Prevalence of oral lesions among patients in the dental faculty of the University of Santiago de Compostela, Spain
March 21, 2019 / Categories: Digital Dentistry, Implant Dentistry

Caeiro Villasenín, Lucía
García García, Abel
Lorenzo Pouso, Alejandro Ismael
Chamorro Petronacci, Cintia
Blanco Carrión, Andrés
Gándara Vila, Pilar
Pérez Sayáns, Mario
Abstract
Background
The main objective of this study was to evaluate the prevalence of white, red and pigmented lesions of the oral cavity among patients attending the dental faculty of the University of Santiago de Compostela, Spain.
Materials and methods
We designed an epidemiological, cross-sectional, descriptive and observational study. White, red and pigmented lesions were evaluated randomly in a total of 100 patients. Data such as patient’s demographics, smoking habit, presence or absence of oral lesions (and their features) and whether the patient was aware of the presence of the lesion were collected. Descriptive statistics were calculated, and contingency tables were constructed using the chi-squared test. Analytical statistics were performed by comparing means in nonparametric analyses using the Mann–Whitney U test.
Results
The total prevalence of oral lesions was 22% (n = 100). The average age of the patients was 54.68 years (SD = 14.64). Most patients with oral lesions were women (60%) and the average size of the lesions was 1.83 cm. Most of the lesions were red (almost 60%) and asymptomatic (> 90%). There was a known causal link for almost all lesions, with a percentage of higher than 80%. Most patients (69.2%) were aware of the presence of the lesion when it was red (P = 0.016).
Conclusion
The most frequent type of lesion in this study population was a red lesion, located on the lip, with a hypertrophic surface, asymptomatic and with a known causal nexus. Periodical check-ups are fundamental to be able to make an early diagnosis of any lesions, as no patient with a white lesion was aware of the risk of it being a premalignant or malignant lesion.
Keywords
Oral mucosa; lesion prevalence; Spanish population.
Introduction
An oral mucosal lesion is defined as any abnormal alteration in color or surface appearance, swelling or loss of integrity of the oral mucosal surface, which may interfere with the quality of daily life of the persons affected. Etiological factors of oral mucosal lesions include infection, local trauma and metabolic, immunological and neoplastic diseases.1Mansour Ghanaei F, Joukar F, Rabiei M, Dadashzadeh A, Kord Valeshabad A. Prevalence of oral mucosal lesions in an adult Iranian population. → Iran Red Crescent Med J. 2013 Jul;15(7):600–4.2Feng J, Zhou Z, Shen X, Wang Y, Shi L, Wang Y, Hu Y, Sun H, Liu W. Prevalence and distribution of oral mucosal lesions: a cross-sectional study in Shanghai, China. → J Oral Pathol Med. 2015 Aug;44(7):490–4. Socio-demographic factors and behavior too have been associated with oral mucosal lesions.3Do LG, Spencer AJ, Dost F, Farah CS. Oral mucosal lesions: findings from the Australian National Survey of Adult Oral Health. → Aust Dent J. 2014 Mar;59(1):114–20.
Studies on distribution of oral lesions allow us to estimate disease prevalence in a population and thus identify a subpopulation of high risk. For these subpopulations, we can then prepare health strategies in the different areas.4Cebeci AR, Gülşahi A, Kamburoglu K, Orhan BK, Oztaş B. Prevalence and distribution of oral mucosal lesions in an adult Turkish population. → Med Oral Patol Oral Cir Bucal. 2009 Jun 1;14(6):E272–7. In several regions of the world, studies have confirmed the wide variation in both prevalence and the most common types of lesions in the oral cavity (Table 1).
The oral mucosa can be affected by a great variety of injuries and conditions. Oral cavity lesions are considered a general health indicator. Early identification is essential for integral medical care. Therefore, soft-tissue examination must be done systematically to include the whole cavity.5Ali M, Joseph B, Sundaram D. Prevalence of oral mucosal lesions in patients of the Kuwait University Dental Center. → Saudi Dent J. 2013 Jul;25(3):111–8. Although most oral lesions are benign and do not need active treatment, some of them can involve a significant pathology. Those lesions associated with a high risk of malignant transformation are especially important. Oral cancer is a malignant tumor with an increasing prevalence. Despite technological and biological advances, its prognosis has not improved in the last decades. Early diagnosis is the most important factor for an improved survival rate. Information about risk factors of oral lesions is the first step toward investigating oral cancer prevention.6Campisi G, Margiotta V. Oral mucosal lesions and risk habits among men in an Italian study population. → J Oral Pathol Med. 2001 Jan;30(1):22–8.
Prevalence of oral mucosal lesions and their associated factors have not been previously registered in the Santiago de Compostela population. This prevalence varies significantly between geographic locations and the extrapolation of other studies’ results would not be meaningful. Accordingly, the main aim of this study was to evaluate the prevalence of white, red and pigmented lesions in the oral cavities of patients attending the dental faculty of the University of Santiago de Compostela. A secondary aim was to analyze patients’ variable features and awareness of their lesions.
Materials and methods
An epidemiological, cross-sectional, descriptive and observational study was designed to determine prevalence of white, red and pigmented lesions among patients attending the dental faculty of the University of Santiago de Compostela. The study was conducted over a period of 8 months between September 2016 and April 2017. All of the procedures were carried out with the proper understanding and written consent of the patients in accordance with the Declaration of Helsinki.
| Country | Year of publication | Sample size | Identified oral lesions (%) |
|---|---|---|---|
| Malaysia | 19977Zain RB, Ikeda N, Razak IA, Axéll T, Majid ZA, Gupta PC, Yaacob M. A national epidemiological survey of oral mucosal lesions in Malaysia. → Community Dent Oral Epidemiol. 1997 Oct;25(5):377–83. | 11-707 | 9.7 |
| Slovenia (Ljubljana) | 20008Kovac-Kovacic M, Skaleric U. The prevalence of oral mucosal lesions in a population in Ljubljana, Slovenia. → J Oral Pathol Med. 2000 Aug;29(7):331–5. | 1-692 | 61.6 |
| Spain (Oviedo) | 20029Garcia-Pola Vallejo MJ, Martinez Diaz-Canel AI, Garcia Martin JM, Gonzalez Garcia M. Risk factors for oral soft tissue lesions in an adult Spanish population. → Community Dent Oral Epidemiol. 2002 Aug;30(4):277–85. | 308 | 51.1 |
| U.S. | 200410Shulman JD, Beach MM, Rivera-Hidalgo F. The prevalence of oral mucosal lesions in U.S. adults: data from the Third National Health and Nutrition Examination Survey, 1988–1994. → J Am Dent Assoc. 2004 Sep;135(9):1279–86. | 17-235 | 27.9 |
| Italy (Turin) | 200811Pentenero M, Broccoletti R, Carbone M, Conrotto D, Gandolfo S. The prevalence of oral mucosal lesions in adults from the Turin area. → Oral Dis. 2008 May;14(4):356–66. | 4-098 | 25.09 |
| India (Karnataka state) | 200812Mathew AL, Pai KM, Sholapurkar AA, Vengal M. The prevalence of oral mucosal lesions in patients visiting a dental school in Southern India. → Indian J Dent Res. 2008 Apr–Jun;19(2):99–103. 1 | 1-190 | 41.2 |
| Saudi Arabia | 200913Al-Mobeeriek A, AlDosari AM. Prevalence of oral lesions among Saudi dental patients. → Ann Saudi Med. 2009 Sep–Oct;29(5):365–8. | 2-552 | 15 |
| Turkey | 200914Cebeci AR, Gülşahi A, Kamburoglu K, Orhan BK, Oztaş B. Prevalence and distribution of oral mucosal lesions in an adult Turkish population. → Med Oral Patol Oral Cir Bucal. 2009 Jun 1;14(6):E272–7. | 5-000 | 15.5 |
| North India | 201315Bhatnagar P, Rai S, Bhatnagar G, Kaur M, Goel S, Prabhat M. Prevalence study of oral mucosal lesions, mucosal variants, and treatment required for patients reporting to a dental school in North India: in accordance with WHO guidelines. → J Family Community Med. 2013 Jan;20(1):41–8. | 8-866 | 16.8 |
| Sweden | 201316Robledo-Sierra J, Mattsson U, Svedensten T, Jontell M. The morbidity of oral mucosal lesions in an adult Swedish population. → Med Oral Patol Oral Cir Bucal. 2013 Sep 1;18(5):e766–72. | 6-448 | 14.7 |
| Kuwait | 201317Ali M, Joseph B, Sundaram D. Prevalence of oral mucosal lesions in patients of the Kuwait University Dental Center. → Saudi Dent J. 2013 Jul;25(3):111–8. | 530 | 58.1 |
| Iran | 201318Mansour Ghanaei F, Joukar F, Rabiei M, Dadashzadeh A, Kord Valeshabad A. Prevalence of oral mucosal lesions in an adult Iranian population. → Iran Red Crescent Med J. 2013 Jul;15(7):600–4. | 1-581 | 19.4 |
| Australia | 201419Do LG, Spencer AJ, Dost F, Farah CS. Oral mucosal lesions: findings from the Australian National Survey of Adult Oral Health. → Aust Dent J. 2014 Mar;59(1):114–20. | 3-551 | 20.5 |
| China (Shanghai) | 201420Feng J, Zhou Z, Shen X, Wang Y, Shi L, Wang Y, Hu Y, Sun H, Liu W. Prevalence and distribution of oral mucosal lesions: a cross-sectional study in Shanghai, China. → J Oral Pathol Med. 2015 Aug;44(7):490–4. | 11-054 | 10.8 |
| Brazil | 201521Gheno JN, Martins MA, Munerato MC, Hugo FN, Sant’ana Filho M, Weissheimer C, Carrard VC, Martins MD. Oral mucosal lesions and their association with sociodemographic, behavioral, and health status factors. → Braz Oral Res. 2015;29. pii: S1806-83242015000100289. doi: 10.1590/1807-3107BOR-2015.vol29.0093. Epub 2015 Aug 4. | 801 | 46.9 |
Eligibility criteria
Inclusion criterion: all adult patients attending the dental faculty of the University of Santiago de Compostela. Exclusion criterion: patients younger than 18 years old.
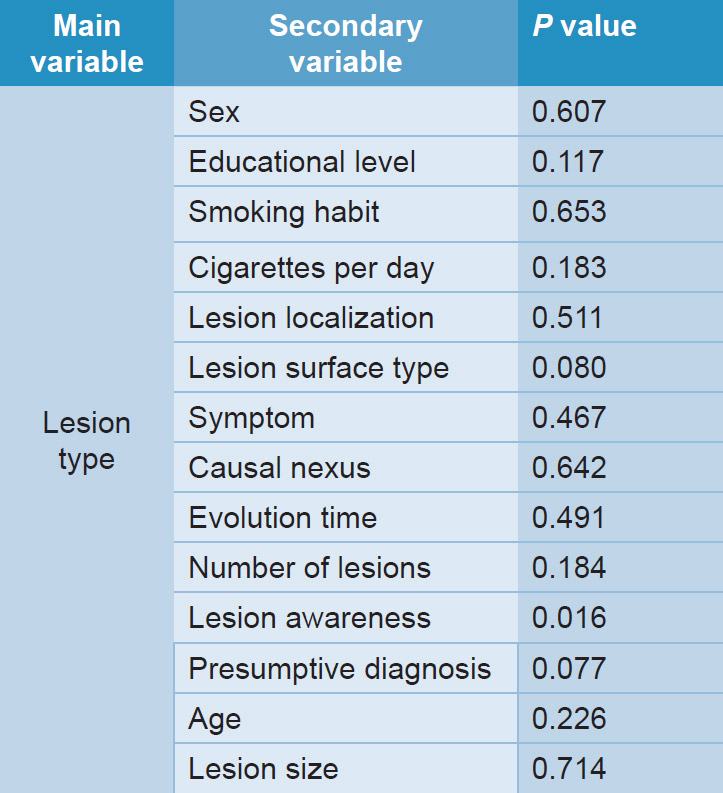
Table 3: Chi-squared test.
Data extraction
Two specific operators performed data collection and extraction, after previous calibration for correct evaluation of the variables. In cases of discrepancy, a third operator corroborated the results. The agreement in this process was calculated using Cohen’s kappa coefficient, and a κ score of 0.8 was obtained.22McHugh ML. Interrater reliability: the kappa statistic. → Biochem Med (Zagreb). 2012;22(3):276–82. Patient exploration was carried out using an exploration kit consisting of a mirror, an exploration probe and a CP12 periodontal probe.
Clinical parameters
Clinical parameters noted from patients were as follows:
• demographic data (age, sex and educational level);
• smoking habit (yes/no and cigarettes per day);
• presence of oral lesions (yes/no);
• lesion features (type, localization, size, presence of symptoms, single/multiple, atrophic/hypertrophic surface, causal nexus [if the patient or the operator found any causal factor], evolution time and presumptive diagnosis);
• whether the patient was aware of the presence of the lesion (if the patient thought that he or she may have a lesion this was considered to demonstrate awareness).
We classified the type of lesion (white/red/pigmented) and surface (atrophic/hypertrophic) according to the most prevalent aspect or the more serious aspect in terms of clinical prognosis in cases of mixed lesions.
Sample size
To estimate the sample size, the greater proportion of patients affected by oral lesions was taken into account according to the literature, that is, 35%. To obtain a statistic potential of 80%, we needed a total of 86 patients. Finally, we analyzed a randomized sample of 100 patients.
Statistical analysis
All data were coded and analyzed using IBM SPSS Statistics software (Version 20). Descriptive statistics were calculated using frequencies and percentages for the categorical variables and means and standard deviations for the quantitative variables. Contingency tables were constructed using the chi-squared test. Analytical statistics were performed by comparing means in nonparametric analyses, using the Mann– Whitney U test and 1-way analysis of variance. All of the differences in which the P value was ≤ 0.05 were considered statistically significant.
Results
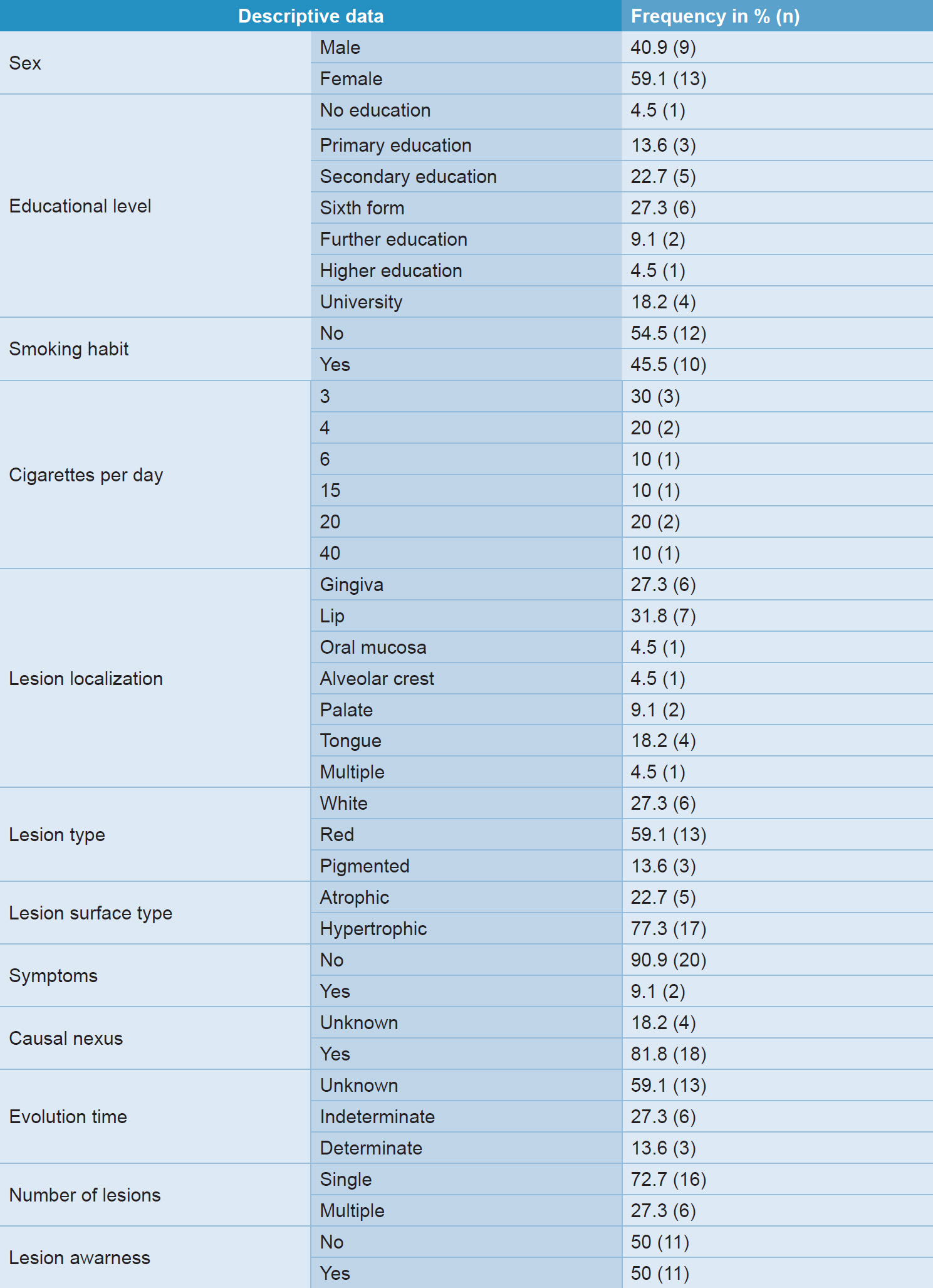
A total of 100 patients were examined. Table 2 summarizes descriptive data of the patients with oral lesions. The patients’ mean age was 54.68 years (SD = 14.64). Most patients with oral lesions were women (almost 60%). The mean lesion size was 1.83 cm (SD = 41.79). In the bivariate analysis, in which the main variable was the type of lesion, white, red or pigmented (Table 3), we observed that the patient was aware of the lesion when the lesion was red (69.2%) or pigmented (66.7%), but not when it was white (0%). Regarding the influence of sex on the type of lesion, we observed that more than 60% of pigmented lesions occurred in males, while red and white lesions were predominant in women.
According to smoking habit, 66.7% of the total pigmented lesions were in smokers. Of those smokers with pigmented lesions, all smoked more than 10 cigarettes per day.
The location affected the type of lesion in the following way: In the case of red lesions, most were located on the lip. In white lesions, most were located on the palatal mucosa. The pigmented ones appeared in the gingivae.
All of the white lesions diagnosed had a hypertrophic surface. Of the red lesions, almost 80% had a hypertrophic surface. However, most of the pigmented lesions had an atrophic surface (66.7%).
More than 80% of the white lesions and more than 70% of the red lesions had a known causal nexus. All of the pigmented lesions in this study had a known causal nexus. More than 80% of the red lesions presented singularly. In the case of white lesions, the majority were also single lesions (66.7%). The pigmented ones, however, presented in multiples. No patient with a white lesion was aware of the lesion. However, almost 70% of patients with red lesions were aware that they had them. These differences are statistically significant, according to the chi-squared test (P = 0.016). Red lesions tended to appear in older patients, and white and pigmented lesions affected younger patients. Pigmented lesions were less frequent than white lesions and white lesions were less frequent than red lesions.
Discussion
Our results revealed a prevalence of 22% of oral lesions in patients attending the dental faculty. Previous studies show that prevalence varies significantly in general populations (range: 9.7–61.6%; Table 1). The majority of the lesions were red (59.1%), followed by white (27.3%) and pigmented ones (13.6%).
According to our study, red lesions are more frequent in older people than white or pigmented ones. A study carried out in an elderly Chilean population agrees with our finding of a higher frequency of red lesions at older ages.23Rivera C, Droguett D, Arenas-Marquez MJ. Oral mucosal lesions in a Chilean elderly population: a retrospective study with a systematic review from thirteen countries. → J Clin Exp Dent. 2017 Feb 1;9(2):e276–e283. doi: 10.4317/jced.53427. In the total number of patients diagnosed with any type of lesion, white, red or pigmented, there was a greater number of women (59.1%). In other studies, a higher prevalence of lesions in women had already been reported.24Kovac-Kovacic M, Skaleric U. The prevalence of oral mucosal lesions in a population in Ljubljana, Slovenia. → J Oral Pathol Med. 2000 Aug;29(7):331–5. Other studies have reported a higher prevalence of lesions in males.25Bhatnagar P, Rai S, Bhatnagar G, Kaur M, Goel S, Prabhat M. Prevalence study of oral mucosal lesions, mucosal variants, and treatment required for patients reporting to a dental school in North India: in accordance with WHO guidelines. → J Family Community Med. 2013 Jan;20(1):41–8.26Jahanbani J, Sandvik L, Lyberg T, Ahlfors E. Evaluation of oral mucosal lesions in 598 referred Iranian patients. → Open Dent J. 2009 Mar 27;3:42–7. However, there are studies that support no significant difference in prevalence between women and men.27Ali M, Joseph B, Sundaram D. Prevalence of oral mucosal lesions in patients of the Kuwait University Dental Center. → Saudi Dent J. 2013 Jul;25(3):111–8.
In our study, 63.6% of patients with lesions had only sixth form and secondary education. We would think that patients with a higher educational level would have a greater concern for oral health and therefore come to the consultation with a suspicion of a lesion. In other studies, a higher prevalence of oral diseases was reported in patients of lower socioeconomic status, which may be the result of a lower educational level.28Sehgal VN, Syed NH, Aggarwal A, Sehgal S. Oral mucosal lesions: miscellaneous—Part III. → Skinmed. 2016 Jun 01;14(3):193–201.
A slightly higher percentage of patients who participated in this study were nonsmokers. We could attribute this to the growing antismoking campaign of recent decades, increasing gradual awareness of the dangers of this habit. In a study conducted in 2001 in Italy, 88% of the sample were already aware of the damage caused by smoking.29Campisi G, Margiotta V. Oral mucosal lesions and risk habits among men in an Italian study population. → J Oral Pathol Med. 2001 Jan;30(1):22–8. In another study conducted in Kuwait in 2013, smoking participants reported that they would consider quitting if an improvement of oral health could be demonstrated as a result.30Ali M, Joseph B, Sundaram D. Prevalence of oral mucosal lesions in patients of the Kuwait University Dental Center. → Saudi Dent J. 2013 Jul;25(3):111–8.
The relative risk of oral cancer increases proportionally with the level and duration of tobacco use. It has been reported that the benefit of stopping smoking is large and can be realized in a relatively short period.31Foy JP, Bertolus C, William WN, Saintigny P. Oral premalignancy: the roles of early detection and chemoprevention. → Otolaryngol Clin North Am. 2013 Aug;46(4):579–97. Two pathogenic factors are fundamentally involved in the development of pigmented lesions: race and smoking.32Foy JP, Bertolus C, William WN, Saintigny P. Oral premalignancy: the roles of early detection and chemoprevention. → Otolaryngol Clin North Am. 2013 Aug;46(4):579–97. Regarding tobacco, it stands out in this study that 66.7% of the total pigmented lesions were in smokers who smoked more than 10 cigarettes per day. Regarding the influence of race, in the Asian population, the prevalence of pigmented lesions was 79%,33Axell T, Zain RB, Siwamogstham P, Tantiniran D, Thampipit J. Prevalence of oral soft tissue lesions in out-patients at two Malaysian and Thai dental schools. → Community Dent Oral Epidemiol. 1990 Apr;18(2):95–9. while in this study it was 3%, similar to that in other studies in European populations.34Salonen L, Axéll T, Helldén L. Occurrence of oral mucosal lesions, the influence of tobacco habits and an estimate of treatment time in an adult Swedish population. → J Oral Pathol Med. 1990 Apr;19(4):170–6.
The location of the most frequent lesions in the present study was the lip (31.8%). We suggest that this is related to the lips being the first barrier to the oral cavity. Because of this, they are constantly exposed to various irritants, which play an important role in the etiology of lesions in this location.35Arslan S, Cobanoglu B, Ural A, Saygin I, Isik AU. A 15-year retrospective study of 160 cases of benign lip lesions. → J Laryngol Otol. 2015 Dec;129(12):1224–7. Most of the lesions had a hypertrophic surface, almost 80%, which could be related to the higher prevalence of traumatic injuries. Only 9.1% of patients reported symptoms. This result was similar to that of other studies.36Robledo-Sierra J, Mattsson U, Svedensten T, Jontell M. The morbidity of oral mucosal lesions in an adult Swedish population. → Med Oral Patol Oral Cir Bucal. 2013 Sep 1;18(5):e766–72.
More than 70% of the lesions diagnosed were single lesions, a fact that coincides with the study of the population of Oviedo, where single lesions also predominated. 37Garcia-Pola Vallejo MJ, Martinez Diaz-Canel AI, Garcia Martin JM, Gonzalez Garcia M. Risk factors for oral soft tissue lesions in an adult Spanish population. → Community Dent Oral Epidemiol. 2002 Aug;30(4):277–85.
None of the patients with white lesions in this study were aware of them, probably because this type of lesion is usually asymptomatic. However, those with red lesions were aware of these (69.2%), as were those with pigmented lesions (66.7%). This is a very important result because it indicates that patients may miss some types of premalignant lesion, resulting in a delay in seeking diagnosis and treatment. The knowledge of risk factors and the recognition of symptoms by patients are crucial factors. A study conducted in Scotland in 2010, which assessed the initial recognition of symptoms in oral cancer patients, described a great variety of symptoms, among which were “bulto” and “white spot.”38Grant E, Silver K, Bauld L, Day R, Warnakulasuriya S. The experiences of young oral cancer patients in Scotland: symptom recognition and delays in seeking professional help. → Br Dent J. 2010 May 22;208(10):465–71. Many of the patients stated that they used self-medication obtained from a pharmacy after noticing the initial symptoms, which generally resulted in delayed diagnosis and treatment.39Grant E, Silver K, Bauld L, Day R, Warnakulasuriya S. The experiences of young oral cancer patients in Scotland: symptom recognition and delays in seeking professional help. → Br Dent J. 2010 May 22;208(10):465–71.
Conclusion
The prevalence of lesions in the oral cavity found in this study was 22%. Most lesions appeared in women. The most frequent type of lesion in this study population was red; in terms of location, the lip was the most prevalent site. Hypertrophic and asymptomatic lesions were more frequent. In more than 80% of the patients, we could identify a known causal nexus. No patient with a white lesion was aware of it. Periodical checkups are fundamental to be able to make an early diagnosis of any lesions, as no patient with a white lesion was aware of the risk of it being a premalignant or malignant lesion.
Competing interests
The authors declare that there are no conflicts of interest in connection with this article, including there being no funding sources.
References
| 1, 18. | ↑ | Mansour Ghanaei F, Joukar F, Rabiei M, Dadashzadeh A, Kord Valeshabad A. Prevalence of oral mucosal lesions in an adult Iranian population. → Iran Red Crescent Med J. 2013 Jul;15(7):600–4. |
| 2, 20. | ↑ | Feng J, Zhou Z, Shen X, Wang Y, Shi L, Wang Y, Hu Y, Sun H, Liu W. Prevalence and distribution of oral mucosal lesions: a cross-sectional study in Shanghai, China. → J Oral Pathol Med. 2015 Aug;44(7):490–4. |
| 3, 19. | ↑ | Do LG, Spencer AJ, Dost F, Farah CS. Oral mucosal lesions: findings from the Australian National Survey of Adult Oral Health. → Aust Dent J. 2014 Mar;59(1):114–20. |
| 4, 14. | ↑ | Cebeci AR, Gülşahi A, Kamburoglu K, Orhan BK, Oztaş B. Prevalence and distribution of oral mucosal lesions in an adult Turkish population. → Med Oral Patol Oral Cir Bucal. 2009 Jun 1;14(6):E272–7. |
| 5, 17, 27, 30. | ↑ | Ali M, Joseph B, Sundaram D. Prevalence of oral mucosal lesions in patients of the Kuwait University Dental Center. → Saudi Dent J. 2013 Jul;25(3):111–8. |
| 6, 29. | ↑ | Campisi G, Margiotta V. Oral mucosal lesions and risk habits among men in an Italian study population. → J Oral Pathol Med. 2001 Jan;30(1):22–8. |
| 7. | ↑ | Zain RB, Ikeda N, Razak IA, Axéll T, Majid ZA, Gupta PC, Yaacob M. A national epidemiological survey of oral mucosal lesions in Malaysia. → Community Dent Oral Epidemiol. 1997 Oct;25(5):377–83. |
| 8, 24. | ↑ | Kovac-Kovacic M, Skaleric U. The prevalence of oral mucosal lesions in a population in Ljubljana, Slovenia. → J Oral Pathol Med. 2000 Aug;29(7):331–5. |
| 9, 37. | ↑ | Garcia-Pola Vallejo MJ, Martinez Diaz-Canel AI, Garcia Martin JM, Gonzalez Garcia M. Risk factors for oral soft tissue lesions in an adult Spanish population. → Community Dent Oral Epidemiol. 2002 Aug;30(4):277–85. |
| 10. | ↑ | Shulman JD, Beach MM, Rivera-Hidalgo F. The prevalence of oral mucosal lesions in U.S. adults: data from the Third National Health and Nutrition Examination Survey, 1988–1994. → J Am Dent Assoc. 2004 Sep;135(9):1279–86. |
| 11. | ↑ | Pentenero M, Broccoletti R, Carbone M, Conrotto D, Gandolfo S. The prevalence of oral mucosal lesions in adults from the Turin area. → Oral Dis. 2008 May;14(4):356–66. |
| 12. | ↑ | Mathew AL, Pai KM, Sholapurkar AA, Vengal M. The prevalence of oral mucosal lesions in patients visiting a dental school in Southern India. → Indian J Dent Res. 2008 Apr–Jun;19(2):99–103. 1 |
| 13. | ↑ | Al-Mobeeriek A, AlDosari AM. Prevalence of oral lesions among Saudi dental patients. → Ann Saudi Med. 2009 Sep–Oct;29(5):365–8. |
| 15, 25. | ↑ | Bhatnagar P, Rai S, Bhatnagar G, Kaur M, Goel S, Prabhat M. Prevalence study of oral mucosal lesions, mucosal variants, and treatment required for patients reporting to a dental school in North India: in accordance with WHO guidelines. → J Family Community Med. 2013 Jan;20(1):41–8. |
| 16, 36. | ↑ | Robledo-Sierra J, Mattsson U, Svedensten T, Jontell M. The morbidity of oral mucosal lesions in an adult Swedish population. → Med Oral Patol Oral Cir Bucal. 2013 Sep 1;18(5):e766–72. |
| 21. | ↑ | Gheno JN, Martins MA, Munerato MC, Hugo FN, Sant’ana Filho M, Weissheimer C, Carrard VC, Martins MD. Oral mucosal lesions and their association with sociodemographic, behavioral, and health status factors. → Braz Oral Res. 2015;29. pii: S1806-83242015000100289. doi: 10.1590/1807-3107BOR-2015.vol29.0093. Epub 2015 Aug 4. |
| 22. | ↑ | McHugh ML. Interrater reliability: the kappa statistic. → Biochem Med (Zagreb). 2012;22(3):276–82. |
| 23. | ↑ | Rivera C, Droguett D, Arenas-Marquez MJ. Oral mucosal lesions in a Chilean elderly population: a retrospective study with a systematic review from thirteen countries. → J Clin Exp Dent. 2017 Feb 1;9(2):e276–e283. doi: 10.4317/jced.53427. |
| 26. | ↑ | Jahanbani J, Sandvik L, Lyberg T, Ahlfors E. Evaluation of oral mucosal lesions in 598 referred Iranian patients. → Open Dent J. 2009 Mar 27;3:42–7. |
| 28. | ↑ | Sehgal VN, Syed NH, Aggarwal A, Sehgal S. Oral mucosal lesions: miscellaneous—Part III. → Skinmed. 2016 Jun 01;14(3):193–201. |
| 31, 32. | ↑ | Foy JP, Bertolus C, William WN, Saintigny P. Oral premalignancy: the roles of early detection and chemoprevention. → Otolaryngol Clin North Am. 2013 Aug;46(4):579–97. |
| 33. | ↑ | Axell T, Zain RB, Siwamogstham P, Tantiniran D, Thampipit J. Prevalence of oral soft tissue lesions in out-patients at two Malaysian and Thai dental schools. → Community Dent Oral Epidemiol. 1990 Apr;18(2):95–9. |
| 34. | ↑ | Salonen L, Axéll T, Helldén L. Occurrence of oral mucosal lesions, the influence of tobacco habits and an estimate of treatment time in an adult Swedish population. → J Oral Pathol Med. 1990 Apr;19(4):170–6. |
| 35. | ↑ | Arslan S, Cobanoglu B, Ural A, Saygin I, Isik AU. A 15-year retrospective study of 160 cases of benign lip lesions. → J Laryngol Otol. 2015 Dec;129(12):1224–7. |
| 38, 39. | ↑ | Grant E, Silver K, Bauld L, Day R, Warnakulasuriya S. The experiences of young oral cancer patients in Scotland: symptom recognition and delays in seeking professional help. → Br Dent J. 2010 May 22;208(10):465–71. |





Leave a Reply
Be the First to Comment!