Subcutaneous emphysema after a direct sinus lift: A case report
June 14, 2019 / Categories: Digital Dentistry, Implant Dentistry

Martorell Calatayud, Luis

Zaragozí Alonso, Regino

Peñarrocha Diago, Miguel

Sevilla Heras, María
Abstract
Objective
Subcutaneous oral emphysema is defined as penetration of pressurized air into the tissue spaces. One possible means of air entry is through the bone window made during a direct sinus lift. There are only 3 cases published in the literature of subcutaneous emphysema with this etiology. It is important that the dentist carefully instruct the patient about the post-surgical protocol that must be carried out to reduce the risk of this complication.
Materials and methods
A 52-year-old patient underwent a maxillary direct sinus lift for the future placement of implants in the posterior area. A few hours after the surgery, the patient repeatedly sneezed with his mouth closed 3 times, immediately causing a large swelling in the left periorbital area that prevented him from opening the eye. After clinical and radiographic examination, it was determined that it was a subcutaneous emphysema. The prescribed treatment was antibiotics.
Conclusion
Subcutaneous emphysema is a benign and usually self-limited entity, which usually resolves spontaneously. Most authors agree on the use of turbines as the most frequent etiology. Other reasons, however, have also been reported in the literature, such as endodontic treatment and the use of dental lasers. The main clinical manifestations that aided us in establishing a correct differential diagnosis were swelling without redness, edema and crepitating palpation of the soft tissue. In general, patients do not report pain, but at worst a slight discomfort due to swelling.
Keywords
Subcutaneous emphysema; periorbital edema; orbital emphysema; complications; sinus floor elevation.
Introduction
Subcutaneous emphysema is defined as the penetration of air pressure into tissue spaces.1Heyman SN, Babayof I. Emphysematous complications in dentistry, 1960–1993: an illustrative case and review of the literature. Quintessence Int. 1995 Aug;26(8):535–43.,2Jawaid MS. Orbital emphysema: nose blowing leading to a blown orbit. → BMJ Case Rep. 2015 Oct 29;2015. pii: bcr2015212554. doi:10.1136/bcr- 2015-212554.,3Fleischman D, Davis RM, Lee LB. Subcutaneous and periorbital emphysema following dental procedure. → Ophthalmic Plast Reconstr Surg. 2014 Mar–Apr;30(2):e43–5. doi: 10.1097/IOP.0b013e 318295f982.,4Romeo U, Galanakis A, Lerario F, Daniele GM, Tenore G, Palaia G. Subcutaneous emphysema during third molar surgery: a case report. → Braz Dent J. 2011;22(1):83–6.,5McKenzie WS, Rosenberg M. Iatrogenic subcutaneous emphysema of dental and surgical origin: a literature review. → J Oral Maxillofac Surg. 2009 Jun;67(6):1265–8.,6Tomasetti P, Kuttenberger J, Bassetti R. Distinct subcutaneous emphysema following surgical wisdom tooth extraction in a patient suffering from “Gilles de la Tourette syndrome”. → J Surg Case Rep. 2015 Jun 14;2015(6). pii: rjv068. doi: 10.1093/jscr/ rjv068.,7Mitsunaga S, Iwai T, Kitajima H, Yajima Y, Ohya T, Hirota M, Mitsudo K, Aoki N, Yamashita Y, Omura S, Tohnai I. Cervicofacial subcutaneous emphysema associated with dental laser treatment. → Aust Dent J. 2013 Dec;58(4):424–7,8Parkar A, Medhurst C, Irbash M, Philpott C. Periorbital oedema and surgical emphysema, an unusual complication of a dental procedure: a case report. → Cases J. 2009 Sep 1;2:8108. doi: 10.4076/1757-1626-2-8108. It is a complication that has been described in the literature for many years. In 1995, Heyman and Babayof reviewed the literature from 1960 to 1993 on emphysematous complications in dental treatment.9Heyman SN, Babayof I. Emphysematous complications in dentistry, 1960–1993: an illustrative case and review of the literature. Quintessence Int. 1995 Aug;26(8):535–43.

Fig 1.
Subcutaneous emphysema does not occur regularly, but it is important to control to avoid complications such as infections that can be harmful to the patient.10Sahoo NK, Singh S, Roy ID, Bhandari A. Early postoperative malignant subcutaneous emphysema: report and review. → J Maxillofac Oral Surg. 2017 Mar;16(1):85–9. The condition is usually the result of treatment with high-speed surgical drills and compressed air syringes during restorative and endodontic procedures.11McKenzie WS, Rosenberg M. Iatrogenic subcutaneous emphysema of dental and surgical origin: a literature review. → J Oral Maxillofac Surg. 2009 Jun;67(6):1265–8. However, in the present case, periorbital edema was observed after several hours of a sinus floor elevation, which makes this case report interesting. There are not many cases reported in the literature about this etiology, which is mostly related to post-surgical maneuvers of the patient (sneezing while keeping the mouth closed, blowing the nose, playing wind instruments).12Farina R, Zaetta A, Minenna L, Trombelli L. Orbital and periorbital emphysema following maxillary sinus floor elevation: a case report and literature review. → J Oral Maxillofac Surg. 2016 Nov;74(11):2192.e1–2192.e7. doi: 10.1016/j. joms.2016.06.186. Epub 2016 Jul 1. The objective of this clinical case is to demonstrate to oral and maxillofacial surgeons the possibility of orbital and periorbital emphysema after an intervention in the maxillary sinus, as well as the procedure to follow in the case of this complication.
Study design and ethical aspects
The present study is a case report. The patient was willing and fully capable of complying with the clinical procedures, and a written informed consent was obtained 7 days before the initiation of treatment.
Case report
The patient was 52 years old and a nonsmoker. He attended the periodontics department (University of Valencia, Valencia, Spain) for checks and controls periodically. The Department of Oral Surgery and Implantology, University of Valencia, Valencia, Spain, requested restoration of his missing teeth with implants.
The third and second molars had been extracted about 20 months before the observation. The patient was willing to have the right maxillary posterior area rehabilitated with a fixed prosthesis (Figs. 1 & 2).
The oral rehabilitation plan called for the placement of an implant 10 mm long and 4 mm wide distal to the maxillary second left premolar. In the right maxilla, an atraumatic sinus lift was sufficient.
The residual height of the bone in the left maxilla was less than 5 mm, which was evaluated by cone beam computed tomography. As there was not enough bone height to place an implant in a standard way, it was decided to proceed with a traumatic sinus lift. The patient did not present any contraindication to or systemic disease that would contraindicate the procedure.
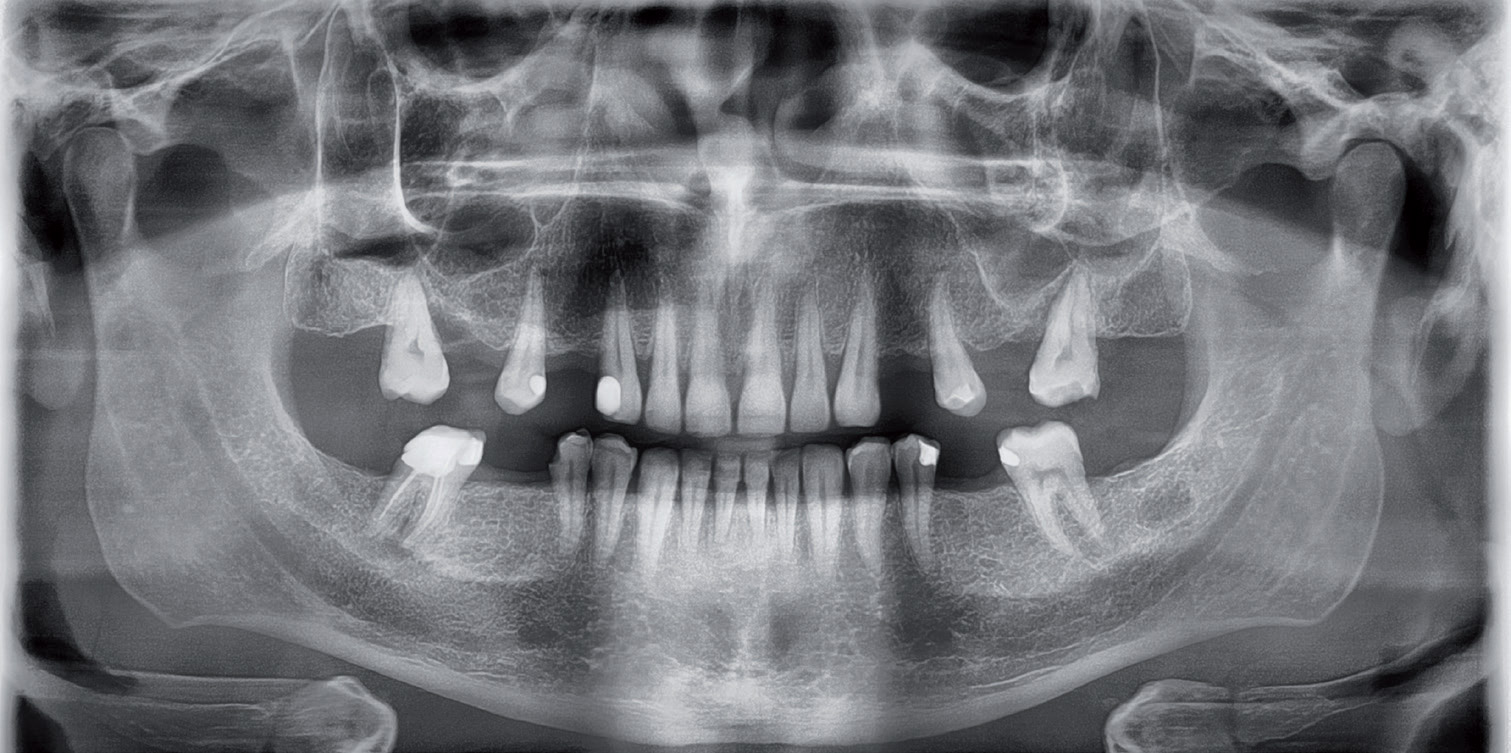
Fig 2.
Surgical procedure
For the intervention of vertical increase of bone in the maxillary sinus, antibiotic pre-medication was prescribed: amoxicillin (500 mg, 1 tablet every 8 h for 7 days), starting 2 days before. It was also recommended to take ibuprofen (600 mg, 1 tablet) 1 h before surgery. Local anesthesia was administered by infiltration with articaine plus 1:100,000 epinephrine (Ultracain, 40 mg; Normon; 3 cartridges of 1.8 mL per cartridge).
A crestal incision was made in the edentulous area, followed by a vertical incision, mesial to the second premolar, surpassing the mucogingival line. A mucoperiosteal flap was raised to full thickness to visualize the lateral wall of the maxillary sinus. The extraction of the first molar was performed prior to access to the maxillary sinus.
The access to the maxillary sinus was performed using the lateral access technique. The window had dimensions of 10 × 8 mm, made first with a handpiece and tungsten carbide drill and then with a piezoelectric instrument (Piezomed, W&H). Then, to elevate the sinus membrane, angulated manual instruments were used in direct contact with the bone (sinus membrane separators 718-EN2, MC-1 and MC-2, Bontempi).
The Valsalva maneuver to check whether the membrane had suffered any perforation was positive. We thus placed a small piece of membrane that covered it completely. Then we filled the whole sinus cavity with a bovine-derived xenograft (Bio-Oss, 0.25–1.00 mm granules; Geistlich Biomaterials). The total amount of xenograft used was 2.5 g. The lateral window was covered with a 13–25 mm resorbable collagen membrane (Bio-Gide, Geistlich Biomaterials). Seven simple sutures were performed with Supramid (5/0, circ., nonresorbable; Steinerberg), starting at the angles and continuing through the crestal and middle incisions. A periapical radiograph (Fig. 3) and a dental panoramic tomogram (Fig. 4) were taken at the end of the intervention.
The patient was provided with post-surgical instructions, both verbal and written. The recommendations included soft and cold food for the first several days, cold application in the surgical area, no smoking and avoiding brushing for the first several days, and use of a 0.12% chlorhexidine rinse (Perio•Aid, 0.2% chlorhexidine and 0.05% cetylpyridinium chloride; Dentaid) for 1 min, 3 times a day for 10 days. The patient was told that he could make use of anti-inflammatory therapy for pain or swelling.
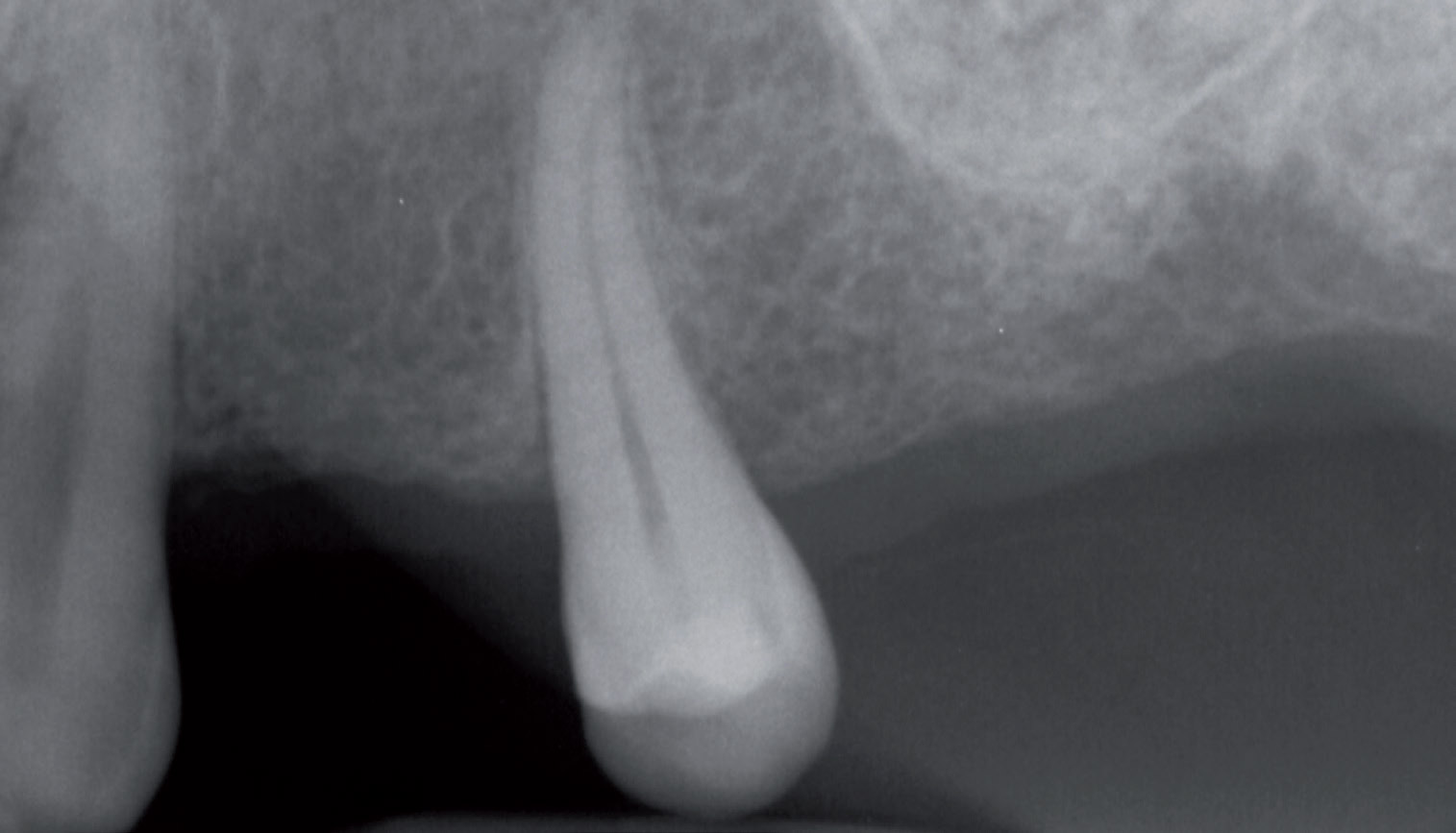
Fig 3.
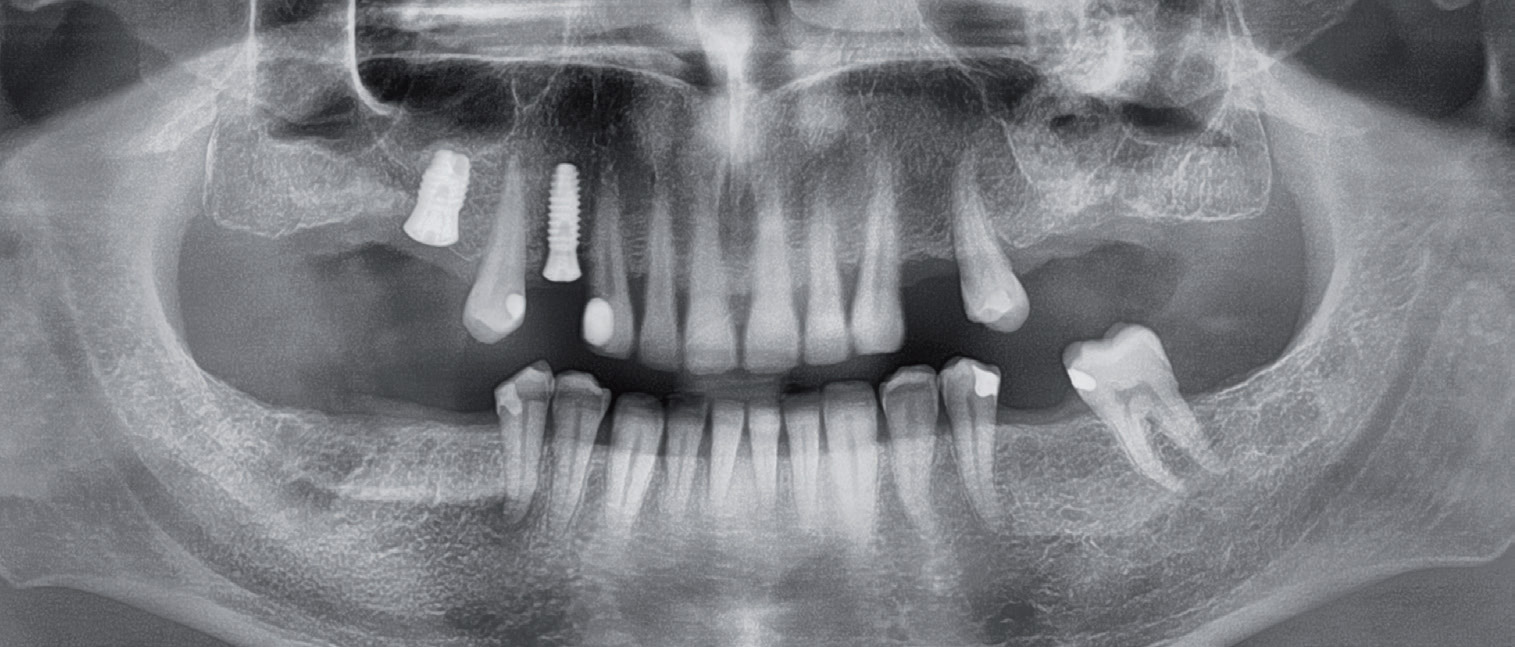
Fig 4.
Clinical management and resolution of orbital and periorbital emphysema
Onset and clinical aspect
On the same day of the surgery, 3 h later, the patient reported a large area of inflammation on the left side of the face that appeared immediately after 3 continuous sneezes (Fig. 5). The patient underwent a clinical examination of the affected area. He had no pain and his sight was unaltered, although the inflammation limited the opening of the eyelid. The extrinsic musculature of the eye was not involved. A visit to an ophthalmological specialist was not considered necessary. A control dental panoramic tomogram was performed and it did not reveal any alteration in the bone elevation. The diagnosis of subcutaneous emphysema was explained to the patient. Amoxicillin, 875 mg, and clavulanic acid, 125 mg, 1 tablet every 8 h for 7 days, was prescribed.
Resolution
By the third day, the reduction of emphysema was already very noticeable, and the inflammation had decreased, disappearing completely after 7 days. The resolution of emphysema occurred without any other complication. The patient did not have an infection or pain.

Fig 5.
Discussion
In the present clinical case, subcutaneous emphysema appeared after powerful sneezing of the patient after elevation of the maxillary sinus. The objective of the report of this case is to communicate the signs and symptoms of subcutaneous emphysema at the level of the periorbital area, as well as the favorable progress in a few days with good pharmacological management.
Many authors have recorded the complication of subcutaneous emphysema, especially after dental interventions. Most of them agree that the use of air-operated handpieces for dental extractions is the most frequent cause.134. ,14Tomasetti P, Kuttenberger J, Bassetti R. Distinct subcutaneous emphysema following surgical wisdom tooth extraction in a patient suffering from “Gilles de la Tourette syndrome”. → J Surg Case Rep. 2015 Jun 14;2015(6). pii: rjv068. doi: 10.1093/jscr/ rjv068.,15Arai I, Aoki T, Yamazaki H, Ota Y, Kaneko A. Pneumomediastinum and subcutaneous emphysema after dental extraction detected incidentally by regular medical checkup: a case report. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Apr;107(4):e33–8. doi: 10.1016/j. tripleo.2008.12.019.,16Tan S, Nikolarakos D. Subcutaneous emphysema secondary to dental extraction: a case report. → Aust Dent J. 2017 Mar;62(1):95–7. However, other reasons have also been described: preparation for and placement of crowns,17Khandelwal V, Agrawal P, Agrawal D, Nayak PA. Subcutaneous emphysema of periorbital region after stainless steel crown preparation in a young child. → BMJ Case Rep. 2013 May 22;2013. pii: bcr2013009952. doi: 10.1136/ bcr-2013-009952. endodontic treatment and retreatment, and the use of the dental laser.18Mitsunaga S, Iwai T, Kitajima H, Yajima Y, Ohya T, Hirota M, Mitsudo K, Aoki N, Yamashita Y, Omura S, Tohnai I. Cervicofacial subcutaneous emphysema associated with dental laser treatment. → Aust Dent J. 2013 Dec;58(4):424–7,19Al-Qudah A, Amin F, Hassona Y. Periorbital emphysema during endodontic retreatment of an upper central incisor: a case report. → Br Dent J. 2013 Nov 8;215(9):459–61.,20Imai T, Michizawa M, Arimoto E, Kimoto M, Yura Y. Cervicofacial subcutaneous emphysema and pneumomediastinum after intraoral laser irradiation. → J Oral Maxillofac Surg. 2009 Feb;67(2):428–30.
It is important to make a differential diagnosis through comparison with other pathologies that produce an increase in volume, such as an allergic reaction or a hematoma. Therefore, a detailed clinical history and the correct palpation of the area to achieve a correct diagnosis is very important. The main manifestations that aided us in establishing a correct differential diagnosis were swelling without redness and the crepitating palpation of the soft tissue.21Tan S, Nikolarakos D. Subcutaneous emphysema secondary to dental extraction: a case report. → Aust Dent J. 2017 Mar;62(1):95–7. Few authors have reported cases related to the eye and orbital tissue.22Farina R, Zaetta A, Minenna L, Trombelli L. Orbital and periorbital emphysema following maxillary sinus floor elevation: a case report and literature review. → J Oral Maxillofac Surg. 2016 Nov;74(11):2192.e1–2192.e7. doi: 10.1016/j. joms.2016.06.186. Epub 2016 Jul 1.,23Arai I, Aoki T, Yamazaki H, Ota Y, Kaneko A. Pneumomediastinum and subcutaneous emphysema after dental extraction detected incidentally by regular medical checkup: a case report. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Apr;107(4):e33–8. doi: 10.1016/j. tripleo.2008.12.019.,24Tan S, Nikolarakos D. Subcutaneous emphysema secondary to dental extraction: a case report. → Aust Dent J. 2017 Mar;62(1):95–7.,25Khandelwal V, Agrawal P, Agrawal D, Nayak PA. Subcutaneous emphysema of periorbital region after stainless steel crown preparation in a young child. → BMJ Case Rep. 2013 May 22;2013. pii: bcr2013009952. doi: 10.1136/ bcr-2013-009952.,26Al-Qudah A, Amin F, Hassona Y. Periorbital emphysema during endodontic retreatment of an upper central incisor: a case report. → Br Dent J. 2013 Nov 8;215(9):459–61.,27Imai T, Michizawa M, Arimoto E, Kimoto M, Yura Y. Cervicofacial subcutaneous emphysema and pneumomediastinum after intraoral laser irradiation. → J Oral Maxillofac Surg. 2009 Feb;67(2):428–30.,28Stacchi C, Sentineri R, Berton F, Lombardi T. Conjunctival chemosis: an uncommon complication after transcrestal lifting of the sinus floor. → Br J Oral Maxillofac Surg. 2016 Nov;54(9):1052–4. Commonly, patients report no pain, but at worst a slight discomfort due to inflammation.
Air can enter the parapharyngeal and retropharyngeal spaces, where accumulation of air can lead to airway compromise, air embolism and soft-tissue infection. Pneumothorax, optic nerve damage and even death by air embolism has been reported.29Heyman SN, Babayof I. Emphysematous complications in dentistry, 1960–1993: an illustrative case and review of the literature. Quintessence Int. 1995 Aug;26(8):535–43.
Prophylactic antibiotics, meticulous observation of the respiratory tract and monitoring of gas extension are recommended.30Heyman SN, Babayof I. Emphysematous complications in dentistry, 1960–1993: an illustrative case and review of the literature. Quintessence Int. 1995 Aug;26(8):535–43.,31Kung JC, Chuang FH, Hsu KJ, Shih YL, Chen CM, Huang IY. Extensive subcutaneous emphysema after extraction of a mandibular third molar: a case report. → Kaohsiung J Med Sci. 2009 Oct;25(10):562–6. To prevent secondary infections, the administration of antibiotics is recommended. In this case, amoxicillin and clavulanic acid as prescribed was sufficient for resolution of the case.
Conclusion
The present case report has shown how subcutaneous emphysema can occur as a result of the sneezing of the patient after maxillary sinus augmentation. It was handled correctly with the use of antibiotics and follow- up. Subcutaneous emphysema did not affect the success of the vertical augmentation procedure.
Competing interests
The authors declare that they have no competing interests.
Legends
Fig. 1 – Preoperative periapical radiograph.
Fig. 2 – Preoperative dental panoramic tomogram.
Fig. 3 – Postoperative periapical radiograph.
Fig. 4 – Postoperative dental panoramic tomogram.
Fig. 5 – Clinical image of subcutaneous emphysema.
References
| 1, 9, 29, 30. | ↑ | Heyman SN, Babayof I. Emphysematous complications in dentistry, 1960–1993: an illustrative case and review of the literature. Quintessence Int. 1995 Aug;26(8):535–43. |
| 2. | ↑ | Jawaid MS. Orbital emphysema: nose blowing leading to a blown orbit. → BMJ Case Rep. 2015 Oct 29;2015. pii: bcr2015212554. doi:10.1136/bcr- 2015-212554. |
| 3. | ↑ | Fleischman D, Davis RM, Lee LB. Subcutaneous and periorbital emphysema following dental procedure. → Ophthalmic Plast Reconstr Surg. 2014 Mar–Apr;30(2):e43–5. doi: 10.1097/IOP.0b013e 318295f982. |
| 4. | ↑ | Romeo U, Galanakis A, Lerario F, Daniele GM, Tenore G, Palaia G. Subcutaneous emphysema during third molar surgery: a case report. → Braz Dent J. 2011;22(1):83–6. |
| 5, 11. | ↑ | McKenzie WS, Rosenberg M. Iatrogenic subcutaneous emphysema of dental and surgical origin: a literature review. → J Oral Maxillofac Surg. 2009 Jun;67(6):1265–8. |
| 6, 14. | ↑ | Tomasetti P, Kuttenberger J, Bassetti R. Distinct subcutaneous emphysema following surgical wisdom tooth extraction in a patient suffering from “Gilles de la Tourette syndrome”. → J Surg Case Rep. 2015 Jun 14;2015(6). pii: rjv068. doi: 10.1093/jscr/ rjv068. |
| 7, 18. | ↑ | Mitsunaga S, Iwai T, Kitajima H, Yajima Y, Ohya T, Hirota M, Mitsudo K, Aoki N, Yamashita Y, Omura S, Tohnai I. Cervicofacial subcutaneous emphysema associated with dental laser treatment. → Aust Dent J. 2013 Dec;58(4):424–7 |
| 8. | ↑ | Parkar A, Medhurst C, Irbash M, Philpott C. Periorbital oedema and surgical emphysema, an unusual complication of a dental procedure: a case report. → Cases J. 2009 Sep 1;2:8108. doi: 10.4076/1757-1626-2-8108. |
| 10. | ↑ | Sahoo NK, Singh S, Roy ID, Bhandari A. Early postoperative malignant subcutaneous emphysema: report and review. → J Maxillofac Oral Surg. 2017 Mar;16(1):85–9. |
| 12, 22. | ↑ | Farina R, Zaetta A, Minenna L, Trombelli L. Orbital and periorbital emphysema following maxillary sinus floor elevation: a case report and literature review. → J Oral Maxillofac Surg. 2016 Nov;74(11):2192.e1–2192.e7. doi: 10.1016/j. joms.2016.06.186. Epub 2016 Jul 1. |
| 13. | ↑ | 4. |
| 15, 23. | ↑ | Arai I, Aoki T, Yamazaki H, Ota Y, Kaneko A. Pneumomediastinum and subcutaneous emphysema after dental extraction detected incidentally by regular medical checkup: a case report. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Apr;107(4):e33–8. doi: 10.1016/j. tripleo.2008.12.019. |
| 16, 21, 24. | ↑ | Tan S, Nikolarakos D. Subcutaneous emphysema secondary to dental extraction: a case report. → Aust Dent J. 2017 Mar;62(1):95–7. |
| 17, 25. | ↑ | Khandelwal V, Agrawal P, Agrawal D, Nayak PA. Subcutaneous emphysema of periorbital region after stainless steel crown preparation in a young child. → BMJ Case Rep. 2013 May 22;2013. pii: bcr2013009952. doi: 10.1136/ bcr-2013-009952. |
| 19, 26. | ↑ | Al-Qudah A, Amin F, Hassona Y. Periorbital emphysema during endodontic retreatment of an upper central incisor: a case report. → Br Dent J. 2013 Nov 8;215(9):459–61. |
| 20, 27. | ↑ | Imai T, Michizawa M, Arimoto E, Kimoto M, Yura Y. Cervicofacial subcutaneous emphysema and pneumomediastinum after intraoral laser irradiation. → J Oral Maxillofac Surg. 2009 Feb;67(2):428–30. |
| 28. | ↑ | Stacchi C, Sentineri R, Berton F, Lombardi T. Conjunctival chemosis: an uncommon complication after transcrestal lifting of the sinus floor. → Br J Oral Maxillofac Surg. 2016 Nov;54(9):1052–4. |
| 31. | ↑ | Kung JC, Chuang FH, Hsu KJ, Shih YL, Chen CM, Huang IY. Extensive subcutaneous emphysema after extraction of a mandibular third molar: a case report. → Kaohsiung J Med Sci. 2009 Oct;25(10):562–6. |





Leave a Reply
Be the First to Comment!