Gingivoplasty and botulinum toxin application result in improvement of severe gummy smile
January 7, 2020 / Categories: Digital Dentistry, Implant Dentistry

Pedron, Irineu Gregnanin

do Lago Pimentel Maia, Marcelo

Utumi, Estevam Rubens

Ferreira de Medeiros, João Marcelo
Shitsuka, Caleb
Penteado Nucci da Silva, Leopoldo
Abstract
Background
Currently, the search for esthetic excellence has become the main objective in dental treatment. Gummy smile is among patients’ complaints, since this condition may influence their self-esteem and social relationships. The development of new techniques such as the application of botulinum toxin may offer more conservative therapeutic options for the treatment of gummy smile.
Case presentation
A patient with dentogingival discrepancy and severe gummy smile was treated with gingivoplasty and application of botulinum toxin in order to optimize the harmony of the smile. The result was satisfactory regarding the harmony of the smile by combination of the treatments. The use of each of these treatments alone could not have achieved the excellence of the result. Initially, the creation of the new gingival zenith after gingivoplasty promoted the new dental architecture, favoring gingival, dental and facial harmony for the patient. Subsequently, the application of botulinum toxin reduced the gummy smile, by the uniform descent of the upper lip, smoothing the facial lines of the smile, as could be seen in the nasolabial folds, adjacent to the nostrils.
Keywords:
Botulinum toxin type A; gingival overgrowth; gingivectomy; gingivoplasty; gummy smile; surgical crown lengthening.
Introduction
The demand for esthetic procedures has grown exponentially. Dental and medical procedures, besides pursuing the principle of promoting health, seek to achieve smile esthetics.1Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,2Narayan S, Narayan TV, Jacob PC. Correction of gummy smile: a report of two cases. → J Indian Soc Periodontol. 2011 Oct;15(4):421–4.,3Pedron IG, Utumi ER, Silva LP, Moretto LE, Lima TC, Ribeiro MA. Cirurgia Gengival Ressectiva no Tratamento da Desarmonia do Sorriso [Gingival resective surgery to the treatment of disharmony of smile]. → Rev Odontol Bras Central. 2010 Apr;19(48):87–91. Portuguese. Facial esthetic harmony is formed by the union of 3 components: teeth, gingiva and lips.4Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,5Narayan S, Narayan TV, Jacob PC. Correction of gummy smile: a report of two cases. → J Indian Soc Periodontol. 2011 Oct;15(4):421–4.,6Pedron IG, Utumi ER, Silva LP, Moretto LE, Lima TC, Ribeiro MA. Cirurgia Gengival Ressectiva no Tratamento da Desarmonia do Sorriso [Gingival resective surgery to the treatment of disharmony of smile]. → Rev Odontol Bras Central. 2010 Apr;19(48):87–91. Portuguese.,7Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7. The smile becomes esthetically pleasing when these elements are arranged in suitable proportion and gingival exposure is limited to 3 mm. When gingival exposure is larger than 3 mm, it characterizes a nonesthetic condition called gummy smile, which affects some patients psychologically.8Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,9Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51.,10Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,11Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70.
-

- Fig. 1

-

- Fig. 2

-

- Fig. 3

-

- Fig. 4

-

- Fig. 5
-

- Fig. 6
-

- Fig. 7
-

- Fig. 8
-

- Fig. 9
Several therapeutic modalities have been proposed for the correction of gummy smile, among them are gingivoplasty, 12Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,13Narayan S, Narayan TV, Jacob PC. Correction of gummy smile: a report of two cases. → J Indian Soc Periodontol. 2011 Oct;15(4):421–4.,14Pedron IG, Utumi ER, Silva LP, Moretto LE, Lima TC, Ribeiro MA. Cirurgia Gengival Ressectiva no Tratamento da Desarmonia do Sorriso [Gingival resective surgery to the treatment of disharmony of smile]. → Rev Odontol Bras Central. 2010 Apr;19(48):87–91. Portuguese.,15Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,16Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51.,17Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,18Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70. myectomy19Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261. and orthognathic surgery.20Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,21Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70.,22Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33. The last 2 procedures are more invasive and present high morbidity.23Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p. However, the use of botulinum toxin can be considered a therapeutic alternative to the larger surgical procedure, as it is a more conservative and effective, faster and safer method compared with surgical procedures.24Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,25Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51.,26Sucupira E, Abramovitz A. A simplified method for smile enhancement: botulinum toxin injection for gummy smile. → Plast Reconstr Surg. 2012 Sep;130(3):726–8.
Botulinum toxin is synthesized by the anaerobic Gram-positive Clostridium botulinum bacterium and inhibits the release of acetylcholine at the neuromuscular junction, impeding muscular contraction.27Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,28Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,29Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70.,30Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33. There are 7 distinct serotypes of the toxin, and type A is the most frequently used clinically and is a stronger subtype.31Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,32Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261. Botulinum toxin has shown efficiency in the treatment of gummy smile, as well as of other disorders, such as temporomandibular dysfunction (bruxism, clenching and masseteric hypertrophy), sialorrhea, facial palsy and orofacial pain.33Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,34Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,35Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51.,36Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,37Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70.,38Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33.,39Sucupira E, Abramovitz A. A simplified method for smile enhancement: botulinum toxin injection for gummy smile. → Plast Reconstr Surg. 2012 Sep;130(3):726–8.,40Niamtu J 3rd. Botox injections for gummy smiles. → Am J Orthod Dentofacial Orthop. 2008 Jun;133(6):782–3; author reply 783–4. The purpose of this article is to report a case of a patient who presented with severe gummy smile and was treated by a combination of gingivoplasty and botulinum toxin.
Case report
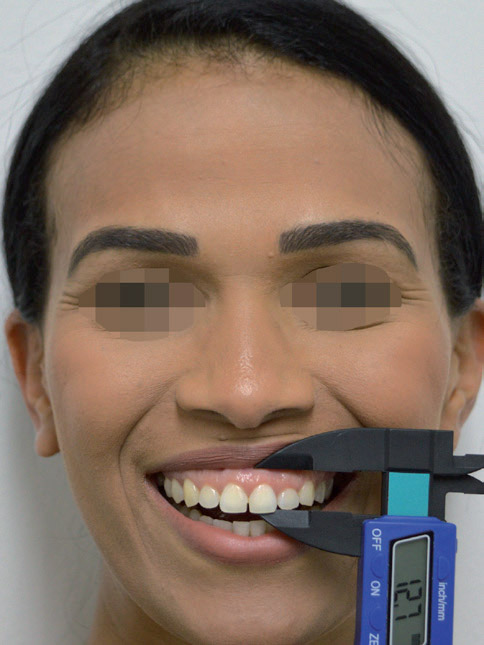
A 36-year-old female patient attended the clinic complaining of gummy smile (Fig. 1). Clinically, the patient presented with an anatomic discrepancy of more than 4 mm between the length of the maxillary teeth (Figs. 2 & 3) and severe gummy smile. Initially, the length of tooth #21 was used as a clinical parameter and was measured as 8.8 mm (Fig. 4). The gummy smile was measured as 12.7 mm in height (Fig. 5).
Systemic alterations were not reported. Gingivoplasty was suggested. However, the application of botulinum toxin was proposed to complement the result of gingivoplasty, and the patient was counseled about the recurrence of gummy smile 6 months after the application. The patient agreed to the proposed treatment and signed the terms of consent for the application of botulinum toxin and use of images.
Under local infiltrative anesthesia, gingivoplasty was performed by determination of the bleeding points with the aid of a millimeter probe and the union of these points with an electric scalpel.41Narayan S, Narayan TV, Jacob PC. Correction of gummy smile: a report of two cases. → J Indian Soc Periodontol. 2011 Oct;15(4):421–4. The length of the teeth was increased, characterizing the gingival zenith. Posteriorly, scraping was performed, resembling the external bevel technique, with the purpose of increasing the tissue reparation (Figs. 6 & 7). There was no need for surgical cement, given that the wound repair process occurs by secondary intention. The patient was instructed on care and analgesics were administered postoperatively.
After 30 days, satisfactory tissue reparation was observed (Fig. 8) and the patient reported no changes or complaints. With use of Chu’s proportion gauge (Hu-Friedy), the improvement of the relation between the length and width of the teeth after the gingivoplasty was observed (Fig. 9). However, the persistence of the gummy smile was observed too (Fig. 10). The length of tooth #21 had been increased from 8.8 mm to 9.7 mm (Fig. 11). The gummy smile had increased because of the higher dynamics of the upper lip, despite gingivoplasty (Fig. 12).
-

- Fig. 10
-

- Fig. 11
-

- Fig. 12
-

- Fig. 13
In the same treatment session, botulinum toxin was applied. Prior to application, the surface of the skin was disinfected with ethanol to avoid local infection and remove the skin oiliness. Posteriorly, local anesthetic (EMLA, Astra) was applied with the purpose of promoting comfort during the procedure. Botulinum toxin type A (Botox 200 units, Allergan Pharmaceuticals) was diluted in 2 ml of saline solution, according to the manufacturer’s instructions, and 2 units were injected at the recommended site, laterally to each nostril, at the level of the nose wing, at the insertion of the levator labii superioris alaeque nasi muscle. After application, the patient was advised not to lower her head or engage in physical activity during the first 4 h after the procedure. After 15 days, the patient was evaluated. She presented with uniform descent of the upper lip (Fig. 13) and reported no side effects or complaints. The clinical effect of botulinum toxin application remained for 6 months.
Discussion
Several etiologies of gummy smile have been suggested, such as vertical excess of the maxilla,42Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,43Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,44Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51.,45Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,46Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70.,47Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33. delayed passive eruption,48Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,49Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,50Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,51Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70. hyperfunction of the muscles involved in smiling52Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,53Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,54Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33. and reduced length of the clinical crowns.55Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,56Narayan S, Narayan TV, Jacob PC. Correction of gummy smile: a report of two cases. → J Indian Soc Periodontol. 2011 Oct;15(4):421–4.,57Pedron IG, Utumi ER, Silva LP, Moretto LE, Lima TC, Ribeiro MA. Cirurgia Gengival Ressectiva no Tratamento da Desarmonia do Sorriso [Gingival resective surgery to the treatment of disharmony of smile]. → Rev Odontol Bras Central. 2010 Apr;19(48):87–91. Portuguese. These etiologies may occur singly or in combination and determine the type of treatment to be applied. In gummy smile caused by muscular hyperfunction, botulinum toxin is indicated. It is the treatment of choice owing to its facility and security of application, besides being a more conservative approach compared with surgical procedures (myectomy or LeFort I osteotomy).58Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,59Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,60Niamtu J 3rd. Botox injections for gummy smiles. → Am J Orthod Dentofacial Orthop. 2008 Jun;133(6):782–3; author reply 783–4.
Smiling is performed by several facial muscles, such as the levator labii superioris, the levator labii superioris alaeque nasi, and the zygomaticus major and minor.61Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,62Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,63Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51.,64Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,65Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70.,66Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33.,67Sucupira E, Abramovitz A. A simplified method for smile enhancement: botulinum toxin injection for gummy smile. → Plast Reconstr Surg. 2012 Sep;130(3):726–8. The fibers of these muscles converge at the same area, forming a triangle, making it possible to include the 3 muscles in a single injection. The proposed site of the injection was lateral to the nose wing.68Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,69Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,70Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70.,71Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33.,72Sucupira E, Abramovitz A. A simplified method for smile enhancement: botulinum toxin injection for gummy smile. → Plast Reconstr Surg. 2012 Sep;130(3):726–8. The toxin, when injected, can spread over an area of 20 mm, allowing effective extension.73Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,74Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,75Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51. The toxin decreases the contraction of the muscles responsible for the elevation of the upper lip, reducing gingival exposure.76Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,77Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51.,78Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,79Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70.,80Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33.,81Sucupira E, Abramovitz A. A simplified method for smile enhancement: botulinum toxin injection for gummy smile. → Plast Reconstr Surg. 2012 Sep;130(3):726–8.
Botulinum toxin is a hydrophilic powder, stored under vacuum, sterile and stable.82Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,83Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,84Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70. Reconstitution is by effortless injection of the diluent (0.9% sodium chloride) into the bottle. It has to be stored at 2–8°C and used within 4–8 h in order to guarantee its effectiveness.85Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,86Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33. Clinical effects present 2–10 days after the injection, and the maximum visible effect occurs after 14 days of injection.87Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,88Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7.,89Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261. This effect lasts for approximately 3–6 months.90Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,91Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51.,92Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261.,93Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33. Contraindications to the use of botulinum toxin include pregnancy and lactation, neurodegenerative and autoimmune diseases, and concurrent use of an aminoglycoside antibiotic that would enhance the action of the toxin.94Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p.,95Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33.
In this report, the result was satisfactory regarding the harmony of the smile by combination of the treatments— gingivoplasty and application of botulinum toxin. Each of these treatments in isolation could not have achieved the same level of excellence. Initially, the creation of the new gingival zenith after gingivoplasty promoted the new dental architecture, favoring gingival, dental and facial harmony for the patient. Subsequently, the application of botulinum toxin reduced the gummy smile, by the uniform descent of the upper lip, smoothing the facial lines of the smile, as can be seen in the nasolabial folds, adjacent to the nostrils, by comparing Figures 1 & 13.
Competing interests
The authors declare that they have no competing interests.
Figure legends
Fig. 1 – Severe gingival exposure, indicating gummy smile.
Fig. 2 – Discrepancy between the lengths of the maxillary teeth.
Fig. 3 – Length of tooth #11 measured with Chu’s proportion gauge.
Fig. 4 – Length of tooth #21 measured with a digital pachymeter (8.8 mm).
Fig. 5 – Gummy smile measured with a digital pachymeter (12.7 mm).
Fig. 6 – Immediate postoperative photograph of teeth #21, 22 and 23.
Fig. 7 – Immediate postoperative photograph after gingivoplasty.
Fig. 8 – Thirty days after gingivoplasty.
Fig. 9 – Improvement of the relation between the length and the width of the teeth after gingivoplasty.
Fig. 10 – Persistence of the gummy smile after gingivoplasty.
Fig. 11 – Increase of the length of tooth #21.
Fig. 12 – Reduction of the gummy smile by the gingivoplasty.
Fig. 13 – Result 15 days after botulinum toxin application.
References
| 1, 4, 8, 12, 23, 24, 27, 31, 33, 42, 48, 52, 55, 58, 61, 68, 73, 82, 85, 87, 90, 94. | ↑ | Pedron IG. Toxina botulínica: aplicações em odontologia. → Florianópolis: Editora Ponto. 2016. 195 p. |
| 2, 5, 13, 41, 56. | ↑ | Narayan S, Narayan TV, Jacob PC. Correction of gummy smile: a report of two cases. → J Indian Soc Periodontol. 2011 Oct;15(4):421–4. |
| 3, 6, 14, 57. | ↑ | Pedron IG, Utumi ER, Silva LP, Moretto LE, Lima TC, Ribeiro MA. Cirurgia Gengival Ressectiva no Tratamento da Desarmonia do Sorriso [Gingival resective surgery to the treatment of disharmony of smile]. → Rev Odontol Bras Central. 2010 Apr;19(48):87–91. Portuguese. |
| 7, 15, 34, 43, 49, 59, 62, 69, 74, 76, 88. | ↑ | Hwang WS, Hur MS, Hu KS, Song WC, Koh KS, Baik HS, Kim ST, Kim HJ, Lee KJ. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. → Angle Orthod. 2009 Jan;79(1):70–7. |
| 9, 16, 25, 35, 44, 63, 75, 77, 91. | ↑ | Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. → J Am Acad Dermatol. 2010 Dec;63(6):1042–51. |
| 10, 17, 19, 20, 28, 32, 36, 45, 50, 53, 64, 78, 83, 89, 92. | ↑ | Polo M. Botulinum toxin type A in the treatment of excessive gingival display. → Am J Orthod Dentofacial Orthop. 2005 Feb;127(2):214–8; quiz 261. |
| 11, 18, 21, 29, 37, 46, 51, 65, 70, 79, 84. | ↑ | Indra AS, Biswas PP, Vineet VT, Yeshaswini T. Botox as an adjunct to orthognathic surgery for a case of severe vertical maxillary excess. → J Maxillofac Oral Surg. 2011 Sep;10(3):266–70. |
| 22, 30, 38, 47, 54, 66, 71, 80, 86, 93, 95. | ↑ | Jaspers GW, Pijpe J, Jansma J. The use of botulinum toxin type A in cosmetic facial procedures. → Int J Oral Maxillofac Surg. 2011 Feb;40(2):127–33. |
| 26, 39, 67, 72, 81. | ↑ | Sucupira E, Abramovitz A. A simplified method for smile enhancement: botulinum toxin injection for gummy smile. → Plast Reconstr Surg. 2012 Sep;130(3):726–8. |
| 40, 60. | ↑ | Niamtu J 3rd. Botox injections for gummy smiles. → Am J Orthod Dentofacial Orthop. 2008 Jun;133(6):782–3; author reply 783–4. |





Leave a Reply
Be the First to Comment!