Evaluation of the muscular activity and myodynamic balance in children with physiological dental occlusion
June 14, 2019 / Categories: Digital Dentistry, Implant Dentistry

Nabiev, Nabi

Klimova, Tatiana

Cesaretti, Gianfranco

Tanaka, Kazushige

Botticelli, Daniele

Persin, Leonid
Abstract
Objective
The objective was to evaluate the homogeneous myoelectric activity of the maxillofacial area and to identify the myodynamic musculature balance in children of different ages with a physiological dental occlusion.
Materials and methods
Sixty children, 30 aged 7–9 years and 30 aged 10–12 years, with an Angle Class I relationship and who had no clinical symptoms, temporomandibular disorders, cross bite, deep bite or open bite, and were not bruxers underwent a surface electromyographic examination. The bioelectric potentials of the left and right temporalis, masseter, suprahyoid and sternocleidomastoid muscles were evaluated in maximum clenching.
Results
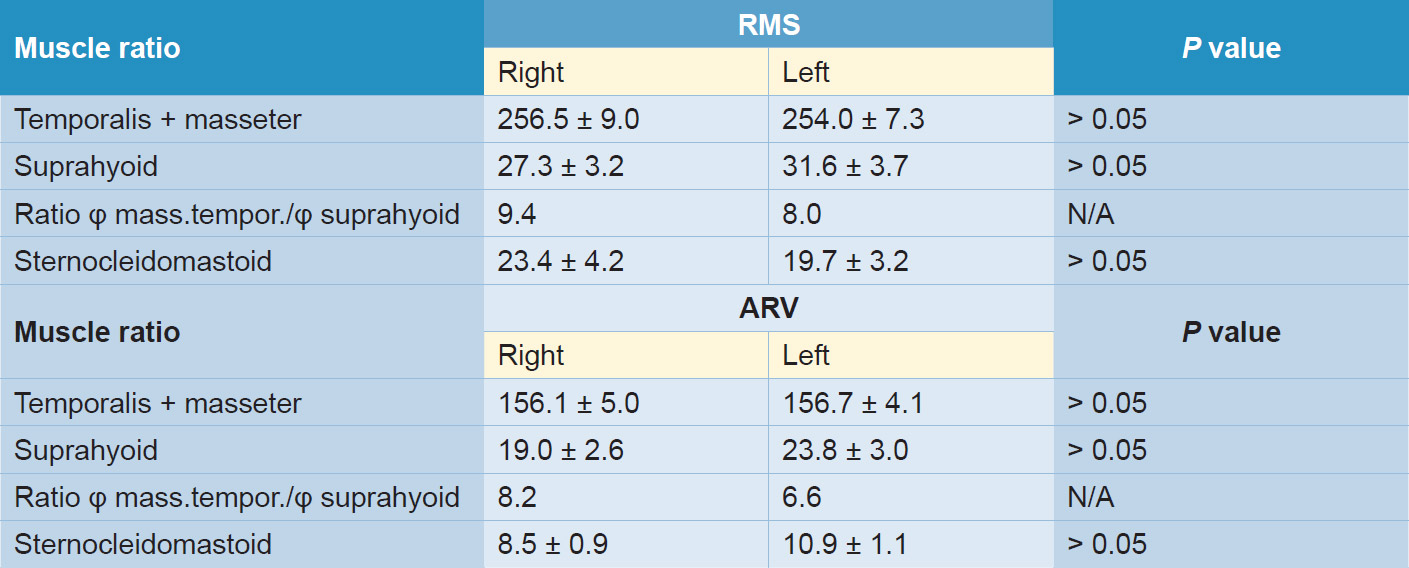
The electroactivity of the muscles measured with root mean square and average rectified value did not present statistically significant differences between the groups, even though different values in relation to age were found. Among the 7- to 9-year-olds, the root mean square index in maximum clenching for the masticatory muscles was 256.5 ± 9.0 μV on the right and 254.0 ± 7.3 μV on the left and for the suprahyoid muscles was 27.3 ± 3.2 μV and 31.6 ± 3.7 μV, respectively. In the group of 10- to 12-year-olds, the values were 374.8 ± 15.5 μV and 354.0 ± 16.4 μV, respectively, for the masticatory muscles and 23.4 ± 1.9 μV and 22.4 ± 2.1 μV, respectively, for the suprahyoid muscles.
Conclusion
Any deviation from the values reported in the present study suggests the presence of occlusal and/or postural problems.
Keywords
Clinical research protocol; clinical trial; randomized controlled trial; dental occlusion; stomatognathic system; masticatory system; orthodontics
Introduction
Surface electromyography (sEMG) is an objective information tool of the functional state of the neuromuscular system of the masticatory apparatus.1Cram JR, Kasman GS, Holtz J. Introduction to surface electromyography. → Gaithersburg (MD): Aspen; 1998. 408 p. Technological progress has made it possible to extend the scope of measurement tools in stomatology; the development of digital techniques has allowed the creation of surface electromyographs that combine analog equipment and computers. The latter receives the signals detected by the surface electromyograph in digital and then processes and displays them in tables, histograms and other graphs (Fig. 1).
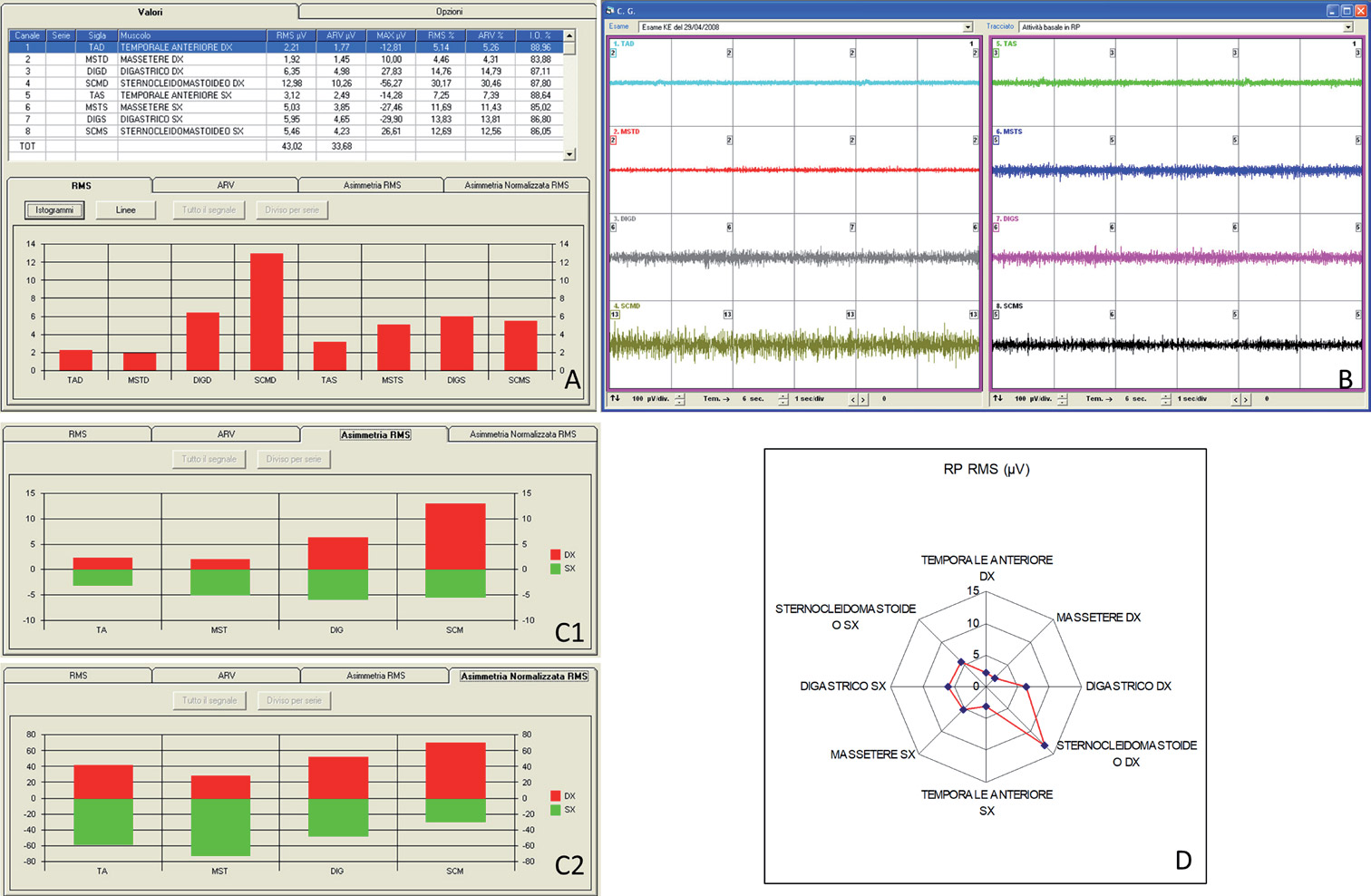
Fig. 1
The use of surface electromyographs requires precise information on the normal average values of average normality of different age groups and of the muscular biopotentials, both for agonist and antagonist muscles, with particular reference to the temporalis, masseter, suprahyoid and sternocleidomastoid muscles. Several studies have compared the outcomes of adults with adults,2Gadotti IC, Bérin F, Biasotto-Gonalez D. Preliminary rapport on head posture and muscle activity in subjects with Class I and II. → J Oral Rehabil. 2005 Nov;32(11):794–9.,3Ferrario VF, Tartaglia GM, Galletta A, Grassi GP, Sforza C. The influence of occlusion on jaw and neck muscle activity: a surface EMG study in healthy young adults. → J Oral Rehabil. 2006 May;33(5):341–8.,4Moreno I, Sánchez T, Ardizone I, Aneiros F, Celemin A. Electromyographic comparisons between clenching, swallowing and chewing in jaw muscles with varying occlusal parameters. → Med Oral Patol Oral Cir Bucal. 2008 Mar 1;13(3):E207–13.,5Cecílio FA, Regalo SC, Palinkas M, Issa JP, Siéssere S, Hallak JE, Machado-de-Sousa JP, Semprini M. Ageing and surface EMG activity patterns of masticatory muscles. → J Oral Rehabil. 2010 Apr;37(4):248–55.,6Petrović D, Vujkov S, Petronijević B, Šarčev I, Stojanac I. Examination of the bioelectrical activity of the masticatory muscles during Angle’s Class II division 2 therapy with an activator. → Vojnosanit Pregl. 2014 Dec;71(12):1116–22. children with adults7Nakakawaji K, Kodachi K, Sakamoto T, Harazaki M, Isshiki Y. Correlation between facial patterns and function of the masticatory muscles in girls and women. → Bull Tokyo Dent Coll. 2002 May;43(2):51–9. and children with children,8Díaz-Serrano KV, Dias TM, Vasconcelos P, Sousa LG, Siéssere S, Regalo S, Palinkas M. Impact of temporomandibular disorders on the stomatognathic system in children. → Med Oral Patol Oral Cir Bucal. 2017 Nov 1;22(6):e723–e729. doi: 10.4317/ medoral.22000.,9Lucas Bde L, Barbosa Tde S, Pereira LJ, Gavião MB, Castelo PM. Electromyographic evaluation of masticatory muscles at rest and maximal intercuspal positions of the mandible in children with sleep bruxism. → Eur Arch Paediatr Dent. 2014 Aug;15(4):269–74.,10De Rossi M, De Rossi A, Hallak JE, Vitti M, Regalo SC. Electromyographic evaluation in children having rapid maxillary expansion. → Am J Orthod Dentofacial Orthop. 2009 Sep;136(3):355–60.,11Andrade AS, Gavião MB, Derossi M, Gameiro GH. Electromyographic activity and thickness of masticatory muscles in children with unilateral posterior crossbite. → Clin Anat. 2009 Mar;22(2):200–6.,12Ueda HM, Miyamoto K, Saifuddin M, Ishizuka Y, Tanne K. Masticatory muscle activity in children and adults with different facial types. → Am J Orthod Dentofacial Orthop. 2000 Jul;118(1):63–8.,13Negoro T, Briggs J, Plesh O, Nielsen I, McNeill C, Miller AJ. Bruxing patterns in children compared to intercuspal clenching and chewing as assessed with dental models, electromyography, and incisor jaw tracing: preliminary study. → ASDC J Dent Child. 1998 Nov–Dec;65(6):449–58, 438. showing in every case different occlusal diseases. To date, the muscular activity of the masticatory complex in healthy children of different ages with a physiological dental occlusion has not been considered.
The present study was aimed at evaluating the homogeneous myoelectric activity of the maxillofacial area and at identifying the myodynamic musculature balance (masseter, temporalis and suprahyoid muscles) in children of different ages with a physiological dental occlusion. Physiological dental occlusion was regarded as an Angle Class I relationship and no clinical symptoms, temporomandibular disorders, cross bite, deep bite, open bite or bruxism. The null hypothesis was that myoelectric activity in children is associated with age, which is the reason 2 age groups were selected.
Materials and methods
Sixty children, 30 aged 7–9 years and 30 aged 10–12 years, with physiological dental occlusion, underwent an electromyographic examination. The bioelectric potentials of the left and right temporalis, masseter, suprahyoid and sternocleidomastoid muscles were evaluated with the BioKeyNet surface electromyograph (Bioket, San Benedetto del Tronto, Italy). The biopotentials of the muscles were recorded using single-use surface electrodes, taking into account the recommendations of various authors.14Cram JR, Kasman GS, Holtz J. Introduction to surface electromyography. → Gaithersburg (MD): Aspen; 1998. 408 p.,15Persin LS. Functional characteristics of properly masticatory muscles and temporomandibular joints in children with normal and prognathic bite during the period of substitution of deciduous dentition [master’s thesis]. → [Мoscow]: University of Moscow; 1974. 215 p.,16Persin LS. Electrophysiological investigations of the muscles in the maxillo-facial area and temporomandibular joints in children with normal and abnormal (prognathic) bites during the period of substitution of deciduous dentition [doctoral thesis]. → [Мoscow]: University of Moscow; 1978. 207 p.
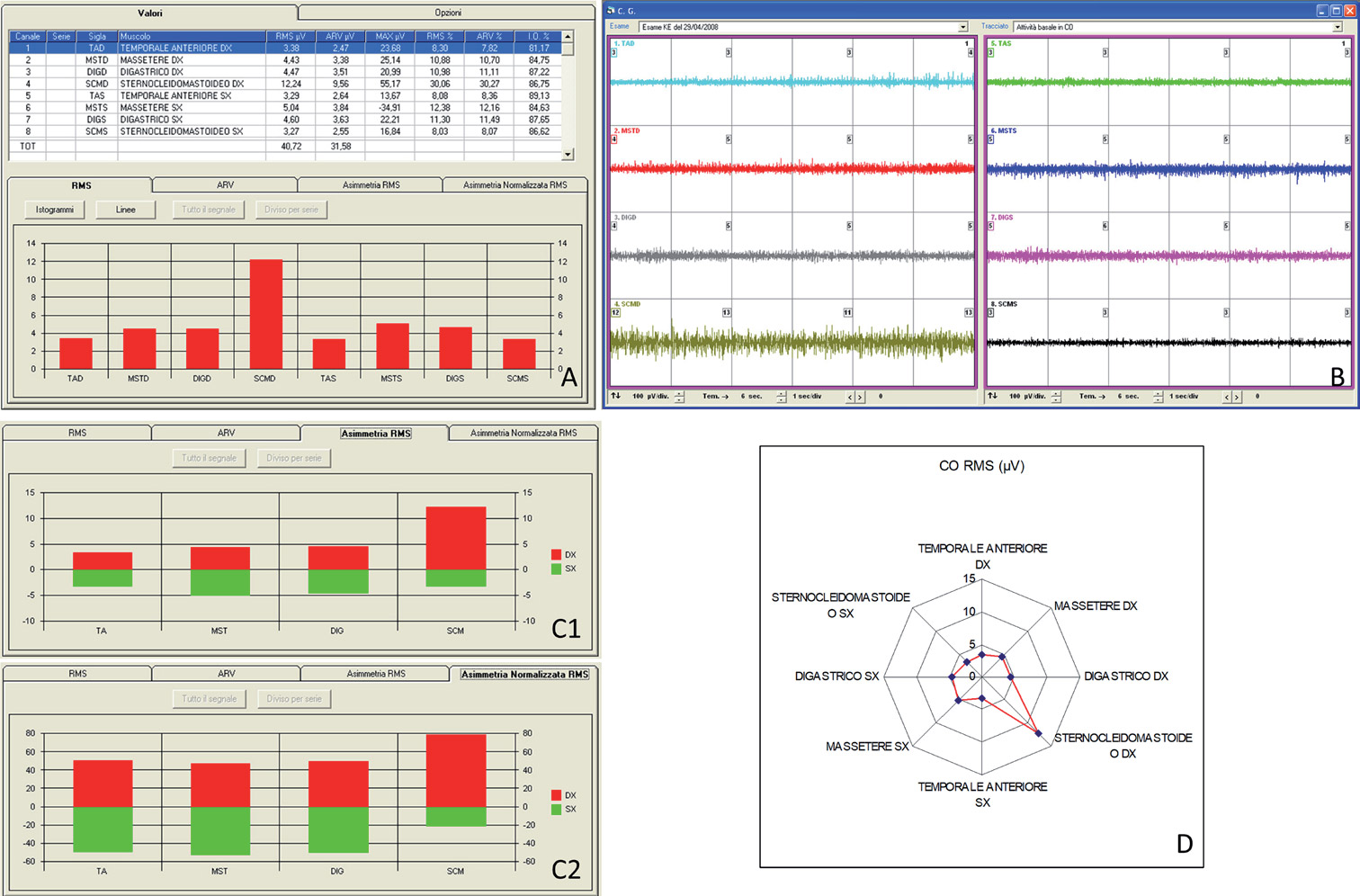
Fig. 2
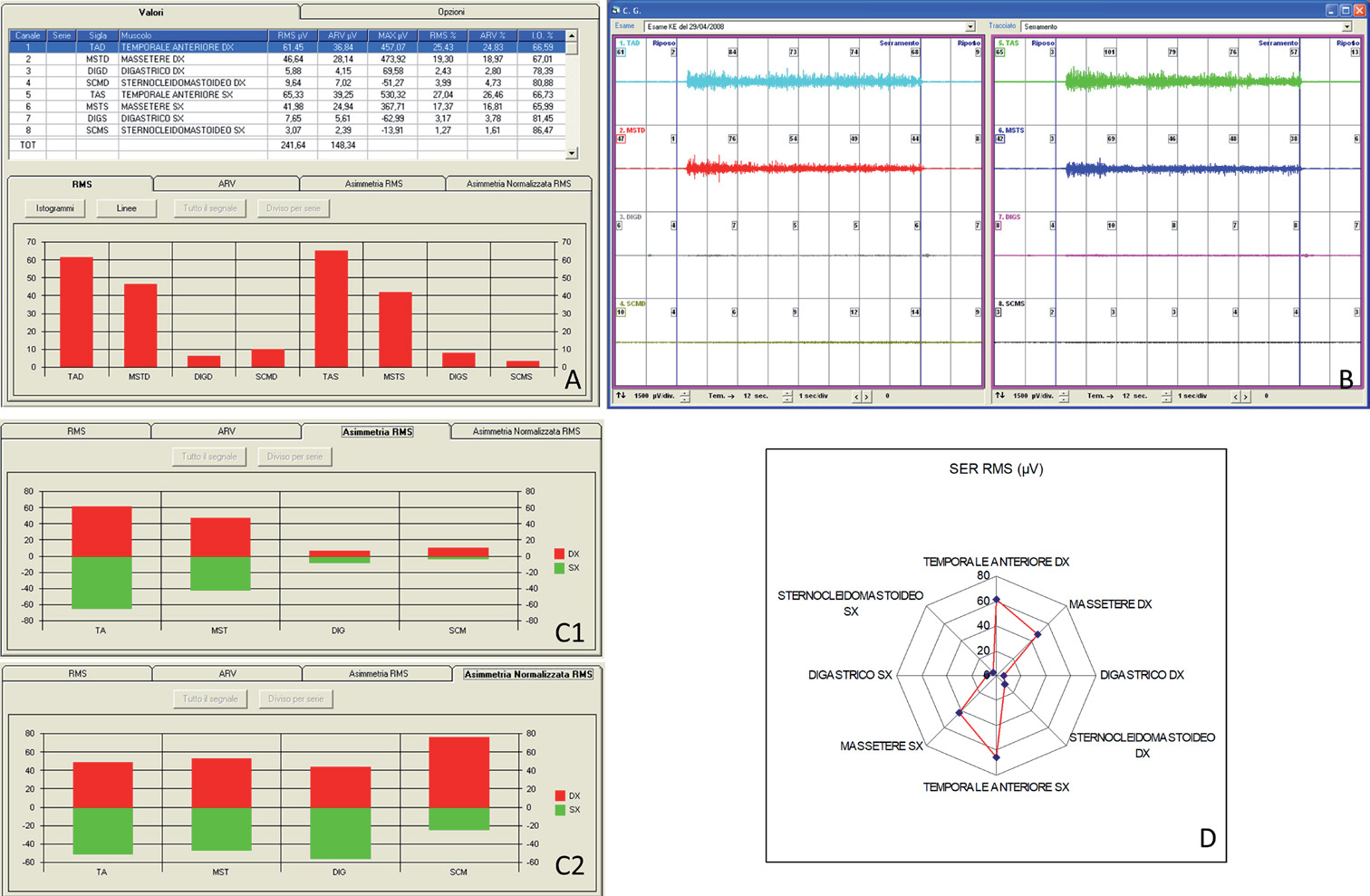
Fig. 3
φ Mass.tempor. = total value of biopotentials of temporalis and masseter muscles.
φ Suprahyoid = mean values of biopotentials of the suprahyoid muscles.
Table 1
Myodynamic balance of maxillofacial muscles at the time of dental clenching at maximum effort in 7- to 9-year-old children 7-9 years old with physiological occlusion (RMS and ARV in μV).
φ Mass.tempor. = total value of biopotentials of temporalis and masseter muscles.
φ Suprahyoid = mean values of biopotentials of the suprahyoid muscles.
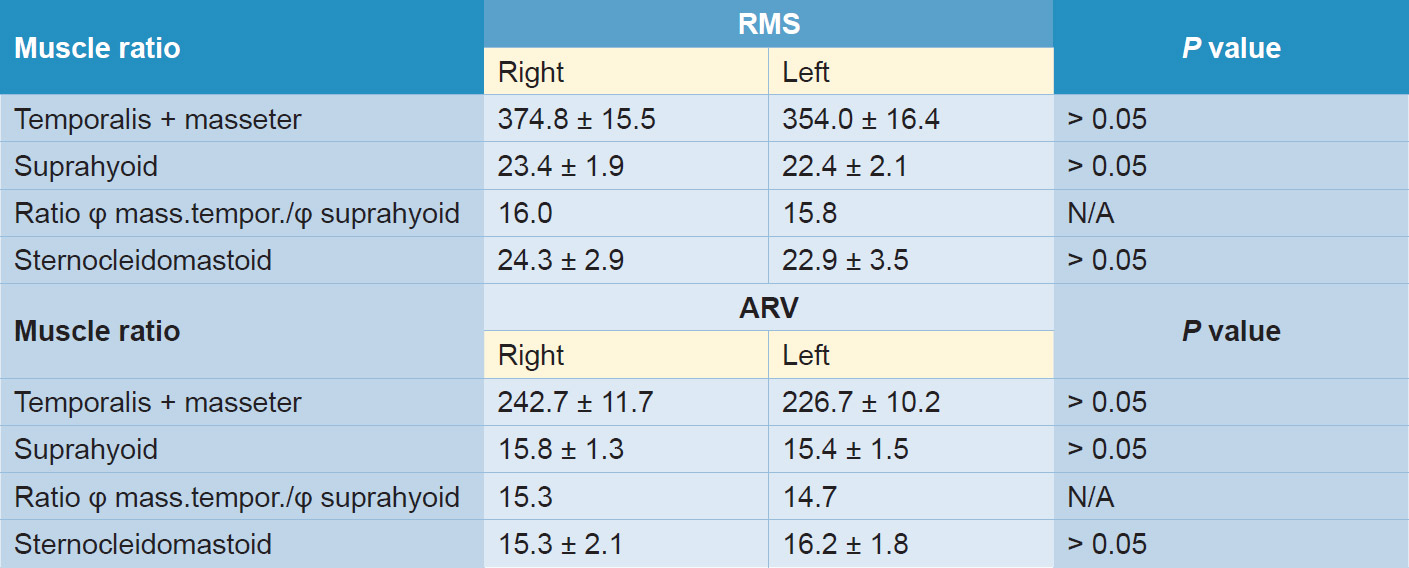
Table 2
Myodynamic balance of maxillofacial muscles at the time of dental clenching at maximum effort in 10- to 12-year-old children with physiological dental occlusion (RMS and ARV in μV).
On the skin in the motor area of the muscle under examination, pre-gelled self-adhesive electrodes based on silver chloride were fixed parallel to the muscular fibers, with an interelectrode distance of 22 mm. The configuration of the input channels of the surface electromyograph is of the differential type: (i) the potential difference between the positive electrode and the negative electrode is detected; (ii) a reference electrode (ground) is placed in a zone nonelectrically connected to the points to be monitored. The bioelectric signal arising from the muscle fibers, when the skin is reached, is detected by the electrodes and then amplified and filtered (elimination of disturbances). The bioelectric signal is acquired, converted into digital form and transmitted to the computer for real-time display on the monitor.
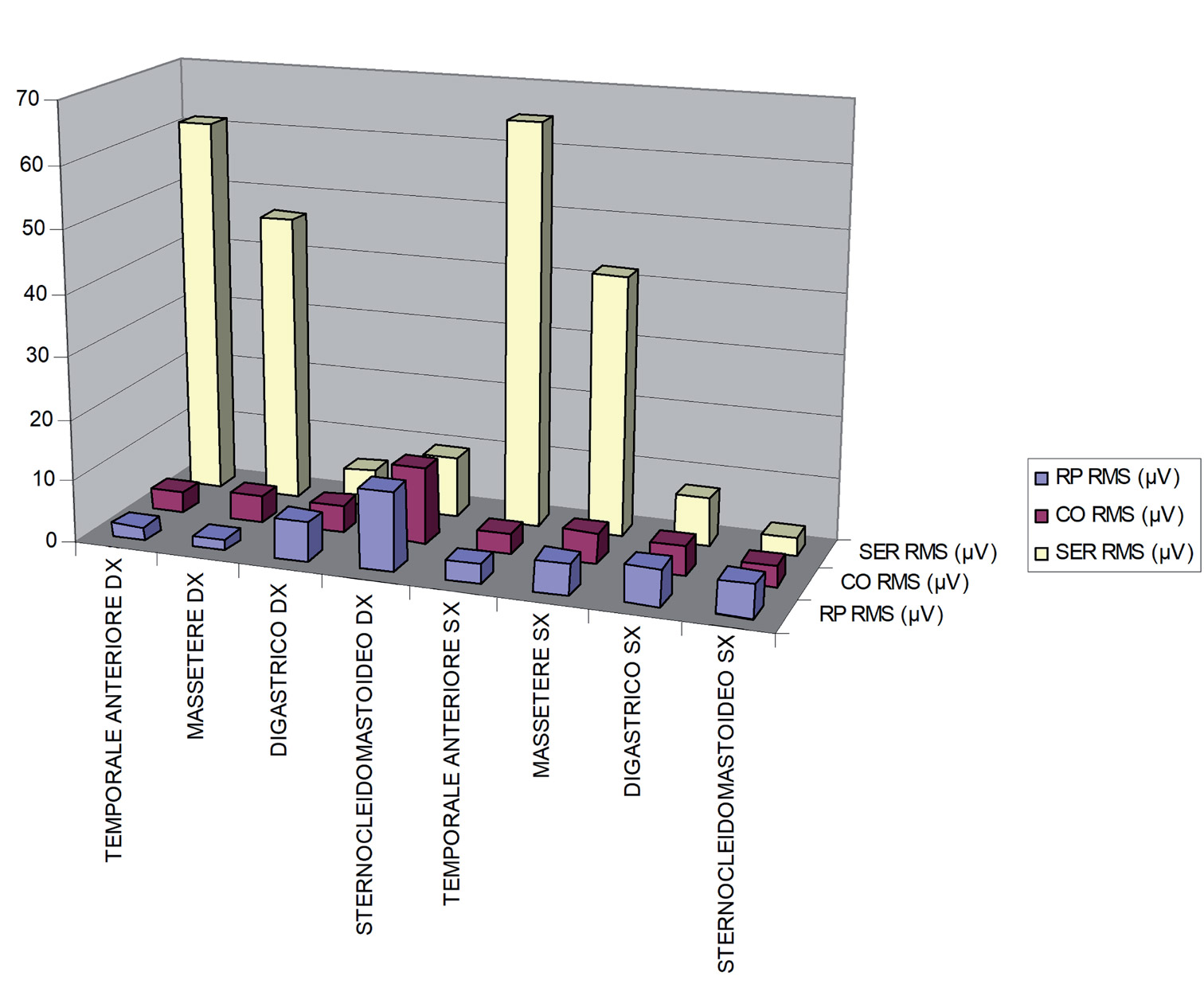
Fig. 4
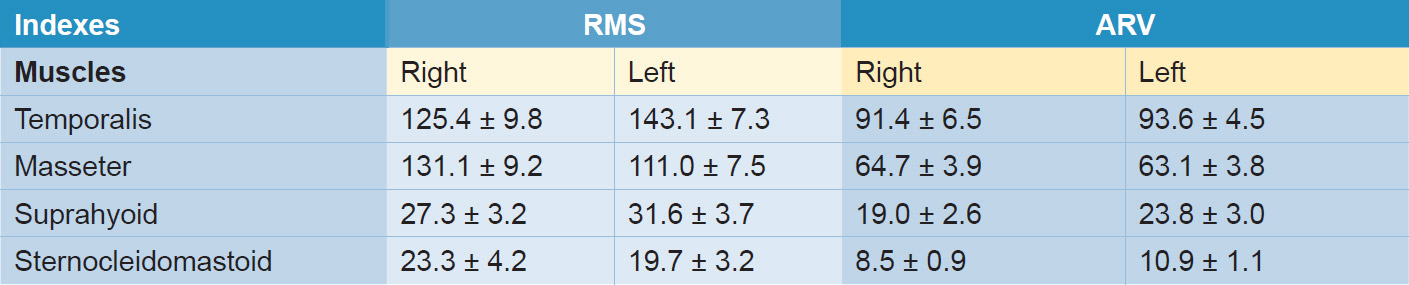
Table 3
Myodynamic balance of maxillofacial muscles at the time of dental clenching at maximum effort in 7- to 9-year-old children with physiological dental occlusion (RMS and ARV in μV).
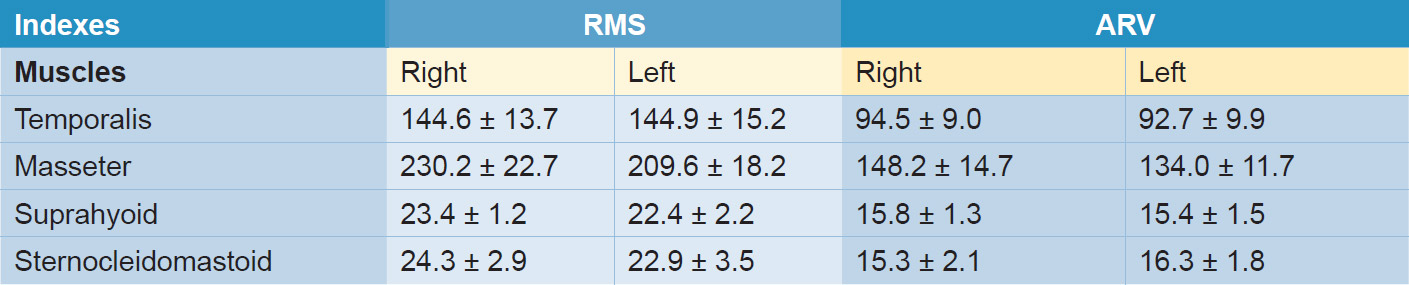
Table 4
Myodynamic balance of maxillofacial muscles at the time of dental clenching at maximum effort in 10- to 12-year-old children with physiological dental occlusion (RMS and ARV in μV).
The sEMG analysis was performed using the following functional tests:
- mandible in relative physiological rest state, that is, teeth not in contact and lips just in contact (Fig. 1);
- mandible in physiological position of occlusion, that is, teeth in contact (Fig. 2); and
- mandible in voluntary clenching to the maximum effort (Fig. 3).
The main index of the functional state of a muscle is the value of the amplitude of its biological potential. Currently, 2 average amplitude indices, root mean square (RMS) and average rectified value (ARV), are mainly used. The maximum amplitude of the electromyographic signal is measured from the maximum positive peak to the maximum negative peak. The individual measured values can be processed to obtain the mean value of the absolute value with respect to the period. This index is the mean value of the adjusted signal (ARV), and it is usually expressed in μV.17Moreno I, Sánchez T, Ardizone I, Aneiros F, Celemin A. Electromyographic comparisons between clenching, swallowing and chewing in jaw muscles with varying occlusal parameters. → Med Oral Patol Oral Cir Bucal. 2008 Mar 1;13(3):E207–13.,18Cecílio FA, Regalo SC, Palinkas M, Issa JP, Siéssere S, Hallak JE, Machado-de-Sousa JP, Semprini M. Ageing and surface EMG activity patterns of masticatory muscles. → J Oral Rehabil. 2010 Apr;37(4):248–55.The RMS index represents the value of a continuous voltage that develops a power equivalent to that of the electromyographic signal (alternating voltage). This index is calculated as the square root of the mean quadratic value of the electromyographic signal, and it is expressed in μV. Most of the other indexes, calculated according to the software, are derived from the ARV and RMS amplitude indices. The following electromyographic indices19Moreno I, Sánchez T, Ardizone I, Aneiros F, Celemin A. Electromyographic comparisons between clenching, swallowing and chewing in jaw muscles with varying occlusal parameters. → Med Oral Patol Oral Cir Bucal. 2008 Mar 1;13(3):E207–13.,20Cecílio FA, Regalo SC, Palinkas M, Issa JP, Siéssere S, Hallak JE, Machado-de-Sousa JP, Semprini M. Ageing and surface EMG activity patterns of masticatory muscles. → J Oral Rehabil. 2010 Apr;37(4):248–55. were analyzed:
- RMS of biopotentials (expressed in μV);
- ARV of biopotentials (expressed in μV);
- total bioelectric activity (Total index, expressed in μV): the sum of all the ARV or RMS indices related to the bioelectric activity of the right and left muscles;
- participation in the bioelectric activity by each muscle in question expressed in % (calculated according to both the ARV and RMS indices)—the calculation of these participation indices was performed by dividing the bioelectric activity index of each muscle (in ARV or RMS) for the total index and subsequently multiplying by 100; and
- maximum amplitude of biopotentials index (Max; expressed in μV). The results of the present study were statistically analyzed using BioStat software (AnalystSoft). An α < 0.05 was used.
Results
Tables 1 and 2 show the sum parameters of the left and right temporalis, masseter, suprahyoid and sternocleidomastoid muscles (Fig. 4). These parameters have been taken from Table 3 for Table 1 and from Table 4 for Table 2, respectively.
The data showed that, in 7- to 9-year-olds with physiological dental occlusion, the position of the mandible at the time of voluntary clenching at maximum effort can be normal only if the total value of the masticatory muscles (RMS; temporalis and masseter) is within the limits of 256.5 ± 9.0 μV on the right and 254.0 ± 7.3 μV on the left, and of the suprahyoid (digastric) muscles within 27.3 ± 3.2 μV on the right and 31.6 ± 3.7 μV on the left. The ratio of the temporalis and masseter muscles to the suprahyoid muscles was 9.4 times on the right and 8.0 on the left for the RMS index, and 8.2 and 6.6 times, respectively, for the ARV index. It should be noted that, in the case of normal posture, the biopotentials of the sternocleidomastoid muscles were within the limits of 23.4 ± 4.2 μV on the right and 19.7 ± 3.2 μV on the left.
The normal position of the jaw at the time of voluntary clenching at maximum effort in the 10- to 12-yearolds was possible when the total value of the temporalis and masseter muscles was within the limits of 374.8 ± 15.5 μV on the right and 354.0 ± 16.4 μV on the left, of the suprahyoid muscles was within 23.4 ± 1.9 μV on the right and 22.4 ± 2.1 μV on the left. The ratio of the temporalis and masseter muscles to the suprahyoid muscles was 16.0 times on the right and 15.8 times on the left for the RMS index, and 15.3 and 14.7 times, respectively, for the ARV index. In the 10- to 12-year-olds in normal posture, the biopotentials of the sternocleidomastoid muscles were within the limits of 24.3 ± 2.9 μV on the right and 22.9 ± 3.5 μV on the left. It should be noted that, in both age groups, no reliable differences were found between the parameters of the masseter, temporalis, suprahyoid and sternocleidomastoid muscles on the right and on the left, respectively.
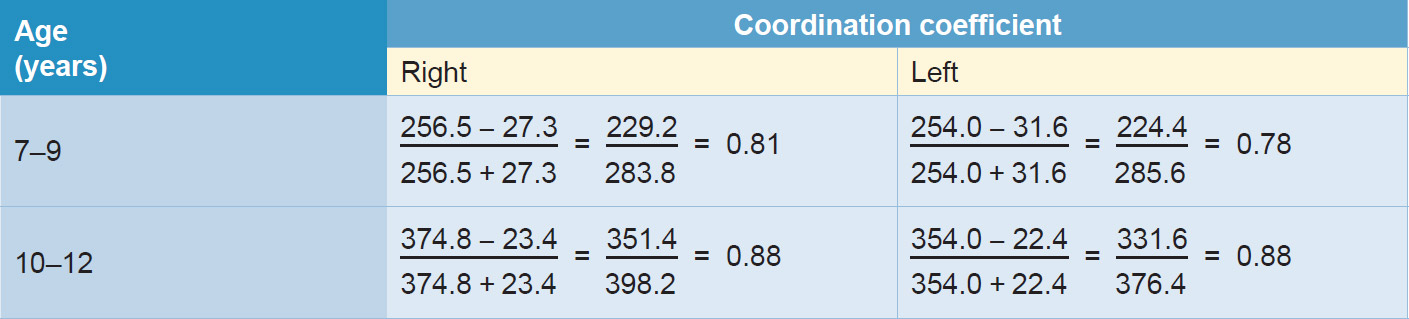
Table 5
Coordination coefficient values in relation to the RMS index at the time of voluntary clenching at maximum effort in children aged 7–9 and 10–12 years with physiological occlusion.
Table 5 shows that the coordination coefficient for the maxillofacial area muscles evaluated at the time of voluntary clenching at maximum effort in the 7- to 9-year-olds was within the limits of 0.81 on the right and 0.78 on the left. In the 10- to 12-year-olds, at the end of the period of transition from primary dentition, the coordination coefficient was higher compared with the 7- to 9-year-olds, and it was the same (0.88) for both sides. This indicates that, toward the end of the replacement of the primary dentition, the muscles of the maxillofacial area on the left and on the right work in a homogeneous regimen.
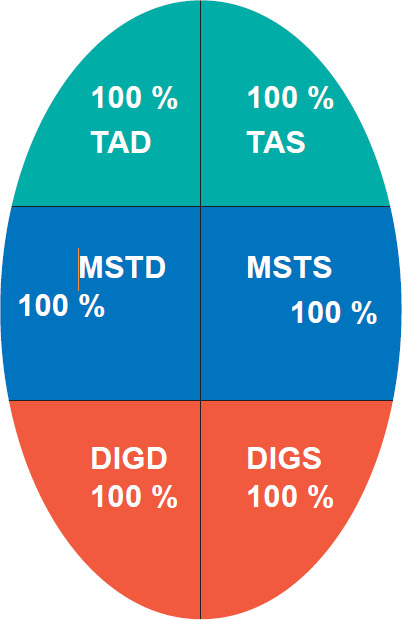
Fig. 5
Discussion
The present study evaluated the homogeneous muscular activity in the maxillofacial area and identified myodynamic balance in children with physiological dental occlusion. The mean biopotential values were identified of the masseter, temporalis and suprahyoid muscles, which participate directly in the retention of the physiological position of the resting jaw at the time of voluntary clenching at maximum effort. The mean values of the biopotentials of the muscles were assessed, as was the muscular myodynamic balance on the right and on the left. It was seen that the homogeneity of the muscular activity improves with age.
It is very important to establish the myodynamic balance of the muscles of the maxillofacial area between the right and left and compare them, since they condition the normal position (normognatic) of the jaw. In unbalanced conditions, the mandible may be displaced either to the right or to the left, as well as in a distal or mesial direction. In addition, to study the myodynamic balance of the muscles of the maxillofacial area, it is necessary to have information on the homogeneous activity of the agonist and antagonist muscles, both in physiological or pathological conditions.
The coordination coefficient provides a value that expresses the balance of the muscles between the right and left in rest position and at maximum clenching. The myodynamic equilibrium and homogeneous muscular activity are illustrated in Figure 5, where the parameters of the masseter, temporalis and suprahyoid muscles in children with physiological dental occlusion are considered to be entirely normal. The intensity of the color changes according to the sEMG parameters and the deviation from the mean.
As mentioned before, previous studies on children compared patients with diseases. However, in those studies, the values in μV were assessed for dental clenching with cotton rolls and expressed as percentages of maximum voluntary clenching. This means that a direct comparison with the data from the present study is difficult. However, it should be considered that the use of cotton rolls during maximum clenching should increase the values in μV compared with maximum clenching without cotton rolls. Nevertheless, varying findings have been reported in several studies performed in children. In a clinical study,21Díaz-Serrano KV, Dias TM, Vasconcelos P, Sousa LG, Siéssere S, Regalo S, Palinkas M. Impact of temporomandibular disorders on the stomatognathic system in children. → Med Oral Patol Oral Cir Bucal. 2017 Nov 1;22(6):e723–e729. doi: 10.4317/ medoral.22000. for example, the electromyographic activity and thickness of the right masseter, left masseter, right temporalis and left temporalis muscles and bite force in children with temporomandibular disorders were evaluated. The bite force was lower in the temporomandibular disorders group than in the control group. In another study,22Lucas Bde L, Barbosa Tde S, Pereira LJ, Gavião MB, Castelo PM. Electromyographic evaluation of masticatory muscles at rest and maximal intercuspal positions of the mandible in children with sleep bruxism. → Eur Arch Paediatr Dent. 2014 Aug;15(4):269–74. the electromyographic activity of the masseter and anterior portion of the temporalis muscles was evaluated in children with and without sleep bruxism. Children with sleep bruxism showed no significant difference in EMG of masticatory muscles at rest and in maximal intercuspal positions of the mandible compared with the control group.
In another study,23De Rossi M, De Rossi A, Hallak JE, Vitti M, Regalo SC. Electromyographic evaluation in children having rapid maxillary expansion. → Am J Orthod Dentofacial Orthop. 2009 Sep;136(3):355–60. the electromyographic activity of the temporalis and masseter muscles was evaluated in children with mixed dentition and a mean age of 8.6 years. All the children were undergoing rapid maxillary expansion with a bonded rapid maxillary expansion appliance. The electromyographic analysis showed that the activity of the temporalis and masseter muscles increased significantly when the expansion appliance was removed. During dental clenching with cotton rolls, the values in μV expressed as percentages of the maximum voluntary clenching increased from ~ 112–113 μV to 143–149 μV for the masseter muscles and from ~ 102 μV to 116–135 μV for the temporalis muscles. In the present study, in children with physiological dental occlusion, the data were higher during maximum voluntary clenching, 256.5 μV for the temporalis and masseter muscles. This might indicate that the removal of the rapid maxillary expansion appliance in the previously discussed study24De Rossi M, De Rossi A, Hallak JE, Vitti M, Regalo SC. Electromyographic evaluation in children having rapid maxillary expansion. → Am J Orthod Dentofacial Orthop. 2009 Sep;136(3):355–60. did not permit normal myoelectric activity of these muscles.
In conclusion, the present study provided the range of physiological function of the masticatory and sternocleidomastoid muscles that children aged 7–9 and 10–12 should present in a myographic examination. Any deviation from these values suggests the presence of occlusal and/or postural problems, and an appropriate intervention to reach the values indicated in the present study should be considered.
Competing interests
The authors declare that they have no competing interests.
Legends
Fig. 1 – (A) Data acquired digitally and represented in the form of tables and histograms. Signal evaluated in relative physiological rest state. (B) Raw signal in relative physiological rest state. (C1) Histogram representation of asymmetrical root mean square signals in relative physiological rest state; (C2) signals normalized. (D) Further graphic representation of the mandible signals in relative physiological rest state.
Fig. 2 – (A) Representation in tables and histograms of the signal in the physiological position of occlusion (teeth in contact). (B) Raw signal in physiological dental occlusion position (teeth in contact). (C1) Histogram representation of asymmetrical root mean square signals in physiological dental occlusion position (teeth in contact); (C2) signals normalized. (D) Further graphic representation of the mandible signals in physiological dental occlusion position (teeth in contact).
Fig. 3 – (A) Representation in tables and histograms of the signal in voluntary clenching at maximum effort. (B) Raw signal in voluntary clenching at maximum effort. (C1) Histogram representation of asymmetrical root mean square signals in voluntary clenching at maximum effort; (C2) signals normalized. (D) Further graphic representation of the mandible signals in voluntary clenching at maximum effort.
Fig. 4 – Summary representation in a histogram of the functional tests performed.
Fig. 5 – Myodynamic equilibrium and homogeneous muscular activity. TAD = Right anterior temporalis; TAS = Left anterior temporalis; MSTD = Right masseter; MSTS = Left masseter; DIGD = Right digastric; DIGS = Left digastric. The intensity of the color Myodynamic balance in children 42 Journal of Oral Science & Rehabilitation | Volume 5 – Issue 2/2019 Myodynamic balance in children changes according to the sEMG parameters and the deviation from the mean. In the present diagram, the color intensity is 100% for each parameter.
References
| 1, 14. | ↑ | Cram JR, Kasman GS, Holtz J. Introduction to surface electromyography. → Gaithersburg (MD): Aspen; 1998. 408 p. |
| 2. | ↑ | Gadotti IC, Bérin F, Biasotto-Gonalez D. Preliminary rapport on head posture and muscle activity in subjects with Class I and II. → J Oral Rehabil. 2005 Nov;32(11):794–9. |
| 3. | ↑ | Ferrario VF, Tartaglia GM, Galletta A, Grassi GP, Sforza C. The influence of occlusion on jaw and neck muscle activity: a surface EMG study in healthy young adults. → J Oral Rehabil. 2006 May;33(5):341–8. |
| 4, 17, 19. | ↑ | Moreno I, Sánchez T, Ardizone I, Aneiros F, Celemin A. Electromyographic comparisons between clenching, swallowing and chewing in jaw muscles with varying occlusal parameters. → Med Oral Patol Oral Cir Bucal. 2008 Mar 1;13(3):E207–13. |
| 5, 18, 20. | ↑ | Cecílio FA, Regalo SC, Palinkas M, Issa JP, Siéssere S, Hallak JE, Machado-de-Sousa JP, Semprini M. Ageing and surface EMG activity patterns of masticatory muscles. → J Oral Rehabil. 2010 Apr;37(4):248–55. |
| 6. | ↑ | Petrović D, Vujkov S, Petronijević B, Šarčev I, Stojanac I. Examination of the bioelectrical activity of the masticatory muscles during Angle’s Class II division 2 therapy with an activator. → Vojnosanit Pregl. 2014 Dec;71(12):1116–22. |
| 7. | ↑ | Nakakawaji K, Kodachi K, Sakamoto T, Harazaki M, Isshiki Y. Correlation between facial patterns and function of the masticatory muscles in girls and women. → Bull Tokyo Dent Coll. 2002 May;43(2):51–9. |
| 8, 21. | ↑ | Díaz-Serrano KV, Dias TM, Vasconcelos P, Sousa LG, Siéssere S, Regalo S, Palinkas M. Impact of temporomandibular disorders on the stomatognathic system in children. → Med Oral Patol Oral Cir Bucal. 2017 Nov 1;22(6):e723–e729. doi: 10.4317/ medoral.22000. |
| 9, 22. | ↑ | Lucas Bde L, Barbosa Tde S, Pereira LJ, Gavião MB, Castelo PM. Electromyographic evaluation of masticatory muscles at rest and maximal intercuspal positions of the mandible in children with sleep bruxism. → Eur Arch Paediatr Dent. 2014 Aug;15(4):269–74. |
| 10, 23, 24. | ↑ | De Rossi M, De Rossi A, Hallak JE, Vitti M, Regalo SC. Electromyographic evaluation in children having rapid maxillary expansion. → Am J Orthod Dentofacial Orthop. 2009 Sep;136(3):355–60. |
| 11. | ↑ | Andrade AS, Gavião MB, Derossi M, Gameiro GH. Electromyographic activity and thickness of masticatory muscles in children with unilateral posterior crossbite. → Clin Anat. 2009 Mar;22(2):200–6. |
| 12. | ↑ | Ueda HM, Miyamoto K, Saifuddin M, Ishizuka Y, Tanne K. Masticatory muscle activity in children and adults with different facial types. → Am J Orthod Dentofacial Orthop. 2000 Jul;118(1):63–8. |
| 13. | ↑ | Negoro T, Briggs J, Plesh O, Nielsen I, McNeill C, Miller AJ. Bruxing patterns in children compared to intercuspal clenching and chewing as assessed with dental models, electromyography, and incisor jaw tracing: preliminary study. → ASDC J Dent Child. 1998 Nov–Dec;65(6):449–58, 438. |
| 15. | ↑ | Persin LS. Functional characteristics of properly masticatory muscles and temporomandibular joints in children with normal and prognathic bite during the period of substitution of deciduous dentition [master’s thesis]. → [Мoscow]: University of Moscow; 1974. 215 p. |
| 16. | ↑ | Persin LS. Electrophysiological investigations of the muscles in the maxillo-facial area and temporomandibular joints in children with normal and abnormal (prognathic) bites during the period of substitution of deciduous dentition [doctoral thesis]. → [Мoscow]: University of Moscow; 1978. 207 p. |





Leave a Reply
Be the First to Comment!