Extraoral chairside digitalization: Clinical reports on a new digital protocol for surgical and prosthetic treatment of completely edentulous patients
July 6, 2018 / Categories: Digital Dentistry, Implant Dentistry

Tallarico, Marco

Xhanari, Erta

Martinolli, Matteo

Baldoni, Edoardo

Meloni, Silvio Mario
Abstract
Aim
Nowadays, virtual planning and the assisted placement of implants in 3-D positions relative to the bone, soft tissue and final planned prosthesis are becoming the gold standard. In order to obtain such visualization, it is necessary to correctly match the anatomical and prosthetic data. The aim of this paper is to present a new extraoral chairside prosthesis scanning protocol for fully edentulous patients.
Materials and methods
This study was designed as a pilot case series study aimed at evaluating the feasibility of a new extraoral chairside prosthesis scanning protocol for guided implant surgery in completely edentulous arches. This new protocol includes 2 extraoral chairside scans using a powdered intraoral scanner. The first part is based on the extraoral chairside digitalization of the current prosthesis with added radiopaque markers made in flowable composite and subsequent imaging superimposition with DICOM data. The second part is based on the extraoral chairside digitalization of conventional scan abutments fixed on a specially designed customized tray, based on the original virtual planning.
Results
Three patients (1 man and 2 women) with a mean age of 58.9 years were treated. A total of 13 implants were placed using a guided approach. All of the patients underwent 2 extraoral chairside digitalizations with no deviation from the original protocol. No implant failed and the prosthetic survival rate was 100%.
Conclusion
Within the limits of this study, it is suggested that extraoral chairside digitalization may provide better accuracy than conventional methods, permitting fast, easy and accurate treatment at a decreased cost. Randomized controlled trials are needed to evaluate predictability andrepeatability of this workflow.
Keywords
Guided surgery; dental implants; intraoral scanner.
Introduction
Advancements in computerized tomography scanning (cone beam computed tomography [CBCT] technologies), coupled with computer-assisted treatment, have allowed for the virtual planning and assisted placement of implants in 3-D positions relative to the bone, soft tissue and final planned prosthesis.1Tallarico M, Meloni S. Retrospective analysis on survival rate, template-related complications, and prevalence of peri-implantitis of 694 anodized implants placed using computer-guided surgery: results between 1 and 10 years of follow-up. → Int J Oral Maxillofac Implants. 2017 Sep–Oct;32(5):1162–71.2Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial. → Eur J Oral Implantol. 2014 Autumn;7(3):229–42.3Tallarico M, Xhanari E, Cocchi F, Canullo L, Schipani F, Meloni SM. Accuracy of computer-assisted template-based implant placement using a conventional impression and scan model or digital impression: a preliminary report from a randomized controlled trial. → J Oral Science Rehabilitation. 2017 Sep;3(3):8–16.4Katsoulis J, Wälchli J, Kobel S, Gholami H, Mericske-Stern R. Complications with computer-aided designed/computer-assisted manufactured titanium and soldered gold bars for mandibular implant-overdentures: short-term observations. → Clin Implant Dent Relat Res. 2015 Jan;17 Suppl 1:e75–85. doi: 10.1111/ cid.12130.5Rinke S, Ziebolz D. Fabrication of an implant-supported overdenture using CAD/CAM technology: a clinical report. → Quintessence Int. 2013 Feb;44(2):127–34. In order to obtain such visualization, it is necessary to correctly match the anatomical and prosthetic data. The prosthetic information can be acquired in different ways, and it depends on whether the patient is edentulous or still has remaining teeth. With edentulous patients, it is possible to create a scan prosthesis by converting a functionally and esthetically correct prosthesis into a scan prosthesis by placing radiopaque markers such as gutta-percha hemispheres (double-scan protocol).6Van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, Wendelhag I. A computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicenter study. → Clin Implant Dent Relat Res. 2005;7 Suppl 1:S111–20. The double-scan protocol is based on 2 separate sets of DICOM files. It can be used for both partially and completely edentulous patients. The first CBCT scan is of the patient wearing the radiographic guide with the radiopaque markers. The second scan is of the patient’s radiographic guide alone. Converting raw data to 3-D information is done by various software available or by sending the data to the master site of the particular software manufacturers. Noticeable drawbacks of the original double-scan technique are the need for 2 CBCT scans and the associated costs, as well as the technique-sensitive nature of the process. Furthermore, extraoral chairside digitalization allows for easy handling of the controlling factors for the accuracy of impression techniques, compared with intraoral scanning.
In order to overcome these disadvantages, a new digital protocol has been introduced to the profession for the treatment of fully edentulous patients. This newly developed protocol involves 2 parts. The first part (planning) is based on extraoral chairside digitalization of the current prosthesis with added radiopaque markers made in flowable composite and subsequent imaging superimposition with the DICOM data.7Tallarico M, Schiappa D, Schipani F, Cocchi F, Annucci M, Xhanari E. Improved fully digital workflow to rehabilitate an edentulous patient with an implant overdenture in 4 appointments: a case report. → J Oral Science Rehabilitation. 2017 Sep;3(3):38–46. The advantage of this new technique is that the surgical template obtained is derived from the intraoral scan that is more precise than the one obtained from CBCT. The second part (finalization) is based on the extraoral chairside digitalization of conventional scan abutments fixed on a specially designed customized tray, based on the original virtual planning. The purpose of this article is to present this new extraoral chairside prosthesis scanning protocol for fully edentulous patients.
Materials and methods
This study was designed as a pilot case series study aimed at evaluating the feasibility of a new protocol for guided implant surgery of completely edentulous arches that includes 2 extraoral chairside scans using a powdered intraoral scanner (True Definition Scanner, 3M Italia, Pioltello, Italy). Three patients (1 man and 2 women) with a mean age of 58.9 years were treated. Basically, patients with an adequate pre-existing or a newly developed removable complete dental prosthesis in at least one jaw and requiring an implant-supported rehabilitation were considered eligible for this pilot study and consecutively treated in a private center in Rome, Italy. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki of 1964 for biomedical research involving human subjects, as amended in 2008. The patients were duly informed about the nature of the study. Written informed consent to surgical treatment was obtained from each patient.
Extraoral chairside digitalization of the current prosthesis
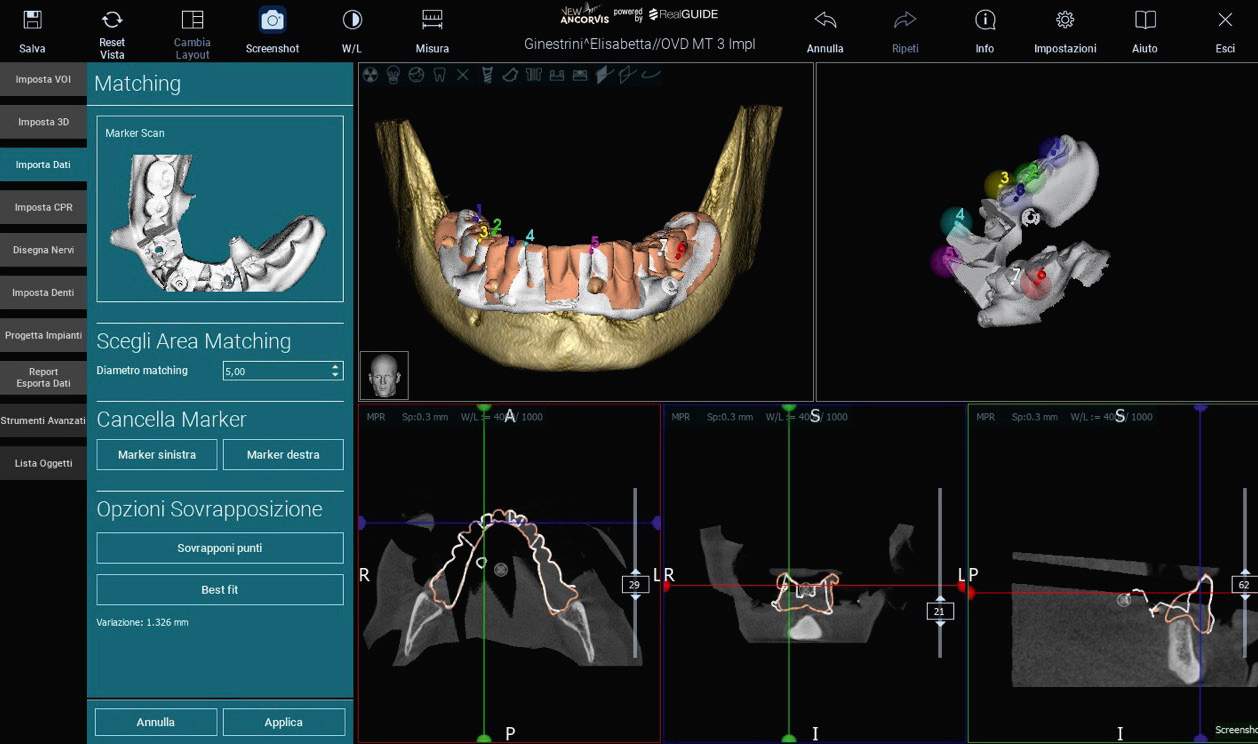
The patient’s medical history was collected, preoperative photographs and radiographs were obtained, and periodontal screening was performed for initial evaluation. During the clinical examination, the existing removable complete dental prosthesis was evaluated for function and esthetics. Then, the fit was carefully assessed, rebasing the existing prosthesis directly chairside if needed (Fig. 1). The prosthetically driven planning workflow started by adding 6–8 drops of flowable composite to the existing prosthesis (Fig. 2). Then, the patient underwent a CBCT scan (CRANEX 3Dx, SOREDEX, Tuusula, Finland) wearing the modified dental prosthesis. A wax bite was used to separate the dental arches (Fig. 3). The second scan was for the extraoral chairside digitalization of the prosthesis with added radiopaque markers (True Definition Scanner). In accordance with the manufacturer’s instructions, the entire area to be scanned was powdered just before scanning (Fig. 4). The STL and DICOM data were imported into a 3-D software planning program (3Diagnosys, Version 5.0, 3DIEMME, Cantù, Italy). The reprocessed surface extrapolated from the DICOM data and the surface of the existing prosthesis generated by the scanning process were merged with the best-fit repositioning tools of the software using the composite radiopaque markers (Fig. 5). Implants (Osstem TSIII, Osstem, Seoul, South Korea) were planned according to the prosthetic setup. After careful functional and esthetic evaluation and final verification, the prosthetically driven plans were approved, and stereolithographic surgical templates were fabricated with a newer rapid prototyping technology (LightSolutions, New Ancorvis, Bargellino, Italy).
-

-
Fig. 1
Pre-existing complete removable denture during intraoral rebasing.
-

-
Fig. 2
Pre-existing complete removable denture with 6–8 drops of radiopaque flowable composite.
-

-
Fig. 3
Pre-existing complete removable denture in the patient’s mouth during CBCT scanning.
-

-
Fig. 4
Powdered pre-existing complete removable denture before extraoral digitalization.
-

-
Fig. 5
Matching of the digitalized pre-existing prosthesis with the CBCT scan.
One hour before implant placement, patients underwent professional oral hygiene and received prophylactic antibiotic therapy (2 g of amoxicillin or 600 mg of clindamycin if allergic to penicillin). A total of 13 implants were placed using a guided approach according to previously published protocols.
Extraoral chairside digitalization of the final implant positions
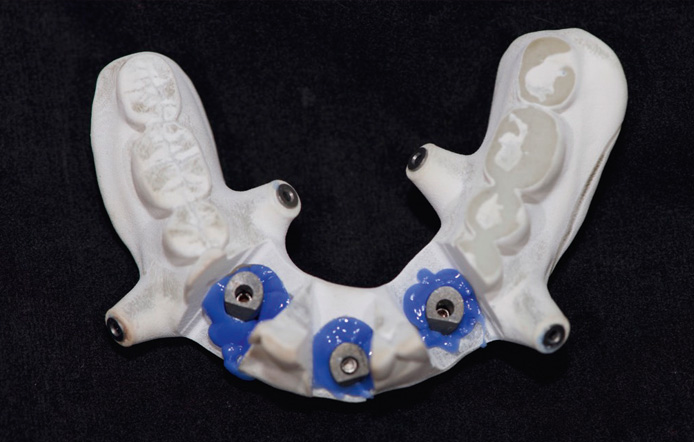
After osseointegration, extraoral chairside digitalization of the final implant positions was performed using dedicated scan abutments (Type AQ, New Ancorvis; Fig. 6) fixed intraorally on a specially designed customized tray based on the approved prosthetic setup (Figs. 7 & 8). In accordance with the manufacturer’s instructions, before scanning (True Definition Scanner), the entire area to be scanned was powdered lightly (Fig. 9). The customized tray was designed maintaining the tooth design, but allowing the screwing on of the scan abutments. The obtained STL files were matched with the previous planning containing all the information about esthetics and function, including occlusal vertical dimension and bite registration in centric relation (Fig. 10).
Definitive restorations were delivered according to the individual treatment plans. Up to 1 year after definitive prosthesis delivery, no implant had failed and the prosthetic survival rate was 100 %.
Discussion
Nowadays, guided surgery is aimed at preparing the implant case and placing implants in the correct prosthetically guided positions. Implant-supported overdentures are an accepted and predictable treatment modality for patients with edentulous jaws.8Rinke S, Ziebolz D. Fabrication of an implant-supported overdenture using CAD/CAM technology: a clinical report. → Quintessence Int. 2013 Feb;44(2):127–34. Clinical studies have documented high survival rates for observation periods of up to 10 years, a high level of patient satisfaction and an improved quality of life compared with conventional dentures.9Slot W, Raghoebar GM, Vissink A, Huddleston Slater JJ, Meijer HJ. A systematic review of implant-supported maxillary overdentures after a mean observation period of at least 1 year. → J Clin Periodontol. 2010 Jan;37(1):98–110.10Cehreli MC, Karasoy D, Kökat AM, Akça K, Eckert S. A systematic review of marginal bone loss around implants retaining or supporting overdentures. → Int J Oral Maxillofac Implants. 2010 Mar–Apr;25(2):266–77.11Emami E, Heydecke G, Rompré PH, de Grandmont P, Feine JS. Impact of implant support for mandibular dentures on satisfaction, oral and general health-related quality of life: a meta-analysis of randomized-controlled trials. → Clin Oral Implants Res. 2009 Jun;20(6):533–44.
-

-
Fig. 6
Scan abutments screwed on to the implants.
-

-
Fig. 7
Specially designed customized tray positioned in the patient’s mouth.
-

-
Fig. 8
Scan abutments fixed to the customized tray.
-
-
Fig. 9
Powdered customized tray before extraoral digitalization.
-
-
Fig. 10
Matching of the digitalized customized tray and the final implant positions with the original plan.
However, it should not be forgotten that the improvement of intraoral scanning techniques and technologies can allow us to make the most of the digital workflow for the finalization of the case and consequently to reduce the number of appointments and costs for the patient. Another advantage is the significant reduction in laboratory time and complexity when compared with more conventional approaches that involve fabrication of the bar patterns with acrylic resin, investment, and casting of dental alloys.12Spyropoulou PE, Razzoog ME, Duff RE, Chronaios D, Saglik B, Tarrazzi DE. Maxillary implant-supported bar overdenture and mandibular implant-retained fixed denture using CAD/CAM technology and 3-D design software: a clinical report. → J Prosthet Dent. 2011 Jun;105(6):356–62. Additionally, because the casting step is eliminated, problems associated with the cost of the alloy, control of the investment expansion, and shrinkage of the alloy are also eliminated.13Abduo J, Lyons K, Bennani V, Waddell N, Swain M. Fit of screw-retained fixed implant frameworks fabricated by different methods: a systematic review. → Int J Prosthodont. 2011 May–Jun;24(3):207–20.14Moeller MS, Duff RE, Razzoog ME. Rehabilitation of malpositioned implants with a CAD/CAM milled implant overdenture: a clinical report. → J Prosthet Dent. 2011 Mar;105(3):143–6.15Spyropoulou PE, Razzoog ME, Duff RE, Chronaios D, Saglik B, Tarrazzi DE. Maxillary implant-supported bar overdenture and mandibular implant-retained fixed denture using CAD/CAM technology and 3-D design software: a clinical report. → J Prosthet Dent. 2011 Jun;105(6):356–62.
After a careful literature review and correctly analyzing the latest technological developments of intraoral scanners, it was decided to modify the double-scan technique proposed by Van Steenberghe et al. that provided for 2 CBCT scans.16Van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, Wendelhag I. A computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicenter study. → Clin Implant Dent Relat Res. 2005;7 Suppl 1:S111–20. In the proposed technique, the second scan results in the extraoral digitalization of the radiographic guide with added 3-D radiopaque markers. The advantage of this new technique is that the surgical template obtained is derived from the intraoral scan that is more precise than the one obtained from CBCT.
Presently, after implant osseointegration, the best way to finalize the case is to take a definitive impression of the implants and to use the temporary prosthesis, if present and functionally and esthetically suitable, to articulate the opposite arch cast to incorporate into the articulator functional information on the provisional (function, vertical dimension, centric relation, esthetics). With the new proposed impression tray, which is derived from the prosthetic setup used for the guided surgery, then already approved by the clinician and the patient, we transfer to the dental technician, with a single appointment, the final implant positions, the centric relation, the vertical dimension, and the esthetic and functional parameters. The limits of this technique are the management of soft tissue, which may require a second scan of the tissue with the scan abutments, always in the same session. The advantage is also that the scan of this new modified tray can be done outside the patient’s mouth, reducing the discomfort for the patient and increasing the accuracy.
Conclusion
Extraoral chairside digitalization may provide better accuracy than conventional methods, permitting fast, easy and accurate treatments at a decreased cost. Randomized controlled trials are needed to evaluate predictability and repeatability of this workflow.
Competing interests
The authors declare that they have no competing interests.

Interview
with Marco Tallarico
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Tallarico M, Meloni S. Retrospective analysis on survival rate, template-related complications, and prevalence of peri-implantitis of 694 anodized implants placed using computer-guided surgery: results between 1 and 10 years of follow-up. → Int J Oral Maxillofac Implants. 2017 Sep–Oct;32(5):1162–71. |
| 2. | ↑ | Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial. → Eur J Oral Implantol. 2014 Autumn;7(3):229–42. |
| 3. | ↑ | Tallarico M, Xhanari E, Cocchi F, Canullo L, Schipani F, Meloni SM. Accuracy of computer-assisted template-based implant placement using a conventional impression and scan model or digital impression: a preliminary report from a randomized controlled trial. → J Oral Science Rehabilitation. 2017 Sep;3(3):8–16. |
| 4. | ↑ | Katsoulis J, Wälchli J, Kobel S, Gholami H, Mericske-Stern R. Complications with computer-aided designed/computer-assisted manufactured titanium and soldered gold bars for mandibular implant-overdentures: short-term observations. → Clin Implant Dent Relat Res. 2015 Jan;17 Suppl 1:e75–85. doi: 10.1111/ cid.12130. |
| 5, 8. | ↑ | Rinke S, Ziebolz D. Fabrication of an implant-supported overdenture using CAD/CAM technology: a clinical report. → Quintessence Int. 2013 Feb;44(2):127–34. |
| 6, 16. | ↑ | Van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, Wendelhag I. A computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicenter study. → Clin Implant Dent Relat Res. 2005;7 Suppl 1:S111–20. |
| 7. | ↑ | Tallarico M, Schiappa D, Schipani F, Cocchi F, Annucci M, Xhanari E. Improved fully digital workflow to rehabilitate an edentulous patient with an implant overdenture in 4 appointments: a case report. → J Oral Science Rehabilitation. 2017 Sep;3(3):38–46. |
| 9. | ↑ | Slot W, Raghoebar GM, Vissink A, Huddleston Slater JJ, Meijer HJ. A systematic review of implant-supported maxillary overdentures after a mean observation period of at least 1 year. → J Clin Periodontol. 2010 Jan;37(1):98–110. |
| 10. | ↑ | Cehreli MC, Karasoy D, Kökat AM, Akça K, Eckert S. A systematic review of marginal bone loss around implants retaining or supporting overdentures. → Int J Oral Maxillofac Implants. 2010 Mar–Apr;25(2):266–77. |
| 11. | ↑ | Emami E, Heydecke G, Rompré PH, de Grandmont P, Feine JS. Impact of implant support for mandibular dentures on satisfaction, oral and general health-related quality of life: a meta-analysis of randomized-controlled trials. → Clin Oral Implants Res. 2009 Jun;20(6):533–44. |
| 12, 15. | ↑ | Spyropoulou PE, Razzoog ME, Duff RE, Chronaios D, Saglik B, Tarrazzi DE. Maxillary implant-supported bar overdenture and mandibular implant-retained fixed denture using CAD/CAM technology and 3-D design software: a clinical report. → J Prosthet Dent. 2011 Jun;105(6):356–62. |
| 13. | ↑ | Abduo J, Lyons K, Bennani V, Waddell N, Swain M. Fit of screw-retained fixed implant frameworks fabricated by different methods: a systematic review. → Int J Prosthodont. 2011 May–Jun;24(3):207–20. |
| 14. | ↑ | Moeller MS, Duff RE, Razzoog ME. Rehabilitation of malpositioned implants with a CAD/CAM milled implant overdenture: a clinical report. → J Prosthet Dent. 2011 Mar;105(3):143–6. |





Leave a Reply
Be the First to Comment!