Evaluation of the incidence and prevalence of temporomandibular joint dysfunction in psychiatric patients using typical antipsychotic drugs
July 6, 2018 / Categories: Digital Dentistry, Implant Dentistry

Costa de Carvalho, Elizabeth Maria
Alves Oliveira Barbosa, Gustavo
Rosario Sobreira Vasconcellos, Ana Cristina
Correia de Araujo, Roberto
Pereira Falcao, Antonio Fernando
Abstract
Objective
The aim of this study was to identify and classify temporomandibular joint dysfunction (TMJD) in psychiatric patients using typical antipsychotics compared with healthy individuals, both physically and mentally.
Materials and methods
The present study had a descriptive cross-sectional design, developed over a 6-month period, at the Teaching Assistant Nucleus of Dentistry and Mental Health affiliated with the Juliano Moreira Psychiatric Hospital, Salvador, Brazil, and the Federal University of Bahia School of Dentistry, Salvador, Brazil. To that end, 120 patients aged 18 years or older, 40 psychiatric patients (20 women and 20 men), all using typical or first-generation antipsychotics of the pharmacological groups of butyrophenones and phenothiazines, and 80 mentally healthy patients (40 women and 40 men), underwent assessment of TMJD severity through an Anamnestic Index.
Results
There were statistically significant differences in the prevalence of TMJD in the group of patients with mental illness. Among the 40 individuals with mental and behavioral disorders, moderate TMJD was the most prevalent (16/40.0%), but in the control group, there was a higher prevalence of mild TMJD (34/42.5%). Two cases of severe TMJD were diagnosed in psychiatric patients.
Conclusion
In this study, it was possible to identify the prevalence and incidence of TMJD among those with mental and behavioral disorders using typical antipsychotic drugs, justifying the importance of their monitoring for TMJD. However, owing to its subjective nature, these patients should be referred for a specialized examination to confirm the diagnosis of TMJD.
Keywords
Temporomandibular joint dysfunction; mental disorder; psychiatric care.
Introduction
Every human being may present with some kind of psychopathological disorder throughout his or her life, and may or may not seek help, and in some cases, the disorder may not be resolved. Each individual constructs within himself or herself a mental organization capable of making frequent adaptations to the outside world, and performing these tasks requires a continuous functioning of regulatory and adaptive mechanisms. The proper development of these mechanisms leads the individual to develop a personality within normal patterns. However, if there is an imbalance of these mechanisms, mental and behavioral disorders may occur.1Wang YP, Minatogawa TM, Júnior HT. Psicofarmacologia dos transtornos psicóticos. In: Teng CT, Demetrio FN, editors. Psicofarmacologia aplicada: manejo prático dos transtornos mentais. 2ª ed. → São Paulo: Atheneu; 2011. p. 17–56.
The oral health of patients with psychiatric disorders is generally more impaired than that of the general population, mainly owing to the precariousness of oral hygiene associated with nonreality and the side effects of the psychotropic drugs used in treatment that affect psychomotor performance, salivary flow and oral soft tissue. Antipsychotic therapy may increase the risk and duration of oral disease, since these drugs are used for a long period, thus justifying the establishment of preventive/educational oral health programs.2Jamelli SR, Mendonça MC, Dinis MG, De Andrade FB, De Melo JF, Ferreira SR, Silva PV. Saúde bucal e percepção sobre o atendimento odontológico em pacientes com transtorno psíquico moradores de residências terapêuticas [Oral health and perceptions regarding dental care in patients with mental disorders living in therapeutic residences]. → Ciêencias & Saúude Coletiva. 2010 Jun;15 Suppl 1:1795–1800.3Jovanovic S, Milovanovic SD, Gajic I, Mandic J, Latas M, Jankovic L. Oral health status of psychiatric in patients in Serbia and implications for their dental care. → Croat Med J. 2010 Oct;51(5):443–450.
Schizophrenic disorders affect about 1% of the general population and are a major problem for health services, since high rates of recurrence and comorbidity may require high long-term costs for the individual, family and society.4Jovanovic S, Milovanovic SD, Gajic I, Mandic J, Latas M, Jankovic L. Oral health status of psychiatric in patients in Serbia and implications for their dental care. → Croat Med J. 2010 Oct;51(5):443–450.5Tanasiewicz M, Skucha-Nowak M, Gren A, Hese RT, Twardawa H, Gorczyca P. Analysis of state of the oral cavity in schizophrenic in patients treated with atypical and classical neuroleptics. → Adv Clin Exp Med. 2011, Mar–Apr; 20(2):187–197. The treatment of schizophrenia often involves antipsychotics (APs) of 2 pharmacological groups: typical and atypical. Typical or conventional first-generation APs represented by dopamine (D2) antagonists—phenothiazine derivatives (such as chlorpromazine) were used initially, and later, in the 1950s, butyrophenone derivatives (such as haloperidol) were introduced—mainly eliminate the psychotic symptoms of schizophrenia. Second-generation, atypical or new-generation APs are APs with specific characteristics, such as minimal extrapyramidal effects, low sedation and rapid dissociation of D2 receptors; these properties are postulated to be due to the blockade of serotonergic and dopaminergic receptors and have a more favorable effect on the negative (chronic) symptoms, which results in an improvement in patients’ quality of life.6Tanasiewicz M, Skucha-Nowak M, Gren A, Hese RT, Twardawa H, Gorczyca P. Analysis of state of the oral cavity in schizophrenic in patients treated with atypical and classical neuroleptics. → Adv Clin Exp Med. 2011, Mar–Apr; 20(2):187–197. Therefore, in patients treated with atypical APs, better hygiene of the oral cavity is expected. In addition, disorders of the oral cavity are exacerbated by a decrease in salivary secretion, mainly caused by typical APs, but also a side effect of some atypical APs, such as risperidone.7Moralez-Cháves MC, Rueda-Delgado YM, Peña-Orozco DA. Prevalence of bucco-dental pathologies in patients with psychiatric disorders. → J Clin Exp Dent. 2014 Feb 1; 6(1):e 7–11. doi: 10.4317/jced.51147.8Elias R. Odontologia de alto risco: pacientes especiais. 1ª ed. → Rio de Janeiro: Revinter; 1995. p. 35–45.9Pereira CC, Felício CM. Os distúrbios miofuncionais orofaciais na literatura odontológica: revisão crítica [The orofacials myofunctional disorders in the dentistry publication: critical review]. → Revev Dental Press Ortodon Ortop Facial. 2005 Jul–Aug;10(4):134– 142.
The scientific literature has reported that those with mental disorders do not have access to adequate dental care owing to dental professionals’ lack of knowledge of how to assist patients with mental disorders, as well as fear, stigma or negative attitudes on behalf of dentists.10Moralez-Cháves MC, Rueda-Delgado YM, Peña-Orozco DA. Prevalence of bucco-dental pathologies in patients with psychiatric disorders. → J Clin Exp Dent. 2014 Feb 1; 6(1):e 7–11. doi: 10.4317/jced.51147. Generally, such patients have poor oral hygiene, a high number of decayed or missing teeth, bad breath, inflammation of the gingival tissue, and, in more severe cases, edentulism and a tendency toward temporomandibular joint dysfunction (TMJD).11Elias R. Odontologia de alto risco: pacientes especiais. 1ª ed. → Rio de Janeiro: Revinter; 1995. p. 35–45. Orofacial movement disorders associated with daily use of psychoactive drugs, particularly typical APs, may have repercussions for the temporomandibular joint (TMJ) and lead to TMJD.12Pereira CC, Felício CM. Os distúrbios miofuncionais orofaciais na literatura odontológica: revisão crítica [The orofacials myofunctional disorders in the dentistry publication: critical review]. → Revev Dental Press Ortodon Ortop Facial. 2005 Jul–Aug;10(4):134– 142.
Although TMJD does not have a definite etiology, its appearance is credited to functional, structural and psychological factors. Conditions such as malocclusion, parafunction and modification of the emotional state (stress) may be present in patients with this dysfunction. The signs and symptoms of TMJD are characterized by TMJ pain and painful masticatory muscles; headache; otological manifestations, such as tinnitus, auricular fullness, vertigo and auditory symptoms; limitation and/or lack of coordination of mandibular movements; limitation of mouth opening; temporary joint blockage; and joint crackling.13Benevides SD. Determinação do padrão da amplitude dos movimentos mandibulares em escolares de 8 a 12 anos [doctoral thesis]. → [Salvador]: Universidade Federal da Bahia, Instituto de Ciências e Saúde; 2013: 132. Therefore, the morphological and functional disorders of the oral cavity influence the skeletal-motor action of the masticatory muscles, leading to a breakdown of the orofacial anatomical and neurological homeostasis, and affecting not only the stomatognathic system but also the general health of the patient.14Pereira CC, Felício CM. Os distúrbios miofuncionais orofaciais na literatura odontológica: revisão crítica [The orofacials myofunctional disorders in the dentistry publication: critical review]. → Revev Dental Press Ortodon Ortop Facial. 2005 Jul–Aug;10(4):134– 142.
Oromandibular dystonia can be diagnosed by the contractions of the jaw, compromised phonation and swallowing. In severe cases, it may cause bilateral displacement of the TMJ.15Karthik MS, Prabhu N. Temporomandibular joint dislocation due to atypical antipsychotic-induced acute dystonia: a case report. → Ther Adv Psychopharmacol. 2014 Dec;4(6):282–284.
The etiology of TMJD is considered complex and multifactorial, with the presence of predisposing, initial and perpetuating factors. Such conditions follow an evolutionary course of days, months or years, occasionally transient and self-limiting, and aggravated by parafunctional habits.16Ferreira KD, Guimarães JP, Batista CH, Júnior AM, Ferreira LA. Fatores psicológicos relacionados à sintomatologia crônica das desordens ttemporomandibulares— revisão de literaturea [Related psychological factors in chronic temporomandibular disorder—literature review]. → Rev Fac Odontol Univ Passo Fundo. 2009 Sep–Dec;14(3):262–267.
Given the strong suspicion of the correlation between TMJD and psychiatric patients and the limited scientific literature on the topic, the objective of this research was to identify and classify TMJD in psychiatric patients using typical APs, using the Anamnestic Index advocated by Fonseca in 1994.17Fonseca, DM. et al. Diagnóstico pela anamnese da disfunção craniomandibular. → Rev. Gauch. Odontol. 1994 Jan/Feb; 42(1): 23-28.
Materials and methods
This study was conducted in accordance with the norms of Resolution No. 466/12 of the National Health Council of the Ministry of Health, published on December 12, 2012, and by the Code of Professional Dental Ethics, according to Resolution No. 179/1993 of the Federal Council of Dentistry. The project was submitted to the Research Ethics Committee of the School of Dentistry of the Federal University of Bahia, Salvador, Brazil, and approved by CONEP under registration CAAE 08119812.0.0000.5024, dated April 14, 2015, Consubstantiated Opinion No. 1023044.
The participants in the test group—40 psychiatric patients, 20 women and 20 men, users of typical APs of the pharmacological grouping of butyrophenones and phenothiazines—were examined at the Teaching Assistant Nucleus of Dentistry and Mental Health affiliated with the Juliano Moreira Psychiatric Hospital, Salvador, Brazil, and the Federal University of Bahia School of Dentistry, Salvador, Brazil. The evaluation of the oral health of the participants in the control group—80 volunteers, 40 women and 40 men clinically healthy from a psychiatric point of view—was carried out at the periodontic clinic of the Federal University of Bahia.
A population of patients with mental and behavioral disorders institutionalized at the Juliano Moreira Psychiatric Hospital, users of typical APs drugs, composed of 10 participants, were evaluated. However, because it was an investigation with psychiatric patients, who, in some situations, do not cooperate to allow the performance of this type of examination, the sample size was chosen by convenience sample, based on the number of individuals who fulfilled the necessary requirements to participate, respecting the exclusion and inclusion criteria established.
The inclusion criteria common to the 2 groups analyzed were: age greater than or equal to 18 years, acceptance to participate and signing of the free and informed consent. For the test group, the following inclusion criteria were also considered: being assisted at the Juliano Moreira Psychiatric Hospital, regardless of the assistance model; being a typical AP user; for ethical-legal reasons, the person responsible and/or the companion signed the informed consent in the case of patients assisted in an outpatient clinic, and for internees, the acceptance was by the chief nurse.
The present study had a descriptive cross-sectional design and data collection started in May 2015 and ended in October 2015. The Anamnestic Index advocated by Fonseca (IAF)18Fonseca, DM. et al. Diagnóstico pela anamnese da disfunção craniomandibular. → Rev. Gauch. Odontol. 1994 Jan/Feb; 42(1): 23-28. was used in this study as a screening instrument aimed primarily at classifying the severity of TMJD symptoms, with an accessible language to be self-completed; however, owing to the fact that the sample was made up of mentally ill patients assisted in a public psychiatric hospital, the interviews for data collection were performed in the presence of the caregiver or the nurse, in the case of hospitalized patients. The IAF consists of 10 questions that verify the presence of TMJ pain in the neck, headache, masticatory and movement difficulties, crackles, parafunctional habits, perception of malocclusion and feelings of emotional stress.19Pereira CC, Felício CM. Os distúrbios miofuncionais orofaciais na literatura odontológica: revisão crítica [The orofacials myofunctional disorders in the dentistry publication: critical review]. → Revev Dental Press Ortodon Ortop Facial. 2005 Jul–Aug;10(4):134– 142. It allows 3 types of responses—yes, sometimes or no—with scoring equivalent to 10, 5 and 0, respectively. By aggregating the points, the index classifies participants into these categories of symptom severity:
(I) no TMJD: 0–15 points
(II) mild TMJD: 20–40 points
(III) moderate TMJD: 45–65 points
(IV) severe TMJD: 70–100 points
Despite its subjective nature, it can be considered as indicative of the need for more accurate tests to confirm the severity of TMJD impairment in patients who present with signs or symptoms compatible with TMJD.20Gurbuz O, Alatas G, Kurt E. Prevalence of temporomandibular disorder signs in patients with schizophrenia. → J Oral Rehabil. 2009 Dec; 36(12): 864–71.
The IAF was chosen because it is a suitable tool for the study of population profiles for TMJD symptoms and for screening potential patients, aiming at the later application of more accurate diagnostic indexes and tests for TMJD—the Diagnostic Criteria for Research on Temporomandibular Disorders.
Statistical analysis
The chi-square (Pearson), Fisher exact and Mann–Whitney test were used for the statistical analysis of the categorical variables. The parametric variables were submitted to the Pearson correlation test and the nonparametric variables to the Spearman correlation test.
All 120 records from the 40 patients with mental and behavioral disorders (test group) and 80 data records from the mentally healthy participants (control group) were included. The data related to the dental clinic record were tabulated in the EpiData program (Version 3.1, EpiData Association, Odense, Denmark) and transferred to the Excel 2010 program for further exploratory analysis, performed through the SPSS for Windows statistical program (Version 13.0, SPSS, Chicago, Ill., U.S.).
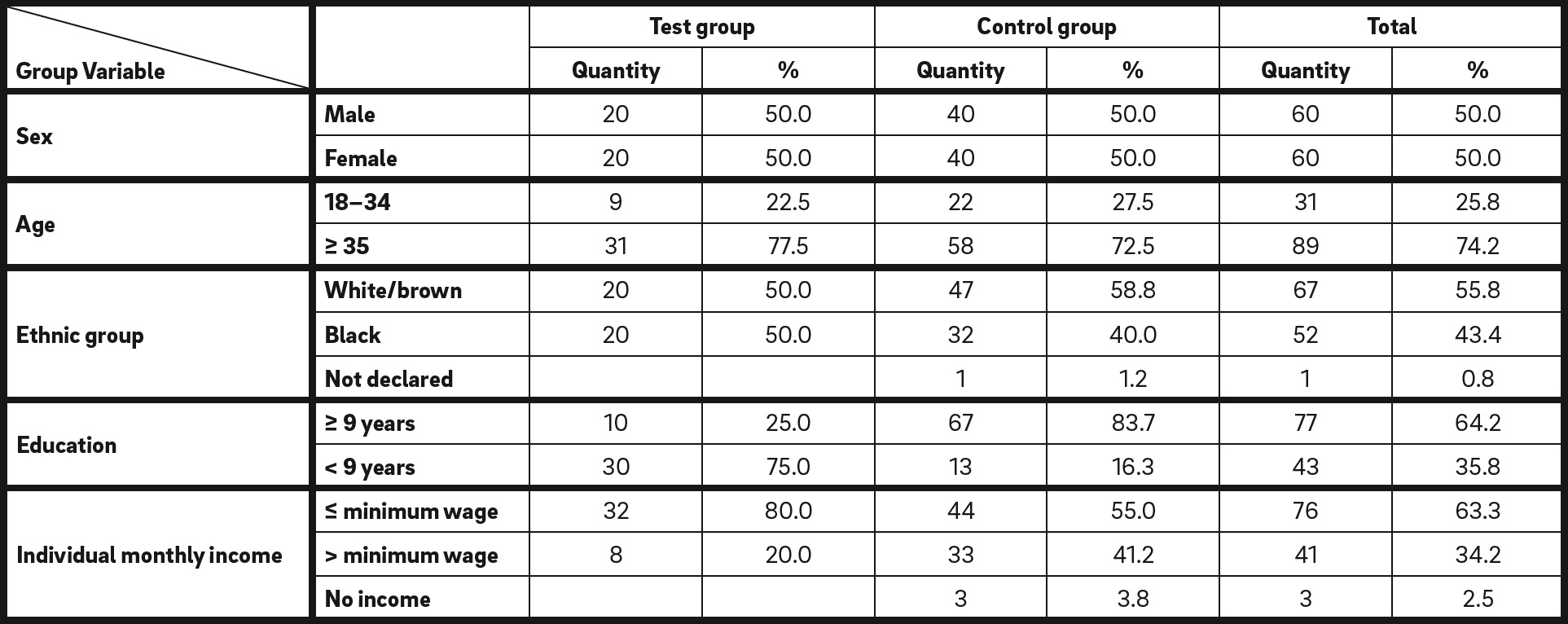
Absolute and relative values of the sample according to sociodemographic variables.
For the descriptive step, we calculated the absolute and relative frequencies, and the measures of central tendency and dispersion presented by means of tables. For the exploratory analysis, the Pearson chi-square association test was used to verify the differences between the 2 groups. For the analyses, a confidence level of 95% and a value of P < 0.05 were considered. Odds ratios and confidence intervals were calculated as significant values of P < 0.05.
For statistical inferences, when the variables presented dependence, that is, when comparing different moments of the same group (test group), the Mann–Whitney test was used for the independent variables, such as in the cases of normality patterns obtained from the asymptomatic participants of the control group, or in the comparisons between the test group and the control group. The decision to use nonparametric tests was due to the small sample size.
Results
According to the entries in the medical records of the 40 patients in the test group—13 of them hospitalized and 27 treated on an outpatient basis, some of whom had more than 1 diagnosis— obtained from the statistical medical archiving service of the hospital, 63.3% had schizophrenia and schizotypal and delusional disorders; 24.5% mood disorders (affective); 8.1% mental retardation and 4.1% schizophrenic- type organic delusional disorder, including World Health Organization (1996) coding for each of these disorders.
The characterization of the sample analyzed in this study considered the following sociodemographic variables: sex, age group, ethnic group, educational level and individual monthly income (Table 1). The sex of the participants was equally distributed: 50% men and 50% women. As for the ethnic group, 50% were white/brown and 50% were black. The majority of the participants (77.5%) were over 35 years old, with a monthly income equal to or less than the minimum wage effective in 2013, in the state of Bahia (80%). The educational level of the participants showed a higher percentage of individuals who had not completed 9 years of study: 75%. From these findings, it can be inferred that, probably, for those with mental disorders and behavioral users of psychoactive drugs, access to school would have been restricted to basic education because of the limitations that the mental pathologies impose, as well as the extrapyramidal effects of APs typical for psychiatric treatment, which may compromise motor coordination.
The assessment of the degree of severity of TMJD was performed with the application of the IAF Test 15, and the data obtained in this research demonstrated statistically significant differences when comparing the presence of TMJD among patients with mental illness to among mentally healthy volunteers: 82.5% of the former had a higher prevalence of TMJD, irrespective of the degree of severity of the dysfunction, and the dysfunction was diagnosed in 55.0% of the volunteers in the control group.
Regarding the degree of TMJD severity as suggested by FONSECA , statistically significant differences were identified between the test and

* P = 0.001.
Absolute and relative values of the sample according to severity of temporomandibular dysfunction.
control groups (P = 0.001). A mild degree of TMJD was recorded in 37.5% of the participants in the test group and 42.5% in the control group; moderate TMJD was diagnosed in 40.0% of the individuals in the test group and 12.5% in the control group; and the only clinical cases of severe TMJD were identified in 2 patients with mental and behavioral disorders (5.0%); 17.5% of the participants in the test group and 45.0% of the control group did not present with TMJD (Table 2).
In the analysis of the association between the possible risk factors for the occurrence of TMJD in the 120 participants and the sociodemographic variables, only a statistically significant correlation was registered considering the different degrees of TMJD severity and ethnic group (P = 0.025), both in the test and in the control groups. Moderate TMJD was diagnosed in 40% of the participants in the test group, 45% white/ brown and 35% black. In addition, in the control group, 55.3% of the white/brown participants did not present with TMJD, but in the test group, only 15.0%. It should be noted that the 2 clinical cases of severe TMJD were diagnosed in 10% of the black participants in the test group (Tables 3 & 4).
Discussion
Epidemiological surveys have shown that 40–75% of the population have at least one sign of TMJD, and 33% at least one symptom, such as face or TMJ pain. In the present study, mild TMJD had a higher occurrence among participants in the control group (42.5%/34) than in the test group (37.5%/15). These results corroborate those of Al-Mobeeriek, who also study the TMJ condition in psychiatric patients and concluded that bruxism and tooth clenching were the most common parafunctions in both groups (34.5% in the control group and 27.0% in the test group).21Al-Mobeeriek A. Oral health status among psychiatric patients in Riyadh, Saudi Arabia. → West Indian Med J. 2012 Aug;61(5):549–554.
It is also worth mentioning the review article by Araújo et al., which calls attention to the decisive role of the adverse effects of psychotropic drugs on the onset of TMJD, associated with constant headache, reported by people with schizophrenia, and the difficulty in diagnosing and treating TMJD in schizophrenic patients who use psychoactive drugs that may cause extrapyramidal effects, and recommends a careful evaluation when such patients complain of orofacial pain.22Araújo AN, Nascimento MA, Sena EP, Baptista AF. Temporomandibular disorders in patients with schizophrenia using antipsychotic agents: a discussion paper. → Drug Healthc Patient Saf. 2014 Mar; 10;(6): 21–27. doi: 10.2147/ DHPS.S57172. Given the impossibility of suspending the use of medications that keep the symptoms of schizophrenia under control, the monitoring of these patients, including occasional evaluations of the orofacial region during dental appointments, is fundamental.
TMJD has already been analyzed in schizophrenic patients, such as in the case–control study carried out by Velasco-Ortega et al., in which 32% of schizophrenics presented with symptoms of TMJD; 24% reported articular clicks on opening and closing of the mouth; and 8%, abnormal displacement of the mandible when opening the mouth.23Velasco-Ortega E, Guil LM, Ponferrada CV, Soteras RM, Egea JJ. Temporomandibular disorders among schizophrenic patients. A case-control study. → Med Oral Patol Oral Cir Bucal. 2005 Aug–Oct;10(4):315–22. Among the control group, only 8% reported cracking of the TMJ. The authors concluded that schizophrenic patients are an at-risk population for TMJD because they present a higher prevalence and severity of TMJD than do normal individuals. In addition, Gurbuz et al. pointed to a high prevalence of TMJD in schizophrenics, with an additional record of severe tooth wear and bruxism.24Gurbuz O, Alatas G, Kurt E. Prevalence of temporomandibular disorder signs in patients with schizophrenia. → J Oral Rehabil. 2009 Dec; 36(12): 864–71. These results are in line with those obtained in the present study, which included 31 schizophrenics among the 40 participants in the test group.
In investigating the most prevalent oral lesions in psychiatric patients, Moralez-Chaves et al. observed that 36.92% presented with noises of the TMJ and 10.76% had muscular pain.25Moralez-Cháves MC, Rueda-Delgado YM, Peña-Orozco DA. Prevalence of bucco-dental pathologies in patients with psychiatric disorders. → J Clin Exp Dent. 2014 Feb 1; 6(1):e 7–11. doi: 10.4317/jced.51147. The authors emphasized the need to implement specific preventive and educational oral health programs for these patients.
Clinical cases of severe TMJD were observed in 2 psychiatric patients, who were older than 35 years and of the black ethnic group and had an educational level of less than 9 years. One was a man with a monthly income greater than the minimum wage and the other a woman with a monthly income of less than the minimum wage in force at the time. The impact of mental disorder and daily use of APs on the onset of TMJD is evident because only 17.5% of the psychiatric patients did not present with TMJ impairment, whereas TMJD was found in 82.5% of the participants of the test group in its different degrees of severity, indicating the need for longitudinal follow-up of these individuals, with a view to improving their quality of life.
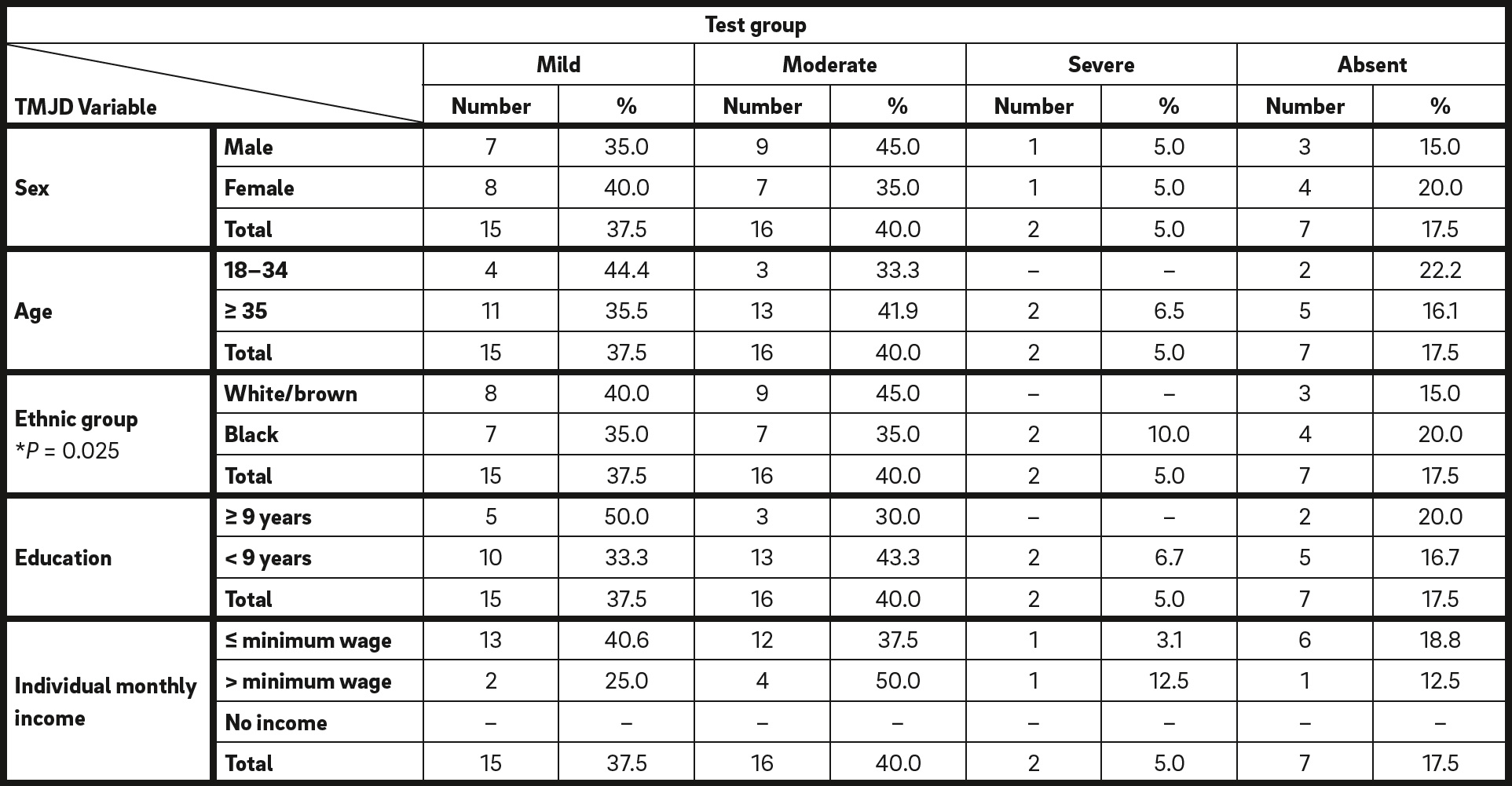
* Pearson chi-square (P < 0.0010).
Absolute and relative values of the test group according to the association between the sociodemographic variablesand the severity levels of temporomandibular dysfunction.
The IAF can be used for the screening of patients for TMJD, since it has acceptable measurement properties, especially concerning internal consistency and reproducibility. However, it is a screening questionnaire, not a diagnostic.26Pedrosa AS. Propriedades de medida do Índice Anamnésico de Fonseca : Universidade Cidade de São Paulo; 2011: 62 http://arquivos.cruzeirodosuleducacional. edu.br/principal/old/mestrado_fisioterapia/ pdf/dissertacao_alexsandra_de_ souza_pedrosa.pdf It should be remembered that this index characterizes only the presence of symptoms and not clinical signs of TMJD.27Chaves TC, Costa D, Grossi DB, Bertolli F. Avaliação anamnésica de sintomas de disfunção temporomandibular em crianças asmáticas. [The anamnestic evaluation of temporomandibular dysfunction symptoms in asthmatic children]. → Fisiot e Pesq. 2005 Jan-Apr;11(1):19–26.
Fonseca was concerned with the development of an anamnestic index for evaluation of TMJD adapted to the Brazilian population that was easy to understand and apply.28Fonseca, DM. et al. Diagnóstico pela anamnese da disfunção craniomandibular. → Rev. Gauch. Odontol. 1994 Jan/Feb; 42(1): 23-28. The simplicity of this index favors its use in epidemiological studies. However, it has not yet been completely validated and does not offer a TMJD diagnostic classification; the data obtained with this index are therefore restricted to the classification of severity of TMJD. Another limitation is its scoring system, since if 3 affirmative answers are given to the questions about headache, cervical pain and perceived emotional tension, the respondent will be classified as having mild TMJD. However, these same symptoms may occur in isolation, with no association with TMJD.29Chaves TC, Oliveira AS, Grossi DB. Principais instrumentos para avaliação da disfunção temporomandibular, parte I: índices e questionários; uma contribuição para a prática clínica e de pesquisa. [Main instruments for assessing temporomandibular disorders, part I: indices and questionnaires; a contribution to clinicians and researchers]. → Fisiot e Pesq. 2008 Mar;15(1):92–100.
In this study, in the group with mental and behavioral disorders (including schizophrenics), 17.5% had no TMJD, 5.0% were diagnosed with severe TMJD, 40.0% moderate TMJD and 37.5% mild TMJD regardless of the diagnosed mental illness. Possibly the subjectivity of the index used to assess the severity of TMJD may have induced these results; however, few studies have evaluated the presence of TMJD in patients with mental and behavioral disorders who are users of typical APs.
Side effects from the use of typical APs are associated with effects on central nervous system transmission sites and receptors and appear in relation to dose and potency levels of the drugs. Patient characteristics, including sex, age and comorbidity, may make patients more or less susceptible to certain side effects of APs. Side effects influence the patient’s quality of life and affect compliance regarding medications.30George W, Arana MD. An overview of side effects caused by typical antipsychotics. → J Clin Psychiatry. 2000; 61 (Suppl 8):5–11.
Few studies have evaluated the presence of TMJD in schizophrenic users of typical APs.
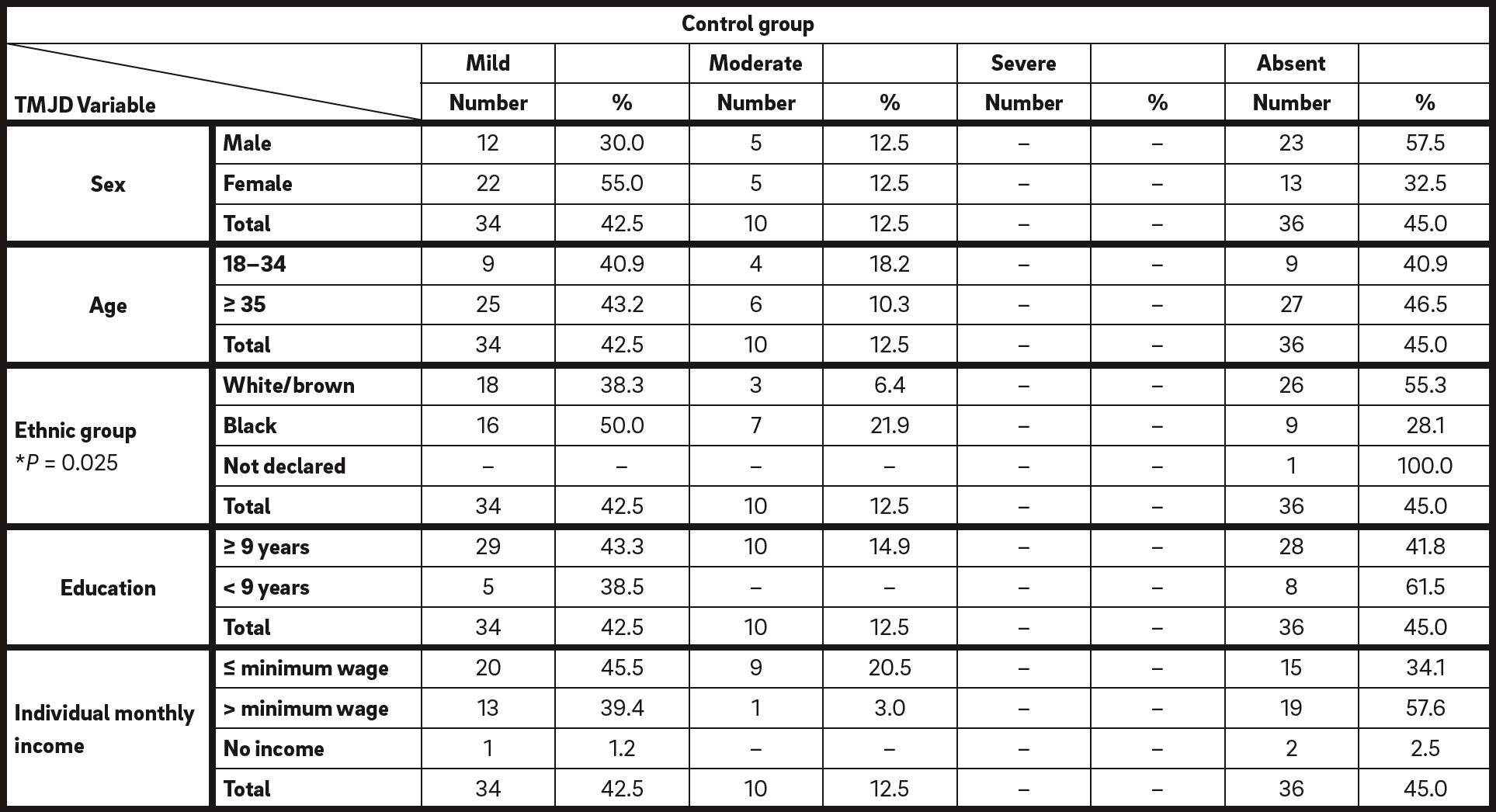
* Pearson chi-square (P < 0.0010).
Absolute and relative values of the control group according to the association between the sociodemographic variables and the severity levels of temporomandibular dysfunction.
The importance of psychiatric disorders associated with TMJD has been reported in the literature, showing a relationship in the clinical appearance, prognosis and treatment of TMJD with psychosocial factors, such as stress, anxiety and depression. The literature states that emotional aspects play an important role in the etiology and symptomatic evolution of TMJD, contributing to the onset or perpetuation of the disorder by increasing the muscular activity and tension of the facial muscles. In addition, cognitive factors suggest an influence on the individual’s response to pain, behavioral factors determine the patient’s attitude, and emotional tension promotes the onset or aggravation of clenching and bruxism. In this sense, studies indicate that anxiety and depression lead to exacerbation of symptoms and modify perception to pain.31Ferreira KD, Guimarães JP, Batista CH, Júnior AM, Ferreira LA. Fatores psicológicos relacionados à sintomatologia crônica das desordens ttemporomandibulares— revisão de literaturea [Related psychological factors in chronic temporomandibular disorder—literature review]. → Rev Fac Odontol Univ Passo Fundo. 2009 Sep–Dec;14(3):262–267.
Delays in the diagnosis of TMJD and incorrect treatment contribute to the onset and perpetuation of pain. However, successful treatment depends on the identification and control of etiological factors and usually requires the efforts of a multidisciplinary team, associating dental approaches with those of other areas, such as those that use different physical, pharmacological or behavioral therapies.32Ferreira KD, Guimarães JP, Batista CH, Júnior AM, Ferreira LA. Fatores psicológicos relacionados à sintomatologia crônica das desordens ttemporomandibulares— revisão de literaturea [Related psychological factors in chronic temporomandibular disorder—literature review]. → Rev Fac Odontol Univ Passo Fundo. 2009 Sep–Dec;14(3):262–267.
There are few reports of published cases of TMJ dislocation due to the use of antipsychotic medication, which is usually associated with the use of haloperidol and less associated with drugs such as risperidone and amisulpride; however, Karthik and Prabhu reported a case of oromandibular dystonia with displacement of the TMJ in a psychotic patient treated with oral risperidone and amisulpride.33Karthik MS, Prabhu N. Temporomandibular joint dislocation due to atypical antipsychotic-induced acute dystonia: a case report. → Ther Adv Psychopharmacol. 2014 Dec;4(6):282–284.
The prevalence of TMJD in schizophrenics was also the focus of a case–control study conducted by Gurbuz et al. in Istanbul, Turkey, in which 339 schizophrenics and 107 healthy adults were selected.34Gurbuz O, Alatas G, Kurt E. Prevalence of temporomandibular disorder signs in patients with schizophrenia. → J Oral Rehabil. 2009 Dec; 36(12): 864–71. The signs and symptoms of TMJD were analyzed using the Diagnostic Criteria for Research on Temporomandibular Disorders and the results pointed to a high prevalence of TMJD in schizophrenic patients (284/339; 83.7%), characterized mainly by pain on palpation and articular cracklings.
Al-Mobeeriek assessed 100 psychiatric patients regularly attending a clinic in Saudi Arabia and compared the results obtained with those of 84 psychologically normal volunteers.35Al-Mobeeriek A. Oral health status among psychiatric patients in Riyadh, Saudi Arabia. → West Indian Med J. 2012 Aug;61(5):549–554. Muscular pain, TMJ crackling, limitation of opening of the mouth, bruxism and harmful habits, such as nail biting and chewing of the lips and cheeks, were the criteria analyzed in both groups that composed the sample. According to the results, the oral health status of psychiatric patients was worse than that of healthy individuals, and those with special needs are more likely to have oral disorders. This study observed the prevalence of pain sensitivity in the masticatory muscles detected in 37.0% and 22.6% of the case and control groups, respectively, with temporal muscular pain present in 50.0% of the psychiatric patients and in 44.1% of the healthy volunteers. Cracking was present in 25.0% of the patients in the case group and in 27.4% of the control group, and only 1 psychiatric patient presented with limitation of mouth opening. Bruxism and tooth clenching were the most common parafunctions in both groups (34.5% in the control group and 27.0% in the case group).
In Latin America, a cross-sectional study was carried out to determine the most prevalent oral lesions in 65 hospitalized psychiatric patients at an institution in Caracas, Venezuela. The presence of TMJD was described, and 36.92% of the participants reported joint sounds and 10.76% reported muscular pain, particularly when the temporal muscle was palpated. Among the most prevalent parafunctional habits, the authors cited bruxism, nail biting and cheek chewing, leading to the conclusion that, in these patients, mouth changes are more often diagnosed than in mentally healthy individuals, and they pointed to the need for the implementation of oral health programs, with the commitment of the entire multidisciplinary team involved in mental health care.36Moralez-Cháves MC, Rueda-Delgado YM, Peña-Orozco DA. Prevalence of bucco-dental pathologies in patients with psychiatric disorders. → J Clin Exp Dent. 2014 Feb 1; 6(1):e 7–11. doi: 10.4317/jced.51147.
Conclusion
In this study, it was possible to observe the role of the adverse effects of typical APs in the onset of TMJD among patients with mental and behavioral disorders, thus justifying the monitoring of these patients through dental consultations. The identification of possible signs and symptoms of TMJD represents an important resource for the early diagnosis of this dysfunction. In this context, the use of indexes has been widely reported in the literature, especially when validated and easy to apply and interpret, and with a view to standardization for data comparison. The IAF can be used in the screening of patients for TMJD, since it has easy application and interpretation; however, owing to its subjective nature, it requires more accurate examination.
Interview
with Elizabeth Maria Costa de Carvalho
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Wang YP, Minatogawa TM, Júnior HT. Psicofarmacologia dos transtornos psicóticos. In: Teng CT, Demetrio FN, editors. Psicofarmacologia aplicada: manejo prático dos transtornos mentais. 2ª ed. → São Paulo: Atheneu; 2011. p. 17–56. |
| 2. | ↑ | Jamelli SR, Mendonça MC, Dinis MG, De Andrade FB, De Melo JF, Ferreira SR, Silva PV. Saúde bucal e percepção sobre o atendimento odontológico em pacientes com transtorno psíquico moradores de residências terapêuticas [Oral health and perceptions regarding dental care in patients with mental disorders living in therapeutic residences]. → Ciêencias & Saúude Coletiva. 2010 Jun;15 Suppl 1:1795–1800. |
| 3, 4. | ↑ | Jovanovic S, Milovanovic SD, Gajic I, Mandic J, Latas M, Jankovic L. Oral health status of psychiatric in patients in Serbia and implications for their dental care. → Croat Med J. 2010 Oct;51(5):443–450. |
| 5, 6. | ↑ | Tanasiewicz M, Skucha-Nowak M, Gren A, Hese RT, Twardawa H, Gorczyca P. Analysis of state of the oral cavity in schizophrenic in patients treated with atypical and classical neuroleptics. → Adv Clin Exp Med. 2011, Mar–Apr; 20(2):187–197. |
| 7, 10, 25, 36. | ↑ | Moralez-Cháves MC, Rueda-Delgado YM, Peña-Orozco DA. Prevalence of bucco-dental pathologies in patients with psychiatric disorders. → J Clin Exp Dent. 2014 Feb 1; 6(1):e 7–11. doi: 10.4317/jced.51147. |
| 8, 11. | ↑ | Elias R. Odontologia de alto risco: pacientes especiais. 1ª ed. → Rio de Janeiro: Revinter; 1995. p. 35–45. |
| 9, 12, 14, 19. | ↑ | Pereira CC, Felício CM. Os distúrbios miofuncionais orofaciais na literatura odontológica: revisão crítica [The orofacials myofunctional disorders in the dentistry publication: critical review]. → Revev Dental Press Ortodon Ortop Facial. 2005 Jul–Aug;10(4):134– 142. |
| 13. | ↑ | Benevides SD. Determinação do padrão da amplitude dos movimentos mandibulares em escolares de 8 a 12 anos [doctoral thesis]. → [Salvador]: Universidade Federal da Bahia, Instituto de Ciências e Saúde; 2013: 132. |
| 15, 33. | ↑ | Karthik MS, Prabhu N. Temporomandibular joint dislocation due to atypical antipsychotic-induced acute dystonia: a case report. → Ther Adv Psychopharmacol. 2014 Dec;4(6):282–284. |
| 16, 31, 32. | ↑ | Ferreira KD, Guimarães JP, Batista CH, Júnior AM, Ferreira LA. Fatores psicológicos relacionados à sintomatologia crônica das desordens ttemporomandibulares— revisão de literaturea [Related psychological factors in chronic temporomandibular disorder—literature review]. → Rev Fac Odontol Univ Passo Fundo. 2009 Sep–Dec;14(3):262–267. |
| 17, 18, 28. | ↑ | Fonseca, DM. et al. Diagnóstico pela anamnese da disfunção craniomandibular. → Rev. Gauch. Odontol. 1994 Jan/Feb; 42(1): 23-28. |
| 20, 24, 34. | ↑ | Gurbuz O, Alatas G, Kurt E. Prevalence of temporomandibular disorder signs in patients with schizophrenia. → J Oral Rehabil. 2009 Dec; 36(12): 864–71. |
| 21, 35. | ↑ | Al-Mobeeriek A. Oral health status among psychiatric patients in Riyadh, Saudi Arabia. → West Indian Med J. 2012 Aug;61(5):549–554. |
| 22. | ↑ | Araújo AN, Nascimento MA, Sena EP, Baptista AF. Temporomandibular disorders in patients with schizophrenia using antipsychotic agents: a discussion paper. → Drug Healthc Patient Saf. 2014 Mar; 10;(6): 21–27. doi: 10.2147/ DHPS.S57172. |
| 23. | ↑ | Velasco-Ortega E, Guil LM, Ponferrada CV, Soteras RM, Egea JJ. Temporomandibular disorders among schizophrenic patients. A case-control study. → Med Oral Patol Oral Cir Bucal. 2005 Aug–Oct;10(4):315–22. |
| 26. | ↑ | Pedrosa AS. Propriedades de medida do Índice Anamnésico de Fonseca : Universidade Cidade de São Paulo; 2011: 62 http://arquivos.cruzeirodosuleducacional. edu.br/principal/old/mestrado_fisioterapia/ pdf/dissertacao_alexsandra_de_ souza_pedrosa.pdf |
| 27. | ↑ | Chaves TC, Costa D, Grossi DB, Bertolli F. Avaliação anamnésica de sintomas de disfunção temporomandibular em crianças asmáticas. [The anamnestic evaluation of temporomandibular dysfunction symptoms in asthmatic children]. → Fisiot e Pesq. 2005 Jan-Apr;11(1):19–26. |
| 29. | ↑ | Chaves TC, Oliveira AS, Grossi DB. Principais instrumentos para avaliação da disfunção temporomandibular, parte I: índices e questionários; uma contribuição para a prática clínica e de pesquisa. [Main instruments for assessing temporomandibular disorders, part I: indices and questionnaires; a contribution to clinicians and researchers]. → Fisiot e Pesq. 2008 Mar;15(1):92–100. |
| 30. | ↑ | George W, Arana MD. An overview of side effects caused by typical antipsychotics. → J Clin Psychiatry. 2000; 61 (Suppl 8):5–11. |





Leave a Reply
Be the First to Comment!