Multifactorial statistical analysis toward evaluation of MBL, PES and PI of a novel nonsubmerged implant to restore a single tooth: A 1-year prospective cohort study
December 7, 2017 / Categories: Digital Dentistry, Implant Dentistry

Prati, Carlo

Zamparini, Fausto

Pirani, Chiara

Montebugnoli, Lucio
Gandolfi, Maria Giovanna
Abstract
Objective
The objective of this study was to evaluate radiographic, clinical and esthetic parameters of a new type of nonsubmerged 2-piece implant placed in patients in need of single-tooth replacement.
Materials and methods
Fifty-four consecutive patients requiring single-tooth replacement received 62 2-piece nonsubmerged flapless implants characterized by an innovative hyperbolic neck. The implant placement timing was as follows: 15 immediately post-extraction (immediate), 18 after 8–12 weeks (early) and 29 after 10–12 months (delayed). Customized abutments with an abutment–implant connection approximately 1–2 mm above the soft-tissue level were positioned after 3 months, loaded with provisional crowns and 20 days later with definitive crowns. Gingival biotype (thin or thick) was investigated in all patients. Periimplant marginal bone level (MBL; mm) was measured single-blinded on periapical radiographs at 1, 3, 6 and 12 months (T1, T3, T6, T12). Papilla index (PI), plaque score and bleeding on probing (BoP) were evaluated as clinical parameters of soft tissue. Pink Esthetic Score (PES) was calculated as the esthetic parameter.
Results
The survival rate was 100%. The dropout rate was 1.85%. The mean MBL was – 0.01 ± 0.26 at T1, – 0.17 ± 0.38 at T3, – 0.28 ± 0.32 at T6 and -0.37 ± 0.41 at T12. The PES (0–14) was 7.30 ± 2.80 at T0 (preoperatively), 11.06 ± 0.97 at T6 and 11.95 ± 1.04 at T12. At (T12), delayed implants showed a greater (P < 0.05) bone loss compared with early and immediate implants. Implants placed in thin biotype tissue showed the greatest bone loss at 12 months with a significant (P < 0.01) difference with respect to that at (T6). PES and PI increased from T0 to T12.
Conclusion
These implants allow preservation of a good MBL and offer a new approach to soft- and hard-tissue management, allowing a reduced healing time with minimally invasive surgery, no additional re-entry and fewer complications.
Keywords
Nonsubmerged dental implants, flapless surgery, marginal bone level (MBL), papilla index (PI), bleeding on probing (BoP), Pink Esthetic Score (PES).
Introduction
Flap raising and surgical trauma,1Raes F, Cosyn J, Crommelink E, Coessens P, De Bruyn H. Immediate and conventional single implant treatment in the anterior maxilla: 1-year results of a case series on hard and soft tissue response and aesthetics.
→ J Clin Periodontol. 2011 Apr;38(4):385–94.2Qian J, Wennerberg A, Albrektsson T. Reasons for marginal bone loss around oral implants.
→ Clin Implant Dent Relat Res. 2012 Dec;14(6):792–807. second re-entry surgeries and application of subgingival abutments3Sánchez-Siles M, Muñoz-Cámara D, Salazar-Sánchez N, Camacho-Alonso F, Calvo-Guirado JL. Crestal bone loss around submerged and non-submerged implants during the osseointegration phase with different healing abutment designs: a randomized prospective clinical study.
→ Clin Oral Implants Res. 2016 Sep 5. doi:10.1111/clr.12981. may lead to both hard- and soft-tissue complications, i.e., crestal bone loss, wound dehiscence and gingival recession.
The need for less-invasive protocols may be useful to avoid these complications. The use of nonsubmerged implants may prevent any surgical re-intervention for cover screw exposure and abutment or further prosthetic phases. The use of a flapless technique may reduce the risk of surgical complications and marginal bone loss.4Becker W, Goldstein M, Becker BE, Sennerby L. Minimally invasive flapless implant surgery: a prospective multicenter study.
→ Clin Implant Dent Relat Res. 2005;7 Suppl 1:S21–7.5Prati C, Zamparini F, Scialabba VS, Gatto MR, Piattelli A, Montebugnoli L, Gandolfi MG. A 3-year prospective cohort study on 132 calcium phosphate-blasted implants: flap vs flapless technique.
→ Int J Oral Maxillofac Implants. 2016 Mar–Apr;31(2):413–23. The type of implant and morphology of the neck may play some critical role in preserving marginal soft and bone tissue.
Recently, a new 2-piece nonsubmerged zirconium dioxide-blasted, acid-etched titanium implant (Prama, Sweden & Martina, Due Carrare, Italy) was marketed based on the biologically oriented preparation technique (BOPT). This prosthetic approach entails the creation of an ideal esthetic contour through gingival adaptation of the crown without the need for invasive surgical procedures. The crown is positioned on a previously prepared tooth with no finishing line, allowing the possibility of creating a new prosthetic cementoenamel junction and allowing the crown’s gingival margin to be shaped as desired.6Cocchetto R, Canullo L. The “hybrid abutment”: a new design for implant cemented restorations in the esthetic zones.
→ Int J Esthet Dent. 2015 Summer;10(2):186–208. This prosthetic technique was first described in the context of natural tooth-supported restorations,7Loi I, Di Felice A. Biologically oriented preparation technique (BOPT): a new approach for prosthetic restoration of periodontically healthy teeth.
→ Eur J Esthet Dent. 2013 Spring;8(1):10–23. but may be applied also to implant rehabilitation. The Prama implant was designed with a 3 mm hyperbolic machined neck that simulates a natural prosthetic abutment without a finishing line.
Short-term case reports and case series are beginning to be published in the literature.8Solá-Ruiz MF, Highsmith JD, Labaig-Rueda C, Agustín-Panadero R. Biologically oriented preparation technique (BOPT) for implant-supported fixed prostheses.
→ J Clin Exp Dent. 2017 Apr 1;9(4):e603–e607.9Prati C, Zamparini F, Chersoni S, Montebugnoli L, Gandolfi MG. 12-months prospective study on two-piece transmucosal-implants in the aesthetic zone.
→ J Dent Res. 2017;96A:202. Preliminary investigations have found promising soft- and hard-tissue management using a flapless technique and indicated that all prosthetic procedures resulted in simpler and easier procedures than with a conventional submerged implant–abutment connection.10Solá-Ruiz MF, Highsmith JD, Labaig-Rueda C, Agustín-Panadero R. Biologically oriented preparation technique (BOPT) for implant-supported fixed prostheses.
→ J Clin Exp Dent. 2017 Apr 1;9(4):e603–e607.11Prati C, Zamparini F, Chersoni S, Montebugnoli L, Gandolfi MG. 12-months prospective study on two-piece transmucosal-implants in the aesthetic zone.
→ J Dent Res. 2017;96A:202.12Canullo L, Tallarico M, Pradies G, Marinotti F, Loi I, Cocchetto R. Soft and hard tissue response to an implant with a convergent collar in the esthetic area: preliminary report at 18 months.
→ Int J Esthet Dent. 2017;12(3):306–23.
The aim of this consecutive prospective cohort study was to evaluate the failure rate and hard- and soft-tissue modifications and parameters during the first year of placement of nonsubmerged Prama implants.
Materials and methods
Study setting and patient selection
The study design was a single-blinded human longitudinal prospective cohort study evaluating clinical and radiographic parameters after 1 year for the treatment of patients who required replacement of a single tooth. The study was conducted in a university endodontic clinical department and 2 private dental offices. Patient recruitment was performed from September 2014 to September 2015. Patients were followed up between October 2014 and May 2017 by the same clinical team.
All of the patients included in this investigation were treated according to the principles established by the Declaration of Helsinki of 1975, as revised in 2013.13World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects.
→ JAMA. 2013 Nov 27;310(20):2191–4. Before enrolment, written and verbal information were given by the clinical staff and each patient gave written consent according to the above-mentioned principles. An additional signed informed consent was obtained from all patients stating that they accepted the treatment plan and agreed to cover the costs and follow the maintenance hygiene program. This report was written according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)14Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, Poole C, Schlesselman JJ, Egger M; STROBE Initiative. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration.
→ PLoS Med. 2007 Oct 16;4(10):e297. and respecting the guidelines published by Dodson in 2007.15Dodson TB. A guide for preparing a patient-oriented research manuscript.
→ Oral Surg Oral Med Oral Pathol Radiol Endod. 2007 Sep;104(3):307–15. The patients were considered eligible for inclusion in the clinical protocol based on the following inclusion criteria:
- aged 18–75;
- presence of a single failing tooth or a single tooth gap with both neighboring teeth present;
- possibility of inclusion in a hygiene recall program and implant control for at least 1 year; and
- smoking less than 10 cigarettes a day.
Exclusion criteria were as follows:
- medical and/or general contraindications for the surgical procedures (American Society of Anesthesiologists Physical Status ≥ 3);
- poor oral hygiene and lack of motivation;
- active clinical periodontal disease in the natural dentition determined by a probing pocket depth > 4 mm and bleeding on probing;
- smoking more than 10 cigarettes a day;
- uncontrolled diabetes mellitus;
- systemic or local disease that could compromise postoperative healing and osseointegration;
- alcohol and/or drug abuse;
- pregnancy or lactation;
- malocclusion or other occlusal disorder (bruxism); and
- bisphosphonate therapy.
Patiental location
The timing of implant placement (immediate, early or delayed according to the third ITI Consensus Conference)16Hämmerle CH, Chen ST, Wilson TG Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets.
→ Int J Oral Maxillofac Implants. 2004;19 Suppl:26–8. was specifically determined by an experienced university clinician following rigorous criteria aimed at best clinical practice (judgmental allocation).17Taxel P, Ortiz D, Shafer D, Pendrys D, Reisine S, Rengasamy K, Freilich M. The relationship between implant stability and bone health markers in post-menopausal women with bisphosphonate exposure.
→ Clin Oral Investig. 2014 Jan;18(1):49–57.
The following groups were defined:
- Immediate post-extraction implant group (type 1 for ITI):18Hämmerle CH, Chen ST, Wilson TG Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets.
→ Int J Oral Maxillofac Implants. 2004;19 Suppl:26–8. placement of the implant into the fresh extraction socket immediately after extraction of a tooth affected by chronic periapical disease or of a seriously damaged, hopeless tooth. Only chronic periapical lesions were present and identified by periapical radiolucency. - Early implant group (type 2 for ITI):19Hämmerle CH, Chen ST, Wilson TG Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets.
→ Int J Oral Maxillofac Implants. 2004;19 Suppl:26–8. placement of the implant in healed bone after 8–12 weeks after extraction of a tooth affected by an acute periapical lesion and/or abscess, pus and clinical symptoms. - Delayed implant group (type 4 for ITI):20Hämmerle CH, Chen ST, Wilson TG Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets.
→ Int J Oral Maxillofac Implants. 2004;19 Suppl:26–8. placement of the implant in edentulous mature bone 10–12 months after tooth extraction.
Preoperative protocol
The day before surgery, all of the patients were subjected to a preventive pharmacological treatment consisting of 1 g of amoxicillin/clavulanic acid (Augmentin, GlaxoSmithKline, Brentford, U.K.; 1 tablet at 24 and 12 h before the surgery) and a 0.12% chlorhexidine digluconate gel (Corsodyl Gel, GlaxoSmithKline; 3 applications per day). Antibiotic administration was continued for 5 days postoperatively.
Implant surgery
Implant surgeries were conducted by the same operator (C.P.) under local anesthesia with 30 mg/mL of mepivacaine hydrochloride (Carboplyina, Dentsply Italia, Rome, Italy) in sterile conditions. All of the implants were placed in 1-stage surgical procedures. No flaps were raised and no surgical guides were used.
A pilot drill of 1.2 mm in diameter was used to mark the position, angle and depth. The drill passed through the mucosa (nonsubmerged), cortical bone and cancellous bone at 225 rpm. A series of calibrated drills working at 225 rpm were used to create a site of adequate depth and diameter.
Prama implants, characterized by a 3 mm transmucosal machined neck with a hyperbolic profile (as illustrated by the environmental scanning electron microscopy image in Fig. 1) were inserted to keep the blasted surface at cortical bone level and the smooth machined neck surface 1–3 mm above the gingival level, according to the transmucosal technique.21Buser D, Sennerby L, De Bruyn H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions.
→ Periodontol 2000. 2017 Feb;73(1):7–21. No sutures were placed. A surgical dressing (COE-PAK, GC America, Alsip, Ill., U.S.) was applied to the implant site and kept in position for 5–7 days.
Postoperative procedures
Patients were instructed to follow a soft diet regime for 1 week, to rinse 3 times per day with a 0.12% chlorhexidine mouthwash for 3 weeks and to perform oral hygiene on the COE-PAK using a normal-medium-hardness toothbrush for the first week and for 2 weeks after removal of the surgical dressing. Thereafter, conventional brushing and flossing were permitted.
Prosthetic restoration
Three months after implant insertion, impressions using polyether materials (Permadyne and Garant, 3M ESPE, St. Paul, Minn., U.S.) were taken using customized resin trays (pickup impression technique). Gypsum model casts were obtained and provisional resin crowns were carefully designed to keep the crown margins at gingival level with the finishing line on the implant hyperbolic neck.
Customized titanium abutments were screwed in after 5–7 days. All of the resin crowns were positioned with temporary cement (Temp Bond, Kerr, Scafati, Italy) for initial prosthetic restoration. In this way, the implant–abutment connection was internal to the crowns. Abutments were intended to increase the retention of the cement–crown monobloc.
Twenty days later, definitive prosthetic metal–ceramic crowns were positioned and fixed with a polycarboxylate cement (Heraeus Kulzer, Hanau, Germany). Definitive crowns were also prepared according to the BOPT so that all metal and ceramic finishing lines corresponded to the implant hyperbolic neck. Fitting of the metal was gently and carefully done to create a mechanical metal–metal friction. Two experienced prosthodontists (C.P. and L.M.) performed all of the prosthetic procedures. Great attention was given to avoiding any cement excess around the restorations.
Follow-up implant evaluation
Active periodontal therapy consisting of motivation, instruction in oral hygiene practice, scaling and root planing was performed until no or modest periodontal disease was present.
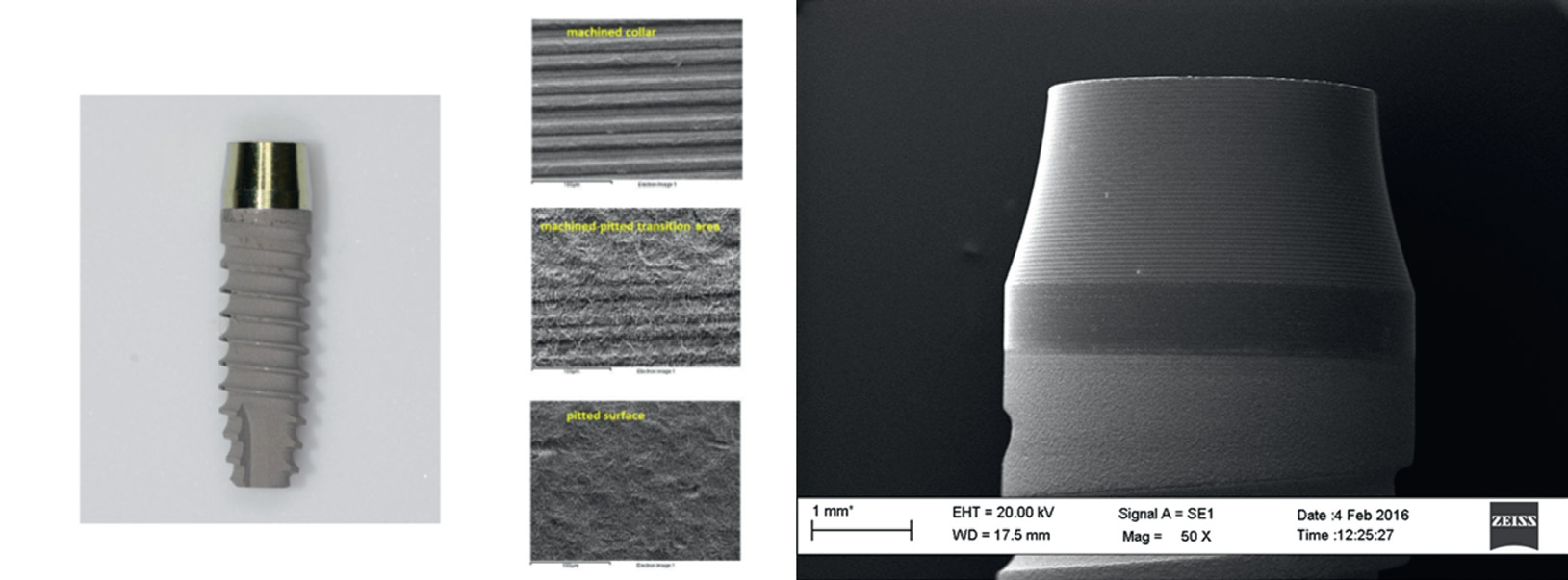
Optical microscopy and environmental scanning electron microscopy images showing the hyperbolic machined collar and the microtopography of the collar, body and apex portions of Prama implant.
Hard- and soft-tissue evaluation
Marginal bone level (MBL): Intraoral periapical radiographs of all of the implants were taken using the paralleling technique with Rinn holders (Dentsply Rinn, Elgin, Ill., U.S.) and analog films (Kodak Ektaspeed Plus, Eastman Kodak, Rochester, N.Y., U.S.) after implant placement (baseline) and at 1, 3, 6 and 12 months (T1, T3, T6, T12) after implant insertion.
All radiographs were scanned with a slide scanner with a resolution of 968 dpi and a magnification factor of ×20. The known lengths and diameters of the implants were used to calibrate the measurement. The crestal marginal bone and the bone–implant interface were examined to evaluate the marginal bone morphology. MBL was assessed at the mesial and distal implant surfaces by measuring the distance between the reference point of the implant platform to the most coronal bone–implant contact level using a scale of 0.1 mm increments according to previous studies22Sanz M, Cecchinato D, Ferrus J, Salvi GE, Ramseier C, Lang NP, Lindhe J. Implants placed in fresh extraction sockets in the maxilla: clinical and radiographic outcomes from a 3-year follow-up examination.
→ Clin Oral Implants Res. 2014 Mar;25(3):321–7.23Thoma DS, Sanz Martin I, Benic GI, Roos M, Hämmerle CH. Prospective randomized controlled clinical study comparing two dental implant systems: demographic and radiographic results at one year of loading.
→ Clin Oral Implants Res. 2014 Feb;25(2):142–9. and corrected according to the known length and diameter of each implant.24Galindo-Moreno P, León-Cano A, Ortega-Oller I, Monje A, Suárez F, ÓValle F, Spinato S, Catena A. Prosthetic abutment height is a key factor in peri-implant marginal bone loss.
→ J Dent Res. 2014 Jul;93(7 Suppl):80S–85S.
Radiographic evaluation was performed single-blinded by 1 additional examiner (F.Z.). Before evaluating the radiographs, the examiner was calibrated using well-defined instructions and reference radiographs with different MBL measures.
Periimplant soft-tissue thickness/gingival biotype: The soft-tissue thickness around the implants and their corresponding mesial/distal neighboring teeth was determined. The soft tissue was pierced midfacially at 3 mm apical to the gingival margin with an endodontic file (No. 20 K-file, Dentsply Maillefer, Switzerland). Gingival biotype was defined as thick (soft-tissue thickness > 2 mm) or thin (soft-tissue thickness ≤ 2 mm).25Ferrari M, Carrabba M, Vichi A, Goracci C, Cagidiaco MC. Influence of abutment color and mucosal thickness on soft tissue color.
→ Int J Oral Maxillofac Implants. 2017 Mar–Apr;32(2):393–9.26Cosgarea R, Gasparik C, Dudea D, Culic B, Dannewitz B, Sculean A. Peri-implant soft tissue colour around titanium and zirconia abutments: a prospective randomized controlled clinical study.
→ Clin Oral Implants Res. 2015 May;26(5):537–44.27Zembic A, Sailer I, Jung RE, Hämmerle CH. Randomized-controlled clinical trial of customized zirconia and titanium implant abutments for single-tooth implants in canine and posterior regions: 3-year results.
→ Clin Oral Implants Res. 2009 Aug;20(8):802–8.
Pink Esthetic Score (PES): PES28Fürhauser R, Florescu D, Benesch T, Haas R, Mailath G, Watzek G. Evaluation of soft tissue around single-tooth implant crowns: the pink esthetic score.
→ Clin Oral Implants Res. 2005 Dec;16(6):639–44. was assessed preoperatively and at T6 and T12. Seven variables were evaluated against a natural reference tooth by 1 trained operator (the contralateral tooth for an incisor and contralateral tooth or neighboring tooth for a premolar) using a 0–2 scoring system (0 being the lowest and 2 being the highest value): mesial papilla, distal papilla, soft-tissue level, soft-tissue contour, alveolar process deficiency, soft-tissue color and soft-tissue texture. The maximum achievable PES was 14. According to Raes et al., a PES < 8 is considered an esthetic failure, while a PES ≥ 12 is considered an (almost) perfect outcome. 29Raes F, Cosyn J, Crommelink E, Coessens P, De Bruyn H. Immediate and conventional single implant treatment in the anterior maxilla: 1-year results of a case series on hard and soft tissue response and aesthetics.
→ J Clin Periodontol. 2011 Apr;38(4):385–94.
Papilla index (PI): PI30Jemt T. Regeneration of gingival papillae after single-implant treatment.
→ Int J Periodontics Restorative Dent. 1997 Aug;17(4):326–33. was assessed mesially and distally by 1 trained operator using a 0–4 scale at T6 and T12. A PI score was given as follows: 0 = no papilla; 1 = papilla fills less than 50% of the interproximal space; 2 = papilla fills more than 50% of the interproximal space, but not entirely; 3 = papilla fills the entire interproximal space harmoniously; 4 = hyperplastic papilla. Plaque score:
Plaque score31Cosyn J, Eghbali A, Hermans A, Vervaeke S, De Bruyn H, Cleymaet R. A 5-year prospective study on single immediate implants in the aesthetic zone.
→ J Clin Periodontol. 2016 Aug;43(8):702–9. was assessed at 4 sites (mesial, distal, vestibular and palatal) around the implant restorations at T6 and T12. A dichotomous score was given (0 = no visible plaque at the soft margin; 1 = visible plaque at the soft margin).
Bleeding on probing (BoP): BoP 32Cosyn J, Eghbali A, Hermans A, Vervaeke S, De Bruyn H, Cleymaet R. A 5-year prospective study on single immediate implants in the aesthetic zone.
→ J Clin Periodontol. 2016 Aug;43(8):702–9. was measured at 4 sites (mesial, distal, vestibular and palatal) around the implant restorations at T6 and T12. A dichotomous score was given (0 = no bleeding; 1 = bleeding).
Statistical analysis of the MBL
Linear regression models were fitted to evaluate the existence of any significant difference regarding placement (immediate, early and delayed), times (1 month, 3 months, 6 months and 12 months), and the interactions between placement and time. In order to take into account the correlation in the data due to the presence of multiple implants per subject, the above-mentioned regression models were estimated following a generalized estimating equation approach. The implant was used as the unit of analysis. We adjusted the estimates of the coefficients’ standard errors and confidence intervals using a robust variance–covariance estimator.33Rogers WH. Regression standard errors in clustered samples.
→ Stata Technical Bulletin. 1993 May;13:19–23. The same analysis was performed for gingival biotype.
A multiple linear regression model with stepwise selection was fitted to evaluate the relationship between MBL at 12 months and the following variables: sex (male/female), location (mandible/maxilla), tooth type (anterior/posterior), endodontically treated adjacent teeth (yes/no), implant placement (immediate, early, delayed), implant diameter (3.80, 4.25 or 5.00 mm), implant length (10.0/11.5 mm) and gingival biotype (thin/thick). All statistical analysis was performed using Stata (Version 13.1, StataCorp, College Station, Texas, U.S.).
Results
Based on the inclusion and exclusion criteria, 54 patients (62 implants) with a mean age of 56.8 ± 12.0 years (26 men and 28 women) were included. Table 1 depicts implant distribution and MBL (mean ± SD) at 12 months according to the pre-, intra- and postoperative parameters evaluated.
The survival rate was 100%. The total patient dropout rate was 1.85%. No wound infection, osteitis, bone graft sequestration or implant loosening occurred during the follow-up period.
Mean MBL values according to implant placement group and gingival biotype are reported in Tables 2 and 3, respectively. The delayed implant group showed the greatest bone loss from T6 to T12, the difference being statistically significant (P < 0.05) with respect to both the early and immediate groups. The early implant group showed the lowest bone loss at all times. Interestingly, all 3 groups showed a statistically different MBL at T3 with respect to T1. Considering gingival thickness, MBL significantly (P < 0.01) decreased with time in both groups, but patients with a thin biotype showed a greater bone loss (P < 0.01) than patients with a thick biotype. A statistically significant difference (P < 0.01) in MBL between groups was found at 6 and at 12 months. The results of the multiple linear regression (Table 4a) showed that implant diameter and gingival biotype were the only variables significantly (P < 0.01) related to MBL at T12, the gingival biotype being the most important one (Table 4b). As soft-tissue evaluation parameters, PES and PI assessment are reported in Tables 5 and 6. Adequate/good PES scores were reported for all implants, increasing from T6 to T12. Also, PI increased from T6 to T12. Plaque score and BoP are reported in Table 7. A clinical photograph sequence of an example of implant rehabilitation is shown in Figure 2. A periapical radiograph sequence of a representative case is presented in Figure 3.
Discussion
The study has demonstrated that the proposed nonsubmerged technique with a hyperbolic neck design allows the achievement of a stable periimplant MBL and an adequate soft-tissue morphology. MBL was evaluated at 1 and 3 months after implant insertion (preloading period) and demonstrated very limited bone loss despite the gingival emergence of a yellow implant neck.
Previous studies have evaluated MBL from initial loading (postloading period), not considering that bone loss may occur during the preloading time.34Prati C, Zamparini F, Scialabba VS, Gatto MR, Piattelli A, Montebugnoli L, Gandolfi MG. A 3-year prospective cohort study on 132 calcium phosphate-blasted implants: flap vs flapless technique.
→ Int J Oral Maxillofac Implants. 2016 Mar–Apr;31(2):413–23. Interestingly, in the present study, a stable MBL was observed after 1 month from insertion. The flapless technique35Chrcanovic BR, Albrektsson T, Wennerberg A. Flapless versus conventional flapped dental implant surgery: a meta-analysis.
→ PLoS ONE. 2014 Jun 20;9(6):e100624.36De Bruyn H, Atashkadeh M, Cosyn J, van der Velde T. Clinical outcome and bone preservation of single TiUnite implants installed with flapless or flap surgery.
→ Clin Implant Dent Relat Res. 2011 Sep;13(3):175–83.37Rousseau P. Flapless and traditional dental implant surgery: an open, retrospective comparative study.
→ J Oral Maxillofac Surg. 2010 Sep;68(9):2299–306. probably minimized surgical trauma that may be responsible for initial marginal bone loss.38Galindo-Moreno P, León-Cano A, Ortega-Oller I, Monje A, O’Valle F, Catena A. Marginal bone loss as success criterion in implant dentistry: beyond 2 mm.
→ Clin Oral Implants Res. 2015 Apr;26(4):e28–34.
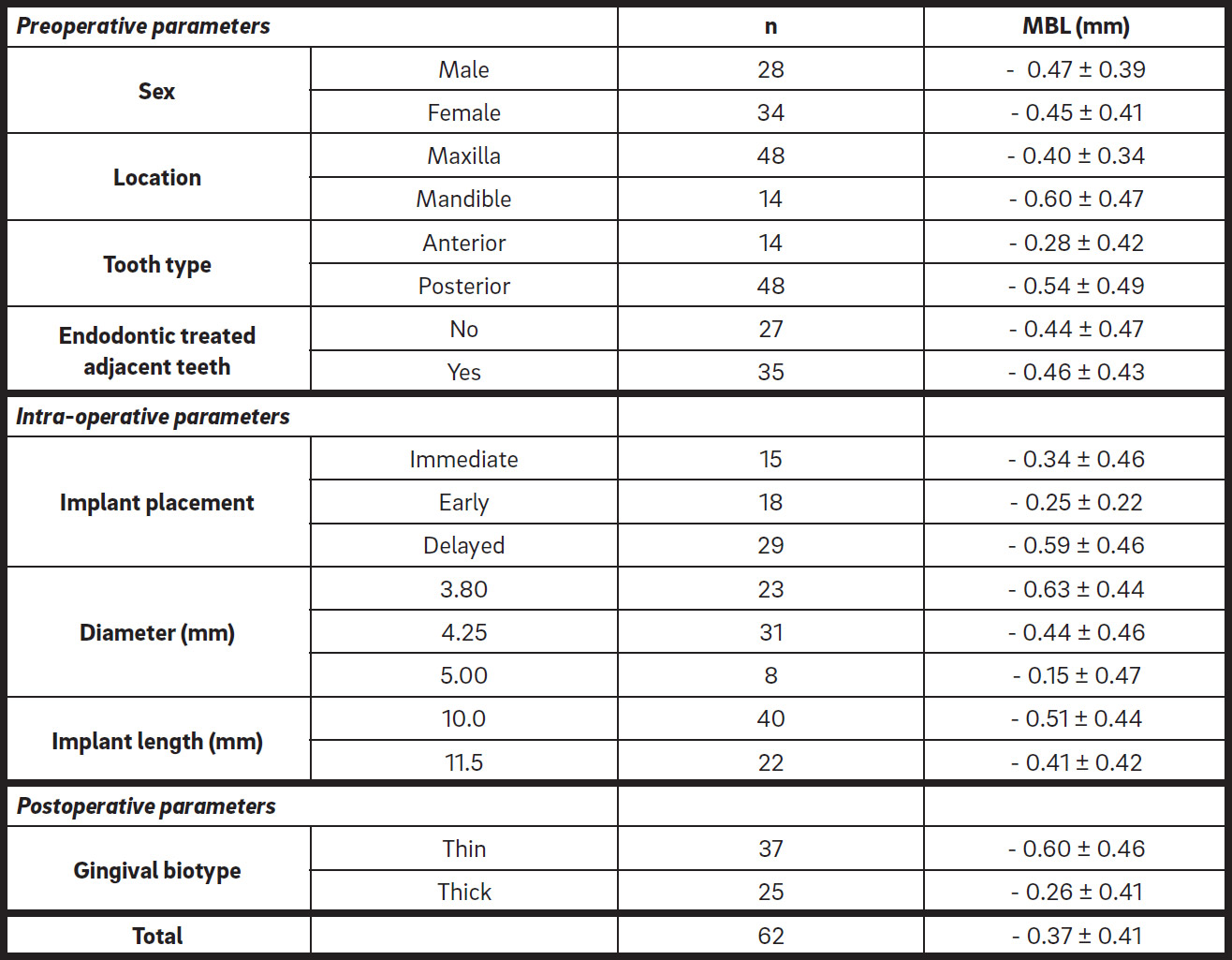
Distribution, number of implants placed (n) and MBL (mean ± SD) at 12 months.
† One patient dropped out 1 month after implant insertion (2 delayed implants). Total dropout was 1.85%.

Linear regression results for implant placement using GEE with the robust covariance estimator to account for correlation in the data. The implant was used as the unit of analysis (MBL values expressed as mean ± SD).
Equal superscript capital letters represent no statistically significant difference between groups (P > 0.05).
Equal superscript small letters represent no statistically significant time-related difference with times in both groups (P > 0.05).
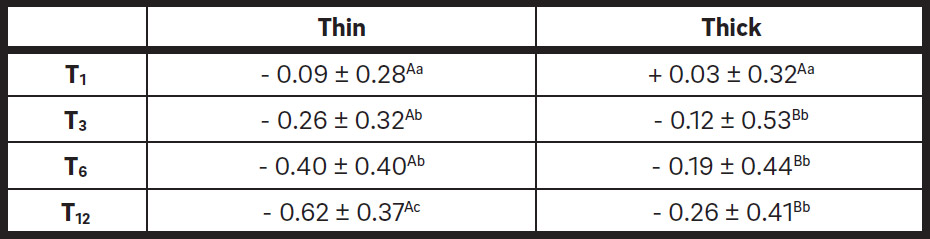
Linear regression results for gingival biotype using GEE with the robust covariance estimator to account for correlation in the data. The implant was used as the unit of analysis (MBL values expressed as mean ± SD).
Equal superscript capital letters represent no statistically significant difference between groups (P > 0.05).
Equal superscript small letters represent no statistically significant time-related difference with times in both groups (P > 0.05).
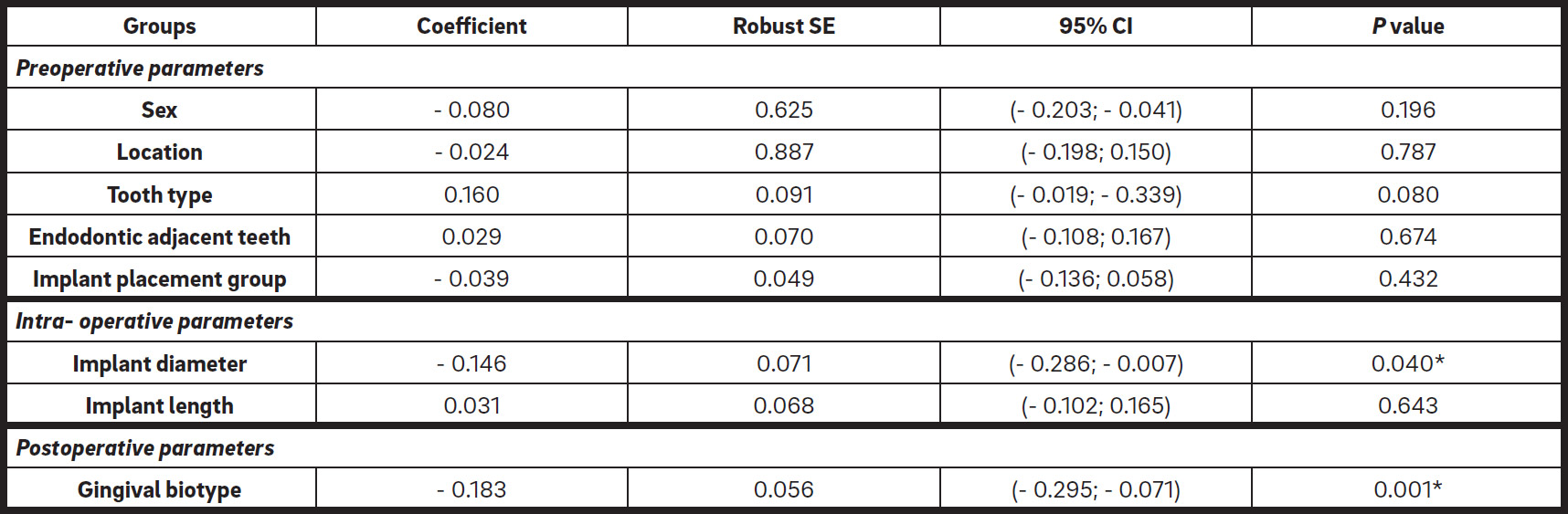
Multiple linear regression relating MBL at 12 months to all variables considered.
* asterisks indicate statistically significant differences (p < 0.05)

Multiple linear regression after stepwise selection.
* asterisks indicate statistically significant differences (p < 0.05)
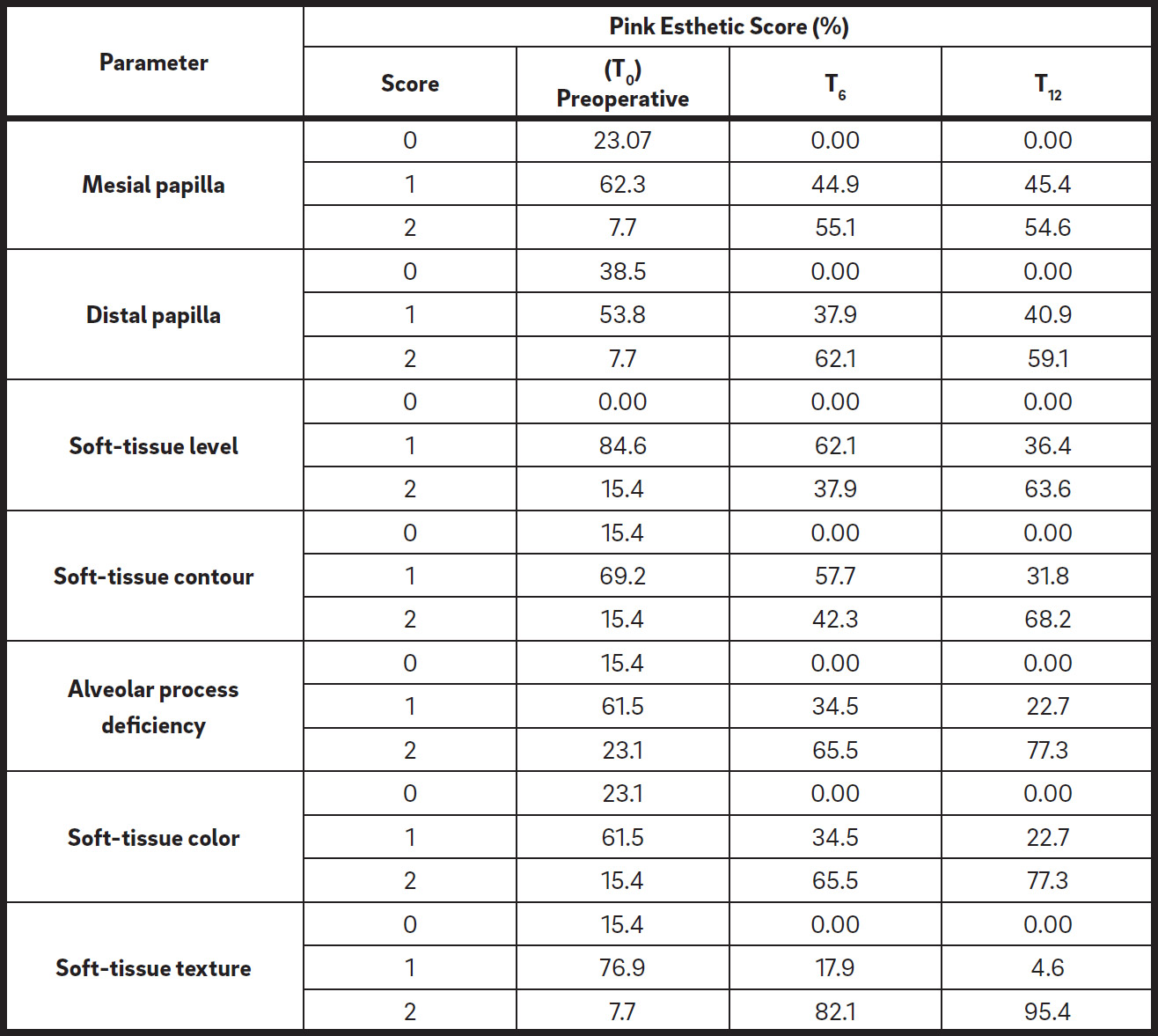
Pink Esthetic Score of single implant (expressed as percentage).

Pink Esthetic Score (0–14).

Papilla index (mean ± SD).
PI-M: papilla index of mesial papilla; PI-D: papilla index of distal papilla.
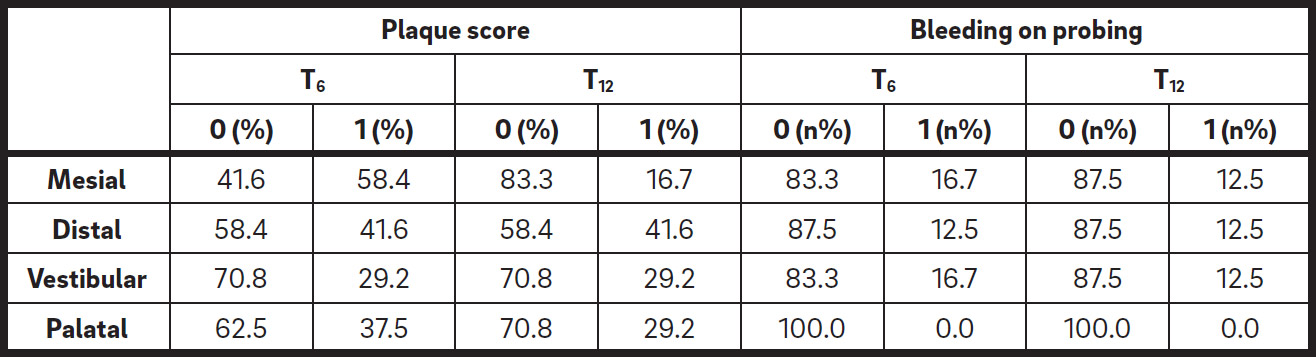
Periodontal parameters around implant restorations after definitive loading.
A 0 value indicates that no bleeding on probing/plaque accumulation was present.
A 1 value indicates that bleeding on probing/plaque accumulation was present.
Our investigation is the first prospective clinical study to evaluate a high number of clinical (BoP, PI and plaque score), radiographic (MBL) and esthetic (PES) parameters and include a reasonable number of implants and patients. Currently, only a case report39Solá-Ruiz MF, Highsmith JD, Labaig-Rueda C, Agustín-Panadero R. Biologically oriented preparation technique (BOPT) for implant-supported fixed prostheses.
→ J Clin Exp Dent. 2017 Apr 1;9(4):e603–e607. and a prospective cohort study40Canullo L, Tallarico M, Pradies G, Marinotti F, Loi I, Cocchetto R. Soft and hard tissue response to an implant with a convergent collar in the esthetic area: preliminary report at 18 months.
→ Int J Esthet Dent. 2017;12(3):306–23. at 18 months with just 14 patients, showing a stable MBL and a soft-tissue improvement, have been published on the Prama implant.
A study on another implant system demonstrated in both flapless and flapped groups a marginal bone loss of 0.5 mm after the stressfree healing period,41Nickening HJ, Wichmann M, Schlegel KA, Nkenke E, Eiter S. Radiographic evaluation of marginal bone levels during healing period, adjacent to parallel-screw cylinder implants inserted in the posterior zone of the jaws, placed with flapless surgery.
→ Clin Oral Implants Res. 2010 Dec;21(12):1386–93. not far from our results. Similar values were reported in other investigations regarding different implant systems and the flapless technique.42De Bruyn H, Atashkadeh M, Cosyn J, van der Velde T. Clinical outcome and bone preservation of single TiUnite implants installed with flapless or flap surgery.
→ Clin Implant Dent Relat Res. 2011 Sep;13(3):175–83.43Rousseau P. Flapless and traditional dental implant surgery: an open, retrospective comparative study.
→ J Oral Maxillofac Surg. 2010 Sep;68(9):2299–306. Long-term results from a randomized clinical trial on a 1-piece implant with a conical neck shape (similar to the hyperbolic profile) have recently been published,44Froum SJ, Khouly I. Survival rates and bone and soft tissue level changes around one-piece dental implants placed with a flapless or flap protocol: 8.5-year results.
→ Int J Periodontics Restorative Dent. 2017 May–Jun;37(3):327–37. reporting high success (96.4%) and survival rates (100%) and acceptable periimplant bone loss (mean MBL: -0.30 ± 0.78 mm). Considering all of the implants placed and evaluated in the present study, a mean MBL of -0.37 ± 0.41 mm was observed at T12, in agreement with standard success criteria and the previous recent study.45Froum SJ, Khouly I. Survival rates and bone and soft tissue level changes around one-piece dental implants placed with a flapless or flap protocol: 8.5-year results.
→ Int J Periodontics Restorative Dent. 2017 May–Jun;37(3):327–37.
-

- Fig. A
-
- Fig. B
-
- Fig. C
-

- Fig. D
-
- Fig. E
-

- Fig. F
-

- Fig. G
-

- Fig. H
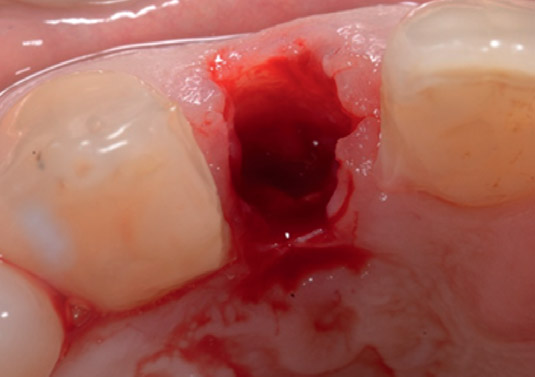
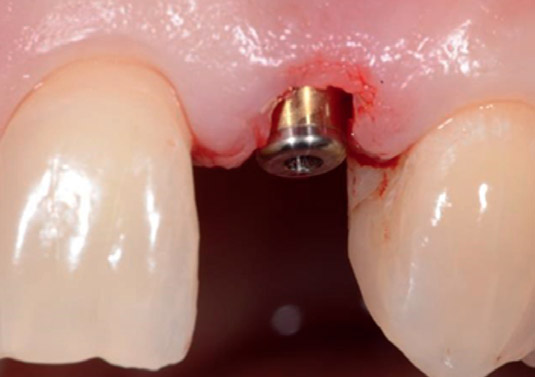
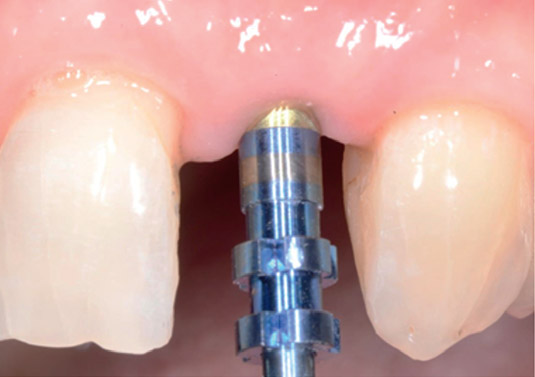
Maxillary left lateral incisor that had previously undergone an apicoectomy. The tooth presented high-grade mobility and extraction was scheduled. (A) Pre-extraction vestibular view. Atraumatic extraction was performed, as well as adequate alveolar socket debridement. (B) Postextraction view. A Prama implant was placed nonsubmerged according to the manufacturer’s instructions; (C) vestibular and (D) occlusal views. After 3 months, impressions were taken (D) and an abutment was fixed (E). No second surgeries were performed to expose the implant neck. A provisional crown was cemented free from tissue compression (F) and a metal–ceramic crown was later cemented (G).
Concerning MBL in relation to placement timing groups (immediate, early and delayed), delayed implants showed greater bone loss (0.61 ± 0.38 mm) at 12 months, while early and immediate implants showed limited bone loss (MBL: 0.25 ± 0.45 mm and 0.34 ± 0.04 mm, respectively). These results were in accordance with another previous published study, which investigated implants with the same surface, but a different neck morphology (tulip-shaped, platform-switched implants).46Prati C, Zamparini F, Pirani C, Gatto MR, Piattelli A, Gandolfi MG. Immediate early and delayed implants: a 2-year prospective cohort study of 131 transmucosal flapless implants placed in sites with different pre-extractive endodontic infections.
→ Implant Dent. 2017 Oct;26(5):654–63. Bone remodeling procedures are probably different in mature (delayed group) or immature bone (early and immediate group), as recently shown in several in vivo animal studies that tested the ZrTi implant surface micromorphology used in Prama implants.47Mainetti T, Lang NP, Bengazi F, Sbricoli L, Soto Cantero L, Botticelli D. Immediate loading of implants installed in a healed alveolar bony ridge or immediately after tooth extraction: an experimental study in dogs.
→ Clin Oral Implants Res. 2015 Apr;26(4):435–41.48Mainetti T, Lang NP, Bengazi F, Favero V, Soto Cantero L, Botticelli D. Sequential healing at implants installed immediately into extraction sockets. An experimental study in dogs.
In all of the patients, periimplant gingival biotype was evaluated after 12 months from implant insertion. Thin gingival biotype demonstrated greater bone loss values at 12 months (P = 0.008). This is in accordance with the findings of a recent study with a different bone level implant.49Puisys A, Linkevicius T. The influence of mucosal tissue thickening on crestal bone stability around bone-level implants. A prospective controlled clinical trial.
→ Clin Oral Implants Res. 2015 Feb;26(2):123–9. Considering all of the parameters evaluated in the statistical analysis, gingival biotype was found to greatly affect MBL.50Zweers J, Thomas RZ, Slot DE, Weisgold AS, Van der Weijden FG. Characteristics of periodontal biotype, its dimensions, associations and prevalence: a systematic review.
→ J Clin Periodontol. 2014 Oct;41(10):958–71. Berglundh and Lindhe demonstrated in an animal study that a thin gingival biotype may affect crestal bone stability.51Berglundh T, Lindhe J. Dimension of the periimplant mucosa. Biological width revisited.
→ J Clin Periodontol. 1996 Oct;23(10):971–3. Thus, also for this type of implant, postoperative gingival biotype may be considered one of the most important clinical parameters that may affect MBL at least after 12 months from placement. Soft-tissue parameters evidenced an improvement from 6 to 12 months, showing a soft-tissue maturation over time. The mean PES was 11.09 at 6 months (2 months from definitive loading) and improved at the 12-month follow-up, showing a mean value of 11.95. This confirms that soft-tissue modifications occur during the first months of loading. Similar PES values are reported in the literature. In a 12-month clinical study, the PES of 2 different implant treatment strategies was evaluated (immediate implants versus conventional loading). Their 12-month mean values were 10.33 and 10.35, respectively.52Raes F, Cosyn J, Crommelink E, Coessens P, De Bruyn H. Immediate and conventional single implant treatment in the anterior maxilla: 1-year results of a case series on hard and soft tissue response and aesthetics.
→ J Clin Periodontol. 2011 Apr;38(4):385–94.
Interestingly, in our study, a high prevalence of the maximum soft-tissue color score was found (65.51% at 6 months and 77.28% at 12 months), despite the presence of an unfavorable preoperative score (approximately a quarter of the preoperative soft-tissue color presented a 0 score). The yellow Prama hyperbolic neck, together with the presence of a thick gingival biotype (60.19%), may explain these results. Demonstrating a healthy gingiva with no inflammation, 95.44% of the implants showed an optimal soft-tissue texture. In order to further consolidate these results, BoP at the 12-month evaluation was negative in approximately 90% of the periimplant sites evaluated.
-

- Preoperative
-
- Post-extraction
-
- Immediate placement
-
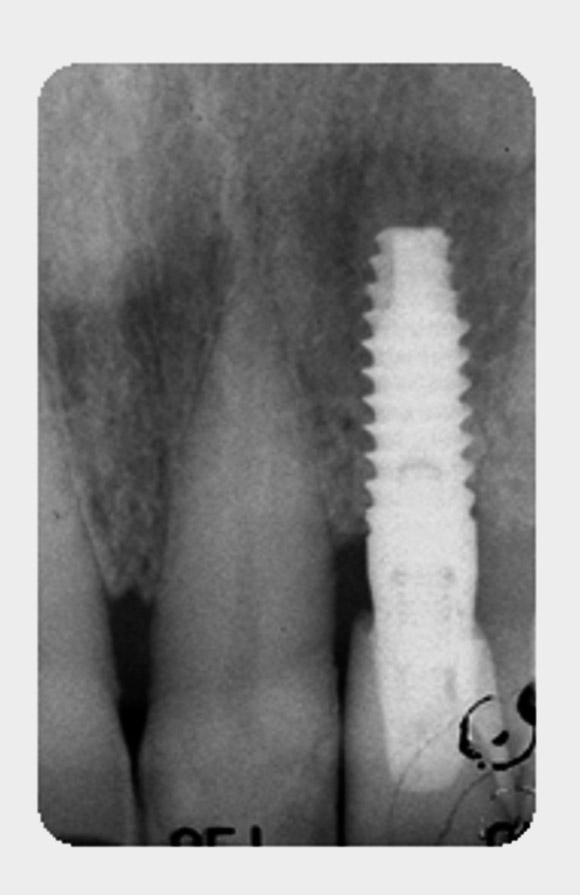
- After 6 months
-

- After 12 months
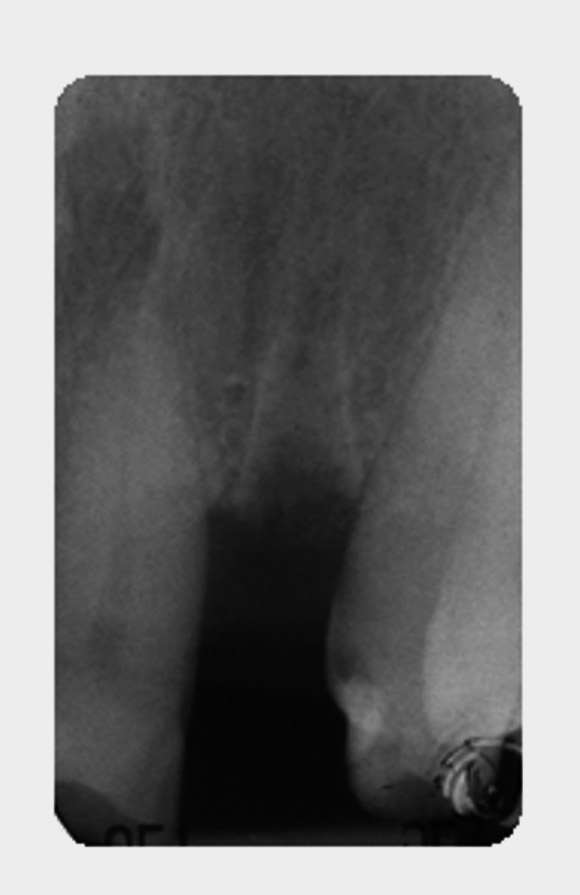
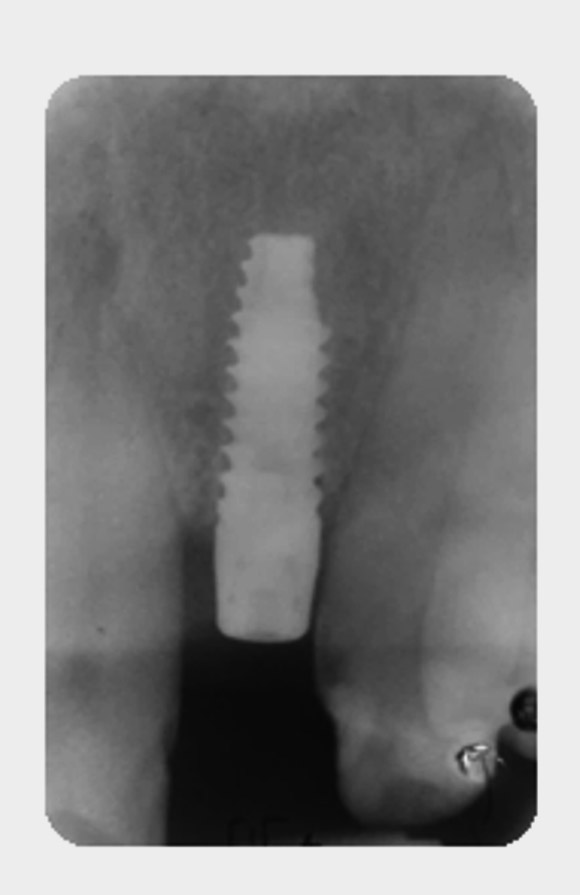
Periapical radiograph sequence of immediate implant placement restoring a fractured endodontically treated lateral incisor. (A) Preoperative radiograph. (B) Post-extraction radiograph. (C) A 3.8 × 11.5 mm implant was placed nonsubmerged immediately after extraction. A stable MBL was observed at 6 months (D) and it remained stable at the 12-month follow-up (E).
It is known that plaque accumulation around implant restorations may induce soft-tissue chronic inflammation, gingival bleeding and, in the long-term, periimplant bone loss.53Berglundh T, Lindhe J. Dimension of the periimplant mucosa. Biological width revisited.
→ J Clin Periodontol. 1996 Oct;23(10):971–3. Little plaque accumulation was present around implant sites at 12 months. Sites totally free from plaque ranged from 58.4% to 83.3%. The 3 mm machined surface of the implant neck, the crown design and the hygienic recall program may also have contributed to this result. It has been reported that machined surfaces may reduce plaque and bacteria accumulation around the implant emergence profile.54Renvert S, Quirynen M. Risk indicators for peri-implantitis. A narrative review.
→ Clin Oral Implants Res. 2015 Sep;26 Suppl 11:15–44.
Limitations of the study are represented by the small sample size and the short-term follow-up. Thus, results should be interpreted with caution. Further investigations in the long term and with a larger study cohort may confirm our results. The Prama implant, following BOPT principles, allows the clinician to model the soft tissue and have the gingival margin level with the periimplant tissue in the same way as natural tooth-supported restorations, as no finishing line is present. Moreover, the implant emergence profile with the hyperbolic configuration allows creation of the crown finishing line corresponding to the gingival margin or to the periimplant sulcus without any tissue compression. Within the limitations of this preliminary study, the results demonstrated some advantages that may be the result of simpler prosthetic management:
- use of a noninvasive flapless technique with no second surgery for neck exposure and no need for a healing screw;
- possibility of positioning the crown margin at different levels close to the periimplant sulcus and corresponding to the (yellow) implant neck;
- implant–abutment connection above the gingival level;
- minimal trauma and stress on the soft tissue during prosthetic procedures to preserve the MBL;
- adequate control to avoid excess cement.
Two drawbacks must be reported:
- Surgical implant positioning is critical, as no modification of the abutment axis may be later performed, so a partial lack of abutment versatility must be included.
- The implant requires adequate distance from the opposite antagonist tooth, as the implant neck plus abutment requires at least 5 mm plus crown restoration.
Conclusion
The use of a 2-piece nonsubmerged implant with a hyperbolic neck profile offers a new approach to the management of soft and hard tissue. In this, the prosthetic preparation makes it possible to preserve a good MBL, to reduce healing time, to perform a minimally invasive surgery, to avoid additional re-entry and to have fewer complications. Competing interests The authors declare that they have no competing interests.

Interview
with Carlo Prati
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
Recently, only a case report and a prospective cohort study with just 14 patients have been published on this innovative implant. Ours is the first clinical study evaluating a high number of parameters and including a reasonable number of implants and patients.
How could your study’s findings have an impact on dentistry?
Moreover, as the implant–abutment connection is approximately 2 mm from the gingival tissue and is covered by the prosthetic crown, the risk of bacterial contamination is likely reduced.
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 52. | ↑ | Raes F, Cosyn J, Crommelink E, Coessens P, De Bruyn H. Immediate and conventional single implant treatment in the anterior maxilla: 1-year results of a case series on hard and soft tissue response and aesthetics. → J Clin Periodontol. 2011 Apr;38(4):385–94. |
| 2. | ↑ | Qian J, Wennerberg A, Albrektsson T. Reasons for marginal bone loss around oral implants. → Clin Implant Dent Relat Res. 2012 Dec;14(6):792–807. |
| 3. | ↑ | Sánchez-Siles M, Muñoz-Cámara D, Salazar-Sánchez N, Camacho-Alonso F, Calvo-Guirado JL. Crestal bone loss around submerged and non-submerged implants during the osseointegration phase with different healing abutment designs: a randomized prospective clinical study. → Clin Oral Implants Res. 2016 Sep 5. doi:10.1111/clr.12981. |
| 4. | ↑ | Becker W, Goldstein M, Becker BE, Sennerby L. Minimally invasive flapless implant surgery: a prospective multicenter study. → Clin Implant Dent Relat Res. 2005;7 Suppl 1:S21–7. |
| 5, 34. | ↑ | Prati C, Zamparini F, Scialabba VS, Gatto MR, Piattelli A, Montebugnoli L, Gandolfi MG. A 3-year prospective cohort study on 132 calcium phosphate-blasted implants: flap vs flapless technique. → Int J Oral Maxillofac Implants. 2016 Mar–Apr;31(2):413–23. |
| 6. | ↑ | Cocchetto R, Canullo L. The “hybrid abutment”: a new design for implant cemented restorations in the esthetic zones. → Int J Esthet Dent. 2015 Summer;10(2):186–208. |
| 7. | ↑ | Loi I, Di Felice A. Biologically oriented preparation technique (BOPT): a new approach for prosthetic restoration of periodontically healthy teeth. → Eur J Esthet Dent. 2013 Spring;8(1):10–23. |
| 8, 10, 39. | ↑ | Solá-Ruiz MF, Highsmith JD, Labaig-Rueda C, Agustín-Panadero R. Biologically oriented preparation technique (BOPT) for implant-supported fixed prostheses. → J Clin Exp Dent. 2017 Apr 1;9(4):e603–e607. |
| 9, 11. | ↑ | Prati C, Zamparini F, Chersoni S, Montebugnoli L, Gandolfi MG. 12-months prospective study on two-piece transmucosal-implants in the aesthetic zone. → J Dent Res. 2017;96A:202. |
| 12, 40. | ↑ | Canullo L, Tallarico M, Pradies G, Marinotti F, Loi I, Cocchetto R. Soft and hard tissue response to an implant with a convergent collar in the esthetic area: preliminary report at 18 months. → Int J Esthet Dent. 2017;12(3):306–23. |
| 13. | ↑ | World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. → JAMA. 2013 Nov 27;310(20):2191–4. |
| 14. | ↑ | Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, Poole C, Schlesselman JJ, Egger M; STROBE Initiative. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. → PLoS Med. 2007 Oct 16;4(10):e297. |
| 15. | ↑ | Dodson TB. A guide for preparing a patient-oriented research manuscript. → Oral Surg Oral Med Oral Pathol Radiol Endod. 2007 Sep;104(3):307–15. |
| 16, 18, 19, 20. | ↑ | Hämmerle CH, Chen ST, Wilson TG Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. → Int J Oral Maxillofac Implants. 2004;19 Suppl:26–8. |
| 17. | ↑ | Taxel P, Ortiz D, Shafer D, Pendrys D, Reisine S, Rengasamy K, Freilich M. The relationship between implant stability and bone health markers in post-menopausal women with bisphosphonate exposure. → Clin Oral Investig. 2014 Jan;18(1):49–57. |
| 21. | ↑ | Buser D, Sennerby L, De Bruyn H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. → Periodontol 2000. 2017 Feb;73(1):7–21. |
| 22. | ↑ | Sanz M, Cecchinato D, Ferrus J, Salvi GE, Ramseier C, Lang NP, Lindhe J. Implants placed in fresh extraction sockets in the maxilla: clinical and radiographic outcomes from a 3-year follow-up examination. → Clin Oral Implants Res. 2014 Mar;25(3):321–7. |
| 23. | ↑ | Thoma DS, Sanz Martin I, Benic GI, Roos M, Hämmerle CH. Prospective randomized controlled clinical study comparing two dental implant systems: demographic and radiographic results at one year of loading. → Clin Oral Implants Res. 2014 Feb;25(2):142–9. |
| 24. | ↑ | Galindo-Moreno P, León-Cano A, Ortega-Oller I, Monje A, Suárez F, ÓValle F, Spinato S, Catena A. Prosthetic abutment height is a key factor in peri-implant marginal bone loss. → J Dent Res. 2014 Jul;93(7 Suppl):80S–85S. |
| 25. | ↑ | Ferrari M, Carrabba M, Vichi A, Goracci C, Cagidiaco MC. Influence of abutment color and mucosal thickness on soft tissue color. → Int J Oral Maxillofac Implants. 2017 Mar–Apr;32(2):393–9. |
| 26. | ↑ | Cosgarea R, Gasparik C, Dudea D, Culic B, Dannewitz B, Sculean A. Peri-implant soft tissue colour around titanium and zirconia abutments: a prospective randomized controlled clinical study. → Clin Oral Implants Res. 2015 May;26(5):537–44. |
| 27. | ↑ | Zembic A, Sailer I, Jung RE, Hämmerle CH. Randomized-controlled clinical trial of customized zirconia and titanium implant abutments for single-tooth implants in canine and posterior regions: 3-year results. → Clin Oral Implants Res. 2009 Aug;20(8):802–8. |
| 28. | ↑ | Fürhauser R, Florescu D, Benesch T, Haas R, Mailath G, Watzek G. Evaluation of soft tissue around single-tooth implant crowns: the pink esthetic score. → Clin Oral Implants Res. 2005 Dec;16(6):639–44. |
| 29. | ↑ | Raes F, Cosyn J, Crommelink E, Coessens P, De Bruyn H. Immediate and conventional single implant treatment in the anterior maxilla: 1-year results of a case series on hard and soft tissue response and aesthetics. → J Clin Periodontol. 2011 Apr;38(4):385–94. |
| 30. | ↑ | Jemt T. Regeneration of gingival papillae after single-implant treatment. → Int J Periodontics Restorative Dent. 1997 Aug;17(4):326–33. |
| 31, 32. | ↑ | Cosyn J, Eghbali A, Hermans A, Vervaeke S, De Bruyn H, Cleymaet R. A 5-year prospective study on single immediate implants in the aesthetic zone. → J Clin Periodontol. 2016 Aug;43(8):702–9. |
| 33. | ↑ | Rogers WH. Regression standard errors in clustered samples. → Stata Technical Bulletin. 1993 May;13:19–23. |
| 35. | ↑ | Chrcanovic BR, Albrektsson T, Wennerberg A. Flapless versus conventional flapped dental implant surgery: a meta-analysis. → PLoS ONE. 2014 Jun 20;9(6):e100624. |
| 36, 42. | ↑ | De Bruyn H, Atashkadeh M, Cosyn J, van der Velde T. Clinical outcome and bone preservation of single TiUnite implants installed with flapless or flap surgery. → Clin Implant Dent Relat Res. 2011 Sep;13(3):175–83. |
| 37, 43. | ↑ | Rousseau P. Flapless and traditional dental implant surgery: an open, retrospective comparative study. → J Oral Maxillofac Surg. 2010 Sep;68(9):2299–306. |
| 38. | ↑ | Galindo-Moreno P, León-Cano A, Ortega-Oller I, Monje A, O’Valle F, Catena A. Marginal bone loss as success criterion in implant dentistry: beyond 2 mm. → Clin Oral Implants Res. 2015 Apr;26(4):e28–34. |
| 41. | ↑ | Nickening HJ, Wichmann M, Schlegel KA, Nkenke E, Eiter S. Radiographic evaluation of marginal bone levels during healing period, adjacent to parallel-screw cylinder implants inserted in the posterior zone of the jaws, placed with flapless surgery. → Clin Oral Implants Res. 2010 Dec;21(12):1386–93. |
| 44, 45. | ↑ | Froum SJ, Khouly I. Survival rates and bone and soft tissue level changes around one-piece dental implants placed with a flapless or flap protocol: 8.5-year results. → Int J Periodontics Restorative Dent. 2017 May–Jun;37(3):327–37. |
| 46. | ↑ | Prati C, Zamparini F, Pirani C, Gatto MR, Piattelli A, Gandolfi MG. Immediate early and delayed implants: a 2-year prospective cohort study of 131 transmucosal flapless implants placed in sites with different pre-extractive endodontic infections. → Implant Dent. 2017 Oct;26(5):654–63. |
| 47. | ↑ | Mainetti T, Lang NP, Bengazi F, Sbricoli L, Soto Cantero L, Botticelli D. Immediate loading of implants installed in a healed alveolar bony ridge or immediately after tooth extraction: an experimental study in dogs. → Clin Oral Implants Res. 2015 Apr;26(4):435–41. |
| 48. | ↑ | Mainetti T, Lang NP, Bengazi F, Favero V, Soto Cantero L, Botticelli D. Sequential healing at implants installed immediately into extraction sockets. An experimental study in dogs. |
| 49. | ↑ | Puisys A, Linkevicius T. The influence of mucosal tissue thickening on crestal bone stability around bone-level implants. A prospective controlled clinical trial. → Clin Oral Implants Res. 2015 Feb;26(2):123–9. |
| 50. | ↑ | Zweers J, Thomas RZ, Slot DE, Weisgold AS, Van der Weijden FG. Characteristics of periodontal biotype, its dimensions, associations and prevalence: a systematic review. → J Clin Periodontol. 2014 Oct;41(10):958–71. |
| 51, 53. | ↑ | Berglundh T, Lindhe J. Dimension of the periimplant mucosa. Biological width revisited. → J Clin Periodontol. 1996 Oct;23(10):971–3. |
| 54. | ↑ | Renvert S, Quirynen M. Risk indicators for peri-implantitis. A narrative review. → Clin Oral Implants Res. 2015 Sep;26 Suppl 11:15–44. |





Leave a Reply
Be the First to Comment!