New perspectives in periapical surgery: Flap detachment and retraction
May 8, 2018 / Categories: Digital Dentistry, Implant Dentistry

Cervera Ballester, Juan

Peñarrocha Oltra, David

Peñarrocha Diago, Maria

Soto Peñaloza, David
Abstract
An update is made of the aspects to be taken into account during flap detachment and retraction in periapical surgery as one of the key elements for treatment success. Raising of the flap and traction must be carried out firmly but gently in order to minimize trauma. This requires an adequate mucoperiosteal incision. Retraction separates the flap in order to facilitate access to and visibility of the bone without damaging the flap. The sulcus technique, described in apicoectomy of the mandibular premolars, allows safe stabilization of the retractor supported on the bone without harming the surrounding tissue. Such support can be complemented by placing a piece of dressing impregnated with epinephrine to improve hemostasis and minimize damage to the flap. Adequate soft-tissue management not only results in a better postoperative course, with less pain and inflammation, but also guarantees optimum wound healing. Furthermore, an adequate flap design will produce more efficient surgery with a shorter operating time.
Keywords
Periapical surgery, flap detachment, flap retraction.
Introduction
In periapical surgery, and after planned incision, the flap is raised and separated from the bone. In this regard, a full-thickness or mucoperiosteal flap (comprising mucosa, connective tissue and periosteum) is detached with the aim of securing sufficient access to the bone and adequate elimination of the diseased periapical tissue. It is important to detach the periosteum from the bone together with the flap in order to minimize bleeding during surgery, reduce inflammation and pain in the postoperative period, and facilitate healing.1Arens DE. Practical lessons in endodontic surgery. → Hanover Park: Quintessence; 1998. 216 p. 45-79. 2Peñarrocha Diago M, Martí Bowen E, Bonet Coloma C. Técnica quirúrgica. → In: Peñarrocha M, editor. Cirugía periapical. Barcelona: Ars Medica; 2004. p. 45–79. Once the flap has been raised, it is retracted in order to keep the bone surface visible and accessible, and to avoid damage to either the flap or the surrounding tissue during the operation.3Arens DE. Practical lessons in endodontic surgery. → Hanover Park: Quintessence; 1998. 216 p. 45-79. The present study aims to review all of the aspects to be taken into account during the detachment and retraction of the flap in periapical surgery.
Fig. 1
Preoperative digital panoramic radiograph with preoperative computed tomography scans.
Flap detachment
The surgical incisions delimit a flap comprising attached gingival tissue, free alveolar mucosa and a fibromucous or periosteal layer that must preserve its vitality and recover its physiological functions after being repositioned. Flap detachment should be performed firmly and gently, taking care to minimize trauma.4Peñarrocha Diago M, Martí Bowen E, Bonet Coloma C. Técnica quirúrgica. → In: Peñarrocha M, editor. Cirugía periapical. Barcelona: Ars Medica; 2004. p. 45–79. This requires a well-defined full-thickness incision with adequate placement of the periosteotome on the bone. During the process, it is useful to revise the incision with a fine dissector (Fig. 1) in order to eliminate any connective tissue or periosteal fibers that have not been dissected by the scalpel. Detachment has a series of particularities, depending on the type of flap involved.
Submarginal incision flap
After a well-defined full-thickness incision, detachment is carried out with a periosteotome held like a pencil and placed at the junction between the horizontal and vertical incisions, with the concave surface, of the instrument facing the bone (Figs. 2A & E). The periosteotome is kept in continuous contact with the bone surface in order to avoid flap tearing or fenestration caused by possible irregularities, such as bone crest exostosis. The instrument is then gradually displaced horizontally, along the incision line, in the apical direction. The flap is raised sufficiently to expose the bone overlying the periapical lesion (Figs. 2F & H).
Neumann intrasulcular incision flap
After completing the incision through the gingival sulcus, the papillae are carefully separated one by one with the help of a fine dissector. The papillae should detach easily if the sulcular incision has correctly sectioned the gingival fibers and their lingual prolongation (Figs. 3A–D). The periosteotome is then positioned at the angle formed by the vertical and horizontal incisions (Fig. 3B).
It must be taken into account that in the presence of periodontal disease the bone crest is blunted or flattened, and greater resistance to detachment in the apical direction may be experienced. In some cases, this is wrongly taken to indicate the presence of a fibrous insertion or resistant insertion of the periosteum, an atypical cementoenamel junction, or an erosive margin (noncarious neck lesion). A series of particularities can be found, depending on the presence of anatomical anomalies or alterations associated with the prior surrounding disease during detachment.
Identification of fibrous or epithelial tracts
In the presence of a long-standing fibrous or epithelial tract, the pathological tissue of the lesion may have become integrated into the mucosa and submucosa, and in this case the flap is first raised from the surrounding tissue. With the flap kept tense, the scalpel blade is then positioned parallel to the bone surface, and the flap is detached without perforating the mucosa. The tearing of frenula or muscle insertions poses no esthetic or functional problem, and these elements should be raised as part of the flap. Once the fistular or fibrous tract has been dissected, raising of the flap is continued (Figs. 4A–E).
Bone exostosis
The soft tissue overlying zones characterized by large bone volumes is very thin and can easily be perforated during detachment. In such cases, it is important to work with a sharp periosteotome, keeping it in continuous contact with the bone surface.5Arens DE. Practical lessons in endodontic surgery. → Hanover Park: Quintessence; 1998. 216 p. 45-79.
-

-
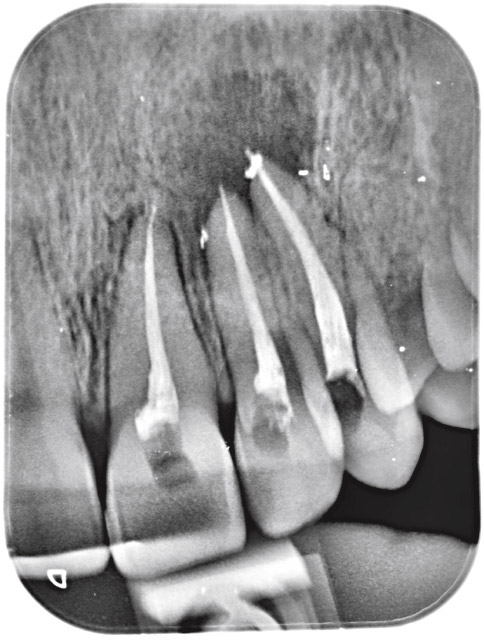
Fig. 2A
Radiograph of an apical lesion involving a maxillary left central incisor, lateral incisor and canine.
-

-
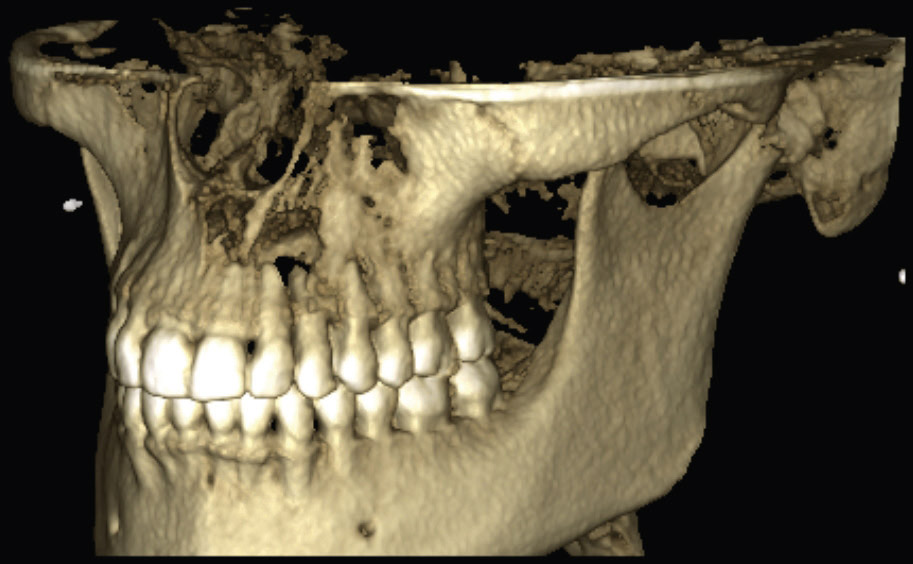
Fig. 2B
Tomographic scan showing the bone defect in the left anterior maxillary region.
-

-
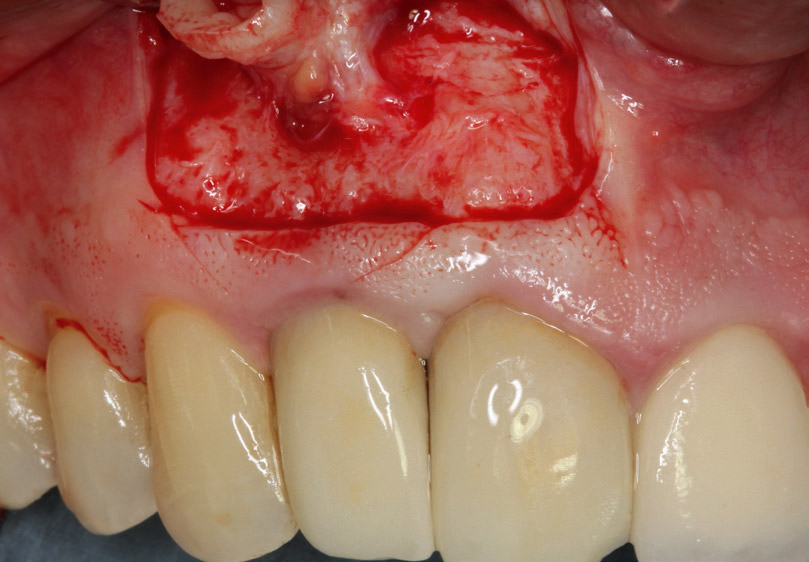
Fig. 2C
Extensive bone defect with cortical bone plate perforation.

-

-
Fig. 2D
Submarginal or full-thickness incision.

-

-
Fig. 2E
The incision is revised with the dissector, placing it between the horizontal and vertical incisions.

-

-
Fig. 2F
Detachment of the flap with the periosteotome, with its concave surface facing the bone.

-

-
Fig. 2G
Flap displaced to visualize the bone overlying the periapical lesion.

-

-
Fig. 2H
Intraoral radiograph after surgery. Perfect retrograde filling of the cavity can be observed.

-

-
Fig. 3A
Well-defined sulcular incision.

-

-
Fig. 3B
The incision is revised with the dissector, placing it at the angle formed by the horizontal and vertical incisions.

-

-
Fig. 3C
Insertion of the periosteotome, with its concave surface facing the bone horizontally, and checking detachment of the papillae.

-

-
Fig. 3D
Full apical retraction of the flap without tearing of the papillae.

-

-
Fig. 4A
Identification of a fibrous tract during flap detachment with submarginal incision.
-

-
Fig. 4B
With the flap kept tense, the scalpel blade is then positioned parallel to the bone surface, taking care not to perforate the mucosa.
-

-
Fig. 4C
Full apical retraction of the flap after dissection of the fistular and/or fibrous tract.

-

-
Fig. 4D
Intraoral photograph of perfect soft-tissue healing.

-

-
Fig. 4E
Intraoral radiograph showing the final aspect of retrograde filling.

-

-
Fig. 5A
Radiograph of a right central incisor with internal root resorption with an apical lesion.

-

-
Fig. 5B
Tomographic scan of the internal resorption and apical bone defect.
-

-
Fig. 5C
Radiograph after orthograde endodontic treatment insufficient to solve root resorption.

-

-
Fig. 5D
Intraoral photograph of the anterior maxillary zone.

-

-
Fig. 5E
Flap retraction. Note the retractor resting stably on the bone tissue.

-

-
Fig. 5F
Access to the apical lesion, care being taken not to affect flap integrity or the lesion.

-

-
Fig. 5G
Soft-tissue healing with a minimal scar, typical of a submarginal flap.

-

-
Fig. 5H
Radiograph showing complete retrograde filling of the internal resorption and cavity.

Flap retraction
Retraction serves to separate the flap, allowing the surgeon to visualize and access the bone without damaging the flap or the adjacent tissue.6Peñarrocha Diago M, Martí Bowen E, Bonet Coloma C. Técnica quirúrgica. → In: Peñarrocha M, editor. Cirugía periapical. Barcelona: Ars Medica; 2004. p. 45–79. The edges of the tissue retractor should rest upon the bone and must not affect flap integrity or the lesion. In order to correctly position the retractor, the flap should be raised sufficiently to adequately expose the bone over the periapical tissue of the affected root (Figs. 5A–H). Different types of retractors are available. Some authors advocate the use of retractors designed with a saw-tooth zone to prevent displacement.7Kim S. Soft tissue management: flap designs, retraction and suturing. → In: Kim S, editor. Color atlas of microsurgery in endodontics. Saunders; 2001. p. 75–84. Such instruments are not very comfortable to use, however, and have poor stability, thereby causing surgeon tension throughout the operation. Other authors prefer large retractors with designs adapted to the different dental groups and anatomical structures.8Rubinstein R. Magnification and illumination in apical surgery. → Endod Topics. 2005 Jul;11(1):56–77.
-

-
Fig. 6A
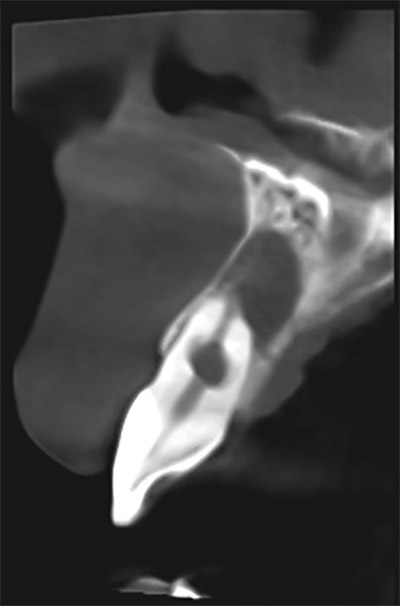
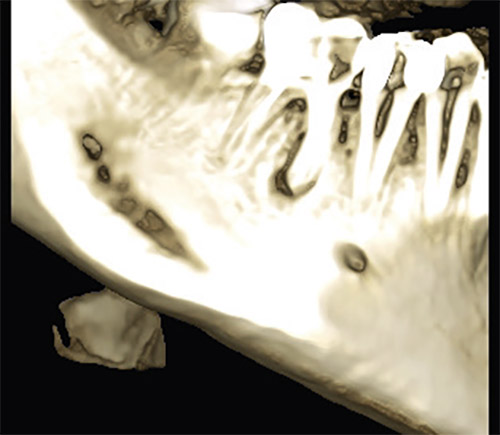
Tomographic scan of an apical lesion of a mandibular second premolar.
-

-
Fig. 6B
Intraoral photograph of the affected tooth. Note the integrity of the gingival margin and the band of keratinized gingiva.

-

-
Fig. 6C
A flap is raised through submarginal incision; after detachment, a narrow groove is made on the most apical portion of the bone tissue, taking care to avoid damage to the flap.

-

-
Fig. 6D
The retractor is positioned in the groove, keeping the soft tissue away from its trajectory.

-

-
Fig. 6E
A continuous suture is used to close the flap.

-

-
Fig. 6F
Intraoral radiograph after surgery. Perfect retrograde filling of the cavity can be observed.

Groove Technique
A useful option is the so-called groove technique,9Kim S. Soft tissue management: flap designs, retraction and suturing. → In: Kim S, editor. Color atlas of microsurgery in endodontics. Saunders; 2001. p. 75–84. which was developed for mandibular premolar apicoectomies with the aim of avoiding damage to the mental nerve. Nevertheless, it can be applied to any tooth and involves the creation of a narrow groove (of scant depth and measuring about 15 mm in length) using a small rounded drill. The tip of the retractor is inserted into this groove, and after firmly fixing the body of the retractor, gentle separation from the bone is performed to safely keep the soft tissue clear of the surgical field (Figs. 6A–F).
It is also possible to place a small piece of dressing impregnated with anesthetic solution between the separator and the flap in order to preserve flap integrity and improve bleeding control (Figs. 7A–E). The tissue tends to dry out when surgery is prolonged. In this case, the flap must be periodically and freely repositioned and humidified with sterile saline solution.10Kim S. Soft tissue management: flap designs, retraction and suturing. → In: Kim S, editor. Color atlas of microsurgery in endodontics. Saunders; 2001. p. 75–84. 11Tetsch P. Development of raised temperature after osteotomies. → J Maxillofac Surg. 1974 Aug;2(2–3):141–5. Optimum surgery is rapid, meticulous and decisive, and should be performed correctly and in an organized way.12Peñarrocha Diago M, Martí Bowen E, Bonet Coloma C. Técnica quirúrgica. → In: Peñarrocha M, editor. Cirugía periapical. Barcelona: Ars Medica; 2004. p. 45–79.
Conclusion
This meticulous surgical technique allows treatment of the soft tissue with delicacy, minimally injuring the vascularization, which is very important in oral surgery, and allowing good healing of the soft tissue and of the incisions. In addition, it achieves an adequate surgical field of work that will aid the clinician in being effective and quick in the surgical procedure, which means a reduced possibility of infection and drying of the tissue.
-

-
Fig. 7A
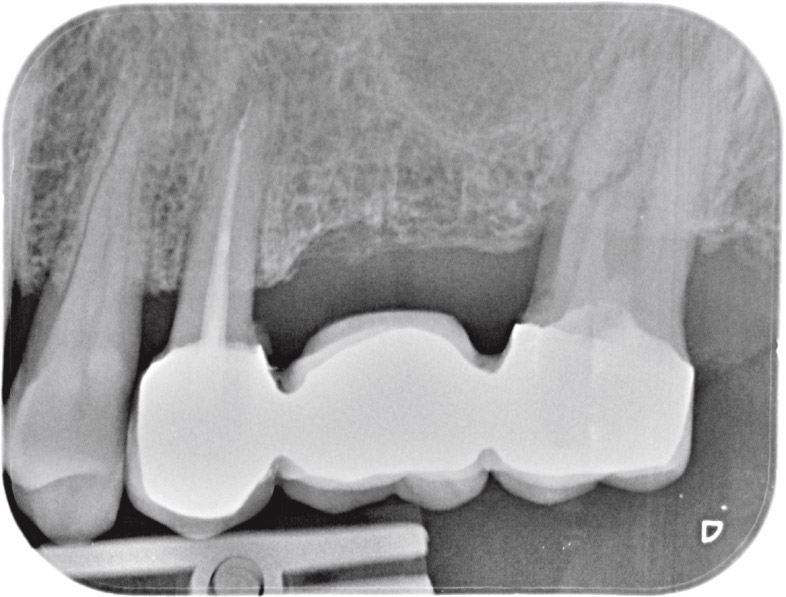
Radiograph of a maxillary second premolar with an apical lesion.
-

-
Fig. 7B
Intraoral photograph of the second premolar with a metal–ceramic crown and slight retraction of the gingival margin.

-

-
Fig. 7C
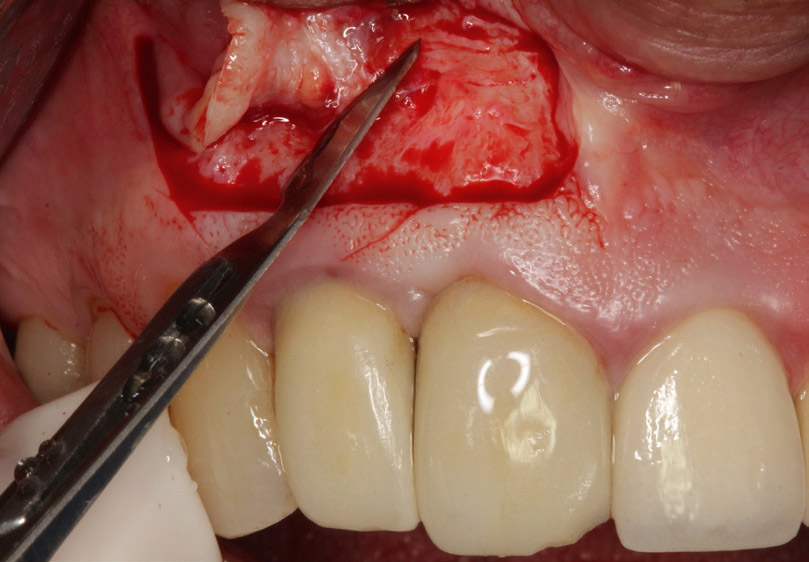
After flap detachment, a narrow groove is made on the bone tissue, always apical to the lesion of the affected tooth.

-

-
Fig. 7D
Before firmly positioning the retractor, a piece of dressing impregnated with epinephrine is inserted to preserve flap integrity and improve bleeding control.

-

-
Fig. 7E
Radiograph of a maxillary second premolar with an apical lesion.


Interview
with David Peñarrocha
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 5. | ↑ | Arens DE. Practical lessons in endodontic surgery. → Hanover Park: Quintessence; 1998. 216 p. 45-79. |
| 2, 12. | ↑ | Peñarrocha Diago M, Martí Bowen E, Bonet Coloma C. Técnica quirúrgica. → In: Peñarrocha M, editor. Cirugía periapical. Barcelona: Ars Medica; 2004. p. 45–79. |
| 3. | ↑ | Arens DE. Practical lessons in endodontic surgery. → Hanover Park: Quintessence; 1998. 216 p. 45-79. |
| 4, 6. | ↑ | Peñarrocha Diago M, Martí Bowen E, Bonet Coloma C. Técnica quirúrgica. → In: Peñarrocha M, editor. Cirugía periapical. Barcelona: Ars Medica; 2004. p. 45–79. |
| 7, 9, 10. | ↑ | Kim S. Soft tissue management: flap designs, retraction and suturing. → In: Kim S, editor. Color atlas of microsurgery in endodontics. Saunders; 2001. p. 75–84. |
| 8. | ↑ | Rubinstein R. Magnification and illumination in apical surgery. → Endod Topics. 2005 Jul;11(1):56–77. |
| 11. | ↑ | Tetsch P. Development of raised temperature after osteotomies. → J Maxillofac Surg. 1974 Aug;2(2–3):141–5. |





Leave a Reply
Be the First to Comment!