Periimplant soft-tissue and bone levels around dental implants with different neck designs and neck surface treatments: A retrospective cohort study with 3-year follow-up
December 7, 2017 / Categories: Digital Dentistry, Implant Dentistry
,

Ribes Lainez, Natalia

Alba, Monreal Bello

Fuster Torres, María Ángeles

Peñarrocha Diago, Miguel
Abstract
Objective
The objective of the study was to assess the influence of the implant neck designs and neck surface treatments on periimplant tissue health and radiographic bone loss after 3 years of functional loading of implants with the same body and prosthetic connection.
Materials and methods
A retrospective cohort study was carried out in the Oral Surgery and Implantology Unit of the University of Valencia, Valencia, Spain. Patients treated with implants presenting a neck design without microthreads and a 1.5 mm machined surface and implants with a 0.7 mm machined surface and microthreads with a rough surface with a minimum of 3 years of follow-up were included. Probing pocket depth, bleeding on probing, presence of mucositis and width of keratinized mucosa were assessed 3 years after prosthesis placement. Marginal bone loss was measured in intraoral radiographs by calculating the difference between the measurements at the prosthesis placement and 3 years after loading.
Results
The final sample consisted of 27 partially edentulous patients with a total of 51 dental implants. No significant differences were observed on evaluating probing pocket depth (P = 0.195), bleeding on probing (P = 0.524), presence of mucositis (P = 0.916), width of keratinized mucosa (P = 0.435) and marginal bone loss (P = 0.217) between both groups.
Conclusion
Within the limitations of the present investigation, implant neck designs and neck surface treatments were not significantly related to periimplant tissue health and radiographic bone loss after 3 years of follow-up.
Keywords
Periimplant hard tissue, periimplant soft tissue, radiology, CT imaging, clinical research, clinical trials.
Introduction
Bone loss after implant integration and through time of function usually begins at the neck and spreads to the first thread of the body or to the first contact between the bone and the rough surface of the implant,1Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success.
→ Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. and can be divided into 2 different phases depending on the time of occurrence.2Lee DW, Choi YS, Park KH, Kim CS, Moon IS. Effect of microthread on the maintenance of marginal bone level: a 3-year prospective study.
→ Clin Oral Implants Res. 2007 Aug;18(4):465–70.3Manz MC. Factors associated with radiographic vertical bone loss around implants placed in a clinical study.
→ Ann Periodontol. 2000 Dec;5(1):137–51.4Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. → Ann Periodontol. 2000 Dec;5(1):119–28.5Bratu EA, Tandlich M, Shapira L. A rough surface implant neck with microthreads reduces the amount of marginal bone loss: a prospective clinical study. → Clin Oral Implants Res. 2009 Aug;20(8):827–32. The first, early bone loss, is related to re-entry surgery after the healing time or prosthetic connection,6Hartman GA, Cochran DL. Initial implant position determines the magnitude of crestal bone remodeling.
→ J Periodontol. 2004 Apr;75(4):572–7. and the second, late bone loss, emerges during the time of implant and prosthesis function.7Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. → Ann Periodontol. 2000 Dec;5(1):119–28. 8Oh TJ, Yoon J, Misch CE, Wang HL. The causes of early implant bone loss: myth or science?
→ J Periodontol. 2002 Mar;73(3):322–33.9. Kronstrom M, Svenson B, Hellman M, Persson GR. Early implant failures in patients treated with Branemark System titanium dental implants: a retrospective study.
→ Int J Oral Maxillofac Implants. 2001 Mar–Apr;16(2):201–7. Criteria for evaluation of implant success are generally based on clinical and radiological aspects, such as probing depth, implant mobility and periimplant bone changes.10. Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors contributing to failures of osseointegrated oral implants. (II). Etiopathogenesis.
→ Eur J Oral Sci. 1998 Jun;106(3):721–64. It has been reported that the criteria for successful implant therapy include a median marginal bone loss of < 1–1.5 mm during the first year, followed by an annual rate of vertical bone loss of ≤ 0.2 mm.11Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz- Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference.
→ Implant Dent. 2008 Mar;17(1):5–15.
In the last few decades, it has been suggested that marginal bone loss is dependent on several factors, such as the implant neck surface design12. Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success.
→ Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25.13Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. → Ann Periodontol. 2000 Dec;5(1):119–28.14Lang NP, Jepsen S; Working Group 4. Implant surfaces and design (Working Group 4).
→ Clin Oral Implants Res. 2009 Sep;20 Suppl 4:228–31. 15Shin YK, Han CH, Heo SJ, Kim S, Chun HJ. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year.
→ Int J Oral Maxillofac Implants. 2006 Sep–Oct;21(5):789–94.16Nickenig HJ, Wichmann M, Schlegel KA, Nkenke E, Eitner S. Radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs.
→ Clin Oral Implants Res. 2009 Jun;20(6):550–4. and characteristics.17Nickenig HJ, Wichmann M, Happe A, Zoller JE, Eitner S. A 5-year prospective radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs.
→ J Craniomaxillofac Surg. 2013 Oct;41(7):564–8.18Penarrocha M, Palomar M, Sanchis JM, Guarinos J, Balaguer J. Radiologic study of marginal bone loss around 108 dental implants and its relationship to smoking, implant location, and morphology.
→ Int J Oral Maxillofac Implants. 2004 Nov–Dec;19(6):861–7. It has been proposed that bone retention elements such as microthreads and a rough surface at the implant neck might help stabilize the marginal bone.19Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success.
→ Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25.20Shin YK, Han CH, Heo SJ, Kim S, Chun HJ. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year.
→ Int J Oral Maxillofac Implants. 2006 Sep–Oct;21(5):789–94.21. Hansson S. The implant neck: smooth or provided with retention elements. A biomechanical approach.
→ Clin Oral Implants Res. 1999 Oct;10(5):394–405.22Tan WC, Lang NP, Schmidlin K, Zwahlen M, Pjetursson BE. The effect of different implant neck configurations on soft and hard tissue healing: a randomized-controlled clinical trial.
→ Clin Oral Implants Res. 2011 Jan;22(1):14–9. Although the conventional smooth implant neck allows the least accumulation of plaque23Teughels W, Van Assche N, Sliepen I, Quirynen M. Effect of material characteristics and/or surface topography on biofilm development.
→ Clin Oral Implants Res. 2006 Oct;17 Suppl 2:68–8124Baldi D, Menini M, Pera F, Ravera G, Pera P. Plaque accumulation on exposed titanium surfaces and peri-implant tissue behavior. A preliminary 1-year clinical study.
→ Int J Prosthodont. 2009 Sep–Oct;22(5):447–55. several studies have evaluated marginal bone loss according to the implant neck involved—machined implant necks and rough necks with microthreads—and have shown more marginal bone loss around these implants compared with implants with a rough surface topography at the implant neck.25Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. → Ann Periodontol. 2000 Dec;5(1):119–28. 26Shin YK, Han CH, Heo SJ, Kim S, Chun HJ. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year.
→ Int J Oral Maxillofac Implants. 2006 Sep–Oct;21(5):789–94. 27Nickenig HJ, Wichmann M, Schlegel KA, Nkenke E, Eitner S. Radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs.
→ Clin Oral Implants Res. 2009 Jun;20(6):550–4. 28Piao CM, Lee JE, Koak JY, Kim SK, Rhyu IC, Han CH, Herr Y, Heo SJ. Marginal bone loss around three different implant systems: radiographic evaluation after 1 year.
→ J Oral Rehabil. 2009 Oct;36(10):748–54. The relatively smooth, machined coronal portion is designed to end slightly above the gingival margin of the periimplant soft tissue, thus making the microgap or interface between implant and restoration easily accessible for oral hygiene and resulting in a supragingival location of the crown margin.29. Hanggi MP, Hanggi DC, Schoolfield JD, Meyer J, Cochran DL, Hermann JS. Crestal bone changes around titanium implants. Part I: a retrospective radiographic evaluation in humans comparing two non-submerged implant designs with different machined collar lengths.
→ J Periodontol. 2005 May;76(5):791–802. Lang et al. in a consensus report concluded that prospective controlled studies on the effects of different implant designs and surfaces had demonstrated that marginal bone levels were generally well preserved after installation of the dental prosthesis (at least for fixed restorations) on a variety of implant types (cumulative bone loss: < 0.5 mm after 3 years).30Lang NP, Jepsen S; Working Group 4. Implant surfaces and design (Working Group 4).
→ Clin Oral Implants Res. 2009 Sep;20 Suppl 4:228–31. However, these studies had a 1-year follow-up and there are no clinical studies comparing the long-term influence of different designs and surface treatments of implant necks on periimplant tissue. The purpose of this study was to assess the effect of the implant neck designs and neck surface treatments on periimplant tissue health and radiographic bone loss after 3 years of functional loading of implants with the same body and prosthetic connection but different neck designs.
Materials and methods
Study design and sample
A retrospective cohort study was carried out in the Oral Surgery and Implantology Unit of the University of Valencia, Valencia, Spain, between September 2015 and December 2016. This study complied with the ethical principles for medical research involving human subjects established in the Declaration of Helsinki of 1975, as revised in 2013, of the World Medical Assembly. All of the patients received information about the study and were asked to sign a written informed consent form before taking part. The study design was approved by the ethics board of the University of Valencia (approval number: H1467620442582).
Patients who had received single or partial prosthetic rehabilitations on TSA or TSA Advance implants (Phibo, Barcelona, Spain), had a minimum of 3 years of follow-up and who agreed to participate in the study and signed an informed consent were included. Patients who had undergone bone grafting procedures (block bone grafts or guided bone regeneration), had immediate post-extraction implants, had systemic diseases, were undergoing drug treatments capable of affecting gingival health, or had a history of bisphosphonate use during control visits, as well as pregnant or nursing women and patients with missing information, were excluded. Patients were classified into 2 cohorts according to the implant design:
- group A (TSA): patients treated with implants presenting a neck design without microthreads, with a 1.5 mm machined surface and an internal connection and without platform switching (Fig. 1a); and
- group B (TSA Advance): patients treated with implants presenting a neck design with a 0.7 mm machined surface and microthreads with a rough surface and an internal connection and without platform switching (Fig. 1b).


Macrodesign of (a) TSA and (b) TSA Advance implants.
Surgical procedure
The surgery was performed under local anesthesia with 4% articaine with 1:100,000 epinephrine (Inibsa, Lliçà de Vall, Spain). A crestal incision was made, and a full-thickness mucoperiosteal flap was raised. The drilling sequence recommended by the manufacturer was followed. Implants were placed at a torque of 35 N and positioned with the limit between rough and polished surfaces at crestal level. Suturing was carried out with 4-0 sutures (Supramid, B. Braun, Barcelona, Spain).
All of the patients received postoperative treatment: 500 mg of amoxicillin (Clamoxyl, GlaxoSmithKline, Madrid, Spain) 3 times daily for 7 days, 600 mg of ibuprofen (Bexistar, Bacino, Barcelona, Spain) to be taken as needed, a 0.12% chlorhexidine mouthwash (GUM, Sunstar, Chicago, Ill., U.S.) twice daily for 2 weeks and brushing with a chlorhexidine toothpaste. The sutures were removed 8–10 days after surgery.
Data collection and follow-up
All of the surgeries were carried out by 1 experienced surgeon (MPD) and control visits were performed by 2 trained and calibrated clinicians at prosthesis placement (T0) and at 6 and 12 months and 3 years after prosthesis placement (T1).
The following variables were collected retrospectively: sex, age, smoking habit (< 10 cigarettes/ day, 10–20 cigarettes/day, > 20 cigarettes/day), implant diameter and length, implant position (anterior, premolar or molar), arch (maxilla or mandible) and antagonist teeth (natural, implant, absent). A millimetric calibrated periodontal probe (Hawe Neos Probe 1395, Hawe, U.K.) was used to assess the following clinical variables:
- probing pocket depth (PPD), measured from the gingival margin to the deepest part of the periimplant pocket, at 6 locations per implant (mesiobuccal, buccal, distobuccal, mesiolingual/- palatal, lingual/palatal and distolingual/- palatal) choosing the largest value;
- bleeding on probing (BoP);
- presence of mucositis, understood as inflammation of the periimplant mucosa without progressing to crestal bone loss;31Albrektsson T, Buser D, Chen ST, Cochran D, DeBruyn H, Jemt T, Koka S, Nevins M, Sennerby L, Simion M, Taylor TD, Wennerberg A. Statements from the Estepona consensus meeting on peri-implantitis, February 2–4, 2012.
→ Clin Implant Dent Relat Res. 2012 Dec;14(6):781–2. and - width of keratinized mucosa in the buccal and lingual region.
Intraoral radiographs were used to measure marginal bone loss. Radiographic exploration was carried out using the intraoral XMind system (Groupe Satelec-Pierre Rolland, Bordeaux, France) and the RVG intraoral digital sensor (Kodak Dental System, Atlanta, Ga., U.S.). In order to reproduce the X-ray angles in posterior reviews, XCP positioners were used (DENTSPLY, Des Plaines, Ill., U.S.), placing the guide bar parallel to the direction of the X-ray beam and perpendicular to the digital sensor.
All of the measurements were carried out by 2 examiners (different from the surgeon), who were initially calibrated to evaluate the interexaminer error using the Dahlberg formula and coefficient of variation. Each examiner measured 30 radiographs to evaluate the interexaminer error. The error according to Dahlberg’s test ranged between 0.63 and 0.93 mm for the various parameters and the coefficient of variation between 5.2% and 6.4%.
-
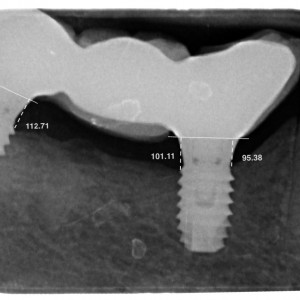
- Fig. 2a
-
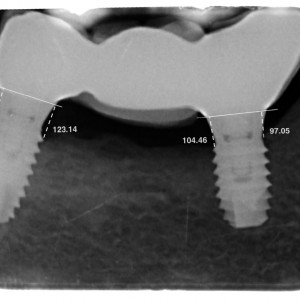
- Fig. 2b
-
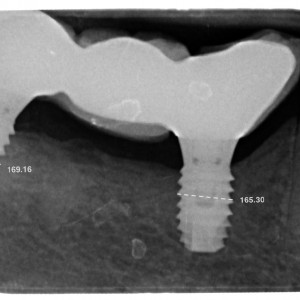
- Fig. 2c
-
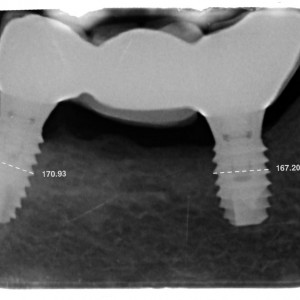
- Fig. 2d
Adimensional measurements of marginal bone loss (a) at prosthesis placement and (b) after 3 years of follow-up. Adimensional measurements across the implant diameter with the objective of calibrating the bone level measurements, knowing the true width of the implant: calibration of (c) the prosthesis placement and (d) the 3-year follow-up radiographs.
Marginal bone loss was measured with the software ImageJ (National Institute of Health, Md., U.S.) to process JPG files as obtained from intraoral radiographs. Two reference points were marked on each implant at the implant–prosthesis interface and joined with a line representing height 0. Two vertical lines were traced perpendicular to the 0 line up to the first mesial and distal bone–implant contacts (Figs. 2a & b). Differences between these perpendicular lines in radiographs taken at the different time points (T0 and T1) were used to calculate bone loss. The highest difference value was chosen between the mesial and the distal values. A line was traced across the implant diameter (Figs. 2c & d) with the objective of calibrating the periapical radiograph measurements, knowing the true width of the implant.
Statistical analysis
The principal predictor variable was the implant neck designs and neck surface treatments (group A and group B). The outcome variables of interest were periimplant tissue health and radiographic bone loss after 3 years of functional loading.
A descriptive analysis of the parameters was performed. Sample distribution of bone loss was assessed, and due to lack of adjustment to normal distribution and dependence of observations, the corresponding nonparametric tests were applied: method for longitudinal data of Brunner and Langer, providing an analysis of variance statistic. Generalized estimating equations models were estimated to analyze the probability of the neck design affecting the various clinical variables through the Wald chi-squared statistic. For the variables BoP and presence of mucositis, a binary logistic regression model was estimated. For PPD and width of keratinized mucosa, an ordinal logistic regression model was estimated. The statistical analysis was performed using SPSS (statistical package for Microsoft Windows, Version 15.0, SPSS, Chicago, Ill., U.S.) and R software (Version 2.15.0, R Foundation for Statistical Computing, Vienna, Austria). The significance level was set at P < 0.05. The statistical methodology, with a confidence level of 95% and the median effect size to detect f = 0.25, reached a power of 0.81 for the contrast of the interaction effect (homogeneity of bone loss in the groups).
Results
Fifty-five patients fulfilled the inclusion criteria. Patients who had undergone guided bone regeneration (n = 9), had immediate implants (n = 3), had missing information (n = 8) or failed to attend control visits (n = 6) were excluded. The final sample consisted of 27 partially edentulous patients, 12 women and 15 men (mean age: 63.5 ± 11.6), with a total of 51 dental implants: 13 patients with 28 implants (group A) and 14 patients with 23 implants (group B). In group A, 22% were smokers, and in group B, 44%. The implant sample was homogeneous regarding the implant diameter, length and position, arch and antagonist dentition (Table 1).
No significant differences were observed on evaluating clinical variables (Table 2). Higher PPD was measured in group B (5.3 ± 0.9 mm) compared with group A (4.8 ± 1.4 mm), with no statistically significant differences (P = 0.195). Group A showed lower BoP (47.1%) compared with group B (60%), although the odds ratio suggested an increased BoP risk with a TSA Advance implant (+27%), but there was insufficient statistical evidence to conclude a true effect (P = 0.524). Mucositis was present in 14.3% in group B and 12.5% in group A, and the odds ratio suggested a higher risk of mucositis with a TSA Advance implant (14%), with no statistically significant differences between the groups (P = 0.916). The higher score on width of keratinized mucosa was found in group A (3.50 ± 2.44 mm) in comparison with group B (2.7 ± 2.4 mm); however, no statistically significant difference was found (P = 0.435). The mean radiographic marginal bone loss with the TSA implants was 0.57 ± 0.55 mm (range: 0.00–2.10 mm) and with the TSA Advance implants was 0.46 ± 0.49 mm (range: 0.00–1.61 mm), and the median was 0.47 mm for the TSA implants and 0.25 mm for the TSA Advance implants (Table 3). Despite the greater marginal bone loss around TSA implants, no statistically significant differences were observed (P = 0.217).
Discussion
This study evaluated and compared 2 implants with the same body and prosthetic connection, but with different neck designs after 3 years of follow-up to assess the influence of these variables on periimplant tissue health and radiographic bone loss. The present study did not find statistical differences between the 2 implants on evaluating PPD, BoP, presence of mucositis, width of keratinized mucosa and marginal bone loss.
It has been suggested that the initial marginal bone level change occurs as an adaptation of the periimplant bone to the occlusal load. 32Puchades-Roman L, Palmer RM, Palmer PJ, Howe LC, Ide M, Wilson RF. A clinical, radiographic, and microbiologic comparison of Astra Tech and Branemark single tooth implants.
→ Clin Implant Dent Relat Res. 2000 Apr;2(2):78–84.33Hallman M, Mordenfeld A, Strandkvist T. A retrospective 5-year follow-up study of two different titanium implant surfaces used after interpositional bone grafting for reconstruction of the atrophic edentulous maxilla.
→ Clin Implant Dent Relat Res. 2005 Jul;7(3):121–6.34Karlsson U, Gotfredsen K, Olsson C. A 2-year report on maxillary and mandibular fixed partial dentures supported by Astra Tech dental implants. A comparison of 2 implants with different surface textures.
→ Clin Oral Implants Res. 1998 Aug;9(4):235–42.35. Van Steenberghe D, De Mars G, Quirynen M, Jacobs R, Naert I. A prospective split-mouth comparative study of two screw-shaped self-tapping pure titanium implant systems.
→ Clin Oral Implants Res. 2000 Jun;11(3):202–9. In studies involving a follow-up of over year,36Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success.
→ Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. 37Puchades-Roman L, Palmer RM, Palmer PJ, Howe LC, Ide M, Wilson RF. A clinical, radiographic, and microbiologic comparison of Astra Tech and Branemark single tooth implants.
→ Clin Implant Dent Relat Res. 2000 Apr;2(2):78–84.38Hallman M, Mordenfeld A, Strandkvist T. A retrospective 5-year follow-up study of two different titanium implant surfaces used after interpositional bone grafting for reconstruction of the atrophic edentulous maxilla.
→ Clin Implant Dent Relat Res. 2005 Jul;7(3):121–6.39Karlsson U, Gotfredsen K, Olsson C. A 2-year report on maxillary and mandibular fixed partial dentures supported by Astra Tech dental implants. A comparison of 2 implants with different surface textures.
→ Clin Oral Implants Res. 1998 Aug;9(4):235–42.40. Van Steenberghe D, De Mars G, Quirynen M, Jacobs R, Naert I. A prospective split-mouth comparative study of two screw-shaped self-tapping pure titanium implant systems.
→ Clin Oral Implants Res. 2000 Jun;11(3):202–9. the greatest bone loss was observed during the first year and then bone loss gradually decreased. The addition of threads or microthreads up to the crestal module of an implant might provide a potentially positive contribution to bone– implant contact, as well as improve preservation of marginal bone.41Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. → Ann Periodontol. 2000 Dec;5(1):119–28. 42. Piao CM, Lee JE, Koak JY, Kim SK, Rhyu IC, Han CH, Herr Y, Heo SJ. Marginal bone loss around three different implant systems: radiographic evaluation after 1 year.
→ J Oral Rehabil. 2009 Oct;36(10):748–54. 43. Puchades-Roman L, Palmer RM, Palmer PJ, Howe LC, Ide M, Wilson RF. A clinical, radiographic, and microbiologic comparison of Astra Tech and Branemark single tooth implants.
→ Clin Implant Dent Relat Res. 2000 Apr;2(2):78–84. 44Abuhussein H, Pagni G, Rebaudi A, Wang H. The effect of thread pattern upon implant osseointegration.
→ Clin Oral Implants Res. 2010 Feb;21(2):129–36. Shin et al. observed that the most effective design for minimizing marginal bone loss during functional loading was a rough surface with microthreads at the implant neck.45Shin YK, Han CH, Heo SJ, Kim S, Chun HJ. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year.
→ Int J Oral Maxillofac Implants. 2006 Sep–Oct;21(5):789–94. Abrahamsson and Berglundh drew a similar conclusion in an experimental study in dogs.46Abrahamsson I, Berglundh T. Effects of different implant surfaces and designs on marginal bone-level alterations: a review.
→ Clin Oral Implants Res. 2009 Sep;20 Suppl 4:207–15. They found that the degree of bone–implant contact within the marginal portion of the implants was significantly higher for the microthreaded implants compared with the implants with polished necks. Lee et al., in a well-controlled split-mouth study, also found that implants with microthreads showed significantly less bone loss compared with implants without them.47Lee DW, Choi YS, Park KH, Kim CS, Moon IS. Effect of microthread on the maintenance of marginal bone level: a 3-year prospective study.
→ Clin Oral Implants Res. 2007 Aug;18(4):465–70. However, although the studied implants were of the same brand and surface characteristics, they differed in their macrodesign: one had a tapered neck and the other had a cylindrical design. In the present study, both implant models, although distinct in thread configuration, had a tapered design. Bratu et al. compared implants of the same brand and with the same dimensions, taper, titanium alloy and surface characteristics but different neck designs: one model with a polished neck and the other with a rough surface and microthreads up to its prosthetic platform.48Bratu EA, Tandlich M, Shapira L. A rough surface implant neck with microthreads reduces the amount of marginal bone loss: a prospective clinical study. → Clin Oral Implants Res. 2009 Aug;20(8):827–32 Unlike the present study, the implants with a rough surface and microthreads displayed statistically significantly less early marginal bone loss and greater bone level stability compared with the polished-neck implants. The results of Piao et al. demonstrated that the amount of marginal bone loss at 12 months of functional loading was significantly different among the 3 groups they analyzed: The rough-surfaced microthread implant group showed less bone loss than the rough-surfaced implant group and the machined hybrid design implant group, but these implants had some differences other than the configuration of the coronal part, so these might have impacted on the results.49Piao CM, Lee JE, Koak JY, Kim SK, Rhyu IC, Han CH, Herr Y, Heo SJ. Marginal bone loss around three different implant systems: radiographic evaluation after 1 year.
→ J Oral Rehabil. 2009 Oct;36(10):748–54.
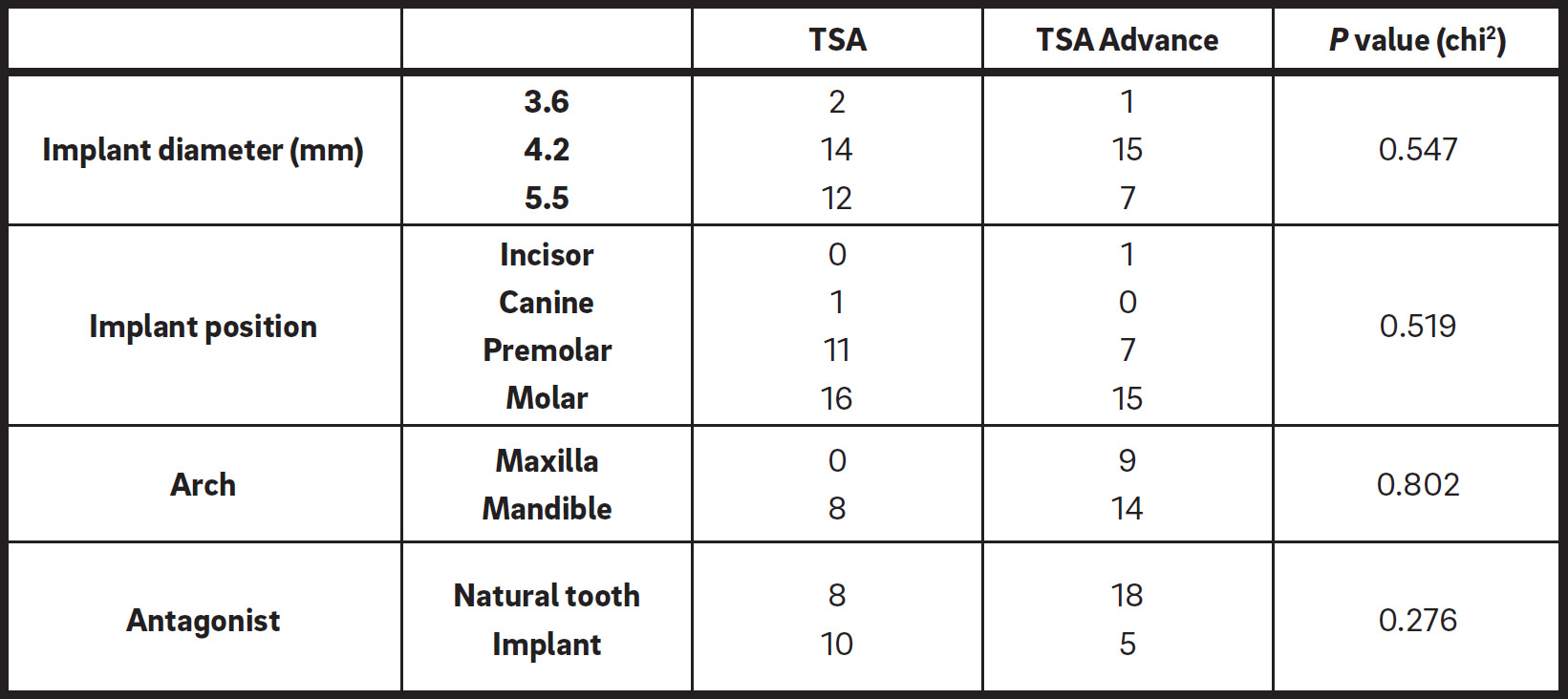
Descriptive statistics of the implant sample.
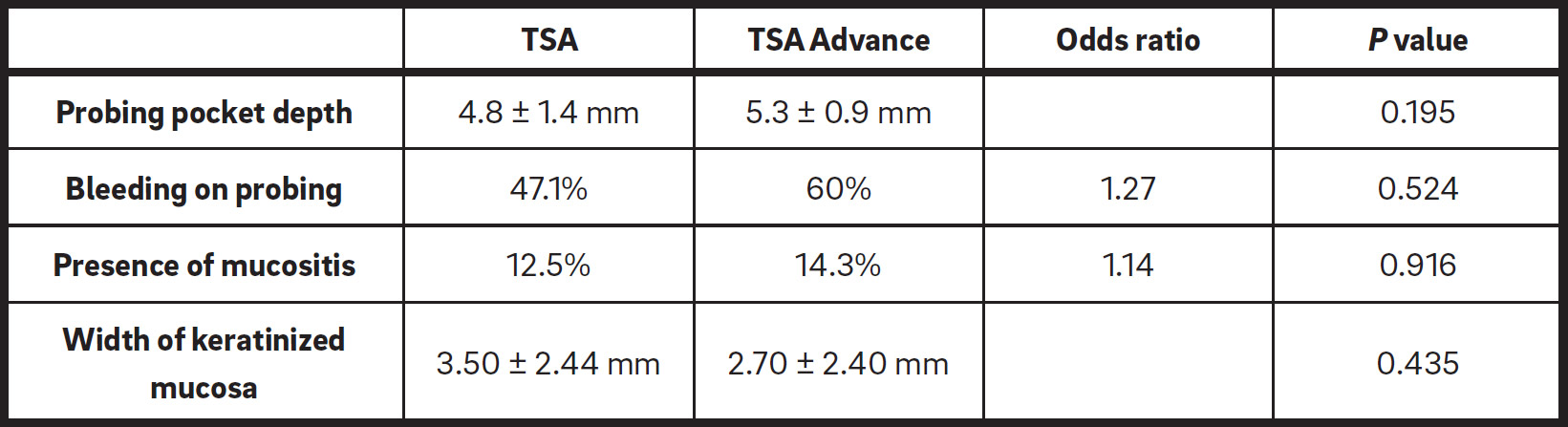
Statistical results regarding periimplant clinical variables.
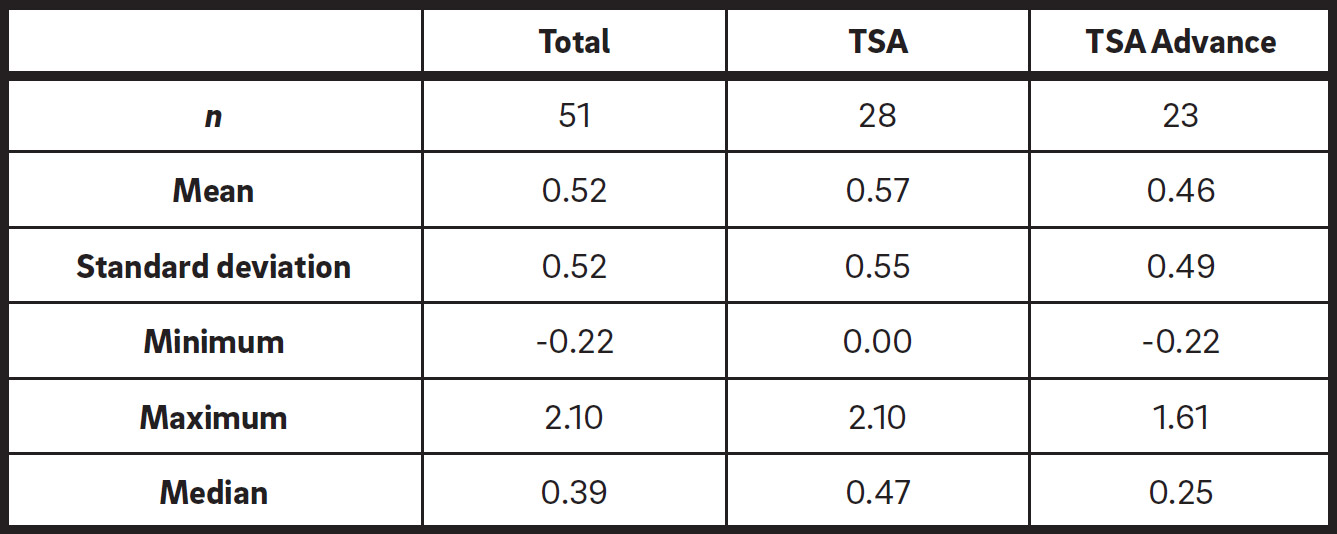
Radiographic marginal bone loss.
Some studies have compared polished-neck implants to rough-neck implants and found significantly greater bone loss with the polished- neck implants.50Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. → Ann Periodontol. 2000 Dec;5(1):119–28. 51Shin YK, Han CH, Heo SJ, Kim S, Chun HJ. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year.
→ Int J Oral Maxillofac Implants. 2006 Sep–Oct;21(5):789–94.52Nickenig HJ, Wichmann M, Schlegel KA, Nkenke E, Eitner S. Radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs.
→ Clin Oral Implants Res. 2009 Jun;20(6):550–453Karlsson U, Gotfredsen K, Olsson C. A 2-year report on maxillary and mandibular fixed partial dentures supported by Astra Tech dental implants. A comparison of 2 implants with different surface textures.
→ Clin Oral Implants Res. 1998 Aug;9(4):235–42. 54. Zechner W, Trinkl N, Watzak G, Busenlechner D, Tepper G, Haas R, Watzek G. Radiologic follow-up of peri-implant bone loss around machine-surfaced and rough-surfaced interforaminal implants in the mandible functionally loaded for 3 to 7 years.
→ Int J Oral Maxillofac Implants. 2004 Mar–Apr;19(2):216–21. 55Hermann JS, Buser D, Schenk RK, Cochran DL. Crestal bone changes around titanium implants. A histometric evaluation of unloaded non-submerged and submerged implants in the canine mandible.
→ J Periodontol. 2000 Sep;71(9):1412–24. 56Stein AE, McGlmphy EA, Johnston WM, Larsen PE. Effects of implant design and surface roughness on crestal bone and soft tissue levels in the esthetic zone.
→ Int J Oral Maxillofac Implants. 2009 Sep–Oct;24(5):910–9.57Schwarz F, Herten M, Bieling K, Becker J. Crestal bone changes at nonsubmerged implants (Camlog) with different machined collar lengths: a histomorphometric pilot study in dogs.
→ Int J Oral Maxillofac Implants. 2008 Mar–Apr;23(2):335–42. In contrast, others have found no statistically significant differences in bone loss.58Piao CM, Lee JE, Koak JY, Kim SK, Rhyu IC, Han CH, Herr Y, Heo SJ. Marginal bone loss around three different implant systems: radiographic evaluation after 1 year.
→ J Oral Rehabil. 2009 Oct;36(10):748–54. 59Hallman M, Mordenfeld A, Strandkvist T. A retrospective 5-year follow-up study of two different titanium implant surfaces used after interpositional bone grafting for reconstruction of the atrophic edentulous maxilla.
→ Clin Implant Dent Relat Res. 2005 Jul;7(3):121–6. 60. Karlsson U, Gotfredsen K, Olsson C. A 2-year report on maxillary and mandibular fixed partial dentures supported by Astra Tech dental implants. A comparison of 2 implants with different surface textures.
→ Clin Oral Implants Res. 1998 Aug;9(4):235–42.61 Astrand P, Engquist B, Dahlgren S, Grondahl K, Engquist E, Feldmann H. Astra Tech and Branemark implants: a 5-year prospective study of marginal bone reactions.
→ Clin Oral Implants Res. 2004 Aug;15(4):413–20.62Den Hartog L, Meijer HJ, Stegenga B, Tymstra N, Vissink A, Raghoebar GM. Single implants with different neck designs in the aesthetic zone: a randomized clinical trial.
→ Clin Oral Implants Res. 2011 Nov;22(11):1289–97. Some studies have evaluated the presence of microthreads at the coronal portion using radiographic evaluation of the marginal bone level and found a positive effect in maintaining the marginal bone level for rough-surfaced implants with microthreads at the coronal portion after functional loading.63Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success.
→ Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25.64Nickenig HJ, Wichmann M, Schlegel KA, Nkenke E, Eitner S. Radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs.
→ Clin Oral Implants Res. 2009 Jun;20(6):550–4.65Piao CM, Lee JE, Koak JY, Kim SK, Rhyu IC, Han CH, Herr Y, Heo SJ. Marginal bone loss around three different implant systems: radiographic evaluation after 1 year.
→ J Oral Rehabil. 2009 Oct;36(10):748–54.66Norton MR. Marginal bone levels at single tooth implants with a conical fixture design. The influence of surface macroand microstructure.
→ Clin Oral Implants Res. 1998 Apr;9(2):91–9. 67Deppe H, Horch H, Kolk A. Microstructured dental implants and palatal mucosal grafts in cleft patients: a retrospective analysis.
→ J Craniomaxillofac Surg. 2004 Aug;32(4):211–5. However, Van de Velde et al. observed that, after 1 year of loading, a microthread design of the implant collar did not seem to improve bone preservation in the mandible.68Van de Velde T, Collaert B, Sennerby L, De Bruyn H. Effect of implant design on preservation of marginal bone in the mandible.
→ Clin Implant Dent Relat Res. 2010 Jun 1;12(2):134–41. Aloy-Prósper et al. in their literature review found that marginal bone loss with polished- neck implants was greater 3 months after implant placement, while bone loss with rough-neck implants with and without microthreads was greater 6 months after insertion of the implants.69Aloy-Prosper A, Maestre-Ferrin L, Penarrocha-Oltra D, Penarrocha-Diago M. Marginal bone loss in relation to the implant neck surface: an update.
→ Med Oral Patol Oral Cir Bucal. 2011 May;16(3):e365–8. Lang et al. in a consensus report concluded that prospective controlled studies on the effects of different implant designs and surfaces demonstrated that marginal bone levels were generally well preserved after installation of the dental prosthesis (at least for fixed restorations) on a variety of implant types (cumulative bone loss: < 0.5 mm after 3 years).70Lang NP, Jepsen S; Working Group 4. Implant surfaces and design (Working Group 4).
→ Clin Oral Implants Res. 2009 Sep;20 Suppl 4:228–31.
Most of the studies measured bone loss from the start of prosthetic loading to the end of follow-up, except Nickenig et al., who measured loss from the time of placement of the implants.71Nickenig HJ, Wichmann M, Happe A, Zoller JE, Eitner S. A 5-year prospective radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs.
→ J Craniomaxillofac Surg. 2013 Oct;41(7):564–8. They compared smooth and rough implants for restoring missing mandibular molars. In their study, for smooth implants, bone loss progressed from 0.5 mm in the healing period to 1.1, 1.3 and 1.4 mm in the second, third and fifth year of follow-up, respectively. In contrast, for the rough-surfaced, microthreaded implants, bone loss progressed from 0.1 mm in the healing period to 0.5, 0.6 and 0.7 mm in the second, third and fifth year of follow-up, respectively. They found a significant difference in bone level changes, suggesting that rough-surfaced, microthreaded implants more effectively minimized overall marginal bone loss than machinedneck implants did, particularly during the healing period.
Even if some studies have shown less marginal bone loss around implants with a rough neck, these implants favor bacterial plaque retention when exposed to the oral environment, and this in turn would imply an increased risk of periimplant disease such as mucositis or periimplantits. 72Cosyn J, Sabzevar MM, De Wilde P, De Rouck T. Two-piece implants with turned versus microtextured collars.
→ J Periodontol. 2007 Sep;78(9):1657–63. 73Bragger U, Hafeli U, Huber B, Hammerle CH, Lang NP. Evaluation of postsurgical crestal bone levels adjacent to non-submerged dental implants.
→ Clin Oral Implants Res. 1998 Aug;9(4):218–24. The relatively smooth implant neck allows the least accumulation of plaque74Teughels W, Van Assche N, Sliepen I, Quirynen M. Effect of material characteristics and/or surface topography on biofilm development.
→ Clin Oral Implants Res. 2006 Oct;17 Suppl 2:68–8175Baldi D, Menini M, Pera F, Ravera G, Pera P. Plaque accumulation on exposed titanium surfaces and peri-implant tissue behavior. A preliminary 1-year clinical study.
→ Int J Prosthodont. 2009 Sep–Oct;22(5):447–55. and is designed as a transmucosal component, thus making the microgap or interface between implant and restoration easily accessible for oral hygiene.76Hanggi MP, Hanggi DC, Schoolfield JD, Meyer J, Cochran DL, Hermann JS. Crestal bone changes around titanium implants. Part I: a retrospective radiographic evaluation in humans comparing two non-submerged implant designs with different machined collar lengths.
→ J Periodontol. 2005 May;76(5):791–802.
Taking into account the results, it is necessary to highlight the limitations of the present study. Sample size and the lack of randomization could limit generalization of the results. Further studies with a larger sample are needed to clarify the influence of implant neck design on periimplant tissue health and periimplant bone remodeling after medium- to long-term functional loading.
Conclusion
According to the results of the present study, the implant neck designs and neck surface treatments did not significantly influence periimplant tissue health and radiographic bone loss after 3 years of follow-up.
Competing interests
The authors declare that they have no competing interests.

Interview
with David Peñarrocha Oltra
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 36. | ↑ | Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. → Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. |
| 2, 47. | ↑ | Lee DW, Choi YS, Park KH, Kim CS, Moon IS. Effect of microthread on the maintenance of marginal bone level: a 3-year prospective study. → Clin Oral Implants Res. 2007 Aug;18(4):465–70. |
| 3. | ↑ | Manz MC. Factors associated with radiographic vertical bone loss around implants placed in a clinical study. → Ann Periodontol. 2000 Dec;5(1):137–51. |
| 4, 13. | ↑ | Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. → Ann Periodontol. 2000 Dec;5(1):119–28. |
| 5. | ↑ | Bratu EA, Tandlich M, Shapira L. A rough surface implant neck with microthreads reduces the amount of marginal bone loss: a prospective clinical study. → Clin Oral Implants Res. 2009 Aug;20(8):827–32. |
| 6. | ↑ | Hartman GA, Cochran DL. Initial implant position determines the magnitude of crestal bone remodeling. → J Periodontol. 2004 Apr;75(4):572–7. |
| 7, 25, 41, 50. | ↑ | Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. → Ann Periodontol. 2000 Dec;5(1):119–28. |
| 8. | ↑ | Oh TJ, Yoon J, Misch CE, Wang HL. The causes of early implant bone loss: myth or science? → J Periodontol. 2002 Mar;73(3):322–33. |
| 9. | ↑ | . Kronstrom M, Svenson B, Hellman M, Persson GR. Early implant failures in patients treated with Branemark System titanium dental implants: a retrospective study. → Int J Oral Maxillofac Implants. 2001 Mar–Apr;16(2):201–7. |
| 10. | ↑ | . Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors contributing to failures of osseointegrated oral implants. (II). Etiopathogenesis. → Eur J Oral Sci. 1998 Jun;106(3):721–64. |
| 11. | ↑ | Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz- Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. → Implant Dent. 2008 Mar;17(1):5–15. |
| 12. | ↑ | . Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. → Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. |
| 14. | ↑ | Lang NP, Jepsen S; Working Group 4. Implant surfaces and design (Working Group 4). → Clin Oral Implants Res. 2009 Sep;20 Suppl 4:228–31. |
| 15, 20, 45, 51. | ↑ | Shin YK, Han CH, Heo SJ, Kim S, Chun HJ. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year. → Int J Oral Maxillofac Implants. 2006 Sep–Oct;21(5):789–94. |
| 16, 27. | ↑ | Nickenig HJ, Wichmann M, Schlegel KA, Nkenke E, Eitner S. Radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs. → Clin Oral Implants Res. 2009 Jun;20(6):550–4. |
| 17. | ↑ | Nickenig HJ, Wichmann M, Happe A, Zoller JE, Eitner S. A 5-year prospective radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs. → J Craniomaxillofac Surg. 2013 Oct;41(7):564–8. |
| 18. | ↑ | Penarrocha M, Palomar M, Sanchis JM, Guarinos J, Balaguer J. Radiologic study of marginal bone loss around 108 dental implants and its relationship to smoking, implant location, and morphology. → Int J Oral Maxillofac Implants. 2004 Nov–Dec;19(6):861–7. |
| 19, 63. | ↑ | Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. → Int J Oral Maxillofac Implants. 1986 Summer;1(1):11–25. |
| 21. | ↑ | . Hansson S. The implant neck: smooth or provided with retention elements. A biomechanical approach. → Clin Oral Implants Res. 1999 Oct;10(5):394–405. |
| 22. | ↑ | Tan WC, Lang NP, Schmidlin K, Zwahlen M, Pjetursson BE. The effect of different implant neck configurations on soft and hard tissue healing: a randomized-controlled clinical trial. → Clin Oral Implants Res. 2011 Jan;22(1):14–9. |
| 23, 74. | ↑ | Teughels W, Van Assche N, Sliepen I, Quirynen M. Effect of material characteristics and/or surface topography on biofilm development. → Clin Oral Implants Res. 2006 Oct;17 Suppl 2:68–81 |
| 24, 75. | ↑ | Baldi D, Menini M, Pera F, Ravera G, Pera P. Plaque accumulation on exposed titanium surfaces and peri-implant tissue behavior. A preliminary 1-year clinical study. → Int J Prosthodont. 2009 Sep–Oct;22(5):447–55. |
| 26. | ↑ | Shin YK, Han CH, Heo SJ, Kim S, Chun HJ. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year. → Int J Oral Maxillofac Implants. 2006 Sep–Oct;21(5):789–94. |
| 28, 49, 65. | ↑ | Piao CM, Lee JE, Koak JY, Kim SK, Rhyu IC, Han CH, Herr Y, Heo SJ. Marginal bone loss around three different implant systems: radiographic evaluation after 1 year. → J Oral Rehabil. 2009 Oct;36(10):748–54. |
| 29. | ↑ | . Hanggi MP, Hanggi DC, Schoolfield JD, Meyer J, Cochran DL, Hermann JS. Crestal bone changes around titanium implants. Part I: a retrospective radiographic evaluation in humans comparing two non-submerged implant designs with different machined collar lengths. → J Periodontol. 2005 May;76(5):791–802. |
| 30, 70. | ↑ | Lang NP, Jepsen S; Working Group 4. Implant surfaces and design (Working Group 4). → Clin Oral Implants Res. 2009 Sep;20 Suppl 4:228–31. |
| 31. | ↑ | Albrektsson T, Buser D, Chen ST, Cochran D, DeBruyn H, Jemt T, Koka S, Nevins M, Sennerby L, Simion M, Taylor TD, Wennerberg A. Statements from the Estepona consensus meeting on peri-implantitis, February 2–4, 2012. → Clin Implant Dent Relat Res. 2012 Dec;14(6):781–2. |
| 32, 37. | ↑ | Puchades-Roman L, Palmer RM, Palmer PJ, Howe LC, Ide M, Wilson RF. A clinical, radiographic, and microbiologic comparison of Astra Tech and Branemark single tooth implants. → Clin Implant Dent Relat Res. 2000 Apr;2(2):78–84. |
| 33, 38. | ↑ | Hallman M, Mordenfeld A, Strandkvist T. A retrospective 5-year follow-up study of two different titanium implant surfaces used after interpositional bone grafting for reconstruction of the atrophic edentulous maxilla. → Clin Implant Dent Relat Res. 2005 Jul;7(3):121–6. |
| 34, 39. | ↑ | Karlsson U, Gotfredsen K, Olsson C. A 2-year report on maxillary and mandibular fixed partial dentures supported by Astra Tech dental implants. A comparison of 2 implants with different surface textures. → Clin Oral Implants Res. 1998 Aug;9(4):235–42. |
| 35, 40. | ↑ | . Van Steenberghe D, De Mars G, Quirynen M, Jacobs R, Naert I. A prospective split-mouth comparative study of two screw-shaped self-tapping pure titanium implant systems. → Clin Oral Implants Res. 2000 Jun;11(3):202–9. |
| 42. | ↑ | . Piao CM, Lee JE, Koak JY, Kim SK, Rhyu IC, Han CH, Herr Y, Heo SJ. Marginal bone loss around three different implant systems: radiographic evaluation after 1 year. → J Oral Rehabil. 2009 Oct;36(10):748–54. |
| 43. | ↑ | . Puchades-Roman L, Palmer RM, Palmer PJ, Howe LC, Ide M, Wilson RF. A clinical, radiographic, and microbiologic comparison of Astra Tech and Branemark single tooth implants. → Clin Implant Dent Relat Res. 2000 Apr;2(2):78–84. |
| 44. | ↑ | Abuhussein H, Pagni G, Rebaudi A, Wang H. The effect of thread pattern upon implant osseointegration. → Clin Oral Implants Res. 2010 Feb;21(2):129–36. |
| 46. | ↑ | Abrahamsson I, Berglundh T. Effects of different implant surfaces and designs on marginal bone-level alterations: a review. → Clin Oral Implants Res. 2009 Sep;20 Suppl 4:207–15. |
| 48. | ↑ | Bratu EA, Tandlich M, Shapira L. A rough surface implant neck with microthreads reduces the amount of marginal bone loss: a prospective clinical study. → Clin Oral Implants Res. 2009 Aug;20(8):827–32 |
| 52. | ↑ | Nickenig HJ, Wichmann M, Schlegel KA, Nkenke E, Eitner S. Radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs. → Clin Oral Implants Res. 2009 Jun;20(6):550–4 |
| 53. | ↑ | Karlsson U, Gotfredsen K, Olsson C. A 2-year report on maxillary and mandibular fixed partial dentures supported by Astra Tech dental implants. A comparison of 2 implants with different surface textures. → Clin Oral Implants Res. 1998 Aug;9(4):235–42. |
| 54. | ↑ | . Zechner W, Trinkl N, Watzak G, Busenlechner D, Tepper G, Haas R, Watzek G. Radiologic follow-up of peri-implant bone loss around machine-surfaced and rough-surfaced interforaminal implants in the mandible functionally loaded for 3 to 7 years. → Int J Oral Maxillofac Implants. 2004 Mar–Apr;19(2):216–21. |
| 55. | ↑ | Hermann JS, Buser D, Schenk RK, Cochran DL. Crestal bone changes around titanium implants. A histometric evaluation of unloaded non-submerged and submerged implants in the canine mandible. → J Periodontol. 2000 Sep;71(9):1412–24. |
| 56. | ↑ | Stein AE, McGlmphy EA, Johnston WM, Larsen PE. Effects of implant design and surface roughness on crestal bone and soft tissue levels in the esthetic zone. → Int J Oral Maxillofac Implants. 2009 Sep–Oct;24(5):910–9. |
| 57. | ↑ | Schwarz F, Herten M, Bieling K, Becker J. Crestal bone changes at nonsubmerged implants (Camlog) with different machined collar lengths: a histomorphometric pilot study in dogs. → Int J Oral Maxillofac Implants. 2008 Mar–Apr;23(2):335–42. |
| 58. | ↑ | Piao CM, Lee JE, Koak JY, Kim SK, Rhyu IC, Han CH, Herr Y, Heo SJ. Marginal bone loss around three different implant systems: radiographic evaluation after 1 year. → J Oral Rehabil. 2009 Oct;36(10):748–54. |
| 59. | ↑ | Hallman M, Mordenfeld A, Strandkvist T. A retrospective 5-year follow-up study of two different titanium implant surfaces used after interpositional bone grafting for reconstruction of the atrophic edentulous maxilla. → Clin Implant Dent Relat Res. 2005 Jul;7(3):121–6. |
| 60. | ↑ | . Karlsson U, Gotfredsen K, Olsson C. A 2-year report on maxillary and mandibular fixed partial dentures supported by Astra Tech dental implants. A comparison of 2 implants with different surface textures. → Clin Oral Implants Res. 1998 Aug;9(4):235–42. |
| 61. | ↑ | Astrand P, Engquist B, Dahlgren S, Grondahl K, Engquist E, Feldmann H. Astra Tech and Branemark implants: a 5-year prospective study of marginal bone reactions. → Clin Oral Implants Res. 2004 Aug;15(4):413–20. |
| 62. | ↑ | Den Hartog L, Meijer HJ, Stegenga B, Tymstra N, Vissink A, Raghoebar GM. Single implants with different neck designs in the aesthetic zone: a randomized clinical trial. → Clin Oral Implants Res. 2011 Nov;22(11):1289–97. |
| 64. | ↑ | Nickenig HJ, Wichmann M, Schlegel KA, Nkenke E, Eitner S. Radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs. → Clin Oral Implants Res. 2009 Jun;20(6):550–4. |
| 66. | ↑ | Norton MR. Marginal bone levels at single tooth implants with a conical fixture design. The influence of surface macroand microstructure. → Clin Oral Implants Res. 1998 Apr;9(2):91–9. |
| 67. | ↑ | Deppe H, Horch H, Kolk A. Microstructured dental implants and palatal mucosal grafts in cleft patients: a retrospective analysis. → J Craniomaxillofac Surg. 2004 Aug;32(4):211–5. |
| 68. | ↑ | Van de Velde T, Collaert B, Sennerby L, De Bruyn H. Effect of implant design on preservation of marginal bone in the mandible. → Clin Implant Dent Relat Res. 2010 Jun 1;12(2):134–41. |
| 69. | ↑ | Aloy-Prosper A, Maestre-Ferrin L, Penarrocha-Oltra D, Penarrocha-Diago M. Marginal bone loss in relation to the implant neck surface: an update. → Med Oral Patol Oral Cir Bucal. 2011 May;16(3):e365–8. |
| 71. | ↑ | Nickenig HJ, Wichmann M, Happe A, Zoller JE, Eitner S. A 5-year prospective radiographic evaluation of marginal bone levels adjacent to parallel-screw cylinder machined-neck implants and rough-surfaced microthreaded implants using digitized panoramic radiographs. → J Craniomaxillofac Surg. 2013 Oct;41(7):564–8. |
| 72. | ↑ | Cosyn J, Sabzevar MM, De Wilde P, De Rouck T. Two-piece implants with turned versus microtextured collars. → J Periodontol. 2007 Sep;78(9):1657–63. |
| 73. | ↑ | Bragger U, Hafeli U, Huber B, Hammerle CH, Lang NP. Evaluation of postsurgical crestal bone levels adjacent to non-submerged dental implants. → Clin Oral Implants Res. 1998 Aug;9(4):218–24. |
| 76. | ↑ | Hanggi MP, Hanggi DC, Schoolfield JD, Meyer J, Cochran DL, Hermann JS. Crestal bone changes around titanium implants. Part I: a retrospective radiographic evaluation in humans comparing two non-submerged implant designs with different machined collar lengths. → J Periodontol. 2005 May;76(5):791–802. |





Leave a Reply
Be the First to Comment!