Influence of nonpassive fit in immediate loading: A pilot study
September 26, 2018 / Categories: Digital Dentistry, Implant Dentistry

Rubio, Nicolas Agustin

Trevino Santos, Alejandro
Abstract
Objective
The objective of this study was to evaluate the influence of nonpassively fitting prostheses on implant osseointegration and possible implant displacement during the healing period.
Materials and methods
Three healthy edentulous patients, ranging from 40 to 60 years, both sexes, were treated in the lower jaw with a 5-implant protocol. A fixed screw-retained prosthesis adapted from a prefabricated complete denture was installed. Implant position was recorded by analogic and virtual impressions, both at the time of implant placement and after the healing period. Also, abutment position was recorded before prosthesis installation. Level of misfit and stress were measured by 4 different clinical methods. Casts, prostheses and intraoral position of implants were compared throughout the study. Implant stability was assessed with resonance frequency analysis and torque control.
Results
Implant osseointegration occurred successfully in all 15 implants. Nonpassive prostheses were installed and passive prostheses were removed after 8 weeks, as implant position changed and strain was released. Implant final position was guided by abutment position in the restoration, as the prostheses showed no change in their structure.
Conclusion
Within the limitations of this study, passivity was not necessary to achieve implant osseointegration. Final implant position was modified, as tension was induced in a phenomenon similar to orthodontic movement. Prosthetic procedures to manufacture final restorations should rely on abutment position in the interim prosthesis rather than on initial implant position.
Keywords
Immediate loading; implant; passive fit.
Introduction
Immediate loading of microtextured implants with 1-piece fixed interim prostheses, in both the edentulous mandible and maxilla, has proved to be as predictable as early and conventional loading.1Papaspyridakos P, Chen CJ, Chuang SK, Weber HP. Implant loading protocols for edentulous patients with fixed prostheses: a systematic review and meta-analysis. → Int J Oral Maxillofac Implants. 2014;29 Suppl:256–70. For the mandible, the procedure is clinically well documented for the use of 2Kapos T, Ashy LM, Gallucci GO, Weber HP, Wismeijer D. Computer-aided design and computer-assisted manufacturing in prosthetic implant dentistry. → Int J Oral Maxillofac Implants. 2009;24 Suppl:110–7.,3Balshi SF, Wolfinger GJ, Balshi TJ. Surgical planning and prosthesis construction using computer technology and medical imaging for immediate loading of implants in the pterygomaxillary region. → Int J Periodontics Restorative Dent. 2006 Jun;26(3):239–47.,4Komiyama A, Petterson A, Huitin M, Näsström K, Kinge B. Virtually planned and template-guided implant surgery: an experimental model matching approach. → Clin Oral Implants Res. 2011 Mar;22(3):308–13. implants,5Wismeijer D, Casentini P, Gallucci G, Chiapasco M. ITI treatment guide, Vol. 4: loading protocols in implant dentistry: edentulous patients. → Berlin: Quintessence. 2010. 248 p. loaded within 7 days after surgery.6Esposito M, Grusovin MG, Willings M, Coulthard P, Worthington HV. Interventions for replacing missing teeth: different times for loading dental implants. → Cochrane Database Syst Rev. 2007 Apr 18;(2):CD003878. In summary of all prosthetic techniques described in the literature, procedures can vary between those in which a provisional restoration is prefabricated by CAD/CAM (together with a guided surgery protocol),7Kapos T, Ashy LM, Gallucci GO, Weber HP, Wismeijer D. Computer-aided design and computer-assisted manufacturing in prosthetic implant dentistry. → Int J Oral Maxillofac Implants. 2009;24 Suppl:110–7. those in which an impression is taken immediately after surgery in order to deliver a manufactured interim prosthesis, and those in which pre-existing complete dentures are adapted to implants by a chairside technique. Whichever method is used, difficulties in delivering a prosthesis with perfect fit are very common.
To begin with, computer-aided surgery is accepted to vary in accuracy, according to postoperative measurements.8Balshi SF, Wolfinger GJ, Balshi TJ. Surgical planning and prosthesis construction using computer technology and medical imaging for immediate loading of implants in the pterygomaxillary region. → Int J Periodontics Restorative Dent. 2006 Jun;26(3):239–47.,9Komiyama A, Petterson A, Huitin M, Näsström K, Kinge B. Virtually planned and template-guided implant surgery: an experimental model matching approach. → Clin Oral Implants Res. 2011 Mar;22(3):308–13. Although apex deviation of the implant (and not its coronal position) is always the most inaccurate aspect of the clinical outcome,10Valente F, Schiroli G, Sbrenna A. Accuracy of computer-aided oral implant surgery: a clinical and radiographic study. → Int J Oral Maxillofac Implants. 2009 Mar–Apr;24(2):234–42. many clinicians recommend the use of tooth-supported or mini-implant-supported templates rather than mucosa-supported guides, in order to improve accuracy.11Geng W, Liu C, Su Y, Li J, Zhou J. Accuracy of different types of computer-aided design/computer-aided manufacturing surgical guides for dental implant placement. → Int J Clin Exp Med. 2015 Jun;8(6):8442–9. Furthermore, open- and closed-tray impression techniques, or even oral welding procedures,12Degidi MI, Nardi D, Sighinolfi G, Piattelli A. Immediate rehabilitation of the edentulous mandible using Ankylos SynCone telescopic copings and intraoral welding: a pilot study. → Int J Periodontics Restorative Dent. 2012 Dec;32(6):189–94. followed by dental laboratory prosthesis manufacturing usually need more than a short period to completely assess the fit of the restoration. Cases have been reported in which changes had to be made to adapt prostheses after manufacturing, even with the use of intraoral welding,13Yilmaz B, Suarez C, McGlumphy E. Correction of misfit in a maxillary immediate metal-resin implant-fixed complete prosthesis placed with flapless surgery on four implants. → Int J Oral Maxillofac Implants. 2011 Sep–Oct;26(5):23–8. while others appeared to have good fit. Finally, chairside procedures turning a complete denture into a hybrid screw-retained prosthesis are well known, and this approach has been described as a simple, low-cost and effective clinical method.14Miguel-Figuero J, Fernandez-Jordan Celorio J. Modificacion de la tecnica all-on-4: protesis fija inmediata implantosoportada sin la intervencion del laboratorio de protesis (caso clinico) [Modification of the All-on-4 technique: fixed, immediate and complete rehabilitation with dental implants without participation of the dental laboratory (clinical case)]. → RCOE. 2006 Mar–Apr;11(2). Spanish.,15Levin BP. A team approach to cost-effective, full-arch immediate loading. → Compend Contin Educ Dent. 2013 Jul–Aug;34(7):530–2. Despite the advantage of improving the fitting by adapting the prosthesis with an intraoral procedure, this pickup technique involves using a great amount of acrylic resin to bond the abutments. Regardless of the pickup method or the resin used, polymerization always tends to induce some degree of tension between the abutments. This tension is released after the pickup itself and results in a misfit when installing the adapted prosthesis.
In light of these considerations a clinical misfit can be found very often when installing interim prostheses in a full-arch immediate loading procedure, regardless of the prosthetic approach selected. This implies a nonpassive structure tightened to implants with a certain amount of tension between them. In general, it is accepted that the need for passivity of fit is greater in implant-supported restorations than in conventional tooth-supported restorations because of the absence of a periodontal ligament.16Karl M, Graef F, Wichmann M, Krafft T. Passivity of fit of CAD/CAM and copy-milled frameworks, veneered frameworks, and anatomically contoured, zirconia ceramic, implant-supported fixed prostheses. → J Prosthet Dent. 2012 Apr;107(4):232–8. However, it is difficult to achieve this passive fit in immediate loading protocols and sometimes excessive torque is used to properly seat full-arch restorations. Nevertheless, implant survival rates in the literature and over many years have succeeded in validating these treatments.17Papaspyridakos P, Chen CJ, Chuang SK, Weber HP. Implant loading protocols for edentulous patients with fixed prostheses: a systematic review and meta-analysis. → Int J Oral Maxillofac Implants. 2014;29 Suppl:256–70. Moreover, there is a phenomenon that occurs during implant osseointegration that helps nonpassive fit become passive. This can be seen when taking out the interim prosthesis and assessing implant osseointegration 6–8 weeks after surgery. It appears that something changes during the healing period, as the prosthesis has a perfect fit and can be tightened without the need for increasing normal torque at this time. Tension is thus dissipated and osseointegration is successfully achieved, at least in the major percentage of cases. It seems that an element, if not all of the constituent parts, changes or moves to relieve this tension.
Gallucci et al. observed screw loosening in all edentulous patients treated with their pickup technique after 2 weeks of control.18Gallucci GO, Bernard JP, Bertosa M, Belser UC. Immediate loading with fixed screw-retained provisional restorations in edentulous jaws: the pickup technique. → Int J Oral Maxillofac Implants. 2004 Jul–Aug;19(4):524–33. This problem was not present in subsequent prosthesis removals and was associated either with gradual wear of the titanium abutments in the zone of contact or with minor implant movement, as implants could respond to tension applied during screw tightening with minimal displacement. Furthermore, a randomized controlled trial by Karl and Taylor succeeded in proving that bone adaptation around statically and dynamically loaded osseointegrated implants occurred, causing a decrease in misfit strain provoked by a nonpassively fitting prosthesis.19Karl M, Taylor TD. Bone adaptation induced by non-passively fitting implant superstructures: a randomized clinical trial. → Int J Oral Maxillofac Implants. 2016 Mar–Apr;31(2):369–75. Moreover, micromotion induced during the implant healing period does not seem to be detrimental to osseointegration and only excessive micromotion is directly implicated in the formation of fibrous encapsulation in experimental models.20Szmuker-Moncler S, Salama H, Reingewirtz Y, Dubruille JH. Timing of loading and effect on micromotion on bone-dental implant interface: a review of experimental literature. → J Biomed Mater Res. 1998 Summer;43(2):192–203.
It is feasible that a modification in the whole bone–implant–abutment–prosthetic structure allows osseointegration in the presence of a nonpassive fit and also allows dissipation of the strain provoked. Thus, the main objectives of the current pilot study were to prove that passivity is not necessary itself to achieve osseointegration and to prove that slight implant movement helps to reduce tension and adapt its position to the prosthetic structure. For that purpose, information on the position of the implants was collected from an in vivo model before implant loading and after the healing period. Analog and digital casts helped assess accurate implant position, and clinical methods were used to assess the fit and passivity of the structures.
The null hypothesis was that passivity was not related to osseointegration success. Additionally, a second hypothesis was that recently placed implants can change their position, guided by the tension applied by a nonpassive screw-retained prosthesis. Otherwise, tension will remain after the healing period or will be released by the acrylic resin or any other element involved.
Materials and methods
For this preliminary study, 3 healthy edentulous patients, ranging from 40 to 60 years, both sexes, were treated in the lower jaw with a 5-implant protocol together with immediate restoration loading. To leave aside the influence of different types of bone,21Lekholm U, Zarb GA. Patient selection and preparation. In: Brånemark PI, Zarb GA, Albrektsson T, editors. Tissue-integrated prostheses: osseointegration in clinical dentistry. → Chicago: Quintessence; 1985. p. 199–209. only inferior arches were included in the study, all of them with insufficient bone in which to place regular implants in the posterior area. Thus, 5 implants were placed between the mental foramina to support a fixed screw-retained prosthesis adapted from a prefabricated complete denture. Implant and abutment position were recorded and compared throughout the study, together with the level of misfit of the structures. Implant stability was assessed with resonance frequency analysis and torque control.
Under local anesthesia, a full flap was raised in the lower jaw to expose mental foramina using a specific surgical approach.22Galante JM, Rubio NA. Surgical approach for the fully edentulous mandible. → Clin Oral Implants Res. 2014;25(10):467. The interforaminal area was flattened if necessary to level the bone height and develop an adequate bone width for installing regular-diameter implants. Osteotomies were performed so that distal implants could be slightly tilted to increase the anterior– posterior spread23De Fabbro M, Bellini CM, Romeo D, Francetti L. Tilted implants for the rehabilitation of edentulous jaws: a systematic review. → Clin Implant Dent Relat Res. 2012 Aug;14(4):612–21. and so that implants could emerge at the occlusal or lingual aspect of the future prosthesis. A surgical guide was made by duplicating the prosthesis. Five dental implants (Straumann Bone Level, Straumann AG) of a minimum length of 10 mm were placed under mechanical torque control (Surgic Pro, NSK-Nakanishi) until 35 N cm2 was reached. Manual insertion continued with a ratchet and torque control device without the driver (Loxim, Straumann AG reaching breaking torque (Fig. 1). Before installing abutments, implant primary stability was measured with radiofrequency (ISQ, Osstell) by a second surgeon, blind to the surgical procedure, and recorded by an assistant (Table 1). All implants reached a minimum of 60 ISQ and this determined the possibility of immediate loading.24Gallucci GO, Benic GI, Eckert SE, Papaspyridakos P, Schimmel M, Schrott A, Weber HP. Consensus statements and clinical recommendations for implant loading protocols. → Int J Oral Maxillofac Implants. 2014;29 Suppl:287–90. Then, the first surgeon selected transmucosal pillar abutments (Multibase, Straumann AG) according to soft-tissue height and torqued them to 35 N cm2. Healing caps were used to facilitate suturing and repositioning of the soft tissue around implants. Interrupted sutures were performed using a polyglycolic acid resorbable suture (Atramat).
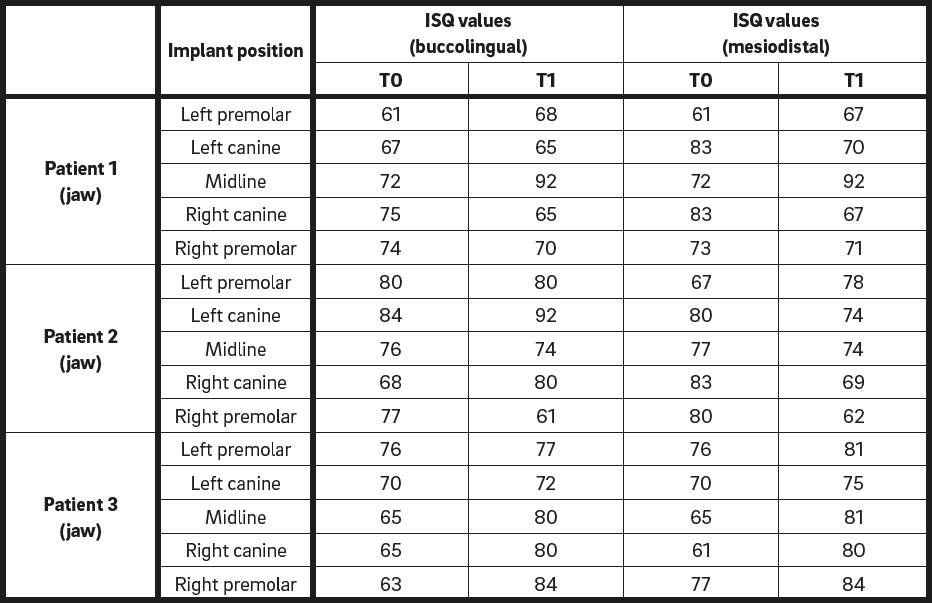
Implant stability values at Time 0 (T0) and Time 1 (T1).
-
-
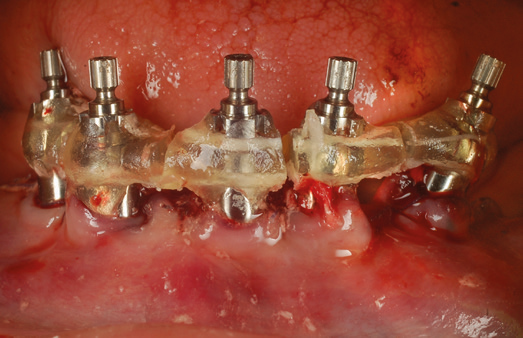
Fig. 4
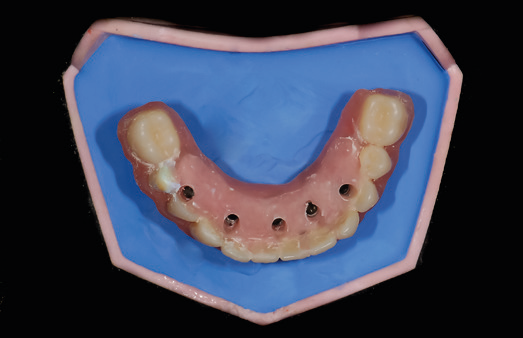
Cast 2: prosthesis after pickup technique with autopolymerizing resin.
-
-
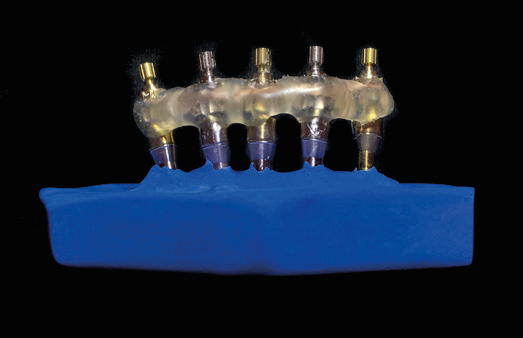
Fig. 3
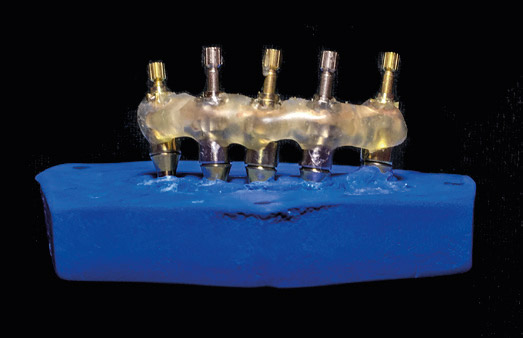
Cast 1: initial implant position recorded with the splint.
-
-
Fig. 2
Splint made with lightactivated polymerization resin.
-
-
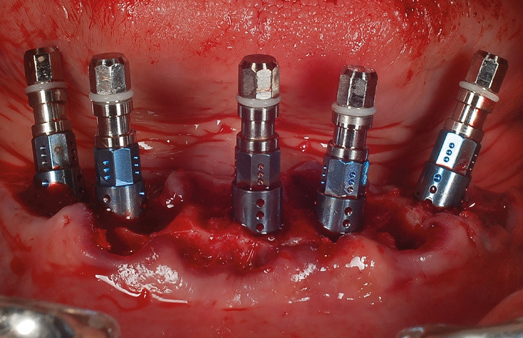
Fig. 1
Implant placement.
Before the pickup procedure, scan bodies were used to take a digital impression using an intraoral scanner (TRIOS, 3Shape). Later, impression posts were screwed in and splinted using light-activated polymerization resin (Triad Gel, Dentsply Sirona), separated with a small-diameter diamond bur (Fig. 2) and splinted again using a minimal amount of resin.25Wee AG, Aquilino SA, Schneider RL. Strategies to achieve fit in implant prosthodontics: a review of the literature. → Int J Prosthodont. 1999 Mar–Apr;12(2):167–78. A stone cast was made with a 2-step technique (passive cast technique) using a low-expansion dental stone (Elite Rock, Zhermack) and a vacuum machine. With these 2 procedures, the virtual and the analog position of the implants were recorded before any prosthetic procedure could modify it. This cast was called Cast 1 (C1) and represented the initial position of the implants (Fig. 3). Later, Multibase temporary abutments were installed and torqued to 15 N cm2, checking for interferences with the hollow prosthesis and the occlusion. Using a pickup technique, they were bonded to the hollow prosthesis with autopolymerizing resin. This procedure was done without taking into account the contraction provoked by using a large amount of acrylic resin and thus the amount of stress generated by said polymerization. The wound was protected with a rubber dam and the prosthesis was held under patient occlusion during the setting of the material. Once the prosthesis had been removed, correct bonding of the abutments was assessed. If any abutment was not firmly attached, the pickup process was repeated. Acrylic resin was added where needed and the prosthesis was adapted to the new design, turning concavities into convexities to allow patient hygiene. Before delivering the prosthesis, a second stone cast was made using the same technique and materials. This cast was called Cast 2 (C2) and represented the position of the abutments in the prosthesis or the prosthesis itself (Fig. 4). For didactical reasons, the intraoral position of the implants was called Cast 3 (C3), meaning the in vivo position of the implants in the patients. Given the experimental model, a first comparison was made on the day of surgery and immediate loading (Time 0). Thus, the second surgeon measured the seating, fit and tension between the casts (C1, C2 and C3) and the assistant recorded the results (Table 2).
Four clinical methods were used to assess prosthesis fit, beginning with the most obvious method and continuing with the more detailed ones. That way, if a misfit was clearly recognized at any point, other methods were not necessary, but if there was not enough information to clearly recognize a misfit, the following method was used. The methods used, following previous revisions made by Kan et al.,26Kan JY, Rungcharassaeng K, Bohsali K, Goodacre CJ, Lang BR. Clinical methods for evaluating implant framework fit. → J Prosthet Dent. 1999 Jan;81(1):7–13 were, in order of accuracy: the alternate pressure technique (securing the prosthesis without screws and applying pressure alternately from 1 thumb to another to determine if rocking movement occurs); direct vision and tactile sensation (magnifying view and an explorer used to check misfit at the platform level); the 1 screw test proposed by Jemt (1 screw tightened at 1 terminal abutment and discrepancies observed at the other abutments);27Jemt T. Failures and complications in 391 consecutively inserted fixed prostheses supported by Brånemark implants in the edentulous jaws: a study of treatment from the time of prosthesis placement to the first annual checkup. → Int J Oral Maxillofac Implants. 1991 Fall;6(3):270–6. and the screw resistance test proposed also by Jemt (with a supposed acceptable misfit interface of 150 μ and a 300 μ distance between most prosthetic screw threads, a maximum of a half turn [180º] is allowed to completely seat the screw and achieve a torque of 10–15 N cm2).28Jemt T. Failures and complications in 391 consecutively inserted fixed prostheses supported by Brånemark implants in the edentulous jaws: a study of treatment from the time of prosthesis placement to the first annual checkup. → Int J Oral Maxillofac Implants. 1991 Fall;6(3):270–6.
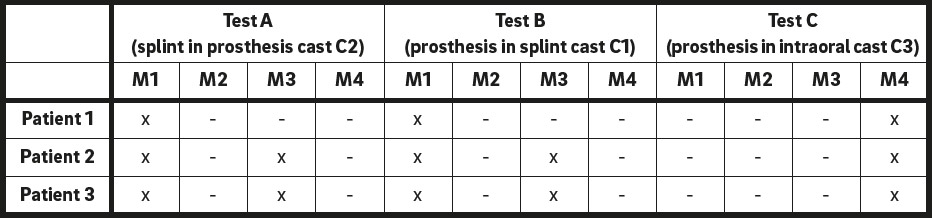
These 4 methods were used between casts as shown in Table 2. To begin with, the first test (Test A) entailed assessing the fit of the splint, passively made of impression posts, in the prosthesis cast (splint in C2), meaning the relationship between initial implant position and abutment position in the prosthesis (Fig. 5). To continue with, the second test (Test B) entailed assessing the fit of the prosthesis in the splint cast (prosthesis in C1), meaning again the relationship between abutment position in the prosthesis and initial implant position. To end with, the third test (Test C) entailed assessing the fit of the prosthesis in the intraoral cast during installation of the interim prosthesis (prosthesis in C3; Figs. 6 & 7). Finding a nonpassive fit is the pillar around which the results obtained after the healing period are discussed.

Method 1 (M1): alternate pressure technique. Method 2 (M2): direct vision and tactile sensation.
Method 3 (M3): 1 screw test. Method 4 (M4): screw resistance test.

Method 1 (M1): alternate pressure technique. Method 2 (M2): direct vision and tactile sensation. Method 3 (M3): 1 screw test. Method 4 (M4): screw resistance test.
Method 1 (M1): alternate pressure technique. Method 2 (M2): direct vision and tactile sensation. Method 3 (M3): 1 screw test. Method 4 (M4): screw resistance test.
Immediate radiographic control consisted of a digital panoramic radiograph to establish the correct fit of the abutments and initial bone crest around implants. A soft diet and careful hygiene were prescribed. Chlorhexidine rinses were prescribed until suture removal. Clinical controls took place at 1, 2, 4, 6 and 8 weeks. Hygiene, occlusion and prosthetic integrity were assessed at every appointment. Sutures were removed at 2 weeks without removing the prosthesis. Sutures remaining unreachable were left to resorb. A final panoramic radiograph was taken to assess the bone crest around the implants and osseointegration at 8 weeks. At this point, the prosthesis was removed and osseointegration was measured by the first surgeon as the assistant recorded the ISQ values. New tests at this time (Time 1) were performed to compare changes (Table 3). To begin with, the first test (Test D) entailed assessing the fit of the splint in the intraoral cast (splint in C3), meaning the possible position change of the implants through the healing period. To continue with, the second test (Test E) entailed assessing the fit of the prosthesis in the intraoral cast (prosthesis in C3), meaning the possible passive fit acquired through the healing period. To end with, the third test (Test F) entailed assessing the fit of the prosthesis in its initial cast (prosthesis in C2), meaning the possible change of the whole prosthetic structure (acrylic resin deformation and/ or abutment movement inside) during the healing period. Finding a new passive fit implied that some element had modified its position or had suffered some deformation to dissipate the stress previously created by a nonpassive prosthesis installed at Time 0.
Moreover, scan bodies were used again to take a digital impression of the implant position at Time 1. Digital information was processed in a software program to determine possible variations of implant position and produce a virtual representation of any variation.
-
-
Fig. 5
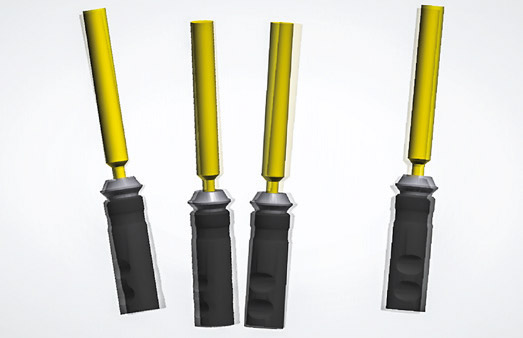
Test A: Using the 1 screw test, the gap confirms the difference between initial implant position and abutments within the prosthesis.
-

-
Fig. 6
Test C: installing prosthesis to assess passiveness.
-

-
Fig. 7
Test C: installing prosthesis to assess passiveness.
-
-
Fig. 8
Digital merging of initial and final implant position. One implant was used as reference to merge scans and determine discrepancies between the others.
Results
The initial results corresponded to Time 0. Implant stability measured with Osstell indicated values of 60 ISQ or more both in the buccolingual and mesiodistal aspects. Fitting tests were recorded with an “x” if fit failed to be passive according to the test, with a “-” if the test was not done or if the result was not conclusive, and with an “OK” if fit proved to be passive according to the test. For Tests A and B, the alternate finger test was more than conclusive to show a misfit in all of the patients. This was also validated with the 1 screw test. Misfit meant that the process of manufacturing the prosthesis had altered the position of the abutments in relationship to the implant position. The initial implant position and prosthesis did not coincide properly in all of the cases, and so resin contraction was assumed to have influenced the abutment position. For Test C, the only conclusive method was the screw resistance test, as soft tissue interfered with other assessment methods. As assumed in Tests A and B, the prosthesis installed failed to have a passive fit. More than a half turn was needed to seat the abutment and reach the desired 15 N cm2. However, panoramic radiographs confirmed the proper seating of the prosthesis.
Later results corresponded to Time 1, which was at 8 weeks in all of the patients. Implant stability was assessed by torque verification and ISQ values in the same way that they were done at Time 0. For Test D, the alternate finger test was conclusive in only 1 patient, while more methods had to be used for the rest. Nevertheless, all of the patients showed a misfit between the splint and the intraoral cast. This meant that the initial position of the implants had changed from Time 0 to Time 1. For Test E, all of the methods succeeded in proving a correct fit of the prosthesis in the intraoral cast. This meant that the nonpassive prostheses installed at Time 0 had turned into passive prostheses at Time 1 in all of the patients as assessed by the 4 clinical methods described. For Test F, all of the methods succeeded in proving a correct fit of the prosthesis in C2 (original prosthesis cast). This meant that the prosthetic structure had not changed at all from Time 0 to Time 1. Thus, the prosthesis was not assumed to participate in the stress releasing process. Moreover, software was used to superimpose the implant position recorded at Time 0 and at Time 1. This process helped to confirm variation of implant position and helped to visualize the degree of variation between implant positions (Fig. 8).
In one patient, the prosthesis had to be removed within the first week to repair a fissure seen at the lingual aspect of the prosthesis, in order to prevent future fracture. To make the most of the situation, the patient agreed to extra tests at this particular time. For the purpose of this study, and out of established protocol, the same tests as planned for Time 1 were performed at that moment (Table 4). First (Test G), the splint failed to prove passivity in the intraoral cast with the second and third methods. This meant that the implant position had already changed within the first 7 days. Second (Test H), the prosthesis almost succeeded in proving total passivity in the intraoral cast, as it showed good results with the first 3 methods, but remained with a slight tension evident during the fourth method (screw resistance test). This meant that the prosthesis had improved its fit considerably within the first 7 days, but still showed a residual strain. Third (Test I), all of the methods succeeded in proving a correct fit of the prosthesis in C2 (original prosthesis cast). This meant that the prosthetic structure, specifically the abutment position, had not changed within the first 7 days.
Discussion
The collected data showed that passivity was not a decisive element to determine successful osseointegration of implants supporting a fixed immediately loaded prosthesis. The chairside method used to transform a complete denture into a hybrid prosthesis (pickup technique) resulted in a nonpassive structure that, for the purpose of this study, was installed provoking an amount of stress between the implants and abutments. Osseointegration was achieved in all 15 implants without showing bone loss or reduced stability after 8 weeks. Tension at the seating of the prosthesis disappeared without modification of the prosthetic structure. Implants showed variation in their position within 8 weeks, recorded with splints, casts and digital images. This was associated with stress release, as suggested by Gallucci et al.,29Gallucci GO, Bernard JP, Bertosa M, Belser UC. Immediate loading with fixed screw-retained provisional restorations in edentulous jaws: the pickup technique. → Int J Oral Maxillofac Implants. 2004 Jul–Aug;19(4):524–33. and could also be seen in one patient at an early stage. Implant movement was thought to occur during the first stage of the healing period, agreeing with Gallucci et al.’s findings30Gallucci GO, Bernard JP, Bertosa M, Belser UC. Immediate loading with fixed screw-retained provisional restorations in edentulous jaws: the pickup technique. → Int J Oral Maxillofac Implants. 2004 Jul–Aug;19(4):524–33. at the 2-week screw loosening. Although digital images were not used to measure (in degrees or millimeters) implant variations, they helped visualize said movement or modification in implant position. In addition, no parameters of induced strain were considered. The literature suggests that there is a critical threshold of micromotion above which fibrous encapsulation prevails over osseointegration.31Szmuker-Moncler S, Salama H, Reingewirtz Y, Dubruille JH. Timing of loading and effect on micromotion on bone-dental implant interface: a review of experimental literature. → J Biomed Mater Res. 1998 Summer;43(2):192–203. Having said that, extreme precaution has to be taken regarding the amount of tension or level of stress generated by these procedures. To reduce the influence of bone type, only interforaminal areas of the jaw were included. However, many variables can have different influences on bone adaptation under stress and loading protocols.32Brunski JB. In vivo bone response to biomechanical loading at the bone/ dental-implant interface. → Adv Dent Res. 1999 Jun;13:99–119.
As this was a preliminary study, the main limitations were the number of patients treated with this particular protocol. Although the phenomenon reported on has been observed in many patients after immediate loading protocols, more controlled cases need to be assessed. Given the foundations of these results and tests, future studies should consist of digital impressions only, in order to reduce clinical time and eliminate modifying factors such as polymerization, stone setting and clinical discrepancies between researchers.
Conclusion
A prosthesis delivered for immediate loading protocols involving implant placement in the edentulous mandible can induce a certain level of stress if passive fit is not achieved, without resulting in a negative influence on osseointegration. Excessive stress should never compromise biomechanical aspects or jeopardize bone healing around implants.
Prosthetic procedures to manufacture final restorations should rely on abutment position placed in the interim prosthesis rather than on initial implant position, as freshly placed implants will adapt to the established abutment position and will not maintain their initial position. This phenomenon can be clinically (not histologically) compared to the bone adaptation that takes place in orthodontic treatment, where a force induces stress to move a tooth to a desired position. In a similar way, the prosthesis induces stress in the implant–abutment interface, and this provokes the recently placed implants to adapt to said induced position at an early stage of the healing period. Additionally, the force induced must be within certain limits, still unknown, such as recommended with orthodontic treatment.
Competing interests
The authors declare they have no competing interests.
Acknowledgments
The authors wish to thank dental technician Thomas Graber and the EPS Lab for their support in terms of implant components and CAD/ CAM technology.
Interview
with Nicolás Agustín Rubio
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 17. | ↑ | Papaspyridakos P, Chen CJ, Chuang SK, Weber HP. Implant loading protocols for edentulous patients with fixed prostheses: a systematic review and meta-analysis. → Int J Oral Maxillofac Implants. 2014;29 Suppl:256–70. |
| 2, 7. | ↑ | Kapos T, Ashy LM, Gallucci GO, Weber HP, Wismeijer D. Computer-aided design and computer-assisted manufacturing in prosthetic implant dentistry. → Int J Oral Maxillofac Implants. 2009;24 Suppl:110–7. |
| 3, 8. | ↑ | Balshi SF, Wolfinger GJ, Balshi TJ. Surgical planning and prosthesis construction using computer technology and medical imaging for immediate loading of implants in the pterygomaxillary region. → Int J Periodontics Restorative Dent. 2006 Jun;26(3):239–47. |
| 4, 9. | ↑ | Komiyama A, Petterson A, Huitin M, Näsström K, Kinge B. Virtually planned and template-guided implant surgery: an experimental model matching approach. → Clin Oral Implants Res. 2011 Mar;22(3):308–13. |
| 5. | ↑ | Wismeijer D, Casentini P, Gallucci G, Chiapasco M. ITI treatment guide, Vol. 4: loading protocols in implant dentistry: edentulous patients. → Berlin: Quintessence. 2010. 248 p. |
| 6. | ↑ | Esposito M, Grusovin MG, Willings M, Coulthard P, Worthington HV. Interventions for replacing missing teeth: different times for loading dental implants. → Cochrane Database Syst Rev. 2007 Apr 18;(2):CD003878. |
| 10. | ↑ | Valente F, Schiroli G, Sbrenna A. Accuracy of computer-aided oral implant surgery: a clinical and radiographic study. → Int J Oral Maxillofac Implants. 2009 Mar–Apr;24(2):234–42. |
| 11. | ↑ | Geng W, Liu C, Su Y, Li J, Zhou J. Accuracy of different types of computer-aided design/computer-aided manufacturing surgical guides for dental implant placement. → Int J Clin Exp Med. 2015 Jun;8(6):8442–9. |
| 12. | ↑ | Degidi MI, Nardi D, Sighinolfi G, Piattelli A. Immediate rehabilitation of the edentulous mandible using Ankylos SynCone telescopic copings and intraoral welding: a pilot study. → Int J Periodontics Restorative Dent. 2012 Dec;32(6):189–94. |
| 13. | ↑ | Yilmaz B, Suarez C, McGlumphy E. Correction of misfit in a maxillary immediate metal-resin implant-fixed complete prosthesis placed with flapless surgery on four implants. → Int J Oral Maxillofac Implants. 2011 Sep–Oct;26(5):23–8. |
| 14. | ↑ | Miguel-Figuero J, Fernandez-Jordan Celorio J. Modificacion de la tecnica all-on-4: protesis fija inmediata implantosoportada sin la intervencion del laboratorio de protesis (caso clinico) [Modification of the All-on-4 technique: fixed, immediate and complete rehabilitation with dental implants without participation of the dental laboratory (clinical case)]. → RCOE. 2006 Mar–Apr;11(2). Spanish. |
| 15. | ↑ | Levin BP. A team approach to cost-effective, full-arch immediate loading. → Compend Contin Educ Dent. 2013 Jul–Aug;34(7):530–2. |
| 16. | ↑ | Karl M, Graef F, Wichmann M, Krafft T. Passivity of fit of CAD/CAM and copy-milled frameworks, veneered frameworks, and anatomically contoured, zirconia ceramic, implant-supported fixed prostheses. → J Prosthet Dent. 2012 Apr;107(4):232–8. |
| 18, 29, 30. | ↑ | Gallucci GO, Bernard JP, Bertosa M, Belser UC. Immediate loading with fixed screw-retained provisional restorations in edentulous jaws: the pickup technique. → Int J Oral Maxillofac Implants. 2004 Jul–Aug;19(4):524–33. |
| 19. | ↑ | Karl M, Taylor TD. Bone adaptation induced by non-passively fitting implant superstructures: a randomized clinical trial. → Int J Oral Maxillofac Implants. 2016 Mar–Apr;31(2):369–75. |
| 20, 31. | ↑ | Szmuker-Moncler S, Salama H, Reingewirtz Y, Dubruille JH. Timing of loading and effect on micromotion on bone-dental implant interface: a review of experimental literature. → J Biomed Mater Res. 1998 Summer;43(2):192–203. |
| 21. | ↑ | Lekholm U, Zarb GA. Patient selection and preparation. In: Brånemark PI, Zarb GA, Albrektsson T, editors. Tissue-integrated prostheses: osseointegration in clinical dentistry. → Chicago: Quintessence; 1985. p. 199–209. |
| 22. | ↑ | Galante JM, Rubio NA. Surgical approach for the fully edentulous mandible. → Clin Oral Implants Res. 2014;25(10):467. |
| 23. | ↑ | De Fabbro M, Bellini CM, Romeo D, Francetti L. Tilted implants for the rehabilitation of edentulous jaws: a systematic review. → Clin Implant Dent Relat Res. 2012 Aug;14(4):612–21. |
| 24. | ↑ | Gallucci GO, Benic GI, Eckert SE, Papaspyridakos P, Schimmel M, Schrott A, Weber HP. Consensus statements and clinical recommendations for implant loading protocols. → Int J Oral Maxillofac Implants. 2014;29 Suppl:287–90. |
| 25. | ↑ | Wee AG, Aquilino SA, Schneider RL. Strategies to achieve fit in implant prosthodontics: a review of the literature. → Int J Prosthodont. 1999 Mar–Apr;12(2):167–78. |
| 26. | ↑ | Kan JY, Rungcharassaeng K, Bohsali K, Goodacre CJ, Lang BR. Clinical methods for evaluating implant framework fit. → J Prosthet Dent. 1999 Jan;81(1):7–13 |
| 27, 28. | ↑ | Jemt T. Failures and complications in 391 consecutively inserted fixed prostheses supported by Brånemark implants in the edentulous jaws: a study of treatment from the time of prosthesis placement to the first annual checkup. → Int J Oral Maxillofac Implants. 1991 Fall;6(3):270–6. |
| 32. | ↑ | Brunski JB. In vivo bone response to biomechanical loading at the bone/ dental-implant interface. → Adv Dent Res. 1999 Jun;13:99–119. |





Leave a Reply
Be the First to Comment!