Immediate implants in the esthetic area: Our perspective and clinical guidelines
May 8, 2018 / Categories: Digital Dentistry, Implant Dentistry

Perez, Alexandre

Valente, Nicola Alberto

Trottet, Lucille

Chatelain, Sibylle

Alfonsi, Fortunato

Barone, Antonio
Abstract
The placement of implants immediately after tooth extraction has proven to be a predictable treatment strategy with a very high success rate. Nevertheless, the success of this surgery involves strict clinical criteria. A description is provided of a clinical orientation and scientific point of view based on our experience and available evidence of when and how to perform this procedure in the esthetic area.
We consider the clinical criteria in relation to
- indications
- tooth extraction;
- soft-tissue management;
- implant placement technique;
- the critical distance and gap filling; and
- immediate versus delayed restoration.
These key factors, including a flapless procedure, presence of an intact buccal bone wall, absence of soft-tissue defects, gap filling to counteract the tissue changes after tooth extraction and immediate restoration when possible, should be considered to achieve good esthetic results.
Keywords
Dental implants, immediate dental implant loading, tooth extraction, alveolar process, bone remodeling.
Immediate placement of dental implants in the esthetic zone
Tooth extraction normally causes a remodeling process of the alveolar ridge, which normally follows a healing pattern with a dimensional shrinkage of the ridge in both shape and volume.1Amler MH. The time sequence of tissue regeneration in human extraction wounds. → Oral Surg Oral Med Oral Pathol. 1969 Mar;27(3):309–18. 2Cardaropoli G, Araújo M, Lindhe J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. → J Clin Periodontol. 2003 Sep;30(9):809–18. 3Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. → J Clin Periodontol. 2005 Feb;32(2):212–8. Thus, as a consequence of the natural healing events, implant placement to restore the missing tooth might be limited because of loss of the adequate amount of bone and because of the absence of the ideal volume of the residual ridge.4Amler MH. The time sequence of tissue regeneration in human extraction wounds. → Oral Surg Oral Med Oral Pathol. 1969 Mar;27(3):309–18. 5Cardaropoli G, Araújo M, Lindhe J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. → J Clin Periodontol. 2003 Sep;30(9):809–18. 6Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. → J Clin Periodontol. 2005 Feb;32(2):212–8. Several surgical procedures have been proposed to preserve or improve the volume of the alveolar ridge after a tooth extraction. Among the several available treatment options to manage a fresh extraction socket, immediate implant placement has been a debated issue in the last 25 years. During a consensus conference in 2003, Chen et al. established that immediate implants showed predictable outcomes in terms of survival rates that were similar to those of implants placed in healed ridges.7Chen ST, Wilson TG Jr, Hämmerle CH. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. → Int J Oral Maxillofac Implants. 2004;19 Suppl:12–25. These authors pointed out the need to better clarify the long-term esthetic outcomes for immediate implants.8Chen ST, Wilson TG Jr, Hämmerle CH. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. → Int J Oral Maxillofac Implants. 2004;19 Suppl:12–25. Moreover, the same authors observed that there was an absence of a clear classification, according to the timing of implant placement in extraction sockets.9Chen ST, Wilson TG Jr, Hämmerle CH. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. → Int J Oral Maxillofac Implants. 2004;19 Suppl:12–25. Thus, different authors10Chen ST, Buser D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla— a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:186–215.11Hämmerle CH, Araújo MG, Simion M; Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:80–2. have well clarified how to classify the timing for implant placement, in an extraction socket; nowadays, the terms “immediate,” “early” and “delayed” in relation to implant placement are universally accepted and recognized. Several publications have reported negative esthetic outcomes associated with immediate implant placement, such as gingival recession, higher marginal bone loss and interdental papillae loss.12Chen ST, Buser D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla— a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:186–215.13Cosyn J, De Rouck T. Aesthetic outcome of single-tooth implant restorations following early implant placement and guided bone regeneration: crown and soft tissue dimensions compared with contralateral teeth. → Clin Oral Implants Res. 2009 Oct;20(10):1063–9.14Botticelli D, Renzi A, Lindhe J, Berglundh T. Implants in fresh extraction sockets: a prospective 5-year follow-up clinical study. → Clin Oral Implants Res. 2008 Dec;19(12):1226–32. According to Buser et al., immediate implant placement in the esthetic area accounts for only 5–10% of cases, and for the rest, a different approach should be chosen, mostly early placement with hard-tissue healing (12–16 weeks), so for this reason, the clinician should develop the ability to both identify and successfully treat these few cases.15Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? → Periodontol 2000. 2017 Feb;73(1):84–102. The aim of this review paper is to report the most debated points in the literature and the clinical approach that could be considered predictable in terms of implant functional and esthetic implant success.
Clinical criteria
1. Indications
Immediate implant placement is certainly a delicate technique that requires experience and accurate case selection, based on certain indications, in order to achieve optimal results. The 3-D positioning of an immediate implant, which will be discussed later in this article, requires that the bone housing should allow for a palatal/lingual placement and a sufficient buccal bone thickness that guarantees support for the facial soft tissue, thus decreasing the risk of facial mucosal recession. When a buccal alveolar bone thickness amounts to less than 2 mm, its integrity is at risk of fenestration, dehiscence and soft-tissue recession.16Gapski R, Wang HL, Misch CE. Management of incision design in symphysis graft procedures: a review of the literature. → J Oral Implantol. 2001;27(3):134–42. 17Becker W, Goldstein M. Immediate implant placement: treatment planning and surgical steps for successful outcome. → Periodontol 2000. 2008 Jun;47(1):79–89.
Also, a possible immediate restoration of the immediate implant should be based on the meas‑ urement of ISQ (Implant Stability Quotient), the value of which has to be more than 62.18Barone A, Marconcini S, Giammarinaro E, Mijiritsky E, Gelpi F, Covani U. Clinical outcomes of implants placed in extraction sockets and immediately restored: a 7-year single-cohort prospective study. → Clin Implant Dent Relat Res. 2016 Dec;18(6):1103–12.
In order to summarize the indications for immediate implant placement in a short checklist that is easy for the clinician to follow, it can be suggested that the decision in favor of this technique should be made when the operator is facing these local clinical scenarios: integrity of buccal bone wall and absence of soft-tissue recession immediately after tooth extraction, presence of adequate interdental bone around adjacent teeth and presence of bone beyond the tooth apex to allow good implant stability. Moreover, the reasons for tooth extraction should be carefully evaluated when considering immediate implant placement, with the aim of identifying clinical conditions that could relatively contraindicate immediate implant placement. For example, tooth trauma, which is commonly associated with a fracture of the buccal bone plate; and periodontal disease, which is commonly associated with interdental bone loss, could represent relative contraindications to immediate implant placement (Figs. 1 & 2).
The presence of an acute infection, lack of bone beyond the tooth apex, proximity to anatomical vital structures and absence of local ideal clinical conditions should be considered as full contraindications to immediate implant placement.
Finally, it should be underlined that the experience of the clinician is a fundamental factor in the execution of this delicate technique. The esthetic outcomes can be compromised by the inexperience of surgeons, especially when the implants are placed in esthetic areas.19Barone A, Toti P, Marconcini S, Derchi G, Saverio M, Covani U. Esthetic outcome of implants placed in fresh extraction sockets by clinicians with or without experience: a medium-term retrospective evaluation. → Int J Oral Maxillofac Implants. 2016 Nov–Dec;31(6):1397–406.
-

- Fig. 1

-

- Fig. 2
Root remnant of first maxillary left premolar, occlusal view.
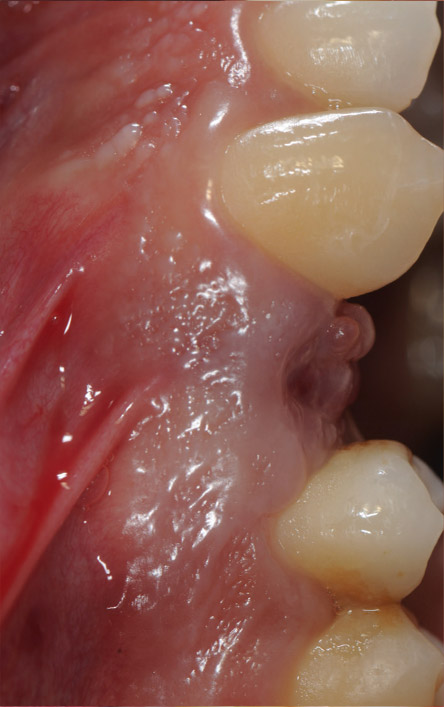
Fig. 2
Root remnant of first maxillary left premolar, lateral view.
2. Tooth extraction
The atraumatic extraction of the tooth to be replaced with an immediate implant is essential to prevent damage to the buccal bone plate and to preserve the interproximal papillae and labial soft tissue. Flapless extraction should be preferred or only a minimal mucoperiosteal flap elevation20Chen ST, Darby IB, Reynolds EC, Clement JG. Immediate implant placement postextraction without flap elevation. → J Periodontol. 2009 Jan;80(1):163–72. to preserve the integrity of the vascular supply from the periosteum and avoid alveolar bone resorption in the exposed area (Fig. 3). 21Kan JY, Rungcharassaeng K, Lozada JL, Zimmerman G. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: a 2- to 8-year follow-up. → Int J Oral Maxillofac Implants. 2011 Jan–Feb;26(1):179–87.22Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. → Int J Oral Maxillofac Implants. 2004;19 Suppl:43–61.
Several measures or instruments can be adopted to aid in an extraction that is the least traumatic as possible, including sectioning the tooth to carefully remove the fragments and the use of a piezoelectric device or microsurgical instrumentation, such as periotomes.
After the extraction, the socket should be thoroughly degranulated by careful curettage. Then, the integrity of the buccal bone and soft tissue should be checked to determine whether it is favorable for immediate implant placement.
3. Soft-tissue management
The maintenance of soft-tissue contour and dimension is one of the most challenging aspects of immediate implant placement. Indeed, midfacial mucosa recession around immediate implants has been reported to occur in a high percentage of cases (40%),23Botticelli D, Renzi A, Lindhe J, Berglundh T. Implants in fresh extraction sockets: a prospective 5-year follow-up clinical study. → Clin Oral Implants Res. 2008 Dec;19(12):1226–32. 24Araújo MG, Sukekava F, Wennstrom JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. → J Clin Periodontol. 2005 Jun;32(6):645–52. 25Kan JY, Rungcharassaeng K, Sclar A, Lozada JL. Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. → J Oral Maxillofac Surg. 2007 Jul;65(7 Suppl 1):13–9. and almost onethird of unsatisfactory esthetic outcomes have been associated with several factors, such as tissue biotype, thickness of facial bone wall and implant positioning.26Chen ST, Darby IB, Reynolds EC, Clement JG. Immediate implant placement postextraction without flap elevation. → J Periodontol. 2009 Jan;80(1):163–72.27Chen ST, Beagle J, Jensen SS, Chiapasco M, Darby I. Consensus statements and recommended clinical procedures regarding surgical techniques. → Int J Oral Maxillofac Implants. 2009;24 Suppl:272–8. It should also be taken into consideration that most of the soft-tissue changes can continue after implant surgery, even on a long-term basis.28Kan JY, Rungcharassaeng K, Lozada JL, Zimmerman G. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: a 2- to 8-year follow-up. → Int J Oral Maxillofac Implants. 2011 Jan–Feb;26(1):179–87. Today, it is well known that the surgical technique influences the soft tissue around immediate implants.29Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. → Int J Oral Maxillofac Implants. 2004;19 Suppl:43–61. 30Grunder U, Gracis S, Capelli M. Influence of the 3-D bone-to-implant relationship on esthetics. → Int J Periodontics Restorative Dent. 2005 Apr;25(2):113–9. The surgical procedure is usually performed flapless,31Covani U, Barone A, Cornelini R, Crespi R. Soft tissue healing around implants placed immediately after tooth extraction without incision: a clinical report. → Int J Oral Maxillofac Implants. 2004 Jul–Aug;19(4):549–53. and it has been shown that it enhances esthetics and decreases gingival recession,32Buser D, Wittneben J, Bornstein MM, Grutter L, Chappuis V, Belser UC. Stability of contour augmentation and esthetic outcomes of implant-supported single crowns in the esthetic zone: 3-year results of a prospective study with early implant placement postextraction. → J Periodontol. 2011 Mar;82(3):342–9. as previously discussed. The soft tissue at the facial level needs to be supported by a buccal bone wall of sufficient height and thickness. Therefore, a volume augmentation through grafting at the time of implant surgery seems to be strongly recommended33Cosyn J, De Rouck T. Aesthetic outcome of single-tooth implant restorations following early implant placement and guided bone regeneration: crown and soft tissue dimensions compared with contralateral teeth. → Clin Oral Implants Res. 2009 Oct;20(10):1063–9.34Buser D, Bornstein MM, Weber HP, Grutter L, Schmid B, Belser UC. Early implant placement with simultaneous guided bone regeneration following single-tooth extraction in the esthetic zone: a cross-sectional, retrospective study in 45 subjects with a 2- to 4-year follow-up. → J Periodontol. 2008 Sep;79(9):1773–81. 35Belser UC, Grütter L, Vailati F, Bornstein MM, Weber HP, Buser D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: a cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. → J Periodontol. 2009 Jan;80(1):140–51. to maintain the bone volume at the facial level on a long-term basis36Orsini G, Scarano A, Piattelli M, Piccirilli M, Caputi S, Piattelli A. Histologic and ultrastructural analysis of regenerated bone in maxillary sinus augmentation using a porcine bone-derived biomaterial. → J Periodontol. 2006 Dec;77(12):1984–90. 37Sbordone L, Levin L, Guidetti F, Sbordone C, Glikman A, Schwartz-Arad D. Apical and marginal bone alterations around implants in maxillary sinus augmentation grafted with autogenous bone or bovine bone material and simultaneous or delayed dental implant positioning. → Clin Oral Implants Res. 2011 May;22(5):485–91. and thus to avoid a soft-tissue collapse, which can be responsible for some negative esthetic effects.38Caneva M, Salata LA, de Souza SS, Bressan E, Botticelli D, Lang NP. Hard tissue formation adjacent to implants of various size and configuration immediately placed into extraction sockets: an experimental study in dogs. → Clin Oral Implants Res. 2010 Sep;21(9):885–90. 39Covani U, Bortolaia C, Barone A, Sbordone L. Bucco-lingual crestal bone changes after immediate and delayed implant placement. → J Periodontol. 2004 Dec;75(12):1605–12. Otherwise, the soft tissue can be managed by a provisional crown, and there is evidence to support that immediate implant placement with temporary restorations can provide stable esthetic results and limited recession.40Tarnow DP, Magner AW, Fletcher P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. → J Periodontol. 1992 Dec;63(12):995–6. In fact, it has been shown that it is advantageous to avoid manipulation of soft tissue during and after initial healing because such an intervention may disrupt the soft-tissue seal.41Abrahamsson I, Berglundh T, Lindhe J. The mucosal barrier following abutment dis/reconnection. An experimental study in dogs. → J Clin Periodontol. 1997 Aug;24(8):568–72. This manipulation is unavoidable when implants are placed according to the traditional two-stage protocol. Thus, the idea is that immediate provisional restoration allows for minimal disturbance of the soft tissue during healing, and as a consequence, it could be expected that the undisturbed soft tissue will result in better maintenance of the bone level position.42Cooper L, Felton DA, Kugelberg CF, Ellner S, Chaffee N, Molina AL, Moriarty JD, Paquette D, Palmqvist U. A multicenter 12-month evaluation of single-tooth implants restored 3 weeks after 1-stage surgery. → Int J Oral Maxillofac Implants. 2001 Mar–Apr;16(2):182–92.

Fig. 3
Tooth socket after careful atraumatic extraction of the root remnant.
4. Implant placement technique
Several factors are involved in the esthetic success of an immediate implant, among which the most important is certainly an appropriate implant positioning. A useful tool in the decision process during the evaluation of the extraction socket hard tissue for possible implant placement is the classification of Juodzbalys et al.43Juodzbalys G, Sakavicius D, Wang HL. Classification of extraction sockets based upon soft and hard tissue components. → J Periodontol. 2008 Mar;79(3):413–24. Once the alveolus is deemed adequate for the purpose, the implant placement should be performed as carefully as the already discussed atraumatic tooth extraction. A strict and standardized protocol should be followed that considers the peculiar anatomical features of a post-extraction socket, especially in the esthetic areas.
The implant site has to be prepared positioning the drills so that they follow the palatal bony wall as a guide and using the apical bone as much as the residual bone height allows. The residual apical bone will provide most of the necessary anchorage and stability for the implant. For this reason, the length of the implant should be accurately chosen accordingly during the planning. Once the implant site has been prepared, a periodontal probe should be used to verify the integrity of the walls. Finally, the implant must be placed with the platform at the marginal level of the buccal bone wall.
The palatally oriented preparation of the osteotomy is dictated by the anatomy of the post-extraction socket. The buccal wall of the socket is generally very thin and in the esthetic areas is generally less than 1 mm.44Vera C, De Kok IJ, Reinhold D, Limpiphipatanakorn P, Yap AK, Tyndall D, Cooper LF. Evaluation of buccal alveolar bone dimension of maxillary anterior and premolar teeth: a cone beam computed tomography investigation. → Int J Oral Maxillofac Implants. 2012 Nov–Dec;27(6):1514–9. According to Huynh-Ba et al., in the upper anterior area, this bone is equal to or less than 0.5 mm thick in 64.1% of cases.45Huynh-Ba G, Pjetursson BE, Sanz M, Cecchinato D, Ferrus J, Lindhe J, Lang NP. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. → Clin Oral Implants Res. 2010 Jan;21(1):37–42. Although early studies supported the hypothesis that immediate implant placement could preserve the initial alveolar crest dimension,46Schwartz-Arad D, Chaushu G. The ways and wherefores of immediate placement of implants into fresh extraction sites: a literature review. → J Periodontol. 1997 Oct;68(10):915–23. 47Werbitt MJ, Goldberg PV. The immediate implant: bone preservation and bone regeneration. → Int J Periodontics Restorative Dent. 1992;12(3):206–17.48Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. → Int J Periodontics Restorative Dent. 2003 Aug;23(4):313–23. later human and animal model studies showed that the ridge will not maintain its original shape for longer than 3–4 months after immediate implant placement.49Araújo MG, Sukekava F, Wennstrom JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. → J Clin Periodontol. 2005 Jun;32(6):645–52. 50Covani U, Bortolaia C, Barone A, Sbordone L. Bucco-lingual crestal bone changes after immediate and delayed implant placement. → J Periodontol. 2004 Dec;75(12):1605–12. For these reasons, it is important to keep a palatally oriented positioning, because the unavoidable resorption of the very thin buccal wall might compromise the success and the long-term survival of the implant if placed in close proximity to the buccal aspect (Figs. 4 & 5).
5. The critical distance and gap filling
According to many authors, the need to graft the gap between the implant and the buccal socket wall is guided by the length of this space.51Botticelli D, Berglundh T, Buser D, Lindhe J. The jumping distance revisited: an experimental study in the dog. → Clin Oral Implants Res. 2003 Feb;14(1):35–42. 52Wilson TG Jr, Schenk R, Buser D, Cochran D. Implants placed in immediate extraction sites: a report of histologic and histometric analyses of human biopsies. → Int J Oral Maxillofac Implants. 1998 May–Jun;13(3):333–41. The critical distance, beyond which a graft is strongly suggested, is considered to be 1.5 mm.53Botticelli D, Berglundh T, Buser D, Lindhe J. The jumping distance revisited: an experimental study in the dog. → Clin Oral Implants Res. 2003 Feb;14(1):35–42. 54Wilson TG Jr, Schenk R, Buser D, Cochran D. Implants placed in immediate extraction sites: a report of histologic and histometric analyses of human biopsies. → Int J Oral Maxillofac Implants. 1998 May–Jun;13(3):333–41. Several approaches have been proposed to fill the gap around implants, aimed at preserving or improving the dimension and contour of the ridge after tooth extraction and immediate implant placement.55Wilson TG Jr, Schenk R, Buser D, Cochran D. Implants placed in immediate extraction sites: a report of histologic and histometric analyses of human biopsies. → Int J Oral Maxillofac Implants. 1998 May–Jun;13(3):333–41. 56Covani U, Cornelini R, Barone A. Bucco-lingual bone remodeling around implants placed into immediate extraction sockets: a case series. → J Periodontol. 2003 Feb;74(2):268–73. Different studies have shown that the use of bone substitutes might also modify the pattern of bone remodeling.57Barone A, Ricci M, Calvo-Guirado JL, Covani U. Bone remodelling after regenerative procedures around implants placed in fresh extraction sockets: an experimental study in Beagle dogs. → Clin Oral Implants Res. 2011 Oct;22(10):1131–7. 58Covani U, Cornelini R, Calvo JL, Tonelli P, Barone A. Bone remodeling around implants placed in fresh extraction sockets. → Int J Periodontics Restorative Dent. 2010 Dec;30(6):601–7.
-

-
Fig. 4
Implant site preparation following the palatal wall of the socket.

-

-
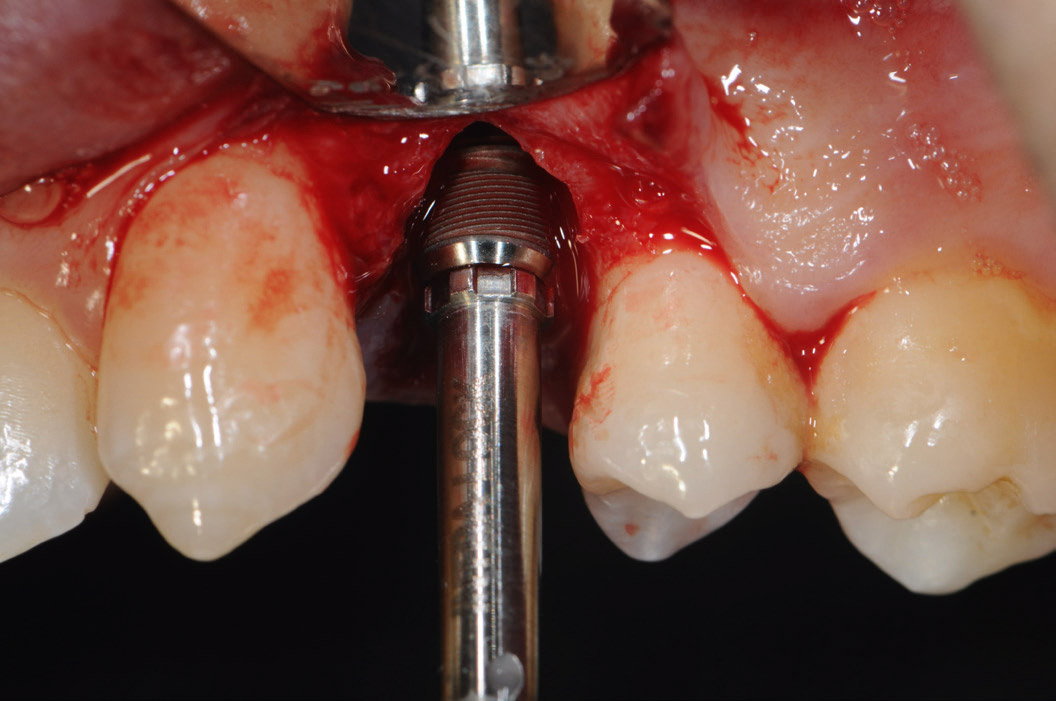
Fig. 5
Implant placement. The post-extraction socket presented a buccal V-shaped fenestration.
-

-
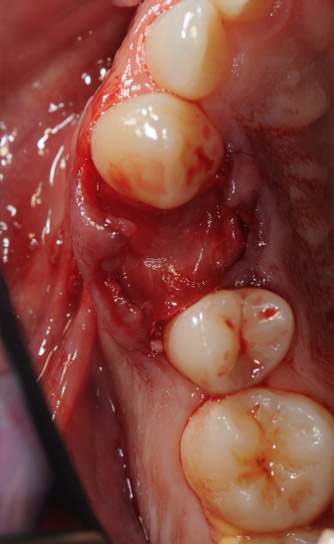
Fig. 6
The gap, coronal area and fenestration were grafted with xenograft particles.

-

-
Fig. 7
A resorbable collagen membrane was placed to cover the graft underneath the gingival margin.
-

-
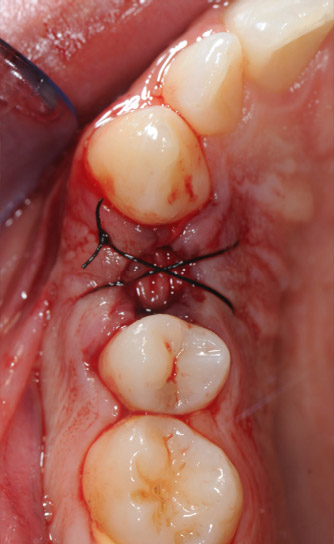
Fig. 8
Suture of the socket to stabilize the membrane.
-

-
Fig. 9
Placement of the final crown 5 months after implant placement.

In general, marginal bone changes around implants, when placed in fresh extraction sockets, may result in unfavorable bone thickness in the long term. For this reason, the use of guided bone regeneration techniques in this situation can be suggested. It is advisable to use corticocancellous porcine bone, which has a slow resorption rate, mixed or not with autogenous bone, and a resorbable membrane to stabilize the graft. The membrane can be left exposed, provided that antibiotic therapy is prescribed to the patient (amoxicillin and clavulanic acid, 1 g twice a day for 5 days, starting the day before surgery). With this technique, it was demonstrated in a previous study that implants have a cumulative survival rate of 94.6% at 7 years (Figs. 6–8).59Barone A, Marconcini S, Giammarinaro E, Mijiritsky E, Gelpi F, Covani U. Clinical outcomes of implants placed in extraction sockets and immediately restored: a 7-year single-cohort prospective study. → Clin Implant Dent Relat Res. 2016 Dec;18(6):1103–12. All of the guided bone regeneration techniques applied in the implant–socket gap are useful to limit buccal wall resorption; however, a complete preservation of the initial contour is never possible and a remodeling will always take place to some extent, although with a slower rate.60Barone A, Ricci M, Calvo-Guirado JL, Covani U. Bone remodelling after regenerative procedures around implants placed in fresh extraction sockets: an experimental study in Beagle dogs. → Clin Oral Implants Res. 2011 Oct;22(10):1131–7.
6. Immediate versus delayed restoration
Several studies have shown that there is no difference in the long-term survival of implants restored with immediate or delayed provisional crowns and that, concerning the success rate, the two restorative procedures seem to be very similar in terms of soft-tissue behavior at the buccal aspect.61Slagter KW, den Hartog L, Bakker NA, Vissink A, Meijer HJ, Raghoebar GM. Immediate placement of dental implants in the esthetic zone: a systematic review and pooled analysis. → J Periodontol. 2014 Jul;85(7):e241–50.62Del Fabbro M, Ceresoli V, Taschieri S, Ceci C, Testori T. Immediate loading of postextraction implants in the esthetic area: systematic review of the literature. → Clin Implant Dent Relat Res. 2015 Feb;17(1):52–70. 63Maló P, Nobre M. Flap vs. flapless surgical techniques at immediate implant function in predominantly soft bone for rehabilitation of partial edentulism: a prospective cohort study with follow-up of 1 year. → Eur J Oral Implantol. 2008 Winter;1(4):293–304. However, various studies regarding immediate implants placed in fresh extraction sockets suggested that wider papillary shrinkage was seen in delayed restorations than in immediate restorations.64Lang NP, Pun L, Lau KY, Li KY, Wong MC. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:39–66. From our point of view, the prosthetic treatment, namely immediate or delayed restoration, has to be based on strict clinical criteria, for example, the insertion torque value that should not be higher than 45 Ncm. Nevertheless, immediate prosthetic restoration may guarantee more predictable results in terms of an excellent hard- and soft-tissue prognosis for all aspects.65Barone A, Toti P, Quaranta A, Derchi G, Covani U. The clinical outcomes of immediate versus delayed restoration procedures on immediate implants: a comparative cohort study for single-tooth replacement. → Clin Implant Dent Relat Res. 2015 Dec;17(6):1114–26.
-

-
Fig. 10
Follow-up at 6 years: The papillae had completely filled the interdental spaces.

-

-
Fig. 11
Periapical radiograph at 6 years, showing optimal maintenance of the marginal bone level.
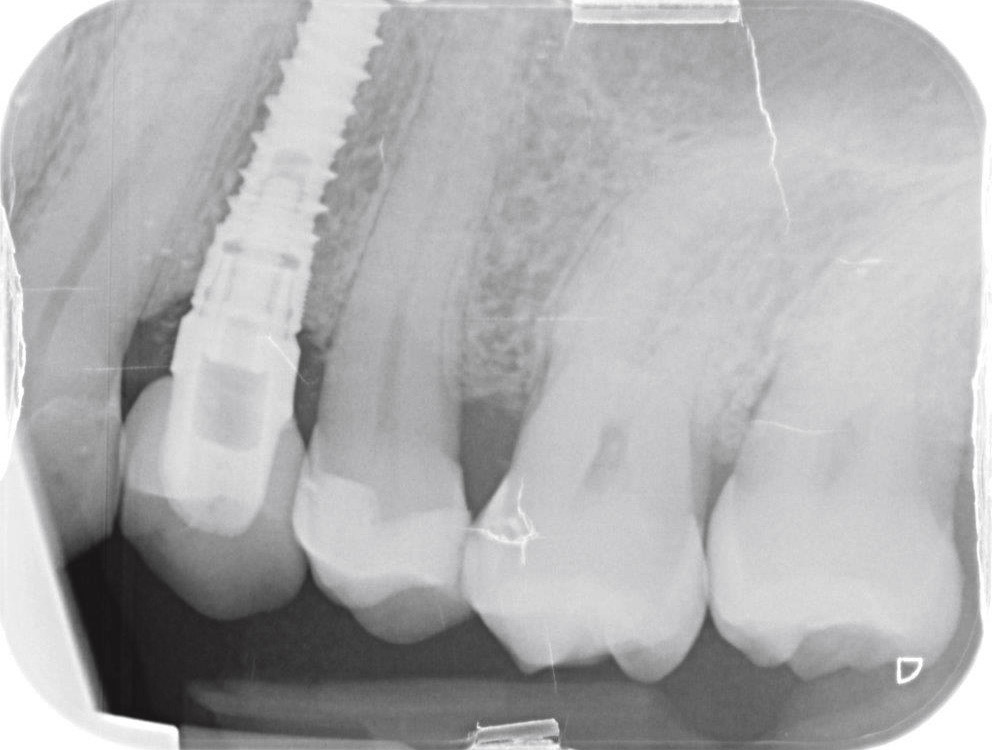
In their study, Barone et al. showed that, with delayed restorations, loss of papillary soft tissue and bone resorption were faster and localized, whereas with immediate restorations, tissue modifications appeared slow and gradual, allowing more predictable results with an excellent soft-tissue prognosis regarding, above all, the mesial and distal aspects.66Barone A, Toti P, Quaranta A, Derchi G, Covani U. The clinical outcomes of immediate versus delayed restoration procedures on immediate implants: a comparative cohort study for single-tooth replacement. → Clin Implant Dent Relat Res. 2015 Dec;17(6):1114–26. Moreover, treatment time until the final restoration is longer with delayed restoration than with immediate restoration.67Del Fabbro M, Ceresoli V, Taschieri S, Ceci C, Testori T. Immediate loading of postextraction implants in the esthetic area: systematic review of the literature. → Clin Implant Dent Relat Res. 2015 Feb;17(1):52–70. Finally, delayed restoration had higher costs than immediate restoration did, 26% more, owing to both the adjunctive second-stage surgery and the higher number of visits required (Figs. 9–11).68Brägger U, Krenander P, Lang NP. Economic aspects of single-tooth replacement. → Clin Oral Implants Res. 2005 Jun;16(3):335–41.
Conclusion
Nowadays, the improvement in implant technology and knowledge of healing patterns after tooth extraction has made it possible to achieve adequate success rates and favorable esthetic outcomes with immediate implants. It should be pointed out that immediate implant placement can be considered as a possible treatment option only when strict clinical criteria are met, such as integrity of the buccal bone plate, integrity of bone peaks of the adjacent teeth, integrity of soft tissue (adequate amount of keratinized gingiva, adequate gingival scallop and adequate interdental papillae) and a thick gingival biotype. Under these clinical conditions, immediate implant placement could be considered as a viable treatment option that shows predictable outcomes. For these reasons, the following points, as discussed in this review, should be considered and reviewed before implant placement in fresh extraction sockets:
- Case selection should be made according to inclusion and exclusion criteria.
- The extraction of the tooth or root remnant should be done as atraumatically as possible in order to avoid any damage to the hard and soft tissue.
- Soft-tissue integrity should be preserved by avoiding flap elevation or, if necessary, only performing a minimal flap elevation. This will also decrease buccal bone resorption.
- The implant placement should follow the palatal wall and a vestibular orientation should be avoided as far as possible to avoid possible fenestration of the implant after unavoidable bone remodeling.
- The gap between the implant and the buccal bone wall should be grafted to avoid resorption and exposure of the buccal aspect of the implant and to provide support to the soft tissue.
- Immediate restoration, when possible, should be preferred because it can guarantee better support to the interdental soft tissue and is less expensive for the patient.
In addition, it should be taken into consideration that, when all of the clinical conditions for immediate placement are present, this procedure is still considered as a complex procedure that requires high surgical skills. When the clinician is not sufficiently experienced or when all of the requirements are not satisfied, other techniques should be considered, such as early implant placement with soft- or hard-tissue healing and late implant placement with or without socket grafting.69Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? → Periodontol 2000. 2017 Feb;73(1):84–102.
Competing interests
The authors declare that they have no competing interests and have not received any support from any companies.
Interview
with Nicola Alberto Valente
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 4. | ↑ | Amler MH. The time sequence of tissue regeneration in human extraction wounds. → Oral Surg Oral Med Oral Pathol. 1969 Mar;27(3):309–18. |
| 2, 5. | ↑ | Cardaropoli G, Araújo M, Lindhe J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. → J Clin Periodontol. 2003 Sep;30(9):809–18. |
| 3, 6. | ↑ | Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. → J Clin Periodontol. 2005 Feb;32(2):212–8. |
| 7, 8, 9. | ↑ | Chen ST, Wilson TG Jr, Hämmerle CH. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. → Int J Oral Maxillofac Implants. 2004;19 Suppl:12–25. |
| 10, 12. | ↑ | Chen ST, Buser D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla— a systematic review. → Int J Oral Maxillofac Implants. 2014;29 Suppl:186–215. |
| 11. | ↑ | Hämmerle CH, Araújo MG, Simion M; Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:80–2. |
| 13, 33. | ↑ | Cosyn J, De Rouck T. Aesthetic outcome of single-tooth implant restorations following early implant placement and guided bone regeneration: crown and soft tissue dimensions compared with contralateral teeth. → Clin Oral Implants Res. 2009 Oct;20(10):1063–9. |
| 14. | ↑ | Botticelli D, Renzi A, Lindhe J, Berglundh T. Implants in fresh extraction sockets: a prospective 5-year follow-up clinical study. → Clin Oral Implants Res. 2008 Dec;19(12):1226–32. |
| 15, 69. | ↑ | Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? → Periodontol 2000. 2017 Feb;73(1):84–102. |
| 16. | ↑ | Gapski R, Wang HL, Misch CE. Management of incision design in symphysis graft procedures: a review of the literature. → J Oral Implantol. 2001;27(3):134–42. |
| 17. | ↑ | Becker W, Goldstein M. Immediate implant placement: treatment planning and surgical steps for successful outcome. → Periodontol 2000. 2008 Jun;47(1):79–89. |
| 18, 59. | ↑ | Barone A, Marconcini S, Giammarinaro E, Mijiritsky E, Gelpi F, Covani U. Clinical outcomes of implants placed in extraction sockets and immediately restored: a 7-year single-cohort prospective study. → Clin Implant Dent Relat Res. 2016 Dec;18(6):1103–12. |
| 19. | ↑ | Barone A, Toti P, Marconcini S, Derchi G, Saverio M, Covani U. Esthetic outcome of implants placed in fresh extraction sockets by clinicians with or without experience: a medium-term retrospective evaluation. → Int J Oral Maxillofac Implants. 2016 Nov–Dec;31(6):1397–406. |
| 20, 26. | ↑ | Chen ST, Darby IB, Reynolds EC, Clement JG. Immediate implant placement postextraction without flap elevation. → J Periodontol. 2009 Jan;80(1):163–72. |
| 21. | ↑ | Kan JY, Rungcharassaeng K, Lozada JL, Zimmerman G. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: a 2- to 8-year follow-up. → Int J Oral Maxillofac Implants. 2011 Jan–Feb;26(1):179–87. |
| 22, 29. | ↑ | Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. → Int J Oral Maxillofac Implants. 2004;19 Suppl:43–61. |
| 23. | ↑ | Botticelli D, Renzi A, Lindhe J, Berglundh T. Implants in fresh extraction sockets: a prospective 5-year follow-up clinical study. → Clin Oral Implants Res. 2008 Dec;19(12):1226–32. |
| 24, 49. | ↑ | Araújo MG, Sukekava F, Wennstrom JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. → J Clin Periodontol. 2005 Jun;32(6):645–52. |
| 25. | ↑ | Kan JY, Rungcharassaeng K, Sclar A, Lozada JL. Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. → J Oral Maxillofac Surg. 2007 Jul;65(7 Suppl 1):13–9. |
| 27. | ↑ | Chen ST, Beagle J, Jensen SS, Chiapasco M, Darby I. Consensus statements and recommended clinical procedures regarding surgical techniques. → Int J Oral Maxillofac Implants. 2009;24 Suppl:272–8. |
| 28. | ↑ | Kan JY, Rungcharassaeng K, Lozada JL, Zimmerman G. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: a 2- to 8-year follow-up. → Int J Oral Maxillofac Implants. 2011 Jan–Feb;26(1):179–87. |
| 30. | ↑ | Grunder U, Gracis S, Capelli M. Influence of the 3-D bone-to-implant relationship on esthetics. → Int J Periodontics Restorative Dent. 2005 Apr;25(2):113–9. |
| 31. | ↑ | Covani U, Barone A, Cornelini R, Crespi R. Soft tissue healing around implants placed immediately after tooth extraction without incision: a clinical report. → Int J Oral Maxillofac Implants. 2004 Jul–Aug;19(4):549–53. |
| 32. | ↑ | Buser D, Wittneben J, Bornstein MM, Grutter L, Chappuis V, Belser UC. Stability of contour augmentation and esthetic outcomes of implant-supported single crowns in the esthetic zone: 3-year results of a prospective study with early implant placement postextraction. → J Periodontol. 2011 Mar;82(3):342–9. |
| 34. | ↑ | Buser D, Bornstein MM, Weber HP, Grutter L, Schmid B, Belser UC. Early implant placement with simultaneous guided bone regeneration following single-tooth extraction in the esthetic zone: a cross-sectional, retrospective study in 45 subjects with a 2- to 4-year follow-up. → J Periodontol. 2008 Sep;79(9):1773–81. |
| 35. | ↑ | Belser UC, Grütter L, Vailati F, Bornstein MM, Weber HP, Buser D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: a cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. → J Periodontol. 2009 Jan;80(1):140–51. |
| 36. | ↑ | Orsini G, Scarano A, Piattelli M, Piccirilli M, Caputi S, Piattelli A. Histologic and ultrastructural analysis of regenerated bone in maxillary sinus augmentation using a porcine bone-derived biomaterial. → J Periodontol. 2006 Dec;77(12):1984–90. |
| 37. | ↑ | Sbordone L, Levin L, Guidetti F, Sbordone C, Glikman A, Schwartz-Arad D. Apical and marginal bone alterations around implants in maxillary sinus augmentation grafted with autogenous bone or bovine bone material and simultaneous or delayed dental implant positioning. → Clin Oral Implants Res. 2011 May;22(5):485–91. |
| 38. | ↑ | Caneva M, Salata LA, de Souza SS, Bressan E, Botticelli D, Lang NP. Hard tissue formation adjacent to implants of various size and configuration immediately placed into extraction sockets: an experimental study in dogs. → Clin Oral Implants Res. 2010 Sep;21(9):885–90. |
| 39, 50. | ↑ | Covani U, Bortolaia C, Barone A, Sbordone L. Bucco-lingual crestal bone changes after immediate and delayed implant placement. → J Periodontol. 2004 Dec;75(12):1605–12. |
| 40. | ↑ | Tarnow DP, Magner AW, Fletcher P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. → J Periodontol. 1992 Dec;63(12):995–6. |
| 41. | ↑ | Abrahamsson I, Berglundh T, Lindhe J. The mucosal barrier following abutment dis/reconnection. An experimental study in dogs. → J Clin Periodontol. 1997 Aug;24(8):568–72. |
| 42. | ↑ | Cooper L, Felton DA, Kugelberg CF, Ellner S, Chaffee N, Molina AL, Moriarty JD, Paquette D, Palmqvist U. A multicenter 12-month evaluation of single-tooth implants restored 3 weeks after 1-stage surgery. → Int J Oral Maxillofac Implants. 2001 Mar–Apr;16(2):182–92. |
| 43. | ↑ | Juodzbalys G, Sakavicius D, Wang HL. Classification of extraction sockets based upon soft and hard tissue components. → J Periodontol. 2008 Mar;79(3):413–24. |
| 44. | ↑ | Vera C, De Kok IJ, Reinhold D, Limpiphipatanakorn P, Yap AK, Tyndall D, Cooper LF. Evaluation of buccal alveolar bone dimension of maxillary anterior and premolar teeth: a cone beam computed tomography investigation. → Int J Oral Maxillofac Implants. 2012 Nov–Dec;27(6):1514–9. |
| 45. | ↑ | Huynh-Ba G, Pjetursson BE, Sanz M, Cecchinato D, Ferrus J, Lindhe J, Lang NP. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. → Clin Oral Implants Res. 2010 Jan;21(1):37–42. |
| 46. | ↑ | Schwartz-Arad D, Chaushu G. The ways and wherefores of immediate placement of implants into fresh extraction sites: a literature review. → J Periodontol. 1997 Oct;68(10):915–23. |
| 47. | ↑ | Werbitt MJ, Goldberg PV. The immediate implant: bone preservation and bone regeneration. → Int J Periodontics Restorative Dent. 1992;12(3):206–17. |
| 48. | ↑ | Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. → Int J Periodontics Restorative Dent. 2003 Aug;23(4):313–23. |
| 51, 53. | ↑ | Botticelli D, Berglundh T, Buser D, Lindhe J. The jumping distance revisited: an experimental study in the dog. → Clin Oral Implants Res. 2003 Feb;14(1):35–42. |
| 52, 54, 55. | ↑ | Wilson TG Jr, Schenk R, Buser D, Cochran D. Implants placed in immediate extraction sites: a report of histologic and histometric analyses of human biopsies. → Int J Oral Maxillofac Implants. 1998 May–Jun;13(3):333–41. |
| 56. | ↑ | Covani U, Cornelini R, Barone A. Bucco-lingual bone remodeling around implants placed into immediate extraction sockets: a case series. → J Periodontol. 2003 Feb;74(2):268–73. |
| 57. | ↑ | Barone A, Ricci M, Calvo-Guirado JL, Covani U. Bone remodelling after regenerative procedures around implants placed in fresh extraction sockets: an experimental study in Beagle dogs. → Clin Oral Implants Res. 2011 Oct;22(10):1131–7. |
| 58. | ↑ | Covani U, Cornelini R, Calvo JL, Tonelli P, Barone A. Bone remodeling around implants placed in fresh extraction sockets. → Int J Periodontics Restorative Dent. 2010 Dec;30(6):601–7. |
| 60. | ↑ | Barone A, Ricci M, Calvo-Guirado JL, Covani U. Bone remodelling after regenerative procedures around implants placed in fresh extraction sockets: an experimental study in Beagle dogs. → Clin Oral Implants Res. 2011 Oct;22(10):1131–7. |
| 61. | ↑ | Slagter KW, den Hartog L, Bakker NA, Vissink A, Meijer HJ, Raghoebar GM. Immediate placement of dental implants in the esthetic zone: a systematic review and pooled analysis. → J Periodontol. 2014 Jul;85(7):e241–50. |
| 62, 67. | ↑ | Del Fabbro M, Ceresoli V, Taschieri S, Ceci C, Testori T. Immediate loading of postextraction implants in the esthetic area: systematic review of the literature. → Clin Implant Dent Relat Res. 2015 Feb;17(1):52–70. |
| 63. | ↑ | Maló P, Nobre M. Flap vs. flapless surgical techniques at immediate implant function in predominantly soft bone for rehabilitation of partial edentulism: a prospective cohort study with follow-up of 1 year. → Eur J Oral Implantol. 2008 Winter;1(4):293–304. |
| 64. | ↑ | Lang NP, Pun L, Lau KY, Li KY, Wong MC. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. → Clin Oral Implants Res. 2012 Feb;23 Suppl 5:39–66. |
| 65, 66. | ↑ | Barone A, Toti P, Quaranta A, Derchi G, Covani U. The clinical outcomes of immediate versus delayed restoration procedures on immediate implants: a comparative cohort study for single-tooth replacement. → Clin Implant Dent Relat Res. 2015 Dec;17(6):1114–26. |
| 68. | ↑ | Brägger U, Krenander P, Lang NP. Economic aspects of single-tooth replacement. → Clin Oral Implants Res. 2005 Jun;16(3):335–41. |





Leave a Reply
Be the First to Comment!