New perspectives in periapical surgery: Hemostasis
September 26, 2018 / Categories: Digital Dentistry, Implant Dentistry

Menéndez Nieto, Isabel

Cervera Ballester, Juan

Peñarrocha Diago, Maria

Peñarrocha Oltra, David
Abstract
Objective
The aim of the current investigation was to review techniques and materials available to achieve bleeding control during periapical surgery. An adequate bleeding control is crucial, since it improves vision in the surgical site, minimizes surgical time, enhances the root-end resection and filling, and reduces surgical blood loss, postsurgical hemorrhage and postsurgical swelling.
Method
An update is made of the aspects to be considered during bleeding control in periapical surgery.
Results
The hemostatic agents that have been proposed in the literature have characteristics that make them very different from each other, such as the mechanism of action, commercial presentation, hemostatic efficacy and systemic effects.
Conclusion
The hemostatic agents that have obtained the best results are ferric sulfate, calcium sulfate, aluminum chloride and epinephrine. Nevertheless, there is no consensus in the literature on which is the ideal hemostatic agent.
Keywords
Endodontic surgery; hemostatic agents; hemostasis; periradicular surgery.
Introduction
The ability to achieve sustained tissue hemostasis in the surgical site is crucial to the performance of periapical surgery. Adequate bleeding control improves vision in the surgical site, minimizes surgical time, enhances the surgical procedures (root-end resection, preparation and filling), and reduces surgical blood loss, postsurgical hemorrhage and postsurgical swelling.1Witherspoon DE, Gutmann JL. Haemostasis in periradicular surgery. → Int Endod J. 1996;29:135–49.
There is no consensus in the literature about what is the ideal hemostatic agent. Kim and Rethnam2Kim S, Rethnam S. Hemostasis in endodontic microsurgery. Dent Clin → North Am. 1997;41:499–511. established in 1997 that a good agent should achieve hemostasis within a short period, be easy to manipulate, be biocompatible, not impair or retard healing, and be relatively inexpensive and reliable.3Kim S, Rethnam S. Hemostasis in endodontic microsurgery. Dent Clin → North Am. 1997;41:499–511. The aim of the current investigation was to review techniques and materials available to achieve bleeding control during periapical surgery.
Hemorrhage control
The hemostatic agents that have been proposed in the literature have characteristics that make them very different from each other, such as the mechanism of action, commercial presentation, hemostatic efficacy and systemic effects.
Bone wax
Bone wax is a nonresorbable material composed of beeswax (88%) and isopropyl palmitate (12%). It is applied to the bony walls with pressure and its mechanism of action is mechanical, tamponading the narrow spaces. Its translucency and deep encrustation into the bone make its removal difficult.4Sauveur G, Roth F, Sobel M, Boucher Y. The control of haemorrhage at the operative site during periradicular surgery. → Int Endod J. 1999;32:225–8.
Ferric sulfate and calcium sulfate
The mechanism of action of ferric sulfate is chemical, producing the coagulation of proteins, so it acts in a similar way to cauterization.5Lemon RR, Steele PJ, Jeansonne BG. Ferric sulfate hemostasis: effect on osseous wound healing. Left in situ for maximum exposure. → J Endod. 1993 Apr;19(4):170–3. Lemon et al. and Jeansonne et al. studied the effects of ferric sulfate in rabbit mandibles; they achieved good hemostasis for 5 min.6Lemon RR, Steele PJ, Jeansonne BG. Ferric sulfate hemostasis: effect on osseous wound healing. Left in situ for maximum exposure. → J Endod. 1993 Apr;19(4):170–3.,7Jeansonne BG, Boggs WS, Lemon RR. Ferric sulfate hemostasis: effect on osseous wound healing. II. With curettage and irrigation. → J Endod. 1993 Apr;19(4):174–6. Scarano et al. compared the hemostatic efficacy of 20% ferric sulfate, calcium sulfate and gauze tamponade, and concluded that calcium sulfate produced a good level of hemostasis.8Scarano A, Artese L, Piattelli A, Carinci F, Mancino C, Iezzi G. Hemostasis control in endodontic surgery: A comparative study of calcium sulfate versus gauzes and versus ferric sulfate. → J Endod. 2012;38:20–3.
Epinephrine
The amine-type sympathomimetic vasoconstrictors have been used as topical agents for the control of hemorrhage in periapical surgery9Kim S, Rethnam S. Hemostasis in endodontic microsurgery. Dent Clin → North Am. 1997;41:499–511. (Figs. 1–8). Epinephrine produces vasoconstriction by stimulation of α-adrenergic receptors. Besner suggested that its use in periapical surgery can produce a systemic cardiovascular response.10Besner E. Systemic effects of racemic epinephrine when applied to the bone cavity during periapical surgery. → Va Dent J. 1972;49:9–12. Vickers et al. evaluated the hemostatic efficacy and cardiovascular effects of ferric sulfate and pellets impregnated with racemic epinephrine, and concluded that both agents produced surgical hemostasis and found no statistically significant differences in systemic cardiovascular parameters with either of the materials.11Vickers FJ, Baumgartner JC, Marshall G. Hemostatic efficacy and cardiovascular effects of agents used during endodontic surgery. → J Endod. 2002;28:322–3. In a similar study, Vy et al. concluded that collagen sponges saturated with epinephrine provided excellent bleeding control without changes in blood pressure or heart rate.12Vy CH, Baumgartner JC, Marshall JG. Cardiovascular effects and efficacy of a hemostatic agent in periradicular surgery. → J Endod. 2004;30:379–83.
Aluminum chloride
In 2001, von Arx et al. used a paste composed of aluminum chloride and kaolin as a hemostatic agent,13Von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: An experimental study of their efficacy and tissue reactions. → Int Endod J. 2006;39:800–8. which is usually used to produce gingival retraction.14Pescatore C. A predictable gingival retraction system. → Compend Contin Educ Dent. 2002 Jan;23(1 Suppl):7–12; quiz 18.,15Shannon A. Expanded clinical uses of a novel tissue-retraction material. → Compend Contin Educ Dent. 2002 Jan;23(1 Suppl):3–6; quiz 18. They applied different hemostatic agents in the calvaria of 6 rabbits: bone wax, ferric sulfate (Stasis), aluminum chloride (Expasyl) and a combination of Expasyl and Stasis.16Von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: An experimental study of their efficacy and tissue reactions. → Int Endod J. 2006;39:800–8. They concluded that Expasyl alone or in combination with Stasis was the most effective agent.17Von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: An experimental study of their efficacy and tissue reactions. → Int Endod J. 2006;39:800–8. Jensen et al. used the same study design to compare 5 hemostatic methods: Expasyl and Stasis; Expasyl, Stasis and freshening the bone defect with a bur; Spongostan; Spongostan and epinephrine; and electrocauterization.18Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, Von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. → Int Endod J. 2010 Jan;43(1):57–63. The most effective methods in the reduction of bleeding were Expasyl and Stasis combined (P < 0.05) and electrocauterization. Menéndez-Nieto et al. compared the hemostatic efficacy of epinephrine and aluminum chloride in 99 patients and concluded that aluminum chloride produced better results (P < 0.05;19Menéndez-Nieto I, Cervera-Ballester J, Maestre-Ferrín L, Blaya-Tárraga JA, Peñarrocha-Oltra D, Peñarrocha-Diago M. Hemostatic Agents in Periapical Surgery: A Randomized Study of Gauze Impregnated in Epinephrine versus Aluminum Chloride. → J Endod. 2016; Figs. 9–14).
-

-
Fig. 1
Radiograph before periapical surgery.

-

-
Fig. 2
Clinical photograph before surgery.

-

-
Fig. 3
Before application of a hemostatic agent.

-

-
Fig. 4
A gauze impregnated in epinephrine was placed into the bony crypt and pressure was applied for 2 min.

-

-
Fig. 5
Hemostasis after application of the epinephrine.

-

-
Fig. 6
Evaluation of the retrograde filling with an endoscope.

-

-
Fig. 7
Tension-free soft-tissue flap closure.

-

-
Fig. 8
Periapical radiograph after periapical surgery.

-

-
Fig. 9
Clinical photograph before surgery.

-

-
Fig. 10
Aluminum chloride was applied with a spatula to the bony crypt for 2 min.

Other agents and techniques
Resorbable gelatin-based sponges,20Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, Von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. → Int Endod J. 2010 Jan;43(1):57–63.,21Ibarrola JL, Bjorenson JE, Peter Austin B, Gerstein H. Osseous reactions to three hemostatic agents. → J Endod. 1985 Feb;11(2):75–83. oxidized cellulose,22Ibarrola JL, Bjorenson JE, Peter Austin B, Gerstein H. Osseous reactions to three hemostatic agents. → J Endod. 1985 Feb;11(2):75–83. electrocauterization,23Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, Von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. → Int Endod J. 2010 Jan;43(1):57–63.,24Rud J, Munksgaard EC, Andreasen JO, Rud V, Asmussen E. Retrograde root filling with composite and a dentin-bonding agent. 1. → Endod Dent Traumatol. 1991 Jun;7(3):118–25.,25Pecora G, De Leonardis D, Ibrahim N, Bovi M, Cornelini R. The use of calcium sulphate in the surgical treatment of a “through and through” periradicular lesion. → Int Endod J. 2001 Apr;34(3):189–97. carbon dioxide laser,26Miserendino LJ. The laser apicoectomy: Endodontic application of the CO2laser for periapical surgery. → Oral Surgery, Oral Med Oral Pathol. 1988;66:615–9. chitosan27Azargoon H, Williams BJ, Solomon ES, Kessler HP, He J, Spears R. Assessment of hemostatic efficacy and osseous wound healing using HemCon dental dressing. → J Endod. 2011;37:807–11. and plant-based hemostatic agents28Dinçol ME, Ozbas H, Yilmaz B, Ersev H, Gokyay S, Olgac V. Effect of the plant-based hemostatic agent Ankaferd Blood Stopper® on the biocompatibility of mineral trioxide aggregate. → BMC Oral Health. 2016;16:1–9.,29Nabavizadeh MR, Zargaran A, Moazami F, Askari F, Sahebi S, Farhadpoor A, et al. Comparison of the Hemostatic Activity of Quercus persica Jaub. & Spach. (Oak) With Ferric Sulfate in Bony Crypts. → J Evidence-Based Complement Altern Med. 2016;21:34–8. have been used to control hemorrhage in periapical surgery; however, their scientific evidence is limited.
Regarding adverse effects, in the presence of bone wax, scarring of the bony crypt is poor, fibers of connective tissue appear, and there is no bone or hematopoietic tissue.30Finn MD, Schow SR, Schneiderman ED. Osseous regeneration in the presence of four common hemostatic agents. → J Oral Maxillofac Surg. 1992 Jun;50(6):608–12. In addition to delaying healing, bone wax increases the predisposition to infection31Nelson DR, Buxton TB, Luu QN, Rissing JP. The promotional effect of bone wax on experimental Staphylococcus aureus osteomyelitis. → J Thorac Cardiovasc Surg. 1990;99:977–80. and produces chronic inflammation with foreign body reactions.32Nelson DR, Buxton TB, Luu QN, Rissing JP. The promotional effect of bone wax on experimental Staphylococcus aureus osteomyelitis. → J Thorac Cardiovasc Surg. 1990;99:977–80.,33Aurelio J, Chenail B, Gerstein H. Foreign-body reaction to bone wax. Report of a case. → Oral Surg Oral Med Oral Pathol. 1984 Jul;58(1):98–100. ,34Solheim E, Pinholt EM, Bang G, Sudmann E. Effect of local hemostatics on bone induction in rats: a comparative study of bone wax, fibrin–collagen paste, and bioerodible polyorthoester with and without gentamicin. → J Biomed Mater Res. 1992 Jun;26(6):791–800. A histologic study showed a marked inflammatory tissue response toward aluminum chloride and bone wax within the immediate site of application, but no adverse tissue reactions were seen in the vicinity of the bone defects.35Von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: An experimental study of their efficacy and tissue reactions. → Int Endod J. 2006;39:800–8. The authors recommended that, before wound closure, the bony crypt be curetted or freshened using rotary instruments to remove any foreign material. Jensen et al. found that aluminum chloride and electrocauterization triggered adverse tissue reactions (necrotic bone, inflammatory cells, lack of bone repair); however, this tissue damage was not observed when the superficial bone layer was removed with rotary instruments.36Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, Von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. → Int Endod J. 2010 Jan;43(1):57–63. Peñarrocha-Diago et al.37Peñarrocha-Diago M, Maestre-Ferrín L, Peñarrocha-Oltra D, Gay-Escoda C, von-Arx T, Peñarrocha-Diago M. Pain and swelling after periapical surgery related to the hemostatic agent used: anesthetic solution with vasoconstrictor or aluminum chloride. → Med Oral Patol Oral Cir Bucal. 2012 Jul 1;17(4):e594–600. observed that the patients for whom aluminum chloride was used as the hemostatic agent suffered greater postoperative swelling than the patients treated with a vasoconstrictor. When ferric sulfate was used,38Lemon RR, Steele PJ, Jeansonne BG. Ferric sulfate hemostasis: effect on osseous wound healing. Left in situ for maximum exposure. → J Endod. 1993 Apr;19(4):170–3.,39Jeansonne BG, Boggs WS, Lemon RR. Ferric sulfate hemostasis: effect on osseous wound healing. II. With curettage and irrigation. → J Endod. 1993 Apr;19(4):174–6. normal healing with a slight foreign body reaction after curetting the cavity thoroughly and irrigating with saline was found. When the material was not completely removed from the cavity, foreign body reactions that delayed healing occurred, and in 2 of 10 cases, the specimens showed abscess formation in the center of the osseous defect40Lemon RR, Steele PJ, Jeansonne BG. Ferric sulfate hemostasis: effect on osseous wound healing. Left in situ for maximum exposure. → J Endod. 1993 Apr;19(4):170–3. No adverse tissue reaction was found when calcium sulfate, epinephrine, resorbable gelatin-based sponges or chitosan were used.41Jang Y, Kim H, Roh BD, Kim E. Biologic response of local hemostatic agents used in endodontic microsurgery. → Restor Dent Endod. 2014 May;39(2):79–88.,42Kamoh A, Swantek J. Hemostasis in oral surgery. → Dent Clin North Am. 2012 Jan;56(1):17–23, vii.
Conclusion
Hemorrhage control is a key aspect of periapical surgery: A hemostatic agent should be biocompatible, easy to manipulate and able to achieve hemostatic efficacy in a short period. The hemostatic agents that have obtained good results are ferric sulfate and aluminum chloride; however, the tissue damage produced when the superficial bone layer was not removed and its relation to the prognosis must be considered. Other agents that have demonstrated good hemostatic efficacy without foreign body reactions are calcium sulfate and epinephrine.
Competing interests
The authors declare that they have no competing interests.
-

-
Fig. 11
Hemostasis after application of the aluminum chloride. The superficial bone layer was removed with rotary instruments.

-

-
Fig. 12
Evaluation of the retrograde filling with an endoscope.

-
-
Fig. 13
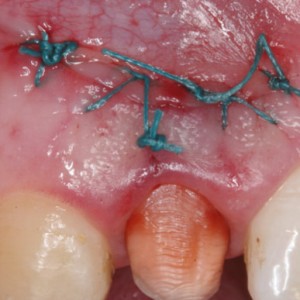
Tension-free soft-tissue flap closure.

-
-
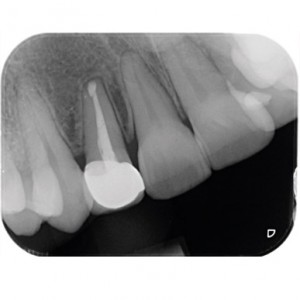
Fig. 14
Periapical radiograph 1 year after the periapical surgery.

Interview
with Isabel Menéndez Nieto
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1. | ↑ | Witherspoon DE, Gutmann JL. Haemostasis in periradicular surgery. → Int Endod J. 1996;29:135–49. |
| 2, 3, 9. | ↑ | Kim S, Rethnam S. Hemostasis in endodontic microsurgery. Dent Clin → North Am. 1997;41:499–511. |
| 4. | ↑ | Sauveur G, Roth F, Sobel M, Boucher Y. The control of haemorrhage at the operative site during periradicular surgery. → Int Endod J. 1999;32:225–8. |
| 5, 6, 38, 40. | ↑ | Lemon RR, Steele PJ, Jeansonne BG. Ferric sulfate hemostasis: effect on osseous wound healing. Left in situ for maximum exposure. → J Endod. 1993 Apr;19(4):170–3. |
| 7, 39. | ↑ | Jeansonne BG, Boggs WS, Lemon RR. Ferric sulfate hemostasis: effect on osseous wound healing. II. With curettage and irrigation. → J Endod. 1993 Apr;19(4):174–6. |
| 8. | ↑ | Scarano A, Artese L, Piattelli A, Carinci F, Mancino C, Iezzi G. Hemostasis control in endodontic surgery: A comparative study of calcium sulfate versus gauzes and versus ferric sulfate. → J Endod. 2012;38:20–3. |
| 10. | ↑ | Besner E. Systemic effects of racemic epinephrine when applied to the bone cavity during periapical surgery. → Va Dent J. 1972;49:9–12. |
| 11. | ↑ | Vickers FJ, Baumgartner JC, Marshall G. Hemostatic efficacy and cardiovascular effects of agents used during endodontic surgery. → J Endod. 2002;28:322–3. |
| 12. | ↑ | Vy CH, Baumgartner JC, Marshall JG. Cardiovascular effects and efficacy of a hemostatic agent in periradicular surgery. → J Endod. 2004;30:379–83. |
| 13, 16, 17, 35. | ↑ | Von Arx T, Jensen SS, Hänni S, Schenk RK. Haemostatic agents used in periradicular surgery: An experimental study of their efficacy and tissue reactions. → Int Endod J. 2006;39:800–8. |
| 14. | ↑ | Pescatore C. A predictable gingival retraction system. → Compend Contin Educ Dent. 2002 Jan;23(1 Suppl):7–12; quiz 18. |
| 15. | ↑ | Shannon A. Expanded clinical uses of a novel tissue-retraction material. → Compend Contin Educ Dent. 2002 Jan;23(1 Suppl):3–6; quiz 18. |
| 18, 20, 23, 36. | ↑ | Jensen SS, Yazdi PM, Hjørting-Hansen E, Bosshardt DD, Von Arx T. Haemostatic effect and tissue reactions of methods and agents used for haemorrhage control in apical surgery. → Int Endod J. 2010 Jan;43(1):57–63. |
| 19. | ↑ | Menéndez-Nieto I, Cervera-Ballester J, Maestre-Ferrín L, Blaya-Tárraga JA, Peñarrocha-Oltra D, Peñarrocha-Diago M. Hemostatic Agents in Periapical Surgery: A Randomized Study of Gauze Impregnated in Epinephrine versus Aluminum Chloride. → J Endod. 2016; |
| 21, 22. | ↑ | Ibarrola JL, Bjorenson JE, Peter Austin B, Gerstein H. Osseous reactions to three hemostatic agents. → J Endod. 1985 Feb;11(2):75–83. |
| 24. | ↑ | Rud J, Munksgaard EC, Andreasen JO, Rud V, Asmussen E. Retrograde root filling with composite and a dentin-bonding agent. 1. → Endod Dent Traumatol. 1991 Jun;7(3):118–25. |
| 25. | ↑ | Pecora G, De Leonardis D, Ibrahim N, Bovi M, Cornelini R. The use of calcium sulphate in the surgical treatment of a “through and through” periradicular lesion. → Int Endod J. 2001 Apr;34(3):189–97. |
| 26. | ↑ | Miserendino LJ. The laser apicoectomy: Endodontic application of the CO2laser for periapical surgery. → Oral Surgery, Oral Med Oral Pathol. 1988;66:615–9. |
| 27. | ↑ | Azargoon H, Williams BJ, Solomon ES, Kessler HP, He J, Spears R. Assessment of hemostatic efficacy and osseous wound healing using HemCon dental dressing. → J Endod. 2011;37:807–11. |
| 28. | ↑ | Dinçol ME, Ozbas H, Yilmaz B, Ersev H, Gokyay S, Olgac V. Effect of the plant-based hemostatic agent Ankaferd Blood Stopper® on the biocompatibility of mineral trioxide aggregate. → BMC Oral Health. 2016;16:1–9. |
| 29. | ↑ | Nabavizadeh MR, Zargaran A, Moazami F, Askari F, Sahebi S, Farhadpoor A, et al. Comparison of the Hemostatic Activity of Quercus persica Jaub. & Spach. (Oak) With Ferric Sulfate in Bony Crypts. → J Evidence-Based Complement Altern Med. 2016;21:34–8. |
| 30. | ↑ | Finn MD, Schow SR, Schneiderman ED. Osseous regeneration in the presence of four common hemostatic agents. → J Oral Maxillofac Surg. 1992 Jun;50(6):608–12. |
| 31, 32. | ↑ | Nelson DR, Buxton TB, Luu QN, Rissing JP. The promotional effect of bone wax on experimental Staphylococcus aureus osteomyelitis. → J Thorac Cardiovasc Surg. 1990;99:977–80. |
| 33. | ↑ | Aurelio J, Chenail B, Gerstein H. Foreign-body reaction to bone wax. Report of a case. → Oral Surg Oral Med Oral Pathol. 1984 Jul;58(1):98–100. |
| 34. | ↑ | Solheim E, Pinholt EM, Bang G, Sudmann E. Effect of local hemostatics on bone induction in rats: a comparative study of bone wax, fibrin–collagen paste, and bioerodible polyorthoester with and without gentamicin. → J Biomed Mater Res. 1992 Jun;26(6):791–800. |
| 37. | ↑ | Peñarrocha-Diago M, Maestre-Ferrín L, Peñarrocha-Oltra D, Gay-Escoda C, von-Arx T, Peñarrocha-Diago M. Pain and swelling after periapical surgery related to the hemostatic agent used: anesthetic solution with vasoconstrictor or aluminum chloride. → Med Oral Patol Oral Cir Bucal. 2012 Jul 1;17(4):e594–600. |
| 41. | ↑ | Jang Y, Kim H, Roh BD, Kim E. Biologic response of local hemostatic agents used in endodontic microsurgery. → Restor Dent Endod. 2014 May;39(2):79–88. |
| 42. | ↑ | Kamoh A, Swantek J. Hemostasis in oral surgery. → Dent Clin North Am. 2012 Jan;56(1):17–23, vii. |





Leave a Reply
Be the First to Comment!