Low implant insertion torque allows minimal bone loss: A multicenter 2-year prospective study
July 6, 2018 / Categories: Digital Dentistry, Implant Dentistry

Man, Yi
Xu, Xin
Wang, Zuolin
Moses, Ofer
Zhonghao, Liu
Abstract
Objective
The aim of this multicenter prospective study was to evaluate the survival rate of implants after insertion using low torque (< 35 N cm), by recording measurements from resonance frequency analysis (RFA), probing pocket depths and changes in interproximal crestal bone level.
Materials and methods
This multicenter prospective clinical study was performed in partially edentulous subjects. The patients treated in the study received 1–4 SPI implants (Alpha-Bio Tec, Petah Tikva, Israel), which were loaded 4 months after implantation. Measurements of torque and RFA were recorded immediately after implant insertion. New RFA measurements were taken at the time of implant exposure surgery, prior to connection of the healing abutments. Baseline measurements of bone level were taken both directly and radiographically immediately after insertion and were compared with measurements taken during the 2-year follow-up period.
Results
Of 88 treated subjects, 83 completed the 2-year follow-up. Of 137 implants, 5 were lost. The survival rate after 2 years of follow-up was 96.5% and the mean marginal bone loss was 0.531 mm. The mean measurement for RFA at the time of implantation was 74.92 and this increased to 76.26 prior to insertion of the prostheses.
Conclusion
Within the limits of the study, implants inserted with low torque (< 35 N cm), displayed high survival rates with high RFA scores and minimal bone loss at the 2-year mark after implantation.
Keywords
Implants; bone loss; RFA; resonance frequency analysis.
Introduction
Nowadays, dental implants are widely used as a treatment for fully and partially edentulous patients, and the survival rate has been reported to be high.1French D, Larjava H, Ofec R. Retrospective cohort study of 4591 Straumann implants in private practice setting, with up to 10-year follow-up. Part 1: multivariate survival analysis. → Clin Oral Implants Res. 2015 Nov;26(11):1345–54.2Andersson B, Bergenblock S, Furst B, Jemt T. Long-term function of single-implant restorations: a 17- to 19-year follow-up study on implant infraposition related to the shape of the face and patients’ satisfaction. → Clin Implant Dent Relat Res. 2013 Aug;15(4):471–80. However, certain risk factors may predispose to an increased risk of implant failure and a lower success rate. Risk factors for implant failure can be divided mainly into 2 groups.3Cakarer S, Selvi F, Can T, Kirli I, Palancioglu A, Keskin B, Yaltirik M, Keskin C. Investigation of the risk factors associated with the survival rate of dental implants. → Implant Dent. 2014 Jun;23(3):328–33. The first group of risk factors includes surgical technique, retention technique, the primary stability of the implant, and variables affecting the implant prosthesis, such as the length, diameter and location of the implant. The second group involves patient-related factors, such as smoking, diabetes, alcohol abuse, oral hygiene habits and a history of periodontitis. Controversy remains, however, concerning the linkage between certain risk factors and dental implant failure.4Cakarer S, Selvi F, Can T, Kirli I, Palancioglu A, Keskin B, Yaltirik M, Keskin C. Investigation of the risk factors associated with the survival rate of dental implants. → Implant Dent. 2014 Jun;23(3):328–33.5Derks J, Schaller D, Hakansson J, Wennstrom JL, Tomasi C, Berglundh T. Effectiveness of implant therapy analyzed in a Swedish population: prevalence of peri-implantitis. → J Dent Res. 2016 Jan;95(1):43–9.6Hasegawa T, Kawabata S, Takeda D, Iwata E, Saito I, Arimoto S, Komori T. Survival of Brånemark System Mk III implants and analysis of risk factors associated with implant failure. → Int J Oral Maxillofac Surg. 2017 Feb;46(2):267–73.7Pommer B, Hof M, Fadler A, Gahleitner A, Watzek G, Watzak G. Primary implant stability in the atrophic sinus floor of human cadaver maxillae: impact of residual ridge height, bone density, and implant diameter. → Clin Oral Implants Res. 2014 Feb;25(2):e109–13.
Dental implant success may be characterized by initial and long-term stability of the implant and healthy periimplant hard and soft tissue.8Mombelli A, Muller N, Cionca N. The epidemiology of peri-implantitis. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:67–76. It is widely accepted that marginal bone loss of approximately 1.0 mm during the first year after prosthetic loading and subsequent annual bone loss not exceeding 0.2 mm are consistent with successful treatment.9Laurell L, Lundgren D. Marginal bone level changes at dental implants after 5 years in function: a meta-analysis. → Clin Implant Dent Relat Res. 2011 Mar;13(1):19–28.10Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: a systematic review. → J Dent Res. 2012 Mar;91(3): 242–8.
A wide variety of techniques have been used for measuring implant stability at various clinically relevant reference points in time. The techniques currently most often used to measure stability are insertion torque, Periotest and resonance frequency analysis (RFA).11Gómez-Polo M, Ortega R, Gómez-Polo C, Martín C, Celemín A, Del Río J. Does length, diameter, or bone quality affect primary and secondary stability in self-tapping dental implants? → J Oral Maxillofac Surg. 2016 Jul;74(7):1344–53. While clinically useful, insertion torque is limited to implant insertion and thus cannot be used to determine secondary stability. Conversely, RFA is a noninvasive and widely used method to quantify implant stability at any stage during implant treatment and the follow-up period.12Manzano-Moreno FJ, Herrera-Briones FJ, Bassam T, Vallecillo-Capilla MF, Reyes-Botella C. Factors affecting dental implant stability measured using the Ostell Mentor device: a systematic review. → Implant Dent. 2015 Oct;24(5):565–77.13Meredith N. Assessment of implant stability as a prognostic determinant. → Int J Prosthodont. 1998 Sep–Oct;11(5):491–501. The RFA technique for measuring implant stability was developed by Meredith and co-workers almost 30 years ago and is commercially available as the Osstell device.14Meredith N. Assessment of implant stability as a prognostic determinant. → Int J Prosthodont. 1998 Sep–Oct;11(5):491–501. A sensor (SmartPeg) is mounted on top of the implant and the sensor is then brought to vibration by gently moving it with magnetic pulses. The sensor will vibrate for a short while and then stop. If the implant stability (stiffness of the bone–implant interface) increases, then the vibration frequency of the sensor will increase. Resistance to vibration of the transducer by the surrounding bone is registered by a small computer device and measured in hertz. Hertz are converted to ISQ (Implant Stability Quotient) values ranging from 1 to 100; the higher the ISQ, the greater the implant stability. This method is known as RFA.15Alsaadi G, Quirynen M, Michiels K, Jacobs R, van Steenberghe D. A biomechanical assessment of the relation between the oral implant stability at insertion and subjective bone quality assessment. → J Clin Periodontol. 2007 Apr;34(4):359–66.
Dentists feel better whenever an implant is inserted using high torque (< 35 N cm). There are some publications claiming that this is an ultimate demand for immediate loading. However, using low insertion torques yields favorable survival rates with optimal marginal bone levels compared with the accepted norm.16Norton MR. The influence of low insertion torque on primary stability, implant survival, and maintenance of marginal bone levels: a closed-cohort prospective study. → Int J Oral Maxillofac Implants. 2017 Jul–Aug;32(4):849–57.
In 2004, the SPI implant system (Alpha-Bio Tec, Petah Tikva, Israel) was introduced to the dental market. The implant has an internal hexagon connection and is available in several lengths and diameters. The implant surface is sandblasted and acid-etched (NanoTec). Its tapered core and sharp threads result in firm bone grip, which enables stable insertion and high primary stability.
The aim of this multicenter prospective study was to evaluate the survival rate of implants after insertion using low torque, by means of recording measurements from RFA, probing pocket depths and monitoring changes in the interproximal crestal bone level.
Materials and methods
Study design
This prospective study was designed as a controlled multicenter clinical trial, and it involved the participation of the following 4 medical centers in China: West China Hospital of Stomatology, Chengdu; Stomatology Hospital of Shandong University, Jinan; Yantai Stomatological Hospital, Yantai; and Affiliated Stomatology Hospital of Tongji University, Shanghai.
The study was conducted in accordance with the 1964 Declaration of Helsinki (and all subsequent amendments) and Good Clinical Practice (ISO 14155:2003). It was approved by the ethics committee of Sichuan University and was submitted to the other centers for approval prior to commencement of the study. The study was registered at www.clinicaltrials. gov (registration No. NCT02367261).
Subjects and implants
Subjects were selected according to the following predetermined inclusion and exclusion criteria:
Inclusion criteria
- Men and women over the age of 18 years who were in need of 1–4 implants.
- Patients able to understand the requirements of the study and willing and able to comply with its instructions and schedules.
- Patients who provided written informed consent to participate in the study prior to any study procedure.
- Patients in good general health in the opinion of the principal investigator, as determined by the medical history and oral examination.
Exclusion criteria
- Immediately loaded implants.
- Patients requiring bone augmentation.
- Patients receiving treatment with bisphosphonates.
- Patients receiving treatment with anticonvulsant drugs or anticoagulant drugs (international normalized ratio under 1.8).
- Patients with untreated periodontal disease and poor oral hygiene.
- Patients with a history of alcohol, narcotic or other drug abuse.
- Patients undergoing steroid therapy.
- Patients receiving radiotherapy, chemotherapy or any other immunosuppressive treatment, or who had received radiotherapy in the last 5 years—patients who had received radiotherapy to the head and neck region at any time in the past.
- Patients with metabolic bone disorders.
- Patients with uncontrolled bleeding disorders, such as hemophilia, thrombocytopenia and granulocytopenia.
- Patients with degenerative diseases.
- Patients with osteoradionecrosis.
- Patients with renal failure.
- Organ transplant recipients.
- HIV-positive patients.
- Patients with malignant diseases.
- Patients with diseases that compromise the immune system.
- Patients with uncontrolled diabetes mellitus (hemoglobin A1c level above 6.5%).
- Patients with psychotic diseases.
- Patients with hypersensitivity to any of the components of the implant in general or to titanium in particular.
- Pregnant or lactating women.
- Lack of patient cooperation.
- Patients with uncontrolled endocrine diseases.
- Patients with any systemic condition that precluded surgical procedures.
- Patients with parafunctional habits, such as bruxism.
- Patients with temporomandibular joint disease.
- Patients with various pathologies of the oral mucosa, such as benign mucous membrane pemphigoid, desquamative gingivitis, erosive lichen planus, oral malignancy and bullous erosive diseases of the oral mucosa.
- Patients who required flapless procedures.
- Patients who smoke over 10 cigarettes a day.
The most important inclusion criteria were subjects over 18 years old who had good general and dental health. The most important exclusion criteria were as follows: immediate implantation, smokers of over 10 cigarettes a day, alcohol abuse, various medical conditions as specified by the clinician, and pregnant or lactating women.
Surgical protocol
All subjects received 1–4 SPI implants. Using a delayed implant approach, all implants were inserted 4 months after tooth extraction. The implants were 3.3–5.0 mm in diameter and 8.0–13.0 mm in length. Implant surgeries were performed under local anesthesia and followed standard surgical techniques. After flap elevation, the implant bed was prepared using medical-grade stainless-steel drills (Alpha-Bio Tec) with progressively increasing diameter, in accordance with the drilling protocol (Table 1). The implant insertion torque was measured with a physiodispenser machine (NSK, Stevenage, U.K.; Nouvag, Goldach, Switzerland), which was placed at the level of the crestal bone. RFA was measured immediately after implant placement using an Osstell device (Osstell, Gothenburg, Sweden). A periapical radiograph was taken as a baseline, using a paralleling technique.
Implants were exposed 4 months after implantation, and RFA measurements were taken immediately prior to connection of the healing abutments. The final prostheses were fabricated 6 months post-implantation. The occlusion of the restorations was adjusted, and oral hygiene was reinforced with the patients. Patients were recalled at intervals of 12 and 24 months after implant insertion surgery in order to evaluate the periimplant bone level and the status of the prosthetic work.
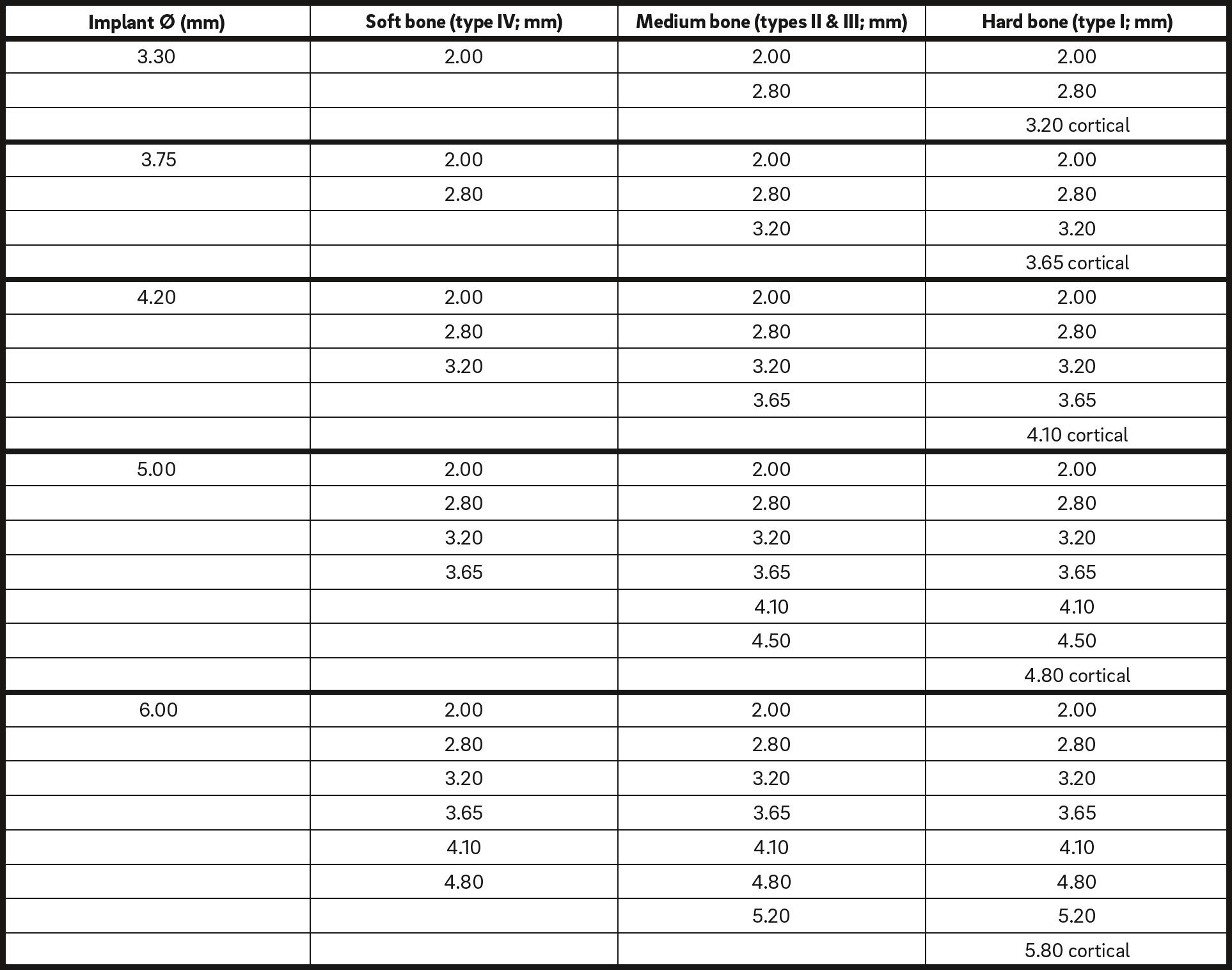
Cortical = Drill through cortical plate
The drilling protocol used in the study.
Implant survival
Survival of implants was defined as those implants that were still in place 24 months after placement and that met the criteria set by Buser et al.: the absence of persistent subjective complaints (e.g., pain, foreign-body sensation and dysesthesia), the absence of periimplant infection with suppuration, the absence of mobility, the absence of a persistent periimplant radiolucency, and the possibility of restoration.17Buser D, Weber HP, Lang NP. Tissue integration of non-submerged implants. 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants. → Clin Oral Implants Res. 1990 Dec;1(1):33–40.
Bone level changes
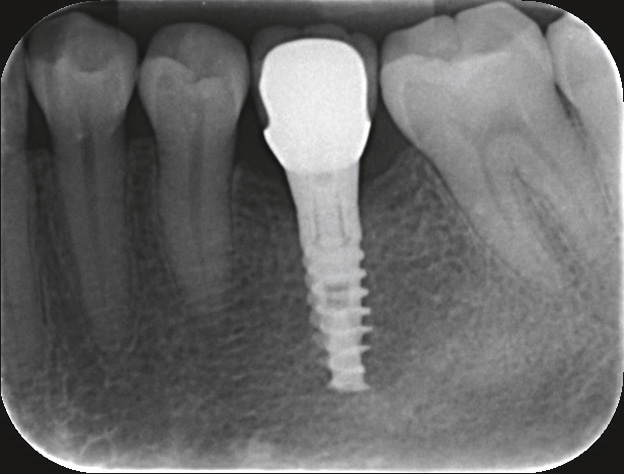
Periapical radiographs with standardized settings were taken as a baseline at the time of implant surgery and were retaken at the time of abutment connection and at 12 and 24 months postsurgery (Figs. 1–3). Digital images were analyzed using ImageJ open software (Version 1.33, National Institutes of Health, Bethesda, Md, U.S.) by an independent reader who was blind to the study material. The implant length was used as a reference measurement, and bone level was therefore defined as the distance from the reference point to the first radiographic bone-to-implant contact; changes in mesial and distal bone levels in this region were considered to be remodeling. Mesial and distal measurements were recorded and the mean of these 2 values was used.
Statistical analysis
Bone level was calculated as the average of the mesial and distal levels at 3 time intervals (baseline and 12 and 24 months later). Repeated measures general linear models with Bonferroni
adjustment for multiple comparisons were used to assess the differences between the 3 time intervals. A similar analysis was performed for pocket depths in 4 locations (buccal, lingual, distal and mesial) at 3 time intervals (6, 12 and 24 months). P < 0.05 was considered statistically significant. All analyses were performed with SPSS (Version 24, IBM Corp, Armonk, N.Y., U.S.). The analysis set was as complete as possible and was as close as possible to the intention-to-treat ideal of including all subjects who had received the therapy at least once.
-

-
Fig. 1
SPI implant immediately after implantation surgery.
-
-
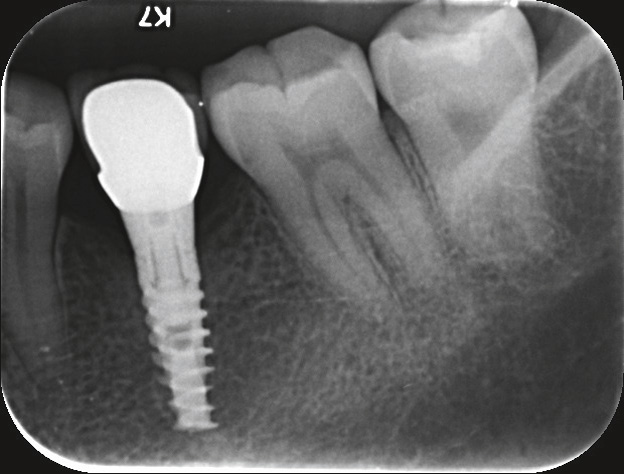
Fig. 2
SPI implant 1 year after implantation surgery.
-
-
Fig. 3
SPI implant 2 years after implantation surgery.

Insertion Torque During the Implantation Surgery.
Results
Eighty-eight patients out of 90 were included in the study. Of the 88 treated subjects, 83 participated up to the 24-month follow-up mark (2 patients had dropped out and 3 had implant failure diagnosed). The study group consisted of 47.73% men and 52.27% women and the mean age of the participants was 47.45 ± 11.15 years. The majority did not smoke at all, and 22% of the subjects smoked less than 10 cigarettes a day.
The average measurement for insertion torque was 33.250 ± 9.913 N cm (Table 2). Of 137 implants, 132 survived. The calculated survival rate of the implants after 2 years was 96.5%. Five implants were lost during the first year of the study, while no implant was lost during the second year.
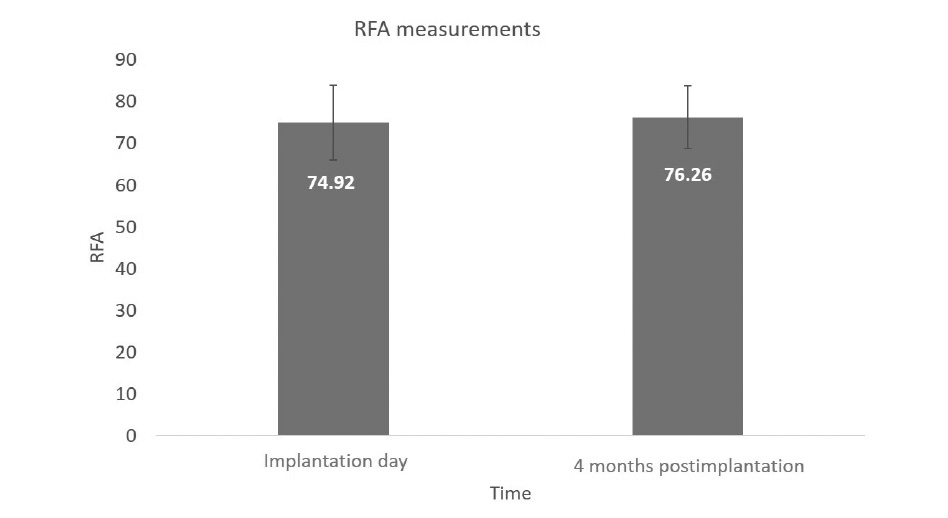
RFA measurements were taken after implant placement and retaken immediately prior to connection of the prostheses (Fig. 4). The mean immediate measurement for RFA was 74.92 ± 8.93, while analysis at the time of implant exposure 4 months later yielded a 76.26 ± 7.42 mean score.
Changes in bone level and soft tissue
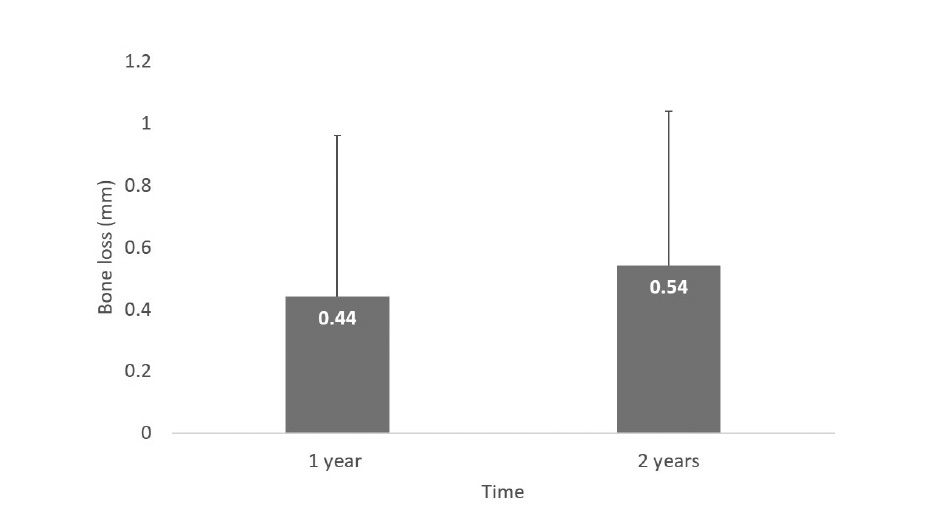
The mean change in marginal bone level at the 1-year follow-up was 0.44 ± 0.52 mm and the mean change at the 2-year follow-up was 0.54 ± 0.50 mm (Fig. 5). The average bone loss between the 1- and 2-year follow-up marks was calculated and found to be 0.105 mm.
Soft-tissue changes were monitored by probing pocket depths at 4 locations: mesial, distal, buccal and lingual (Fig. 6). The probing depths before connection of the final restoration averaged 1.04 ± 1.08 mm mesially, 0.91 ± 0.93 mm buccally, 1.04 ± 1.42 mm distally and 0.86 ± 0.88 mm lingually. At 12 months postsurgery, the average probing depths were 2.40 ± 0.80 mm, 2.08 ± 0.82 mm, 2.30 ± 0.85 mm and 2.10 ± 0.80 mm, respectively. At 24 months postsurgery, the average probing depths were 2.60 ± 1.05 mm, 2.10 ± 0.98 mm, 2.55 ± 1.11 mm and 2.33 ± 1.20 mm, respectively.
Discussion
This was a controlled multicenter prospective study that evaluated performance of the SPI implant system with 24 months of follow-up. The study demonstrated a stable survival rate of 96.5% after 1 and 2 years of follow-up. This finding correlates with previously performed studies by Artzi et al.18Artzi Z, Kohen J, Carmeli G, Karmon B, Lor A, Ormianer Z. The efficacy of full-arch immediately restored implant-supported reconstructions in extraction and healed sites: a 36-month retrospective evaluation. → Int J Oral Maxillofac Implants. 2010 Mar–Apr;25(2):329–35. and Ormianer et al.19Ormianer Z, Duda M, Block J, Matalon S. One- and two-piece implants placed in the same patients: clinical outcomes after 5 years of function. → Int J Prosthodont. 2015 Nov–Dec;29(6):608–10. that showed similar implant survival rates of 96.95% and 96.6%, respectively, over longer follow-up periods.
-
-
Fig. 4
RFA measurements immediately after implantation and during reopening surgery.
-
-
Fig. 5
Changes in bone loss over time.
According to Chrcanovic et al., failures of dental implants can be subdivided into early and late failures, depending on whether they occur either before/at abutment connection surgery (early) or after occlusal loading of a prosthetic restoration (late).20Chrcanovic BR, Kisch J, Albrektsson T, Wennerberg A. Factors influencing early dental implant failures. → J Dent Res. 2016 Aug;95(9):995–1002. Failures in each of these 2 distinct periods may be associated with different factors. Early failure of an implant results from an inability to establish intimate bone-to-implant contact. Based on our data, the excellent stability and integration of SPI implants was evident within 4 months after implantation (before connection surgery), even though the average insertion torque did not exceed 35 N cm.
The average insertion torque used in this multicenter study yielded quite a low degree of bone loss 2 years after implant insertion surgery. The drilling protocol used in the study resulted in a low insertion torque, accompanied by quite a high RFA reading. The torque in this study is much lower than the values reported in the literature.21De Santis D, Cucchi A, Rigoni G, Longhi C, Nocini PF. Relationship between primary stability and crestal bone loss of implants placed with high insertion torque: a 3-year prospective study. → Int J Oral Maxillofac Implants. 2016 Sep–Oct;31(5):1126–34.22Maló P, Lopes A, de Araújo Nobre M, Ferro A. Immediate function dental implants inserted with less than 30 N·cm of torque in full-arch maxillary rehabilitations using the All-on-4 concept: retrospective study. → Int J Oral Maxillofac Surg. 2018 May 4. pii: S0901-5027(18)30138-3. doi: 10.1016/j.ijom.2018.04.008. [Epub ahead of print] Lower insertion torques yield favorable survival rates with optimal marginal bone levels compared with the accepted norm.23Norton MR. The influence of low insertion torque on primary stability, implant survival, and maintenance of marginal bone levels: a closed-cohort prospective study. → Int J Oral Maxillofac Implants. 2017 Jul–Aug;32(4):849–57.24Norton MR. The influence of insertion torque on the survival of immediately placed and restored single-tooth implants. → Int J Oral Maxillofac Implants. 2011 Nov–Dec;26(6):1333–43. In contrast, studies in which high insertion torque was implemented demonstrated significant bone loss compared with low insertion torque.25De Santis D, Cucchi A, Rigoni G, Longhi C, Nocini PF. Relationship between primary stability and crestal bone loss of implants placed with high insertion torque: a 3-year prospective study. → Int J Oral Maxillofac Implants. 2016 Sep–Oct;31(5):1126–34.26Maló P, Lopes A, de Araújo Nobre M, Ferro A. Immediate function dental implants inserted with less than 30 N·cm of torque in full-arch maxillary rehabilitations using the All-on-4 concept: retrospective study. → Int J Oral Maxillofac Surg. 2018 May 4. pii: S0901-5027(18)30138-3. doi: 10.1016/j.ijom.2018.04.008. [Epub ahead of print]

Fig. 6
Changes in pocket depth at 4 locations over time.
In order to identify the risk factors associated with implant failure, a multivariate Cox model was formulated, and a rigorous model was selected that was constructed with statistically significant variables (P < 0.05) identified by bivariate Cox regression analysis. As a result, 2 variables were statistically associated with implant failure: tobacco use (P = 0.021) and alcohol use (P = 0.047). In the multivariate model, however, only tobacco use remained statistically associated with implant failure. These results are in accordance with those of several previous studies.27Chrcanovic BR, Kisch J, Albrektsson T, Wennerberg A. Factors influencing early dental implant failures. → J Dent Res. 2016 Aug;95(9):995–1002.28Hinode D, Tanabe S, Yokoyama M, Fujisawa K, Yamauchi E, Miyamoto Y. Influence of smoking on osseointegrated implant failure: a meta-analysis. → Clin Oral Implants Res. 2006 Aug;17(4):473–8.29Renvert S, Aghazadeh A, Hallstrom H, Persson GR. Factors related to peri-implantitis—a retrospective study. → Clin Oral Implants Res. 2014 Apr;25(4):522–9.
The mean amount of bone loss detected in the study was 0.426 mm at 1 year postimplantation and 0.531 mm at the 2-year mark. These results are in agreement with those of Artzi et al.30Artzi Z, Kohen J, Carmeli G, Karmon B, Lor A, Ormianer Z. The efficacy of full-arch immediately restored implant-supported reconstructions in extraction and healed sites: a 36-month retrospective evaluation. → Int J Oral Maxillofac Implants. 2010 Mar–Apr;25(2):329–35. and Ormianer et al.31Ormianer Z, Duda M, Block J, Matalon S. One- and two-piece implants placed in the same patients: clinical outcomes after 5 years of function. → Int J Prosthodont. 2015 Nov–Dec;29(6):608–10., which reported bone loss of 0.78 mm at the 3-year follow-up and 2.00 mm at the 9-year follow-up.
In addition, this minimal rate of bone loss was accompanied by improved RFA measurements, which may be associated with increased implant stability. The results suggest that the SPI implants allowed progressive biological integration with their bony housing.
Probing depths before connection of the final restoration connection were 1.04 ± 1.08 mm mesially, 0.91 ± 0.93 mm buccally, 1.04 ± 1.42 mm distally and 0.86 ± 0.88 mm lingually. At 1 year postimplantation, the probing depth measurements had increased to 2.40 ± 0.80 mm, 2.08 ± 0.82 mm, 2.30 ± 0.85 mm and 2.10 ± 0.80 mm, respectively, and at 2 years postimplantation, they had increased to 2.60 ± 1.05 mm, 2.10 ± 0.98 mm, 2.55 ± 1.11 mm and 2.33 ± 1.20 mm, respectively.
The analysis thus revealed that probing depths increased moderately compared with the baseline over the period of the study, and one may conclude that a more fastidious oral hygiene regimen was required by all subjects, especially with regard to the implant sites, even though bone loss measurements were not found to be higher at these sites. None of the implants were diagnosed with periimplant mucositis or periimplantitis, according to the diagnostic criteria,32Roos-Jansåker AM, Lindahl C, Renvert H, Renvert S. Nine- to fourteen-year follow-up of implant treatment. Part I: implant loss and associations to various factors. → J Clin Periodontol. 2006 Apr;33(4):283–9. such as bleeding on probing.
Conclusion
Within the limits of the study, implants inserted with low torque displayed high RFA scores, minimal bone loss and a high survival rate at 24 months after implantation.
Competing interests
The authors declare that there are no competing interests. Prof. Ofer Moses serves as an external medical adviser for Alpha-Bio Tec. The study was funded by Alpha-Bio Tec.
Interview
with Ofer Moses
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | French D, Larjava H, Ofec R. Retrospective cohort study of 4591 Straumann implants in private practice setting, with up to 10-year follow-up. Part 1: multivariate survival analysis. → Clin Oral Implants Res. 2015 Nov;26(11):1345–54. |
| 2. | ↑ | Andersson B, Bergenblock S, Furst B, Jemt T. Long-term function of single-implant restorations: a 17- to 19-year follow-up study on implant infraposition related to the shape of the face and patients’ satisfaction. → Clin Implant Dent Relat Res. 2013 Aug;15(4):471–80. |
| 3, 4. | ↑ | Cakarer S, Selvi F, Can T, Kirli I, Palancioglu A, Keskin B, Yaltirik M, Keskin C. Investigation of the risk factors associated with the survival rate of dental implants. → Implant Dent. 2014 Jun;23(3):328–33. |
| 5. | ↑ | Derks J, Schaller D, Hakansson J, Wennstrom JL, Tomasi C, Berglundh T. Effectiveness of implant therapy analyzed in a Swedish population: prevalence of peri-implantitis. → J Dent Res. 2016 Jan;95(1):43–9. |
| 6. | ↑ | Hasegawa T, Kawabata S, Takeda D, Iwata E, Saito I, Arimoto S, Komori T. Survival of Brånemark System Mk III implants and analysis of risk factors associated with implant failure. → Int J Oral Maxillofac Surg. 2017 Feb;46(2):267–73. |
| 7. | ↑ | Pommer B, Hof M, Fadler A, Gahleitner A, Watzek G, Watzak G. Primary implant stability in the atrophic sinus floor of human cadaver maxillae: impact of residual ridge height, bone density, and implant diameter. → Clin Oral Implants Res. 2014 Feb;25(2):e109–13. |
| 8. | ↑ | Mombelli A, Muller N, Cionca N. The epidemiology of peri-implantitis. → Clin Oral Implants Res. 2012 Oct;23 Suppl 6:67–76. |
| 9. | ↑ | Laurell L, Lundgren D. Marginal bone level changes at dental implants after 5 years in function: a meta-analysis. → Clin Implant Dent Relat Res. 2011 Mar;13(1):19–28. |
| 10. | ↑ | Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: a systematic review. → J Dent Res. 2012 Mar;91(3): 242–8. |
| 11. | ↑ | Gómez-Polo M, Ortega R, Gómez-Polo C, Martín C, Celemín A, Del Río J. Does length, diameter, or bone quality affect primary and secondary stability in self-tapping dental implants? → J Oral Maxillofac Surg. 2016 Jul;74(7):1344–53. |
| 12. | ↑ | Manzano-Moreno FJ, Herrera-Briones FJ, Bassam T, Vallecillo-Capilla MF, Reyes-Botella C. Factors affecting dental implant stability measured using the Ostell Mentor device: a systematic review. → Implant Dent. 2015 Oct;24(5):565–77. |
| 13, 14. | ↑ | Meredith N. Assessment of implant stability as a prognostic determinant. → Int J Prosthodont. 1998 Sep–Oct;11(5):491–501. |
| 15. | ↑ | Alsaadi G, Quirynen M, Michiels K, Jacobs R, van Steenberghe D. A biomechanical assessment of the relation between the oral implant stability at insertion and subjective bone quality assessment. → J Clin Periodontol. 2007 Apr;34(4):359–66. |
| 16, 23. | ↑ | Norton MR. The influence of low insertion torque on primary stability, implant survival, and maintenance of marginal bone levels: a closed-cohort prospective study. → Int J Oral Maxillofac Implants. 2017 Jul–Aug;32(4):849–57. |
| 17. | ↑ | Buser D, Weber HP, Lang NP. Tissue integration of non-submerged implants. 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants. → Clin Oral Implants Res. 1990 Dec;1(1):33–40. |
| 18, 30. | ↑ | Artzi Z, Kohen J, Carmeli G, Karmon B, Lor A, Ormianer Z. The efficacy of full-arch immediately restored implant-supported reconstructions in extraction and healed sites: a 36-month retrospective evaluation. → Int J Oral Maxillofac Implants. 2010 Mar–Apr;25(2):329–35. |
| 19, 31. | ↑ | Ormianer Z, Duda M, Block J, Matalon S. One- and two-piece implants placed in the same patients: clinical outcomes after 5 years of function. → Int J Prosthodont. 2015 Nov–Dec;29(6):608–10. |
| 20, 27. | ↑ | Chrcanovic BR, Kisch J, Albrektsson T, Wennerberg A. Factors influencing early dental implant failures. → J Dent Res. 2016 Aug;95(9):995–1002. |
| 21, 25. | ↑ | De Santis D, Cucchi A, Rigoni G, Longhi C, Nocini PF. Relationship between primary stability and crestal bone loss of implants placed with high insertion torque: a 3-year prospective study. → Int J Oral Maxillofac Implants. 2016 Sep–Oct;31(5):1126–34. |
| 22, 26. | ↑ | Maló P, Lopes A, de Araújo Nobre M, Ferro A. Immediate function dental implants inserted with less than 30 N·cm of torque in full-arch maxillary rehabilitations using the All-on-4 concept: retrospective study. → Int J Oral Maxillofac Surg. 2018 May 4. pii: S0901-5027(18)30138-3. doi: 10.1016/j.ijom.2018.04.008. [Epub ahead of print] |
| 24. | ↑ | Norton MR. The influence of insertion torque on the survival of immediately placed and restored single-tooth implants. → Int J Oral Maxillofac Implants. 2011 Nov–Dec;26(6):1333–43. |
| 28. | ↑ | Hinode D, Tanabe S, Yokoyama M, Fujisawa K, Yamauchi E, Miyamoto Y. Influence of smoking on osseointegrated implant failure: a meta-analysis. → Clin Oral Implants Res. 2006 Aug;17(4):473–8. |
| 29. | ↑ | Renvert S, Aghazadeh A, Hallstrom H, Persson GR. Factors related to peri-implantitis—a retrospective study. → Clin Oral Implants Res. 2014 Apr;25(4):522–9. |
| 32. | ↑ | Roos-Jansåker AM, Lindahl C, Renvert H, Renvert S. Nine- to fourteen-year follow-up of implant treatment. Part I: implant loss and associations to various factors. → J Clin Periodontol. 2006 Apr;33(4):283–9. |





Leave a Reply
Be the First to Comment!