Guided bone regeneration around 1-stage nonsubmerged dental implants with periimplant bone defects: A retrospective case series study
July 6, 2018 / Categories: Digital Dentistry, Implant Dentistry

Aloy Prosper, Amparo

Peñarrocha Oltra, David

Pellicer Chover, Hilario

Peñarrocha Diago, Miguel

Peñarrocha Diago, Maria
Abstract
Objective
The aim was to evaluate the 3-year outcome of nonsubmerged dental implants with buccal periimplant defects treated with a guided bone regeneration technique in a 1-stage approach.
Method and materials
A retrospective chart review of consecutive patients treated with dental implants and bone regeneration at the time of implant placement, left nonsubmerged, and with a minimum follow-up of 3 years after implant loading was performed. Patients were treated between January 2005 and December 2009 at the Oral Surgery Unit of the University of Valencia, Valencia, Spain. The following variables were assessed: complications with the healing procedure, implant success (based on Buser et al.1Buser D, Mericske-Stern R, Dula K, Lang NP. Clinical experience with one-stage, non-submerged dental implants. → Adv Dent Res. 1999 Jun;13:153–61.), and periimplant marginal bone loss. Statistical analysis was performed applying Chi2 test, Spearman’s test and the Mann-Whitney test, using alpha set at 0.05.
Results
A total of 50 patients (26 women, 24 men) with a mean age of 54.8 ± 13.6 years (range: 25–79) and 75 implants were included. Seventy-one dehiscences (average height: 1.97 ± 1.06 mm) and 4 fenestrations (average height: 2.75 ± 0.95 mm) were treated. Five membrane exposures were recorded (10%). After 3 years post-loading, the implant success rate was 94% and mean marginal bone loss was 0.50 ± 0.27 mm.
Conclusion
Despite the limitations of this study, a nonsubmerged approach in connection with guided bone regeneration to treat periimplant bone defects is a feasible option with few healing complications and a good prognosis.
Keywords
Guided bone regeneration; periimplant defects; dental implants; marginal bone loss; success rate; nonsubmerged.
Introduction
The application of guided bone regeneration (GBR) provides clinicians with the ability to place implants in areas of insufficient amounts of bone.2Benić GI, Jung RE, Siegenthaler DW, Hammerle CH. Clinical and radiographic comparison of implants in regenerated or native bone: 5-year results. → Clin Oral Implants Res. 2009 May;20(5):507–13. The 1-stage approach, using grafting material with or without membranes at the time of implant placement, has the advantage of shortening the total treatment time.3Hammerle CH, Jung RE. Bone augmentation by means of barrier membranes. → Periodontology 2000. 2003 Oct;33:36–53. GBR utilizing a 1-stage procedure around submerged implants has been widely documented in humans4Benić GI, Jung RE, Siegenthaler DW, Hammerle CH. Clinical and radiographic comparison of implants in regenerated or native bone: 5-year results. → Clin Oral Implants Res. 2009 May;20(5):507–13.5Lorenzoni M, Pertl C, Polansky RA, Jakse N, Wegscheider WA. Evaluation of implants placed with barrier membranes. A retrospective follow-up study up to five years. → Clin Oral Implants Res. 2002 Jun;13(3):274–80.6Zitzmann NU, Scharer P, Marinello CP. Long-term results of implants treated with guided bone regeneration: a 5-year prospective study. → Int J Oral Maxillofac Implants. 2001 May–Jun;16(3):355–66. and animals.7Hammerle CH, Bragger U, Schmid B, Lang NP. Successful bone formation at immediate transmucosal implants: a clinical report. → Int J Oral Maxillofac Implants. 1998 Jul–Aug;13(4):522–30.8Hurzeler MB, Kohal RJ, Naghshbandi J, Mota LF, Conradt J, Hutmacher D, Caffesse RG. Evaluation of a new bioresorbable barrier to facilitate guided bone regeneration around exposed implant threads. An experimental study in the monkey. → Int J Oral Maxillofac Surg. 1998 Aug;27(4):315–20.9Carmagnola D, Berglundh T, Araujo M, Albrektsson T, Lindhe J. Bone healing around implants placed in a jaw defect augmented with Bio-Oss. An experimental study in dogs. → J Clin Periodontol. 2000 Nov;27(11):799–805. Several experimental studies in animals on nonsubmerged immediate implants placed in extraction sockets with GBR indicated that bone regeneration around these implants was possible;10Brunel G, Benque E, Elharar F, Sansac C, Duffort JF, Barthet P, Baysse E, Miller N. Guided bone regeneration for immediate non-submerged implant placement using bioabsorbable materials in Beagle dogs. → Clin Oral Implants Res. 1998 Oct;9(5):303–12.11Kohal RJ, Trejo PM, Wirsching C, Hurzeler MB, Caffesse RG. Comparison of bioabsorbable and bioinert membranes for guided bone regeneration around non-submerged implants. An experimental study in the mongrel dog. → Clin Oral Implants Res. 1999 Jun;10(3):226–37.12Fiorellini JP, Engebretson SP, Donath K, Weber HP. Guided bone regeneration utilizing expanded polytetrafluoroethylene membranes in combination with submerged and nonsubmerged dental implants in beagle dogs. → J Periodontol. 1998 May;69(5):528–35. and clinical studies on humans confirmed these results with good long-term outcomes.13Siciliano VI, Salvi GE, Matarasso S, Cafiero C, Blasi A, Lang NP. Soft tissues healing at immediate transmucosal implants placed into molar extraction sites with buccal self-contained dehiscences. A 12-month controlled clinical trial. → Clin Oral Implants Res. 2009 May;20(5):482–8.14Cordaro L, Torsello F, Roccuzzo M. Clinical outcome of submerged vs. non-submerged implants placed in fresh extraction sockets. → Clin Oral Implants Res. 2009 Dec;20(12):1307–13.
Defects from fresh extraction sockets are characterized by the maintenance of intact surrounding bone walls, which offer favorable conditions for regenerative processes. However, when dental implants are placed in narrow ridges, the lack of 1 or more walls leads to open defects, which are less favorable for the regenerative process, since the blood clot is less protected, grafted bone particles are more subject to displacement, and a membrane placed to cover the defect may collapse. 15Vanden Bogaerde L. A proposal for the classification of bony defects adjacent to dental implants. → Int J Periodontics Restorative Dent. 2004 Jun;24(3):264–71. Despite the 1-stage approach having the advantage of shortening the total treatment time, different systematic reviews on clinical outcomes of GBR procedures to correct periimplant dehiscences and fenestrations show that in most of the included studies dental implants were left submerged. There are few studies on GBR around nonsubmerged implants for treating periimplant bone defects in narrow alveolar ridges.16De Boever AL, De Boever JA. Guided bone regeneration around non-submerged implants in narrow alveolar ridges: a prospective long-term clinical study. → Clin Oral Implants Res. 2005 Oct;16(5):549–56.17Christensen DK, Karoussis IK, Joss A, Hammerle CH, Lang NP. Simultaneous or staged installation with guided bone augmentation of transmucosal titanium implants. A 3-year prospective cohort study. → Clin Oral Implants Res. 2003 Dec;14(6):680–6.18Nevins M, Mellonig JT, Clem DS 3rd, Reiser GM, Buser DA. Implants in regenerated bone: long-term survival. → Int J Periodontics Restorative Dent. 1998 Feb;18(1):34–45.19Juodzbalys G, Raustia AM, Kubilius R. A 5-year follow-up study on one-stage implants inserted concomitantly with localized alveolar ridge augmentation. → J Oral Rehabil. 2007 Oct;34(10):781–9.20De Boever AL, De Boever JA. A one-stage approach for nonsubmerged implants using a xenograft in narrow ridges: a report of seven cases. → Int J Periodontics Restorative Dent. 2003 Apr;23(2):169–75.21Cochran DL, Douglas HB. Augmentation of osseous tissue around nonsubmerged endosseous dental implants. → Int J Periodontics Restorative Dent. 1993 Dec;13(6):506–19. The purpose of the present study was to evaluate the 3-year outcome of 1-stage nonsubmerged dental implants with buccal periimplant defects treated with a GBR technique and resorbable membranes.
Materials and methods
Patient selection
A retrospective clinical study was conducted of patients with a minimum of 1 dental implant demonstrating a dehiscence or fenestration bony defect with an exposed implant surface during implant placement and thus undergoing simultaneous particulate bone grafting with resorbable membranes and left nonsubmerged. Patients were treated between January 2005 and December 2009 at the Oral Surgery Unit of the University of Valencia, Valencia, Spain, and were monitored annually for a minimum of 3 years post-loading. The study was performed following the guidelines of the Declaration of Helsinki for human research. Surgical procedures were performed by the same surgeon with extensive experience in regenerative procedures. Patients were given full information about the surgical procedures and duly signed informed consent forms. Preoperative analysis included registering complete medical histories and performing clinical and radiographic examinations.
Subject and site inclusion criteria:
- Dental implant with a dehiscence or fenestration bony defect during implant placement treated with particulate bone graft and resorbable membranes.
- Nonsubmerged dental implants.
- Tooth/teeth at implant site extracted > 6 months previously.
- Rehabilitation with a fixed or removable implant-supported prosthesis.
- Age > 18 years.
- No relevant medical conditions.
- Nonsmoking or smoking ≤ 20 cigarettes/day (all pipe or cigar smokers were excluded).
- Follow-up for at least three years after prosthetic loading.
Subject and site exclusion criteria:
- Patients with systemic or local conditions contraindicating implant therapy (previous chemotherapy, previous irradiation of the head and neck region, active progressive periodontitis and/or immunosuppression).
- Pregnant or lactating patients.
- Sites with acute infection.
- Poor oral hygiene.
- Implants with sinus augmentation.
- Immediate implants or placed in bone with a recent extraction (< 6 months).
- Reimplantation. –– Implants placed in bone previously regenerated with bone grafting.
- Patients failing to attend follow-up visits. The present study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement.22Kuller LH, Goldstein BD. Suggestions for STROBE recommendations. → Epidemiology. 2007 Nov;18(6):792–3.
-

-
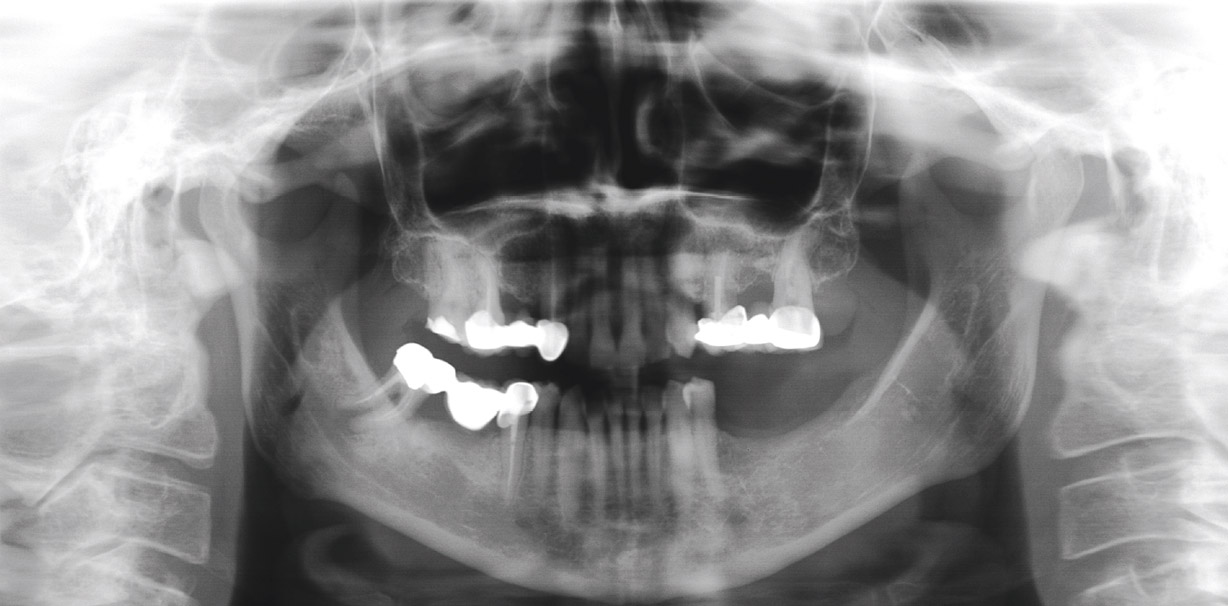
Fig. 1A
Preoperative panoramic radiograph.
-
-
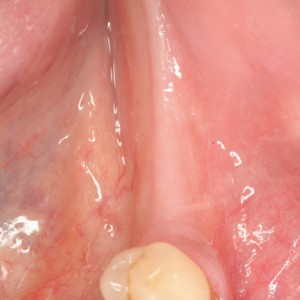
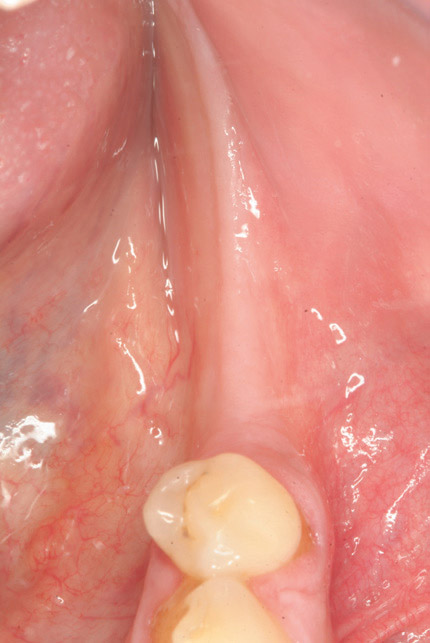
Fig. 1B
Preoperative occlusal view.
-
-
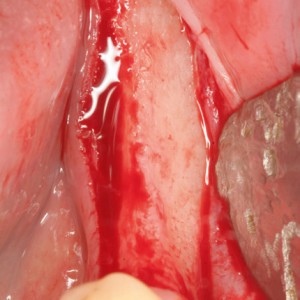
Fig. 1C
Bone atrophy of the alveolar ridge visualized after flap elevation.

-

-
Fig. 1D
Implant insertion in positions #35, 36 and 37.

-

-
Fig. 1E
Synthetic bone over dehiscences.

-

-
Fig. 1F
Resorbable membrane over bone graft.

Preoperative evaluation
Thorough medical histories, clinical examinations and panoramic radiographs were performed in all cases. Cone-beam computed tomographic scans were obtained to assess the availability of bone whenever the surgeon considered this necessary. Periodontal treatment was provided whenever necessary to control inflammation prior to implant placement surgery. Within 10 days of the implant placement surgery, a full-mouth professional prophylaxis appointment was scheduled.
Surgical procedures
All procedures were performed under local anesthesia using 4% articaine with 1:100,000 epinephrine (Inibsa, Lliçà de Vall, Spain) and intravenous conscious sedation with a 1% propofol solution, administered by an anesthesiologist. An initial incision was made slightly palatal/lingual of the alveolar crest. One or 2 releasing incisions were made and a mucoperiosteal flap was raised. The exposed alveolar bone was curetted to remove all soft tissue. In order to enhance primary stability, drills and osteotomes were combined to prepare implant beds. TSA implants with the Avantblast surface (Phibo Dental Solutions, Sentmenat, Spain) were inserted using standard procedures following the manufacturer’s guidelines. These implants had a polished surface portion of 1.5 mm. All implants were placed with adequate primary stability (≥ 35 N cm). All implants were treated by guided bone regeneration with autologous bone grafts harvested from the conformation of implant beds during drilling and adjusted to the bone contour, or a mix with synthetic bone of 0.25–1 mm of particle (Kera–Os, Keramat, Coruña, Spain) when the autologous bone obtained was insufficient to cover the periimplant defects. Grafted bone was protected with a textured collagen membrane (Lyopstic, B-Braun, Aesculap, Tuttlingen, Germany). Periosteal incisions were made to allow flap mobilization and tension-free primary wound closure. Afterward, the mucoperiosteal flap was resutured, leaving the implant head exposed to the oral cavity (Fig. 1). No provisional restorations were loaded on the implants. Patients were prescribed 1 g of amoxicillin (GlaxoSmithKline, Madrid, Spain) twice daily for 6 days, starting 1 h prior to surgery,23Esposito M, Grusovin MG, Loli V, Coulthard P, Worthington HV. Does antibiotic prophylaxis at implant placement decrease early implant failures? A Cochrane systematic review. → Eur J Oral Implantol. 2010 Summer;3(2):101–10. 600 mg of ibuprofen (Bexistar, Laboratorio Bacino, Barcelona, Spain) 3 times per day for 5 days and a mouthrinse containing 0.12% chlorhexidine (GUM, John O. Butler/Sunstar, Chicago, Ill., U.S.) twice daily, commencing 3 days prior to surgery and for 2 weeks thereafter. Patients were instructed in adequate hygiene maintenance. Patients were not allowed to use removable prostheses for 3 weeks after bone grafting surgeries. A soft diet was recommended for 1 week, and patients were instructed to avoid brushing or any other trauma to the surgical sites. Sutures were removed 2 weeks after surgery.
-

-
Fig. 1G
Sutures.

-

-
Fig. 1H
Healed soft tissue.

-

-
Fig. 1I
Occlusal view of prosthesis placement.

-

-
Fig. 1J
Lateral view of prosthesis placement.

-

-
Fig. 1K
One-year post-loading panoramic radiograph.
-

-
Fig. 1L
Three-year post-loading panoramic radiograph.
Data collection and follow-up
All data collection was carried out by a single trained clinician different from the surgeon or the prosthodontist following a pre-established protocol. All patients were included in a maintenance program involving annual examinations and professional prophylaxis. Occlusal adjustment was performed when necessary.
Patient age (at implant placement), sex, hygiene and smoking habits (none/< 10 cigarettes per day/10–20 cigarettes per day) were registered. For each implant, the position, and the type and dimensions of defects (dehiscence/ fenestration) were registered. Defects were measured using a millimetric periodontal probe (UNC, Hu-Friedy, Chicago, Ill., U.S.) placed parallel or perpendicular to the long axis of the implant. Measurements were recorded to the nearest 1 mm mark. The type of graft was recorded (autologous bone or mixed). The definitive prosthesis design (single or partial) and type of prosthesis (cemented or screwed) were recorded. The following outcome measures were recorded:
Receptor site healing: Membrane exposure. Implant success: The definition of implant success was based on the clinical and radiographic criteria put forward by Buser et al.24Buser D, Mericske-Stern R, Dula K, Lang NP. Clinical experience with one-stage, non-submerged dental implants. → Adv Dent Res. 1999 Jun;13:153–61. The implant success rate was provided per patient. Radiographic periimplant marginal bone loss: Intraoral radiographs were taken at the moment of prosthetic loading (baseline), 1 year post-loading and 3 years post-loading (control radiographs), using the X-Mind intraoral system (Satelec-Pierre Rolland Group, Merignac, France) and an RVG intraoral digital receptor (Dürr Dental, Bietigheim-Bissingen, Germany) with the aid of a Rinn XCP film holder (Dentsply Rinn, Elgin, Ill., U.S.) to achieve parallelism. The images were calibrated with CliniView (Version 5.1, Instrumentarium Imaging, Tuusula, Finland). Each image was calibrated using the known length of the implants. The vertical distance from the outer edge of the implant shoulder (reference point) to the most coronal point of bone-to-implant contact was evaluated at the mesial and distal aspects of each implant to the nearest 0.1 mm. Periimplant marginal bone resorption at 3 years post-loading was calculated from the change in bone level between the 1-year post-loading and the 3-year control radiographs; for each pair of measurements (mesial and distal), the largest value was used. Intraexaminer calibration was analyzed before evaluating the entire implant sample by reassessing bone loss at a total of 30 randomly selected sites (using the random function of Microsoft Excel 2010) on duplicate measurements performed on different days. An intraclass correlation coefficient of 0.898 was obtained, showing a high concordance between the 2 sets of data. According to Dahlberg’s d value, a 0.049 mm error was estimated for the measurement method.
Statistical analysis
Statistical analysis was performed using nonparametric tests for implant success, as this was a noncontinuous variable, and marginal bone loss, as this had an asymmetric distribution. The chi-square test was used to study the relationship between the survival and success rates with respect to sex, smoking and hygiene habits, position and location of the implants, type defect, type of graft, prosthesis design and membrane exposure. Spearman’s test was used to relate the mean of bone loss and age and mean periimplant defect dimensions; and the Mann-Whitney test to relate this variable with type of graft and exposure membrane. Statistical analysis was performed using SPSS software (Version 17.0, SPSS, Chicago, Ill., U.S.).
Results
A total of 66 patients with GBR around nonsubmerged dental implants performed owing to the presence of dehiscences and fenestrations were included. Sixteen patients were excluded as a result of failing to attend control visits. The final study sample was 50 patients (26 women, 24 men) with a mean age of 54.8 ± 13.6 years (range: 25–79). Hygiene maintenance was good in 39 patients and regular in 11. Thirty-eight patients were nonsmokers, 9 smoked < 10 cigarettes per day and 3 between 10 and 20 cigarettes.
A total of 75 dental implants were placed: 28 maxillary (9 anterior, 19 posterior) and 47 mandibular (10 anterior, 37 posterior). Seventy-seven defects around 75 implants were produced (73 dehiscences, 4 fenestrations). The mean dimensions of the resulting dehiscence defects were 1.97 ± 1.06 mm (range: 1.5–8.0) in height and 3.29 mm (range: 3.0–5.5) in width. The mean dimensions of the resulting fenestration defects were 2.75 ± 0.95 mm (range: 2.0–4.0) in height and 2.1 mm (range: 1.5–3.0) in width. Regarding the type of graft, 12 implants received autologous bone and 63 a mix with synthetic bone. With regard to prosthetic rehabilitation, 21 implants had single crowns and 54 fixed bridges, and 28 prostheses were cemented and 47 screwed.
Receptor site healing
Wound dehiscence with membrane exposure during the early postoperative period occurred in 5 grafted sites in 5 patients. These exposures did not exceed 3 mm in diameter. In these cases, 0.2% chlorhexidine gel was prescribed for application 3 times daily to the exposed membrane for 6 weeks after surgery. All sites re-epithelialized uneventfully.
Implant success rate, and periimplant marginal bone loss
Three implants in 3 patients were lost, all of them before loading, between 1 and 3 months. All 3 implants had periimplant bone dehiscences of 2 mm in width and length. Two patients were men with an average age of 40–63 years and 1 a woman of 46 years. All these patients maintained regular oral hygiene. One was a nonsmoker and 2 were smokers. All failed implants had been placed in posterior sites (2 mandibular and 1 maxillary) and did not exceed 10.0 mm in length and 4.2 mm in width.
Implant success rate per patient was 94% after 1 year post-loading. Mean periimplant marginal bone loss at 1 year post-loading was 0.42 ± 0.31 mm (range: 0.1–1.9). At 3 years post-loading, no further implants had been lost and were considered successful according to Buser et al.’s criteria.25Buser D, Mericske-Stern R, Dula K, Lang NP. Clinical experience with one-stage, non-submerged dental implants. → Adv Dent Res. 1999 Jun;13:153–61. Mean periimplant marginal bone loss at 3 years post-loading was 0.50 ± 0.27 mm (range: 0.2–1.8).
No significant differences were found between success rate and bone loss regarding patient factors (age, sex and smoking habit) or implant variables (location, type defect, defect dimensions, type of graft, prostheses design or membrane exposure). However, all implant failures occurred in patients with regular oral hygiene (100%); these results showed a moderate tendency to significance, but were nevertheless nonsignificant (P value: 0.073).
Discussion
This study was designed to evaluate, after a minimum of 3 years of prosthetic loading, the survival and success rates of nonsubmerged implants with periimplant bone defects treated with particulate bone grafts and resorbable membranes in a 1-stage approach. The results of this study show that a nonsubmerged approach is a feasible option when periimplant bone defects are produced during implant surgery owing to anatomical reasons.
The outcomes of the present study are comparable with those of studies on submerged implants.26Benić GI, Jung RE, Siegenthaler DW, Hammerle CH. Clinical and radiographic comparison of implants in regenerated or native bone: 5-year results. → Clin Oral Implants Res. 2009 May;20(5):507–13.27Zitzmann NU, Scharer P, Marinello CP. Long-term results of implants treated with guided bone regeneration: a 5-year prospective study. → Int J Oral Maxillofac Implants. 2001 May–Jun;16(3):355–66.28Blanco J, Alonso A, Sanz M. Long-term results and survival rate of implants treated with guided bone regeneration: a 5-year case series prospective study. → Clin Oral Implants Res. 2005 Jun;16(3):294–301.29Hammerle CH, Jung RE, Feloutzis A. A systematic review of the survival of implants in bone sites augmented with barrier membranes (guided bone regeneration) in partially edentulous patients. → J Clin Periodontol. 2002;29 Suppl 3:226–31; discussion 232–3. In a recent systematic review, Chiapasco and Zaniboni reported that the overall survival rate of implants with periimplant defects treated with GBR, irrespective of the timing of the implants, the type of membrane and grafting materials, was 95.7% (range: 84.7–100) within the observation period, varying from 1 to 9 years.30Chiapasco M, Zaniboni M. Clinical outcomes of GBR procedures to correct peri-implant dehiscences and fenestrations: a systematic review. → Clin Oral Implants Res. 2009 Sep;20 Suppl 4:113–23. In only 1 out of 7 studies included in the review had nonsubmerged implants been placed.31De Boever AL, De Boever JA. Guided bone regeneration around non-submerged implants in narrow alveolar ridges: a prospective long-term clinical study. → Clin Oral Implants Res. 2005 Oct;16(5):549–56. De Boever and De Boever studied long-term outcomes of nonsubmerged implants placed with a xenograft and a nonresorbable membrane to cover large dehiscences in a 1-stage approach and reported a 93.75% survival rate and stable marginal bone loss after a 5-year follow-up.32De Boever AL, De Boever JA. Guided bone regeneration around non-submerged implants in narrow alveolar ridges: a prospective long-term clinical study. → Clin Oral Implants Res. 2005 Oct;16(5):549–56. Nonresorbable membranes are still regarded as the gold standard in GBR; however, frequently reported soft-tissue problems, such as exposure of the membrane and subsequent infection, as well as the need to remove the membrane, have led to the development and use of resorbable membranes. 33Urban IA, Nagursky H, Lozada JL. Horizontal ridge augmentation with a resorbable membrane and particulated autogenous bone with or without anorganic bovine bone-derived mineral: a prospective case series in 22 patients. → Int J Oral Maxillofac Implants. 2011 Mar–Apr;26(2):404–14.34Ramel CF, Wismeijer DA, Hammerle CH, Jung RE. A randomized, controlled clinical evaluation of a synthetic gel membrane for guided bone regeneration around dental implants: clinical and radiologic 1- and 3-year results. → Int J Oral Maxillofac Implants. 2012 Mar–Apr;27(2):435–41. The use of bioresorbable membranes almost always requires autologous bone or deproteinized bovine bone mineral as a scaffold for the membrane.35Kohal RJ, Trejo PM, Wirsching C, Hurzeler MB, Caffesse RG. Comparison of bioabsorbable and bioinert membranes for guided bone regeneration around non-submerged implants. An experimental study in the mongrel dog. → Clin Oral Implants Res. 1999 Jun;10(3):226–37. In the present study, all defects were treated with autologous bone graft alone, or in combination with synthetic bone, and a resorbable membrane.
Regarding receptor site healing, Blanco et al. studied 26 implants with periimplant defects treated with nonresorbable membranes combined with autogenous bone grafts or decalcified freeze-dried bone allograft and reported 11.5% membrane exposure that required premature removal.3623. Blanco J, Alonso A, Sanz M. Long-term results and survival rate of implants treated with guided bone regeneration: a 5-year case series prospective study. → Clin Oral Implants Res. 2005 Jun;16(3):294–301. In the present study, membrane exposure occurred in 10% of grafting sites. These results agree with those of Juodzbalys et al., who reported a 5% resorbable membrane exposure rate.37Juodzbalys G, Raustia AM, Kubilius R. A 5-year follow-up study on one-stage implants inserted concomitantly with localized alveolar ridge augmentation. → J Oral Rehabil. 2007 Oct;34(10):781–9. The periapical radiographs of the sites showed no continuous periimplant radiolucency at the 3-year follow-up examination. The mean marginal bone loss after 3 years was 0.50 ± 0.27 mm. The results of this study are in agreement with those reported by De Boever and De Boever on GBR around nonsubmerged implants; these authors reported no marginal periimplant bone resorption except for 1 implant after 12–114 months of follow-up.38Cochran DL, Douglas HB. Augmentation of osseous tissue around nonsubmerged endosseous dental implants. → Int J Periodontics Restorative Dent. 1993 Dec;13(6):506–19. Nevins et al., in a retrospective multicenter study, reported a mean radiographic bone loss, over a 74-month period post-loading, of 0.64 mm (range: 0.3–0.8).39Nevins M, Mellonig JT, Clem DS 3rd, Reiser GM, Buser DA. Implants in regenerated bone: long-term survival. → Int J Periodontics Restorative Dent. 1998 Feb;18(1):34–45. These results agree with those reported on a submerged implant approach; Ramel et al. reported a mean bone loss of 0.43 ± 0.56 mm 1 year post-loading and a further bone loss of 0.17 mm in the following 2 years.40Ramel CF, Wismeijer DA, Hammerle CH, Jung RE. A randomized, controlled clinical evaluation of a synthetic gel membrane for guided bone regeneration around dental implants: clinical and radiologic 1- and 3-year results. → Int J Oral Maxillofac Implants. 2012 Mar–Apr;27(2):435–41. Juodzbalys et al. reported that 90% of all sites presented with stable crestal bone levels.41Juodzbalys G, Raustia AM, Kubilius R. A 5-year follow-up study on one-stage implants inserted concomitantly with localized alveolar ridge augmentation. → J Oral Rehabil. 2007 Oct;34(10):781–9. Christensen et al. found that 14% of the sites treated with GBR showed 1.5 mm of bone loss 3 years post-loading.42Christensen DK, Karoussis IK, Joss A, Hammerle CH, Lang NP. Simultaneous or staged installation with guided bone augmentation of transmucosal titanium implants. A 3-year prospective cohort study. → Clin Oral Implants Res. 2003 Dec;14(6):680–6.
The results of the study seem to show that bone regenerated with GBR around nonsubmerged dental implants remains stable over time with a good prognosis for the implants; however, some limitations should be noted. The first limitation is that the study did not include a control group and re-entries were not performed, so it provides no evidence of the effectiveness regarding bone regeneration, and the effectiveness of this technique was thus based on the postoperative complications and dental implant survival and success rates. The second limitation of the study is the absence of a radiographic outcome that could measure the amount of regenerated bone, because using a one-stage approach does not make it possible to measure it directly.43Meloni SM, Jovanovic SA, Urban I, Canullo L, Pisano M, Tallarico M. Horizontal Ridge augmentation using GBR with a native collagen membrane and 1:1 ratio of particulated xenograft and autologous bone: a 1-year prospective clinical study. → Clin Implant Dent Relat Res. 2017 Feb;19(1):38–45. Finally, the third limitation is the retrospective nature of this research.
Conclusion
Despite the limitations of this study, nonsubmerged implant placement in connection with GBR to treat periimplant bone defects is a feasible option with few healing complications and good long-term prognosis. Further longterm studies with appropriate controls and larger sample sizes and longer follow-ups should be conducted in order to confirm or reject these findings.

Interview
with Amparo Aloy Prósper
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 24, 25. | ↑ | Buser D, Mericske-Stern R, Dula K, Lang NP. Clinical experience with one-stage, non-submerged dental implants. → Adv Dent Res. 1999 Jun;13:153–61. |
| 2, 4, 26. | ↑ | Benić GI, Jung RE, Siegenthaler DW, Hammerle CH. Clinical and radiographic comparison of implants in regenerated or native bone: 5-year results. → Clin Oral Implants Res. 2009 May;20(5):507–13. |
| 3. | ↑ | Hammerle CH, Jung RE. Bone augmentation by means of barrier membranes. → Periodontology 2000. 2003 Oct;33:36–53. |
| 5. | ↑ | Lorenzoni M, Pertl C, Polansky RA, Jakse N, Wegscheider WA. Evaluation of implants placed with barrier membranes. A retrospective follow-up study up to five years. → Clin Oral Implants Res. 2002 Jun;13(3):274–80. |
| 6, 27. | ↑ | Zitzmann NU, Scharer P, Marinello CP. Long-term results of implants treated with guided bone regeneration: a 5-year prospective study. → Int J Oral Maxillofac Implants. 2001 May–Jun;16(3):355–66. |
| 7. | ↑ | Hammerle CH, Bragger U, Schmid B, Lang NP. Successful bone formation at immediate transmucosal implants: a clinical report. → Int J Oral Maxillofac Implants. 1998 Jul–Aug;13(4):522–30. |
| 8. | ↑ | Hurzeler MB, Kohal RJ, Naghshbandi J, Mota LF, Conradt J, Hutmacher D, Caffesse RG. Evaluation of a new bioresorbable barrier to facilitate guided bone regeneration around exposed implant threads. An experimental study in the monkey. → Int J Oral Maxillofac Surg. 1998 Aug;27(4):315–20. |
| 9. | ↑ | Carmagnola D, Berglundh T, Araujo M, Albrektsson T, Lindhe J. Bone healing around implants placed in a jaw defect augmented with Bio-Oss. An experimental study in dogs. → J Clin Periodontol. 2000 Nov;27(11):799–805. |
| 10. | ↑ | Brunel G, Benque E, Elharar F, Sansac C, Duffort JF, Barthet P, Baysse E, Miller N. Guided bone regeneration for immediate non-submerged implant placement using bioabsorbable materials in Beagle dogs. → Clin Oral Implants Res. 1998 Oct;9(5):303–12. |
| 11, 35. | ↑ | Kohal RJ, Trejo PM, Wirsching C, Hurzeler MB, Caffesse RG. Comparison of bioabsorbable and bioinert membranes for guided bone regeneration around non-submerged implants. An experimental study in the mongrel dog. → Clin Oral Implants Res. 1999 Jun;10(3):226–37. |
| 12. | ↑ | Fiorellini JP, Engebretson SP, Donath K, Weber HP. Guided bone regeneration utilizing expanded polytetrafluoroethylene membranes in combination with submerged and nonsubmerged dental implants in beagle dogs. → J Periodontol. 1998 May;69(5):528–35. |
| 13. | ↑ | Siciliano VI, Salvi GE, Matarasso S, Cafiero C, Blasi A, Lang NP. Soft tissues healing at immediate transmucosal implants placed into molar extraction sites with buccal self-contained dehiscences. A 12-month controlled clinical trial. → Clin Oral Implants Res. 2009 May;20(5):482–8. |
| 14. | ↑ | Cordaro L, Torsello F, Roccuzzo M. Clinical outcome of submerged vs. non-submerged implants placed in fresh extraction sockets. → Clin Oral Implants Res. 2009 Dec;20(12):1307–13. |
| 15. | ↑ | Vanden Bogaerde L. A proposal for the classification of bony defects adjacent to dental implants. → Int J Periodontics Restorative Dent. 2004 Jun;24(3):264–71. |
| 16, 31, 32. | ↑ | De Boever AL, De Boever JA. Guided bone regeneration around non-submerged implants in narrow alveolar ridges: a prospective long-term clinical study. → Clin Oral Implants Res. 2005 Oct;16(5):549–56. |
| 17, 42. | ↑ | Christensen DK, Karoussis IK, Joss A, Hammerle CH, Lang NP. Simultaneous or staged installation with guided bone augmentation of transmucosal titanium implants. A 3-year prospective cohort study. → Clin Oral Implants Res. 2003 Dec;14(6):680–6. |
| 18, 39. | ↑ | Nevins M, Mellonig JT, Clem DS 3rd, Reiser GM, Buser DA. Implants in regenerated bone: long-term survival. → Int J Periodontics Restorative Dent. 1998 Feb;18(1):34–45. |
| 19, 37, 41. | ↑ | Juodzbalys G, Raustia AM, Kubilius R. A 5-year follow-up study on one-stage implants inserted concomitantly with localized alveolar ridge augmentation. → J Oral Rehabil. 2007 Oct;34(10):781–9. |
| 20. | ↑ | De Boever AL, De Boever JA. A one-stage approach for nonsubmerged implants using a xenograft in narrow ridges: a report of seven cases. → Int J Periodontics Restorative Dent. 2003 Apr;23(2):169–75. |
| 21, 38. | ↑ | Cochran DL, Douglas HB. Augmentation of osseous tissue around nonsubmerged endosseous dental implants. → Int J Periodontics Restorative Dent. 1993 Dec;13(6):506–19. |
| 22. | ↑ | Kuller LH, Goldstein BD. Suggestions for STROBE recommendations. → Epidemiology. 2007 Nov;18(6):792–3. |
| 23. | ↑ | Esposito M, Grusovin MG, Loli V, Coulthard P, Worthington HV. Does antibiotic prophylaxis at implant placement decrease early implant failures? A Cochrane systematic review. → Eur J Oral Implantol. 2010 Summer;3(2):101–10. |
| 28. | ↑ | Blanco J, Alonso A, Sanz M. Long-term results and survival rate of implants treated with guided bone regeneration: a 5-year case series prospective study. → Clin Oral Implants Res. 2005 Jun;16(3):294–301. |
| 29. | ↑ | Hammerle CH, Jung RE, Feloutzis A. A systematic review of the survival of implants in bone sites augmented with barrier membranes (guided bone regeneration) in partially edentulous patients. → J Clin Periodontol. 2002;29 Suppl 3:226–31; discussion 232–3. |
| 30. | ↑ | Chiapasco M, Zaniboni M. Clinical outcomes of GBR procedures to correct peri-implant dehiscences and fenestrations: a systematic review. → Clin Oral Implants Res. 2009 Sep;20 Suppl 4:113–23. |
| 33. | ↑ | Urban IA, Nagursky H, Lozada JL. Horizontal ridge augmentation with a resorbable membrane and particulated autogenous bone with or without anorganic bovine bone-derived mineral: a prospective case series in 22 patients. → Int J Oral Maxillofac Implants. 2011 Mar–Apr;26(2):404–14. |
| 34, 40. | ↑ | Ramel CF, Wismeijer DA, Hammerle CH, Jung RE. A randomized, controlled clinical evaluation of a synthetic gel membrane for guided bone regeneration around dental implants: clinical and radiologic 1- and 3-year results. → Int J Oral Maxillofac Implants. 2012 Mar–Apr;27(2):435–41. |
| 36. | ↑ | 23. Blanco J, Alonso A, Sanz M. Long-term results and survival rate of implants treated with guided bone regeneration: a 5-year case series prospective study. → Clin Oral Implants Res. 2005 Jun;16(3):294–301. |
| 43. | ↑ | Meloni SM, Jovanovic SA, Urban I, Canullo L, Pisano M, Tallarico M. Horizontal Ridge augmentation using GBR with a native collagen membrane and 1:1 ratio of particulated xenograft and autologous bone: a 1-year prospective clinical study. → Clin Implant Dent Relat Res. 2017 Feb;19(1):38–45. |





Leave a Reply
Be the First to Comment!