Sinus lift surgery in severely resorbed maxillae: One-year follow-up
May 8, 2018 / Categories: Digital Dentistry, Implant Dentistry

Canullo, Luigi
Abstract
Objective
The aim of this prospective study was to clinically analyze the behavior of implants inserted into severely resorbed maxillae after sinus grafting.
Materials and methods
Twenty-six wide-diameter implants with a rough surface over their entire length were inserted during 13 consecutive sinus lifts. Radiographic analysis was preoperatively requested for each patient. After Schneiderian membrane elevation, a magnesium-enriched hydroxyapatite (Mg-e HA) and collagen-based scaffold with a porous 3-D structure was used to prevent perforation during implant placement. Sinus grafting was performed using a biomimetic Mg-e HA. No membrane was used to cover the buccal window. The preoperative residual bone height ranged between 1 and 4 mm (mean value: 2.5 mm; SD: 1.0 mm). After 6 months of healing, uncovering was carried out and the definitive restoration was seated after 2 weeks. In order to monitor the stability changes, resonance frequency analysis was performed and ISQ (Implant Stability Quotient) values were collected at the first surgery (baseline, T0), at the abutment connection (T1) and at the 1-year follow-up (T2). In order to measure bone changes, the patients underwent panoramic radiographs after 2-year follow-up. Image analysis software calculated the grafted bone height changes at the level of the implant site, comparing preoperative and follow-up panoramic radiographs.
Results
No postoperative complications were observed. The mean ISQ value was 42.5 (SD: 2.7) at T0, 75.3 (SD: 8.2) at T1 and 81.5 (SD: 2.6) at T2. Statistically significant differences (P ≤ 0.005) regarding mean ISQ values were found between T1 and T0, as well as between T1 and T2. After 12 months of functional loading, only 1 implant was lost (cumulative survival rate: 96.15%). During the same observation period, the mean radiographic vertical height of the grafted sinus floor was 11.05 mm (SD: 2.10 mm), with a mean gain of 8.50 mm.
Conclusion
Within the limitations of this study, despite preoperative critical residual bone height, maxillary sinus lift restoration using a biomimetic Mg-e HA and an Mg-e HA/collagen-based scaffold with a porous 3-D structure seems to be a reliable procedure.
Keywords
Sinus lift, magnesium enriched hydroxyapatite, x-ray analysis, ISQ.
Introduction
Sinus floor augmentation has recently become a widely accepted surgical procedure to improve the amount of bone volume before implant placement. Although the use of autogenous bone appears to be the gold standard,1Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone.
→ J Oral Surg. 1980 Aug;38(8):613–6.2Cordaro L. Bilateral simultaneous augmentation of the maxillary sinus floor with particulated mandible. Report of a technique and preliminary results.
→ Clin Oral Implants Res. 2003 Apr;14(2):201–6. much attention has been paid to the use of bone substitutes. After the harvesting procedure, donor site morbidity has to be taken into consideration.33. Raghoebar GM, Meijndert L, Kalk WW, Vissink A. Morbidity of Mandibular Bone Harvesting: A Comparative Study.
→ Int J Oral Maxillofac Implants. 2007 May–Jun;22(3):359–65. Additional disadvantages for autografts are the limited availability and the tendency to resorb.4Maiorana C, Redemagni M, Rabagliati M, Salina S. Treatment of maxillary ridge resorption by sinus augmentation with iliac cancellous bone, anorganic bovine bone, and endosseous implants: a clinical and histologic report.
→ Int J Oral Maxillofac Implants. 2000 Nov–Dec;15(6):873–8. In order to overcome these limitations, several biomaterials have been evaluated in experimental and clinical studies, such as demineralized freeze-dried bone allograft,5Cammack GV, Nevins M, Clem DS, Hatch JP, Mellonig JT. Histologic evaluation of mineralized and demineralized freeze-dried bone allograft for ridge and sinus augmentations.
→ Int J Periodontics Restorative Dent. 2005 Jun;25(3):231–7. bovine bone matrix,6Maiorana C, Redemagni M, Rabagliati M, Salina S. Treatment of maxillary ridge resorption by sinus augmentation with iliac cancellous bone, anorganic bovine bone, and endosseous implants: a clinical and histologic report.
→ Int J Oral Maxillofac Implants. 2000 Nov–Dec;15(6):873–8. composite bone graft including platelet-rich plasma,7Galindo-Moreno P, Avila G, Fernández-Barbero JE, Aguilar M, Sánchez-Fernández E, Cutando A, Wang HL. Evaluation of sinus floor elevation using a composite bone graft mixture.
→ Clin Oral Implants Res. 2007 Jun;18(3):376–82. resorbable and nonresorbable hydroxyapatite8Karabuda C, Ozdemir O, Tosun T, Anil A, Olgaç V. Histological and clinical evaluation of 3 different grafting materials for sinus lifting procedure based on 8 cases.
→ J Periodontol. 2001 Oct;72(10):1436–42.9Ewers R, Goriwoda W, Schopper C, Moser D, Spassova E. Histologic findings at augmented bone areas supplied with two different bone substitute materials combined with sinus floor lifting. Report of one case.
→ Clin Oral Implants Res. 2004 Feb;15(1):96–100. and beta-tricalcium phosphate. 10Zerbo IR, Zijderveld SA, de Boer A, Bronckers AL, de Lange G, ten Bruggenkate CM, Burger EH. Histomorphometry of human sinus floor augmentation using a porous beta-tricalcium phosphate: a prospective study.
→ Clin Oral Implants Res. 2004 Dec;15(6):724–32. In particular, bioceramics based on calcium phosphate are widely used owing to their biocompatibility, absence of immunogenic factors and osteoconductivity; although, the high temperature during the sintering process could negatively influence osteoconductivity and resorption time.11Vikram D, Nather A, Kalid KA. Role of ceramics as bone graft substitutes.
→ In: Nather A, editor. Bone graft and bone substitutes. Basic science and clinical applications. Hackensack, N.J.: World Scientific; 2005. p. 445–58. New hydroxyapatites enriched with magnesium (Mg-e HAs) have recently been introduced on the market. Mg-e HA has been demonstrated to allow complete healing of the tissue around a graft and undergoes almost complete resorption already after 1 year.12Canullo L, Wiel Marin G, Tallarico M, Canciani E, Musto F, Dellavia C. Histological and histomorphometrical evaluation of postextractive sites grafted with Mg-enriched nano-hydroxyapatite: a randomized controlled trial comparing 4 versus 12 months of healing.
→ Clin Implant Dent Relat Res. 2016 Oct;18(5):973–83. Despite its high predictability, the more recent literature has highlighted possible complications after this procedure.13Al-Dajani M. Incidence, risk factors, and complications of Schneiderian membrane perforation in sinus lift surgery: a meta-analysis.
→ Implant Dent. 2016 Jun;25(3):409–15. The main complication is membrane perforation, mostly during implant insertion. Mg-e HA/collagen-based scaffolds have been successfully used for sinus augmentation procedures, demonstrating bone formation after 6 months already.14Scarano A, Lorusso F, Staiti G, Sinjari B, Tampieri A, Mortellaro C. Sinus augmentation with biomimetic nanostructured matrix: tomographic, radiological, histological and histomorphometrical results after 6 months in humans.
→ Front Physiol. 2017 Aug 3;8:565. doi: 10.3389/ fphys.2017.00565. Owing to its properties, this material might be suitable to protect the sinus membrane from eventual perforation during implant insertion.
The present preliminary prospective study was designed to evaluate clinically and radiologically implant restorations 12 months after prosthetic loading in severely resorbed maxillae requiring 1-stage sinus lift surgery. The graft used was an Mg-e HA and Mg-e HA/collagen-based scaffold with a porous 3-D structure and was used to prevent Schneiderian membrane perforation.
Materials and methods
Study design and patient selection
One dental center consecutively recruited 13 patients scheduled for implant-supported restoration in the posterior maxilla with a sinus augmentation procedure. A total of 26 wide-diameter implants with a rough surface over their entire length were inserted in extremely resorbed posterior maxillae. The present study was performed following the principles outlined in the Declaration of Helsinki of 1975, as revised in 2013, on experimentation involving human subjects. All of the patients were in general good health. They were informed about the procedure and required to sign a consent form. They were followed for a period of 12 months after prosthetic rehabilitation. The principal inclusion criterion was a residual bone crest (distance between the sinus floor and bone crest) ranging between 1 and 3 mm in height and allowing wide-diameter implant insertion. Additional inclusion and exclusion criteria are summarized below:
Subject inclusion criteria:
- Need for fixed implant-supported prosthesis in the posterior maxilla.
- Aged > 18 years. ––No relevant medical conditions.
- Nonsmoker or smoked ≤ 10 cigarettes/day (pipe or cigar smokers were excluded).
- Full-mouth plaque score and full-mouth bleeding score of ≤ 25%.
Study site inclusion criteria:
- Native bone height of 1–3 mm in the sinus zone.
Subject and site exclusion criteria:
- Acute infection of the Schneiderian membrane or chronic sinusitis.
- Allergies involving the respiratory system.
- A history of bisphosphonate therapy.
- Uncontrolled diabetes (glycated hemoglobin A1c > 6%, glycemic level > 110 mg/dL).
Preoperative and postoperative medication
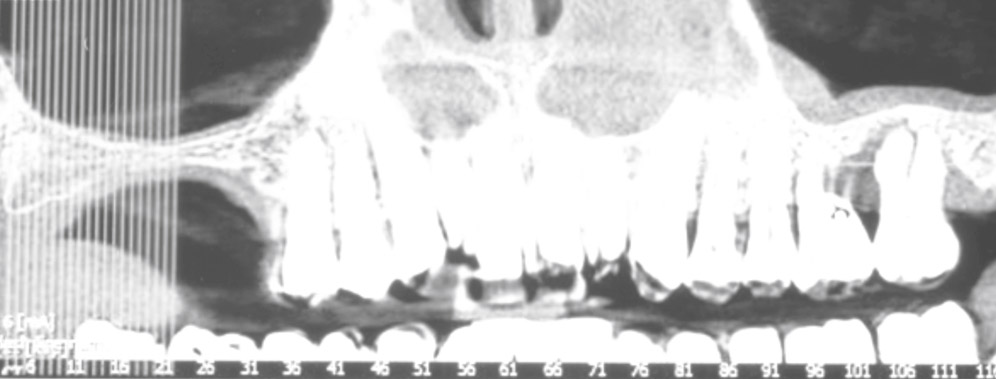
The patients underwent a preoperative digital panoramic radiograph, subsequently used as baseline. A cone beam computed tomography scan was also required to investigate antral anatomy (Fig. 1). One week before the surgical procedure, full-mouth professional prophylaxis was performed. The patients were instructed to use 1 g of penicillin clavulanate 1 day prior to surgery and continue with 2 g per day for 6 days. Just before surgery, the patients underwent a 5-min mouth rinse with 0.2% chlorhexidine gluconate.
-

- Fig. 1A
-

- Fig. 1B
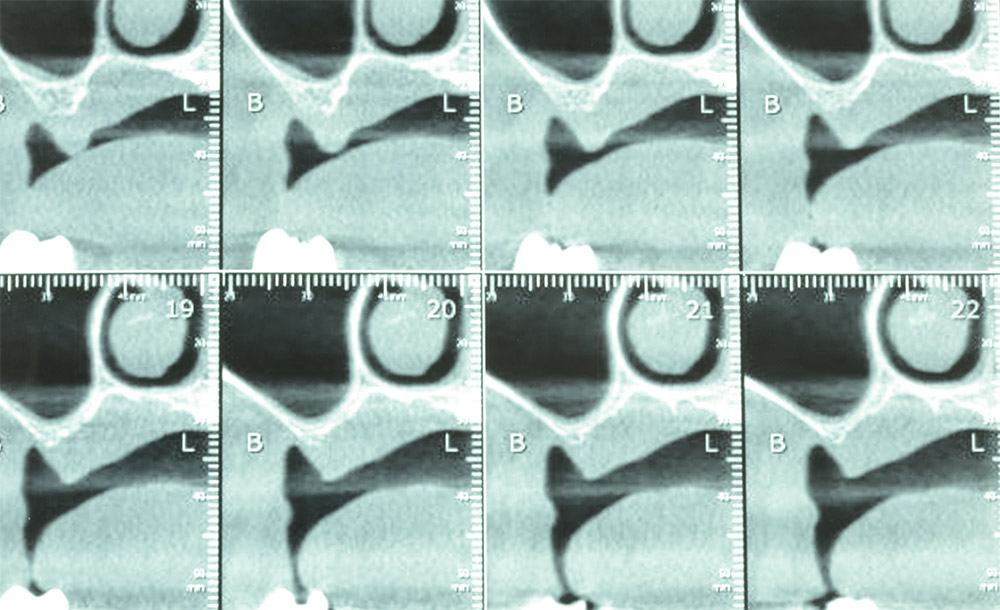
Preoperative digital panoramic radiograph with preoperative computed tomography scans.
Surgical technique
The sinus area was prepared under local anesthesia, as described by Boyne and James.15Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone.
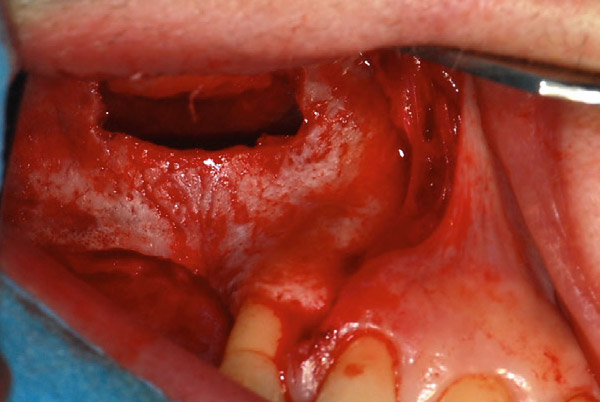
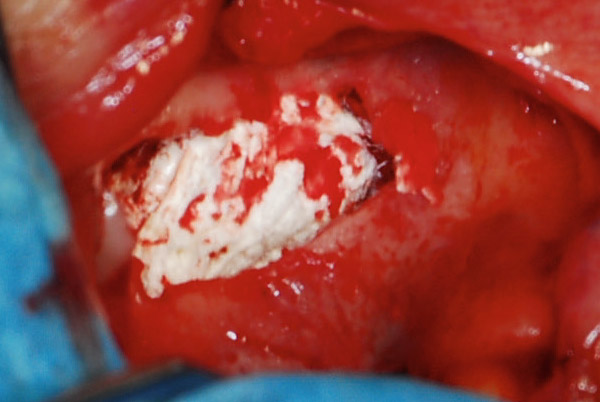
→ J Oral Surg. 1980 Aug;38(8):613–6. The bony window was left attached to the Schneiderian membrane. The sinus mucosa was elevated, taking care to avoid laceration. In all cases, an Mg-e HA/collagen-based scaffold with a porous 3-D structure (RegenOss, Finceramica, Faenza, Italy) was used to protect the Schneiderian membrane and prevent any mechanical complication during grafting and implant insertion. Implant sites were marked using a surgical template. In order to increase primary stability, osteotomies were performed using the narrowest drill able to allow implant insertion, to avoid buccal bone fracture. Residual bone height was assessed using a modified probe with a small hood. Then, the graft material (HA granules, 600–900 μ, SINTlife, Finceramica) was placed at the superior aspect of the sinus and against the medial aspect of the grafted compartment created in the sinus cavity. The graft material was meticulously condensed at each stage. Then, 2 implants (5 mm in diameter, 10–13 mm in length, Premium SP, Sweden & Martina, Due Carrare, Italy) were placed at a torque value of > 10 Ncm. The root-shaped implant used in this study had a sandblasted and acid-etched surface over its entire length. No membrane was used to cover the buccal window (Fig. 2). The oral mucosa was then sutured with 5-0 resorbable interrupted sutures (Vicryl, Ethicon, New Brunswick, N.J., U.S.).
Postoperative treatment
The patients were instructed to avoid blowing their noses for at least 7 days after surgery and to cough or sneeze with an open mouth to prevent increased pressure in the operated sinus. They underwent a new digital panoramic radiograph for postoperative evaluation. Clinical and surgical postoperative complications were measured.
-

- Fig. 2A
-

- Fig. 2B
-

- Fig. 2C
-

- Fig. 2D

-

- Fig. 2E
-

- Fig. 2F

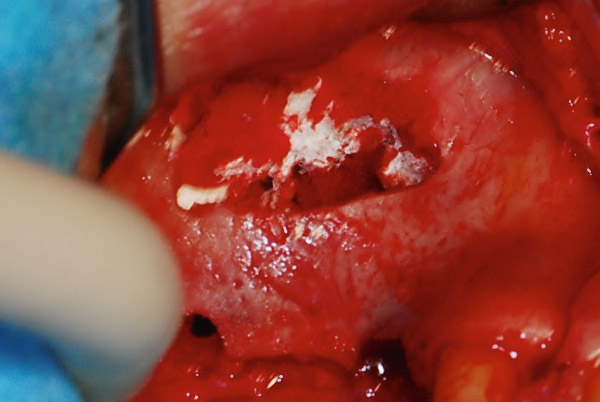
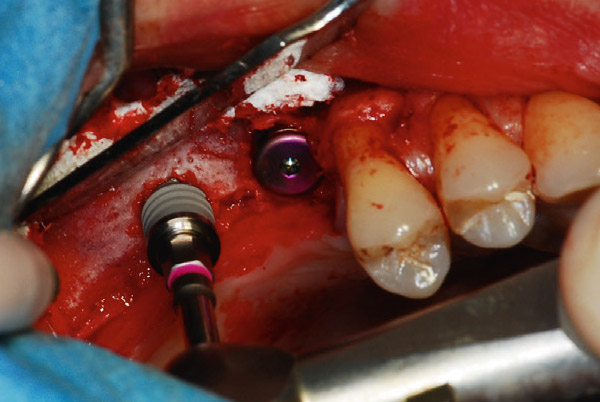
(A) Following the limits of the sinus, a bone window was outlined along the sinus edge with a round diamond bur (2,000 rpm) under copious irrigation.
(B) The sinus mucosa was elevated, taking care to avoid laceration, and RegenOss was inserted to protect the membrane during insertion of the graft material.
(C) An Mg-e HA collagenbased scaffold was elevated to allow particulate graft material to fill the sinus cavity.
(D) SINTlife graft material was compacted in the sinus cavity.
(E) Implants were inserted. Final step of the surgery: No membrane was used. Implant insertion.
(F) Final filling of the sinus cavity.
Second -stage procedure and follow-up evaluation
Second-stage surgery to expose the implants was performed 6 months after implant placement. After performing a minimal crestal incision just over the area corresponding to the implant, the cover screws were exposed and removed. Attached keratinized mucosa was left on both the palatal and buccal aspects around all of the implants, and healing abutments were screwed in at a torque of 10 Ncm. Clinical evaluation criteria at the time of implant exposure included stability in all directions, eventual crestal bone resorption, and any reported pain or discomfort. One week later, after impression taking using pickup coping transfers, titanium abutments were screwed in at a torque of 32 Ncm. In the same procedure, an additional impression of the screwed-in abutment was taken using the metallic structure. The provisional restoration was seated. In order to allow better distribution of the occlusal forces, splinted crowns were used. Implants inserted in residual neighboring bone without augmentation were not splinted to the ones inserted in augmented bone. One week later, definitive crowns were cemented using a provisional cement (Temp-Bond, Kerr, Orange, Calif., U.S.) Twelve months after prosthetic loading, a digital panoramic radiograph was obtained to assess the newly formed bone and its interface with the implant (Fig. 3).
Implant stability measurements
Immediately after implant insertion (baseline, T0), resonance frequency analysis (RFA; Osstell Mentor, Osstell, Gothenburg, Sweden) for each implant was carried out and the values were used as baseline. The transducer was handscrewed into the implant body as recommended by manufacturer. The RFA value is represented by a quantitative parameter called ISQ (Implant Stability Quotient). The ISQ ranges between 1 and 100. The measurements were repeated for each implant after 6 (T1) and 12 months after prosthetic loading (T2). Each measurement was taken twice buccolingually and the mean value was used. Because each transducer had a unique fundamental RF, the measurements were calibrated using a calibration block. All stable implants were considered successful.
Complications
Any technical (implant fracture, screw loosening, etc.) and/or biological (pain, swelling, suppuration, etc.) complications were considered.
Radiographic evaluation
The grafted area was evaluated with a computerized measuring technique applied to the digital panoramic radiographs (preoperative and 12-month follow-up). In each case, the surface of grafted sinus was marked with a virtual marking instrument. An image analysis software program (AutoCAD 2006, Version Z 54.10, Autodesk) calculated the total (native + grafted) bone height changes at the level of the implant site, comparing preoperative and follow-up panoramic radiographs, with the ability to compensate for eventual radiographic distortion.16Hatano N, Shimizu Y, Ooya K. A clinical long-term radiographic evaluation of graft height changes after maxillary sinus floor augmentation with a 2:1 autogenous bone/xenograft mixture and simultaneous placement of dental implants.
→ Clin Oral Implants Res. 2004 Jun;15(3):339–45.17Schwartz Z, Goldstein M, Raviv E, Hirsch A, Ranly DM, Boyan BD. Clinical evaluation of demineralized bone allograft in a hyaluronic acid carrier for sinus lift augmentation in humans: a computed tomography and histomorphometric study.
→ Clin Oral Implants Res. 2007 Apr;18(2):204–11. All measurements were conducted and recorded by the same trained independent examiner, without input from the implant surgeon.

Fig. 3
Digital panoramic radiograph 12 months after prosthetic loading.
Statistical analysis
Descriptive statistics, including mean values and standard deviation, were used to describe changes in implant stability over the time and bone area. Student’s t-test for paired data was performed to test the significant difference between ISQ values at T0, T1 and T2. Student’s t-test was used to perform bone area comparison. Significance was set at P > 0.05.
Results
A total of 13 consecutive patients (8 females and 5 males) were treated. The mean age was 62.1 years (SD: 11.05 years). No patient dropped out during the study. The preoperative mean residual bone level was 2.5 mm (SD: 1.0 mm). Minimal perforation of the sinus membrane occurred in 4 cases. The healing period after sinus augmentation was without complication for all of the patients. Minor nosebleeds occurred in 1 case. No clinical symptoms of maxillary sinusitis occurred in any patient. Only 1 implant was mobilized during the uncovering procedure, in a light smoker. For the failed implant, the preoperative height was 2 mm, the ISQ value was 39 at T0 and 42 at T1. The patient did not report any symptoms during the healing period. After surgical debridement, the implant was substituted with an implant 6 mm in diameter at the same surgical stage and restored after an additional 3 months of healing. All of the other implants were osseointegrated after 12 months of prosthetic loading (cumulative survival rate: 96.15%).
The mean ISQ value was 42.5 (SD: 2.7) at T0, 75.3 (SD: 8.2) at T1 and 81.5 (SD: 2.6) at T2. Statistically significant differences (P ≤ 0.0005) regarding mean ISQ values were found between T1 and T0, as well as between T1 and T2. The mean radiographic vertical height of the grafted sinus floor was 13.75 mm (SD: 1.30 mm) after 12 months of prosthetic loading (P ≤ 0.0005).
Discussion
This prospective study demonstrated that, even in critical conditions, osseointegration and longitudinal stability of implants with a rough surface over their entire length could be a reliable clinical outcome when placed in maxillary sinuses grafted with a biomimetic Mg-e HA. Additionally, the use of an Mg-e HA/collagen-based scaffold with a porous 3-D structure seems to prevent surgical complications due to microperforation of the Schneiderian membrane.
The main limitations of the present study were the short-term follow-up (1 year) and small sample size (13 patients). However, this study is a preliminary report proving the feasibility of the combination of an Mg-e HA/collagen-based scaffold with a biomimetic HA. Additionally, the absence of a control group does not allow for demonstration of any additional benefit compared with the gold standard in sinus lift surgery.
The graft material investigated in this study was a new generation of HA, biomimetic scaffolds, and was studied as an alternative to overcome the disadvantages of conventional graft material, simulating bone structure not only from a chemical point of view, but also microscopically, reproducing micropores and their interconnections. Within this graft material category, Mg-e HAs have chemical and morphological properties close to that of natural bone and have showed comparable results to autologous bone in regenerative procedures. This configuration seems to be able to induce migration, adhesion and proliferation of osteoblasts inside the pore network and to promote angiogenesis inside.18Canullo L, Wiel Marin G, Tallarico M, Canciani E, Musto F, Dellavia C. Histological and histomorphometrical evaluation of postextractive sites grafted with Mg-enriched nano-hydroxyapatite: a randomized controlled trial comparing 4 versus 12 months of healing.
→ Clin Implant Dent Relat Res. 2016 Oct;18(5):973–83.
A recent literature review showed the residual bone crestal height to be one of the most critical factor influencing implant survival rate. At the same time, a minimum bone height of 4–5 mm is recommended for a 1-stage implant insertion.19Del Fabbro M, Testori T, Francetti L, Weinstein R. Systematic review of survival rates for implants placed in the grafted maxillary sinus.
→ Int J Periodontics Restorative Dent. 2004 Dec;24(6):565–77. However, according to Peleg et al., despite severely resorbed maxillae, a 1-stage surgical technique was adopted in the present study.20Peleg M, Garg AK, Mazor Z. Predictability of simultaneous implant placement in the severely atrophic posterior maxilla: a 9-year longitudinal experience study of 2132 implants placed into 731 human sinus grafts.
→ Int J Oral Maxillofac Implants. 2006 Jan–Feb;21(1):94–102.
This approach finally reported only 1 implant failure, according to the results obtained by Fugazzotto and Vlassis21Fugazzotto PA, Vlassis J. Report of 1633 implants in 814 augmented sinus areas in function for up to 180 months.
→ Implant Dent. 2007 Dec;16(4):369–78. in their retrospective report and according to Wallace and Froum22Wallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review.
→ Ann Periodontol. 2003 Dec;8(1):328–43. and Del Fabbro et al.23Del Fabbro M, Testori T, Francetti L, Weinstein R. Systematic review of survival rates for implants placed in the grafted maxillary sinus.
→ Int J Periodontics Restorative Dent. 2004 Dec;24(6):565–77. in their reviews. Furthermore, in their systematic review, Wallace and Froum indicated membrane placement over the lateral window to be an important factor to improve the quality of regenerated bone.24Wallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review.
→ Ann Periodontol. 2003 Dec;8(1):328–43. An absorbable collagen membrane placed on the buccal sinus wall, in fact, seemed to protect the graft from soft-tissue invasion, which would reduce the amount and the quality of the de novo-formed mineralized tissue.25Tawil G, Mawla M. Sinus floor elevation using a bovine bone mineral (Bio-Oss) with or without the concomitant use of a bilayered collagen barrier (Bio-Gide): a clinical report of immediate and delayed implant placement.
→ Int J Oral Maxillofac Implants. 2001 Sep–Oct;16(5):713–21.26Carmagnola D, Adriaens P, Berglundh T. Healing of human extraction sockets filled with Bio-Oss.
→ Clin Oral Implants Res. 2003 Apr;14(2):137–43. This finding was also confirmed by a published systematic review.27Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):216–40. In this study, Pjetursson et al. showed an annual implant failure rate significantly higher (4.0% vs. 0.7%) when no membrane was used to cover the lateral window after the grafting procedure.28Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation.
→ J Clin Periodontol. 2008 Sep;35(8 Suppl):216–40.
Results from the present study showed that a membrane may not be a critical factor for the implant survival rate. An additional result to be noted is the absence of any postsurgical complication in the case of microperforation of the membrane. In fact, sinus membrane perforation is a typical surgical complication. This event could occur during membrane elevation before graft insertion or after graft insertion at the time of implant positioning. According to the literature, the second possibility is often clinically unknown, and it is probably due to membrane compression from the graft shifting subsequent to the implant insertion.29Al-Dajani M. Incidence, risk factors, and complications of Schneiderian membrane perforation in sinus lift surgery: a meta-analysis.
→ Implant Dent. 2016 Jun;25(3):409–15.
In order to prevent this complication, an Mg-e HA/collagen-based scaffold with a porous 3-D matrix was placed between the sinus membrane and the graft. The clinically relevant peculiarity of this scaffold is its appearance, which is similar to that of a collagen membrane, and therefore its similar elasticity. The scaffold was advantageous, preventing perforation of the sinus mucosa by the graft material particles. At the same time, the scaffold acted as not only a membrane but, as demonstrated by the literature,30Scarano A, Lorusso F, Staiti G, Sinjari B, Tampieri A, Mortellaro C. Sinus augmentation with biomimetic nanostructured matrix: tomographic, radiological, histological and histomorphometrical results after 6 months in humans.
→ Front Physiol. 2017 Aug 3;8:565. doi: 10.3389/ fphys.2017.00565. also a graft material itself. From a surgical point of view, despite very resorbed maxillae, no postoperative problems or complications were observed when implants were inserted simultaneously with the graft material. Although the literature describes problems during the surgical phase in sinus augmentation in patients with 1–4 mm residual bone height,31Mardinger O, Nissan J, Chaushu G. Sinus floor augmentation with simultaneous implant placement in the severely atrophic maxilla: technical problems and complications.
→ J Periodontol. 2007 Oct;78(10):1872–7. the use of wide-diameter implants allows a sufficient primary stability.32Turkyilmaz I, Aksoy U, McGlumphy EA. Two alternative surgical techniques for enhancing primary implant stability in the posterior maxilla: a clinical study including bone density, insertion torque, and resonance frequency analysis data.
→ Clin Implant Dent Relat Res. 2008 Dec;10(4):231–7.
Although the mean value of ISQ at T0 was very low, the data reported at T1 are in line with that of previously reported findings. In fact, Lai et al. reported the same findings for rough-surfaced implants installed after minor sinus floor elevation.33Lai H, Zhang ZY, Wang F, Zhuang LF, Liu X. Resonance frequency analysis of stability on ITI implants with osteotome sinus floor elevation technique without grafting: a 5-month prospective study.
→ Clin Oral Implants Res. 2008 May;19(5):469–75.
The statistically significant increase of ISQ values between T0 and T1 could be evidence of fast maturation of the graft, after just 3 months. An additional increase between T1 and T2 could indicate a further maturation of the material after 12 months of prosthetic loading. Despite some clinical studies suggesting positive results with the use of RegenOss alone in sinus lift procedures after 6 months,34Al-Dajani M. Incidence, risk factors, and complications of Schneiderian membrane perforation in sinus lift surgery: a meta-analysis.
→ Implant Dent. 2016 Jun;25(3):409–15. controversial outcomes with the use of a soft matrix were reached in the literature.35Caneva M, Lang NP, Garcia Rangel IJ, Ferreira S, Caneva M, De Santis E, Botticelli D. Sinus mucosa elevation using Bio-Oss® or Gingistat® collagen sponge: an experimental study in rabbits.
→ Clin Oral Implants Res. 2017 Jul;28(7):e21–30. doi: 10.1111/ clr.12850. In fact, Caneva et al. suggested the use of rigid materials to counteract negative pressure during respiration.36Caneva M, Lang NP, Garcia Rangel IJ, Ferreira S, Caneva M, De Santis E, Botticelli D. Sinus mucosa elevation using Bio-Oss® or Gingistat® collagen sponge: an experimental study in rabbits.
→ Clin Oral Implants Res. 2017 Jul;28(7):e21–30. doi: 10.1111/ clr.12850.
Conclusion
The present study, within its limitations, demonstrated that the use of a soft matrix in association with a graft material allows bone regeneration without postoperative complications. However, further studies should aim to measure discrepancies between preoperative and longterm postoperative increments using the promising matrix used in the present study.
Interview
with Luigi Canullo
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 15. | ↑ | Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. → J Oral Surg. 1980 Aug;38(8):613–6. |
| 2. | ↑ | Cordaro L. Bilateral simultaneous augmentation of the maxillary sinus floor with particulated mandible. Report of a technique and preliminary results. → Clin Oral Implants Res. 2003 Apr;14(2):201–6. |
| 3. | ↑ | 3. Raghoebar GM, Meijndert L, Kalk WW, Vissink A. Morbidity of Mandibular Bone Harvesting: A Comparative Study. → Int J Oral Maxillofac Implants. 2007 May–Jun;22(3):359–65. |
| 4, 6. | ↑ | Maiorana C, Redemagni M, Rabagliati M, Salina S. Treatment of maxillary ridge resorption by sinus augmentation with iliac cancellous bone, anorganic bovine bone, and endosseous implants: a clinical and histologic report. → Int J Oral Maxillofac Implants. 2000 Nov–Dec;15(6):873–8. |
| 5. | ↑ | Cammack GV, Nevins M, Clem DS, Hatch JP, Mellonig JT. Histologic evaluation of mineralized and demineralized freeze-dried bone allograft for ridge and sinus augmentations. → Int J Periodontics Restorative Dent. 2005 Jun;25(3):231–7. |
| 7. | ↑ | Galindo-Moreno P, Avila G, Fernández-Barbero JE, Aguilar M, Sánchez-Fernández E, Cutando A, Wang HL. Evaluation of sinus floor elevation using a composite bone graft mixture. → Clin Oral Implants Res. 2007 Jun;18(3):376–82. |
| 8. | ↑ | Karabuda C, Ozdemir O, Tosun T, Anil A, Olgaç V. Histological and clinical evaluation of 3 different grafting materials for sinus lifting procedure based on 8 cases. → J Periodontol. 2001 Oct;72(10):1436–42. |
| 9. | ↑ | Ewers R, Goriwoda W, Schopper C, Moser D, Spassova E. Histologic findings at augmented bone areas supplied with two different bone substitute materials combined with sinus floor lifting. Report of one case. → Clin Oral Implants Res. 2004 Feb;15(1):96–100. |
| 10. | ↑ | Zerbo IR, Zijderveld SA, de Boer A, Bronckers AL, de Lange G, ten Bruggenkate CM, Burger EH. Histomorphometry of human sinus floor augmentation using a porous beta-tricalcium phosphate: a prospective study. → Clin Oral Implants Res. 2004 Dec;15(6):724–32. |
| 11. | ↑ | Vikram D, Nather A, Kalid KA. Role of ceramics as bone graft substitutes. → In: Nather A, editor. Bone graft and bone substitutes. Basic science and clinical applications. Hackensack, N.J.: World Scientific; 2005. p. 445–58. |
| 12, 18. | ↑ | Canullo L, Wiel Marin G, Tallarico M, Canciani E, Musto F, Dellavia C. Histological and histomorphometrical evaluation of postextractive sites grafted with Mg-enriched nano-hydroxyapatite: a randomized controlled trial comparing 4 versus 12 months of healing. → Clin Implant Dent Relat Res. 2016 Oct;18(5):973–83. |
| 13, 29, 34. | ↑ | Al-Dajani M. Incidence, risk factors, and complications of Schneiderian membrane perforation in sinus lift surgery: a meta-analysis. → Implant Dent. 2016 Jun;25(3):409–15. |
| 14, 30. | ↑ | Scarano A, Lorusso F, Staiti G, Sinjari B, Tampieri A, Mortellaro C. Sinus augmentation with biomimetic nanostructured matrix: tomographic, radiological, histological and histomorphometrical results after 6 months in humans. → Front Physiol. 2017 Aug 3;8:565. doi: 10.3389/ fphys.2017.00565. |
| 16. | ↑ | Hatano N, Shimizu Y, Ooya K. A clinical long-term radiographic evaluation of graft height changes after maxillary sinus floor augmentation with a 2:1 autogenous bone/xenograft mixture and simultaneous placement of dental implants. → Clin Oral Implants Res. 2004 Jun;15(3):339–45. |
| 17. | ↑ | Schwartz Z, Goldstein M, Raviv E, Hirsch A, Ranly DM, Boyan BD. Clinical evaluation of demineralized bone allograft in a hyaluronic acid carrier for sinus lift augmentation in humans: a computed tomography and histomorphometric study. → Clin Oral Implants Res. 2007 Apr;18(2):204–11. |
| 19, 23. | ↑ | Del Fabbro M, Testori T, Francetti L, Weinstein R. Systematic review of survival rates for implants placed in the grafted maxillary sinus. → Int J Periodontics Restorative Dent. 2004 Dec;24(6):565–77. |
| 20. | ↑ | Peleg M, Garg AK, Mazor Z. Predictability of simultaneous implant placement in the severely atrophic posterior maxilla: a 9-year longitudinal experience study of 2132 implants placed into 731 human sinus grafts. → Int J Oral Maxillofac Implants. 2006 Jan–Feb;21(1):94–102. |
| 21. | ↑ | Fugazzotto PA, Vlassis J. Report of 1633 implants in 814 augmented sinus areas in function for up to 180 months. → Implant Dent. 2007 Dec;16(4):369–78. |
| 22, 24. | ↑ | Wallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. → Ann Periodontol. 2003 Dec;8(1):328–43. |
| 25. | ↑ | Tawil G, Mawla M. Sinus floor elevation using a bovine bone mineral (Bio-Oss) with or without the concomitant use of a bilayered collagen barrier (Bio-Gide): a clinical report of immediate and delayed implant placement. → Int J Oral Maxillofac Implants. 2001 Sep–Oct;16(5):713–21. |
| 26. | ↑ | Carmagnola D, Adriaens P, Berglundh T. Healing of human extraction sockets filled with Bio-Oss. → Clin Oral Implants Res. 2003 Apr;14(2):137–43. |
| 27, 28. | ↑ | Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. → J Clin Periodontol. 2008 Sep;35(8 Suppl):216–40. |
| 31. | ↑ | Mardinger O, Nissan J, Chaushu G. Sinus floor augmentation with simultaneous implant placement in the severely atrophic maxilla: technical problems and complications. → J Periodontol. 2007 Oct;78(10):1872–7. |
| 32. | ↑ | Turkyilmaz I, Aksoy U, McGlumphy EA. Two alternative surgical techniques for enhancing primary implant stability in the posterior maxilla: a clinical study including bone density, insertion torque, and resonance frequency analysis data. → Clin Implant Dent Relat Res. 2008 Dec;10(4):231–7. |
| 33. | ↑ | Lai H, Zhang ZY, Wang F, Zhuang LF, Liu X. Resonance frequency analysis of stability on ITI implants with osteotome sinus floor elevation technique without grafting: a 5-month prospective study. → Clin Oral Implants Res. 2008 May;19(5):469–75. |
| 35, 36. | ↑ | Caneva M, Lang NP, Garcia Rangel IJ, Ferreira S, Caneva M, De Santis E, Botticelli D. Sinus mucosa elevation using Bio-Oss® or Gingistat® collagen sponge: an experimental study in rabbits. → Clin Oral Implants Res. 2017 Jul;28(7):e21–30. doi: 10.1111/ clr.12850. |





Leave a Reply
Be the First to Comment!