigns can be placed in low-density bone, tapered implants with a wide thread appear to produce better results in terms of insertion torque, ISQ and crestal bone loss 4 months after placement.
Keywords
Dental implant macrodesign; tapered implant; cylindrical implant; low-density bone; thread.
Introduction
Bone density and especially cortical thickness are important factors in achieving adequate primary stability and a successful clinical outcome when placing dental implants.1Rozé J, Babu S, Saffarzadeh A, Gayet-Delacroix M, Hoomaert, A, Layrolle P. Correlating implant stability to bone structure. → Clin Oral Implants Res. 2009 Oct;20(10):1140–5. Primary stability is defined as the absence of movement after the intraosseous insertion of the implant.2Bahat O, Sullivan RM. Parameters for successful implant integration revisited part I: immediate loading considered in light of the original prerequisites for osseointegration. → Clin Implant Dent Relat Res. 2010 May;12 Suppl 1:e2–12. doi: 10.1111/j.1708- 8208.2010.00279.x. Different types of bone in the jaws have been clinically classified in various ways according to structural characteristics related to the proportion of cortical to trabecular bone. The most commonly used classification is that of Lekholm and Zarb,3Norton MR, Gamble C. Bone classification: an objective scale of bone density using the computerized tomography scan. → Clin Oral Implants Res. 2001 Feb;12(1):79–84. according to which type I is the most densely compacted bone type, and type IV the most trabeculated, with lower density and thinner cortical bone, which is generally considered less suitable for supporting dental implants.4He J, Zhao B, Deng C, Shang D, Zhang C. Assessment of implant cumulative survival rates in sites with different bone density and related prognostic factors: an 8-year retrospective study of 2,684 implants. → Int J Oral Maxillofac Implants. 2015 Mar–Apr;30(2):360–71. Nevertheless, none of the classification systems take the bone’s biological capacity into account.5Li J, Yin X, Huang L, Mouraret S, Brunski JB, Cordova L, Salmon B, Helms JA. Relationships among bone quality, implant osseointegration, and Wnt signaling. → J Dent Res. 2017 Jul;96(7):822–31.
In recent years, various quantitative methods for assessing primary stability have been introduced. These can be used to monitor implant stability repeatedly over time.6Cehreli MC, Karasoy D, Akca K, Eckert SE. Meta-analysis of methods used to assess implant stability. → Int J Oral Maxillofac Implants. 2009 Nov–Dec;24(6):1015–32. Resonance frequency analysis (RFA) consists of applying a bending load that imitates clinical implant loading and its direction. This provides information about the rigidity of the bone-to-implant union, and the result is registered as a parameter known as the implant stability quotient (ISQ). ISQ values range from 1 (low stability) to 100 (maximum stability).7Sennerby L, Meredith N. Implant stability measurements using resonance frequency analysis: biological and biomechanical aspects and clinical implications. → Periodontol 2000. 2008 Jun;47:51–66. Alternatively, insertion torque is a direct measure of the bone’s cutting resistance during implant insertion surgery.8Meredith N. Assessment of implant stability as a prognostic determinant. → Int J Prosthodont. 1998 Sep–Oct;11(5):491–501. But insertion torque is a mechanical parameter that can be influenced by the surgical procedure, implant design and bone quality.
The success of an implant depends largely on its primary stability, as mechanical stability provides a basis for osseointegration.9Suer BT, Yaman Z, Buyuksarac B. Correlation of fractal dimension values with implant insertion torque and resonance frequency values at implant recipient sites. → Int J Oral Maxillofac Implants. 2016 Jan–Feb;31(1):55–62. Bone density and quality, surgical technique, primary stability and, of course, the implant’s geometry are all important factors in achieving implant osseointegration.10Suer BT, Yaman Z, Buyuksarac B. Correlation of fractal dimension values with implant insertion torque and resonance frequency values at implant recipient sites. → Int J Oral Maxillofac Implants. 2016 Jan–Feb;31(1):55–62.,11Bahat O, Sullivan RM. Parameters for successful implant integration revisited part I: immediate loading considered in light of the original prerequisites for osseointegration. → Clin Implant Dent Relat Res. 2010 May;12 Suppl 1:e2–12. doi: 10.1111/j.1708- 8208.2010.00279.x.,12Dos Santos MV, Elias CN, Cavalcanti Lima JH. The effects of superficial roughness and design on the primary stability of dental implants. → Clin Implant Dent Relat Res. 2011 Sep;13(3):215–23.
Implant design and shape have undergone various modifications over the years, aimed at increasing the contact between implant surface and bone, and increasing primary and secondary stability.13Pimentel Lopes de Oliveira G, Leite FC, Pontes AE, Sakakura CE, Junior EM. Comparison of the primary and secondary stability of implants with anodized surfaces and implants treated by acids: a split-mouth randomized controlled clinical trial. → Int J Oral Maxillofac Implants. 2016 Jan–Feb;31(1):186–90.,14Abuhussein H, Pagni G, Rebaudi A, Wang HL. The effect of thread pattern upon implant osseointegration. → Clin Oral Implants Res. 2010 Feb;21(2):129–36. An adequate macrodesign must balance compression and traction forces and minimize shear forces,15Abuhussein H, Pagni G, Rebaudi A, Wang HL. The effect of thread pattern upon implant osseointegration. → Clin Oral Implants Res. 2010 Feb;21(2):129–36. to maintain micromovement at a level below 50–150 μm during the healing period.16Szmukler-Moncler S, Salama H, Reingewirtz Y, Dubruille JH. Timing of loading and effect of micromotion on bone-dental implant interface: review of experimental literature. → J Biomed Mater Res. 1998 Summer;43(2):192–203. A tapered shape provides the implant with a good basis for primary stability, as it allows the gradual expansion of the bone and minimizes stress at its interface with the surrounding bone.10 It has been shown clinically that implants with a tapered design present better stability in areas with lower bone density.17Pozzi A, Tallarico M, Moy PK. Immediate loading with a novel implant featured by variable-threaded geometry, internal conical connection and platform shifting: three-year results from a prospective cohort study. → Eur J Oral Implantol. 2015 Spring;8(1):51–63.,18Sakoh J, Wahlmann U, Stender E, Nat R, Al-Nawas B, Wagner W. Primary stability of a conical implant and a hybrid, cylindric screw-type implant in vitro. → Int J Oral Maxillofac Implants. 2006 Jul–Aug;21(4):560–6. The pitch and shape of the thread also influence primary stability, stress and initial bone-toimplant contact.19Kielbassa AM, Marrinez-de Fuentes R, Goldstein M, Arnhart C, Barlattani A, Jackowski J, Knauf M, Lorenzoni M, Maiorana C, Mericske-Stern R, Rompen E, Sanz M. Randomized controlled trial comparing a variable-thread novel tapered and a standard tapered implant: interim one-year results. → J Prosthet Dent. 2009 May;101(5):293–305. According to some studies, a reduced pitch improves surface contact with bone, reduces the distribution of stress and improves primary stability in low-density bone.20Chung SH, Heo SJ, Koak JY, Kim SK, Lee JB, Han JS, Han CH, Rhyu IC, Lee SJ. Effects of implant geometry and surface treatment on osseointegration after functional loading: a dog study. → J Oral Rehabil. 2008 Mar;35(3):229–36.,21Orsini E, Giavaresi G, Trirè A, Ottani V, Salgarello S. Dental implant thread pitch and its influence on the osseointegration process: an in vivo comparison study. → Int J Oral Maxillofac Implants. 2012 Mar–Apr;27(2):383–92.
Thus, the aim of this split-mouth prospective randomized controlled study was to evaluate the clinical behavior of 2 implants of different macrodesigns at the moment of insertion in the low-density bone of the posterior upper jaw and during bone healing.
Methods and materials
Recruitment and patient characteristics
The study protocol was approved by the University of Murcia’s ethics committee (Spain) (1933/2018) and was carried out between June 2018 and December 2018 at the university’s dental clinic. Subjects were treated according to guidelines established by the Declaration of Helsiki for medical research involving human subjects. All the subjects provided their informed consent to participate. The entire protocol (clinical, surgical and radiographic) was carried out by a single clinician.
-
- Fig. 1
-
- Fig. 2
The inclusion criteria were as follows: aged over 18 years; total edentulism in the maxilla necessitating bilateral implant insertion in the posterior third in type III bone within a range of 350–830 Hounsfield units (HU), according to Norton and Gamble’s classification;22Norton MR, Gamble C. Bone classification: an objective scale of bone density using the computerized tomography scan. → Clin Oral Implants Res. 2001 Feb;12(1):79–84. absence of medical contraindications to oral surgical procedures (ASA I/II); and willingness to provide informed consent to take part. The exclusion criteria were as follows: presence of a disease or condition or use of medication that could compromise healing or osseointegration (diabetes mellitus, severe osteoporosis or bisphosphonate administration); pregnancy or lactation; and radiotherapy of the head and neck during the previous 18 months; and refusal to provide informed consent to take part.
Thirty patients fulfilled the inclusion criteria and were invited to take part in the trial. Before surgery, the patients’ sociodemographic data were registered, as well as their status regarding smoking and alcohol consumption, and their complete medical histories.
Bone mineral density measurements
To measure bone mineral density (BMD) in the maxillary posterior third in cone beam computed tomography (CBCT) images, a 3D circular region of interest was determined in each and it was between 10 and 20 mm2 in area. BMD was calculated in HU. The CBCT images were taken using a Kodak CS 8100 CBCT unit (Kodak) with the following specifications: 18 × 21 cm field of view, 90 kVp, 10 mA, exposure time of 15 s, and spatial resolution of 10 lp/cm and 0.2 mm voxel size. This CBCT unit was calibrated every 6 months in accordance with the Spanish Royal Decree of Dec. 23, 1976/1999. Images were constructed with Carestream 3D imaging software (Carestream Health).
Dental implant surgery and randomization
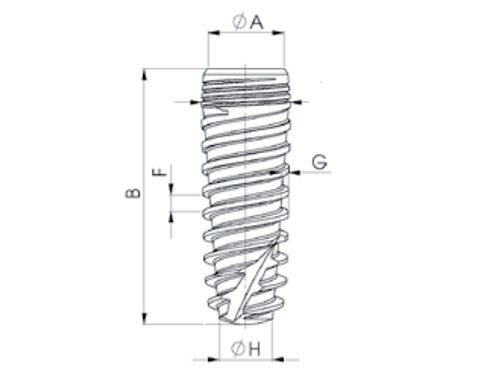
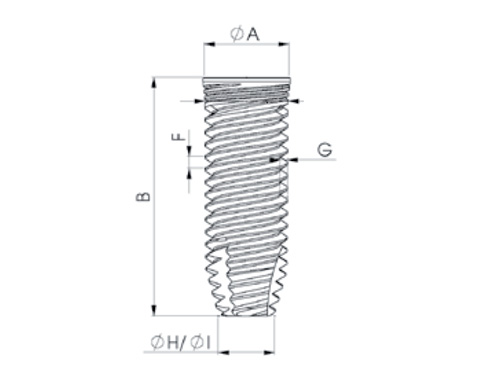
All the surgical interventions were performed under local anesthesia (1:100,000 articaine) by a single clinician at the same drilling speed of 50 rpm with irrigation. Each patient received 2 Avinent dental implants (Avinent Implant System), 1 tapered implant with a wide thread (OCEAN) and 1 cylindrical implant with a narrow thread (CORAL). The insertion of one or the other design in each posterior region was determined using an online randomization service (www.randomization. com). The characteristics of the tapered implant with a wide thread were as follows: internal hex connection, wide thread pitch (1.5 mm), square-shaped thread and thread depth of 0.5 mm. The characteristics of the cylindrical implant with a narrow thread were as follows: narrow thread pitch (0.5 mm), V-shaped thread and thread depth of 0.36 mm (Figs. 1 & 2). The insertion torque of the 60 implants was registered with an Implantmed SI-1023 surgical micromotor (W&H), first establishing an initial insertion torque of 20 N cm and then increasing torque by 5 N cm increments as necessary until the required insertion torque was reached. All the implants were submerged. No healing abutments or provisionalization crowns were placed during the 4-month healing period. In all the cases, the postoperative medication prescribed was amoxicillin (500 mg) every 8 h for 7 days (in case of penicillin allergy, clindamycin [300 mg] every 8 h was prescribed) and ibuprofen (600 mg) every 8 h for 3 days.
Resonance frequency analysis
RFA was performed at baseline and 30 days after implant insertion using the Osstell Mentor (Integration Diagnostics). Each measurement was performed twice, 1 from each 90° angle, parallel to the crestal line; the highest ISQ value was taken as the reference value.
Radiographic parameters
For evaluation of radiographic bone loss (1 and 4 months after implant placement), a digital radiographic system (RVG 5100, Kodak) was used with Rinn XCP support (DENTSPLY RINN). All the radiographs were captured at 70 kV, 8 mA and a focal distance of 30 cm. Mesial, distal and total crestal bone loss (mesial + distal/2; vertical distance from the implant shoulder to the first bone-to-implant contact) were measured using ImageJ digital image analysis software (Version 1.46, National Institutes of Health).
-

-
Table 1: Study population characteristics.
† SD = standard deviation.
-

-
Table 2: Comparison of primary stability (at baseline) between study groups (Student t test).
† SD = standard deviation.
-
-
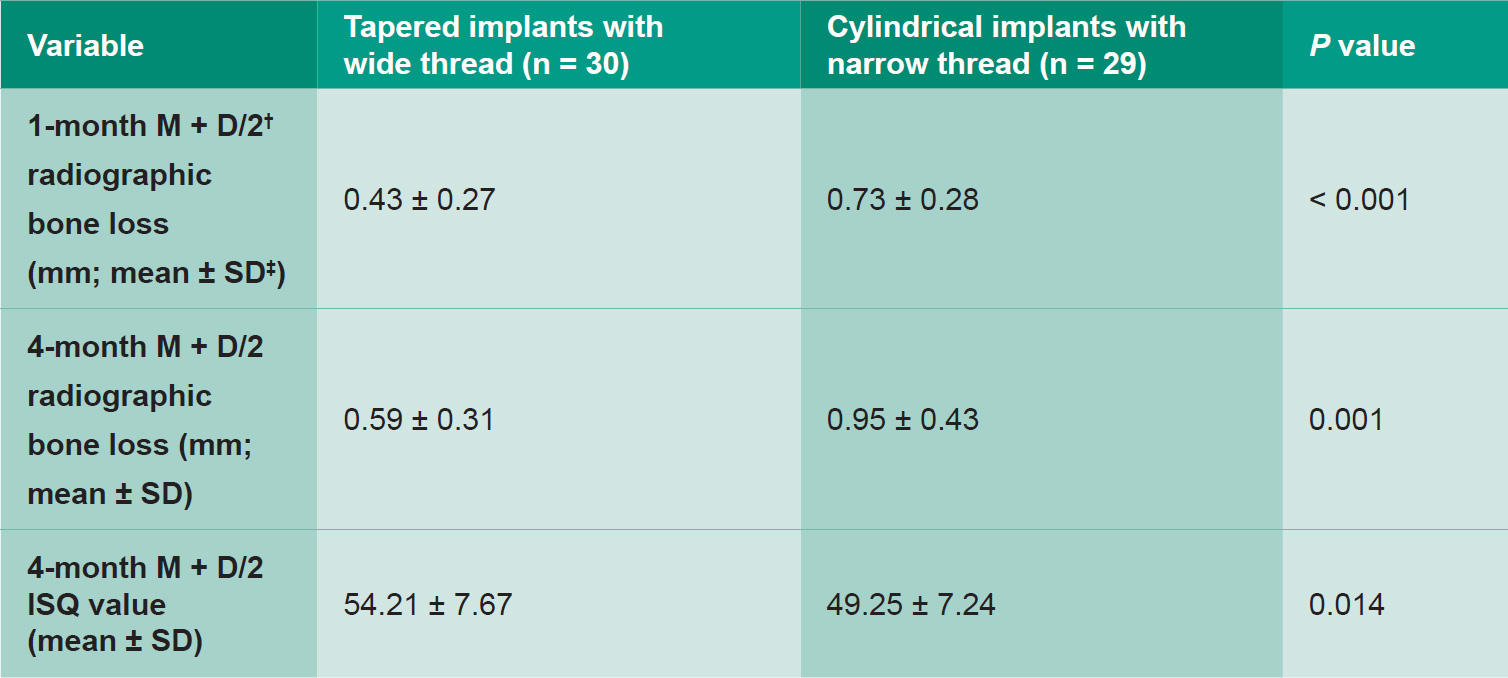
Table 3: Comparison of implant osseointegration between study groups (Student t test).
† M + D/2 = average mesial and distal surface values;
‡ SD = standard deviation.
Statistical analysis
Data were analyzed using the SPSS statistical package (Version 20.0, IBM Corp.). A descriptive study of each variable was performed. The Student t test for 2 independent samples was used in application to quantitative variables, in each case determining whether variances were homogeneous. Statistical significance was established at P ≤ 0.05.
Results
This study recruited 30 patients (9 men and 21 women), with an average age of 64.07 ± 9.02 years. Most did not smoke (73.34%) or drink alcohol (83.33%; Table 1). At baseline, both insertion torque and ISQ values were higher for tapered implants with a wide thread (29.14 ± 3.85 and 53.66 ± 2.04, respectively) than for cylindrical implants with a narrow thread (26.25 ± 3.94 and 49.48 ± 7.66, respectively), and the differences in insertion torque were statistically significant (P = 0.008; Table 2). There was less periimplant crestal bone loss at 1 and 4 months with tapered implants (0.43 ± 0.27 mm and 0.59 ± 0.31 mm, respectively) than with cylindrical implants (0.73 ± 0.28 mm and 0.95 ± 0.43 mm, respectively), and the differences at both evaluation times were significant (P < 0.001 and P = 0.001, respectively; Table 3). Lastly, the ISQ values at 4 months after implant insertion were higher for tapered implants (54.21 ± 7.67) than for cylindrical implants (49.25 ± 7.24), and the difference was statistically significant (P = 0.014; Table 3).
Discussion
This study included 30 patients who received a total of 60 dental implants in the posterior third of the maxilla (with low type III BMD), 30 with a tapered design with a wide thread and 30 with a cylindrical design with a narrow thread. Insertion torque, ISQ and crestal bone loss were measured during the first 4 months of healing.
Insertion torque was found to be higher for tapered implants than for cylindrical implants. This finding coincides with the results obtained in most other investigations of this topic. Menicucci et al. compared insertion torque achieved for tapered and cylindrical implants and also obtained significantly higher torque values for tapered implants (31.5 N cm) than for cylindrical implants (25.5 N cm).23Menicucci G, Pachie E, Lorenzetti M, Migliaretti G, Carossa S. Comparison of primary stability of straightwalled and tapered implants using an insertion torque device. → Int J Prosthodont. 2012 Sep–Oct;25(5):465–71. In 2000, O’Sullivan et al. also obtained similar results in an ex vivo study,24O’Sullivan D, Sennerby L, Meredith N. Measurements comparing the initial stability of five designs of dental implants: a human cadaver study. → Clin Implant Dent Relat Res. 2000 Apr;2(2):85–92. and in 2006, Akça et al. concluded that tapered implants achieve higher insertion torque than cylindrical implants do.25Akça K, Chang TL, Tekdemir I, Fanuscu MI. Biomechanical aspects of initial intraosseous stability and implant design: a quantitative micro-morphometric analysis. → Clin Oral Implants Res. 2006 Aug;17(4):465–72. They also argued that insertion torque values are more sensitive than ISQ values in terms of revealing biomechanical conditions at the bone-to-implant interface.26García-Vives N, Andrés-García R, Rios-Santos V, Fernández-Palacín A, Bullón-Fernández P, Herrero-Climent M, Herrero-Climent F. In vitro evaluation of the type of implant bed preparation with osteotomes in bone type IV and its influence on the stability of two implant systems. → Med Oral Patol Oral Cir Bucal. 2009 Sep;14(9):e455–60.
As for ISQ, tapered implants obtained higher values both at baseline and after 4 months of osseointegration (although without a statistically significant difference at baseline). Other studies have also registered ISQ obtaining higher values for tapered implants than for cylindrical implants.27Romanos GE, Basha-Hijazi A, Gupta B, Ren YF, Malmstrom H. Role of clinician’s experience and implant design on implant stability. An ex vivo study in artificial soft bones. → Clin Implant Dent Relat Res. 2014 Apr;16(2):166–71.,28García-Vives N, Andrés-García R, Rios-Santos V, Fernández-Palacín A, Bullón-Fernández P, Herrero-Climent M, Herrero-Climent F. In vitro evaluation of the type of implant bed preparation with osteotomes in bone type IV and its influence on the stability of two implant systems. → Med Oral Patol Oral Cir Bucal. 2009 Sep;14(9):e455–60. This finding could be due to tapered implants exerting higher lateral compression force against the crestal and middle bone walls, leading to small differences in ISQ values between implant types, despite significant differences in insertion torque. Similar results were obtained by Sakoh et al., who found no differences in ISQ values between tapered and cylindrical implants in an in vitro study.29Sakoh J, Wahlmann U, Stender E, Nat R, Al-Nawas B, Wagner W. Primary stability of a conical implant and a hybrid, cylindric screw-type implant in vitro. → Int J Oral Maxillofac Implants. 2006 Jul–Aug;21(4):560–6. Other authors have also reported that, although insertion torque was higher for tapered implants, ISQ values were similar for the 2 types of implant.30Dos Santos MV, Elias CN, Cavalcanti Lima JH. The effects of superficial roughness and design on the primary stability of dental implants. → Clin Implant Dent Relat Res. 2011 Sep;13(3):215–23.,31Sakoh J, Wahlmann U, Stender E, Nat R, Al-Nawas B, Wagner W. Primary stability of a conical implant and a hybrid, cylindric screw-type implant in vitro. → Int J Oral Maxillofac Implants. 2006 Jul–Aug;21(4):560–6.,32Friberg B, Jisander S, Widmark G, Lundgren A, Ivanoff CJ, Sennerby L, Thorén C. One-year prospective three-center study comparing the outcome of a “soft bone implant” (prototype Mk IV) and the standard Brånemark implant. → Clin Implant Dent Relat Res. 2003;5(2):71–7.,33Al-Nawas B, Wagner W, Grötz KA. Insertion torque and resonance frequency analysis of dental implant systems in an animal model with loaded implants. → Int J Oral Maxillofac Implants. 2006 Sep–Oct;21(5):726–32.
Thread geometry can be considered an important factor of implant stability and osseointegration. In a study by Steigenga et al., 72 implants with differing thread geometries were placed (V-shaped vs. squareshaped thread) in 12 New Zealand rabbit tibias.34Steigenga J, Al-Shammari K, Misch C, Nociti FH Jr, Wang HL. Effects of implant thread geometry on percentage of osseointegration and resistance to reverse torque in the tibia of rabbits. → J Periodontol. 2004 Sep;75(9):1233–41. After 12 weeks, the outcomes were analyzed by radiography and histomorphometric analysis, registering the bone-to-implant contact area and reverse torque. It was concluded that the square thread shape obtained better results in all the analyses performed.
Few studies have been published on the influence of implant shape on implant stability, osseointegration and survival when the implant is placed in lowdensity bone (such as the posterior third of the maxilla), as shown by the systematic review by Alshehri and Alshehri of clinical studies in humans of tapered and/or cylindrical implants in the posterior maxilla.35Alshehri M, Alshehri F. Influence of implant shape (tapered vs cylindrical) on the survival of dental implants placed in the posterior maxilla: a systematic review. → Implant Dent. 2016 Dec;25(6):855–60. For this reason, further prospective clinical trials are needed to confirm that tapered implants could be a better option for maximizing primary stability and bone healing in critical areas with low bone density.
Conclusion
In conclusion, although both the implant designs tested (tapered and cylindrical) may be inserted in lowdensity bone (such as the posterior third of the maxilla), tapered implants with a wide thread would appear to offer better results in terms of insertion torque, ISQ and crestal bone loss at 4 months after insertion.
Competing interests
The authors declare that they have no competing interests.
Figure legends
Fig. 1 – Tapered implant with wide thread (A = 3.5 mm, B = 11.5 mm, F = 1.5 mm, G = 0.5 mm, H = 4.1 mm).
Fig. 2 – Cylindrical implant with narrow thread (A = 4.1 mm, B = 11.5 mm, F = 0.5 mm, G = 0.36 mm, H = 4.1 mm).
Interview
with Dr. Fabio Camacho-Alonso
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Rozé J, Babu S, Saffarzadeh A, Gayet-Delacroix M, Hoomaert, A, Layrolle P. Correlating implant stability to bone structure. → Clin Oral Implants Res. 2009 Oct;20(10):1140–5. |
| 2, 11. | ↑ | Bahat O, Sullivan RM. Parameters for successful implant integration revisited part I: immediate loading considered in light of the original prerequisites for osseointegration. → Clin Implant Dent Relat Res. 2010 May;12 Suppl 1:e2–12. doi: 10.1111/j.1708- 8208.2010.00279.x. |
| 3, 22. | ↑ | Norton MR, Gamble C. Bone classification: an objective scale of bone density using the computerized tomography scan. → Clin Oral Implants Res. 2001 Feb;12(1):79–84. |
| 4. | ↑ | He J, Zhao B, Deng C, Shang D, Zhang C. Assessment of implant cumulative survival rates in sites with different bone density and related prognostic factors: an 8-year retrospective study of 2,684 implants. → Int J Oral Maxillofac Implants. 2015 Mar–Apr;30(2):360–71. |
| 5. | ↑ | Li J, Yin X, Huang L, Mouraret S, Brunski JB, Cordova L, Salmon B, Helms JA. Relationships among bone quality, implant osseointegration, and Wnt signaling. → J Dent Res. 2017 Jul;96(7):822–31. |
| 6. | ↑ | Cehreli MC, Karasoy D, Akca K, Eckert SE. Meta-analysis of methods used to assess implant stability. → Int J Oral Maxillofac Implants. 2009 Nov–Dec;24(6):1015–32. |
| 7. | ↑ | Sennerby L, Meredith N. Implant stability measurements using resonance frequency analysis: biological and biomechanical aspects and clinical implications. → Periodontol 2000. 2008 Jun;47:51–66. |
| 8. | ↑ | Meredith N. Assessment of implant stability as a prognostic determinant. → Int J Prosthodont. 1998 Sep–Oct;11(5):491–501. |
| 9, 10. | ↑ | Suer BT, Yaman Z, Buyuksarac B. Correlation of fractal dimension values with implant insertion torque and resonance frequency values at implant recipient sites. → Int J Oral Maxillofac Implants. 2016 Jan–Feb;31(1):55–62. |
| 12, 30. | ↑ | Dos Santos MV, Elias CN, Cavalcanti Lima JH. The effects of superficial roughness and design on the primary stability of dental implants. → Clin Implant Dent Relat Res. 2011 Sep;13(3):215–23. |
| 13. | ↑ | Pimentel Lopes de Oliveira G, Leite FC, Pontes AE, Sakakura CE, Junior EM. Comparison of the primary and secondary stability of implants with anodized surfaces and implants treated by acids: a split-mouth randomized controlled clinical trial. → Int J Oral Maxillofac Implants. 2016 Jan–Feb;31(1):186–90. |
| 14, 15. | ↑ | Abuhussein H, Pagni G, Rebaudi A, Wang HL. The effect of thread pattern upon implant osseointegration. → Clin Oral Implants Res. 2010 Feb;21(2):129–36. |
| 16. | ↑ | Szmukler-Moncler S, Salama H, Reingewirtz Y, Dubruille JH. Timing of loading and effect of micromotion on bone-dental implant interface: review of experimental literature. → J Biomed Mater Res. 1998 Summer;43(2):192–203. |
| 17. | ↑ | Pozzi A, Tallarico M, Moy PK. Immediate loading with a novel implant featured by variable-threaded geometry, internal conical connection and platform shifting: three-year results from a prospective cohort study. → Eur J Oral Implantol. 2015 Spring;8(1):51–63. |
| 18, 29, 31. | ↑ | Sakoh J, Wahlmann U, Stender E, Nat R, Al-Nawas B, Wagner W. Primary stability of a conical implant and a hybrid, cylindric screw-type implant in vitro. → Int J Oral Maxillofac Implants. 2006 Jul–Aug;21(4):560–6. |
| 19. | ↑ | Kielbassa AM, Marrinez-de Fuentes R, Goldstein M, Arnhart C, Barlattani A, Jackowski J, Knauf M, Lorenzoni M, Maiorana C, Mericske-Stern R, Rompen E, Sanz M. Randomized controlled trial comparing a variable-thread novel tapered and a standard tapered implant: interim one-year results. → J Prosthet Dent. 2009 May;101(5):293–305. |
| 20. | ↑ | Chung SH, Heo SJ, Koak JY, Kim SK, Lee JB, Han JS, Han CH, Rhyu IC, Lee SJ. Effects of implant geometry and surface treatment on osseointegration after functional loading: a dog study. → J Oral Rehabil. 2008 Mar;35(3):229–36. |
| 21. | ↑ | Orsini E, Giavaresi G, Trirè A, Ottani V, Salgarello S. Dental implant thread pitch and its influence on the osseointegration process: an in vivo comparison study. → Int J Oral Maxillofac Implants. 2012 Mar–Apr;27(2):383–92. |
| 23. | ↑ | Menicucci G, Pachie E, Lorenzetti M, Migliaretti G, Carossa S. Comparison of primary stability of straightwalled and tapered implants using an insertion torque device. → Int J Prosthodont. 2012 Sep–Oct;25(5):465–71. |
| 24. | ↑ | O’Sullivan D, Sennerby L, Meredith N. Measurements comparing the initial stability of five designs of dental implants: a human cadaver study. → Clin Implant Dent Relat Res. 2000 Apr;2(2):85–92. |
| 25. | ↑ | Akça K, Chang TL, Tekdemir I, Fanuscu MI. Biomechanical aspects of initial intraosseous stability and implant design: a quantitative micro-morphometric analysis. → Clin Oral Implants Res. 2006 Aug;17(4):465–72. |
| 26, 28. | ↑ | García-Vives N, Andrés-García R, Rios-Santos V, Fernández-Palacín A, Bullón-Fernández P, Herrero-Climent M, Herrero-Climent F. In vitro evaluation of the type of implant bed preparation with osteotomes in bone type IV and its influence on the stability of two implant systems. → Med Oral Patol Oral Cir Bucal. 2009 Sep;14(9):e455–60. |
| 27. | ↑ | Romanos GE, Basha-Hijazi A, Gupta B, Ren YF, Malmstrom H. Role of clinician’s experience and implant design on implant stability. An ex vivo study in artificial soft bones. → Clin Implant Dent Relat Res. 2014 Apr;16(2):166–71. |
| 32. | ↑ | Friberg B, Jisander S, Widmark G, Lundgren A, Ivanoff CJ, Sennerby L, Thorén C. One-year prospective three-center study comparing the outcome of a “soft bone implant” (prototype Mk IV) and the standard Brånemark implant. → Clin Implant Dent Relat Res. 2003;5(2):71–7. |
| 33. | ↑ | Al-Nawas B, Wagner W, Grötz KA. Insertion torque and resonance frequency analysis of dental implant systems in an animal model with loaded implants. → Int J Oral Maxillofac Implants. 2006 Sep–Oct;21(5):726–32. |
| 34. | ↑ | Steigenga J, Al-Shammari K, Misch C, Nociti FH Jr, Wang HL. Effects of implant thread geometry on percentage of osseointegration and resistance to reverse torque in the tibia of rabbits. → J Periodontol. 2004 Sep;75(9):1233–41. |
| 35. | ↑ | Alshehri M, Alshehri F. Influence of implant shape (tapered vs cylindrical) on the survival of dental implants placed in the posterior maxilla: a systematic review. → Implant Dent. 2016 Dec;25(6):855–60. |





Leave a Reply
Be the First to Comment!