Prevalence of esthetic gingival recession in university health care in a region of Spain
January 7, 2020 / Categories: Digital Dentistry, Implant Dentistry

Pérez Sayáns, Mario
Rodríguez Lorenzo, Alba
García García, Abel
Gándara Vila, Pilar
Gallas Torreira, Mercedes
Chamorro Petronacci, Cintia Micaela
Lorenzo Pouso, Alejandro Ismael
Abstract
Objective
The objective of the study was to evaluate, in a random population sample, the prevalence of gingival recession in the anterior zone of patients at the dental faculty of the University of Santiago de Compostela.
Materials and methods
We designed a cross-sectional epidemiological study. A random sample of 100 patients at the faculty was studied. We obtained and analyzed data regarding demographics, smoking habit, recession characteristics, dental history and esthetic importance for the patient.
Results
The prevalence of recession in the anterior zone was relatively frequent at 26%. There were statistically significant relationships between the location of the recession and smoking habit and number of teeth with recession. We also observed statistically significant results between the number of teeth with recession and sex, molar relationship, periodontal disease and periodontal biotype. In patients with more than 4 teeth with recession, most had a nonassessable molar relationship, and most had periodontal disease. It is important to note the significant relationships established between distance of the recession from the cementoenamel junction, pocket depth and loss of supporting tissue, and periodontal disease and plaque index.
Conclusion
The presence of recession in the anterior zone was relatively frequent in our setting. There are many factors related to the presence of recession, such as smoking, periodontal disease, pocket depth, loss of supporting tissue and nonassessable molar relationship.
Keywords:
Gingival recession; periodontal disease; periodontal biotype; plaque index.
Introduction
The presence of gingival recession is frequent in the adult population, causing not only esthetic alterations but also sensitivity problems and/or root caries.1Albandar JM, Kingman A. Gingival recession, gingival bleeding, and dental calculus in adults 30 years of age and older in the United States, 1988–1994. → J Periodontol. 1999 Jan;70(1):30–43.,2Bouchard P, Malet J, Borghetti A. Decision-making in aesthetics: root coverage revisited. → Periodontol 2000. 2001;27:97–120. We define gingival recession as the apical migration of the gingival margin from the cementoenamel junction, resulting in root exposure. Although in adults the presence of gingival recession is frequent, the prevalence, extent and severity present differences between the various populations studied, age, sex, oral hygiene level and brushing technique being among the main contributing factors.3Cairo F, Pagliaro U, Nieri M. Treatment of gingival recession with coronally advanced flap procedures: a systematic review. → J Clin Periodontol. 2008 Sep;35(8 Suppl):136–62.
Upon analyzing the prevalence rates in various studies, we observed disparate results. In a study conducted in the U.S. with 9,689 subjects, the prevalence of gingival recession was 58% for individuals between 30 and 90 years of age, yielding an average of 22.3% of affected teeth per person.4Albandar JM, Kingman A. Gingival recession, gingival bleeding, and dental calculus in adults 30 years of age and older in the United States, 1988–1994. → J Periodontol. 1999 Jan;70(1):30–43. Geiger found that between 78% and 100% of middle-aged individuals have recession, present around between 22% and 53% of the teeth.5Geiger AM. Mucogingival problems and the movement of mandibular incisors: a clinical review. → Am J Orthod. 1980 Nov;78(5):511–27. In a longitudinal study conducted in Barcelona, gingival recession was observed in 85% of the individuals in the sample, a prevalence that did not change in a follow-up test performed 10 years later; however, the average number of teeth with recession per person varied (a total of 210 in the initial examination and 299 in the second examination), and the average height of the recession increased, while the control variable, plaque, decreased.6Gorman WJ. Prevalence and etiology of gingival recession. → J Periodontol. 1967 Jul–Aug;38(4):316–22.
Regarding etiology, we know that this condition is determined by both susceptibility factors and anatomical factors, such as fenestration and dehiscence of the alveolar bone or an abnormal position of the tooth in the arch. These factors can result in thinner alveolar bone than usual, which can be more susceptible to resorption.7Bouchard P, Malet J, Borghetti A. Decision-making in aesthetics: root coverage revisited. → Periodontol 2000. 2001;27:97–120. Gingival recession is also conditioned by causal factors, such as physiological and pathological factors; physiological factors, such as orthodontic movements of the teeth out of the buccal and lingual cortical bone;8Bouchard P, Malet J, Borghetti A. Decision-making in aesthetics: root coverage revisited. → Periodontol 2000. 2001;27:97–120.,9Haffajee AD, Socransky SS. Relationship of cigarette smoking to attachment level profiles. → J Clin Periodontol. 2001 Apr;28(4):283–95. and pathological factors, such as incorrect brushing technique and the types of brush and bristles, intraoral and perioral piercings, occlusal trauma or poor oral hygiene that leads to the accumulation of bacterial plaque.10Bouchard P, Malet J, Borghetti A. Decision-making in aesthetics: root coverage revisited. → Periodontol 2000. 2001;27:97–120.,11Haffajee AD, Socransky SS. Relationship of cigarette smoking to attachment level profiles. → J Clin Periodontol. 2001 Apr;28(4):283–95.,12Hägewald S, Spahr A, Rompola E, Haller B, Heijl L, Bernimoulin JP. Comparative study of Emdogain and coronally advanced flap technique in the treatment of human gingival recessions. A prospective controlled clinical study. → J Clin Periodontol. 2002 Jan;29(1):35–41.,13Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. → J Am Dent Assoc. 2003 Feb;134(2):220–5.,14Löe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. → J Periodontol. 1992 Jun;63(6):489–95.,15Marini MG, Greghi SL, Passanezi E, Sant’ana AC. Gingival recession: prevalence, extension and severity in adults. → J Appl Oral Sci. 2004 Sep;12(3):250–5.,16Matas F, Sentis J, Mendieta C. Ten-year longitudinal study of gingival recession in dentists. → J Clin Periodontol. 2011 Dec;38(12):1091–8. Since the presence of gingival recession is commonly observed in the daily practice at a dental clinic, we considered it important to study its prevalence owing to the esthetic and health consequences. Therefore, we analyzed the relationship between different variables (such as smoking habit, periodontal biotype and molar relationship) and the presence of recession and its characteristics (such as distance of the recession from the cementoenamel junction and number of teeth with recession).
The main objective of this study was to evaluate, in a random population sample, the prevalence of gingival recession in the anterior zone, whether or not the recession was symptomatic. The study’s secondary objective was to study the factors associated with this recession.
Materials and methods
We designed a cross-sectional epidemiological study of the prevalence of gingival recession in the anterior zone of patients at the dental faculty of the University of Santiago de Compostela (USC). This study was approved by the USC ethics committee (reference no. TFG 2016/23).
The data were obtained by collecting specific standardized variables for this study, which were always measured by 2 specific operators. The operators had previously performed a calibration for the correct evaluation of the variables. In cases of discrepancy, a third operator corroborated the results. These variables were grouped as follows:
- demographics (age, sex, level of education and other demographic information);
- smoking habit (those who had stopped up to 5 years before the study were considered smokers);
- lesion characteristics (location of the recession, distance of recession from the cementoenamel junction, pocket depth, supporting tissue loss, root caries and other characteristics);
- dental history (molar and canine relationship, presence or absence of periodontal disease, periodontal biotype and other factors); and
- esthetic importance for the patient.
Next, periodontal disease was evaluated as follows:
- Regarding periodontal disease, we differentiated between whether periodontal disease was or was not present; in cases where it was present, we determined the degree of severity (mild, moderate or severe). The disease was considered mild when there was between 1 and 2 mm of supporting tissue loss, moderate when there was between 3 and 4 mm of supporting tissue loss, and severe when there was greater than 5 mm of supporting tissue loss.17Papapanou PN, Sanz M, Buduneli N, Dietrich T, Feres M, Fine DH, Flemmig TF, Garcia R, Giannobile WV, Graziani F, Greenwell H, Herrera D, Kao RT, Kebschull M, Kinane DF, Kirkwood KL, Kocher T, Kornman KS, Kumar PS, Loos BG, Machtei E, Meng H, Mombelli A, Needleman I, Offenbacher S, Seymour GJ, Teles R, Tonetti MS. Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. → J Periodontol. 2018 Jun;89 Suppl 1:173–82. Regarding the plaque index, there was also differentiation between whether or not plaque was present. In such cases, plaque could be mild or abundant: Plaque was considered mild when it covered less than one-third of the clinical crown and abundant when it was equal to or greater than onethird of the crown.18Kayalvizhi G, Radha S, Prathima GS, Mohandoss S, Ramesh V, Arumugam SB. Comparative evaluation of plaque removal effectiveness of manual and chewable toothbrushes in children: a randomized clinical trial. → Int J Clin Pediatr Dent. 2019 Mar–Apr;12(2):107–10.
- To classify the patient’s periodontal biotype, we distinguished between thin and thick.19Zweers J, Thomas RZ, Slot DE, Weisgold AS, Van der Weijden FG. Characteristics of periodontal biotype, its dimensions, associations and prevalence: a systematic review. → J Clin Periodontol. 2014 Oct;41(10):958–71. In the thin biotype, the gingival margin was thin and scalloped, the papillae were high, the coronal morphology was long and conical, with a point of fine contact, the root morphology was convex, and the bony crest was very thin and scalloped. In the thick biotype, the gingival margin was thick and only slightly scalloped, the papillae were low, the coronal morphology was short and square, with a wide contact point, the root morphology was concave, and the bony crest was thick.
- For the variable “cause of the recession,” we studied different causes, such as brushing technique,20Gorman WJ. Prevalence and etiology of gingival recession. → J Periodontol. 1967 Jul–Aug;38(4):316–22.,21Rajapakse PS, McCracken GI, Gwynnett E, Steen ND, Guentsch A, Heasman PA. Does tooth brushing influence the development and progression of non-inflammatory gingival recession? A systematic review. → J Clin Periodontol. 2007 Dec;34(12):1046–61. periodontal disease, bruxism, orthodontic treatment22Bin Bahar BS, Alkhalidy SR, Kaklamanos EG, Athanasiou AE. Do orthodontic patients develop more gingival recession in anterior teeth compared to untreated individuals? A systematic review of controlled studies. → Int Orthod. 2019 Nov 1. pii: S1761-7227(19)30155-X. doi: 10.1016/ j.ortho.2019.08.025. and piercing, as well as mixed causes and other causes. In this last category, we included anomalous tooth positions, other direct traumatic factors and all cases in which recession was not related to any of the causes already mentioned. We considered the cause of recession to be mixed when the recession was due to 2 or more causes. For the collection of these data, we used an exploration kit consisting of a mirror, an exploration probe and a CP12 periodontal probe.
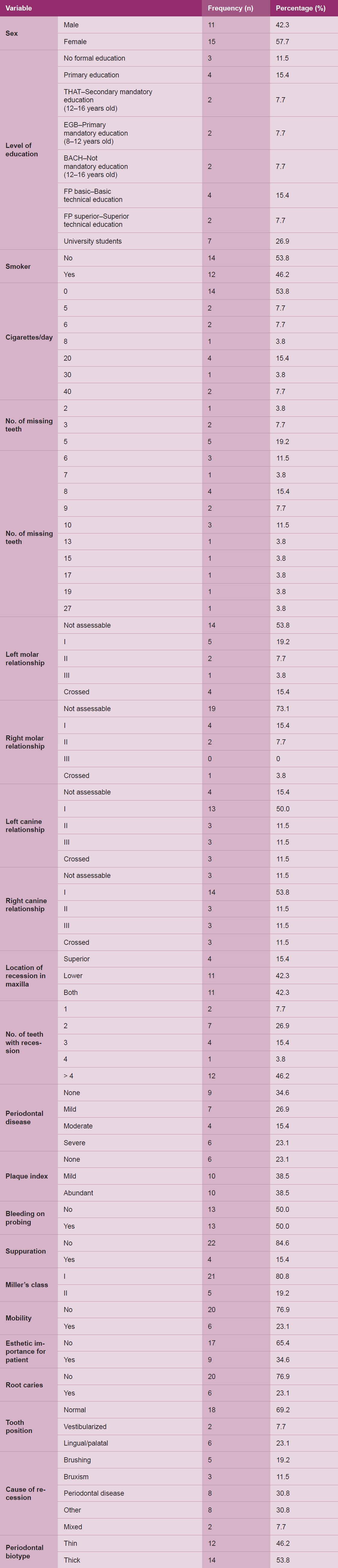
Table 1 Descriptive data of qualitative variables of the study.

Table 2 Descriptive data of quantitative variables of the study.

Table 3 Levels of significance for the variable “location of recession in maxilla”.
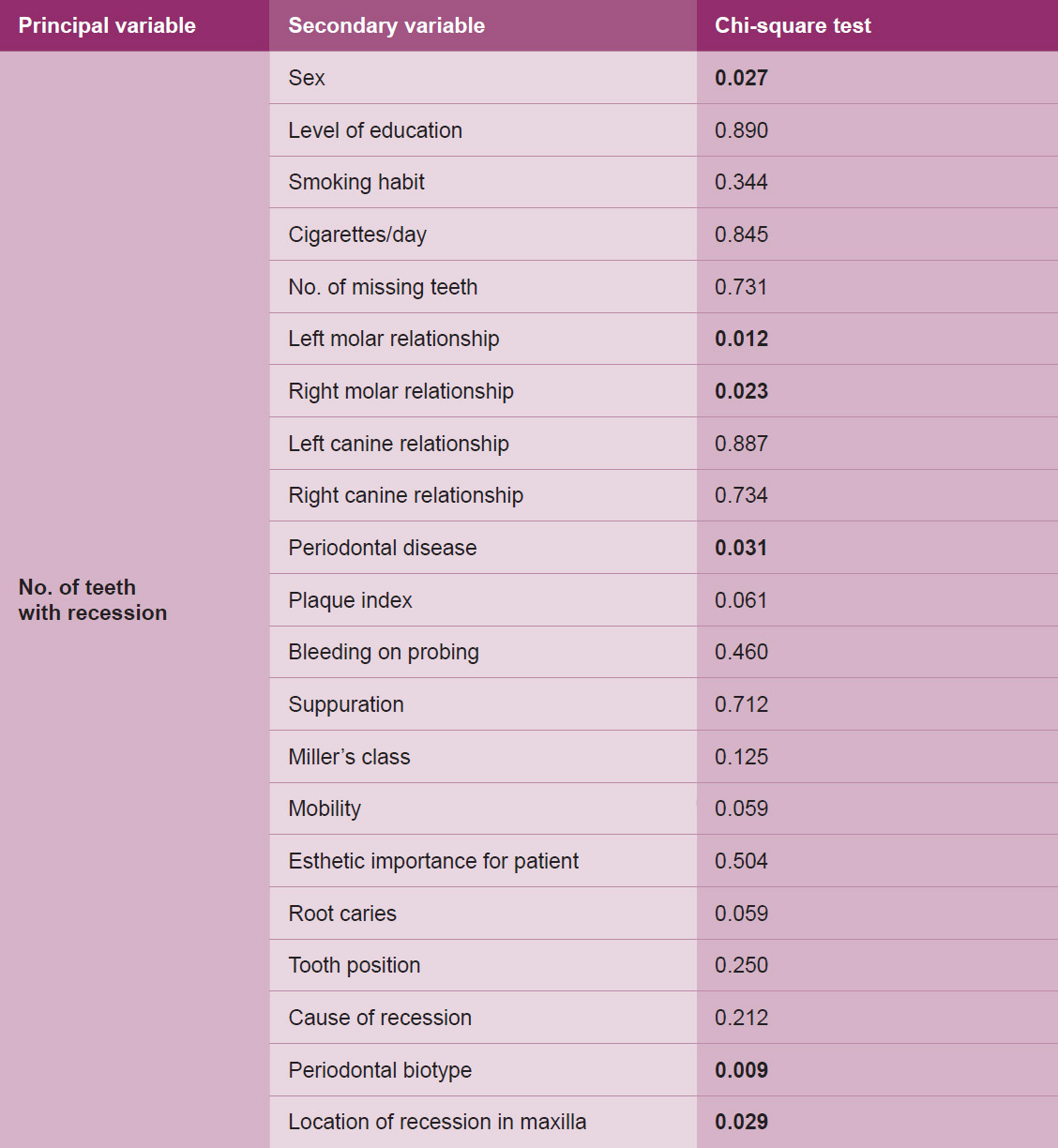
Table 4 Levels of significance for the variable “number of teeth with recession”.
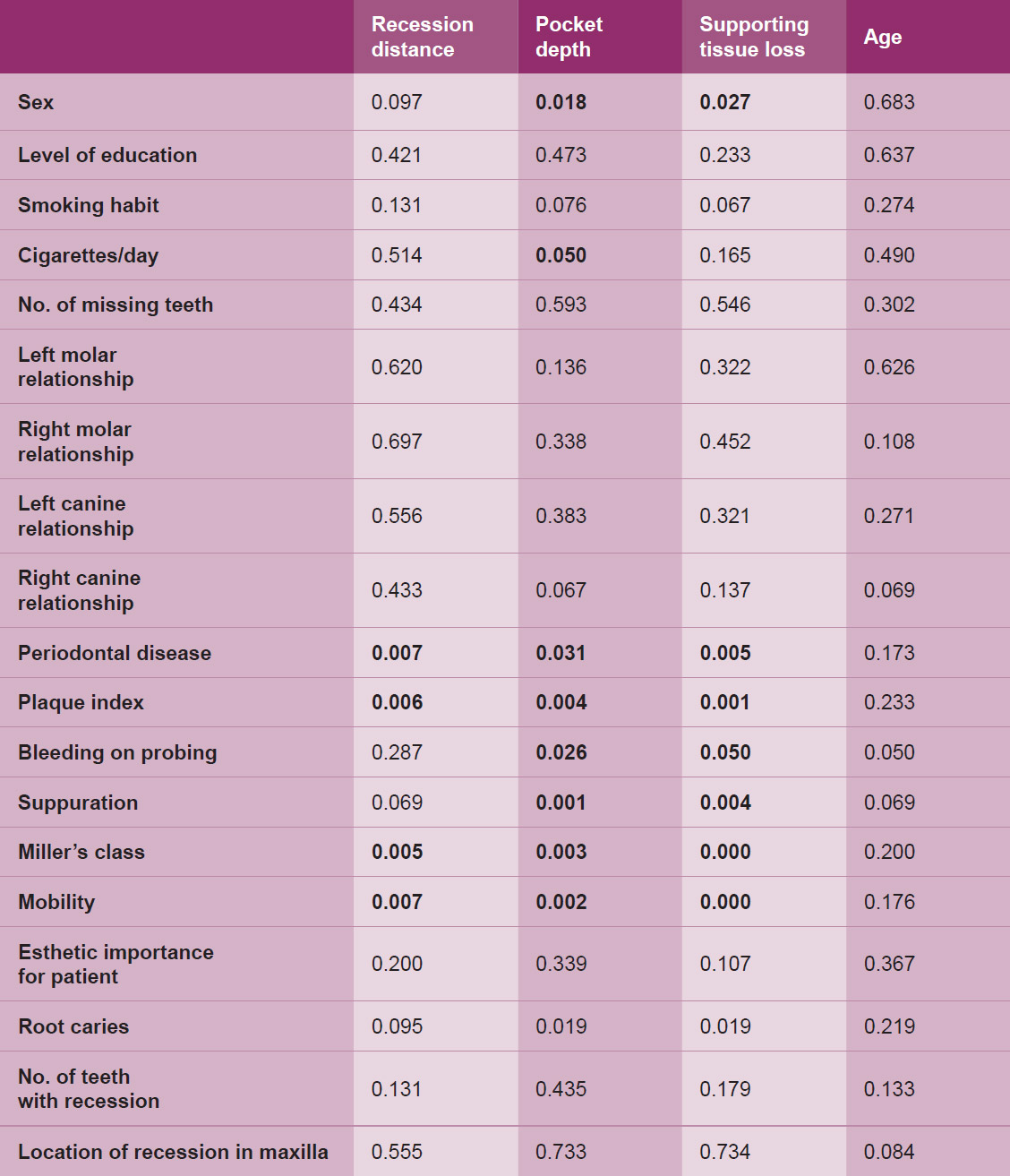
Table 5 Levels of significance for the quantitative variables “recession distance,” “pocket depth,” “supporting tissue loss” and “age”.
Sample size
The study was conducted during a period of 8 months between September 2016 and April 2017. For calculation of the sample size, the proportion of patients exposed to the etiological factors and who had gingival recession according to the literature was taken into account, that is, 35%. Therefore, we would have to obtain an odds ratio of 0.290; for a statistical power of 80%, we would need a sample of 86 patients. A random sample of 100 patients was analyzed from patients at the USC dental faculty, of which 26 had gingival recession, symptomatic or nonsymptomatic in the anterior zone. In these 26 patients, an additional evaluation of the recession characteristics was performed. To participate in this study, the patients’ consent was obtained to proceed with the data collection.
Statistical analysis
All data were coded and analyzed using the SPSS program (Version 20.0, IBM Corp.). Descriptive statistics were calculated using the frequencies and percentages for the categorical variables and the means and the standard deviations for the quantitative variables. Contingency tables were constructed using the chi-square test. Statistical analysis was performed by comparing means in nonparametric analysis using the Mann–Whitney test and 1-way analysis of variance. All the differences in which the value of P was less than or equal to 0.05 were considered statistically significant.
Results
The descriptive results of the study are summarized in Tables 1 and 2. The prevalence of recession in the anterior zone in patients at the USC dental faculty was 26% (n = 100). The average age of the patients in this study was 53.35 years. Of the total patients with gingival recession in the anterior zone, 57.7% were women.
Regarding smoking habit, 14 of the 26 patients who had recession in the anterior zone were nonsmokers. When we considered the molar relationship presented by the patients, both the left and right molar relationships were generally not assessable: 53.8% (left molar relationship) and 73.1% (right molar relationship). Among the 26 patients, 46.2% had more than 4 teeth with recession. Approximately 65% of the patients had periodontal disease, and almost 77% had plaque. However, the vast majority did not have suppuration of the teeth with recession (22 of 26 patients). All instances of recession in our study were classified as Miller class I or II. A total of 76.9% of the teeth with recession did not present with either mobility or root caries. Most teeth with recession had normal positioning in the arch (69.2%), and 65.4% of the patients did not regard the recession as esthetically important. The main cause of recession, in up to 30% of cases, was periodontal disease, and 53.8% of the patients had a thick periodontal biotype. We established 6 main variables: location of the recession in the maxilla, number of teeth with recession, age, distance of the recession from the cementoenamel junction (in millimeters), pocket depth and supporting tissue loss (Tables 3–5). There were statistically significant relationships between location of the recession in the maxilla and smoking habit and number of teeth with recession (chi-square test, P = 0.037). When recession were present in both arches, most patients were smokers and most had more than 4 teeth with recession. We also observed statistically significant associations between the number of teeth with recession and sex (chi-square test, P = 0.027), molar relationship (chi-square test, P = 0.012 and P = 0.023), periodontal disease presence (chi-square test, P = 0.031) and periodontal biotype (chi-square test, P = 0.009). In patients with more than 4 teeth with recession, 53.84% had a nonassessable molar relationship and 65.38% had periodontal disease; 50% of them had severe periodontal disease.
We observed that patients with 2 teeth with recession had a thick periodontal biotype, whereas among individuals with more than 4 teeth with recession, 83.7% had a thin periodontal biotype.
Regarding the other main variables, it is worth mentioning the statistically significant relationships established between distance of the recession from the cementoenamel junction, pocket depth and loss of supporting tissue, and periodontal disease and plaque index. The greater the severity of the periodontal disease and the higher the plaque index, the greater the measurements of recession distance, pocket depth and loss of supporting tissue. Statistically significant relationships were also observed between these 3 main variables and Miller’s class and the presence or absence of mobility. In the case of a Miller class II recession with or without mobility, the average recession distance, pocket depth and supporting tissue loss were significantly higher.
Discussion
In this study, which used a sample of 100 patients with an average age of 53.35 years, we obtained a prevalence of recession in the anterior zone of 26%. Comparison with other studies is difficult because most of them did not limit the study only to the presence of recession in the anterior zone. Even so, when comparing the prevalence rates with other research, taking the 26% into account, we noted that our prevalence rate was relatively lower.23Albandar JM, Kingman A. Gingival recession, gingival bleeding, and dental calculus in adults 30 years of age and older in the United States, 1988–1994. → J Periodontol. 1999 Jan;70(1):30–43.,24Gorman WJ. Prevalence and etiology of gingival recession. → J Periodontol. 1967 Jul–Aug;38(4):316–22.,25Matas F, Sentís J, Mendieta C. Ten-year longitudinal study of gingival recession in dentists. → J Clin Periodontol. 2011 Dec;38(12):1091–8.
In our study, recession was more frequent in women (57%) than in men. However, among patients with more than 4 teeth with recession, more than half were men. In our study, the number of missing teeth in relation to the presence of recession did not present a statistical relationship, as in other studies reviewed.26Vehkalahti M. Occurrence of gingival recession in adults. → J Periodontol. 1989 Nov;60(11):599–603. However, we did find a strong association between molar relationship and the number of teeth with recession. A large portion of the patients with more than 4 teeth with recession had a nonassessable molar relationship. This finding makes us think that the absence of the molars is likely to cause an excess of force on the anterior teeth and, as a consequence, the appearance of recession around more of those teeth.
Regarding smoking habit and its established relationship with the location of the recession in the maxilla, when patients had recession in both arches, more than 70% were smokers or had been until less than 5 years before. The same did not occur in patients who only had recession in 1 arch; more than 80% were nonsmokers. We have found studies in which the same relationship was established, including two that suggest the possible local effect of cigarettes. 27Haffajee AD, Socransky SS. Relationship of cigarette smoking to attachment level profiles. → J Clin Periodontol. 2001 Apr;28(4):283–95.,28Sarfati A, Bourgeois D, Katsahian S, Mora F, Bouchard P. Risk assessment for buccal gingival recession defects in an adult population. → J Periodontol. 2010 Oct;81(10):1419–25.
In our study, we noted that all instances of recession were classified into Miller class I or II, a finding that coincides with that of another study, in which most of the teeth observed were also classified as Miller class I or II.29Sarfati A, Bourgeois D, Katsahian S, Mora F, Bouchard P. Risk assessment for buccal gingival recession defects in an adult population. → J Periodontol. 2010 Oct;81(10):1419–25. Most studies argue that a thin periodontal biotype is a predisposing factor for recession.30Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. → J Am Dent Assoc. 2003 Feb;134(2):220–5.,31Palkovics D, Gera I. [The significance of biotype in the predictability of dental-periodontal treatment]. Hungarian. → Fogorv Sz. 2016 Jun;109(2):45–55. However, in this present study, more than half of the patients had a thick periodontal biotype and still had recession. However, the majority of patients with more than 4 teeth with recession had a thin periodontal biotype. The number of teeth with recession, the recession distance, the pocket depth and the supporting tissue loss presented strong associations with the presence of periodontal disease.
The exposure of the root to the oral cavity either directly by recession or by the presence of a periodontal pocket was directly related to an increased risk of root caries.32Tugnait A, Clerehugh V. Gingival recession—its significance and management. → J Dent. 2001 Aug;29(6):381–94. At the same time, our research revealed a relationship between the loss of supporting tissue and pocket depth. Based on the results obtained, the previous literature supports some of the established relationships, such as between the location of the recession in the maxilla and smoking or the relationships between supporting tissue loss, periodontal disease and plaque index. However, we also made findings in opposition to those of previous studies, as in the case of the relationship between the presence of recession and the periodontal biotype. One of the limitations of this study is the limited number of published studies to which to compare some of the relationships established between variables in our work.
Conclusion
The prevalence of recession in the anterior zone was relatively frequent in our setting, at 26% in this study. Comparison with other studies was difficult because others were not limited only to the anterior zone. There are many factors related to the presence of recession, such as smoking, periodontal disease, pocket depth, loss of supporting tissue and nonassessable molar relationship. It is necessary to identify these factors incipiently to prevent recession and associated complications. To make more powerful inferences, it would be necessary to conduct studies in broader subpopulations.
Competing interests
The authors declare that they have no competing interests.
Legends
Table 1 – Descriptive data of qualitative variables of the study.
Table 2 – Descriptive data of quantitative variables of the study.
Table 3 – Levels of significance for the variable “location of recession in maxilla”.
Table 4 – Levels of significance for the variable “number of teeth with recession”.
Table 5 – Levels of significance for the quantitative variables “recession distance,” “pocket depth,” “supporting tissue loss” and “age”.
References
| 1, 4, 23. | ↑ | Albandar JM, Kingman A. Gingival recession, gingival bleeding, and dental calculus in adults 30 years of age and older in the United States, 1988–1994. → J Periodontol. 1999 Jan;70(1):30–43. |
| 2, 7, 8, 10. | ↑ | Bouchard P, Malet J, Borghetti A. Decision-making in aesthetics: root coverage revisited. → Periodontol 2000. 2001;27:97–120. |
| 3. | ↑ | Cairo F, Pagliaro U, Nieri M. Treatment of gingival recession with coronally advanced flap procedures: a systematic review. → J Clin Periodontol. 2008 Sep;35(8 Suppl):136–62. |
| 5. | ↑ | Geiger AM. Mucogingival problems and the movement of mandibular incisors: a clinical review. → Am J Orthod. 1980 Nov;78(5):511–27. |
| 6, 20, 24. | ↑ | Gorman WJ. Prevalence and etiology of gingival recession. → J Periodontol. 1967 Jul–Aug;38(4):316–22. |
| 9, 11, 27. | ↑ | Haffajee AD, Socransky SS. Relationship of cigarette smoking to attachment level profiles. → J Clin Periodontol. 2001 Apr;28(4):283–95. |
| 12. | ↑ | Hägewald S, Spahr A, Rompola E, Haller B, Heijl L, Bernimoulin JP. Comparative study of Emdogain and coronally advanced flap technique in the treatment of human gingival recessions. A prospective controlled clinical study. → J Clin Periodontol. 2002 Jan;29(1):35–41. |
| 13, 30. | ↑ | Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. → J Am Dent Assoc. 2003 Feb;134(2):220–5. |
| 14. | ↑ | Löe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. → J Periodontol. 1992 Jun;63(6):489–95. |
| 15. | ↑ | Marini MG, Greghi SL, Passanezi E, Sant’ana AC. Gingival recession: prevalence, extension and severity in adults. → J Appl Oral Sci. 2004 Sep;12(3):250–5. |
| 16. | ↑ | Matas F, Sentis J, Mendieta C. Ten-year longitudinal study of gingival recession in dentists. → J Clin Periodontol. 2011 Dec;38(12):1091–8. |
| 17. | ↑ | Papapanou PN, Sanz M, Buduneli N, Dietrich T, Feres M, Fine DH, Flemmig TF, Garcia R, Giannobile WV, Graziani F, Greenwell H, Herrera D, Kao RT, Kebschull M, Kinane DF, Kirkwood KL, Kocher T, Kornman KS, Kumar PS, Loos BG, Machtei E, Meng H, Mombelli A, Needleman I, Offenbacher S, Seymour GJ, Teles R, Tonetti MS. Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. → J Periodontol. 2018 Jun;89 Suppl 1:173–82. |
| 18. | ↑ | Kayalvizhi G, Radha S, Prathima GS, Mohandoss S, Ramesh V, Arumugam SB. Comparative evaluation of plaque removal effectiveness of manual and chewable toothbrushes in children: a randomized clinical trial. → Int J Clin Pediatr Dent. 2019 Mar–Apr;12(2):107–10. |
| 19. | ↑ | Zweers J, Thomas RZ, Slot DE, Weisgold AS, Van der Weijden FG. Characteristics of periodontal biotype, its dimensions, associations and prevalence: a systematic review. → J Clin Periodontol. 2014 Oct;41(10):958–71. |
| 21. | ↑ | Rajapakse PS, McCracken GI, Gwynnett E, Steen ND, Guentsch A, Heasman PA. Does tooth brushing influence the development and progression of non-inflammatory gingival recession? A systematic review. → J Clin Periodontol. 2007 Dec;34(12):1046–61. |
| 22. | ↑ | Bin Bahar BS, Alkhalidy SR, Kaklamanos EG, Athanasiou AE. Do orthodontic patients develop more gingival recession in anterior teeth compared to untreated individuals? A systematic review of controlled studies. → Int Orthod. 2019 Nov 1. pii: S1761-7227(19)30155-X. doi: 10.1016/ j.ortho.2019.08.025. |
| 25. | ↑ | Matas F, Sentís J, Mendieta C. Ten-year longitudinal study of gingival recession in dentists. → J Clin Periodontol. 2011 Dec;38(12):1091–8. |
| 26. | ↑ | Vehkalahti M. Occurrence of gingival recession in adults. → J Periodontol. 1989 Nov;60(11):599–603. |
| 28, 29. | ↑ | Sarfati A, Bourgeois D, Katsahian S, Mora F, Bouchard P. Risk assessment for buccal gingival recession defects in an adult population. → J Periodontol. 2010 Oct;81(10):1419–25. |
| 31. | ↑ | Palkovics D, Gera I. [The significance of biotype in the predictability of dental-periodontal treatment]. Hungarian. → Fogorv Sz. 2016 Jun;109(2):45–55. |
| 32. | ↑ | Tugnait A, Clerehugh V. Gingival recession—its significance and management. → J Dent. 2001 Aug;29(6):381–94. |





Leave a Reply
Be the First to Comment!